Submitted:
09 April 2026
Posted:
11 April 2026
You are already at the latest version
Abstract
Background: Malnutrition and systemic inflammation are increasingly recognized as important determinants of prognosis in patients with heart failure. Several immuno-nutritional indices, including the Prognostic Nutritional Index (PNI), the Controlling Nutritional Status (CONUT) score, and the C-reactive protein–albumin–lymphocyte (CALLy) index, have been proposed as markers of nutritional and inflammatory status. However, their prognostic value in elderly patients with heart failure with preserved ejection fraction (HFpEF) remains incompletely defined. This study aimed to evaluate the prognostic significance of these immunonutritional indices in elderly patients with HFpEF over a long-term follow-up period. Methods: This retrospective observational study included 200 elderly patients hospitalized with HFpEF (mean age 86.6 ± 6.5 years). Clinical, laboratory, and echocardiographic parameters were collected at admission. Nutritional status was assessed using PNI, CONUT score, and CALLy index. Patients were followed for mortality during long-term follow-up. Survival analyses were performed using Cox regression models, receiver operating characteristic (ROC) curves, and Kaplan–Meier analysis. Median follow-up was 3.8 years (IQR 2.1–5.9). Results: During follow-up, 123 patients (61.5%) died, while 77 patients (38.5%) were alive at the end of observation. In univariate analysis, PNI, CONUT score, left ventricular ejection fraction (LVEF), and the tricuspid annular plane systolic excursion to systolic pulmonary artery pressure (TAPSE/sPAP) ratio were significantly associated with mortality. In multivariate analysis, the CONUT score, LVEF, and the TAPSE/sPAP ratio remained independent predictors of mortality. ROC analysis showed strong prognostic performance for the TAPSE/sPAP ratio (AUC 0.932), CONUT score (AUC 0.925), and LVEF (AUC 0.897). Optimal cut-off values for mortality prediction were CONUT ≥6, LVEF ≥65%, and TAPSE/sPAP ≤0.55. Kaplan–Meier analysis confirmed significantly reduced survival among patients with higher CONUT scores, higher LVEF, and an impaired TAPSE/sPAP ratio. Conclusions: In elderly patients with HFpEF, nutritional status and cardiopulmonary functional parameters are important determinants of long-term prognosis. The CONUT score emerged as the most informative immunonutritional index, while echocardiographic parameters reflecting ventricular function and right ventricular–pulmonary arterial coupling provided additional prognostic information. Integrating nutritional assessment with echocardiographic evaluation may improve risk stratification in elderly patients with HFpEF.
Keywords:
HFpEF
; nutritional status
; CONUT score
; Prognostic Nutritional Index
; CALLy index
; TAPSE/sPAP ratio
; elderly patients
; heart failure prognosis
1. Introduction
Heart failure (HF) represents one of the leading causes of morbidity and mortality worldwide and constitutes a major public health burden, particularly in aging populations [1,2,3]. The progressive aging of Western societies has resulted in a growing number of elderly patients affected by HF, with a substantial proportion of hospitalizations and deaths occurring in individuals over 80 years of age [4,5,6,7]. In this setting, heart failure with preserved ejection fraction (HFpEF) has become the predominant HF phenotype among older patients, accounting for more than half of HF cases in individuals of advanced age [8,9,10,11].
HFpEF is a complex and heterogeneous syndrome characterized by multiple comorbidities, systemic inflammation, and age-related physiological changes [12,13,14]. Unlike heart failure with reduced ejection fraction, HFpEF is strongly influenced by non-cardiac factors such as renal dysfunction, frailty, metabolic disorders, and systemic inflammatory conditions [15,16,17,18]. In very old patients, the clinical course of HFpEF is often determined not only by cardiac dysfunction but also by extra-cardiac factors including infections, nutritional status, and immune dysregulation [19,20,21,22,23,24].
Malnutrition has emerged as an important determinant of prognosis in patients with HF. Nutritional impairment is highly prevalent in HF and has been associated with worse clinical outcomes, including increased mortality and hospitalizations [25,26,27,28]. The mechanisms underlying malnutrition in HF are multifactorial and include chronic inflammation, neurohormonal activation, reduced appetite, gastrointestinal congestion, and metabolic abnormalities [29,30,31]. These processes are particularly relevant in elderly individuals, in whom malnutrition frequently coexists with frailty and immunological impairment [32,33,34].
For this reason, increasing attention has been directed toward the assessment of nutritional status using simple and reproducible indices. Among these, the Prognostic Nutritional Index (PNI), based on serum albumin levels and lymphocyte count, reflects both nutritional and immune status and has been investigated as a prognostic marker in cardiovascular diseases and HF populations [35,36,37,38]. Similarly, the Controlling Nutritional Status (CONUT) score, which incorporates serum albumin, total cholesterol levels, and lymphocyte count, was initially developed as a screening tool for hospital malnutrition and has subsequently been validated as a prognostic marker in several cardiovascular conditions, including acute and chronic HF [39,40,41,42,43,44,45,46,47,48,49]. More recently, the C-reactive protein–albumin–lymphocyte (CALLy) index has been proposed as a composite marker integrating nutritional and inflammatory parameters. By combining C-reactive protein, albumin concentration, and lymphocyte count, this index aims to capture the interaction between systemic inflammation and nutritional impairment [50,51,52,53,54]. However, evidence regarding its prognostic role in HF populations remains limited.
In elderly patients with HF, the interplay between malnutrition, inflammation, and immune dysfunction plays a key role in prognosis. Aging-related immunosenescence predisposes to infections and systemic inflammation [55], which may exacerbate catabolic processes and disease progression; infections, particularly respiratory, are frequent causes of hospitalization and death in this population [56,57].
Despite the recognized prognostic importance of nutritional status in HF, data on immunonutritional indices in very elderly HFpEF patients remain limited. This population is characterized by a high burden of comorbidities, frailty, and functional impairment, all of which may influence outcomes [58].
Our group has previously investigated clinical features of elderly HF patients, including HF with supranormal ejection fraction and risk scores [59,60,61], but the prognostic role of nutritional and immunological markers has not been systematically assessed.
Therefore, this study aimed to evaluate the prognostic value of PNI, CONUT, and CALLy indices in very elderly HFpEF patients, assessing their association with all-cause mortality and their ability to improve risk stratification.
2. Materials and Methods
2.1. Study Design and Population
The present study was designed as a retrospective observational cohort study aimed at evaluating the prognostic role of immunonutritional indices in elderly patients with HFpEF. The study population consisted of consecutive patients admitted to the Internal Medicine and Cardiology Units of IRCCS MultiMedica—San Giuseppe Hospital (Milan, Italy) for HF between January 2020 and December 2020.
A total of 200 patients were included in the study. HFpEF was defined according to current guideline criteria as the presence of signs and symptoms of HF in association with a left ventricular ejection fraction (LVEF) ≥50% and echocardiographic findings consistent with diastolic dysfunction [62].
All patients were followed longitudinally to assess long-term outcomes, with follow-up extending until February 2026.
Part of this cohort has been previously investigated by our research group in earlier studies exploring different clinical aspects of elderly patients with HF, including the characteristics of patients with supranormal ejection fraction and the prognostic value of clinical risk scores in elderly individuals with HF [59,60,61]. However, the present analysis specifically focuses on the prognostic role of immunonutritional indices in this population.
2.2. Data Collection
Clinical, laboratory, and instrumental data were retrospectively obtained from electronic medical records at the time of hospital admission. Demographic information including age and sex was collected together with data regarding cardiovascular risk factors such as hypertension, diabetes mellitus, dyslipidemia, smoking status, and obesity.
Information on non-cardiovascular comorbidities including chronic kidney disease, chronic obstructive pulmonary disease, hypothyroidism, and cognitive impairment was also recorded. In addition, cardiovascular comorbidities such as coronary artery disease, previous transient ischemic attack or stroke, and peripheral artery disease were documented.
Vital signs measured at admission were recorded, including systolic and diastolic blood pressure, heart rate, and body temperature. Information regarding the primary cause of hospital admission, pharmacological therapies administered during hospitalization, and length of hospital stay was also retrieved from the medical records.
2.3. Laboratory Assessment
Blood samples were collected at hospital admission as part of routine clinical evaluation. Laboratory parameters included hemoglobin levels, white blood cell count, neutrophil count, lymphocyte count, platelet count, serum glucose, serum iron, serum creatinine, estimated glomerular filtration rate (eGFR) [63], sodium and potassium levels, serum calcium, total bilirubin, albumin concentration, uric acid levels, and lipid profile including total cholesterol, high-density lipoprotein cholesterol (HDL cholesterol), low-density lipoprotein cholesterol (LDL cholesterol), and triglycerides.
Additional laboratory measurements included thyroid-stimulating hormone, C-reactive protein, N-terminal pro–brain natriuretic peptide (NT-proBNP), and high-sensitivity cardiac troponin.
2.4. Nutritional Risk Scores
Three immunonutritional indices were calculated for each patient using laboratory parameters obtained at hospital admission.
The PNI was calculated using a formula combining serum albumin concentration and total lymphocyte count. Specifically, PNI was derived using the equation PNI = 10 × serum albumin (g/dL) + 0.005 × total lymphocyte count (cells/mm3) [35,36,37,38].
The CONUT score was calculated using three laboratory parameters: serum albumin concentration, total cholesterol level, and total lymphocyte count. According to the original scoring system proposed by Ignacio de Ulíbarri and colleagues [64], each parameter contributes to a weighted score reflecting the degree of nutritional impairment. Serum albumin levels ≥3.5 g/dL correspond to 0 points, levels between 3.0 and 3.49 g/dL correspond to 2 points, levels between 2.5 and 2.99 g/dL correspond to 4 points, and levels <2.5 g/dL correspond to 6 points. For total lymphocyte count, values ≥1600 cells/mm3 correspond to 0 points, values between 1200 and 1599 cells/mm3 correspond to 1 point, values between 800 and 1199 cells/mm3 correspond to 2 points, and values <800 cells/mm3 correspond to 3 points. Regarding total cholesterol concentration, values ≥180 mg/dL correspond to 0 points, values between 140 and 179 mg/dL correspond to 1 point, values between 100 and 139 mg/dL correspond to 2 points, and values <100 mg/dL correspond to 3 points. The final CONUT score is obtained by summing the points assigned to each parameter, with higher scores indicating more severe nutritional impairment and immune dysfunction [42,44,46].
The CALLy index was calculated as a composite biomarker integrating inflammatory and nutritional parameters. The CALLy index was derived using the following formula: CALLy index = (serum albumin [g/dL] × lymphocyte count [/mm3]) / C-reactive protein (mg/dL) [50,51,52,53,54].
To facilitate the interpretation of the immunonutritional indices used in the present study, the commonly reported reference ranges and risk categories for the PNI, the CONUT score, and the CALLy index are summarized in Table 1.
2.5. Echocardiographic Assessment
All patients underwent transthoracic echocardiography during hospitalization as part of routine clinical evaluation. Echocardiographic examinations were performed within 48 hours of hospital admission using standard ultrasound equipment.
All echocardiographic studies were performed by a single experienced operator, in order to minimize inter-observer variability. Measurements were obtained according to current recommendations for cardiac chamber quantification and echocardiographic assessment [65,66].
Standard two-dimensional and Doppler parameters were recorded, including interventricular septal thickness, posterior wall thickness, left ventricular end-diastolic diameter, relative wall thickness, left ventricular end-diastolic and end-systolic volumes, and left ventricular ejection fraction (LVEF). Doppler measurements included the E/A ratio and E/e’ ratio for the evaluation of diastolic function.
Left atrial dimensions and volume were measured, and the presence and severity of valvular abnormalities were assessed [67]. Right ventricular function was evaluated by measuring tricuspid annular plane systolic excursion (TAPSE), while systolic pulmonary artery pressure (sPAP) was estimated using Doppler-derived measurements [68].
The ratio between TAPSE and sPAP was calculated as a noninvasive index of right ventricular–pulmonary arterial (RV–PA) coupling [69].
2.6. Follow-Up and Outcome Definition
Patients were followed longitudinally from the time of hospital admission until 2026. Follow-up data were obtained through hospital records and clinical follow-up information.
The primary outcome of the study was all-cause mortality during the follow-up period. Based on survival status at the end of follow-up, patients were categorized into two groups: those who were alive and those who had died during the observation period.
2.7. Statistical Analysis
Continuous variables were expressed as mean ± standard deviation or as median and interquartile range depending on the distribution of the data. Categorical variables were presented as absolute numbers and percentages.
Comparisons between groups were performed using Student’s t-test or the Mann–Whitney U test for continuous variables and the chi-square test for categorical variables.
Univariate Cox proportional hazards regression analysis was used to identify variables associated with mortality. A predefined set of clinically relevant variables, including demographic characteristics, comorbidities, laboratory parameters, and echocardiographic indices, was initially considered based on prior evidence and pathophysiological plausibility in HFpEF populations. To ensure model parsimony and avoid overfitting given the sample size and number of events, only variables showing significant associations in univariate analysis were subsequently entered into multivariate Cox regression models. In addition, variables with potential collinearity or overlapping biological meaning (particularly among immunonutritional indices) were carefully evaluated, and only the most informative parameters were retained in the final model.
Receiver operating characteristic (ROC) curve analysis was performed to evaluate the predictive performance of nutritional scores and echocardiographic parameters. The area under the curve (AUC) was calculated for each variable, and optimal cut-off values were determined using the Youden index.
Kaplan–Meier survival curves were constructed to evaluate differences in survival between groups, and statistical significance was assessed using the log-rank test.
A p-value lower than 0.05 was considered statistically significant. All statistical analyses were performed using SPSS software version 28 (SPSS Inc., Chicago, IL, USA).
2.8. Ethical Approval
The study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was reviewed and approved by the local Ethics Committee (reference number 464.2021). Because of the study’s retrospective design and the use of anonymized clinical data, the requirement for written informed consent was waived in accordance with national regulations.
2.9. Use of Artificial Intelligence Tools
Artificial intelligence (AI) assistance was used exclusively for linguistic revision and improvement of language clarity during manuscript preparation. ChatGPT (OpenAI, San Francisco, CA, USA) was employed only to help refine grammar, spelling, and readability of the text. AI tools were not involved in literature screening, data collection, statistical analyses, or interpretation of the study findings. The authors retain full responsibility for the scientific content and conclusions presented in this work.
3. Results
3.1. Baseline Characteristics
The study population consisted of 200 elderly patients hospitalized for HFpEF. The demographic and clinical characteristics of the study population are summarized in Table 2.
The overall cohort was characterized by advanced age and a predominance of female patients. The prevalence of traditional cardiovascular risk factors, including hypertension, diabetes mellitus, dyslipidemia, smoking, and obesity, was similar between patients who survived and those who died during follow-up.
Among non-cardiovascular comorbidities, chronic kidney disease and cognitive impairment were more frequently observed among patients who died during follow-up. In contrast, other comorbid conditions such as chronic obstructive pulmonary disease and hypothyroidism showed comparable distributions between the two groups.
Regarding clinical presentation at admission, some differences were observed in vital parameters between patients who survived and those who died during follow-up. In particular, patients who died tended to present with lower systolic blood pressure and higher heart rate at admission, suggesting a more compromised hemodynamic profile.
Body temperature at admission also differed between groups, with fever being more frequently documented among patients who died during follow-up. In contrast, symptoms related to congestion, including dyspnea and peripheral edema, were similarly distributed between the two groups.
3.2. Laboratory Findings and Nutritional Scores
Laboratory parameters and immunonutritional indices at hospital admission are reported in Table 3.
Markers of systemic inflammation and hematologic parameters differed between the two groups, with higher inflammatory activity observed among patients who died during follow-up. In particular, patients who died exhibited higher white blood cell and neutrophil counts, together with lower lymphocyte levels, indicating a shift toward a more pronounced inflammatory and immune-dysregulated profile. Differences were also observed in renal function parameters and selected metabolic variables. Specifically, the deceased group showed higher creatinine levels and lower eGFR, consistent with more advanced renal impairment, as well as lower serum iron concentrations.
Parameters reflecting nutritional status showed significant differences between groups. In particular, serum albumin and lipid profile parameters were lower among patients who died during follow-up. This pattern was characterized by reduced albumin levels and lower total, HDL, and LDL cholesterol concentrations, suggesting a state of protein–calorie malnutrition and reduced metabolic reserve in non-survivors.
Similarly, biomarkers related to HF severity, including natriuretic peptides, were higher among patients who died compared with those who survived. In addition, inflammatory burden was further supported by higher CRP levels, while NT-proBNP concentrations were markedly elevated, reflecting greater hemodynamic stress and disease severity in this group.
The distribution of the three immunonutritional indices evaluated in the present study—the PNI, the CONUT score, and the CALLy index—is also shown in Table 3. Significant differences between groups were observed for all three indices, with lower PNI and CALLy index values and higher CONUT scores among patients who died during follow-up. Overall, non-survivors displayed a consistent pattern of worse immunonutritional status, characterized by lower PNI, markedly reduced CALLy index values, and substantially higher CONUT scores, indicating the coexistence of malnutrition, systemic inflammation, and immune dysfunction.
3.3. Instrumental Findings
Chest radiography, electrocardiographic, and echocardiographic findings at hospital admission are shown in Table 4.
Regarding chest radiography, differences were observed in the distribution of radiographic patterns between groups. In particular, radiographic evidence of pulmonary infection was more frequently observed among patients who died during follow-up, whereas a normal radiographic pattern was more common among survivors. Pulmonary congestion was observed with comparable frequency in the two groups.
Electrocardiographic findings were largely similar between groups in terms of rhythm and conduction abnormalities. The prevalence of sinus rhythm, atrial fibrillation, and most conduction patterns did not differ significantly. However, right bundle branch block was more frequent among patients who died during follow-up, suggesting greater conduction system involvement or right ventricular dysfunction, whereas other abnormalities were comparable between groups.
Echocardiographic parameters describing cardiac structure showed some differences between patients who survived and those who died during follow-up. In particular, patients who died were characterized by smaller left ventricular cavity dimensions and a more pronounced pattern of concentric remodeling. This was reflected by higher indices of wall thickness and relative wall thickness, suggesting a more hypertrophic ventricular geometry.
In addition, left ventricular systolic function appeared more hyperdynamic among patients who died during follow-up, with higher ejection fraction values compared with survivors.
Differences were also observed in parameters reflecting right ventricular function and pulmonary hemodynamics. In particular, patients who died showed lower TAPSE and higher pulmonary pressures, resulting in markedly lower values of the TAPSE/sPAP ratio.
3.4. Clinical Characteristics, Causes of Admission, and In-Hospital Treatment
Clinical characteristics at admission, etiological factors, causes leading to hospitalization, and treatments administered during hospitalization are reported in Table 5.
With respect to functional status at admission, differences were observed between patients who died during follow-up and those who survived. In particular, NYHA class IV was more frequently observed among patients who died, whereas NYHA class III was more common among survivors.
Differences were also found in the underlying etiology of HF. Pulmonary hypertension was significantly more frequent among patients who died, while hypertensive heart disease was more commonly observed among survivors. Other etiologies, including coronary artery disease and valvular heart disease, showed comparable distributions between the two groups.
The clinical conditions leading to hospital admission also differed between groups. Acute respiratory conditions represented the most frequent cause of admission among patients who died, whereas congestive HF was more commonly observed among survivors. In addition, the presence of two or more concurrent causes of admission was more frequent among patients who died during follow-up.
Regarding in-hospital treatment, some differences in pharmacological therapy were observed. ACE inhibitors or angiotensin receptor blockers were more frequently prescribed among survivors, while statins, antibiotic therapy, and oxygen therapy were more commonly administered to patients who died during follow-up.
Finally, length of hospital stay was longer among patients who died during follow-up compared with those who survived.
3.5. Follow-Up and Clinical Events
Follow-up data were available for the entire study population. The median duration of follow-up was 3.8 years (interquartile range 2.1–5.9 years).
During the observation period, a substantial proportion of patients died, while the remaining individuals were alive at the end of follow-up but frequently experienced non-fatal clinical events. The distribution of mortality and the types of clinical events observed during follow-up are summarized in Table 6.
Respiratory and infectious conditions represented the most frequent causes of death in this cohort, followed by cardiovascular causes and other non-cardiovascular medical conditions. A proportion of deaths was also associated with progressive clinical deterioration and frailty-related complications.
Among patients who survived during follow-up, several experienced non-fatal events requiring medical evaluation, emergency department visits, or hospital admissions. These events were most commonly related to respiratory conditions, although cardiovascular complications, infectious diseases, metabolic disturbances, and trauma-related events were also observed.
Early mortality during the index hospitalization was relatively uncommon, occurring in 11 patients (5.5% of the study population), while the vast majority of deaths occurred during the post-discharge follow-up period.
3.6. Univariate and Multivariate Cox Regression Analysis
Univariate Cox regression analysis was performed to identify clinical, laboratory, and echocardiographic variables associated with mortality during follow-up. The results of both univariate and multivariate analyses are reported in Table 7.
In univariate analysis, several variables showed significant associations with mortality, including the PNI, the CONUT score, LVEF, and the TAPSE/sPAP ratio.
Variables that reached statistical significance in univariate analysis were subsequently entered into a multivariate Cox regression model. In the multivariate analysis, CONUT score, LVEF, and TAPSE/sPAP ratio remained independently associated with mortality. In contrast, the association between PNI and mortality was no longer significant after adjustment for other variables.
3.7. ROC Analysis
ROC curve analysis was performed to evaluate the ability of selected nutritional and echocardiographic parameters to predict mortality during follow-up. The ROC curves are shown in Figure 1.
The TAPSE/sPAP ratio demonstrated the highest discriminative performance, with an AUC of 0.932 (95% CI 0.897–0.967; p < 0.001). The CONUT score also showed excellent predictive ability, with an AUC of 0.925 (95% CI 0.887–0.964; p < 0.001). In addition, LVEF demonstrated good prognostic performance, with an AUC of 0.897 (95% CI 0.851–0.944; p < 0.001).
Overall, these results indicate that both nutritional status assessed by the CONUT score and cardiopulmonary functional parameters such as TAPSE/sPAP ratio and LVEF showed strong discriminative capacity for predicting mortality in this cohort.
3.8. Kaplan–Meier Survival Analysis
Kaplan–Meier survival curves were constructed to evaluate differences in survival according to the main prognostic variables identified in the regression analyses. The survival curves are presented in Figure 2.
Using the optimal thresholds derived from ROC curve analysis, patients were stratified according to CONUT score ≥6, LVEF ≥65%, and TAPSE/sPAP ratio ≤0.55. The CONUT cut-off of 5.5 showed a sensitivity of 88.6% and a specificity of 84.4% for predicting mortality. The optimal LVEF threshold was 65%, corresponding to a sensitivity of 87.8% and a specificity of 83.1%. For the TAPSE/sPAP ratio, the best prognostic cut-off was 0.55, with a sensitivity of 85.4% and a specificity of 96.1%.
Patients with CONUT scores ≥6 showed significantly lower survival probabilities during follow-up compared with patients with lower scores. Similarly, a TAPSE/sPAP ratio ≤0.55 was associated with markedly worse survival. Survival differences were also observed according to LVEF values: patients with supranormal LVEF (≥65%) exhibited lower survival rates compared with those with normal LVEF (<65%), suggesting that very high ejection fraction values are associated with poorer outcomes.
The differences between groups were statistically significant according to the log-rank test, confirming the prognostic relevance of these parameters.
4. Discussion
4.1. Principal Findings
The present study evaluated the prognostic relevance of three immunonutritional indices—PNI, CONUT score, and CALLy index—in a cohort of elderly patients hospitalized with HFpEF and followed over a prolonged observational period.
Several relevant findings emerge from our analysis and contribute to a better understanding of the determinants of prognosis in this complex and understudied population.
First, our data highlight the important role of nutritional status in the prognostic stratification of elderly patients with HFpEF. Among the indices analyzed, the CONUT score showed the strongest and most consistent association with mortality, maintaining its prognostic significance even after adjustment for other clinical and echocardiographic variables. In contrast, the prognostic value of PNI was attenuated after multivariable adjustment, while the CALLy index did not emerge as an independent predictor of outcome. These results indicate that composite immunonutritional indices may provide incremental prognostic information beyond conventional clinical markers.
It should be noted, however, that these three indices are not entirely independent constructs. All of them share partially overlapping components—particularly serum albumin and lymphocyte count—and therefore reflect closely related biological domains linking nutritional status, immune competence, and systemic inflammation. The stronger prognostic performance of the CONUT score observed in our study may therefore be explained by its broader multidimensional structure, as it incorporates an additional parameter (total cholesterol) reflecting caloric depletion and metabolic reserve. Accordingly, CONUT may offer a more comprehensive representation of the biological vulnerability typical of very elderly HFpEF patients.
Second, echocardiographic parameters reflecting ventricular function and cardiopulmonary interaction also played a central role in risk stratification. In particular, markers related to right ventricular performance and RV–PA coupling emerged as powerful predictors of outcome. The TAPSE/sPAP ratio showed a strong association with survival, highlighting the importance of right ventricular function and pulmonary hemodynamics in determining prognosis in patients with HFpEF. In addition, left ventricular systolic function, although preserved by definition in this population, showed a significant relationship with mortality when considered across its physiological range.
Consistent with these findings, the comparison between patients who died and those who survived during follow-up revealed distinct clinical and functional characteristics associated with adverse outcomes. Patients who died tended to present at admission with a more compromised hemodynamic profile, characterized by lower systolic blood pressure and higher heart rate. They also showed a higher prevalence of systemic inflammatory activation and markers suggestive of impaired nutritional status.
From a structural and functional standpoint, the echocardiographic profile of patients who died was characterized by features consistent with a more advanced HFpEF phenotype. These patients frequently exhibited smaller left ventricular cavity dimensions together with increased wall thickness, suggesting a pattern of concentric remodeling or hypertrophy. In addition, left ventricular systolic function tended to be more hyperdynamic in this group. At the same time, indices reflecting right ventricular function and pulmonary circulation were markedly impaired among patients who died, particularly the TAPSE/sPAP ratio, indicating a significant alteration in RV–PA coupling.
Finally, the long-term follow-up of this cohort confirmed the high burden of mortality and clinical instability typical of very elderly patients with HFpEF. Deaths occurred progressively during follow-up and were often preceded by episodes of clinical deterioration, with respiratory and infectious conditions representing frequent causes of clinical events. Overall, these observations highlight the interplay between nutritional impairment, systemic inflammation, and cardiopulmonary dysfunction in shaping prognosis in this population.
4.2. Interpretation of Findings and Comparison with Previous Studies
The findings of the present study contribute to the growing body of evidence supporting the prognostic relevance of nutritional status in patients with HF. In our cohort of elderly patients with HFpEF, nutritional impairment assessed through composite immunonutritional indices was strongly associated with long-term outcomes.
Among the indices evaluated, the CONUT score showed the most robust prognostic performance, remaining independently associated with mortality after adjustment for clinical and echocardiographic variables. These results are consistent with previous studies demonstrating that malnutrition and immune dysfunction represent important determinants of adverse outcomes in patients with HF. Several investigations have shown that the CONUT score, which integrates serum albumin levels, lymphocyte count, and cholesterol concentration, is associated with mortality and hospitalization risk in patients with both reduced and preserved ejection fraction [42,44,46]. In addition, previous reports have highlighted that CONUT may provide incremental prognostic information beyond traditional risk markers in HF populations [43,45].
Similarly, the PNI has been investigated as a marker of nutritional and inflammatory status in cardiovascular disease. Several studies have demonstrated that lower PNI values are associated with increased mortality and worse clinical outcomes in patients with HF and other cardiovascular conditions [35,36,37,38]. However, the independent prognostic value of PNI appears to be less consistent across studies, particularly after adjustment for clinical and laboratory variables, which is consistent with the attenuation observed in our multivariate analysis.
The CALLy index, originally proposed as an inflammatory-nutritional biomarker in oncologic and systemic diseases, has more recently been explored in cardiovascular populations. Although previous studies have suggested that this index may reflect the interaction between inflammation and nutritional status [50], its prognostic value in HF remains less clearly established. In the present study, the CALLy index showed a weaker association with mortality compared with CONUT and did not remain significant after multivariable adjustment.
These findings are in line with previous literature suggesting that different immunonutritional indices may capture partially distinct aspects of the complex interaction between malnutrition, systemic inflammation, and immune dysfunction in HF populations [70,71,72].
Beyond nutritional status, our findings also emphasize the importance of cardiopulmonary functional parameters in determining prognosis in HFpEF. In particular, the TAPSE/sPAP ratio emerged as a strong predictor of mortality, highlighting the critical role of RV–PA coupling. Previous studies have demonstrated that impaired right ventricular function and increased pulmonary pressures are key determinants of adverse outcomes in HFpEF [73,74,75,76].
Interestingly, our study also identified LVEF as a variable associated with outcome despite the preserved ejection fraction typical of this population. This observation likely reflects the complex relationship between ventricular geometry, myocardial mechanics, and systemic conditions in elderly patients with HFpEF. In particular, patients who died in our cohort frequently exhibited concentric remodeling and relatively hyperdynamic ventricular function, a phenotype previously reported in HF populations [77,78,79,80].
4.3. Clinical Implications
The findings of the present study have several potential implications for the clinical management of elderly patients with HFpEF.
First, our results indicate that simple and widely available immunonutritional indices may provide meaningful prognostic information in routine clinical practice. Among these, the CONUT score emerged as the most informative marker in our cohort. Because it can be easily calculated from routinely available laboratory parameters, this score may represent a practical tool for identifying elderly HFpEF patients at increased risk of adverse outcomes. Early recognition of impaired nutritional status may allow clinicians to implement targeted strategies aimed at improving nutritional balance, reducing systemic inflammatory burden, and optimizing overall clinical management.
Second, the strong prognostic value observed for the TAPSE/sPAP ratio underscores the importance of systematically assessing right ventricular function and pulmonary hemodynamics in patients with HFpEF. Incorporation of this parameter into routine echocardiographic evaluation may improve risk stratification and facilitate the identification of patients with more advanced cardiopulmonary impairment.
Third, the combined evaluation of nutritional markers and echocardiographic parameters may allow a more comprehensive assessment of patient vulnerability. Elderly individuals with HFpEF often present with a complex interaction between comorbidities, systemic inflammation, and cardiovascular dysfunction. In this population, malnutrition, chronic inflammatory activation, and acute infectious conditions frequently coexist and may contribute to a state of heightened biological vulnerability. Systemic inflammation may promote endothelial dysfunction, microvascular impairment, and myocardial remodeling, whereas malnutrition may exacerbate frailty, impair immune response, and reduce physiological reserve [81].
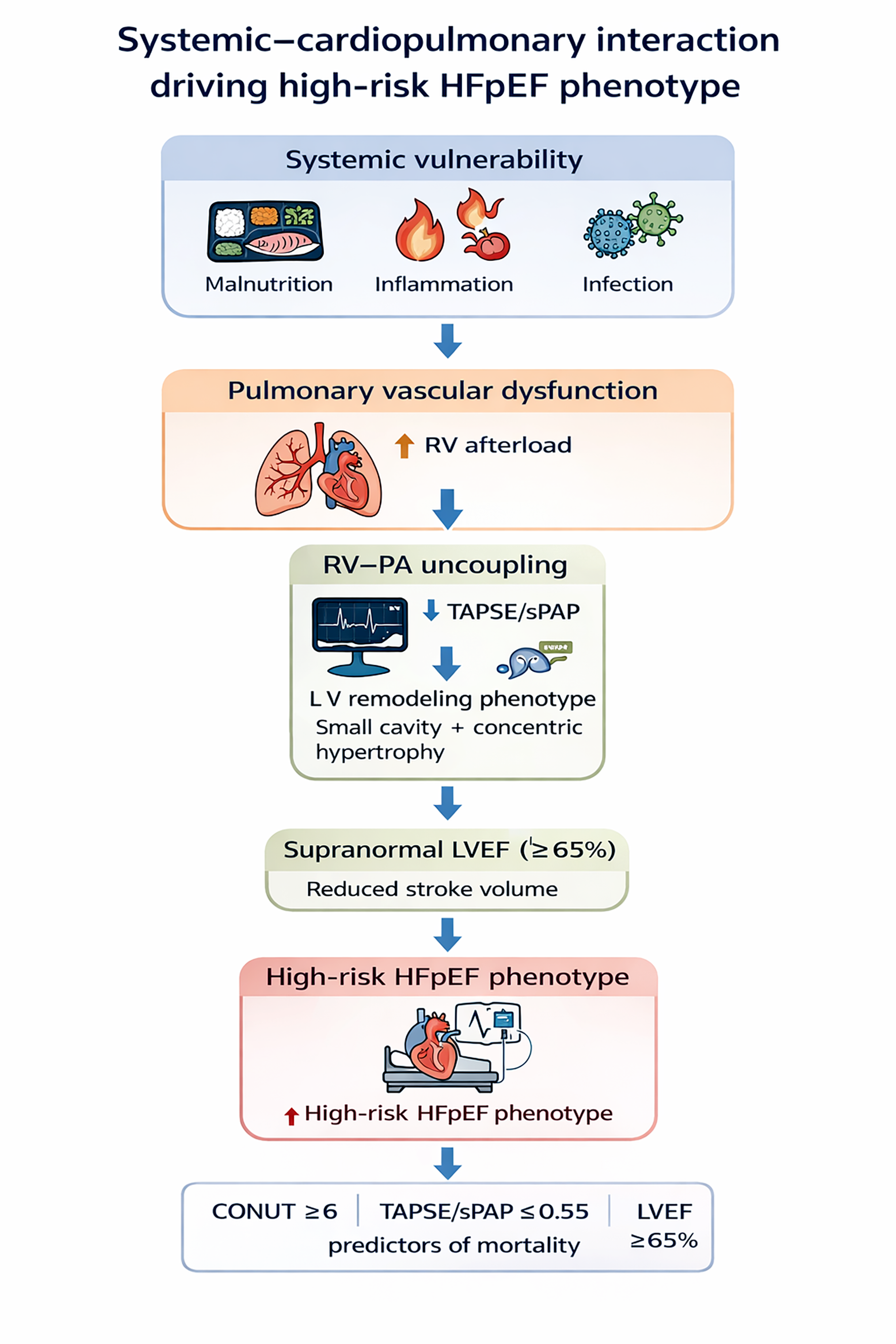
Within this framework, the coexistence of impaired nutritional status and cardiopulmonary dysfunction may identify a particularly high-risk clinical phenotype. Catabolic and inflammatory states associated with malnutrition and infection may contribute to worsening pulmonary vascular function and increased right ventricular afterload, thereby favoring the development of RV–PA uncoupling. At the same time, these systemic processes may influence left ventricular structure and performance, contributing to the complex hemodynamic profile typically observed in elderly HFpEF patients.
Consistent with this pathophysiological framework, patients who died during follow-up frequently exhibited a distinct cardiac phenotype characterized by smaller left ventricular cavity dimensions, increased wall thickness, and relatively hyperdynamic systolic function, consistent with concentric remodeling and supra-normal ejection fraction.
Over the last two decades, several studies have investigated the prognostic significance of supra-normal ejection fraction (≥65%), demonstrating a U-shaped relationship between ejection fraction and mortality in both general cardiovascular populations [82,83] and HF cohorts [77,78,79,80]. These findings suggest that markedly elevated ejection fraction values may reflect a maladaptive hemodynamic state rather than preserved cardiac function.
The mechanisms underlying HFsnEF are likely multifactorial and include increased ventricular stiffness, reduced cavity size, elevated arterial elastance, and severe diastolic dysfunction [84]. These alterations may impair ventricular filling and reduce effective stroke volume, explaining the paradox of elevated ejection fraction despite reduced forward flow [85].
In our cohort, supra-normal ejection fraction was often observed in the setting of acute infections, particularly respiratory conditions, where dehydration and sympathetic activation may promote a hypercontractile state. In addition, systemic inflammation may further exacerbate hemodynamic instability through vasodilation and endothelial dysfunction, interacting with pre-existing HFpEF-related structural abnormalities.
Taken together, these findings suggest that the coexistence of malnutrition, systemic inflammation, infection, supra-normal ejection fraction, and RV–PA uncoupling may identify a particularly vulnerable HFpEF phenotype, underscoring the need for an integrated and multidimensional clinical approach.
4.4. Strengths and Limitations
The present study has several strengths. First, it included a relatively large cohort of elderly patients with HFpEF, a population that remains underrepresented in many HF studies despite the increasing prevalence of HFpEF in advanced age. Second, the study provides long-term follow-up data, allowing a comprehensive evaluation of survival and clinical events over several years after hospitalization. Third, the analysis simultaneously evaluated multiple immunonutritional indices, enabling a direct comparison of their prognostic performance within the same patient population. Finally, the integration of clinical, laboratory, and echocardiographic variables, including indices of RV–PA coupling, allowed a multidimensional assessment of factors associated with prognosis.
However, several limitations should also be acknowledged. First, its retrospective and single-center design may limit the generalizability of the findings and introduces the possibility of selection bias. Second, although a comprehensive set of clinical, laboratory, and echocardiographic variables was included in the analysis, residual confounding due to unmeasured factors cannot be excluded. Third, the study population consisted of very elderly patients with HFpEF, and therefore the results may not be directly applicable to younger populations or to patients with different heart failure phenotypes.
In addition, immunonutritional indices were assessed only at hospital admission, and no longitudinal evaluation of their changes over time was performed. Dynamic variations in nutritional and inflammatory status may provide additional prognostic information that was not captured in the present analysis.
Finally, patient enrollment was conducted during 2020, coinciding with the COVID-19 pandemic. This may have influenced both clinical presentation and outcomes, as infection rates, healthcare system burden, and management strategies were significantly altered during this period. Therefore, the potential impact of the pandemic context should be considered when interpreting the results.
Overall, these limitations should be considered when interpreting the results, although they do not detract from the relevance of the findings regarding the prognostic role of nutritional status and cardiopulmonary functional parameters in elderly patients with HFpEF.
5. Conclusions
In this cohort of very elderly patients hospitalized with HFpEF and followed over a prolonged period, both nutritional status and cardiopulmonary functional parameters emerged as key determinants of long-term prognosis. Among the immunonutritional indices evaluated, the CONUT score demonstrated the strongest independent association with mortality, suggesting that combined alterations in nutritional and immune status play a relevant role in outcome stratification in this population.
In addition, echocardiographic parameters reflecting cardiopulmonary interaction, particularly the TAPSE/sPAP ratio, together with LVEF, provided complementary prognostic information related to RV–PA coupling and ventricular functional reserve.
Taken together, these findings highlight the potential clinical value of integrating simple nutritional indices with echocardiographic assessment of cardiopulmonary coupling in the risk stratification of elderly patients with HFpEF. A multidimensional approach combining systemic and cardiovascular markers may help identify particularly vulnerable phenotypes within this heterogeneous syndrome.
Future prospective studies are needed to confirm these observations and to determine whether targeted nutritional strategies and interventions aimed at improving cardiopulmonary function may translate into better outcomes in this high-risk population.
Author Contributions
Conceptualization, A.S.; methodology, A.S. and C.L.; software, A.S.; validation, C.L., F.N. and G.L.N.; formal analysis, A.S., C.L., A.D. and F.N.; investigation, A.S. and A.D.; resources, A.S.; data curation, A.S. and A.D.; writing—original draft preparation, A.S.; writing—review and editing, C.L., F.N. and G.L.N.; visualization, M.B. and M.L.; supervision, M.B., M.L. and S.H.; project administration, A.S.; funding acquisition, A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Italian Ministry of Health, Ricerca Corrente IRCCS MultiMedica.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee IRCCS MultiMedica (Committee’s reference number 464.2021), date of approval 21 January 2021.
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
The datasets generated and analyzed during the current study are publicly available on Zenodo at https://zenodo.org.
Acknowledgments
The authors wish to thank Monica Fumagalli for her graphical support. During the preparation of this manuscript, the authors used ChatGPT (OpenAI) exclusively for language editing and grammar improvement. After using this tool, the authors reviewed and edited the content as needed.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Savarese, G.; Becher, P.M.; Lund, L.H.; Seferovic, P.; Rosano, G.M.C.; Coats, A.J.S. Global burden of heart failure: A comprehensive and updated review of epidemiology. Cardiovasc. Res. 2023, 118, 3272–3287. [Google Scholar]
- Montalto, M.; D’Ignazio, F.; Camilli, S.; Di Francesco, S.; Fedele, M.; Landi, F.; Gallo, A. Heart failure in older patients: An update. J. Clin. Med. 2025, 14, 1982. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.; Zheng, Z.; Li, J.; Wu, S.; Sun, H.; Pang, J.; Chen, Y. Global burden of heart failure in older adults: Trends, socioeconomic inequalities, and future projections from 1990 to 2035. Eur. Heart J. Qual. Care Clin. Outcomes 2025, 11, 1123–1136. [Google Scholar] [CrossRef] [PubMed]
- Gök, G.; Zoghi, M.; Sinan, Ü.Y.; Kılıç, S.; Tokgözoğlu, L. Elder-Turk Study Investigators. Demographics of patients with heart failure who were over 80 years old and were admitted to the cardiology clinics in Turkey. Anatol. J. Cardiol. 2019, 21, 196–205. [Google Scholar] [PubMed]
- Boully, C.; Vidal, J.S.; Guibert, E.; Ghazali, F.N.; Pesce, A.; Beauplet, B.; Roger, J.D.; Carrière, I.; Timbely, B.; Idiri, H.; et al. National survey on the management of heart failure in individuals over 80 years of age in French geriatric care units. BMC Geriatr. 2019, 19, 204. [Google Scholar] [CrossRef]
- Svahn, S.; Appelblad, L.; Lövheim, H.; Gustafson, Y.; Olofsson, B.; Gustafsson, M. Prevalence of heart failure and trends in its pharmacological treatment between 2000 and 2017 among very old people. BMC Geriatr. 2024, 24, 701. [Google Scholar] [CrossRef]
- de Boer, R.A.; Abdellatif, M.; Bauersachs, J.; Roger, V.L. Heart failure in the elderly: Epidemiology, mechanisms, and management. Eur. Heart J. 2026, 47, ehag110. [Google Scholar] [CrossRef]
- Upadhya, B.; Kitzman, D.W. Heart failure with preserved ejection fraction in older adults. Heart Fail. Clin. 2017, 13, 485–502. [Google Scholar]
- Tromp, J.; Shen, L.; Jhund, P.S.; Anand, I.S.; Carson, P.E.; Desai, A.S.; Granger, C.B.; Komajda, M.; McKelvie, R.S.; Pfeffer, M.A.; et al. Age-related characteristics and outcomes of patients with heart failure with preserved ejection fraction. J. Am. Coll. Cardiol. 2019, 74, 601–612. [Google Scholar]
- Kobak, K.A.; Zarzycka, W.; Chiao, Y.A. Age and sex differences in heart failure with preserved ejection fraction. Front. Aging 2022, 3, 811436. [Google Scholar] [CrossRef]
- Gharagozloo, K.; Mehdizadeh, M.; Heckman, G.; Rose, R.A.; Howlett, J.; Howlett, S.E.; Nattel, S. Heart failure with preserved ejection fraction in the elderly population: Basic mechanisms and clinical considerations. Can. J. Cardiol. 2024, 40, 1424–1444. [Google Scholar] [CrossRef]
- Juillière, Y.; Venner, C.; Filippetti, L.; Popovic, B.; Huttin, O.; Selton-Suty, C. Heart failure with preserved ejection fraction: A systemic disease linked to multiple comorbidities, targeting new therapeutic options. Arch. Cardiovasc. Dis. 2018, 111, 766–781. [Google Scholar] [CrossRef] [PubMed]
- Roh, J.; Hill, J.A.; Singh, A.; Valero-Muñoz, M.; Sam, F. Heart failure with preserved ejection fraction: Heterogeneous syndrome, diverse preclinical models. Circ. Res. 2022, 130, 1906–1925. [Google Scholar] [CrossRef] [PubMed]
- Epelde, F. Heterogeneity in heart failure with preserved ejection fraction: A systematic review of phenotypic classifications and clinical implications. J. Clin. Med. 2025, 14, 4820. [Google Scholar] [CrossRef] [PubMed]
- Ather, S.; Chan, W.; Bozkurt, B.; Aguilar, D.; Ramasubbu, K.; Zachariah, A.A.; Wehrens, X.H.; Deswal, A. Impact of noncardiac comorbidities on morbidity and mortality in a predominantly male population with heart failure and preserved versus reduced ejection fraction. J. Am. Coll. Cardiol. 2012, 59, 998–1005. [Google Scholar]
- Rakisheva, A.; Soloveva, A.; Shchendrygina, A.; Giverts, I. Heart failure with preserved ejection fraction and frailty: From young to superaged coexisting HFpEF and frailty. Int. J. Heart Fail. 2024, 6, 93–106. [Google Scholar]
- Radakrishnan, A.; Agrawal, S.; Singh, N.; Barbieri, A.; Shaw, L.J.; Gulati, M.; Lala, A. Underpinnings of heart failure with preserved ejection fraction in women—From prevention to improving function. Am. J. Prev. Cardiol. 2025, 23, 100928. [Google Scholar] [CrossRef]
- Tanacli, R.; Trivedi, R.K.; Tajdini, M.; Jani, V.; Tian, J.; Hahn, V.S.; Vaishnav, J.; Damluji, A.A.; Gerstenblith, G.; Buta, B.; et al. Frailty status predicts adverse outcomes in ambulatory heart failure with preserved ejection fraction. JACC Adv. 2026, 5, 102560. [Google Scholar]
- Schiattarella, G.G.; Alcaide, P.; Condorelli, G.; Gillette, T.G.; Heymans, S.; Jones, E.A.V.; Kallikourdis, M.; Lichtman, A.; Marelli-Berg, F.; Shah, S.; et al. Immunometabolic mechanisms of heart failure with preserved ejection fraction. Nat. Cardiovasc. Res. 2022, 1, 211–222. [Google Scholar] [CrossRef]
- Talha, K.M.; Pandey, A.; Fudim, M.; Butler, J.; Anker, S.D.; Khan, M.S. Frailty and heart failure: State-of-the-art review. J. Cachexia Sarcopenia Muscle 2023, 14, 1959–1972. [Google Scholar]
- Zainul, O.; Perry, D.; Pan, M.; Lau, J.; Zarzuela, K.; Kim, R.; Konerman, M.C.; Hummel, S.L.; Goyal, P. Malnutrition in heart failure with preserved ejection fraction. J. Am. Geriatr. Soc. 2023, 71, 3367–3375. [Google Scholar] [CrossRef] [PubMed]
- Zhou, R.; Xia, Y.Y.; Li, Z.; Wu, L.D.; Shi, Y.; Ling, Z.Y.; Zhang, J.X. HFpEF as systemic disease: Insight from a diagnostic prediction model reminiscent of systemic inflammation and organ interaction in HFpEF patients. Sci. Rep. 2024, 14, 5386. [Google Scholar] [CrossRef]
- Gorica, E.; Geiger, M.A.; Di Venanzio, L.; Atzemian, N.; Kleeberger, J.A.; Grigorian, D.; Mongelli, A.; Emini Veseli, B.; Mohammed, S.A.; Ruschitzka, F.; et al. Cardiometabolic heart failure with preserved ejection fraction: From molecular signatures to personalized treatment. Cardiovasc. Diabetol. 2025, 24, 265. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Jankauskas, S.S.; Mone, P.; Varzideh, F.; Santulli, G. Immunology of heart failure with preserved ejection fraction. Expert Rev. Clin. Immunol. 2025, 21, 1725–1739. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Liu, J.; Wang, J.; Yan, Z.; Liang, Q.; Wang, X.; Wang, Z.; Liu, M.; Luan, X. Prevalence and impact of malnutrition on readmission among hospitalized patients with heart failure in China. ESC Heart Fail. 2022, 9, 4271–4279. [Google Scholar]
- Bansal, N.; Alharbi, A.; Shah, M.; Altorok, I.; Assaly, R.; Altorok, N. Impact of malnutrition on the outcomes in patients admitted with heart failure. J. Clin. Med. 2024, 13, 4215. [Google Scholar] [CrossRef]
- Abe, Y.; Horiuchi, Y.; Akiho, M.; Kimura, M.; Tanaka, H.; Tanaka, J.; Aoki, J.; Tanabe, K. Prognostic significance of malnutrition and physical function in patients with heart failure. Circ. Rep. 2025, 7, 904–912. [Google Scholar] [CrossRef]
- Knobloch, I.D.S.; Zucatti, K.P.; de Carvalho, B.Z.O.; da Costa-Pereira, J.P.; Hartmann, A.S.; Razzera, E.L.; Vale, M.D.M.; Souza, G.C.; Silva, F.M. Prevalence of malnutrition and its association with outcomes in heart failure: A systematic review and meta-analysis. Nutrition 2025, 28 140, 112913. [Google Scholar] [CrossRef]
- Esteban-Fernández, A.; Villar-Taibo, R.; Alejo, M.; Arroyo, D.; Bonilla Palomas, J.L.; Cachero, M.; Joaquin, C.; Méndez Bailón, M.; Pérez-Rivera, J.Á.; Romero-Vigara, J.C.; et al. Diagnosis and management of malnutrition in patients with heart failure. J. Clin. Med. 2023, 12, 3320. [Google Scholar] [CrossRef]
- Maeda, D.; Fujimoto, Y.; Nakade, T.; Abe, T.; Ishihara, S.; Jujo, K.; Matsue, Y. Frailty, sarcopenia, cachexia, and malnutrition in heart failure. Korean Circ. J. 2024, 54, 363–381. [Google Scholar] [CrossRef]
- Liu, M.; Chen, H.; Zhang, F.; Liu, S.; Sun, X.; Xu, Y.; Wu, R.; Chen, L.; Xiong, X. Factors influencing malnutrition in patients with heart failure: A scoping review based on the biopsychosocial model. Risk Manag. Healthc. Policy 2025, 18, 4011–4026. [Google Scholar] [CrossRef] [PubMed]
- Verdu-Rotellar, J.M.; Calero, E.; Duran, J.; Navas, E.; Alonso, S.; Argemí, N.; Casademunt, M.; Furió, P.; Casajuana, E.; Vinyoles, E.; et al. Impact of malnutrition on the quality of life in older patients with advanced heart failure: A cohort study. Rev. Clin. Esp. 2024, 224, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Noda, T.; Maekawa, E.; Maeda, D.; Uchida, S.; Yamashita, M.; Hamazaki, N.; Nozaki, K.; Saito, H.; Saito, K.; Ogasahara, Y.; et al. Prevalence and prognostic value of cachexia diagnosed by new definition for Asian people in older patients with heart failure. J. Cachexia Sarcopenia Muscle 2024, 15, 2660–2668. [Google Scholar] [CrossRef]
- El-Sheikh, M.; El Caidi, N.O.; Kandiah, A.; Tonning, S.H.; Taraldsen, I.A.; Wisborg, F.D.; Andersen, O.; Hove, J.D.; Grand, J. Prevalence and prognostic significance of malnutrition assessed by two scoring systems in hospitalised elderly patients with chronic heart failure. Card. Fail. Rev. 2025, 11, e26. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.Y.; Wen, J.X.; Lu, M.T.; Jian, X.Y.; Wan, X.L.; Xu, Z.W.; Liang, J.Q.; Wu, J.D. Association between prognostic nutritional index and prognosis in patients with heart failure: A meta-analysis. Front. Cardiovasc. Med. 2022, 9, 918566. [Google Scholar] [CrossRef]
- Yoshihisa, A.; Kanno, Y.; Watanabe, S.; Yokokawa, T.; Abe, S.; Miyata, M.; Sato, T.; Suzuki, S.; Oikawa, M.; Kobayashi, A.; et al. Impact of nutritional indices on mortality in patients with heart failure. Open Heart 2018, 5, e000730. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, J.; Liu, F.; Li, W.; Zhang, T.; Fang, B.; Zhang, Z.; Xie, Q.; Yang, Y.; Li, X. Prognostic nutritional index as a predictor in patients with metabolic syndrome and heart failure. Diabetes Metab. Syndr. Obes. 2023, 16, 2503–2514. [Google Scholar] [CrossRef]
- Solano, S.; Yang, M.; Tolomeo, P.; Kondo, T.; Shen, L.; Jhund, P.S.; Anand, I.S.; Desai, A.S.; Lam, C.S.P.; Maggioni, A.P.; et al. Clinical characteristics and outcomes of patients with heart failure with preserved ejection fraction and with reduced ejection fraction according to the prognostic nutritional index: Findings from PARADIGM-HF and PARAGON-HF. J. Am. Heart Assoc. 2025, 14, e037782. [Google Scholar] [CrossRef]
- Lo Buglio, A.; Bellanti, F.; Capurso, C.; Vendemiale, G. Controlling nutritional status (CONUT) score as a predictive marker in hospitalized frail elderly patients. J. Pers. Med. 2023, 13, 1119. [Google Scholar] [CrossRef]
- Di Vincenzo, O.; D’Elia, L.; Ballarin, G.; Pasanisi, F.; Scalfi, L. Controlling nutritional status (CONUT) score and the risk of mortality or impaired physical function in stroke patients: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 1501–1510. [Google Scholar] [CrossRef]
- Fărcaș, D.A.; Cerghizan, A.; Maior, R.; Mîndrilă, A.C.; Tarcea, M. CONUT score as a predictor of mortality risk in acute and chronic heart failure: A meta-analytic review. Nutrients 2025, 17, 1736. [Google Scholar] [CrossRef]
- Takada, T.; Jujo, K.; Inagaki, K.; Abe, T.; Kishihara, M.; Shirotani, S.; Endo, N.; Watanabe, S.; Suzuki, K.; Minami, Y.; et al. Nutritional status during hospitalization is associated with the long-term prognosis of patients with heart failure. ESC Heart Fail. 2021, 8, 5372–5382. [Google Scholar] [CrossRef] [PubMed]
- Kinugasa, Y.; Sota, T.; Kamitani, H.; Nakayama, N.; Nakamura, K.; Hirai, M.; Yanagihara, K.; Kato, M.; Ono, T.; Takahashi, M.; et al. Diagnostic performance of nutritional indicators in patients with heart failure. ESC Heart Fail. 2022, 9, 2096–2106. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zheng, H.; He, Y. Prognostic significance of controlling nutritional status in older adults with heart failure with preserved ejection fraction: A prospective comparative study with other objective nutritional indices. Aging Clin. Exp. Res. 2023, 35, 1305–1315. [Google Scholar] [CrossRef] [PubMed]
- Iida, Y.; Kamiya, K.; Adachi, T.; Iwatsu, K.; Kamisaka, K.; Iritani, N.; Imoto, S.; Yamada, S.; FLAGSHIP Collaborators. Prognostic impact of nutrition measures in patients with heart failure varies with coexisting physical frailty. ESC Heart Fail. 2023, 10, 3364–3372. [Google Scholar] [CrossRef]
- Xu, D.; Shen, R.; Hu, M.; Fan, Q.; Wu, J. Prognostic impact of CONUT score in older patients with chronic heart failure. BMC Geriatr. 2024, 24, 738. [Google Scholar] [CrossRef]
- Liu, S.; Fu, T.; Deng, T.; Cai, X.; Zhan, Y.; Zhu, H. Association between inflammation- and nutrition-related indicators and mortality in patients with heart failure: A cohort study. Front. Nutr. 2025, 12, 1617069. [Google Scholar] [CrossRef]
- Lu, H.; Claggett, B.L.; Minamisawa, M.; Ostrominski, J.W.; Foà, A.; Pabón, M.A.; Kalayci, A.; Vaduganathan, M.; Cikes, M.; Shah, A.M.; et al. Prognostic significance of nutritional scores in patients with heart failure: Insights from the PARAGON-HF trial. J. Am. Heart Assoc. 2025, 14, e038872. [Google Scholar] [CrossRef]
- Xie, S.; Xia, Z.; Chen, X.; Hu, H.; Lu, K.; Xiao, H. Prognostic value of CONUT, PNI, albumin, and BMI in patients with heart failure and atrial fibrillation: A retrospective cohort study. Medicine (Baltimore) 2025, 104, e44439. [Google Scholar] [CrossRef]
- Mancinetti, F.; Guazzarini, A.G.; Gaspari, M.; Croce, M.F.; Serra, R.; Mecocci, P.; Boccardi, V. Integrating nutrition, inflammation, and immunity: The CALLY index as a novel prognostic biomarker in acute geriatric care. Nutrients 2025, 17, 3192. [Google Scholar] [CrossRef]
- He, Q.; Cao, Y.; Fan, X.; Li, B.; He, Q.; Zhang, H. Long-term prognostic value of CRP-albumin-lymphocyte index in elderly patients with heart failure with preserved ejection fraction. Exp. Gerontol. 2025, 204, 112744. [Google Scholar] [CrossRef]
- Arın, C.B.; Dahir, O.F.; Adan, A.S.; Abdi, I.A.; Karataş, M. Systemic inflammatory indices and mortality risk in heart failure: A retrospective cohort study. Front. Cardiovasc. Med. 2025, 12, 1626470. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Zhang, S.; Xie, L.; Lu, H.; Wang, Q.; Xiong, Z.; Wu, Z.; Zhang, J.; Jian, Y.; Huang, W.; et al. Evaluating the prognostic significance of the modified prognostic nutritional index-C-reactive protein-to-albumin-to-lymphocyte index in acute decompensated heart failure: Special attention to the impact of diabetes. Front. Nutr. 2025, 12, 1636685. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Wu, J.; Fu, L.; Xu, D.; Li, Y. Association of the C-reactive protein-albumin-lymphocyte index with heart failure prevalence and mortality risk in older adults with hypertension: A cohort study. J. Int. Med. Res. 2026, 54, 3000605261416756. [Google Scholar] [CrossRef] [PubMed]
- Goyani, P.; Christodoulou, R.; Vassiliou, E. Immunosenescence: Aging and immune system decline. Vaccines 2024, 12, 1314. [Google Scholar] [CrossRef]
- Amara, M.; Stoler, O.; Birati, E.Y. The role of inflammation in the pathophysiology of heart failure. Cells 2025, 14, 1117. [Google Scholar] [CrossRef]
- Palin, V.; Brown, O.; Hamilton, F.; Lillie, P.; Kearney, M.; Cubbon, R.; Drozd, M. Infection in people with heart failure: An overlooked cause of adverse outcomes. Clin. Med. 2025, 25, 100497. [Google Scholar] [CrossRef]
- Lisiak, M.; Jędrzejczyk, M.; Wleklik, M.; Lomper, K.; Czapla, M.; Uchmanowicz, I. Nutritional risk, frailty and functional status in elderly heart failure patients. ESC Heart Fail. 2025, 12, 3426–3434. [Google Scholar] [CrossRef]
- Sonaglioni, A.; Lonati, C.; Scime’, V.; Nicolosi, G.L.; Bruno, A.; Lombardo, M.; Harari, S. Supra-normal ejection fraction at hospital admission stratifies mortality risk in HFpEF patients aged ≥70 years. J. Clin. Med. 2025, 14, 426. [Google Scholar]
- Sonaglioni, A.; Lonati, C.; Tescaro, L.; Nicolosi, G.L.; Proietti, M.; Lombardo, M.; Harari, S. Prevalence and clinical outcome of main echocardiographic and hemodynamic heart failure phenotypes in a population of hospitalized patients 70 years old and older. Aging Clin. Exp. Res. 2022, 34, 1081–1094. [Google Scholar] [CrossRef]
- Sonaglioni, A.; Lonati, C.; Rigamonti, E.; Viganò, M.; Nicolosi, G.L.; Proietti, M.; Lombardo, M.; Harari, S. CHA2DS2-VASc score stratifies mortality risk in heart failure patients aged 75 years and older with and without atrial fibrillation. Aging Clin. Exp. Res. 2022, 34, 1707–1720. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A Tool for Controlling Nutritional Status. First Validation in a Hospital Population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Fleisher, L.A.; Jneid, H.; Mack, M.J.; McLeod, C.J.; O’Gara, P.T.; et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e1159–e1195. [Google Scholar] [CrossRef]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Respir. J. 2023, 61, 2200879. [Google Scholar] [CrossRef]
- Tello, K.; Wan, J.; Dalmer, A.; Vanderpool, R.; Ghofrani, H.A.; Naeije, R.; Roller, F.; Mohajerani, E.; Seeger, W.; Herberg, U.; et al. Validation of the tricuspid annular plane systolic excursion/systolic pulmonary artery pressure ratio for the assessment of right ventricular-arterial coupling in severe pulmonary hypertension. Circ. Cardiovasc. Imaging 2019, 12, e009047. [Google Scholar] [CrossRef]
- Nakagomi, A.; Kohashi, K.; Morisawa, T.; Kosugi, M.; Endoh, I.; Kusama, Y.; Atarashi, H.; Shimizu, W. Nutritional status is associated with inflammation and predicts a poor outcome in patients with chronic heart failure. J. Atheroscler. Thromb. 2016, 23, 713–727. [Google Scholar] [CrossRef]
- Chen, M.; Wang, S.A.; Yang, J.; Bai, J.; Gu, J.; Luo, H.; Zhang, X.; Han, Y.; Shao, J.; Xu, Y.; et al. Association of systemic immune-inflammation index with malnutrition among Chinese hospitalized patients: A nationwide, multicenter, cross-sectional study. Front. Nutr. 2024, 11, 1375053. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Fu, T.; Deng, T.; Cai, X.; Zhan, Y.; Zhu, H. Association between inflammation- and nutrition-related indicators and mortality in patients with heart failure: A cohort study. Front. Nutr. 2025, 12, 1617069. [Google Scholar] [CrossRef] [PubMed]
- Guazzi, M.; Bandera, F.; Pelissero, G.; Castelvecchio, S.; Menicanti, L.; Ghio, S.; Temporelli, P.L.; Arena, R. Tricuspid annular plane systolic excursion and pulmonary arterial systolic pressure relationship in heart failure: An index of right ventricular contractile function and prognosis. Am. J. Physiol. Heart Circ. Physiol. 2013, 305, H1373–H1381. [Google Scholar] [PubMed]
- Gorter, T.M.; van Veldhuisen, D.J.; Voors, A.A.; Hummel, Y.M.; Lam, C.S.P.; Berger, R.M.F.; van Melle, J.P.; Hoendermis, E.S. Right ventricular-vascular coupling in heart failure with preserved ejection fraction and pre- vs. post-capillary pulmonary hypertension. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 425–432. [Google Scholar]
- Pestelli, G.; Fiorencis, A.; Trevisan, F.; Luisi, G.A.; Smarrazzo, V.; Mele, D. New measures of right ventricle-pulmonary artery coupling in heart failure: An all-cause mortality echocardiographic study. Int. J. Cardiol. 2021, 329, 234–241. [Google Scholar] [CrossRef]
- Inciardi, R.M.; Abanda, M.; Shah, A.M.; Cikes, M.; Claggett, B.; Skali, H.; Vaduganathan, M.; Prasad, N.; Litwin, S.; Merkely, B.; et al. Right ventricular function and pulmonary coupling in patients with heart failure and preserved ejection fraction. J. Am. Coll. Cardiol. 2023, 82, 489–499. [Google Scholar] [CrossRef]
- Curtis, J.P.; Sokol, S.I.; Wang, Y.; Rathore, S.S.; Ko, D.T.; Jadbabaie, F.; Portnay, E.L.; Marshalko, S.J.; Radford, M.J.; Krumholz, H.M. The association of left ventricular ejection fraction, mortality, and cause of death in stable outpatients with heart failure. J. Am. Coll. Cardiol. 2003, 42, 736–742. [Google Scholar]
- Rosch, S.; Kresoja, K.P.; Besler, C.; Fengler, K.; Schöber, A.R.; von Roeder, M.; Lücke, C.; Gutberlet, M.; Klingel, K.; Thiele, H.; et al. Characteristics of heart failure with preserved ejection fraction across the range of left ventricular ejection fraction. Circulation 2022, 146, 506–518. [Google Scholar] [CrossRef]
- Toma, M.; Ezekowitz, J.A.; Bakal, J.A.; O’Connor, C.M.; Hernandez, A.F.; Sardar, M.R.; Zolty, R.; Massie, B.M.; Swedberg, K.; Armstrong, P.W.; et al. The relationship between left ventricular ejection fraction and mortality in patients with acute heart failure: Insights from the ASCEND-HF Trial. Eur. J. Heart Fail. 2014, 16, 334–341. [Google Scholar]
- Ohte, N.; Kikuchi, S.; Iwahashi, N.; Kinugasa, Y.; Dohi, K.; Takase, H.; Masai, K.; Inoue, K.; Okumura, T.; Hachiya, K.; et al. Unfavourable outcomes in patients with heart failure with higher preserved left ventricular ejection fraction. Eur. Heart J. Cardiovasc. Imaging 2023, 24, 293–300. [Google Scholar]
- Paulus, W.J.; Zile, M.R. From systemic inflammation to myocardial fibrosis: The heart failure with preserved ejection fraction paradigm revisited. Circ. Res. 2021, 128, 1451–1467. [Google Scholar] [CrossRef]
- Wehner, G.J.; Jing, L.; Haggerty, C.M.; Suever, J.D.; Leader, J.B.; Hartzel, D.N.; Kirchner, H.L.; Manus, J.N.A.; James, N.; Ayar, Z.; et al. Routinely reported ejection fraction and mortality in clinical practice: Where does the nadir of risk lie? Eur. Heart J. 2020, 41, 1249–1257. [Google Scholar] [CrossRef]
- Stewart, S.; Playford, D.; Scalia, G.M.; Currie, P.; Celermajer, D.S.; Prior, D.; Codde, J.; Strange, G.; NEDA Investigators. Ejection fraction and mortality: A nationwide register-based cohort study of 499 153 women and men. Eur. J. Heart Fail. 2021, 23, 406–416. [Google Scholar] [CrossRef]
- Kawaguchi, M.; Hay, I.; Fetics, B.; Kass, D.A. Combined ventricular systolic and arterial stiffening in patients with heart failure and preserved ejection fraction: Implications for systolic and diastolic reserve limitations. Circulation 2003, 107, 714–720. [Google Scholar] [CrossRef]
- Cheng, S.; Fernandes, V.R.; Bluemke, D.A.; McClelland, R.L.; Kronmal, R.A.; Lima, J.A. Age-related left ventricular remodeling and associated risk for cardiovascular outcomes: The Multi-Ethnic Study of Atherosclerosis. Circ. Cardiovasc. Imaging 2009, 2, 191–198. [Google Scholar] [CrossRef]
Figure 1.
Receiver operating characteristic (ROC) curves evaluating the prognostic performance of selected nutritional and echocardiographic parameters for the prediction of mortality during follow-up in patients with heart failure with preserved ejection fraction (HFpEF). (A) Controlling Nutritional Status (CONUT) score. (B) Left ventricular ejection fraction (LVEF). (C) Tricuspid annular plane systolic excursion-to-systolic pulmonary artery pressure ratio (TAPSE/sPAP). The area under the curve (AUC) values with 95% confidence intervals are reported within each panel.
Figure 1.
Receiver operating characteristic (ROC) curves evaluating the prognostic performance of selected nutritional and echocardiographic parameters for the prediction of mortality during follow-up in patients with heart failure with preserved ejection fraction (HFpEF). (A) Controlling Nutritional Status (CONUT) score. (B) Left ventricular ejection fraction (LVEF). (C) Tricuspid annular plane systolic excursion-to-systolic pulmonary artery pressure ratio (TAPSE/sPAP). The area under the curve (AUC) values with 95% confidence intervals are reported within each panel.

Figure 2.
Kaplan–Meier survival curves illustrating differences in survival according to (A) CONUT score (<6 vs ≥6), (B) left ventricular ejection fraction (LVEF <65% vs ≥65%), and (C) tricuspid annular plane systolic excursion-to-systolic pulmonary artery pressure ratio (TAPSE/sPAP >0.55 vs ≤0.55). Survival differences between groups were assessed using the log-rank test.
Figure 2.
Kaplan–Meier survival curves illustrating differences in survival according to (A) CONUT score (<6 vs ≥6), (B) left ventricular ejection fraction (LVEF <65% vs ≥65%), and (C) tricuspid annular plane systolic excursion-to-systolic pulmonary artery pressure ratio (TAPSE/sPAP >0.55 vs ≤0.55). Survival differences between groups were assessed using the log-rank test.


Table 1.
Reference ranges and clinical interpretation of immunonutritional indices used in the study.
Table 1.
Reference ranges and clinical interpretation of immunonutritional indices used in the study.
| Index | Calculation | Normal / Low Risk | Mild Nutritional Risk | Moderate–Severe Nutritional Risk |
|---|---|---|---|---|
| PNI | 10 × albumin (g/dL) + 0.005 × lymphocyte count (/mm3) | ≥45–50 | 40–45 | <40 |
| CONUT Score | Based on albumin, total cholesterol, and lymphocyte count | 0–1 | 2–4 | ≥5 |
| CALLy Index | (Albumin × lymphocyte count) / CRP | Higher values indicate better nutritional and inflammatory status; values ≥2–3 generally associated with better prognosis | <2–3 indicates increased risk | Lower values associated with worse prognosis |
Thresholds reported in the literature may vary slightly depending on the study population and clinical context. In general, higher CONUT scores and lower PNI or CALLy values reflect more severe nutritional impairment and systemic inflammatory burden. CALLy, C-reactive protein–albumin–lymphocyte index; CONUT, Controlling Nutritional Status score; CRP, C-reactive protein; PNI, Prognostic Nutritional Index.
Table 2.
Baseline clinical characteristics of elderly patients with HFpEF according to survival status.
Table 2.
Baseline clinical characteristics of elderly patients with HFpEF according to survival status.
| All patients (n = 200) | Dead (n = 123) | Alive (n = 77) | P value | |
|---|---|---|---|---|
| Demographics | ||||
| Age (years) | 86.6 ± 6.5 | 87.0 ± 6.6 | 86.0 ± 6.3 | 0.29 |
| Females (%) | 140 (70.0) | 84 (68.3) | 56 (72.7) | 0.50 |
| Cardiovascular risk factors | ||||
| Hypertension (%) | 151 (75.5) | 91 (74.0) | 60 (77.9) | 0.49 |
| Smoking (%) | 31 (15.5) | 18 (14.6) | 13 (16.9) | 0.65 |
| Diabetes (%) | 57 (28.5) | 38 (30.9) | 19 (24.7) | 0.36 |
| Dyslipidemia (%) | 99 (49.5) | 60 (48.8) | 39 (50.6) | 0.80 |
| Obesity (%) | 25 (12.5) | 15 (12.2) | 10 (13.0) | 0.87 |
| Noncardiovascular comorbidities | ||||
| CKD (%) | 109 (54.5) | 79 (64.2) | 30 (39.0) | <0.001 |
| COPD (%) | 42 (21.0) | 26 (21.1) | 16 (20.8) | 0.96 |
| Hypothyroidism (%) | 37 (18.5) | 25 (20.3) | 12 (15.6) | 0.39 |
| Cognitive impairment (%) | 82 (41.0) | 60 (48.8) | 22 (28.6) | 0.007 |
| Cardiovascular comorbidities | ||||
| History of CAD (%) | 39 (19.5) | 28 (22.8) | 11 (14.3) | 0.16 |
| Previous TIA/stroke (%) | 37 (18.5) | 27 (22.0) | 10 (13.0) | 0.13 |
| PAD (%) | 48 (24.0) | 34 (27.6) | 14 (18.2) | 0.15 |
| Physical examination | ||||
| Dyspnea | 100 (50.0) | 60 (48.8) | 40 (51.9) | 0.68 |
| Leg swelling | 34 (17.0) | 22 (17.9) | 12 (15.6) | 0.65 |
| SBP (mmHg) | 135 (120–150) | 130.8 ± 31.0 | 140 (120–160) | 0.02 |
| DBP (mmHg) | 70 (60–80) | 69.3 ± 15.1 | 70 (60–80) | 0.18 |
| HR (bpm) | 78.5 ± 17.2 | 80.9 ± 13.9 | 74.6 ± 13.3 | 0.01 |
| Body temperature ≥37.5° (%) | 78 (39.0) | 63 (51.2) | 15 (19.5) | <0.001 |
Continuous variables are presented as mean ± standard deviation or median (interquartile range), as appropriate. Categorical variables are presented as number (percentage). Comparisons were performed between patients who died during follow-up and those who were alive at the end of follow-up. CAD, coronary artery disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DBP, diastolic blood pressure; HR, heart rate; PAD, peripheral artery disease; SBP, systolic blood pressure; TIA, transient ischemic attack.
Table 3.
Laboratory parameters and nutritional risk scores according to survival status.
| All patients (n = 200) | Dead (n = 123) | Alive (n = 77) | P value | |
|---|---|---|---|---|
| Blood tests | ||||
| Hemoglobin (g/dl) | 11.1 (9.0–12.8) | 11.1 (9.2–12.1) | 11.1 (9.7–13.2) | 0.37 |
| WBCs (× 109/L) | 9.35 (6.85–13.02) | 10.62 (7.34–14.08) | 9.12 (6.64–12.45) | <0.001 |
| Neutrophils (×109/L) | 7.94 (4.81–11.63) | 8.69 (5.92–14.44) | 6.49 (3.91–9.79) | <0.001 |
| Lymphocytes (×109/L) | 1.10 (0.79–1.59) | 0.94 (0.69–1.19) | 1.40 (0.92–2.01) | 0.01 |
| Platelets (×109/L) | 232 (164–297) | 232 (164–291) | 234 (174–299) | 0.59 |
| Glucose (mg/dL) | 121 (97–155) | 125 (99–157) | 109 (97–135) | 0.92 |
| Iron (µg/dL) | 45 (25–65) | 40 (22–66) | 50 (33–73) | 0.003 |
| Creatinine (mg/dL) | 1.23 (0.87–2.05) | 1.39 (0.92–2.21) | 1.06 (0.65–1.83) | 0.02 |
| eGFR (ml/min/m2) | 39 (23–60) | 38 (23.5–60) | 46 (29–82) | 0.006 |
| Sodium (mEq/L) | 140 (136–144) | 140 (135.3–144.0) | 138 (134–142) | 0.03 |
| Potassium (mEq/L) | 4.15 ± 0.71 | 4.15 ± 0.65 | 3.96 (3.57–4.54) | 0.92 |
| Calcium (mmol/L) | 2.10 (1.14–2.30) | 2.10 (1.34–2.20) | 2.20 (2.10–2.30) | 0.16 |
| Total bilirubin (mg/dL) | 0.70 (0.40–1.10) | 0.60 (0.40–0.90) | 0.70 (0.40–1.10) | 0.15 |
| Albumin (g/dL) | 2.99 (2.57–3.31) | 2.79 (2.42–3.16) | 3.36 (3.05–3.66) | <0.001 |
| Uric acid (mg/dL) | 7.30 (5.40–9.80) | 7.60 (5.55–9.60) | 6.70 (4.90–8.30) | 0.14 |
| Total cholesterol (mg/dL) | 139.5 (119.8–165.2) | 134 (110–160) | 150 (132–174) | <0.001 |
| HDL cholesterol (mg/dL) | 37.0 (27.0–45.0) | 34 (24–42) | 40 (32–55) | <0.001 |
| LDL cholesterol (mg/dL) | 77.0 (60.9–98.8) | 73.4 (51–90.8) | 92 (75–118) | <0.001 |
| Triglycerides (mg/dL) | 107 (86–147) | 107 (85.5–146) | 113 (89–147) | 0.11 |
| TSH (mIU/L) | 1.39 (0.82–2.00) | 1.39 (0.82–2.00) | 1.29 (0.64–2.05) | 0.45 |
| CRP (mg/dL) | 6.20 (1.20–15.80) | 6.50 (2.90–15.36) | 2.95 (0.80–7.50) | <0.001 |
| NT-proBNP (pg/mL) | 1566.5 (345.0–5055.5) | 1750 (396–7331) | 1017 (173–3596) | <0.001 |
| hs-cTn (ng/mL) | 40.0 (20.0–84.5) | 40 (20–140) | 40 (10–80) | 0.27 |
| Nutritional risk scores | ||||
| PNI | 35.9 (31.6–39.7) | 33.3 (29.6–36.8) | 43.7 (36.6–44.7) | <0.001 |
| CONUT score | 7 (5–9) | 8 (7–9) | 3.8 (2–5) | <0.001 |
| CALLy index | 0.063 (0.015–0.199) | 0.035 (0.014–0.075) | 0.22 (0.09–0.46) | <0.001 |
Continuous variables are presented as mean ± standard deviation or median (interquartile range), as appropriate. Comparisons were performed between patients who died during follow-up and those who were alive at the end of follow-up. Statistically significant results are shown in bold. CALLy, C-reactive protein–albumin–lymphocyte index; CONUT, controlling nutritional status score; CRP, C-reactive protein; eGFR, estimated glomerular filtration rate; HDL, high-density lipoprotein; hs-cTn, high-sensitivity cardiac troponin; LDL, low-density lipoprotein; NT-proBNP, N-terminal pro-B-type natriuretic peptide; PNI, prognostic nutritional index; TSH, thyroid-stimulating hormone; WBC, white blood cells.
Table 4.
Chest X-ray, electrocardiographic, and echocardiographic findings according to survival status.
Table 4.
Chest X-ray, electrocardiographic, and echocardiographic findings according to survival status.
| All patients (n = 200) | Dead (n = 123) | Alive (n = 77) | P value | |
|---|---|---|---|---|
| Chest X-ray findings | ||||
| Normal radiographic pattern (%) | 42 (21.0) | 14 (11.4) | 28 (36.4) | <0.001 |
| Pulmonary congestion (%) | 118 (59.0) | 74 (60.2) | 44 (57.1) | 0.66 |
| Radiographic evidence of pneumonia (%) | 40 (20.0) | 35 (28.4) | 5 (6.5) | <0.001 |
| ECG findings | ||||
| Sinus rhythm (%) | 141 (70.5) | 84 (68.3) | 57 (74) | 0.39 |
| AF (%) | 59 (29.5) | 39 (31.7) | 20 (26) | 0.39 |
| Normal IV conduction (%) | 88 (44.0) | 50 (40.7) | 38 (49.4) | 0.21 |
| LAFB (%) | 54 (27.0) | 32 (26) | 22 (28.6) | 0.68 |
| LBBB (%) | 8 (4.0) | 4 (3.3) | 4 (5.2) | 0.57 |
| RBBB (%) | 50 (25.0) | 37 (30) | 13 (16.9) | 0.04 |
| Conventional TTE parameters | ||||
| IVS (mm) | 13 (12–15) | 14.0 (12.0–16.0) | 13 (12–15) | 0.77 |
| PW (mm) | 10 (9–11) | 10.0 (9.0–11.0) | 10 (9–11) | 0.55 |
| LVEDD (mm) | 42 (39–47) | 41.0 ± 6.5 | 44 (39–48) | 0.001 |
| RWT | 0.50 (0.44–0.55) | 0.50 ± 0.09 | 0.47 ± 0.07 | 0.01 |
| LVEDV (ml) | 60 (45–88) | 55.0 (44.0–75.0) | 66 (50–95) | 0.02 |
| LVESV (ml) | 20 (15–28) | 17.6 (14.4–22.8) | 25.0 (19.3–34.0) | <0.001 |
| LVEF (%) | 65 (60–70) | 68.0 ± 4.8 | 60 (55–65) | <0.001 |
| E/A | 0.77 (0.66–1.55) | 0.82 (0.66–1.55) | 0.70 (0.60–1.25) | 0.08 |
| E/e’ | 16 (11–23) | 17.0 (11.0–23.0) | 16.0 (11.0–21.0) | 0.30 |
| LA A-P diameter (mm) | 46 (41–52) | 47.0 (41.0–53.0) | 46 (40–53) | 0.83 |
| LA longitudinal diameter (mm) | 56 (50–63) | 57.0 (50.0–64.0) | 56 (50–65) | 0.82 |
| LAV (ml) | 77 (55–110) | 85 (55–110) | 75 (57–110) | 0.54 |
| More than mild MR (%) | 63 (31.5) | 38 (30.9) | 25 (32.5) | 0.82 |
| More than mild AR (%) | 8 (4.0) | 3 (2.4) | 5 (6.5) | 0.13 |
| More than mild AS (%) | 23 (11.5) | 13 (10.6) | 10 (13) | 0.63 |
| More than mild TR (%) | 57 (28.5) | 36 (29.3) | 21 (27.3) | 0.77 |
| RVIT (mm) | 30 (26–35) | 30.0 (26.0–35.0) | 31 (27–35) | 0.28 |
| TAPSE (mm) | 18 (14–22) | 16 (11–28) | 22 (20–25) | <0.001 |
| sPAP (mmHg) | 45 (25–100) | 49 (24–100) | 40 (25–100) | <0.001 |
| TAPSE/sPAP (mm/mmHg) | 0.45 (0.31–0.63) | 0.32 (0.25–0.45) | 0.74 (0.63–0.88) | <0.001 |
| Aortic root (mm) | 34.1 ± 4.1 | 33.0 ± 4.7 | 34.5 ± 4.6 | 0.13 |
| Ascending aorta (mm) | 35.3 ± 4.6 | 35.0 ± 4.6 | 36.0 ± 4.7 | 0.14 |
Continuous variables are presented as mean ± standard deviation or median (interquartile range), as appropriate. Categorical variables are presented as number (percentage). Comparisons were performed between patients who died during follow-up and those who were alive at the end of follow-up. Significant differences are indicated in bold. AF, atrial fibrillation; AR, aortic regurgitation; AS, aortic stenosis; ECG, electrocardiogram; IVS, interventricular septum; LA, left atrium; LAFB, left anterior fascicular block; LAV, left atrial volume; LBBB, left bundle branch block; LVEDD, left ventricular end-diastolic diameter; LVEDV, left ventricular end-diastolic volume; LVEF, left ventricular ejection fraction; LVESV, left ventricular end-systolic volume; MR, mitral regurgitation; PW, posterior wall; RBBB, right bundle branch block; RVIT, right ventricular inflow tract; RWT, relative wall thickness; sPAP, systolic pulmonary artery pressure; TAPSE, tricuspid annular plane systolic excursion; TR, tricuspid regurgitation; TTE, transthoracic echocardiography.
Table 5.
Clinical presentation at admission, underlying etiology of heart failure, causes of hospitalization, and in-hospital treatment according to survival status.
Table 5.
Clinical presentation at admission, underlying etiology of heart failure, causes of hospitalization, and in-hospital treatment according to survival status.
| All patients (n = 200) | Dead (n = 123) | Alive (n = 77) | P value | |
|---|---|---|---|---|
| NYHA functional status at admission | ||||
| NYHA III (%) | 124 (62) | 68 (55.3) | 56 (72.7) | 0.01 |
| NYHA IV (%) | 76 (38) | 55 (44.7) | 21 (27.3) | 0.01 |
| Underlying etiology of heart failure | ||||
| CAD (%) | 64 (32) | 44 (35.8) | 20 (26) | 0.14 |
| VHD (%) | 42 (21) | 26 (21.1) | 16 (20.8) | 0.95 |
| HHD (%) | 60 (30) | 30 (24.4) | 30 (39) | 0.03 |
| PH (%) | 34 (17) | 30 (24.4) | 4 (5.2) | 0.001 |
| Main causes leading to hospital admission | ||||
| CHF (%) | 48 (24) | 10 (8.1) | 38 (49.3) | <0.001 |
| Acute respiratory conditions (%) | 87 (43.5) | 68 (55.3) | 19 (24.7) | <0.001 |
| Gastro-intestinal disorders (%) | 8 (4) | 6 (4.9) | 2 (2.6) | 0.42 |
| Severe anemia (%) | 16 (8) | 11 (8.9) | 5 (6.5) | 0.44 |
| Severe CKD (%) | 9 (4.5) | 5 (4.1) | 4 (5.2) | 0.72 |
| Cancers (%) | 8 (4) | 5 (4.1) | 3 (3.9) | 0.95 |
| Hyponatremia (%) | 16 (8) | 12 (9.8) | 4 (5.2) | 0.22 |
| Hypernatremia (%) | 5 (2.5) | 4 (3.3) | 1 (1.3) | 0.36 |
| Neurological disorders (%) | 3 (1.5) | 2 (1.6) | 1 (1.3) | 0.86 |
| ≥2 causes of admission (%) | 58 (29) | 45 (36.6) | 13 (16.9) | 0.002 |
| Pharmacological therapy during hospitalization | ||||
| Antiplatelets (%) | 74 (37) | 47 (38.2) | 27 (35.1) | 0.64 |
| Anticoagulants (%) | 82 (41) | 50 (40.7) | 32 (41.6) | 0.89 |
| ACEIs/ARBs (%) | 84 (42.0) | 40 (32.5) | 44 (57.1) | <0.001 |
| CCB (%) | 51 (25.5) | 29 (23.6) | 22 (28.6) | 0.46 |
| BB (%) | 115 (57.5) | 68 (55.3) | 47 (61) | 0.43 |
| Digoxin (%) | 59 (29.5) | 39 (31.7) | 20 (26) | 0.36 |
| Loop diuretics (%) | 132 (66) | 82 (66.7) | 50 (64.9) | 0.77 |
| MRAs (%) | 73 (36.5) | 47 (38.2) | 26 (33.8) | 0.55 |
| Statins (%) | 58 (29) | 28 (22.8) | 30 (39.0) | 0.02 |
| Corticosteroids (%) | 58 (29) | 41 (33.3) | 17 (22.1) | 0.08 |
| Antibiotics (%) | 126 (63) | 101 (82.1) | 25 (32.5) | <0.001 |
| Oxygen therapy (%) | 73 (36.5) | 53 (43.1) | 20 (26) | 0.02 |
| Oral hypoglycemic agents (%) | 20 (10) | 10 (8.1) | 10 (13) | 0.28 |
| Insulin (%) | 25 (12.5) | 18 (14.6) | 7 (9.1) | 0.29 |
| LOS (days) | 9.4 ± 6.2 | 10.6 ± 6.5 | 7.5 ± 5.3 | 0.01 |
Continuous variables are presented as mean ± standard deviation, whereas categorical variables are presented as number (percentage). Comparisons were performed between patients who died during follow-up and those who were alive at the end of follow-up. Statistically significant values are shown in bold. ACEIs, angiotensin-converting enzyme inhibitors; ARBs, angiotensin receptor blockers; BB, beta-blockers; CAD, coronary artery disease; CCB, calcium channel blockers; CHF, congestive heart failure; CKD, chronic kidney disease; HHD, hypertensive heart disease; LOS, length of stay; MRAs, mineralocorticoid receptor antagonists; NYHA, New York Heart Association; PH, pulmonary hypertension; VHD, valvular heart disease.
Table 6.
Mortality distribution and non-fatal clinical events during follow-up.
| Category | n (%) |
|---|---|
| Overall mortality | 123 (61.5) |
| Patients alive at end of follow-up | 77 (38.5) |
| Causes of death (n = 123) | |
| Respiratory infections / respiratory failure | 48 (39.0) |
| Cardiovascular causes (HF progression, acute cardiac events) | 31 (25.2) |
| Multisystem deterioration / frailty-related conditions | 21 (17.1) |
| Other non-cardiovascular causes | 23 (18.7) |
| Non-fatal events among survivors (n = 77) | |
| Respiratory events (dyspnea, infections, COPD exacerbation) | 30 (39.0) |
| Cardiovascular events (HF worsening, ACS) | 14 (18.2) |
| Non-respiratory infections | 10 (13.0) |
| Renal/metabolic complications | 9 (11.7) |
| Trauma/falls/fractures | 8 (10.4) |
| Other medical causes | 6 (7.8) |
Values are presented as number (percentage). Causes of death are reported among patients who died during follow-up (n = 123). Non-fatal events are reported among patients who were alive at the end of follow-up (n = 77). Percentages for causes of death and non-fatal events are calculated within the corresponding subgroup. ACS, acute coronary syndrome; COPD, chronic obstructive pulmonary disease; HF, heart failure.
Table 7.
Univariate and multivariate Cox regression analysis for predictors of all-cause mortality.
| Variable | Univariate HR (95% CI) | P value | Multivariate HR (95% CI) | P value |
|---|---|---|---|---|
| Age | 1.00 (0.97–1.03) | 0.755 | — | — |
| Female sex | 0.70 (0.48–1.03) | 0.077 | — | — |
| Diabetes mellitus | 1.37 (0.93–2.02) | 0.111 | — | — |
| Coronary artery disease | 1.21 (0.79–1.84) | 0.377 | — | — |
| Systolic blood pressure | 0.997 (0.992–1.003) | 0.324 | — | — |
| eGFR | 0.995 (0.986–1.004) | 0.225 | — | — |
| Sodium | 1.002 (0.979–1.026) | 0.872 | — | — |
| Loop diuretics | 1.20 (0.81–1.77) | 0.354 | — | — |
| E/e’ | 1.01 (0.99–1.04) | 0.366 | — | — |
| PNI | 0.935 (0.909–0.961) | <0.001 | 1.001 (0.967–1.036) | 0.940 |
| CONUT score | 1.244 (1.153–1.343) | <0.001 | 1.136 (1.027–1.256) | 0.013 |
| CALLy index | 0.96 (0.69–1.34) | 0.829 | — | — |
| LVEF | 1.093 (1.055–1.132) | <0.001 | 1.056 (1.014–1.099) | 0.008 |
| TAPSE/sPAP ratio | 0.086 (0.035–0.213) | <0.001 | 0.222 (0.082–0.603) | 0.003 |
Hazard ratios (HR) with corresponding 95% confidence intervals (CI) were calculated using Cox proportional hazards regression analysis. Variables significantly associated with mortality in the univariate analysis were entered into the multivariate model to identify independent predictors of all-cause mortality during follow-up. Statistically significant values are in bold. CALLy, C-reactive protein–albumin–lymphocyte index; CI, confidence interval; CONUT, controlling nutritional status score; eGFR, estimated glomerular filtration rate; HR, hazard ratio; LVEF, left ventricular ejection fraction; PNI, prognostic nutritional index; TAPSE, tricuspid annular plane systolic excursion; sPAP, systolic pulmonary artery pressure.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



