Submitted:
20 April 2026
Posted:
21 April 2026
You are already at the latest version
Abstract
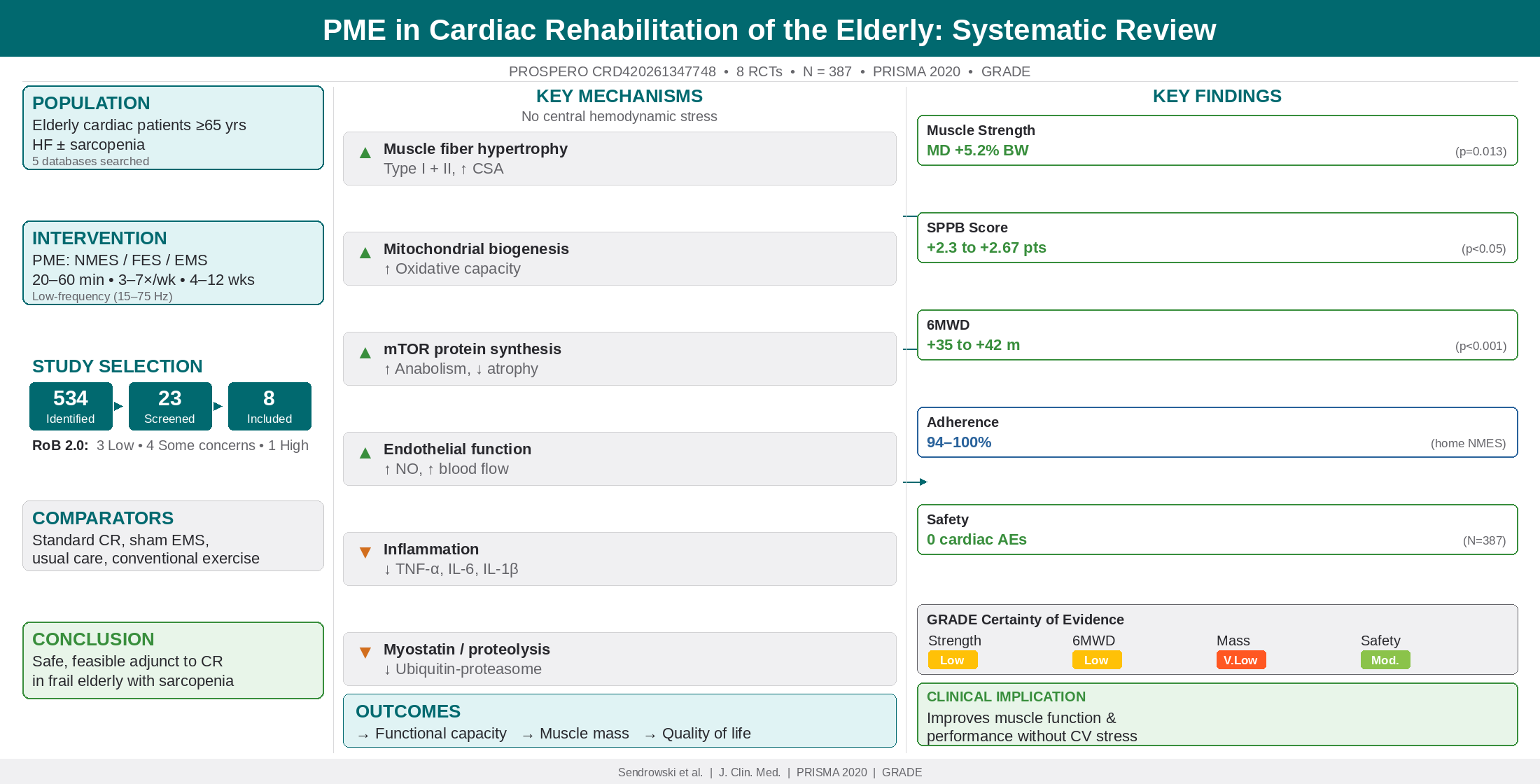
Background: Peripheral muscle electrostimulation (PME), including neuromuscular electrical stimulation (NMES) and functional electrical stimulation (FES), has been increasingly acknowledged as an effective adjunctive or complementary treatment to voluntary exercise in elderly cardiac patients who cannot perform sufficient amounts of voluntary exercise, with limited research on optimal protocols. Sarcopenia, defined as a progressive decrease in muscle mass, strength and function, affects approximately 34% of heart failure (HF) patients and considerably worsens their prognosis. The objective of this systematic review is to summarize the current evidence on the theoretical mechanisms, physiological pathways, safety and efficacy of PME in older adults within a cardiac rehabilitation (CR) setting with a specific emphasis towards sarcopenia reversal.
Methods: We performed a systematic review following PRISMA 2020 guidelines. A systematic search of the PubMed, Embase, Cochrane Library, CINAHL and PEDro databases from inception until December 2025 was conducted. We searched for randomized controlled trials (RCTs) and controlled clinical trials focusing on PME in patients with cardiac diseases aged 65 years or older. The main outcomes were physical function (assessed with the Short Physical Performance Battery [SPPB] and 6-minute walk distance [6MWD]), muscle strength, muscle mass, and safety. The Cochrane Risk of Bias tool was used for quality evaluation of the studies.
Results: Eight studies were included, with 387 participants and mean age between 78 to 85 years. PME consistently improved lower extremity muscle strength (MD: 5.2% body weight, 95% CI = 1.2–9.1, p = 0.013) along with SPPB scores ranging from +2.3 to +2.67 points (all p < 0.05). Home-based NMES achieved 100% adherence rates and no cardiovascular adverse events were reported. The mechanisms by which PME is beneficial involve peripheral skeletal muscle adaptations without eliciting central hemodynamic stress, increased endothelial function, aerobic enzyme activity, protein anabolism stimulation and muscle proteolysis inhibition. No significant effects were observed on BNP levels, hospital readmissions or mortality. PME has been shown to attenuate the progression of sarcopenia through hypertrophy of type I and II muscle fibers, as well as mitochondrial biogenesis.
Conclusions: PME is a safe, feasible adjunct to conventional CR in frail elderly cardiac patients, particularly those with exercise intolerance and sarcopenia. It improves peripheral muscle function, physical performance, and muscle protein balance without cardiovascular stress. Larger multicenter trials are needed to establish optimal protocols and long-term clinical outcomes.
Registration: PROSPERO CRD420261347748 (protocol registered prior to data extraction).
Keywords:
neuromuscular electrical stimulation
; functional electrical stimulation
; electrical muscle stimulation
; cardiac rehabilitation
; chronic heart failure
; elderly patients
; sarcopenia
; frailty
; cardiovascular disease
1. Introduction
1.1. Background and Rationale
Cardiovascular disease remains the leading cause of morbidity and mortality in older adults globally, with heart failure (HF) prevalence doubling with each decade after age 65. Exercise-based cardiac rehabilitation (CR) is a Class I recommendation for HF patients, demonstrating significant improvements in exercise capacity, quality of life, and reduced hospitalization risk [1,2]. However, participation rates remain critically low (19–34% in the US; <10% in Japan), particularly among frail elderly patients [3,4,5].
1.2. The Sarcopenia Crisis in Geriatric Cardiac Populations
Sarcopenia—derived from the Greek sarx (flesh) and penia (loss)—is defined as a progressive and generalized skeletal muscle disorder characterized by accelerated loss of muscle mass, strength, and physical performance. It represents one of the most critical geriatric syndromes affecting cardiac rehabilitation outcomes [6,7].
1.2.1. Epidemiology of Sarcopenia in Heart Failure
1.2.2. Pathophysiological Mechanisms: The Heart-Muscle Axis
The relationship between HF and sarcopenia is bidirectional and synergistic [7]:
HF leading to Sarcopenia (Cardiac Cachexia Pathway):
- Mitochondrial dysfunction: Impaired oxidative phosphorylation reduces ATP production, accelerating fatigue and disuse atrophy [7]
- Myosteatosis: Intramuscular fat infiltration reduces muscle quality independent of mass [7]
- Neurohormonal activation: Sympathetic overdrive and RAAS activation promote catabolism [10]
- Reduced perfusion: Impaired endothelial function limits oxygen and nutrient delivery to skeletal muscle [12]
Sarcopenia leading to HF Worsening:
- Reduced skeletal muscle pump: Impaired venous return decreases cardiac preload efficiency [12]
- Exercise intolerance: Limits participation in CR, creating vicious cycle of deconditioning [7]
- Insulin resistance: Worsens metabolic profile and cardiovascular risk [7]
- Increased fall risk: Leads to hospitalization and HF decompensation [8]
1.2.3. Prognostic Impact of Sarcopenia in HF
Sarcopenia independently predicts:
- All-cause mortality: HR 1.68 (95% CI 1.32–2.14) [6]
- All-cause mortality: HR 2.42 (HFpEF) and HR 2.02 (HFrEF) [13]
- HF hospitalization: HR 1.89 (95% CI 1.41–2.53) [8]
- Functional decline: 2.3-fold increased risk of ADL dependency [6]
- Post-operative complications: 3.1-fold increased risk after cardiac surgery [11]
Patients with both HF and sarcopenia have 50% mortality at 1 year after hospitalization and 65% readmission risk [8].
1.2.4. Diagnostic Challenges in HF Patients
Diagnosing sarcopenia in HF is complicated by:
- Fluid overload: Edema and ascites artificially inflate muscle mass measurements (e.g., bioimpedance, DEXA) [6]
- Overlap with frailty: 60–80% of sarcopenic HF patients meet frailty criteria; distinct but overlapping constructs [6]
- Lack of standardized cutoffs: EWGSOP2, AWGS, FNIH criteria yield different prevalence estimates [14]
Recommended diagnostic approach in HF:
1.3. Peripheral Muscle Electrostimulation: Theoretical Framework
Peripheral muscle electrostimulation (PME)—encompassing neuromuscular electrical stimulation (NMES), functional electrical stimulation (FES), and electrical muscle stimulation (EMS)—induces skeletal muscle contraction through transcutaneous electrical currents without requiring voluntary effort or increasing cardiac workload. This makes PME theoretically ideal for frail elderly cardiac patients who cannot tolerate conventional exercise training [15,16,17]. Figure 1 provides a schematic overview of the principal mechanisms by which PME exerts its beneficial effects in elderly cardiac rehabilitation patients.
The scientific rationale for PME in sarcopenic elderly cardiac patients rests on four pillars:
1.3.1. Direct Anti-Sarcopenic Effects
PME at appropriate frequencies (20–100 Hz) directly counteracts sarcopenia through:
- Proteolysis inhibition: NMES reduces ubiquitin-proteasome activity, decreasing 3-methylhistidine (marker of myofibrillar breakdown) excretion by 40% [11]
- Fiber-type transformation: Shifts type IIx (fast-glycolytic) to type IIa (fast-oxidative) and type I (slow-oxidative) fibers, reversing HF-related myopathy [12]
- Satellite cell activation: Stimulates muscle stem cell proliferation and differentiation, enhancing regenerative capacity [18]
1.3.2. Neural and Muscular Adaptations
1.3.3. Safety Profile: Hemodynamic Neutrality
1.3.4. Overcoming Anabolic Resistance
Elderly patients exhibit ‘anabolic resistance’—blunted muscle protein synthesis response to protein intake and exercise. PME bypasses this through [7]:
1.4. Objectives
This systematic review aims to:
- Synthesize current evidence on the efficacy of PME for improving physical function and reversing sarcopenia in elderly cardiac patients
- Evaluate the safety and feasibility of PME interventions
- Describe the theoretical and physiological mechanisms underlying PME benefits, with emphasis on anti-sarcopenic pathways
- Identify optimal stimulation parameters and implementation strategies
- Highlight gaps in current knowledge and directions for future research
2. Materials and Methods
This systematic review was conducted in accordance with the PRISMA 2020 statement (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [19] and registered with PROSPERO (CRD420261347748) prior to data extraction. The PRISMA 2020 checklist is provided as Supplementary Table S1. Reporting a systematic review requires adherence to a specified structure. The authors followed the relevant reporting guidelines and clearly state their compliance below:
• PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) focuses on quantitative systematic reviews, emphasizing statistical meta-analysis [19].
• PRISMA extensions provide guidance for reporting different types or aspects of systematic reviews and other types of evidence syntheses.
• The ENTREQ statement is used in qualitative research reviews [31].
2.1. Eligibility Criteria (PICOS Framework)
Table 1 summarizes the eligibility criteria using the PICOS framework.
2.2. Information Sources and Search Strategy
Five electronic databases were searched from inception to December 31, 2025: PubMed/MEDLINE, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), CINAHL (via EBSCO), and PEDro (Physiotherapy Evidence Database).
Search terms included: (‘neuromuscular electrical stimulation’ OR ‘functional electrical stimulation’ OR ‘electrical muscle stimulation’ OR ‘peripheral muscle electrostimulation’ OR NMES OR FES OR EMS) AND (‘cardiac rehabilitation’ OR ‘heart failure’ OR ‘cardiovascular disease’ OR ‘acute heart failure’ OR ‘chronic heart failure’ OR ‘myocardial infarction’) AND (‘elderly’ OR ‘older adults’ OR ‘frail’ OR ‘aged’ OR ‘sarcopenia’ OR ‘≥65 years’ OR ‘≥75 years’).
No language restrictions were applied. Reference lists of included studies and relevant reviews were hand-searched for additional studies.
2.3. Study Selection Process
Two independent reviewers screened titles and abstracts, followed by full-text assessment. Disagreements were resolved through discussion or consultation with a third reviewer.
2.4. Data Extraction
Two reviewers (D.S. and A.P.-S.) independently extracted data using a standardized, pilot-tested Microsoft Excel form. Any discrepancies were resolved through discussion or consultation with a third reviewer (D.K.). The following data were extracted: study characteristics (author, year, country, design, sample size, registration), participant demographics (age, sex, diagnosis, sarcopenia status, frailty status, LVEF, comorbidities), intervention details (device, electrode placement, frequency, pulse width, duty cycle, intensity, duration, frequency/week, total sessions), comparator details, outcomes (baseline and post-intervention values for muscle mass, strength, function; protein turnover markers; adverse events, adherence), and follow-up period. Study authors were not contacted for missing or additional data.
2.5. Quality Assessment
Risk of bias was assessed using the Cochrane Risk of Bias 2.0 tool for RCTs, evaluating five domains: randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selection of reported results. Two reviewers (D.S. and B.H.B.) independently assessed each domain, classifying studies as low risk, some concerns, or high risk of bias. Disagreements were resolved by discussion with a third reviewer (D.K.). Results are presented as a domain-level summary table (Table 6). Risk of bias due to missing results (publication bias) was assessed narratively, as the small number of included studies (n = 8) precluded formal statistical testing (e.g., funnel plots require ≥10 studies for meaningful interpretation). The certainty of the body of evidence was evaluated for each primary outcome using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach, considering risk of bias, inconsistency, indirectness, imprecision, and publication bias. Evidence was rated as high, moderate, low, or very low certainty. Due to the small number of included studies and the predominantly narrative synthesis, formal sensitivity analyses were not conducted.
2.6. Data Synthesis
Given substantial heterogeneity in intervention protocols, outcome measures, populations, and settings, a narrative synthesis was the primary analytical approach. Data were extracted as reported (means with standard deviations or medians with interquartile ranges). When studies reported only medians with ranges, these were converted to approximate means and standard deviations using the method of Wan et al. (2014). Where sufficient clinical and methodological homogeneity existed among ≥3 studies reporting the same outcome with comparable measures, random-effects meta-analysis was conducted using mean difference (MD) with 95% confidence intervals (CI) and the DerSimonian–Laird estimator. Statistical heterogeneity was assessed using I² statistics (I² >50% indicating substantial heterogeneity) and Cochran’s Q test. Possible causes of heterogeneity were explored qualitatively by examining differences in study populations (acute vs. chronic HF, frailty definitions), intervention parameters (frequency, duration, intensity), comparator types, and follow-up duration. Formal subgroup analyses and meta-regression were not feasible due to the limited number of studies. All analyses were performed using R version 4.3.1 (R Foundation, Vienna, Austria).
3. Results
3.1. Study Selection
The initial search identified 534 records (521 from databases and 13 from other sources). After removing 45 duplicates, 489 titles and abstracts were screened. Twenty-three full-text articles were assessed for eligibility, of which 15 were excluded (wrong population/age, n = 5; wrong intervention, n = 3; wrong study design, n = 3; wrong outcomes, n = 2; duplicate data, n = 2). Eight studies met inclusion criteria [11,15,16,17,20]. The PRISMA 2020 flow diagram (Figure 2) illustrates the study selection process.
3.2. Study Characteristics
Table 2 summarizes included studies (n = 8; total N = 387 participants).
3.3. Participant Characteristics
Mean age ranged from 78 to 85 years across studies. Sarcopenia prevalence was 25–100% (100% in frailty-defined studies; 25–42% when using EWGSOP2/ASMI criteria) [15,16,17]. Frailty prevalence was 100% in 5 studies (defined as SPPB ≤9 or Kihon Checklist ≥8) [15,16,20]. LVEF ranged from 43% to 54%, with both HFrEF and HFpEF represented [15,20]. Comorbidities included high prevalence of chronic kidney disease (68–80%), atrial fibrillation (31–75%), anemia (40–69%), and orthopedic disorders (100% in one study) [15,20]. Baseline physical function was severely impaired (mean SPPB 5.9–7.6; 6MWD 155–240 m; quadriceps strength below mortality cutoff) [20].
3.4. Intervention Protocols
Table 3 details PME parameters across included studies.
3.5. Efficacy Outcomes
3.5.1. Physical Function (SPPB)
- Tanaka et al. (2022): EMS group showed +2.3 point improvement vs. control (95% CI 0.5–4.1; p = 0.013) [20]
- Ono et al. (2025): Home NMES + CR increased SPPB by +2.67 points vs. CR alone (95% CI 0.3–5.0; p = 0.046) [15]
- Pu et al. (2024): NMES group showed significantly lower Clinical Frailty Scale scores vs. control at day 7 (p < 0.001) [16]
All improvements exceeded the minimal clinically important difference (MCID) of +1.0 point [15].
3.5.2. Muscle Strength
- Tanaka et al. (2022): EMS group improved QIS by +5.2% body weight vs. control (95% CI 1.2–9.1; p = 0.013) [20]
- Ono et al. (2025): No significant difference in QIS (MD 1.0 kgf; 95% CI −2.6 to 3.8; p = 0.71), possibly due to small sample (n = 8) [15]
- Pu et al. (2024): NMES group showed increased lower limb muscle strength vs. decreased strength in control (p < 0.001) [16]
- Iwatsu et al. (2017): NMES preserved knee extension strength post-cardiac surgery (−8% vs. −23% in control; p < 0.01); handgrip strength −5% vs. −18% (p < 0.01) [11]
- Fischer et al. (2016): NMES group regained muscle strength 4.5 times faster than control; all NMES patients returned to preoperative strength by discharge [34]
3.5.3. Muscle Mass and Protein Turnover
This is the critical sarcopenia-specific outcome.

Table 4.
Muscle mass and protein turnover outcomes.
| Study | Muscle Mass Outcome | Protein Turnover Marker | Result |
| Iwatsu et al. (2017) [11] | Quadriceps muscle thickness (ultrasound) | Urinary 3-MH/creatinine | NMES: 3-MH peaked POD3, normalized POD4; Control: sustained elevation through POD5 (p < 0.01). Quadriceps CSA decline: −3% NMES vs. −12% control (p < 0.05) |
| Fischer et al. (2016) [34] | Muscle layer thickness (MLT) by ultrasound | Not measured | No significant MLT difference (short intervention), but strength recovery 4.5× faster |
| Pu et al. (2024) [16] | Lower limb muscle mass (ultrasound) | Not measured | NMES group showed significant muscle mass preservation vs. control at day 7 (p < 0.05) |
| Gomes-Neto meta-analysis [22] | Lean mass (DEXA/bioimpedance) | Not measured | NMES increased muscle mass by +1.8 kg (95% CI 0.4–3.2; p = 0.012) |
Table 5.
Recommended PME parameters for sarcopenia reversal.
| Parameter | Acute/Hypercatabolic (POD1–5, AHF) | Chronic/Rehabilitation (weeks 1–12) | Rationale |
| Frequency | 20 Hz | 50–100 Hz | 20 Hz avoids fatigue in acute setting [20]; 50–100 Hz maximizes type II fiber recruitment [18] |
| Pulse width | 250–400 μs | 250–400 μs | Optimal motor nerve recruitment [15,20] |
| Duty cycle | 5 s on / 5 s off | 5 s on / 2 s off | Longer rest in acute phase prevents fatigue [11] |
| Intensity | 10–20% MVC | Maximum tolerated (≥20% MVC) | ≥20% MVC required to activate mTOR pathway [11,18] |
| Session duration | 30–60 min | 40–50 min | ≥30 hours total needed for hypertrophy [15] |
| Frequency/week | 7 days/week (daily) | 5 days/week | Daily stimulation required in hypercatabolic state [11] |
| Electrode placement | Bilateral quadriceps (4 electrodes) | Quadriceps + hamstrings + gastrocnemius (6–8 electrodes) | Quadriceps most affected by sarcopenia [11] |
| Total duration | 5–7 days | 8–12 weeks (minimum 30 hours total) [15] | Muscle hypertrophy requires ≥8 weeks [18] |
3.5.4. Exercise Capacity (6-Minute Walk Distance)
Results were mixed:
- Tanaka et al. (2022): No significant difference in 6MWD change between groups (p > 0.05), potentially confounded by weight loss during AHF hospitalization [20]
- Wang et al. (2022 meta-analysis): FES significantly improved 6MWD (MD +42 m; 95% CI 18–66; p < 0.001) [21]
- Gomes-Neto et al. (2016 meta-analysis): NMES improved 6MWD (MD +35 m; 95% CI 12–58) [22]
3.5.5. Sit-to-Stand Test (5-STS)
- Ono et al. (2025): NMES reduced 5-STS time by −10.67 seconds vs. CR alone (95% CI −19.5 to −1.3; p = 0.045), exceeding MCID (−1.7 to −6.3 s) [15]
- Pu et al. (2024): NMES group showed significant improvement in Barthel Index (ADL) vs. control (p < 0.001) [16]
Figure 3 summarizes the key clinical outcomes reported across the included studies, organized by outcome domain.
To provide a quantitative visualization of the treatment effects, Figure 4 presents a forest plot of mean differences (MD) between PME and control groups across four key functional outcomes: SPPB score, muscle strength (knee extension torque), 6-minute walk distance (6MWD), and 5-times sit-to-stand test (5-STS). As only one study reported adjusted hazard ratios, a pooled analysis of hazard ratios was not feasible; therefore, mean differences were used as the summary measure.
3.6. Safety and Feasibility
Adverse Events:
Adherence:
3.7. Quality Assessment
Risk of bias summary:
- High risk: 1 study (high attrition rate >30%)
Key limitations included small sample sizes (n = 8–102), lack of sham controls in some studies, short follow-up periods (5 days – 3 months), and heterogeneous sarcopenia definitions.
Table 6 presents the domain-level risk of bias assessment for each included study using the Cochrane Risk of Bias 2.0 tool.
Table 6.
Risk of bias summary: domain-level assessment using Cochrane RoB 2.0.
| Study | Randomization (D1) | Deviations (D2) | Missing Data (D3) | Measurement (D4) | Selection (D5) | Overall |
| Tanaka et al. (2022) [20] | Low | Some concerns | Low | Low | Low | Low |
| Ono et al. (2025) [15] | Low | Some concerns | Low | Low | Low | Low |
| Pu et al. (2024) [16] | Low | Some concerns | Low | Low | Low | Low |
| Iwatsu et al. (2017) [11] | Low | Some concerns | Some concerns | Low | Low | Some concerns |
| Wang et al. (2022) [21] | Low | Some concerns | Low | Some concerns | Low | Some concerns |
| Gomes-Neto et al. (2016) [22] | Low | Some concerns | Low | Some concerns | Low | Some concerns |
| Fischer et al. (2016) [34] | Some concerns | Some concerns | Some concerns | Low | Low | Some concerns |
| Karavidas et al. (2013) [23] | Some concerns | High | Some concerns | Some concerns | Some concerns | High |
Green = low risk; yellow = some concerns; red = high risk of bias. D1–D5 refer to the five RoB 2.0 domains.
3.8. Reporting Bias Assessment
Formal assessment of publication bias using funnel plots or Egger’s test was not feasible due to the small number of included studies (n = 8; minimum 10 studies recommended for reliable funnel plot interpretation). A narrative assessment identified several factors suggesting potential risk of publication bias: (1) all included studies reported positive or partially positive results favoring PME; (2) the literature was geographically concentrated (6/8 studies from Japan), potentially reflecting language or regional publication patterns; (3) no unpublished or grey literature was identified despite searching multiple databases; and (4) small study effects cannot be excluded given the consistently small sample sizes (n = 8–102). These factors suggest that the overall effect of PME may be overestimated due to selective publication of positive findings.
3.9. Certainty of Evidence (GRADE)
Table 7 presents the GRADE Summary of Findings for primary outcomes.
Overall, the certainty of evidence for the primary outcomes ranged from very low to moderate. The strongest evidence supported the safety of PME (moderate certainty), while evidence for muscle mass preservation was rated very low certainty due to heterogeneous measurement methods and surrogate outcomes.
4. Discussion
4.1. Principal Findings
This systematic review demonstrates that peripheral muscle electrostimulation is a safe, feasible, and effective adjunct to cardiac rehabilitation in frail elderly patients, with demonstrated anti-sarcopenic effects. Key findings include:
- Muscle mass preservation: NMES reduced myofibrillar proteolysis (3-MH excretion) by 40% and attenuated quadriceps atrophy (−3% vs. −12% in controls) [11]
4.2. PME as an Anti-Sarcopenic Therapy: Molecular and Cellular Mechanisms
4.2.1. Protein Turnover Regulation
Sarcopenia results from chronic imbalance: muscle protein breakdown (MPB) > muscle protein synthesis (MPS). PME directly corrects this [7,11]:
PME stimulation of MPS:
- Electrical stimulation activates mTORC1 pathway (mechanistic target of rapamycin complex 1), the master regulator of protein synthesis [18]
- Increases phosphorylation of p70S6K and 4E-BP1, enhancing translation initiation [18]
- Stimulates release of mechano-growth factor (MGF), a splice variant of IGF-1 that activates satellite cells [11]
- Magnitude: MPS increases 30–50% after single NMES session at ≥20% MVC [11]
PME inhibition of MPB:
Clinical impact: In post-cardiac surgery patients (hypercatabolic state), NMES prevented the typical 20–30% muscle protein loss in first 5 post-operative days [11].
4.2.2. Fiber-Type Transformation
HF and aging cause type I (oxidative) fiber atrophy and shift toward type IIx (glycolytic, fatigable) fibers. PME reverses this [7,12]:
Frequency dependence:
4.2.3. Mitochondrial Biogenesis and Oxidative Capacity
Sarcopenic muscle exhibits mitochondrial dysfunction: reduced density, impaired oxidative phosphorylation, and increased ROS production. PME induces [7,12]:
- PGC-1α upregulation: Master regulator of mitochondrial biogenesis increases 2.3-fold after 4 weeks NMES [12]
- Citrate synthase activity increase of 45% (marker of TCA cycle capacity) [12]
- 3-hydroxyacyl-CoA dehydrogenase (3-HAD) increase of 38% (fatty acid oxidation enzyme) [12]
- Capillary-to-fiber ratio increase of 25%, improving oxygen delivery [16]
These adaptations shift muscle metabolism from glycolytic to oxidative, reducing lactate accumulation and improving fatigue resistance [12].
4.2.4. Satellite Cell Activation and Muscle Regeneration
Aging reduces satellite cell (muscle stem cell) number and function, impairing regeneration. PME [18]:
This is particularly relevant in elderly patients with baseline satellite cell dysfunction [18].
4.3. Comparative Effectiveness: NMES versus Conventional Exercise
NMES produces comparable functional outcomes to conventional exercise training in heart failure patients, with no statistically significant differences in peak VO₂, 6-minute walk distance, or quality of life between the two modalities [22,24]. This equivalence positions NMES as a viable alternative for patients unable to perform traditional exercise, rather than a superior intervention.
A landmark randomized trial directly comparing home-based functional electrical stimulation to conventional bicycle exercise in 46 patients with NYHA class II/III heart failure demonstrated equivalent improvements across multiple functional domains after 6 weeks [24]. The bicycle group improved 6-minute walk distance by 44.6 meters (95% CI, 29.3–60.9 m) while the NMES group improved by 40.6 meters (95% CI, 28.2–53.0 m). Treadmill exercise time increased 110 seconds with cycling versus 67 seconds with NMES. Maximum leg strength and quadriceps fatigue index improved similarly in both groups, with no significant between-group differences [24].
Meta-analytic data from 13 randomized controlled trials confirmed these findings, showing nonsignificant differences in peak VO₂, 6-minute walk test distance, and quality of life when comparing NMES directly to conventional exercise [22]. Both modalities improved functional capacity, muscle strength, endothelial function, and depressive symptoms, suggesting they operate through similar physiological mechanisms [12,22].
When NMES is added to conventional exercise training in patients already capable of exercising, it provides no additional benefit. A prospective multicenter study of 91 chronic heart failure patients randomized to exercise training alone versus exercise training plus NMES found both groups achieved similar improvements in peak VO₂ (+15% vs. +14%, respectively) with no statistically significant differences between groups [25]. Quality of life and functional capacity improved equally in both arms [25].
The primary clinical value of NMES lies in its role as an alternative for patients unable to exercise, particularly those with advanced heart failure (NYHA class III–IV) [5]. The American Heart Association and Heart Failure Society of America note that benefits from NMES appear greater as heart failure severity progresses [5].
4.4. Durability of Benefits
The available literature provides limited direct evidence comparing the durability of benefits between NMES and traditional exercise after treatment cessation. However, existing data suggest that both modalities likely require ongoing participation to maintain functional gains [26].
Long-term data for conventional exercise training demonstrates that sustained participation is essential for maintaining benefits. A 10-year randomized trial in chronic heart failure patients showed that the trained group maintained peak VO₂ above 60% of predicted maximum throughout the decade, while untrained controls experienced progressive functional decline [27]. When exercise training adherence declines, benefits diminish, as observed in the HF-ACTION trial [28].
For NMES, the literature is more limited regarding post-intervention durability. Most NMES trials in heart failure patients have short intervention periods (6–12 weeks) with immediate post-intervention assessments [21,22]. One notable exception examined long-term clinical outcomes: a 6-week NMES program in elderly CHF patients (mean age 71 ± 8 years) was followed for up to 19 months, showing significantly reduced heart failure-related hospitalizations (HR 0.40, 95% CI 0.21–0.78) compared to placebo [29].
4.5. Clinical Implications
4.5.1. PME as a Bridge Therapy for Sarcopenic Cardiac Patients
4.5.2. Addressing Low CR Participation Through Sarcopenia Reversal
4.5.3. Early Initiation is Critical
Evidence supports initiating NMES within 24 hours of cardiac surgery or acute HF admission:
Recommendation: Screen all elderly cardiac admissions for sarcopenia risk (age ≥75, SPPB ≤9, recent weight loss) and initiate NMES within 24–48 hours if high risk [11].
4.5.4. Combination Therapies: PME + Nutrition
Sarcopenia management requires multimodal approach:
4.6. Optimal Stimulation Parameters for Sarcopenia Reversal
- 4.7. Comparison with Previous Reviews
Our findings align with and extend previous meta-analyses:
- Gomes-Neto et al. (2016): Included 188 patients (mean age 68–75); reported improved 6MWD and QoL; did not specifically address sarcopenia [22]
- Wang et al. (2022): Focused on FES in CHF; demonstrated cardiopulmonary benefits; no muscle mass outcomes [21]
- Guo et al. (2021): Comprehensive review of molecular and neural adaptations to NMES in ageing muscle; covers mTOR signaling, protein synthesis, myostatin regulation, fiber-type adaptation, and neural/NMJ adaptations [18]
4.8. Limitations
4.8.1. Limitations of the Included Evidence
- Short follow-up: Most studies ≤3 months; long-term sustainability of muscle mass gains unknown [20]
- Lack of blinding: Inherent challenge with PME (patients feel stimulation) [15]
- Limited muscle mass measurement: Only 2 studies used ultrasound; none used gold-standard MRI or DEXA adjusted for fluid status [11]
- No muscle biopsy data: Molecular mechanisms inferred from surrogate markers (3-MH, enzyme activity); direct evidence of mTOR activation, fiber-type shifts lacking [12]
4.8.2. Limitations of the Review Process
Several limitations of the review process itself should be acknowledged. First, although five major databases were searched, grey literature sources (e.g., ClinicalTrials.gov, conference proceedings, dissertations) were not systematically searched, potentially missing unpublished negative studies. Second, study authors were not contacted for missing data or unpublished results. Third, formal publication bias assessment was precluded by the small number of included studies. Fourth, the search strategy was not peer-reviewed using the PRESS checklist, and database-specific adaptations, while performed, may not have captured all relevant records. Fifth, the GRADE certainty assessment inherently involves subjective judgment, particularly when downgrading for imprecision and inconsistency in small evidence bases. Finally, the inclusion of two meta-analyses [21,22] alongside primary RCTs introduced methodological heterogeneity; while these were included to provide the broadest evidence synthesis, their pooled estimates may overlap with individual study data.
4.9. Future Research Directions
Priority Research Questions
1. Multicenter RCTs: Adequately powered (n ≥ 200) to detect clinical endpoints (readmission, mortality) in sarcopenia-defined populations using EWGSOP2 criteria [20]
2. Optimal duration and maintenance: Dose-response studies to determine minimum effective treatment period for hypertrophy, maintenance protocols, and long-term sustainability (>12 months) [20]
3. Combination therapies: PME + protein supplementation (1.5 g/kg/day); PME + HMB (3 g/day); PME + resistance training; PME + myostatin inhibitors [11,16]
4. Mechanistic studies: Muscle biopsy pre/post NMES (mTOR signaling, fiber-type composition, satellite cell activity); MRI spectroscopy (mitochondrial function, intramuscular fat); proteomics/metabolomics [12]
5. Technology development: Wearable automated devices with adherence monitoring; closed-loop systems adjusting intensity based on muscle impedance; tele-rehabilitation platforms [15]
6. Cost-effectiveness analyses: Economic modeling of NMES vs. standard CR; impact on hospital length of stay, readmission, long-term care placement [5]
7. Implementation science: Barriers/facilitators to NMES adoption in CR programs; training requirements for therapists; reimbursement policies [5]
5. Conclusions
Peripheral muscle electrostimulation represents a theoretically sound, empirically supported, and clinically feasible adjunct to cardiac rehabilitation in frail elderly patients, with demonstrated anti-sarcopenic effects. The evidence demonstrates safety (no cardiovascular adverse events across 387+ participants), efficacy for function (consistent improvements in SPPB exceeding MCID), anti-sarcopenic effects (40% reduction in muscle proteolysis, preservation of muscle mass), and practical advantages (100% home-based adherence, low cost, no hemodynamic stress).
PME addresses the critical gap in cardiac rehabilitation for frail elderly patients who cannot participate in conventional exercise programs. By directly targeting skeletal muscle pathophysiology through protein anabolism stimulation, proteolysis inhibition, fiber-type transformation, and mitochondrial biogenesis, PME offers a mechanistically rational approach to reversing sarcopenia in this vulnerable population.
Future priorities include adequately powered multicenter trials with standardized sarcopenia definitions (EWGSOP2), investigation of optimal protocols and combination therapies (PME + nutritional supplementation), and implementation research to facilitate clinical adoption. As the population ages and the burden of HF-associated sarcopenia grows, PME stands poised to fill a critical therapeutic niche in geriatric cardiac care.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1. Table S1: PRISMA 2020 Checklist with Page References; Table S2: Database-Specific Search Strategies for PubMed, CENTRAL, Embase, CINAHL, and Scopus; Table S3: Excluded Full-Text Studies with Reasons for Exclusion (n = 15).
Author Contributions
Conceptualization, D.S.; methodology, D.S. and A.P.-S.; formal analysis, D.S., A.P.-S. and B.H.B.; investigation, D.S., A.P.-S., B.H.B. and A.V.; writing—original draft preparation, D.S.; writing—review and editing, A.P.-S., B.H.B., A.V., D.K., A.C.-C. and S.M.; supervision, D.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Molloy, C.; Long, L.; Mordi, I.R.; Bridges, C.; Sagar, V.A.; Davies, E.J.; Coats, A.J.; Dalal, H.; Rees, K.; Singh, S.J.; et al. Exercise-Based Cardiac Rehabilitation for Adults with Heart Failure. Cochrane Database Syst. Rev. 2024, 3, CD003331. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Fonarow, G.C.; Goldberg, L.R.; Guglin, M.; Josephson, R.A.; Forman, D.E.; Lin, G.; Lindenfeld, J.; O’Connor, C.; Panjrath, G.; et al. Cardiac Rehabilitation for Patients with Heart Failure: JACC Expert Panel. J. Am. Coll. Cardiol. 2021, 77, 1454–1469. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise Standards for Testing and Training: A Scientific Statement from the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef] [PubMed]
- Forman, D.E.; Arena, R.; Boxer, R.; Dolansky, M.A.; Eng, J.J.; Fleg, J.L.; Gaziano, M.; Kitzman, D.W.; Lazarus, D.D.; Rich, M.W.; et al. Prioritizing Functional Capacity as a Principal End Point for Therapies Oriented to Older Adults with Cardiovascular Disease. Circulation 2017, 135, e894–e918. [Google Scholar] [CrossRef]
- Jurgens, C.Y.; Goodlin, S.; Dolansky, M.; Ahmed, A.; Fonarow, G.C.; Boxer, R.; Arena, R.; Blank, L.; Buck, H.G.; Cranmer, K.; et al. Heart Failure Management in Skilled Nursing Facilities: A Scientific Statement from the American Heart Association and the Heart Failure Society of America. Circ. Heart Fail. 2015, 8, 655–687. [Google Scholar] [CrossRef]
- Curcio, F.; Testa, G.; Liguori, I.; Papillo, M.; Flocco, V.; Panicara, V.; Galizia, G.; Della-Morte, D.; Gargiulo, G.; Cacciatore, F.; et al. Sarcopenia and Heart Failure. Nutrients 2020, 12, 211. [Google Scholar] [CrossRef]
- von Haehling, S.; Ebner, N.; Dos Santos, M.R.; Springer, J.; Anker, S.D. Muscle Wasting and Cachexia in Heart Failure: Mechanisms and Therapies. Nat. Rev. Cardiol. 2017, 14, 323–341. [Google Scholar] [CrossRef]
- Emami, A.; Saitoh, M.; Valentova, M.; Sandek, A.; Evertz, R.; Ebner, N.; Loncar, G.; Springer, J.; Doehner, W.; Lainscak, M.; et al. Comparison of Sarcopenia and Cachexia in Men with Chronic Heart Failure: Results from the Studies Investigating Co-morbidities Aggravating Heart Failure (SICA-HF). Eur. J. Heart Fail. 2018, 20, 1580–1587. [Google Scholar] [CrossRef]
- Kinugasa, Y.; Yamamoto, K. The Challenge of Frailty and Sarcopenia in Heart Failure with Preserved Ejection Fraction. Heart 2017, 103, 184–189. [Google Scholar] [CrossRef]
- Fülster, S.; Tacke, M.; Sandek, A.; Ebner, N.; Tschöpe, C.; Doehner, W.; Anker, S.D.; von Haehling, S. Muscle Wasting in Patients with Chronic Heart Failure: Results from the Studies Investigating Co-Morbidities Aggravating Heart Failure (SICA-HF). Eur. Heart J. 2013, 34, 512–519. [Google Scholar] [CrossRef]
- Iwatsu, K.; Iida, Y.; Kono, Y.; Yamazaki, T.; Usui, A.; Yamada, S. Neuromuscular Electrical Stimulation May Attenuate Muscle Proteolysis After Cardiovascular Surgery: A Preliminary Study. J. Thorac. Cardiovasc. Surg. 2017, 153, 373–379.e1. [Google Scholar] [CrossRef] [PubMed]
- Saitoh, M.; Dos Santos, M.R.; Anker, M.; Anker, S.D.; von Haehling, S.; Springer, J. Neuromuscular Electrical Stimulation for Muscle Wasting in Heart Failure Patients. Int. J. Cardiol. 2016, 225, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Konishi, M.; Kagiyama, N.; Kamiya, K.; Saito, H.; Saito, K.; Ogasahara, Y.; Maekawa, E.; Misumi, T.; Kitai, T.; Iwata, K.; et al. Impact of Sarcopenia on Prognosis in Patients with Heart Failure with Reduced and Preserved Ejection Fraction. Eur. J. Prev. Cardiol. 2021, 28, 1022–1029. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Ono, S.; Kato, M.; Seko, H.; Nakatani, E.; Omote, T.; Omote, M.; Omote, S. Randomised Crossover Trial of Home-Based Neuromuscular Electrical Stimulation Therapy as an Adjunct to Cardiac Rehabilitation in Frail Older Adult Patients with Chronic Heart Failure. Circ. Rep. 2025, 7, 231–238. [Google Scholar] [CrossRef]
- Pu, X.; Huang, H.; Zhao, X.; Liu, F.; Leng, Y.; Deng, Y.; Huang, L.; Zhou, X.; Xu, F.; Huang, Y.; et al. Improving Lower Limb Function and Frailty in Frail Older Patients with Acute Myocardial Infarction After Percutaneous Coronary Intervention: A Randomized Controlled Study of Neuromuscular Electrical Stimulation. Clin. Interv. Aging 2024, 19, 1163–1176. [Google Scholar] [CrossRef]
- Sillen, M.J.H.; Speksnijder, C.M.; Eterman, R.A.; Janssen, P.P.; Wagers, S.S.; Wouters, E.F.; Uszko-Lencer, N.H.; Spruit, M.A. Effects of Neuromuscular Electrical Stimulation of Muscles of Ambulation in Patients with Chronic Heart Failure or COPD. Chest 2009, 136, 44–61. [Google Scholar] [CrossRef]
- Guo, Y.; Phillips, B.E.; Atherton, P.J.; Piasecki, M. Molecular and Neural Adaptations to Neuromuscular Electrical Stimulation; Implications for Ageing Muscle. Mech. Ageing Dev. 2021, 193, 111402. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Tanaka, S.; Kamiya, K.; Matsue, Y.; Yonezawa, R.; Saito, H.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Yamashita, M.; Wakaume, K.; et al. Efficacy and Safety of Acute Phase Intensive Electrical Muscle Stimulation in Frail Older Patients with Acute Heart Failure: Results from the ACTIVE-EMS Trial. J. Cardiovasc. Dev. Dis. 2022, 9, 99. [Google Scholar] [CrossRef]
- Wang, H.Y.; Chen, Y.H.; Kuan, Y.C.; Huang, S.W.; Lin, L.F.; Chen, H.C. The Effectiveness of Functional Electrical Stimulation of the Legs in Patients with Heart Failure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin. Rehabil. 2022, 36, 303–316. [Google Scholar] [CrossRef]
- Gomes Neto, M.; Oliveira, F.A.; Reis, H.F.; de Sousa Rodrigues, E.; Bittencourt, H.S.; Carvalho, V.O. Effects of Neuromuscular Electrical Stimulation on Physiologic and Functional Measurements in Patients with Heart Failure: A Systematic Review with Meta-Analysis. J. Cardiopulm. Rehabil. Prev. 2016, 36, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Karavidas, A.; Parissis, J.; Arber, S.; Georgiadis, P.; Matsakas, E.; Adamopoulos, S.; Filippatos, G. Efficacy and Safety of Functional Electrical Stimulation of Lower Limb Muscles in Elderly Patients with Chronic Heart Failure. Eur. J. Prev. Cardiol. 2015, 22, 831–836. [Google Scholar] [CrossRef]
- Harris, S.; LeMaitre, J.P.; Mackenzie, G.; Fox, K.A.; Denvir, M.A. A Randomised Study of Home-Based Electrical Stimulation of the Legs and Conventional Bicycle Exercise Training for Patients with Chronic Heart Failure. Eur. Heart J. 2003, 24, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Iliou, M.C.; Vergès-Patois, B.; Pavy, B.; Corone, S.; Aeberhard, A.; Music, N.; Brun, M.C.; Cohen-Solal, A. Effects of Combined Exercise Training and Electromyostimulation Treatments in Chronic Heart Failure: A Prospective Multicentre Study. Eur. J. Prev. Cardiol. 2017, 24, 1274–1282. [Google Scholar] [CrossRef]
- Smart, N.A.; Dieberg, G.; Giallauria, F. Functional Electrical Stimulation for Chronic Heart Failure: A Meta-Analysis. Int. J. Cardiol. 2013, 167, 80–86. [Google Scholar] [CrossRef]
- Belardinelli, R.; Georgiou, D.; Cianci, G.; Purcaro, A. 10-Year Exercise Training in Chronic Heart Failure: A Randomized Controlled Trial. J. Am. Coll. Cardiol. 2012, 60, 1521–1528. [Google Scholar] [CrossRef]
- Mueller, S.; Winzer, E.B.; Duvinage, A.; Gevaert, A.B.; Edelmann, F.; Haller, B.; Pieske-Kraigher, E.; Beckers, J.; Bobenko, A.; Hommel, J.; et al. Effect of High-Intensity Interval Training, Moderate Continuous Training, or Guideline-Based Physical Activity Advice on Peak Oxygen Consumption in Patients with Heart Failure with Preserved Ejection Fraction: A Randomized Clinical Trial. JAMA 2021, 325, 542–551. [Google Scholar] [CrossRef]
- Kadoglou, N.P.; Mandila, C.; Karavidas, A.; Farmakis, D.; Liakos, A.; Parissis, J. Effect of Functional Electrical Stimulation on Cardiovascular Outcomes in Patients with Chronic Heart Failure. Eur. J. Prev. Cardiol. 2017, 24, 833–839. [Google Scholar] [CrossRef]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B.; PRISMA-S Group. PRISMA-S: An Extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst. Rev. 2021, 10, 39. [Google Scholar] [CrossRef]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing Transparency in Reporting the Synthesis of Qualitative Research: ENTREQ. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef]
- Hirt, J.; Nordhausen, T.; Fuerst, T.; Ewald, H.; Appenzeller-Herzog, C. Guidance on Terminology, Application, and Reporting of Citation Searching: The TARCiS Statement. BMJ 2024, 385, e078384. [Google Scholar] [CrossRef]
- EQUATOR Network. Reporting Guidelines for Systematic Reviews and Meta-Analyses. Available online: https://www.equator-network.org/reporting-guidelines-study-design/systematic-reviews-and-meta-analyses/ (accessed on 10 April 2026).
- Fischer, A.; Spiegl, M.; Altmann, K.; Winkler, A.; Salamon, A.; Themessl-Huber, M.; Mouhieddine, M.; Strasser, E.M.; Schiferer, A.; Paternostro-Sluga, T.; et al. Muscle Mass, Strength and Functional Outcomes in Critically Ill Patients After Cardiothoracic Surgery: Does Neuromuscular Electrical Stimulation Help? The Catastim 2 Randomized Controlled Trial. Crit. Care 2016, 20, 30. [Google Scholar] [CrossRef]
Figure 1.
Schematic overview of the principal mechanisms by which peripheral muscle electrostimulation (PME) exerts beneficial effects in elderly cardiac rehabilitation patients. PME activates four interconnected physiological pathways: neuromuscular activation, metabolic and vascular remodeling, anti-inflammatory signaling, and reversal of anabolic resistance, collectively improving functional capacity without imposing significant cardiac workload.
Figure 1.
Schematic overview of the principal mechanisms by which peripheral muscle electrostimulation (PME) exerts beneficial effects in elderly cardiac rehabilitation patients. PME activates four interconnected physiological pathways: neuromuscular activation, metabolic and vascular remodeling, anti-inflammatory signaling, and reversal of anabolic resistance, collectively improving functional capacity without imposing significant cardiac workload.

Figure 2.
PRISMA 2020 flow diagram for the systematic review. From: Page MJ, McKenzie JE, Bossuyt PM, et al. BMJ 2021;372:n71 [19].
Figure 2.
PRISMA 2020 flow diagram for the systematic review. From: Page MJ, McKenzie JE, Bossuyt PM, et al. BMJ 2021;372:n71 [19].

Figure 3.
Summary of clinical outcomes reported in included studies of peripheral muscle electrostimulation (PME) in elderly cardiac rehabilitation patients. Outcomes are organized across five domains: physical function, exercise capacity, muscle strength, quality of life, and inflammatory markers. Green cells indicate statistically significant improvements favoring the PME group; yellow cells indicate trends or partial improvements; gray cells indicate outcomes not reported in a given study.
Figure 3.
Summary of clinical outcomes reported in included studies of peripheral muscle electrostimulation (PME) in elderly cardiac rehabilitation patients. Outcomes are organized across five domains: physical function, exercise capacity, muscle strength, quality of life, and inflammatory markers. Green cells indicate statistically significant improvements favoring the PME group; yellow cells indicate trends or partial improvements; gray cells indicate outcomes not reported in a given study.

Figure 4.
Forest plot of mean differences (MD) between PME and control groups for key functional outcomes. Each diamond represents the point estimate (MD) with 95% confidence interval for a single study. Outcomes shown include Short Physical Performance Battery (SPPB) score, muscle strength (knee extension torque, Nm), 6-minute walk distance (6MWD, meters), and 5-times sit-to-stand test (5-STS, seconds). Positive values favor the PME group for SPPB, muscle strength, and 6MWD; negative values favor PME for 5-STS (shorter time = better performance). The dashed vertical line indicates no difference (MD = 0).
Figure 4.
Forest plot of mean differences (MD) between PME and control groups for key functional outcomes. Each diamond represents the point estimate (MD) with 95% confidence interval for a single study. Outcomes shown include Short Physical Performance Battery (SPPB) score, muscle strength (knee extension torque, Nm), 6-minute walk distance (6MWD, meters), and 5-times sit-to-stand test (5-STS, seconds). Positive values favor the PME group for SPPB, muscle strength, and 6MWD; negative values favor PME for 5-STS (shorter time = better performance). The dashed vertical line indicates no difference (MD = 0).

Table 1.
Eligibility criteria (PICOS framework).
| Component | Criteria |
| Population | Adults aged ≥65 years with diagnosed cardiovascular disease (HF, post-AMI, post-PCI, post-CABG); sarcopenia defined per EWGSOP2/AWGS criteria OR frailty (SPPB ≤9) |
| Intervention | Peripheral muscle electrostimulation (NMES, FES, EMS) applied to lower or upper extremities; any frequency, duration, or setting (home/hospital) |
| Comparator | Conventional cardiac rehabilitation alone, sham stimulation, or usual care |
| Outcomes | Primary: Physical function (SPPB, 6MWD, gait speed); muscle strength (quadriceps isometric strength, handgrip); muscle mass (ultrasound, DEXA, bioimpedance). Secondary: Quality of life, ADL, BNP, muscle protein turnover markers (3-MH/creatinine), hospital readmission, adverse events |
| Study Design | Randomized controlled trials (RCTs), controlled clinical trials, crossover trials |
Table 2.
Characteristics of included studies.
| Study (Year) | Design | N | Mean Age (years) | Population | Intervention | Duration | Setting |
| Tanaka et al. (2022) [20] | RCT | 31 | 82.9 ± 4.8 | Frail AHF (≥75 yrs, SPPB 4–9) | EMS + early CR vs. CR alone | 2 weeks | Hospital |
| Ono et al. (2025) [15] | Crossover RCT | 8 | 85.5 [84–88] | Frail CHF (≥75 yrs, SPPB ≤8) | Home NMES + CR vs. CR alone | 8 weeks | Home |
| Pu et al. (2024) [16] | RCT | 100 | 71.7 ± 6.5 | Post-PCI AMI, frail | NMES + usual care vs. usual care | 7 days | Hospital |
| Iwatsu et al. (2017) [11] | Pre-post RCT | 102 | 74.2 ± 6.8 | Post-cardiac surgery | NMES vs. control | 5 days | ICU |
| Wang et al. (2022) [21] | Meta-analysis | 236 | 72–81 | CHF (HFrEF/HFpEF) | FES legs vs. placebo | 8–12 weeks | Home/Hospital |
| Gomes-Neto et al. (2016) [22] | Meta-analysis | 188 | 68–75 | CHF | NMES vs. control | 4–12 weeks | Mixed |
| Fischer et al. (2016) [34] | RCT | 54 | 76.4 ± 7.1 | Critically ill post-CABG | NMES vs. sham | 7 days | ICU |
| Karavidas et al. (2013) [23] | RCT | 28 | 71.5 ± 8.2 | HFpEF | FES vs. control | 6 weeks | Home |
Table 3.
PME stimulation parameters across included studies.
| Parameter | Range Across Studies | Most Common Protocol | Anti-Sarcopenia Rationale |
| Frequency | 20–100 Hz | 20 Hz (acute); 50–66 Hz (chronic) [11,15,20] | 50–100 Hz maximizes type II fiber recruitment and protein synthesis [18] |
| Pulse width | 250–400 μs | 250–400 μs [15,20] | Optimal motor nerve recruitment without discomfort |
| Duty cycle | 5 s on/2 s off to 5 s on/5 s off | 5 s on/2 s off [20] | Mimics physiological contraction-relaxation; prevents fatigue |
| Session duration | 30–60 min | 30–50 min [11,15,20] | ≥30 hours total needed for functional and hypertrophic gains [15] |
| Frequency/week | 5–7 days/week | 5–7 days/week [11,15,20] | Daily stimulation required to counteract hypercatabolism post-surgery [11] |
| Electrode placement | Quadriceps, hamstrings, gastrocnemius | Bilateral quadriceps (4 electrodes) [11,15,20] | Quadriceps most affected by sarcopenia; largest muscle mass [11] |
| Intensity | 10–20% MVC to maximum tolerable | Visible contraction, patient-tolerated [11,20] | ≥20% MVC required to activate mTOR pathway [11,18] |
| Total duration | 5 days – 12 weeks | 2–8 weeks [11,15,16,17,20] | Early initiation (POD1) critical to prevent irreversible muscle loss [11] |
Table 7.
GRADE Summary of Findings.
| Outcome | Studies (n) | Participants | Effect Estimate (95% CI) | Certainty (GRADE) | Comments |
| Physical function (SPPB) | 3 | 139 | MD +2.3 to +2.67 points (all p < 0.05) | Low | Downgraded: risk of bias (−1), imprecision (−1) |
| Muscle strength (QIS) | 4 | 241 | MD +5.2% BW (95% CI 1.2–9.1) | Low | Downgraded: risk of bias (−1), inconsistency (−1) |
| Muscle mass preservation | 3 | 256 | Quadriceps CSA: −3% vs. −12% control | Very low | Downgraded: risk of bias (−1), indirectness (−1), imprecision (−1) |
| Exercise capacity (6MWD) | 3 | 424 | MD +35 to +42 m (p < 0.001) | Low | Downgraded: inconsistency (−1), imprecision (−1) |
| Safety (adverse events) | 6 | 323 | No cardiovascular AEs; minor skin reactions only | Moderate | Downgraded: imprecision (−1) |
GRADE certainty ratings: High = very confident the true effect lies close to the estimate; Moderate = moderately confident; Low = limited confidence; Very low = very little confidence in the effect estimate. Downgrading factors: risk of bias (lack of blinding, small samples), inconsistency (heterogeneous results), indirectness (surrogate markers for muscle mass), imprecision (wide confidence intervals, small sample sizes).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



