Submitted:
30 March 2026
Posted:
31 March 2026
You are already at the latest version
Abstract
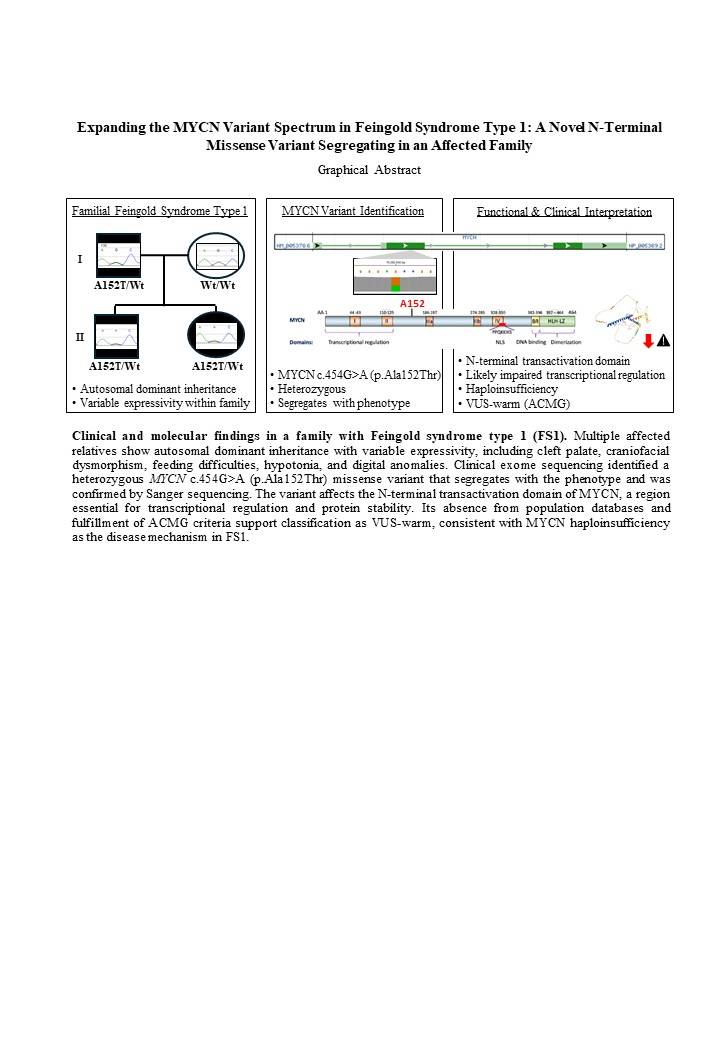
This study reports a previously unrecognized heterozygous MYCN missense variant, c.454G>A (p.Ala152Thr), identified in a child and two affected relatives with clinical findings consistent with Feingold syndrome type 1, an autosomal dominant developmental disorder most commonly caused by loss-of-function variants in MYCN. The proband presented with cleft palate, craniofacial dysmorphism, feeding difficulties, hypotonia, and characteristic digital anomalies. Similar features were observed in the father and sibling. Clinical exome sequencing revealed the novel MYCN variant, which was confirmed by Sanger sequencing and demonstrated co-segregation with the phenotype. Although most pathogenic MYCN variants leading to FS1 truncate the protein, this missense change lies within the N-terminal transactivation domain, a region involved in transcriptional regulation and protein stability. The physicochemical alteration introduced at residue Ala152 may plausibly affect MYCN function, consistent with haploinsufficiency as the established disease mechanism. According to the 2024 ACGS Best Practice Guidelines, the variant is classified as a Variant of Uncertain Significance leaning toward pathogenicity (VUS-warm). This report expands the mutational spectrum of MYCN, supports the potential clinical relevance of N-terminal missense variation in MYCN, and highlights intrafamilial phenotypic variability in FS1.
Keywords:
Feingold syndrome type I
; MYCN
; developmental disorder
; congenital abnormalities
; case report
Introduction
Feingold Syndrome (FS) is a rare autosomal dominant developmental disorder first described in 1975, characterized by microcephaly, digital anomalies, craniofacial dysmorphism, gastrointestinal (GI) atresia, and mild-to-moderate intellectual disability. Core manifestations include brachymesophalangy of the 2nd and 5th digits, 5th finger clinodactyly, toe syndactyly, and microcephaly. Historically, FS has also been referred to as ODED, MODED, and MMT syndromes (MIM 164280). Penetrance is generally complete with marked variable expressivity, and approximately 60% of cases are inherited [1,2,3,4,5,6,7,8,9].
Two molecularly distinct forms are recognized (Table 1). FS type 1 (FS1, MIM 164280) is caused by loss-of-function (LoF) variants in MYCN (MIM 164840) at 2p24.3. MYCN encodes N-Myc, a transcription factor of the MYC family, essential for embryonic development of the nervous system, limbs, and viscera [5,10,11]. The canonical protein, encoded by exons 2 and 3, contains C-terminal bHLH and leucine-zipper domains required for dimerization and DNA binding. FS1 results from MYCN haploinsufficiency, most commonly due to nonsense or frameshift variants that truncate the protein and disrupt these domains [5,6].
In contrast, gain-of-function (GoF) missense variants in MYCN cause Megalencephaly-Polydactyly Syndrome (MPS, MIM 620748), a phenotypic mirror of FS1 characterized by megalencephaly and postaxial polydactyly. These variants (e.g., T58M, P60Leu) impair Thr58 phosphorylation, increasing protein stability [12].
FS type 2 (FS2, MIM 614326) results from heterozygous deletion of 13q31.3, including MIR17HG, leading to miR-17~92 haploinsufficiency [13,14]. Although FS1 and FS2 overlap clinically, they involve distinct molecular pathways [4,15].
In this work, we identify the novel heterozygous missense MYCN variant c.454G>A (p.Ala152Thr), classified as VUS-warm, segregating in a family with FS1 features, expanding the MYCN variant spectrum and contributing to genotype-phenotype refinement.
Materials and Methods
Clinical Data
The proband and first-degree relatives were evaluated at the Genetics Department of Málaga Regional University Hospital. Clinical assessment included physical examination and detailed personal and family history. Written informed consent for participation and publication was obtained.
Genomic DNA (gDNA) Extraction
Genomic DNA was extracted from peripheral blood (Magna Pure 24, Roche). DNA quantity and quality were assessed by Qubit 3.0 and NanoDrop ND-2000. DNA integrity and purity were evaluated based on 260/280 and 260/230 absorbance ratios.
Sanger Sequencing Analysis
Exon 2 of MYCN was amplified by PCR and sequenced by automated Sanger sequencing using M13-tagged primers. Sequences were aligned to NM_005378.6 with Mutation Surveyor software. Primer sequences were: MYCN_2F (Forward): 5′- GTAAAACGACGGCCAGTctgcatgtggagcggcttc -3′ and MYCN_2R (Reverse): 5′- AGCGGATAACAATTTCACACAGGgccaagacatacgagcactaacaaa -3′.
Clinical Exome Sequencing
Whole exome sequencing (WES) was performed using KAPA HyperPlus library preparation and KAPA HyperExome capture, sequenced on an Illumina NextSeq 550 platform. Bioinformatic analysis included quality control, alignment to hg19, SNV/indel and CNV detection, coverage assessment, and annotation (GenoSystem software). Variant classification followed ACMG/AMP guidelines with ACGS 2024 refinements [15,16]. Variants classified as pathogenic, likely pathogenic, or of VUS were reviewed by a multidisciplinary team in collaboration with the referring clinician.
Approval from the ethics committee is not required for standard clinical practice. In any case, the committee was informed. However, patients and their legal representatives were asked to provide authorization for the publication of their medical data and relevant photographs through informed consent. All procedures adhered to ethical standards and the Declaration of Helsinki.
Results
Clinical Evaluation
The proband is a three-year-old child referred for incomplete cleft palate. She was born at 39+6 weeks (birth weight 2,600 g; head circumference 35 cm, 35th percentile) after an uncomplicated pregnancy. She presents feeding difficulties requiring nasogastric tube feeding. Newborn metabolic screening was normal.
Examination revealed incomplete cleft palate and craniofacial dysmorphism, including hypotelorism, low nasal bridge, epicanthal folds, bilateral orbital insufficiency with proptosis, anteverted nares, and retrognathia. Additional findings included widely spaced nipples and syndactyly of the third, fourth, and fifth toes of the right foot with hypoplasia of the fourth toe (Figure 1). Neurological examination revealed mild axial hypotonia and intermittent strabismus; deep tendon reflexes were normal. Transfontanellar ultrasound was normal.
Family history revealed that the father has complete cleft palate, short stature treated with growth hormone, and syndactyly. The six-year-old sibling presents syndactyly and milder dysmorphic features than her sister (hypotelorism, epicanthal folds, and bilateral orbital insufficiency with proptosis) (Figure 1). The mother is asymptomatic. No additional congenital anomalies have been reported among relatives.
Genetic analyses
WES identified a previously unreported heterozygous MYCN variant, c.454G>A (p.Ala152Thr), in exon 2 (NM_005378.6) (Table 2, Figure 2C). Sanger sequencing confirmed the variant and demonstrated co-segregation in two informative meioses. The variant substitutes alanine with threonine at position 152, a moderately conserved residue located in the N-terminal transactivation domain near Myc boxes (Figure 2A), a region critical for transcriptional regulation and cofactor interaction [17].
This variant was evaluated using ACMG/AMP criteria with ClinGen/ACGS-specific refinements. The variant is absent from gnomAD (PM2_moderate), co-segregation supports PP1, and the phenotype is highly specific to MYCN-related Feingold syndrome (PP4_supporting), while in silico analyses support BP4 (supporting benign). Integration of these criteria within the ACGS Bayesian framework does not reach the posterior probability threshold for likely pathogenic classification. Therefore, the variant is classified as a Variant of Uncertain Significance leaning toward pathogenicity (VUS-warm).
Additional complementary studies provided by the proband (karyotype and 180K array CGH) did not show structural or numerical abnormalities.
Discussion
The novel MYCN p.Ala152Thr variant lies within the N-terminal regulatory region, outside the canonical bHLH–LeuZ domains. Although most FS1-associated variants are truncating, missense variants affecting regulatory regions have also been reported, particularly when they affect regions essential for protein stability, transcriptional regulation, or post-translational modification [6,18,19,20].
The N-terminal region of MYCN contains regulatory elements that govern protein turnover, including phosphorylation sites and motifs that modulate proteasomal degradation. Although Ala152 is not part of a known phosphorylation consensus sequence, its location places it near regions critical for maintaining the structural configuration required for proper targeting to ubiquitin-mediated degradation pathways [17].
The substitution introduces a polar residue capable of hydrogen bonding, which may plausibly influence local protein conformation or interaction surfaces, potentially affecting transcriptional activity or protein stability (Figure 2A). However, functional studies would be required to confirm the precise molecular impact.
The segregation of the variant with the phenotype in the proband, father, and sibling provides supportive evidence for its clinical relevance. All affected individuals exhibit features consistent with FS1; these findings are compatible with reduced MYCN function during embryogenesis, consistent with the established haploinsufficiency mechanism. The absence of the variant from population databases supports rarity, although this alone does not establish pathogenicity. Although in silico tools predict a tolerated effect, these algorithms may underestimate pathogenicity in regions where structural changes have subtle but functionally relevant consequences. Indeed, several pathogenic MYCN missense variants reported in FS1 involve residues outside the C-terminal domains and exert their effect through impairment of transcriptional function rather than through gross structural disruption.
The phenotypic presentation in this family also highlights the variable expressivity that characterizes FS1. The proband presents more pronounced craniofacial features and feeding difficulties, while the father shows a milder but clearly overlapping spectrum. Such intra-familial variability is well documented in FS1 and likely reflects modifier genes or environmental influences that modulate the impact of MYCN haploinsufficiency.
It is important to note that the variant described here differs mechanistically from the GoF missense variants associated with MPS, which cluster around residues critical for MYCN phosphorylation and stabilization (e.g., Thr58, Pro60). These GoF variants enhance protein stability and activity, producing clinical manifestations that are the inverse of FS1. The p.Ala152Thr variant is located outside this hotspot, supporting a mechanism consistent with reduced MYCN activity.
This report contributes to the expanding variant spectrum of MYCN and underscores the importance of careful interpretation of missense variants within regulatory domains. Further accumulation of molecular, segregation, and functional data will be essential to clarify the clinical significance of this variant and to refine genotype–phenotype correlations in MYCN-related Feingold syndrome.
Author Contributions
FJM: Writing–review and editing. JPP: Data curation, Writing–review and editing. IOM: Writing–original draft, Writing–review and editing.
Conflicts of Interest
The authors declare no conflicts of interest.
A Data Availability Statement
Data sharing is not applicable to this article as no publicly available datasets were generated or analysed in this study.
Consent
Written consent was obtained for the publication of this case.
References
- Marcelis CLM, de Brouwer APM. Feingold Syndrome 1. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, eds. GeneReviews®. Seattle (WA): University of Washington, Seattle; June 30, 2009.
- Brunner, H. G., & Winter, R. M. (1991). Autosomal dominant inheritance of abnormalities of the hands and feet with short palpebral fissures, variable microcephaly with learning disability, and oesophageal/duodenal atresia. Journal of Medical Genetics, 28(6), 389–394. [CrossRef]
- Feingold, M., Hall, B. D., Lacassie, Y., & Martínez-Frías, M. L. (1997). Syndrome of microcephaly, facial and hand abnormalities, tracheoesophageal fistula, duodenal atresia, and developmental delay. American Journal of Medical Genetics, 69(3), 245–249.
- Celli, J., van Beusekom, E., Hennekam, R. C. M., Gallardo, M. E., Smeets, D. F. C. M., de Córdoba, S. R., Innis, J. W., Frydman, M., König, R., Kingston, H., Tolmie, J., Govaerts, L. C. P., van Bokhoven, H., & Brunner, H. G. (2000). Familial syndromic esophageal atresia maps to 2p23-p24. American Journal of Human Genetics, 66(2), 436–444. [CrossRef]
- van Bokhoven, H., Celli, J., van Reeuwijk, J., Rinne, T., Glaudemans, B., van Beusekom, E., Rieu, P., Newbury-Ecob, R. A., Chiang, C., & Brunner, H. G. (2005). MYCN haploinsufficiency is associated with reduced brain size and intestinal atresias in Feingold syndrome. Nature Genetics, 37(5), 465–467. [CrossRef]
- Marcelis, C. L. M., Hol, F. A., Graham, G. E., Rieu, P. N. M. A., Kellermayer, R., Meijer, R. P. P., Lugtenberg, D., Scheffer, H., van Bokhoven, H., Brunner, H. G., & de Brouwer, A. P. M. (2008). Genotype-phenotype correlations in MYCN-related Feingold syndrome. Human Mutation, 29(9), 1125–1132. [CrossRef]
- Burnside, R. D., Molinari, S., Botti, C., Brooks, S. S., Chung, W. K., Mehta, L., Schwartz, S., & Papenhausen, P. (2018). Features of Feingold syndrome 1 dominate in subjects with 2p deletions including MYCN. American Journal of Medical Genetics Part A, 176(9), 1956–1963. [CrossRef]
- Muriello, M., Kim, A. Y., Sondergaard Schatz, K., Beck, N., Gunay-Aygun, M., & Hoover-Fong, J. E. (2019). Growth hormone deficiency, aortic dilation, and neurocognitive issues in Feingold syndrome 2. American Journal of Medical Genetics Part A, 179(3), 410–416. [CrossRef]
- Zeka, N., Bejiqi, R., Gerguri, A., Zogaj, L., & Jashari, H. (2022). A new variant of MYCN gene as a cause of Feingold syndrome. Clinical Case Reports, 10(5), e05886. [CrossRef]
- Ruiz-Pérez MV, Henley AB, Arsenian-Henriksson M. The MYCN Protein in Health and Disease. Genes (Basel). 2017;8(4):113. Published 2017 Mar 30. [CrossRef]
- Ota, S., Zhou, Z. Q., Keene, D. R., Knoepfler, P., & Hurlin, P. J. (2007). Activities of N-Myc in the developing limb link control of skeletal size with digit separation. Development, 134(8), 1583–1592. [CrossRef]
- Nishio Y, Kato K, Tran Mau-Them F, et al. Gain-of-function MYCN causes a megalencephaly-polydactyly syndrome manifesting mirror phenotypes of Feingold syndrome. HGG Adv. 2023;4(4):100238. [CrossRef]
- de Pontual, L., Yao, E., Callier, P., Faivre, L., Drouin, V., Cariou, S., Van Haeringen, A., Geneviève, D., Goldenberg, A., Oufadem, M., Manouvrier, S., Munnich, A., Vidigal, J. A., Vekemans, M., Lyonnet, S., Henrion-Caude, A., Ventura, A., & Amiel, J. (2011). Germline deletion of the miR-17 ~ 92 cluster causes skeletal and growth defects in humans. Nature Genetics, 43(10), 1026–1030. [CrossRef]
- Tassano, E., Di Rocco, M., Signa, S., & Gimelli, G. (2013). De novo 13q31.1–q32.1 interstitial deletion encompassing the miR-17-92 cluster in a patient with Feingold syndrome-2. American Journal of Medical Genetics Part A, 161A(4), 894–896. [CrossRef]
- Richards S, Aziz N, Bale S, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015;17(5):405-424. [CrossRef]
- Durkie M, Cassidy EJ, Berry I, et al. ACGS Best Practice Guidelines for Variant Classification in Rare Disease. Association for Clinical Genomic Science; 2024. Accessed [15 Feb 2026].
- Liu Z, Chen SS, Clarke S, Veschi V, Thiele CJ. Targeting MYCN in Pediatric and Adult Cancers. Front Oncol. 2021;10:623679.
- Blaumeiser, B., Oehl-Jaschkowitz, B., Borozdin, W., & Kohlhase, J. (2008). Feingold syndrome associated with two novel MYCN mutations in sporadic and familial cases including monozygotic twins. American Journal of Medical Genetics Part A, 146A(17), 2304–2307. [CrossRef]
- Cognet M, Nougayrede A, Malan V, et al. Dissection of the MYCN locus in Feingold syndrome and isolated oesophageal atresia. Eur J Hum Genet. 2011;19(5):602-606. [CrossRef]
- Peleg, A., Kurolap, A., Sagi-Dain, L., Larom-Khan, G., Adir, V., Mory, A., Paperna, T., Shuldiner, A. R., Gonzaga-Jauregui, C., Adir, N., Baris Feldman, H., & Wollstein, R. (2021). A novel mutation in MYCN gene causing congenital absence of the flexor pollicis longus tendon as an unusual presentation of Feingold syndrome 1. Clinical Dysmorphology, 30(2), 71–75. [CrossRef]
Figure 1.
Overlapping physical features. (A) From top to bottom: right eye, right foot, left eye and left foot of the proband. (B) and (C) show, from right to left, the right eye, right foot, left eye and left foot of the father and sibling, respectively.
Figure 1.
Overlapping physical features. (A) From top to bottom: right eye, right foot, left eye and left foot of the proband. (B) and (C) show, from right to left, the right eye, right foot, left eye and left foot of the father and sibling, respectively.

Figure 2.
Results of genetic analyses. (A) The structure and functional domains of MYCN, showing the position of the A152T variant (adapted from Liu et al., 2021 25). (B) Pedigree of the family showing the affected proband (II-2). The father (I-1) and sibling (II-1) are also affected, while the mother (I-2) is unaffected with the wild-type alleles. (C) Integrative Genomics Viewer (IGV) image from whole-exome sequencing (WES) showing the heterozygous missense variant at the MYCN gene on chromosome 2 (Chr2:16082640, hg19). (D) The result of a family segregation study using Sanger sequencing confirms the presence of a heterozygous missense mutation (c.454G>A; p.Ala152Thr) in the proband, their father and their sibling, and its absence in their mother.
Figure 2.
Results of genetic analyses. (A) The structure and functional domains of MYCN, showing the position of the A152T variant (adapted from Liu et al., 2021 25). (B) Pedigree of the family showing the affected proband (II-2). The father (I-1) and sibling (II-1) are also affected, while the mother (I-2) is unaffected with the wild-type alleles. (C) Integrative Genomics Viewer (IGV) image from whole-exome sequencing (WES) showing the heterozygous missense variant at the MYCN gene on chromosome 2 (Chr2:16082640, hg19). (D) The result of a family segregation study using Sanger sequencing confirms the presence of a heterozygous missense mutation (c.454G>A; p.Ala152Thr) in the proband, their father and their sibling, and its absence in their mother.


Table 1.
Clinical and Genetic Features of Feingold Syndrome Type 1 (FS1) vs Type 2 (FS2).
| Feature | FS1 | FS2 |
| Gene involved | MYCN (loss-of-function: missense, nonsense, frameshift mutations, deletions) | MIR17HG (deletions or variants affecting the miRNA cluster) |
| Digital anomalies | Brachymesophalangy: 94–100%; Toe syndactyly: 43–97%; Thumb hypoplasia: 14–17% (Marcelis 2008; Burnside 2018; Piersall 2000) | Brachymesophalangy: 100% (Grote 2015; Muriello 2019) |
| Microcephaly | 70–89% (Burnside 2018; Grote 2015; Marcelis 2008) | 88–89% (Grote 2015; Muriello 2019) |
| Gastrointestinal atresia (GA) | 24–55%; EA/TEF up to 35%; DA up to 27% (Marcelis 2008; Piersall 2000; Grote 2015) | Absent (Grote 2015; Muriello 2019) |
| Neurocognitive | Developmental delay/Intellectual disability: 45–71%; severe ID possible; white matter T2 hyperintensities reported (Burnside 2018; Marcelis 2008; Tedesco 2021) | ID/Learning disability: 100% (Muriello 2019) |
| Short stature | 56–60% (Burnside 2018; Marcelis 2008) | 86% (Muriello 2019) |
| Cardiac anomalies | 15–30% (Burnside 2018; Marcelis 2008) | 40% (Grote 2015; Low 2015; Muriello 2019) |
| Renal anomalies | 18–29% (Burnside 2018; Marcelis 2008) | Not commonly reported |
| Hearing loss | 7–43% (Burnside 2018; Marcelis 2008; Dodds 1999) | 66% (Muriello 2019) |
| Other features | Vertebral anomalies, laryngeal cleft, congenital absence of flexor pollicis longus tendon (Peleg 2021) | Keratoconus, cognitive issues (memory impairment, insomnia) (Sirchia 2017; Fiori 2015) |
Table 2.
Reported MYCN Pathogenic Variants and Associated Phenotypes.
| Feingold Syndrome Type 1 | |||||
| ToV | Localization | Mechanism | Reported variants | References | |
| Deletion | 2p24.1- 2p24.3 |
HI | del2p24.2-p25.1 microdeletion in 2p23-p24 1.2Mb microdeletion DelFAM84A_MYCN; DelMYCNOS_MYCN exon2; DelFAM84A_MYCN; DelMYCNOS_MYCN 425 Kb del 2p24.3 2p 3.4-16.8 deletions 4.4 Mb microdeletion in 2p24.3-p24.2 del2p24.3; del2p24.3-p24.2 |
Saal et al., 1996 Celli et al., 2000 van Bokhoven et al., 2005 Marcelis et al., 2008 Cognet et al., 2011 Chen et al., 2012 Burnside et al., 2018 Tedesco et al., 2021 |
|
| Nonsense / Frameshift | Exons 2/3 | LoF | c.626dupC (p.A319Gfs) | Blaumeiser et al., 2008 | |
| c.134dupC (p.E47fs); c.217G>T (p.E73*); c.231G>A (p.W77*); c.302delG (p.G101fs); c.451G>T (p.G151*); c.662C>A (p.S221X); c.683delC (p.P228fs); c.836_837dup (p.V280fs); c.881_882dup (p.T295fs); c.915_916insT (p.A306fs); c.964C>T (p.R322*); c.1005delC (p.S336fs); c.1097dupA (p.A367fs); c.1105_1106dup (p.S369fs); c.1117C>T (p.R373*); c.1207delA (p.T403fs); c.1274dupA (p.A426fs); c.1293delC (p.S432fs); c.1338delA (p.K446fs) | Marcelis et al., 2008 |
||||
| c.1110insG (p.S371Efs); c.928-930insGT (p.P310Rfs); c.474-514del (p.G161Pfs) | Cognet et al., 2011 | ||||
| c.503_543del (p.A171Rfs); c.1117C>T (p.Arg373*); c.1168 G>T (p.E390*) | Tedesco et al., 2021 | ||||
| c.266dupG (p.S90Qfs) | Klaniewska et al., 2023 | ||||
| Missense | Exon 3 | LoF | c.1145G>A (p.R382H) c.1177C>A (p.R393S); c.1178G>A (p.R393H); c.1181G>A (p.R394H); c.1226C>T (p.P409L) c.1177C>T (p.R393C) c.1171C>T (p.R391C) |
Blaumeiser et al., 2008 Marcelis et al., 2008 Cognet et al., 2011 Peleg et al., 2021 |
|
| Missense | Exon 2 | Likely LoF | c.454G>A (p.Ala152Thr) | This study | |
| Megalencephaly-Polydactyly Syndrome | |||||
| ToV | Localization | Mechanism | Reported variants | References | |
| Missense | Exon 2 | GoF | c.173C>T (p.T58M) c.179C>T (p.P60L) |
Kato et al., 2019 Kato et al., 2023 |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



