Submitted:
29 March 2026
Posted:
31 March 2026
You are already at the latest version
Abstract
Tuberculosis (TB) remains a leading cause of infectious mortality worldwide, reflecting persistent gaps in diagnosis, risk stratification, and treatment monitoring. Host RNA transcriptomic signatures have emerged as promising tools for capturing dynamic im-mune responses across the TB disease spectrum. Among these, the six-gene RISK6 signa-ture has attracted attention due to its parsimonious design and potential for clinical translation. This review provides a clinically oriented synthesis of current evidence on host transcriptomic biomarkers, with a particular focus on the application of RISK6 in di-agnosis, prediction of disease progression, and treatment monitoring. Available data suggest that RISK6 demonstrates robust diagnostic performance and reliable short-term prognostic value, while also reflecting dynamic changes during therapy. However, varia-bility across populations and the limited evidence in multidrug-resistant TB remain im-portant constraints. In practice, RISK6 is unlikely to function optimally as a standalone biomarker. Its clinical value appears greater when interpreted within integrated frame-works that combine transcriptomic, microbiological, and clinical data. Further validation in diverse populations and real-world settings will be essential to support meaningful clinical implementation.
Keywords:
tuberculosis
; RISK6
; transcriptomic signature
; biomarkers
; treatment monitoring
; disease progression
; multidrug-resistant tuberculosis
1. Introduction
Tuberculosis is one of the leading causes of death by a single infectious agent worldwide, resulting in approximately 10 million new cases and 1.3 million deaths per year. [1] Although advanced diagnostic technologies exist, current strategies rely on sputum-based testing methods such as microscopy and molecular assays. [2,3] These tools have significant limitations, mainly in patients with paucibacillary disease, extrapulmonary TB or if one is unable to produce sputum, and they provide little information regarding disease activity or response to treatment.
Moreover, immunological studies including interferon-γ release assays (IGRAs) cannot separate latent TB infection (LTBI) from active TB disease, and possess little predictive value for progression. [2,3] For that reason, there are also still key gaps in both early diagnosis and risk stratification and longitudinal monitoring — necessary tools for TB control in these very challenging settings.
To overcome these challenges, there is growing interest in host-derived biomarkers that describe the interaction between Mycobacterium TB and the host immune system. Whole-blood gene expression profiling has yielded host RNA transcriptomic signatures, which have shown great potential to capture dynamic immune responses across the disease spectrum of TB. [4,5] Such signatures offer a systems-level view of disease behavior and offer potential utility for identifying active TB, predicting progression from latent infection and monitoring treatment response. [6,7,8]
Parsimonious gene signatures, among the number of transcriptomic models, have attracted particular attention owing to their clinical translation potential. The RISK6 signature, a six-gene ratio-based transcriptomic model, is one of the most thoroughly validated host biomarkers in TB. In contrast to previous multi-gene signatures, RISK6 adopts a pair-ratio strategy that increases analytical robustness and lowers technical variability and supports deployment using quantitative PCR-based platforms. [9]
Accumulating evidence shows that RISK6 can effectively differentiate between active TB and latent infection and healthy controls, as well as determine short-term progression to disease. [10,11,12] In addition, RISK6 scores are also shown to decrease during effective anti-tuberculosis therapy which reflects dynamic alterations of disease activity thus justifying RISK6 as a treatment monitoring biomarker. [9,13] These phenotypes, together with the robust response profiles, provide an attractive basis for using RISK6 as a multi-functional biomarker for the continuum of TB care.
But even with such promising data, several key points remain. Gene function of transcriptomic signatures differ by population and geographical location and prediction is degraded with time, and its accuracy drops over long time horizons. [11,12,14] Also, there is little evidence on drug-resistant TB populations which is a clear gap considering growing global prevalence of MDR-TB and need of better techniques for treatment and monitoring.
In context of this literature, a systematic and translational synthesis of the available evidence is necessary to progress beyond a descriptive summary to a clinic-specific structure. This review presents an integrated evaluation of host RNA transcriptomic biomarkers in the context of TB, particularly the RISK6 signature as a novel translational platform for host RNA transcriptomes. We look at its biological basis, its clinical applications through diagnosis, prognosis, and treatment monitoring, and its place in drug-resistant TB, and highlight major challenges and future lines of clinical action.
Importantly, although multiple transcriptomic signatures have been proposed, their clinical translation has been inconsistent across settings. This highlights the need for approaches that balance biological performance with scalability and clinical feasibility.
2. Materials and Methods
2.1. Study Design
The present work was a concentrated narrative review in which the current study aimed at finding clear patterns in the current evidence base for RISK6 gene signature in TB. The review aimed to evaluate biological roots, application, treatment monitoring abilities of RISK6 and translational potential across diagnosis, prognosis and monitoring progress in terms of treatment.
2.2. Literature Search Strategy
A systematic literature search was conducted to find studies evaluating host RNA transcriptomic biomarkers in TB including the RISK6 signature. Electronic databases (PubMed, Scopus, and Web of Science) for articles published until December 2025 were used and no limits were placed on study design.
The search strategy merged the keywords and Medical Subject Headings (MeSH) terms such as: “tuberculosis,” “RISK6,” “transcriptomic signature,” “RNA biomarker,” “gene expression,” “treatment monitoring,” and “disease progression.” References to relevant studies were then screened to identify other studies.
2.3. Study Selection
Title and abstract screening was conducted by screening the included studies. Articles were found if they met the following criteria:
- Aims to assess the RISK6 transcriptomic signature in TB.
-
Reports of clinical applications such as:
- diagnosis
- prediction of disease progression
- treatment monitoring
- Conducted in human populations.
Studies excluded were analyzed if they:
- did not evaluate RISK6 in particular
- were non-original reports lacking relevant data (e.g., editorials without any analysis)
- were not available in English.
2.4. Data Extraction and Synthesis
Appropriate data were extracted from the included studies such as:
- the study design and participants
- clinical utility (diagnostic, prognostic or monitoring)
- key findings
- performance metrics (e.g., AUC, sensitivity, specificity)
- reported limitations
Data were obtained qualitatively for a comprehensive account of biological, clinical, and limitations of RISK6. In addition results were cross-compared across studies whenever possible to identify recurring patterns and sources of heterogeneity.
2.5. Analytical Framework
The findings were grouped into three broad domains in order to improve the clinical context:
- Diagnostic application
- Prognostic application (progression of disease)
- Treatment monitoring
Furthermore, a translational dimension was examined to consider potential incorporation into clinical practice of RISK6 including its use in TB resistance to drug therapy, alongside its amalgamation with microbiological and clinical aspects.
The selection of studies included in this focused analysis is illustrated in Figure 1.
Although this review follows a structured approach, it does not represent a formal systematic review. The findings should therefore be interpreted within the context of a narrative synthesis of the available evidence.
3. Results
3.1. Biological Basis of RISK6
The RISK6 transcriptomic signature is based on host immunologic responses to Mycobacterium TB and on interferon-based pathways associated with the pathogenesis of TB. [4,5] Type I and type II interferon signalling are closely related to active disease and are marked by the upregulation of genes that play roles in the innate immune activation response, antimicrobial response, and inflammation. [4] Such transcriptomic alterations mirror a systemic immune response that transcends just a localized pulmonary reaction.
RISK6 comprises six genes arranged in paired ratios, including three upregulated genes (GBP2, FCGR1B, and SERPING1) and three downregulated genes (TUBGCP6, TRMT2A, and SDR39U1). [9] The upregulation of these genes is mainly associated with interferon-inducible pathways and immune activation and of their downregulated expression it reflects cellular homeostasis and metabolic regulatory aspects. This bidirectional pattern of up and down gene expression increases the discriminatory potential in the signature and offers a biologically meaningful description of disease activity.
Crucially, the alteration in gene expression appears before clinically detectable TB, which is consistent with evidence supporting incipient or subclinical disease. [6,7,15,16] These early features involve a potentiation of interferonal signalling and immune activation that worsens with disease progression from latent infection to disease. Such a time-dependent effect contributes to the ability of transcriptomic biomarkers as RISK6 for short-term disease prediction.
For a strong methodological choice among RISK6 methodologies, the ratio-based process is preferred to standard expression pattern and limits technical heterogeneity between tools and sample situations. [9] Where previous transcriptomic signatures have relied on absolute expression of genes, this method improves analytical robustness and clinical translation in specific PCR-based methodologies. [17,18]
The biological implications of RISK6 for TB disease go beyond mechanistic analysis, and it accounts for the entire host immune response, over the spectrum of disease states, from an interpretive perspective. Higher RISK6 scores demonstrate enhanced immune activation during latency between infection and incipient and active TB infection, whereas low scores during effective therapy show the complete remission of inflammatory response. [9] This dynamic character-signal behavior favors its functional use as a biomarker of disease activity instead of a static diagnostic metric.
In general, the biological base of RISK6 is based on well-characterized immunopathological mechanisms of TB, and thus makes it a dynamic indicator of host response during various stages of infection. This mechanistic basis forms an important basis for the association of molecular signature with clinical utility, in which RISK6 can serve as a translational biomarker for tuberculosis.
The biological basis of RISK6 and its relationship to disease progression across the TB spectrum are illustrated in Figure 2.
While the biological basis of RISK6 provides important mechanistic insights into host immune responses in tuberculosis, its clinical value is best demonstrated through evidence from studies evaluating its performance across different applications. The key characteristics and findings of studies evaluating the RISK6 transcriptomic signature across different clinical applications are summarized in Table 1. Collectively, these studies demonstrate the multi-dimensional clinical utility of RISK6 in TB, particularly in diagnosis, short-term risk prediction, and treatment monitoring across diverse populations and settings.
4. Discussion
4.1. Clinical Applications of RISK6
The RISK6 transcriptomic signature demonstrates clinically relevant applications across multiple domains of TB management, including diagnosis, prediction of disease progression, and treatment monitoring. Its capacity to track dynamic host immune response renders it fundamentally different from traditional microbiological and immunologic methods providing a more holistic approach to evaluate disease response.
4.1.1. Diagnostic Application
RISK6 has consistently shown strong diagnostic performance distinguishing active TB from LTBI and healthy individuals. Multicohort validation studies demonstrate AUC values of up to 0.94 with good sensitivity and specificity. [10,19] These findings are consistent with its potential use as a non-sputum-based triage, especially in patients with paucibacillary disease or those with no sputum production.
Unlike pathogen-driven diagnostics, host transcriptomic biomarkers demonstrate a host’s overall immune response, and provide complementary data to microbiological testing. [2,3] Nevertheless, such limited specificity in the setting of other inflammatory or infectious diseases is an apparent limitation and there is requirement to integrate it with clinical and microbial information.
4.1.2. Prognostic Application (Prediction of Disease Progression)
Among the most important clinical uses of RISK6 is identifying progression of disease progression from latent infection to active TB. Prospective cohort studies indicate that RISK6 works best in the short-term, usually to the 6–9 months before disease development. [8,11] This corresponds with the idea of incipient TB, in which early immune activation leads to clinical presentation.
A limitation of long-term risk stratification tools is that its prediction is limited by larger follow-up periods. [11,17,18] Thus, to the best of our knowledge, these results demonstrate that RISK6 is most relevant for detecting people at imminent increased risk for disease progression, and further preventive and screening strategy development is warranted.
4.1.3. Treatment Monitoring
RISK6 is also showing good promise as a biomarker for treatment response monitoring. As several studies have demonstrated RISK6 scores drop dramatically with treatment with effective anti-TB and are associated with decreased disease activity. [9,15,19,21] This adaptive behavior points to RISK6 as being one of early predictors of treatment response, possibly preceding customary microbiological markers including sputum culture conversion.
This is especially relevant for patients with smear-negative or extrapulmonary TB, where microbiological surveillance is less common. Furthermore, to assess early treatment response can help medical professionals make better clinical decisions. Whether patients are at risk of poor outcomes or failure of treatment might be seen that way.
4.1.4. Integration into Clinical Practice
With these findings under scrutiny, it seems there is great potential to integrate RISK6 as an additional biomarker in clinical workflows alongside microbiological diagnostics. This approach may integrate host-derived markers with pathogen-complementary measurements to offer a more nuanced understanding of disease status that can include immune response in addition to bacillary burden.
For instance, the incorporation of RISK6 with microbiological measures of time to positivity (TTP) or culture conversion might improve monitoring of treatments and clinical decision. [21] In addition, RISK6 may facilitate risk stratification and, consequently, personalized TB management in line with emerging precision medicine paradigms.
4.1.5. Relevance to Drug-Resistant TB
Although promising and in need of evaluation, there is little evidence supporting the utilization of RISK6 in drug-resistant TB. Much of the literature on MDR-TB represents information only available in drug-sensitive TB populations. [14] Consequently addressing this gap, better tools to inform treatment and monitoring are crucial in this high-risk population.
RISK6 might be particularly advantageous from a translational perspective in MDR-TB. Being capable of mirroring dynamic response of the host, it has demonstrated potential benefits for early treatment response evaluation and identification of patients potentially at the risk of treatment failure. But before a translation into clinical use, strong validation in MDR-TB cohorts is needed.
This integrated approach aligns with the shift toward precision TB medicine, where biomarker-guided strategies may enable earlier diagnosis, improved risk stratification, and more responsive treatment monitoring. The clinical applications of RISK6 across diagnosis, prognosis, and treatment monitoring, along with their strengths, limitations, and translational implications, are summarized in Table 2.
This new evidence shows that the integrated use of transcriptomic signatures could improve predictive performance, and hence, RISK6 would be more efficacious as a constituent part of integrated biomarker strategies than as a stand-alone tool. [20]
4.1.6. Translational Perspective
Collectively, the clinical applications of RISK6 indicate that it serves as a multi-functional biomarker that has promise as a multi-functional marker which can be used as a multi-drug marker across the TB disease spectrum. When used individually, rather than as a test in isolation, RISK6 is positioned as an integrated platform of a transcriptomic, microbiological and clinical diagnostic test, making them all more efficient than its standalone diagnostic tool.
4.2. Limitations and Challenges
Nevertheless, prior to the dissemination of the RISK6 transcriptomic signature to the clinic, a number of major limitations regarding the RISK6 could be observed. These hurdles cover biological specificity, predicting ability, population variation, as well as translational potential, and represent the complexity of host-derived markers in TB.
4.2.1. Variability Across Populations
One main weakness of the RISK6 approach are the variation in performance between geographic area and epidemiological groups. Multicohort studies have shown that transcriptomic signatures such as RISK6 do not consistently demonstrate WHO target product profile performance consistency between patients, and in many populations, the WHO target product profile for WHO products such as RISK6 does not hold water with multicentre random sampling studies. [12,20] Differences in host genetics, environmental exposures, TB endemicity and, in particular, co-infections affecting immune responses and gene expression profiles, that particularly HIV infection, might profoundly influence the effect on the overall performance diagnostic and prognostic assessment, have been shown. [5,22] The evidence suggests there might be limitations of the models for clinical application that need context-specific validation and recalibration.
4.2.2. Limited Long-Term Predictive Performance
While RISK6 shows good accuracy in predicting the rate of short-term progression to active TB, it is poorer for longer periods of time. The transcriptomic signatures have been reported to have a peak performance in 6–12 month prior to disease onset and less sensitivity beyond that window. [8,11] This restriction suggests RISK6 works best for an incipient or subclinical disease, rather than for an early risk of disease in a longer-range context and thus can have limited utility as an independent screening tool for continuous risk stratification.
4.2.3. Limited Specificity of Interferon-Driven Signatures
RISK6 is mainly driven by interferon-inducible gene expression that is not TB specific and may be upregulated in other infectious or inflammatory diseases. [4,5] Viral infections and autoimmune diseases, for instance, can contribute to the same transcriptional profiles resulting in false-positive outcomes. The inherent lack of specificity is a core issue for host-based biomarkers and reveals the necessity to integrate transcriptomic signatures with clinical and microbiological data to enhance diagnostic accuracy.
4.2.4. Lack of Standardized Thresholds
The absence of defined thresholds for interpreting RISK6 scores also presents a major roadblock for clinical application. While multiple studies show strong discriminatory performance, no cut-off for clinical decision-making yet exists. [12,23] This absence of standardization also hampers cross-study comparisons and restricts incorporation into established diagnostic protocols.
4.2.5. Limited Evidence in Drug-Resistant TB
The evidence for the use of RISK6 in drug-resistant TB is still scarce. Most studies to date have concentrated on drug-sensitive TB populations, limited by the scarcity of data in MDR-TB cohorts. [14] In view of the unique clinical obstacles posed by MDR-TB (longer treatment duration, enhanced rates of treatment failure), this is a relevant knowledge deficit. More studies may be required to explore the efficacy of RISK6 for therapy-related performance of culture conversion and treatment response in drug-resistant disease.
4.2.6. Need for Multi-Biomarker Approaches
Emerging evidence indicates that a single transcriptomic signature cannot adequately reflect the complexity of TB pathogenesis. There is evidence to support the combining of more than one biomarker, including combining transcriptomic metrics with some clinical and microbiological characterization to enhance performance and specificity of disease prediction. [20,24,25] This suggests that RISK6 may represent only one aspect of a potentially composite biomarker strategy, rather than a stand-alone tool.
4.2.7. Implementation Challenges
Problems in practice to carry out interventions remain especially acute in resource-limited settings. These challenges include the costs of molecular testing, the requirement for laboratory infrastructure, and difficulties in incorporating transcriptomic assays into all TB diagnostic workflows. [2,3] Furthermore, the scaling of RNA-based diagnostics and the establishment of point-of-care platforms continue to pose major translational challenges.
4.2.8. Translational Perspective on Limitations
This combination of a few limitations suggests that although RISK6 is an attractive biomarker, the specific use of RISK6 would be its optimal use within an integrated, context-sensitive framework, not as a stand-alone diagnostic system. Fulfilling these challenges will demand a comprehensive effort in standardization, validation in a wide range of population and in terms of accessible diagnostic platforms for their uptake in the real world.
These considerations suggest that transcriptomic biomarkers, including RISK6, are best interpreted as context-dependent tools rather than universally applicable solutions.
4.3. Comparison with Other Transcriptomic Signatures
Developments of host blood transcriptomic biomarkers for TB have uncovered a range of gene expression signatures that have implications, both diagnostically and for prognosis. This context requires that the RISK6 signature is conceptualized in relation to previous and modern transcriptomic models in order to establish relative strengths, limitations, and clinical placement.
4.3.1. Comparison with Early Multi-Gene Signatures
Early transcriptomic signatures (e.g., with the ACS 16-gene and ACS 11-gene models) further established support for the proposition that blood RNA profiles could predict active TB progression prior to clinical disease. [6,17,18] These signatures are well predictive but complex, which precludes them to be routinely used clinically.
In contrast, RISK6 was constructed as a parsimonious 6-gene signature with the paired-ratio approach to enhance analytical stability and minimize vulnerability to technical variation. [9] This decrease in gene count represents a significant advantage in terms of scalability and potential incorporation into PCR-based diagnostic systems.
4.3.2. Comparison in Prognostic Performance
In other words, on the prognostic performance, RISK6 shows a similar distribution to other transcriptomic signatures, demonstrating high predictive accuracy in the short-term window before disease onset. [8,11] However, results similar to previous models indicate performance drops during longer follow-up periods, corresponding to the common shortcoming of host-response biomarkers. [17,18]
No one transcriptomic signature proves to out-perform all other such signatures, and performance is affected by cohort level factors, including geographic variation and host characteristics, as shown by comparative analyses. [12]
4.3.3. Comparison in Diagnostic Application
Some transcriptomic signatures are considered as non-sputum based triage tools that were used in TB prediction. Multiple models showed similar diagnostic precision, although population specific differences was a persistent problem. [12,23]
A major difference is the multi-activity nature of RISK6, which has evaluated diagnosis, prognosis, and treatment monitoring, while several previous signatures had mainly been tailored to be used for predictive purpose and risk prediction. Such application to a wider range of applications increases its possible clinical relevance in multimodal diagnostic paradigms.
4.3.4. Comparison in Treatment Monitoring
One critical element of RISK6 is its potential for use in treatment supervision, a field with limited treatment consideration for many other transcriptomics signatures. Risk-specific proteins like RISK6, on the other hand, are well-established in some studies because the score decreases with effective therapy and is associated with disease activity, thus supporting their use as a dynamic biomarker. [9,13]
In contrast, several of the earlier signatures were largely developed for prognostic reasons and have not been systematically validated in longitudinal treatment applications. This distinction emphasizes a possible role for RISK6 as a new type of biomarker in monitoring treatment response, particularly in areas where microbial markers are scarce.
4.3.5. Emerging Role of Composite Signatures
Recent research suggests combining multiple transcriptomic signatures or integrating them well with clinical and microbiological variables may offer much more precision and enhanced accuracy. [20,24,25] These integrated approaches seek to rectify the problems of single biomarkers by embracing parallel aspects of disease biology.
In this context, RISK6 would be placed best not as a sole solution but as part of multi-biomarker strategies. It is simple and robust enough to supplement more complex models.
4.3.6. Overall Positioning of RISK6
In general, RISK6 is in an intermediate category between several TB transcriptomic biomarkers. To overcome constraints such as simplicity, scalability, and multi-domain clinical applicability, the proposed approach is the best balanced approach. Nevertheless, we shouldn't imagine that it consistently outperforms all other signatures in every scenario at this time. The best role of RISK6 is probably most suitable within integrated and context-specific architectures.
A comparative overview of RISK6 and other transcriptomic signatures, including their performance characteristics, strengths, limitations, and clinical positioning, is presented in Table 3.
Notably, the advantage of RISK6 lies less in consistently outperforming other signatures and more in achieving a pragmatic balance between performance, simplicity, and translational feasibility.
4.4. Future Perspectives and Relevance to Drug-Resistant TB
In contrast, the mounting evidence base of host transcriptomic biomarkers suggests the utility of RISK6 in advanced therapeutic and precision-oriented TB management. Implementing this potential in clinical settings, though, necessarily involves further testing, incorporation, and adoption for real-world applications.
4.4.1. Toward Precision TB Medicine
Among those emerging applications, the use of RISK6 is promising for the future in the optimization of precision TB treatment. By monitoring the dynamic immune responses of living hosts, RISK6 may support increased risk stratification, early detection of disease progression and real-time tracking of treatment response. This approach is complemented by new methods to customize the clinical decision making to the individual biological profiles, which should be a primary factor compared to treatment algorithm uniformity. [24,26]
4.4.2. Expanding the Role in MDR-TB
One of the main limitations in research at this phase is the relatively unexplored assessment of RISK6 in drug-resistant TB. Multidrug-resistant TB is a significant challenge worldwide, where treatment duration is longer in some cases, patient toxicity is greater and treatment failure rates higher. [14,27]
RISK6 might then have several merits given this context. Its capability to mirror dynamic host immune responses would be an early marker of treatment response and could allow for actionable information before conventional microbiological markers such as culture conversion. Moreover, sustained elevation of RISK6 during therapy might assist with the identification of treatment-risk-prone patients, paving the way for earlier therapeutic titration.
Robust evidence of these applications in MDR-TB populations is currently lacking. Future studies could provide further longitudinal testing of RISK6, compared to clinically meaningful parameters of time-to-positivity, culture conversion, and treatment response.
4.4.3. Integration with Microbiological Markers
Integrating RISK6 with established microbiological and clinical indicators holds great promise in future studies. Microbiological markers describe bacillary burden, but the transcriptomic signatures of hosts capture systemic immune responses and are used to supplement these data. [13]
The integration of host- and pathogen-derived markers could enhance diagnostication, and support treatment control and allow for a more complete characterization and status of disease. These can be very promising integrated strategies particularly in scenarios that are hard to study such as extrapulmonary TB and drug-resistant TB.
4.4.4. Toward Multi-Biomarker Models
There is currently some evidence (the inclusion of transcriptomic signatures with other biomarkers and clinical data has potential to improve the predictive performance) that merging these methods will be beneficial. [24,25] Machine learning and data integration innovation can allow to create composite models to represent most aspects of the disease biology.
RISK6 could be a practical and scalable aspect of multi-biomarker strategies which may offer a solution with the middle ground of simplicity and clinical application within this paradigm. And these measures could benefit accurate risk categorization and personalized therapy in TB.
4.4.5. Translation into Clinical Practice
The translation of RISK6 to feasible diagnostic platforms is required for its clinical impact. Simpler PCR assays and point-of-care technology development that can be easily implemented, even in high-burden and resource-poor countries, may be an important facilitator. [2,3]
Several challenges remain, however, including standardizing thresholds, allowing for validation across many populations, and integration into existing diagnostic algorithms. Addressing these obstacles is critical to connecting the two worlds of biomarker discovery and clinical application.
4.4.6. Future Directions
The future of RISK6 primarily stems from its incorporation within a multi-dimensional approach to TB management. Not as a standalone biomarker, but when it comes to microbiological, clinical and computational analysis, RISK6 is expected to be most effective.
Significantly, the comparatively small evidence base on its involvement in drug-resistant TB is an important area for research that needs to be explored further. Closing this gap may present new opportunities for better management of monitoring and treatment outcomes in this high-risk cohort.
In addition, implementation studies in real-world clinical settings will be critical to determine whether transcriptomic biomarkers can meaningfully influence clinical decision-making and patient outcomes.
5. Conclusions
Host transcriptomic biomarkers represent a meaningful shift toward host-directed approaches in tuberculosis, offering insights that extend beyond pathogen detection alone. Within this evolving landscape, RISK6 provides a practical balance between biological relevance, scalability, and multi-domain clinical applicability.
Current evidence supports its role in short-term risk prediction and treatment monitoring. However, variability across populations and limited validation in drug-resistant TB remain important constraints. These limitations suggest that the clinical value of RISK6 lies less in its use as an isolated test and more in its integration with existing diagnostic and monitoring strategies.
The clinical impact of RISK6 will ultimately depend on its incorporation into composite biomarker models and its validation in diverse, real-world settings. Addressing these gaps is essential to translate transcriptomic advances into clinically actionable tools, particularly in high-burden and drug-resistant TB contexts.
6. Patents
Not applicable.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, C.M., A.S., L.C., P., P.S. and P.A.; methodology, C.M.; validation, C.M., A.S., and L.C.; formal analysis, C.M.; investigation, C.M.; resources, A.S.; data curation, C.M.; writing—original draft preparation, C.M.; writing—review and editing, C.M., A.S., and L.C.; visualization, C.M.; supervision, A.S.; project administration, C.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
The authors acknowledge institutional academic support in the preparation of this manuscript. During the preparation of this manuscript, the authors used AI-assisted tools for language refinement. The authors reviewed and edited the content and take full responsibility for the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| TB | Tuberculosis |
| MDR-TB | Multidrug-Resistant Tuberculosis |
| LTBI | Latent Tuberculosis Infection |
| RISK6 | Six-gene transcriptomic signature for tuberculosis risk, diagnosis, and treatment monitoring |
| RNA | Ribonucleic Acid |
| PCR | Polymerase Chain Reaction |
| IFN | Interferon |
| IGRA | Interferon-Gamma Release Assay |
| AUC | Area Under the Curve |
| TTP | Time to Positivity |
| WHO | World Health Organization |
| TPP | Target Product Profile |
References
- World Health Organization, Global Tuberculosis Report 2025, no. September. Geneva, 2025. [Online]. Available: https://iris.who.int/server/api/core/bitstreams/e97dd6f4-b567-4396-8680-717bac6869a9/content.
- Pai, M.; Behr, M.A.; Dowdy, D.; Dheda, K.; Divangahi, M.; Boehme, C.C., “Tuberculosis,” Nat Rev Dis Prim., vol. 2, p. 16076, 2016. [CrossRef]
- Lawn, S.D.; Zumla, A.I., “Tuberculosis,” Lancet, vol. 378, no. 9785, pp. 57–72, 2011. [CrossRef]
- Berry, M.P.R.; Graham, C.M.; McNab, F.W.; Xu, Z.; Bloch, S.A.A.; Oni, T., “An interferon-inducible neutrophil-driven blood transcriptional signature in human tuberculosis,” Nature, vol. 466, no. 7309, pp. 973–977, 2010. [CrossRef]
- O’Garra, A.; Redford, P.S.; McNab, F.W.; Bloom, C.I.; Wilkinson, R.J.; Berry, M.P.R., “The Immune Response in Tuberculosis,” Annu Rev Immunol, vol. 31, pp. 475–527, 2013. [CrossRef]
- Zak, D.E.; Penn-Nicholson, A.; Scriba, T.J.; Thompson, E.; Suliman, S.; Amon, L.M., “A prospective blood RNA signature for tuberculosis disease risk,” Lancet, vol. 387, no. 10035, pp. 2312–22, 2016. [CrossRef]
- Suliman et al, S., “Four-gene pan-African blood signature predicts progression to tuberculosis,” Am. J. Respir. Crit. Care Med., vol. 197, no. 9, pp. 1198–1208, 2018. [CrossRef]
- Gupta et al, R.K., “Concise whole blood transcriptional signatures for incipient tuberculosis: A systematic review and patient-level pooled meta-analysis,” Lancet Respir. Med., vol. 8, no. 4, pp. 395–406, 2020. [CrossRef]
- Penn-Nicholson et al, A., “RISK6, a 6-gene transcriptomic signature of TB disease risk, diagnosis and treatment response,” Sci. Rep., vol. 10, no. 1, pp. 1–21, 2020. [CrossRef]
- Bayaa et al, R., “Multi-country evaluation of RISK6, a 6-gene blood transcriptomic signature, for tuberculosis diagnosis and treatment monitoring,” Sci. Rep., vol. 11, no. 1, pp. 1–12, 2021. [CrossRef]
- Mendelsohn et al, S.C., “Transcriptomic Signatures of Progression to Tuberculosis Disease among Close Contacts in Brazil,” J. Infect. Dis., vol. 230, no. 6, pp. e1355–e1365, 2024. [CrossRef]
- Muwanga et al, V.M., “Blood transcriptomic signatures for symptomatic tuberculosis in an African multicohort study,” Eur. Respir. J., vol. 64, no. 2, 2024. [CrossRef]
- Neumann et al, M., “The molecular bacterial load assay predicts treatment responses in patients with pre-XDR/XDR-tuberculosis more accurately than GeneXpert Ultra MTB/Rif,” J. Infect., vol. 90, no. 2, p. 106399, 2025. [CrossRef]
- Lange, C.; Dheda, K.; Chesov, D.; Mandalakas, A.M.; Udwadia, Z.; Jr, C.R.H., “Management of drug-resistant tuberculosis,” vol. 394, no. 10202, pp. 953–966, 2019. [CrossRef]
- Cliff et al, J.M., “Distinct phases of blood gene expression pattern through tuberculosis treatment reflect modulation of the humoral immune response,” J. Infect. Dis., vol. 207, no. 1, pp. 18–29, 2013. [CrossRef]
- Esmail et al, H., “Complement pathway gene activation and rising circulating immune complexes characterize early disease in HIV-associated tuberculosis,” Proc. Natl. Acad. Sci. U. S. A., vol. 115, no. 5, pp. E964–E973, 2018. [CrossRef]
- Warsinske, H.; Vashisht, R.; Khatri, P., “Host-response-based gene signatures for tuberculosis diagnosis: A systematic comparison of 16 signatures,” PLoS Med., vol. 16, no. 4, pp. 1–19, 2019. [CrossRef]
- Turner et al, C.T., “Blood transcriptional biomarkers for active pulmonary tuberculosis in a high-burden setting: A prospective, observational, diagnostic accuracy study,” Lancet Respir. Med., vol. 8, no. 4, pp. 407–419, 2020. [CrossRef]
- Burel et al, J.G., “Distinct blood transcriptomic signature of treatment in latent tuberculosis infected individuals at risk of developing active disease,” Tuberculosis, vol. 131, pp. 1–24, 2021. [CrossRef]
- Lundell, S.; Kaipilyawar, V.; Johnson, W.E.; Dietze, R.; Jerrold, J., “Combining blood transcriptomic signatures improves the prediction of progression to tuberculosis among household contacts in Brazil .,” 2025.
- Pitaloka, D.A.E.; Syamsunarno, M.R.A.A.A.; Abdulah, R.; Chaidir, L., “Omics Biomarkers for Monitoring Tuberculosis Treatment: A Mini-Review of Recent Insights and Future Approaches,” Infect. Drug Resist., vol. 15, no. May, pp. 2703–2711, 2022. [CrossRef]
- World Health Organization, High-priority target product profiles for new tuberculosis diagnostics: Report of a consensus meeting, no. April. Geneva, 2014.
- World Health Organization, WHO Consolidated Guidelines on Tuberculosis Module 4: Treatment and care. Geneva, 2025.
- Roe et al, J.K., “Blood transcriptomic diagnosis of pulmonary and extrapulmonary tuberculosis,” JCI Insight, vol. 1, no. 16, pp. 1–14, 2016. [CrossRef]
- Sambarey et al, A., “Unbiased Identification of Blood-based Biomarkers for Pulmonary Tuberculosis by Modeling and Mining Molecular Interaction Networks,” EBioMedicine, vol. 15, pp. 112–126, 2017. [CrossRef]
- Maertzdorf et al, J., “Concise gene signature for point-of-care classification of tuberculosis,” EMBO Mol. Med., vol. 8, no. 2, pp. 86–95, 2016. [CrossRef]
- Diacon et al, A.H., “Multidrug-Resistant Tuberculosis and Culture Conversion with Bedaquiline,” N. Engl. J. Med., vol. 371, no. 8, pp. 723–732, 2014. [CrossRef]
Figure 1.
Study selection process for the focused analysis of RISK6 transcriptomic studies. Studies evaluating the RISK6 transcriptomic signature were identified from the broader literature on RNA biomarkers in tuberculosis and included based on predefined relevance to clinical applications.
Figure 1.
Study selection process for the focused analysis of RISK6 transcriptomic studies. Studies evaluating the RISK6 transcriptomic signature were identified from the broader literature on RNA biomarkers in tuberculosis and included based on predefined relevance to clinical applications.

Figure 2.
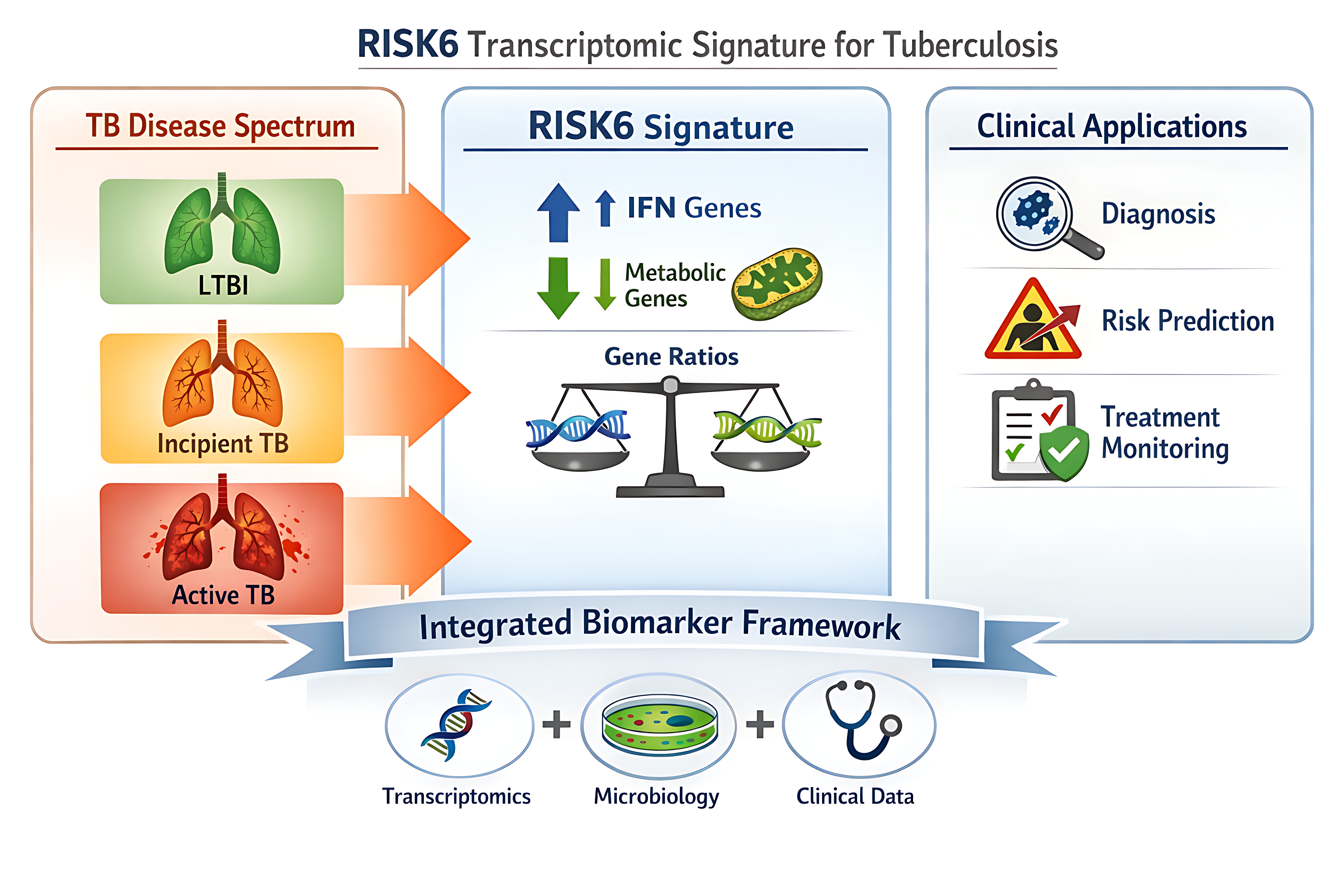
Biological basis and disease progression reflected by the RISK6 transcriptomic signature. The transition from LTBI to incipient and active TB is characterized by increased expression of interferon (IFN)-related genes and decreased expression of metabolic genes. These changes are associated with progressive disease activity and are reflected by an increasing RISK6 score, corresponding to a shift from low to high risk across the TB disease spectrum.
Figure 2.
Biological basis and disease progression reflected by the RISK6 transcriptomic signature. The transition from LTBI to incipient and active TB is characterized by increased expression of interferon (IFN)-related genes and decreased expression of metabolic genes. These changes are associated with progressive disease activity and are reflected by an increasing RISK6 score, corresponding to a shift from low to high risk across the TB disease spectrum.


Table 1.
Key studies evaluating the RISK6 transcriptomic signature in TB and their clinical implications.
Table 1.
Key studies evaluating the RISK6 transcriptomic signature in TB and their clinical implications.
| Study | Population / Setting | Design | Application | Key Findings | Performance | Limitations | Clinical Interpretation |
|---|---|---|---|---|---|---|---|
| Penn-Nicholson et al., 2020 [9] | Multicohort | Prospective / validation | Diagnosis, prognosis, monitoring | Correlates with disease activity; declines during treatment | AUC >0.85; dynamic change | Limited MDR-TB data; no standardized cut-off | Multi-purpose biomarker; promising for treatment monitoring |
| Bayaa et al., 2021 [10] | Multicountry | Validation | Diagnosis | Differentiates active TB vs LTBI/healthy | AUC ≈ 0.94; Se ~90.9%; Sp ~87.8% | Variability; overlap with inflammation | Potential triage tool (non-sputum-based) |
| Mendelsohn et al., 2024 [11] | Household contacts | Prospective cohort | Prognosis | Strong short-term prediction (≤6–9 months) | Meets WHO TPP short-term | Weak ≥12 months | Best for short-term risk stratification (incipient TB) |
| Muwanga et al., 2024 [12] | Multicountry | Cross-cohort | Diagnosis, prognosis | Performance varies by geography | AUC ~0.75–0.85 | Heterogeneity | Requires population-specific calibration |
| Burel et al., 2021 [19] | TB vs LTBI | Observational | Diagnosis | Distinguishes TB states (host response) | AUC ~0.85–0.90 | Not RISK6-specific | Supports biological validity of host signatures |
| Lundell et al., 2025 [20] | Integrated cohorts | Modeling | Prognosis (composite) | Combined signatures ↑ accuracy | Se ~90%; Sp ~88% | Complexity | RISK6 may be stronger in composite panels |
Collectively, the evidence highlights the multi-dimensional clinical utility of RISK6 across diagnosis, prognosis, and treatment monitoring. While strong diagnostic performance and short-term predictive accuracy are consistently observed, important limitations remain, including variability across populations, reduced long-term predictive performance, and limited validation in drug-resistant tuberculosis. These findings underscore the need for context-specific validation and support the integration of RISK6 within broader clinical and biomarker frameworks.
Table 2.
Clinical Applications of RISK6 in TB.
| Domain | Key Evidence | Strengths | Limitations | Clinical Role |
|---|---|---|---|---|
| Diagnosis | Bayaa et al. [10]; Muwanga et al. [12]; Burel et al. [19] | High diagnostic accuracy (AUC up to 0.94); non-sputum-based | Reduced specificity in inflammatory conditions; variability across populations | Potential triage tool, especially in paucibacillary TB |
| Prognosis (Disease Progression) | Penn-Nicholson et al. [9]; Mendelsohn et al. [11] | Strong short-term prediction (≤6–9 months); aligns with incipient TB concept | Declining performance over longer intervals | Useful for identifying high-risk individuals for targeted prevention |
| Treatment Monitoring | Penn-Nicholson et al. [9]; Muwanga et al. [12] | Dynamic decline during therapy; reflects disease activity | Lack of standardized thresholds; limited MDR-TB data | Potential early marker of treatment response and failure |
| Drug-Resistant TB (Emerging) | Limited evidence [14] | Theoretical relevance for response monitoring | Insufficient validation in MDR-TB populations | Promising but requires further validation |
| Integrated / Composite Biomarker Models | Lundell et al. [20] | Improved predictive accuracy when combined with other signatures | Increased complexity; reduced scalability | RISK6 may be most effective as part of multi-biomarker strategies |
Overall, these findings highlight the role of RISK6 as a multi-functional biomarker with greatest utility in short-term risk prediction and treatment monitoring, while emphasizing the need for integration with clinical and microbiological parameters.
Table 3.
Comparison of RISK6 with other blood transcriptomic signatures for TB.
| Signature | No. of Genes | Primary Application | Performance Characteristics | Strengths | Limitations | Clinical Positioning |
|---|---|---|---|---|---|---|
| RISK6 | 6 | Diagnosis, prognosis, monitoring | AUC up to 0.94; strong short-term prediction; dynamic treatment response | Parsimonious; ratio-based; multi-functional; PCR-compatible | Reduced long-term prediction; variability across populations; lack of standard cut-offs | Most clinically versatile; suitable for integrated diagnostic and monitoring strategies |
| ACS16 / RISK16 | 16 | Prognosis | Strong prediction of progression to active TB | Well-characterized IFN-driven signature | Large gene set; limited scalability | Useful for research and risk prediction; less practical for routine use |
| ACS11 / RISK11 | 11 | Prognosis | Moderate predictive performance | Reduced gene set vs ACS16 | Limited long-term performance; reduced specificity | Potential for targeted risk stratification with further validation |
| PREDICT29 | 29 | Prognosis | High performance in selected cohorts | Broad biological coverage | Complex; limited generalizability | Promising but not yet clinically scalable |
| Composite / Integrated Models | Variable | Prognosis, risk stratification | Improved sensitivity and specificity (~90%) | Highest predictive accuracy; adaptable | High complexity; cost; standardization challenges | Likely future direction; RISK6 may serve as a component of these models |
Overall, while more complex signatures may offer higher predictive accuracy, RISK6 provides a favorable balance between performance, scalability, and clinical applicability, supporting its role within integrated biomarker strategies.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



