Submitted:
25 April 2026
Posted:
28 April 2026
You are already at the latest version
Abstract
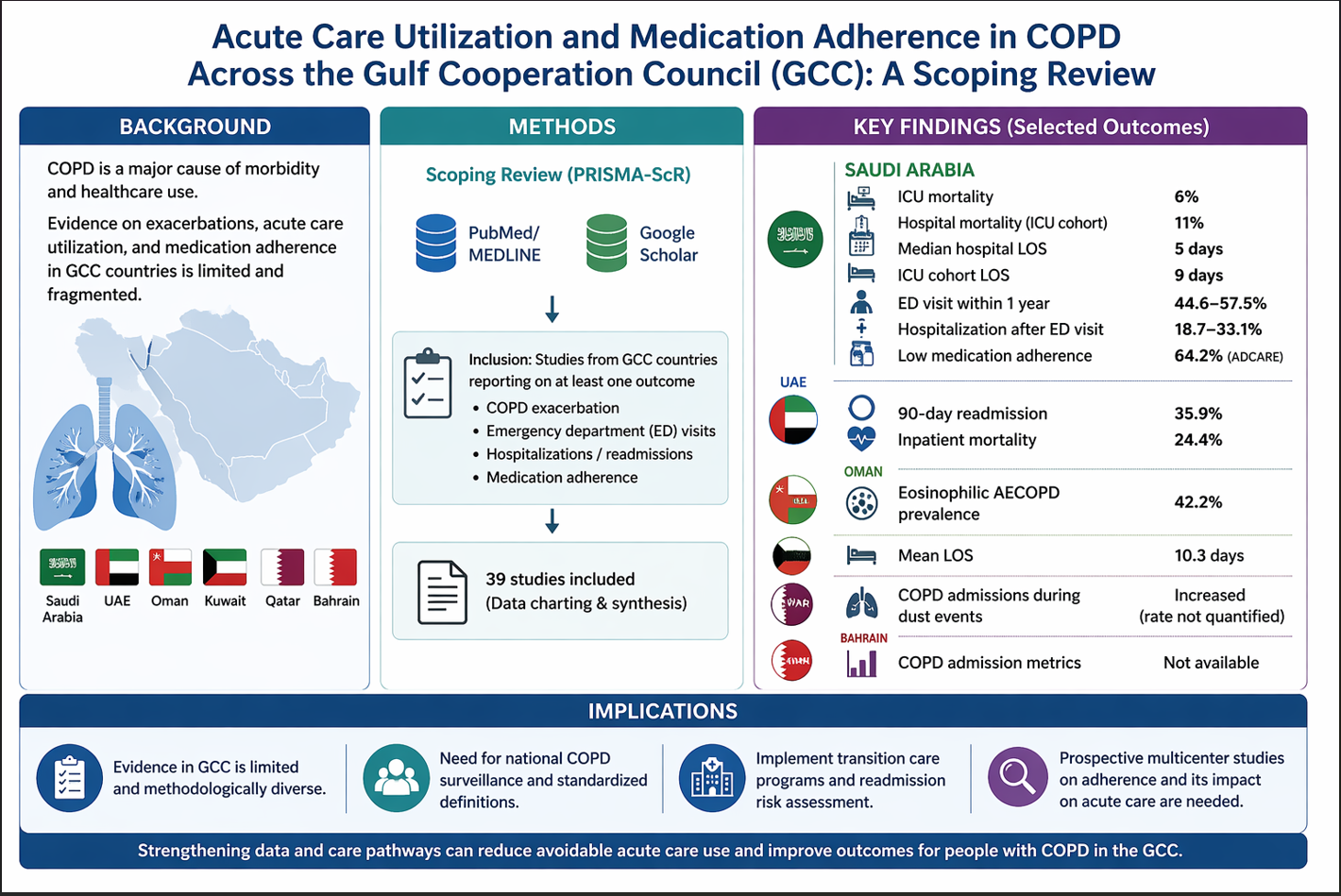
Background: Chronic obstructive pulmonary disease (COPD) remains one of the major sources of morbidity and mortality worldwide. The disease leads to considerable use of acute care due to exacerbations. This scoping review aimed to map and characterize the available literature on exacerbations, emergency department (ED) visits, hospitalizations/re-admissions, and medication compliance among patients with COPD in Gulf Cooperation Council (GCC) as region-specific evidence remains fragmented.
Methods: This scoping review adhered to the PRISMA-ScR guidelines. The databases searched were PubMed/MEDLINE and Google Scholar (last search date: February 1, 2026). Eligible studies were those carried out in GCC nations or providing estimates for GCC nations on at least one outcome measure of interest, such as COPD exacerbation, ED visits, hospitalizations, rehospitalizations, and/or adherence to medications. Two-phase screening (title and abstract, followed by full article) and standardized data charting, along with evidence synthesis and tabulation, were conducted.
Results: The evidence base in Saudi Arabia and the United Arab Emirates (UAE) generally consisted of retrospective cohorts (hospital/ICU) and adherence/utilization studies. In Saudi Arabia, ICU mortality was found to be 6%, while hospital mortality for those admitted into the ICU for COPD exacerbation was 11%. The median length of stay (LOS) for patients was 5 days. Notably, one study examining the relationship between adherence and utilization found higher 1-year ED visits and post-ED hospitalization for low-adherence patients (n = 266). In the UAE (multicenter study, n = 512), the 90-day readmission rate was 35.9% and the mortality rate was 24.4% for patients admitted with acute exacerbation, with a DECAF score AUC ≈0.8 for predicting mortality and 90-day readmission. In Oman, evidence on hospitalized acute exacerbation (n = 102) showed that patients with eosinophilia had a shorter LOS but a higher 1-year readmission rate. Few studies in Kuwait and Qatar provided direct evidence (e.g., older inpatient exacerbation or environmental-trigger studies), while Bahrain lacked specific studies in COPD acute care.
Conclusions: Evidence concerning acute-care use associated with COPD in the GCC region is limited and methodologically diverse. It is therefore imperative that a national COPD surveillance program be implemented, adopting uniform criteria regarding the definition of time periods related to exacerbations, admissions, and readmissions. Multicenter prospective studies assessing compliance and its association with acute care are warranted. Transition care programs and readmission risk assessment in acute exacerbations should be key objectives.
Keywords:
chronic obstructive pulmonary disease (COPD)
; acute exacerbation of COPD (AECOPD)
; acute-care utilization
; hospitalization
; readmission
; emergency department visits
; medication adherence
; Gulf Cooperation Council (GCC)
1. Introduction
Chronic obstructive pulmonary disease (COPD) is a prevalent, preventable lung condition that is defined by persistent respiratory symptoms and airflow obstruction. Worldwide, COPD continues to be a leading cause of mortality and morbidity. According to the World Health Organization, the estimated number of COPD deaths reached 3.5 million (about 5% of all deaths globally) in 2021.[1] Data provided by the Global Burden of Disease study recorded about 212 million prevalent cases of COPD in 2019, alongside 3.3 million COPD deaths and tens of millions of disability-adjusted life years.[2] COPD exacerbations account for a considerable portion of health care utilization and related costs, which include emergency department (ED) visits, hospitalizations, and multiple admissions, especially among older patients with multiple health problems. In Gulf Cooperation Council (GCC) health care systems, given the rapid rate of demographic shifts, high cardiometabolic comorbidity levels, and risk factors linked to COPD, such as tobacco smoking, exposure to dusts/fumes at work, and outdoor air pollution, COPD exacerbation and readmission issues are central topics in assessing quality and capacity.[1] Nonetheless, there exists no clear literature review on these issues in GCC nations.
Adherence to medications is a modifiable determinant of the outcomes of COPD, including symptom management and exacerbation reduction. For instance, the ADCARE study performed in Saudi Arabia and Turkey confirmed that adherence to COPD treatments is generally poor and correlated with increased impacts of the disease and lower quality of life, which underlines the importance of adherence research in relation to the exacerbation-related utilization of healthcare services in the GCC region.[3] Nevertheless, GCC-specific exacerbation utilization measures, such as ED visits, hospitalizations, and readmissions, have been rarely documented beyond Saudi Arabia and the United Arab Emirates (UAE).
This scoping review aims to synthesize existing peer-reviewed and grey literature discussing COPD exacerbation, ED visits, admissions/readmissions, and medication adherence among GCC countries to outline evidence gaps within this area of research.
2. Methods
This scoping review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines.[4] Prior to starting this project, a review protocol was formulated based on the aims of the exploratory study, which involved examining the breadth, scope, and nature of the evidence on the use of acute care services and adherence to medications among COPD patients in the GCC region. The selection of scoping review methodology was based on the heterogeneity of the studies that exist in the field, which prevents quantitative analysis yet allows for comprehensive evidence mapping.
Eligibility criteria were set before article selection and are presented in Table 1. The studies were considered for inclusion when their subjects were human patients with COPD, whether they involved cohorts with COPD exacerbations or subjects reporting acute care utilization or medication adherence outcomes. An outcome of interest had to be present within at least one category out of the following: COPD exacerbations (definitions taken verbatim from sources whenever possible), ED visits, hospitalizations, re-hospitalizations (within timeframes of 28-day, 30/31-day, 90-day, or 1-year), or medication adherence measured through validated self-report tools (e.g., Morisky Medication Adherence Scale (MMAS-8)), refill-based metrics such as medication possession ratio (MPR), or inhaler-based measures. Moreover, only those studies published within GCC nations (Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and the UAE) or international studies providing GCC country-specific information were be selected. Sources used in this study include peer-reviewed journal articles, conference papers, dissertations and theses, government and health system reports, and preprints. Studies excluded from this review included non-human studies, studies not containing GCC-specific data, studies providing only the prevalence of COPD without any outcome measure, and editorials without any primary data.
Literature review was carried out using PubMed/MEDLINE as the primary search engine and Google Scholar as the secondary search engine. Keywords and phrases were generated from specific subject areas related to GCC nations and grey literature. This process involved an iterative search approach. Details of the searches performed can be found in Appendix A.
Study selection consisted of a two-step procedure. First, independent screening of titles and abstracts was conducted to assess their eligibility, and then full-text screening was done on potentially relevant studies. Data extraction was done using a standardized data-charting form. The extracted variables were study characteristics (i.e., author name, publication year, country, research design, study setting), definition of outcome measures and duration, and key findings. Other variables extracted were frequency and estimate of effect size (when provided along with their confidence intervals), reason for hospitalization or readmission (e.g., infection, pneumonia, or comorbidity decompensation), hospital stay duration, mortality outcome measures, methods and frequency of adherence measurement, interventions (when available), predictors or risk factors, statistical method, and study limitations. Data not captured or unavailable were indicated as "unspecified".
Following the scoping review protocol, no exclusions were made based on methodological quality. Nevertheless, to improve understanding of results, an assessment of methodological rigor was undertaken using relevant Joanna Briggs Institute (JBI) critical appraisal checklists, depending on design (e.g., cross-sectional and cohort studies). Moreover, the likelihood of publication in predatory journals was considered on a qualitative basis where applicable, especially for studies that lacked clear indexing and editorial processes; those studies were kept, though highlighted during synthesis.
Since there was great variability in terms of the population (ICU, inpatients, outpatients, and survey samples), design, and definition of outcomes between studies, meta-analysis could not be conducted. Instead, the results were analyzed via narrative synthesis, taking into consideration ranges of outcomes by country and outcome type, commonly found reasons for hospitalization, as well as potential predictors and risk factors for GCC countries.
3. Results
3.1. Study Selection
The PRISMA-ScR flow diagram of the study selection process is provided in Figure 1, and additional information is available in Supplementary Material B. From the search results, only a few articles were found that reported information regarding the utilization of acute care and adherence to medication among GCC countries with COPD. The overall evidence pool was not evenly distributed in the GCC countries. Most of the selected studies were from Saudi Arabia and the UAE, whereas there were considerably fewer articles from Kuwait, Oman, Qatar, and Bahrain.
3.2. Study Characteristics
The characteristics of the studies included are described in Table 2. In terms of design, the majority of articles were observational retrospective cohort studies based on electronic medical record data, especially from Saudi Arabia and the UAE. Moreover, multicenter cross-sectional studies assessing medication adherence were included, especially from Saudi Arabia.
Other studies were conducted in specific populations, such as those with acute exacerbation needing hospitalization or ICU care. For instance, a study conducted in Saudi Arabia was conducted in an acute exacerbation population that needed ICU admission. A multicenter cohort study in the UAE assessed the DECAF score for patients with acute exacerbations, reporting inpatient mortality and 90-day readmission outcomes.
Data relating to other GCC countries was highly variable and sparse. For example, an observational study conducted at a hospital in Oman looked at the association between eosinophilia and outcomes, such as length of stay (LOS) and one-year readmission rates. Cohort data from Kuwait included information regarding factors affecting prognosis and the average hospital LOS for COPD exacerbation patients. Information from Qatar and Bahrain was limited, focusing mostly on general utilization related to respiratory conditions or environmental triggers, rather than COPD outcomes. See Figure 2.
3.3. Utilization Outcomes, Readmissions, and Mortality
3.3.1. Hospital Admissions and Length of Stay (LOS)
The average LOS in the hospital among COPD patients in Saudi Arabia admitted from 2017 to 2022 was 5 days, with male gender and presence of cancer among the factors that could result in an extended hospital stay. Among COPD patients who needed ICU admissions due to exacerbations, their median LOS was 9 days, while their median ICU LOS was 3 days. In Kuwait, the average hospital LOS among COPD patients was 10.3 days, with adverse prognostic indicators such as comorbidity, acidemia, and mechanical ventilation.
3.3.2. Readmissions
The strongest evidence for readmission rates comes from a study conducted in the UAE that involved multiple centers (n = 512), which reported a 90-day readmission rate of 35.9% for patients admitted with an exacerbation of the disease. Eosinophilic exacerbations in Oman had higher one-year readmission rates when compared to non-eosinophilic exacerbations, although the absolute readmission rates were not consistently reported.
3.3.3. Mortality
The estimates on mortality varied widely between countries and different health facilities, see Figure 3. For instance, in a Saudi ICU cohort study, the mortality estimates were 6% and 11%, respectively, for ICU admissions and overall hospital admissions for COPD exacerbations. Another study conducted in the UAE reported a mortality rate of 24.4% for hospitalized exacerbation cases. This disparity may be attributed to different factors affecting both patient populations and healthcare environments.
3.3.4. Reasons for Admission and Readmission
Respiratory infections were identified as the main cause of acute-care use across different studies. Respiratory infections contributed to 86% of the incidence of acute respiratory failure among ICU patients in Saudi Arabia. Similarly, regional evidence from Oman showed that diseases of the respiratory system and pneumonia were highly over-represented among initial readmissions, which further emphasizes the significance of infectious causes in COPD-associated healthcare utilization. See Figure 4.
3.4. Medication Adherence and Associations with Acute-Care Utilization
The medication adherence results are shown in Table 3, which were based on two types of measurements for adherence: self-reported adherence and objective refill-based adherence.
3.4.1. Self-Reported Adherence
According to a large cross-sectional study performed in Saudi Arabia (ADCARE study), 64.2% of patients suffering from COPD were characterized by poor adherence (MMAS-8 score ≤ 6), while 11.6% patients demonstrated high adherence. Furthermore, at least one exacerbation occurred in 61.3% of patients in the previous year, defined as a hospitalization or ED visit. Poor adherence correlated with high disease burden, poor quality of life, and high levels of depression, which proved to be the main predictors of non-adherence.
3.4.2. Objective Adherence (Refill-Based Measures)
In a retrospective cohort study conducted in Saudi Arabia (n = 266), utilizing fixed medication possession ratio (FMPR) as an adherence measure, low adherence (FMPR <0.80) was shown to correlate with increased healthcare utilization. Patients with low adherence had higher rates of ED visits (57.5% vs. 44.6%) and subsequent hospitalizations (33.1% vs. 18.7%). Overall, a statistically significant difference in the LOS was not detected.
3.5. External Regional Context
Additional details were obtained from the BREATHE study[5], which was a multinational survey conducted among Middle East and North Africa countries, including Saudi Arabia and the UAE (Table 2). In this study, physician visits, use of emergency departments, and hospital admissions were estimated among the participants in addition to the symptom burden. The study is not restricted to the GCC countries, but it is a rare source that provides data on COPD-related healthcare utilization for multiple countries.
3.6. Critical Appraisal Summary
The quality of the studies included differed. Many were observational, and the majority were designed as retrospective cohort studies. Other limitations were lack of control for confounders, missing information on relevant study population characteristics, or self-reported adherence in included cross-sectional studies. However, multicenter cohort studies provided higher quality data concerning outcome assessment and reporting. Governmental and ecological data provided information on relevant contextual factors. Moderate quality evidence base. Overall, the body of evidence was of moderate quality, see Table 4.
4. Discussion
According to the above scoping review, there is a shortage of existing evidence related to COPD exacerbations, ED visits, hospitalizations and re-hospitalizations, mortality rates, and medication adherence within the GCC. While most of the direct evidence was provided for countries such as Saudi Arabia and the UAE, other regions, such as Kuwait, Oman, Qatar, and Bahrain, have little evidence on COPD and medication adherence. Notwithstanding those gaps, there are certain implications concerning acute care utilization and adherence behavior among patients with COPD found in the existing studies. In other words, COPD and health services utilization within the GCC are relevant clinically, but the evidence base is limited by inconsistent outcome definitions, variable study populations, and heterogeneous adherence measurement tools.
Acute exacerbations of COPD continue to be a major contributor to emergency department visits and hospital admissions across healthcare systems. Patients commonly present with sever dyspnea requiring rapid stabilization, bronchodilator therapy, and oxygen guidelines.[6,7] Recurrent ED utilization is frequently linked to poor medication adherence and suboptimal outpatient dieses control, underscoring the importance of discharge education and continuity of care to reduce future exacerbation and readmissions.[8,11] In the GCC context, this pattern may further reflect gaps in access to structured outpatient follow-up and variability in chronic disease management across healthcare settings.
Several recurring themes were observed across the articles selected for analysis. First, infections and pneumonia play a significant role in hospitalizations and early hospital readmission. These assertions are corroborated by findings in Saudi Arabia, which show that infection played a key role in acute respiratory failure among ICU-admitted COPD cases and by readmission figures from Oman, where an overrepresentation of respiratory diseases and pneumonia was observed.[9,17] Second, medication non-adherence was a recurring theme in all studies from Saudi Arabia, regardless of whether it was measured through subjective self-reporting measures such as MMAS-8 or objective refill-based measures such as the FMPR. Non-compliance was linked to poor health status, quality of life, and increased acute-care utilization.[12,3] Third, the burden of readmissions may be high in the UAE; a multicenter study found that over a third of patients hospitalized for exacerbations had been readmitted within 90 days. In conclusion, these findings suggest that the management of COPD in the GCC is influenced not only by the severity of the condition but also by infection-related triggers, discontinuity of care, and compliance issues.
A comparison with other studies conducted around the world reinforces the importance of these results. The rates of readmission for COPD differ greatly among various countries due to the healthcare system, coding, severity criteria, and follow-up definitions. In other studies, the rate of 30-day readmissions was between 8.8% and 26.0%, whereas the rate of 90-day readmissions was between 17.5% and 39.0%.[18] Considering this information, the 90-day readmission rate estimated for the UAE (35.9%) falls in the upper range of published readmission rates.[12,18] Although caution should be exercised when comparing results directly, due to differences in sample selection and study methodology, these findings suggest that readmissions contribute significantly to the problem in some GCC countries.
Implications of the studies reviewed are extremely relevant to the healthcare system planning and policy of the GCC region. COPD exacerbations are a burden for hospitals due to the strain placed on hospital beds, emergency services, and patient discharge management programs. For tertiary centers serving complex and multimorbid patients, measures related to care transition would have positive impacts on patient outcomes. Such measures might encompass drug reconciliation, assessment of inhaler technique, early follow-ups, discharge advice, and adherence assistance.[1,18] The results suggest that regional characteristics need to be considered when developing preventive and treatment policies in the GCC countries. Apart from the impact of tobacco smoking, exposure to occupational and environmental agents such as indoor pollutants, dust, and particulate matter could play a role in the burden of COPD and its exacerbations in GCC countries.[1,19] Consequently, GCC countries need to develop their COPD policies based on both clinical and environmental risk factors.
4.1. Implications
The findings of this review have several implications for the management of COPD and other chronic respiratory diseases within the GCC healthcare system. First, there should be standardized approaches to measuring disease outcomes in terms of exacerbations, admissions, and readmissions. More precise definitions for these factors could increase comparability in future studies, which will allow for effective benchmarking of hospitals and countries in terms of their achievements.[18] Additionally, standardized definitions could facilitate the organization of future multicenter studies and registries.
Second, the existing data provides strong evidence for the introduction of discharge bundles for high-risk groups of patients. Individuals who suffer from COPD accompanied by comorbidities, take multiple medications, experience frequent exacerbations, or demonstrate poor compliance with treatment regimens can particularly benefit from such programs.[11,17] Since non-adherence was identified as a factor associated with poorer outcomes, patient education should be regarded as an integral part of COPD treatment rather than a separate process.
Third, the review emphasizes the need to build multicenter registries of COPD patients in the GCC region, specifically those with inadequate evidence bases. The optimal composition of a registry would entail the inclusion of spirometry-confirmed diagnoses, disease severity, comorbidities, environmental risk factors, medications used, and post-discharge indicators, such as re-hospitalization rates and mortality.[11,3] Such registries would serve to strengthen surveillance, enhance benchmarking, and identify predictors of poor health outcomes.
Lastly, future research must incorporate holistic methods for assessing adherence. A multi-modal strategy involving the use of refill-based assessments, valid self-reports, and direct observations would result in a better-informed understanding of adherence and how it is connected to the incidence of emergencies, admissions, and re-admissions. Prospective studies would be highly beneficial in determining modifiable risk factors.
4.2. Health-System Context and GCC Benchmarking
The health system perspective of the GCC should be taken into consideration when discussing the implications of the findings of the current study. Many countries in this region depend on tertiary/quaternary centers for managing complicated diseases such as respiratory conditions, which might lead to the higher identification of severe COPD cases during clinical studies conducted in hospitals. Such a scenario may partly account for the high mortality and readmission rates recorded by some of the selected populations in the literature.[9,12] However, inadequate follow-up and a lack of organized programs to manage chronic illnesses may lead to avoidable utilization rates.
Comparing the results of GCC studies with global statistics is helpful, though it requires much carefulness due to differences in the precision of coding, criteria for admissions, discharges, and availability of healthcare facilities that could significantly impact the application of such measures. Nevertheless, available GCC literature reveals that the frequency of hospitalizations due to COPD should not be neglected, as it can equal or even surpass the global statistics.[18] Therefore, improvement in surveillance activities and incorporation of indicators of quality care into COPD management could become necessary. This benchmarking may allow us to pinpoint high-quality care models, leading to optimal resource allocation in the future.
4.3. Strengths and Limitations
There are various strengths of the scoping review. It is a well-conducted synthesis of the evidence regarding the use of acute care facilities and adherence to medications in COPD patients within the GCC region. Data on this issue is widely dispersed and difficult to collectively interpret. When carrying out the scoping review, the authors considered various information sources, ranging from peer-reviewed articles to grey literature. This helped to cover all possible gaps in the GCC region literature. Lastly, the choice of conducting a scoping review on the matter was justified due to the diversity of available evidence.[4]
Nonetheless, the study has several limitations. First, there were substantial disparities between countries. Literature on the utilization and readmission rates of COPD patients from Bahrain, Qatar, and Kuwait was lacking, whereas scarce single-center data from Oman were available.[14,15,16,17] Second, there were inconsistencies regarding the definition of exacerbations from each source. While some studies used either admission or visits to the ED to determine an exacerbation episode, other studies employed either clinically diagnosed or coded exacerbations.[8,3] Finally, the outcomes were not reported in a uniform manner. Information regarding the confidence interval or multivariate effect estimates was rarely provided, preventing deeper quantitative interpretation.[8,11]
Other limitations include those associated with biases in publications and indexing. The information regarding the GCC may have been found in other sources, such as locally published journals, conference presentations, institutional dashboards, and governmental reports, which are not indexed in major biomedical databases or freely available online. Therefore, existing literature may not represent the full scope of regional data. In addition, the review has been limited by the inability to access certain subscription-based databases to conduct full exports and deduplications, as well as the need for repeated searches for gray literature. The latter makes it impossible to provide an exact PRISMA count report. Finally, the lack of causation between adherence and risk factors in relation to outcomes can be noted because of the nature of the included research studies.
In summary, the findings from the current systematic review highlight the clinical importance of acute-care usage among COPD patients in the GCC and the need for multicenter research. It is now imperative to construct a strong foundation for COPD policymaking and care continuity improvements.
5. Conclusion
Most research conducted on the utilization of acute care services and medication compliance in COPD patients has been predominantly undertaken in Saudi Arabia and the UAE, with very little and inconsistent data on such parameters in other GCC countries. The lack of a standardized definition for outcome measures, measurement techniques, and target populations poses difficulties when comparing results or setting benchmarks between different nations.
Future research needs to move beyond fragmented, unorganized studies to systematic efforts. Goals for future research include defining terms for COPD exacerbations and admissions, including 30- and 90-day criteria; developing multi-center registries that consider spirometry-verified information on disease severity, co-morbidity, and medication compliance with clinical endpoints; and evaluating transitional care initiatives to reduce avoidable hospital admissions. This will be critical in achieving consistency in the management of COPD in the GCC health systems.
Author Contributions
Conceptualization, A.E.; methodology, A.E., software, A.E.; I.S.; validation, I.S.; A.A.; O.A.; S.A.; formal analysis, I.S.;O.A.; investigation, A.E.; I.S.;, A.A.; O.A.; S.A.; resources, I.S.;, A.A.; O.A.; S.A.; data curation, A.E.; I.S.; writing—original draft preparation, A.E.; I.S.;, A.A.; O.A.; S.A.; writing—review and editing, A.E.; I.S.;, A.A.; O.A.; S.A.; visualization, A.E.; A.A.; supervision, A.E.; project administration, A.E.: All authors have read and agreed to the published version of the manuscript.
Funding statement: This research received no external funding.
Data Availability:No new data were created or analyzed in this study.
Acknowledgments
The authors thank the College of Health Sciences at the University of Doha for Science & Technology for the support of the study.
Conflicts of interest
The authors report there are no competing interests to declare.
References
- World Health Organization. Chronic obstructive pulmonary disease (COPD) fact sheet. Updated 6 November 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd) (accessed on 1 March 2026).
- Safiri, S.; Carson-Chahhoud, K.; Noori, M.; Nejadghaderi, S.A.; Sullman, M.J.M.; Ahmadian Heris, J.; Ansarin, K.; Mansournia, M.A.; Collins, G.S.; Kolahi, A.A.; et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990–2019: Results from the Global Burden of Disease Study 2019. BMJ 2022, 378, e069679. [Google Scholar] [CrossRef] [PubMed]
- Al Sibani, M.; Al Alawi, A.M.; Al Aghbari, J. Elevated peripheral blood eosinophils during acute exacerbation of chronic obstructive pulmonary disease: Prevalence and clinical significance. Sultan Qaboos Univ. Med. J. 2022, 22, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Polatli, M.; Ben Kheder, A.; Wali, S.; Javed, A.; Khattab, A.; Mahboub, B.; et al. Chronic obstructive pulmonary disease and associated healthcare resource consumption in the Middle East and North Africa: The BREATHE study. Respir. Med. 2012, 106, S75–S85. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2024 report.
- Ford, E.S. Hospital discharges, readmissions, and emergency department visits for COPD or bronchiectasis among US adults: findings from national datasets. Chest 2015, 147(4), 989–998. [Google Scholar] [CrossRef] [PubMed]
- Stolz, D.; Kostikas, K.; Blasi, F.; Boersma, W.; Milenkovic, B.; et al. COPD exacerbations: a clinical update. Eur. Respir. Rev. 2018, 27(147), 170103. [Google Scholar] [CrossRef]
- Alaithan, A.M.; Memon, J.I.; Rehmani, R.S.; Qureshi, A.A.; Salam, A. Chronic obstructive pulmonary disease: Hospital and intensive care unit outcomes in the Kingdom of Saudi Arabia. Int. J. Chron. Obstruct. Pulmon. Dis. 2012, 7, 819–823. [Google Scholar] [CrossRef] [PubMed]
- Alotaibi, T.F.; Othman, F.; Alrasheed, B.A.; Aldraiwish, B.M.; Alharthi, M.M.; Alotaibi, H.G.; Alghamdi, A.S.; Aljohani, H.; Alqahtani, M.M.; Ismaeil, T.T.; et al. Length of stay and comorbidity prevalence among individuals with chronic obstructive pulmonary disease in a tertiary care healthcare center in Saudi Arabia: A cross-sectional study. Medicine 2025, 104, e41855. [Google Scholar] [CrossRef] [PubMed]
- Alshehri, S.; Alshibani, M. Impact of medication adherence on emergency department visits in patients with COPD in a single tertiary hospital in Saudi Arabia. Int. J. Chron. Obstruct. Pulmon. Dis. 2023, 18, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Almarshoodi, K.; Echevarria, C.; Kassem, A.; Mahboub, B.; Salameh, L.; Ward, C. An international validation of the DECAF score to predict disease severity and hospital mortality in acute exacerbation of COPD in the UAE. Hosp. Pharm. 2024, 59, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Kokturk, N.; Polatli, M.; Oguzulgen, I.K.; Saleemi, S.; Al Ghobain, M.; Khan, J.; Doble, A.; Tariq, L.; Aziz, F.; El Hasnaoui, A. Adherence to COPD treatment in Turkey and Saudi Arabia: Results of the ADCARE study. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 1377–1388. [Google Scholar] [CrossRef] [PubMed]
- Onadeko, B.O.; Khadadah, M.; Abdella, N.; Mukhtar, M.; Mourou, M.; Qurtom, M.; Samad, M.; Al-Shayeb, A. Prognostic factors in the management of exacerbation of chronic obstructive pulmonary disease in Kuwait. Med. Princ. Pract. 2005, 14, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Bener, A.; Dogan, M.; Ehlayel, M.S.; Shanks, N.J.; Sabbah, A. The impact of air pollution on hospital admission for respiratory and cardiovascular diseases in an oil and gas-rich country. Eur. Ann. Allergy Clin. Immunol. 2009, 41, 80–84. [Google Scholar] [PubMed]
- Bahrain Ministry of Health. Annual Health Statistic 2021–2022 Report (Arabic). Available online: https://www.moh.gov.bh/Content/Upload/File/638728900891148417-Annual-Health-Statistic-2021-2022--Report_ar.pdf (accessed on 14 February 2026).
- Al Sibani, M.; Al-Maqbali, J.S.; Yusuf, Z.; Al Alawi, A.M. Incidence and risk factors for 28 days hospital readmission: A retrospective study from Oman. Oman Med. J. 2022, 37, e423. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, J.S.; Njoku, C.M.; Bereznicki, B.; Wimmer, B.C.; Peterson, G.M.; Kinsman, L.; Aldabayan, Y.S.; Alrajeh, A.M.; Aldhahir, A.M.; Mandal, S.; et al. Risk factors for all-cause hospital readmission following exacerbation of COPD: A systematic review and meta-analysis. Eur. Respir. Rev. 2020, 29, 190166. [Google Scholar] [CrossRef] [PubMed]
- Albahar, S.; Li, J.; Al-Zoughool, M.; Al-Hemoud, A.; Gasana, J.; Aldashti, H.; Alahmad, B. Air pollution and respiratory hospital admissions in Kuwait: The epidemiological applicability of predicted PM2.5 in arid regions. Int. J. Environ. Res. Public Health 2022, 19, 5998. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA-ScR study selection flow chart.

Figure 2.
Conceptual pathway linking COPD severity, comorbidities, environmental exposures, medication adherence, and acute care utilization and readmission risk.
Figure 2.
Conceptual pathway linking COPD severity, comorbidities, environmental exposures, medication adherence, and acute care utilization and readmission risk.

Figure 3.
Outcome Ranges for selected COPD acute-care endpoints across included GCC sources.

Figure 4.
Frequency of reported reasons for COPD admission/readmission across included GCC sources.


Table 1.
Inclusion/exclusion criteria for article selection.
| Criteria | Inclusion | Exclusion |
|---|---|---|
| Research focus | COPD-related acute-care utilization and/or medication adherence; GCC-country–specific data (Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, the UAE); human participants | Not COPD-focused; no acute-care utilization or adherence outcome; no GCC-specific results (region aggregated only); non-human/in vitro |
| Study design | Observational quantitative (cohort, case–control, cross-sectional, time-series); interventional(RCT,quasi-experimental); qualitative/mixed-methods;registry/administrative datasets with defined COPD criteria | Reviews (narrative/systematic/scoping) and meta-analyses (for inclusion as evidence); protocols without results; editorials/letters/opinions without primary data; animal models |
| Language | English; Arabic (if translation is feasible by the review team) | Languages not feasible for screening/translation by the review team |
| Publication year | No date restriction; database inception to the last search date | Published after the last search date |
| Population | Adults with clinician- or spirometry-confirmed COPD; acute exacerbation cohorts; COPD-coded administrative datasets when the COPD case definition is stated | Asthma-only; non-COPD respiratory conditions without separable COPD subgroup; pediatric-only populations; mixed cohorts without extractable COPD-specific results |
| Setting and geography | GCC countries; any care setting (ED, inpatient, ICU, outpatient, community) | Outside GCC; multi-country studies with only aggregated results (no GCC-country estimates) |
| Outcomes (≥1 required) | Exacerbations (as defined by source); ED visits; hospital admissions; LOS; mortality (ICU/inpatient/short-term as reported); readmission/revisit (e.g., 28/30/90-day, 1-year); adherence/persistence (e.g., MMAS, MPR/PDC/FMPR, inhaler adherence) | No target outcomes; COPD prevalence-only studies; physiologic-only studies without utilization/adherence endpoints |
| Publication type/status | Peer-reviewed full-text articles; preprints; theses/dissertations; government/health-system reports; conference abstracts/proceedings with extractable outcomes | Duplicate publications; abstract-only records without extractable data; non-scholarly media; commentary pieces |
| Full-text availability | Full text retrievable (open access, institutional access, author contact) with sufficient detail for screening and data charting | Full text not available; title/abstract insufficient for eligibility confirmation |
Table 2.
COPD Acute-Care Utilization Outcomes by Country.
| Country | Outcome | Value | Study |
|---|---|---|---|
| Saudi Arabia | ICU mortality | 6% | Alaithan 2012 |
| Saudi Arabia | Hospital mortality (ICU cohort) | 11% | Alaithan 2012 |
| Saudi Arabia | Median hospital LOS | 5 days | Alotaibi 2025 |
| Saudi Arabia | ICU cohort LOS | 9 days | Alaithan 2012 |
| Saudi Arabia | ED visit within 1 year | 44.6–57.5% | Alshehri 2023 |
| Saudi Arabia | Hospitalization after ED visit | 18.7–33.1% | Alshehri 2023 |
| Saudi Arabia | Low medication adherence | 64.2% | ADCARE |
| UAE | 90-day readmission | 35.9% | Almarshoodi 2023 |
| UAE | Inpatient mortality | 24.4% | Almarshoodi 2023 |
| Oman | Eosinophilic AECOPD prevalence | 42.2% | Al Sibani 2022 |
| Kuwait | Mean LOS | 10.3 days | Abdellaa 2005 |
| Qatar | COPD admissions during dust events | Increased (rate not quantified) | Bener 2009 |
| Bahrain | COPD admission metrics | Not available | MoH report |
Table 3.
Predictors/risk factors and effect sizes (where reported).
| Study | Outcome | Predictor | Effect |
|---|---|---|---|
| Kokturk 2018 | Low adherence | Depression | OR 2.50 |
| Kokturk 2018 | Low adherence | Living in Saudi vs Turkey | OR 3.20 |
| Kokturk 2018 | Lower disease impact | Adherent vs low adherence | OR 0.56 |
| Alotaibi 2025 | LOS | Male sex | +1.30 days |
| Alotaibi 2025 | LOS | Cancer | +2.73 days |
| Almarshoodi 2023 | Mortality prediction | DECAF score | AUROC ≈0.80 |
Table 4.
Joanna Briggs Institute (JBI) Critical Appraisal.
| Study | Country | Study Design | Selection Bias | Measurement Validity | Confounding | Outcome Reporting | Overall Appraisal |
|---|---|---|---|---|---|---|---|
| Alaithan et al., 2012 | Saudi Arabia | Retrospective cohort | Yes | Yes | No | Yes | Moderate |
| Alotaibi et al., 2025 | Saudi Arabia | Cross-sectional | Yes | Yes | No | Yes | Moderate |
| Alshehri et al., 2023 | Saudi Arabia | Retrospective cohort | Yes | Yes | Unclear | Yes | Moderate |
| Kokturk et al., 2018 | Saudi Arabia (subset) | Cross-sectional | Yes | No (self-report bias) | No | Yes | Low-Moderate |
| Almarshoodi et al., 2023 | UAE | Multicenter cohort | Yes | Yes | Yes | Yes | High |
| Al Sibani et al., 2022 | Oman | Retrospective cohort | Yes | Unclear | No | Yes | Moderate |
| Onadeko et al., 2005 | Kuwait | Observational cohort | Yes | Unclear | No | Yes | Moderate |
| Bener et al., 2009 | Qatar | Ecological/time-series | Yes | Yes | No | Yes | Moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



