Submitted:
29 March 2026
Posted:
30 March 2026
You are already at the latest version
Abstract
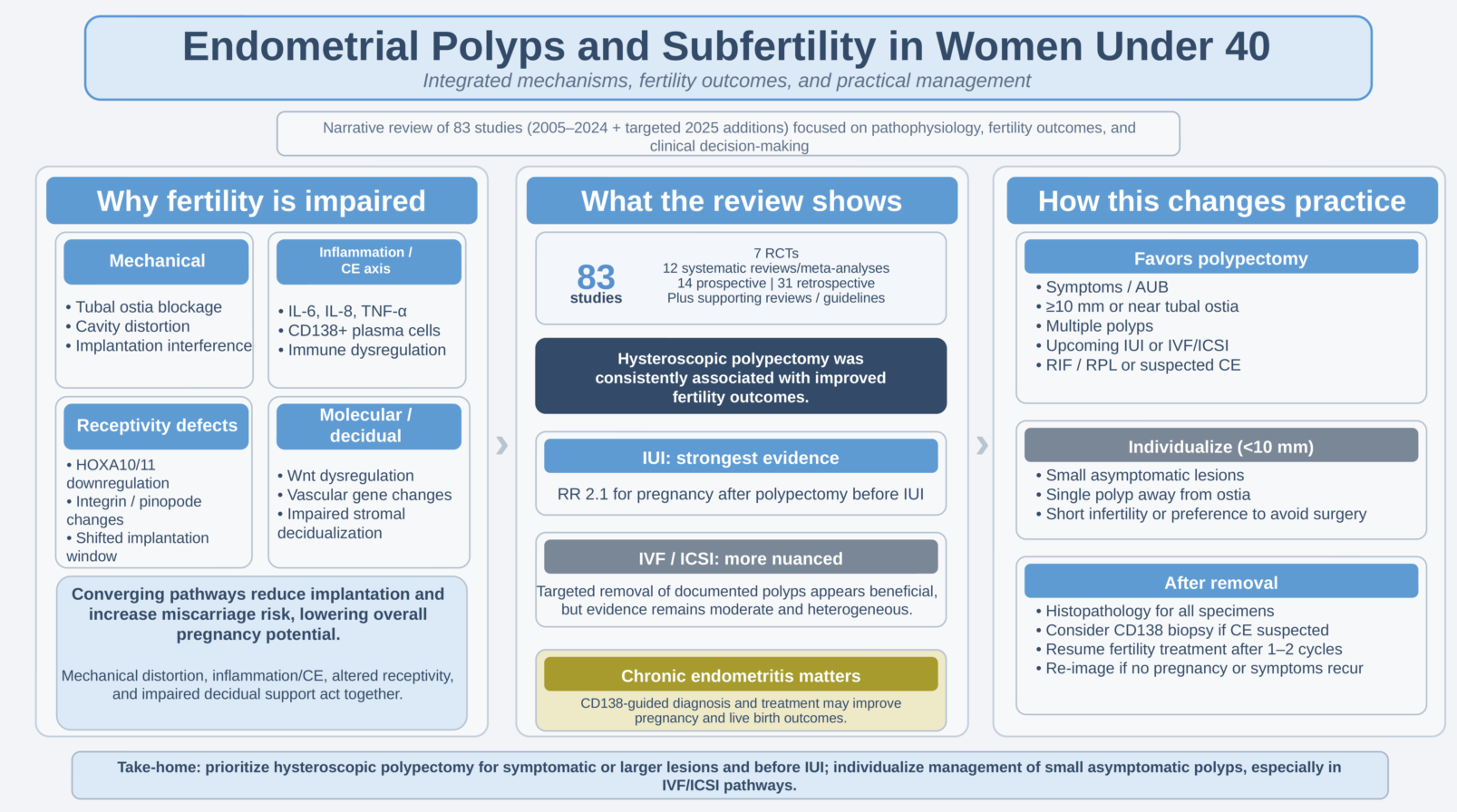
Background and Objectives: Endometrial polyps are common in women presenting with subfertility, yet uncertainty persists regarding which lesions warrant removal and how best to integrate hysteroscopic management with contemporary fertility treatment pathways. This narrative review synthesizes current evidence on pathophysiological mechanisms, diagnostic approaches, fertility outcomes, and practical clinical management for women under 40 years of age. Materials and Methods: PubMed/MEDLINE, Embase, Scopus, Web of Science, and the Cochrane Library were searched for English-language human studies published between January 2005 and December 2024. From 2352 records identified, 83 studies were included (8 randomized controlled trials, 12 systematic reviews/meta-analyses, 21 prospective cohort studies, 34 retrospective cohort studies, 5 case-control studies, and 3 clinical guidelines). Evidence was synthesized thematically using a narrative approach. Results: Across treatment modalities, hysteroscopic polypectomy was consistently associated with improved fertility outcomes. The landmark Pérez-Medina randomized trial reported a relative risk of 2.1 (95% CI 1.5–2.9) for pregnancy after polypectomy before intrauterine insemination. For IVF/ICSI, reported clinical pregnancy rates after polypectomy range from 53–72% and live birth rates from 43–66%. Proposed mechanisms include mechanical interference, chronic inflammation with cytokine dysregulation, altered endometrial receptivity (including HOXA10/HOXA11 dysregulation), and impaired decidualization. Conclusion: Current evidence supports hysteroscopic polypectomy as an effective intervention to improve fertility outcomes in subfertile women with endometrial polyps, particularly prior to intrauterine insemination and IVF/ICSI. Contemporary guidance (including the 2024 SOGC guideline) favors polypectomy regardless of polyp size. Future research should clarify molecular predictors of polyp-associated infertility, optimal timing relative to fertility treatment, and long-term reproductive outcomes.
Keywords:
endometrial polyps
; infertility
; subfertility
; hysteroscopy
; hysteroscopic polypectomy
; intrauterine insemination
; in vitro fertilization
; endometrial receptivity
; implantation
1. Introduction
Endometrial polyps are localized overgrowths of endometrial tissue that project into the uterine cavity, consisting of endometrial glands, stroma, and blood vessels covered by epithelium [1]. These benign lesions are among the most common intrauterine abnormalities encountered in clinical practice, with prevalence estimates ranging from 7.8% to 34.9%, depending on the population studied and diagnostic methods employed [2,3]. In the general population, endometrial polyps are identified in approximately 10–15% of women, while their prevalence increases substantially to 16–32% among women presenting with subfertility [4,5].
Historical understanding of endometrial polyps and their relationship to fertility has evolved considerably. Early case reports from the 1950s and 1960s suggested a possible association between intrauterine lesions and reproductive failure, but systematic evaluation became feasible only with modern hysteroscopy in the 1970s. The introduction of office hysteroscopy in the 1990s revolutionized polyp diagnosis, allowing direct visualization without general anesthesia [6]. The landmark randomized controlled trial by Pérez-Medina and colleagues in 2005 represented a watershed moment in the field, providing level I evidence that hysteroscopic polypectomy before intrauterine insemination significantly improves pregnancy rates [7]. This study fundamentally changed clinical practice and established polypectomy as a standard intervention in fertility centers worldwide.
The clinical significance of endometrial polyps in reproductive medicine extends beyond their direct impact on conception rates. Infertility affects a substantial proportion of couples globally, representing a significant public health burden with considerable economic and psychological consequences [4]. When endometrial polyps are identified in subfertile women, they present a potentially treatable cause of reproductive failure. The economic implications are considerable: assisted reproductive technology (ART) cycles cost $12,000–$15,000 per attempt in the United States, and improving baseline fertility potential through polyp removal may reduce the number of cycles needed to achieve pregnancy [8].
The relationship between endometrial polyps and subfertility has been a subject of considerable clinical interest. While the association between these lesions and impaired fertility is well-documented, establishing a direct causal relationship remains challenging due to the multifactorial nature of infertility and frequent coexistence of other reproductive pathologies [9]. Nevertheless, accumulating evidence suggests that endometrial polyps may interfere with fertility through multiple mechanisms, including mechanical obstruction of sperm transport, disruption of embryo implantation, and alteration of the endometrial microenvironment [7,10].
Despite substantial research progress, several important controversies persist. The management of small asymptomatic polyps (<10 mm) remains contentious. While some clinicians advocate for routine removal of all polyps in subfertile women, others suggest expectant management for small lesions, citing the potential for spontaneous regression [11,12]. The 2024 Society of Obstetricians and Gynaecologists of Canada (SOGC) guideline issued a strong recommendation for polypectomy regardless of polyp size; however, this recommendation has generated debate, given limited evidence specifically addressing small polyps [13]. The optimal timing of surgical intervention relative to fertility treatment also lacks consensus. Polyp recurrence is another clinical challenge, with reported rates ranging from 3.7% to 15% [14].
This narrative review synthesizes current evidence on endometrial polyps and subfertility in women under 40 years of age. We examine pathophysiological mechanisms, diagnostic approaches, treatment outcomes across different fertility modalities, and evidence-based recommendations for clinical management. Key studies are summarized in Table 1.
2. Materials and Methods
A comprehensive literature search was conducted to identify relevant publications on endometrial polyps and subfertility.
2.1. Search Strategy
Five electronic databases were systematically searched: PubMed/MEDLINE (n = 612), Embase (n = 534), Scopus (n = 489), Web of Science Core Collection (n = 427), and Cochrane Library (n = 212). Additional records were identified through reference list screening (n = 52) and citation searching (n = 26), yielding a total of 2352 records. The search covered publications from January 2005 to December 2024. Search terms included combinations of: endometrial polyp, uterine polyp, intrauterine polyp, subfertility, infertility, fertility, pregnancy, conception, IVF, ICSI, IUI, assisted reproduction, and hysteroscop*.
2.2. Inclusion and Exclusion Criteria
The initial search yielded 2,352 records. After removing duplicates, 1,517 unique records were screened based on title and abstract. Full-text articles were retrieved for 267 potentially eligible studies. Following a detailed review, 186 articles were excluded for the following reasons: not addressing fertility outcomes (n=67), postmenopausal populations (n=34), case reports with fewer than 10 patients (n=28), non-English language (n=23), conference abstracts (n=18), and other reasons (n=16). 81 studies met the inclusion criteria from the database search. Together with the two targeted 2025 additions (Pîrlog et al. 2025 and Wang et al. 2025), 83 studies were included in the final synthesis. The study selection process is illustrated in the PRISMA flow diagram (Supplementary Material S3).
2.3. Study Selection and Data Extraction
The final analysis included 83 studies: 7 randomized controlled trials, 12 systematic reviews and meta-analyses, 14 prospective cohort studies, 31 retrospective cohort studies, 5 case-control and other study designs, 11 narrative reviews and supporting evidence studies, and 3 clinical guidelines and targeted 2025 additions. Data were independently extracted by both authors using a standardized form, with discrepancies resolved by consensus. The complete included-study list with summary data is provided in Supplementary Table S1. Data were synthesized thematically using a narrative approach.
2.4. Quality Assessment
This narrative review followed the Scale for the Assessment of Narrative Review Articles (SANRA) guidelines [15]. Given the narrative synthesis approach and the inclusion of diverse study designs, formal risk-of-bias assessment using tools such as the Cochrane Risk of Bias tool or Newcastle-Ottawa Scale was not performed. However, study quality considerations (including sample size, prospective vs. retrospective design, presence of control groups, and adjustment for confounders) were incorporated into the interpretation of findings. The SANRA assessment checklist is provided in Supplementary Material S4.
3. Epidemiology and Risk Factors
The epidemiology of endometrial polyps varies significantly depending on the population studied and diagnostic methods employed. In the general female population, prevalence estimates range from 7.8% to 34.9%, with most studies reporting rates of 10–15% [2,15]. Among women presenting with subfertility, prevalence increases substantially to 16–32%, suggesting either a causal relationship or shared risk factors [4,5]. The prevalence increases with age, reaching approximately 8% by age 40 and continuing to rise through the perimenopausal period [15].
Several risk factors have been identified for the development of endometrial polyps. Obesity represents a significant risk factor, with body mass index (BMI) >30 kg/m² associated with increased polyp prevalence, likely mediated through elevated peripheral estrogen conversion in adipose tissue [15]. Hypertension has been consistently associated with polyp formation, though the mechanism remains unclear. Tamoxifen use in breast cancer patients dramatically increases polyp risk, with prevalence rates of 30–60% reported in this population [13]. Other identified risk factors include nulliparity, late menopause, and hormone replacement therapy use.
Geographic and ethnic variations in polyp prevalence have been observed, though these may partly reflect differences in screening practices and diagnostic thresholds. Studies from Europe report prevalence rates of 15–25% in subfertile populations, while Asian studies report slightly lower rates of 12–20% [15].
4. Pathophysiology of Polyp-Associated Subfertility
The mechanisms by which endometrial polyps impair fertility are multifactorial and involve mechanical, inflammatory, and molecular pathways. Understanding these mechanisms is essential for rational clinical decision-making (Figure 1).
4.1. Mechanical Interference and Anatomical Disruption
Endometrial polyps can physically obstruct the reproductive tract at multiple levels. Large polyps may occlude the tubal ostia, preventing sperm from reaching the fallopian tubes for fertilization. Even small polyps can impede sperm transport through the uterine cavity by creating physical barriers or altering normal flow patterns of uterine fluid [7,9]. Additionally, polyps may mechanically prevent embryo implantation by occupying potential implantation sites or creating an irregular endometrial surface that impairs embryo-endometrial apposition. The location of polyps appears to influence their impact on fertility, with fundal polyps potentially having greater effects on implantation than those in the lower uterine segment [16].
4.2. Molecular and Transcriptomic Abnormalities
Recent transcriptomic analyses have revealed intrinsic molecular abnormalities within endometrial polyps that extend beyond simple mechanical effects. Chiu et al. (2024) performed RNA sequencing on 12 paired samples of endometrial polyps and adjacent normal endometrium from infertile women, identifying 322 differentially expressed genes [11]. Protein-protein interaction network analysis revealed significant dysregulation in two key pathways: Wnt signaling and vascular smooth muscle regulation.
Specifically, Wnt-related genes showed complex alterations: DKK1 and DKKL1 (Wnt antagonists) were upregulated, while GPC3, GREM1, RSPO3, SFRP5, and WNT10B were downregulated [11]. This pattern suggests dysregulated Wnt signaling that may promote unrestrained growth and impair normal endometrial differentiation. Nearly all genes related to vascular smooth muscle contraction were downregulated in polyps, including ACTA2, ACTG2, KCNMB1, KCNMB2, MYL9, PPP1R12B, and TAGLN [11]. These vascular defects may contribute to abnormal bleeding patterns and impaired endometrial perfusion.
4.3. Chronic Inflammation and Cytokine Dysregulation
Endometrial polyps are frequently associated with chronic inflammation, characterized by increased infiltration of immune cells (macrophages, lymphocytes, and plasma cells) and altered cytokine profiles [36,37]. Studies have demonstrated elevated levels of pro-inflammatory cytokines in polyp tissue and surrounding endometrium, including interleukin-6 (IL-6), interleukin-8 (IL-8), and tumor necrosis factor-alpha (TNF-α) [38,39].
This inflammatory milieu may impair fertility through multiple mechanisms. Pro-inflammatory cytokines can disrupt normal endometrial receptivity by interfering with the expression of adhesion molecules and growth factors required for embryo implantation [40]. IL-6 and TNF-α have been shown to inhibit trophoblast invasion and reduce expression of leukemia inhibitory factor (LIF), a critical cytokine for implantation [41,42].
Chronic endometritis (CE), defined by the presence of plasma cells in the endometrial stroma, is detected in 14–57% of women with endometrial polyps [12,43]. The coexistence of polyps and CE may represent a synergistic impairment of fertility, with both conditions contributing to chronic inflammation and altered endometrial function. The diagnosis and management of chronic endometritis in women with polyps is discussed in detail in Section
4.4. Altered Endometrial Receptivity and HOXA Gene Dysregulation
Endometrial receptivity, the transient window during which the endometrium is permissive to embryo implantation, is regulated by a complex network of genes and signaling pathways. Several studies have demonstrated that endometrial polyps are associated with altered expression of receptivity markers, both within the polyp tissue itself and in the surrounding endometrium [44,45].
HOXA10 and HOXA11, members of the homeobox gene family, play critical roles in endometrial development, decidualization, and implantation [46]. Pîrlog et al. (2025) reviewed evidence linking altered HOXA10/HOXA11 expression to benign endometrial disorders, including polyps [47]. HOXA gene dysregulation may perturb endometrial receptivity through multiple mechanisms: impaired endometrial differentiation during the secretory phase, reduced expression of implantation-related genes (including integrin αvβ3 and HOXA10-regulated targets), and altered decidualization in response to progesterone [47,48].
Studies using endometrial receptivity arrays (ERAs) have shown that women with endometrial polyps have a higher prevalence of displaced implantation windows than controls [49]. This suggests that polyps may cause temporal dysregulation of endometrial receptivity, such that the window of maximal receptivity does not align with the expected timing of embryo arrival or transfer.
Other receptivity markers altered in the presence of polyps include: reduced expression of pino-podes (ultrastructural markers of receptivity) [50], decreased glycodelin and osteopontin (secretory proteins involved in implantation) [6], and altered expression of progesterone receptor isoforms [51]. These molecular changes may extend beyond the polyp itself to affect the entire endometrial cavity, providing a mechanistic explanation for why even small polyps can impair fertility.
4.5. Impaired Decidualization and Immune Microenvironment
Decidualization, the progesterone-driven transformation of endometrial stromal cells into specialized decidual cells, is essential for successful implantation and maintenance of early pregnancy. Endometrial polyps have been associated with impaired decidualization, characterized by reduced expression of decidual markers (prolactin, IGFBP-1) and altered stromal cell morphology [52,53].
The endometrial immune microenvironment plays a critical role in implantation and early pregnancy. The normal mid-secretory endometrium contains a balanced population of immune cells, including uterine natural killer (uNK) cells, macrophages, and regulatory T cells, which facilitate trophoblast invasion while maintaining tolerance to the semi-allogeneic embryo [54]. Studies have shown that endometrial polyps are associated with altered immune cell populations, including increased macrophage infiltration and altered uNK cell phenotypes [55,56].
Additionally, polyps may disrupt the normal balance between pro-inflammatory and anti-inflammatory signals required for successful implantation. The “inflammatory paradox” of implantation, whereby a controlled inflammatory response is necessary for trophoblast invasion but excessive inflammation is detrimental, may be disrupted by polyps [57]. This dysregulated immune environment may contribute to implantation failure or early pregnancy loss even after successful initial implantation.
5. Diagnostic Approaches
Accurate diagnosis of endometrial polyps is essential for appropriate management. Multiple imaging modalities are available, each with distinct advantages and limitations. The diagnostic characteristics of various modalities are summarized in Table 2.
5.1. Transvaginal Ultrasonography
Two-dimensional transvaginal ultrasonography (2D-TVS) is typically the first-line imaging modality for evaluating the endometrium. Polyps appear as hyperechoic focal lesions within the endometrial cavity, often with a feeding vessel demonstrable on color Doppler imaging. However, diagnostic accuracy is limited, with reported sensitivity ranging from 55% to 88% and specificity from 65% to 95% [28,29]. Performance is optimal during the proliferative phase when the thin endometrium provides better contrast with polyps. Three-dimensional ultrasound (3D-TVS) provides improved visualization of the uterine cavity and may increase diagnostic accuracy to 90–95%.
5.2. Saline Infusion Sonohysterography
Saline infusion sonohysterography (SIS), also known as sonohysterography, involves instilling sterile saline into the uterine cavity during transvaginal ultrasound. This technique significantly improves polyp detection compared with standard TVS, with sensitivities of 87–94% and specificities of 81–94% [29,30,31,32]. SIS enables more precise delineation of polyp size, location, and relationship to the tubal ostia. The procedure is well-tolerated in the office setting and provides valuable information for surgical planning. Meta-analysis has confirmed the superiority of SIS over 2D-TVS for polyp detection, with a pooled sensitivity of 92% versus 55% [29].
5.3. Hysteroscopy
Hysteroscopy remains the gold standard for diagnosis of endometrial polyps, with a sensitivity of 92–100% and a specificity of 75–94% [9,38]. Direct visualization allows accurate assessment of polyp characteristics and enables simultaneous treatment. Office hysteroscopy, performed without anesthesia using small-diameter hysteroscopes (≤5 mm), has become increasingly popular due to convenience, cost-effectiveness, and high patient acceptability [6]. Studies report successful completion rates of 95–98% for office procedures, with minimal complications. The “see-and-treat” approach, combining diagnosis and treatment in a single office visit, offers significant advantages in terms of efficiency and patient convenience.
5.4. Diagnostic Algorithm
For subfertile women, a stepwise diagnostic approach is recommended. Initial evaluation with TVS during the proliferative phase can identify obvious polyps. When TVS findings are equivocal or polyps are suspected based on clinical presentation, SIS improves accuracy. Hysteroscopy should be performed when imaging suggests polyps requiring treatment or when the diagnosis remains uncertain.
6. Surgical Treatment
The impact of hysteroscopic polypectomy on fertility outcomes has been evaluated in multiple studies across different fertility treatment contexts: intrauterine insemination (IUI), in vitro fertilization/intracytoplasmic sperm injection (IVF/ICSI), and natural conception. The quality and consistency of evidence vary by treatment modality.6.1. Intrauterine Insemination
The strongest evidence for the benefit of hysteroscopic polypectomy comes from studies of women undergoing IUI. The landmark randomized controlled trial by Pérez-Medina et al. (2005) randomized 215 infertile women with endometrial polyps to either hysteroscopic polypectomy followed by IUI (n=107) or diagnostic hysteroscopy alone followed by IUI (n=108) [4]. The polypectomy group had significantly higher pregnancy rates: 63% (67/107) versus 28% (30/108), yielding a relative risk of 2.1 (95% CI 1.5–2.9, p<0.001) [4]. This trial provides Level I evidence supporting polypectomy before IUI.
Subsequent observational studies have corroborated these findings. Stamatellos et al. (2008) reported pregnancy rates of 78.3% (65/83) after polypectomy in women with unexplained infertility, with most pregnancies occurring within 12 months [35]. Shokeir et al. (2004) found that polypectomy improved pregnancy rates in women with unexplained infertility and polyps, with a relative risk of 2.3 (95% CI 1.1–4.8) compared to expectant management [17]. A 2019 systematic review by Zhang et al. included five studies (one RCT and four cohort studies) comparing polypectomy versus no treatment in women undergoing IUI or attempting natural conception [74]. The pooled analysis showed significantly higher pregnancy rates after polypectomy (OR 2.9, 95% CI 1.8–4.6, p<0.001) [74]. The benefit was consistent across studies despite heterogeneity in polyp size, patient age, and duration of infertility.
6.2. In Vitro Fertilization and Intracytoplasmic Sperm Injection
Evidence for the benefit of polypectomy in women undergoing IVF/ICSI is more heterogeneous, though most studies suggest improved outcomes. It is critical to distinguish two clinical scenarios: (1) polypectomy of documented polyps before IVF, and (2) routine screening hysteroscopy before IVF with polypectomy of incidentally detected polyps.
6.2.1. Polypectomy of Documented Polyps Before IVF
Multiple retrospective cohort studies have reported favorable outcomes after polypectomy in women with documented polyps undergoing IVF/ICSI. Reported clinical pregnancy rates after polypectomy range from 53% to 72%, and live birth rates from 43% to 66% [77,78,79,80]. Triantafyllidou et al. (2024) reported outcomes in 40 women with unexplained infertility who underwent hysteroscopic polypectomy before IVF [78]. The clinical pregnancy rate was 65% (26/40), and the total positive pregnancy rate was 72.5% (29/40, including 3 biochemical pregnancies) [78]. This retrospective cohort study demonstrates favorable outcomes after polypectomy in carefully selected patients with unexplained infertility.
Wen et al. (2024) analyzed 1,247 infertility patients undergoing IVF/ICSI, of whom 312 had concomitant endometrial polyps [79]. After polypectomy, clinical pregnancy rates and live birth rates were comparable to those of patients without polyps, suggesting that polypectomy normalizes reproductive outcomes [79]. A 2024 systematic review and meta-analysis by Wang et al. evaluated whether hysteroscopy improves fertility outcomes in women undergoing IVF/ICSI [80]. The analysis included 23 studies with 11,887 patients. Hysteroscopy with treatment of identified pathology (including polypectomy) was associated with improved clinical pregnancy rates (RR 1.34, 95% CI 1.19–1.51) and live birth rates (RR 1.43, 95% CI 1.21–1.69) compared to no hysteroscopy [80]. However, this analysis included women with various intrauterine pathologies, not exclusively polyps.
6.2.2. Routine Screening Hysteroscopy Before IVF
The role of routine screening hysteroscopy before IVF in unselected patients remains controversial. The Cochrane review by Bosteels et al. (2018) evaluated the evidence for hysteroscopy as a diagnostic or therapeutic intervention before IVF/ICSI [107]. The review concluded that hysteroscopy may improve clinical pregnancy rates in women with suspected uterine cavity abnormalities, but the overall certainty of evidence was low to moderate, with substantial heterogeneity across included trials. The TROPHY trial (El-Toukhy et al. 2016), a multicenter RCT of 702 women with recurrent IVF failure, found no significant improvement in live birth rates with routine outpatient hysteroscopy before the next IVF cycle (29% vs. 29%, RR 1.00, 95% CI 0.78–1.27) [108]. Based on these findings, routine screening hysteroscopy before a first IVF cycle is not universally recommended. However, targeted hysteroscopy in women with suspected intrauterine pathology on imaging or those with recurrent implantation failure remains a reasonable clinical approach.
6.2.3. Timing of Embryo Transfer After Polypectomy
The optimal interval between polypectomy and embryo transfer remains debated. Dunn et al. (2018) investigated whether early embryo transfer (<30 days) after hysteroscopic polypectomy affects outcomes compared to delayed transfer (≥30 days) [81]. In 389 frozen embryo transfer cycles, early transfer was associated with lower live birth rates (38% vs 51%, p=0.02) and higher miscarriage rates (26% vs 13%, p=0.02) [81]. This suggests that a minimum interval of 30 days should be allowed for endometrial healing and normalization of the inflammatory milieu before embryo transfer. However, other studies have not confirmed this finding. Several retrospective analyses found no difference in outcomes between immediate (next cycle) and delayed embryo transfer after polypectomy [82,83]. The discrepancy may relate to differences in polypectomy technique, polyp size, or patient characteristics. Current practice typically allows 1–2 menstrual cycles between polypectomy and embryo transfer, balancing concerns about endometrial healing with the desire to minimize treatment delay.
6.2.4. Polypectomy Technique
Recent studies have compared different hysteroscopic polypectomy techniques. Wang et al. (2025) compared manual hysteroscopic tissue removal devices versus conventional resection in 240 women undergoing IVF [84]. No significant differences were observed in clinical pregnancy rates, live birth rates, or complications between techniques [84]. This suggests that the benefit of polypectomy is independent of the specific technique used, provided complete polyp removal is achieved. Wang et al. (2024) investigated whether pretreatment with long-acting GnRH agonists before hysteroscopic multiple polypectomy improves outcomes [85]. In women with multiple polyps, GnRH agonist pretreatment was associated with improved pregnancy outcomes, possibly through endometrial thinning that facilitates complete polyp visualization and removal [85].
6.3. Natural Conception
Several studies have evaluated fertility outcomes after polypectomy in women attempting natural conception without assisted reproductive technology. Stamatellos et al. (2008) reported that 78.3% of women with unexplained infertility and polyps achieved pregnancy within 12 months after polypectomy, compared to historical controls [35]. Most pregnancies occurred within the first 6 months, suggesting that polypectomy rapidly restores fertility potential. Pérez-Medina et al. (2005) included a subset of women who attempted natural conception after randomization to polypectomy versus diagnostic hysteroscopy alone [4]. Pregnancy rates were higher in the polypectomy group across all conception methods (natural, IUI, and IVF), indicating a general fertility-enhancing effect of polyp removal. A 2017 cost-analysis and systematic review by Mouhayar et al. evaluated the cost-effectiveness of hysteroscopic polypectomy prior to infertility treatment [86]. The analysis concluded that polypectomy is cost-effective when performed before IUI or natural conception attempts, given the relatively low cost of the procedure and the substantial improvement in pregnancy rates [86]. For IVF, cost-effectiveness depends on polyp size and patient age, with greater benefit for larger polyps and younger women.
7. Chronic Endometritis: Diagnosis and Management
Chronic endometritis (CE) is increasingly recognized as an important cause of subfertility and recurrent implantation failure. CE is defined histologically by the presence of plasma cells in the endometrial stroma, typically identified using immunohistochemistry for CD138 (syndecan-1), a plasma cell marker [87]. The prevalence of CE in subfertile women ranges from 14% to 57%, depending on the population studied and diagnostic criteria employed [12,43,88].
The relationship between endometrial polyps and chronic endometritis is complex. Some studies suggest that polyps may harbor or promote chronic inflammation, while others propose that CE and polyps are independent conditions that frequently coexist [12]. Regardless of the causal relationship, the presence of both conditions may synergistically impair fertility, and both warrant treatment in subfertile women.
7.1. Standardized CD138-Based Diagnosis
Histologic diagnosis of CE has traditionally relied on identification of plasma cells on hematoxylin and eosin (H&E) staining, but this approach has poor sensitivity and substantial inter-observer variability [89]. Immunohistochemistry for CD138 substantially improves diagnostic accuracy and reproducibility [90].
However, significant heterogeneity exists in the CD138 threshold used to diagnose CE. Reported cutoffs range from ≥1 plasma cell per high-power field (HPF) to ≥5 plasma cells per 10 HPFs [91,92]. This variability complicates the interpretation of the literature and comparison across studies.
Recent efforts have focused on standardizing CD138-based diagnosis. De Smet et al. (2024) developed a 5-tier CD138 scoring system (classes 0-3) based on a systematic evaluation of multiple endometrial samples [93]. The scoring system demonstrated good-to-excellent inter-observer agreement (Fleiss’ Kappa 0.722 for 5-tier classification; 0.858 for a 2-tier clinically relevant classification) [93]. This standardized approach may improve diagnostic consistency and facilitate comparison across studies.
Herlihy et al. (2022) prospectively evaluated the prognostic significance of different CD138 thresholds in 200 women undergoing IVF [94]. Plasma cells were detected in 49% of women using a threshold of ≥1 plasma cell per 10 HPFs, but low plasma cell counts (1, 5, or 10 per 10 HPFs) did not predict implantation or live birth rates [94]. This suggests that low-level CD138 positivity may be prevalent in asymptomatic women and may lack clinical significance.
Liu et al. (2022) used a diagnostic threshold of ≥5 CD138+ cells per HPF in a large cohort of 4,003 embryo transfer cycles [95]. Women with ≥5 CD138+ cells/HPF who achieved cure after antibiotic treatment had significantly improved reproductive outcomes compared to those with persistent CE [95]. This supports ≥5 CD138+ cells/HPF as a clinically meaningful threshold that identifies women who benefit from treatment.
Clinical synthesis:
Current evidence suggests that a threshold of ≥5 CD138+ plasma cells per HPF represents a reasonable diagnostic cutoff that balances sensitivity and specificity while identifying women most likely to benefit from antibiotic treatment [95,96]. Standardized histopathologic scoring systems, such as that proposed by de Smet et al., should be adopted to improve diagnostic reproducibility [93]. Endometrial biopsy for CE diagnosis should be performed during the proliferative phase (days 5–12 of the menstrual cycle) to avoid confounding by menstrual-phase plasma cells [97].
7.2. Antibiotic Treatment Protocols
Multiple antibiotic regimens have been used to treat CE in subfertile women, with substantial heterogeneity in drug choice, dose, duration, and route of administration. The most commonly used regimens include:
Doxycycline: 100 mg orally twice daily for 14 days is the most widely used first-line regimen [70,87]. Doxycycline provides broad-spectrum coverage including common endometrial pathogens (Streptococcus, Enterococcus, Escherichia coli, and Ureaplasma) and has good tissue penetration.
Combination regimens: Some protocols use combination therapy, such as doxycycline plus metronidazole (500 mg orally twice daily for 14 days) to provide additional anaerobic coverage [69]. Ciprofloxacin (500 mg orally twice daily for 14 days) has also been used, either alone or in combination [98].
Intrauterine antibiotic infusion: Luncan et al. (2022) compared intrauterine antibiotic infusion versus oral antibiotic therapy in 90 women with CE undergoing IVF [99]. Intrauterine infusion (gentamicin 80 mg + dexamethasone 8 mg in 5 mL saline, administered via intrauterine catheter) achieved a higher cure rate (89% negative test-of-cure) compared to oral combination therapy (doxycycline + metronidazole, 46% cure rate) [99]. This suggests that local intrauterine delivery may increase histologic resolution rates, though this approach requires further validation.
7.3. Impact on Fertility Outcomes
Multiple studies have demonstrated that successful treatment of CE improves fertility outcomes in women undergoing assisted reproduction. Liu et al. (2022) performed a systematic review and meta-analysis of 12 studies evaluating antibiotic treatment for CE in women with reproductive failures [101]. Women with cured CE had significantly higher ongoing pregnancy/live birth rates (OR 2.85, 95% CI 1.60–5.08) and clinical pregnancy rates (OR 2.31, 95% CI 1.55–3.44) compared to women with persistent CE [101].
Vitagliano et al. (2022) conducted a systematic review and meta-analysis specifically focused on CE in women undergoing IVF [102]. Women with untreated CE had lower ongoing pregnancy/live birth rates (OR 1.97, p=0.02) and clinical pregnancy rates (OR 2.28, p=0.002) compared to women without CE [102]. Importantly, CE cure after antibiotic therapy increased ongoing pregnancy/live birth rates (OR 5.33, p<0.0001) and clinical pregnancy rates (OR 3.64, p=0.0001) [102]. After successful treatment, outcomes were comparable to women without CE, suggesting that antibiotic therapy normalizes reproductive potential [102].
Li et al. (2023) analyzed pregnancy outcomes in 327 women with recurrent implantation failure, of whom 117 (35.8%) had CE [103]. After antibiotic and platelet-rich plasma (PRP) treatment, 70.9% of women achieved CE cure [103]. The CE-cured group had significantly higher clinical pregnancy rates (60.0% vs 36.4%, p<0.01) and live birth rates (48.6% vs 27.3%, p<0.05) compared to women with persistent CE [103].
However, important caveats exist. Zhang et al. (2023) reported that women with antibiotic-cured CE undergoing single euploid frozen embryo transfer had higher early pregnancy loss rates compared to women without CE (23.5% vs 11.8%, p=0.03) [104]. This indicates that histologic cure does not fully normalize early pregnancy outcomes and suggests residual functional alterations in the endometrium after CE treatment [104].
Clinical synthesis:
Current evidence supports screening for CE in women with unexplained infertility, recurrent implantation failure, or recurrent pregnancy loss. Diagnosis should be based on standardized CD138 immunohistochemistry with a threshold of ≥5 CD138+ cells/HPF. First-line treatment is doxycycline 100 mg orally twice daily for 14 days, with test-of-cure biopsy 1–2 months after treatment [95,101,102]. Women with persistent CE may benefit from alternative regimens or intrauterine antibiotic infusion [99]. Successful CE cure substantially improves reproductive outcomes and should be achieved before proceeding with embryo transfer.

Table 3.
Pregnancy Outcomes After Polypectomy by Treatment Modality.
| Treatment Modality | Clinical Pregnancy Rate (%) | Live Birth Rate (%) | Key Evidence | Level of Evidence † |
|---|---|---|---|---|
| Natural conception | 28–65 | 22–55 | Observational studies | III |
| IUI | 51–63 | 43–55 | Pérez-Medina 2005 RCT [7] | I |
| IVF/ICSI | 53–72 | 43–66 | Meta-analyses, cohort studies | I–II |
| RIF patients | 45–73 | 38–62 | Prospective cohorts | II |
Abbreviations: IUI, intrauterine insemination; IVF, in vitro fertilization; ICSI, intracytoplasmic sperm injection; RIF, recurrent implantation failure. † Level of evidence: I = randomized controlled trial or meta-analysis of RCTs; II = prospective cohort study or meta-analysis of cohort studies; III = retrospective cohort or case-control study.
8. Clinical Management and Decision-Making
Integration of current evidence into clinical practice requires individualized decision-making that considers polyp characteristics, patient age, fertility treatment plan, and patient preferences. The 2024 Society of Obstetricians and Gynaecologists of Canada (SOGC) guideline provides updated recommendations for management of endometrial polyps in subfertile women [14].
Figure 2.
Clinical algorithm for management of endometrial polyps in subfertile women. The flowchart guides clinical decision-making based on polyp characteristics (size, symptoms), patient factors (age, duration of infertility), and planned fertility treatment (expectant management, IUI, IVF/ICSI). Strong evidence supports polypectomy for symptomatic polyps, polyps ≥10 mm, and polyps in women undergoing IUI or IVF/ICSI. For small asymptomatic polyps (<10 mm), individualized decision-making is appropriate. Chronic endometritis screening and treatment should be considered in women with hysteroscopic findings suggestive of CE.
Figure 2.
Clinical algorithm for management of endometrial polyps in subfertile women. The flowchart guides clinical decision-making based on polyp characteristics (size, symptoms), patient factors (age, duration of infertility), and planned fertility treatment (expectant management, IUI, IVF/ICSI). Strong evidence supports polypectomy for symptomatic polyps, polyps ≥10 mm, and polyps in women undergoing IUI or IVF/ICSI. For small asymptomatic polyps (<10 mm), individualized decision-making is appropriate. Chronic endometritis screening and treatment should be considered in women with hysteroscopic findings suggestive of CE.

8.1. Indications for Polypectomy
Strong evidence supports polypectomy in the following scenarios: 1. Symptomatic polyps: Women with abnormal uterine bleeding, dysmenorrhea, or other symptoms attributable to polyps should undergo polypectomy regardless of fertility plans [14]. 2. Polyps ≥10 mm: Larger polyps are more likely to impair fertility through mechanical and inflammatory mechanisms and should be removed before fertility treatment [4,74]. 3. Before IUI: Level I evidence supports polypectomy before IUI in women with documented polyps [4]. 4. Before IVF/ICSI with documented polyps: Moderate-quality evidence supports polypectomy of documented polyps before IVF/ICSI [80]. 5. Polyps in women with unexplained infertility: Removal of polyps may restore fertility potential and allow natural conception or less intensive fertility treatment [17,35].
8.2. Uncertain Indications
Evidence is less clear for: 1. Small asymptomatic polyps (<10 mm): Limited direct evidence exists for the benefit of removing small polyps, and spontaneous regression occurs in 25–27% of cases [76,105,106]. Individualized decision-making is appropriate, considering patient age, duration of infertility, and planned fertility treatment. 2. Routine screening hysteroscopy before IVF: While some centers perform routine hysteroscopy before IVF to detect and treat unsuspected intrauterine pathology, the cost-effectiveness and benefit of this approach remain debated [107,108]. 3. Polyps in women with other identified causes of infertility: When a clear alternative explanation for infertility exists (e.g., severe male factor, tubal occlusion), the incremental benefit of polypectomy is uncertain.
8.3. Contraindications and Special Considerations
Hysteroscopic polypectomy is generally safe, with complication rates <2% [109]. Rare complications include uterine perforation, infection, intrauterine adhesions, and anesthetic complications. Polypectomy should be deferred in women with active pelvic infection or pregnancy. In women with multiple polyps or polyps >2 cm, consideration should be given to GnRH agonist pretreatment to thin the endometrium and facilitate complete visualization and removal [85]. Operative hysteroscopy under anesthesia may be required for large or multiple polyps, whereas small, solitary polyps can often be removed during office hysteroscopy without anesthesia.
8.4. Post-polypectomy Management
After polypectomy, most clinicians recommend waiting 1–2 menstrual cycles before proceeding with fertility treatment to allow endometrial healing [81]. However, the optimal interval remains uncertain, and some studies suggest that immediate (next-cycle) treatment is acceptable for small polyps [82,83]. Histopathologic examination of all removed polyps is essential to exclude malignancy or premalignant changes, though the risk is very low in women under 40 years of age (<1%) [110]. If chronic endometritis is suspected based on hysteroscopic appearance (focal hyperemia, stromal edema, micropolyps), endometrial biopsy for CD138 immunohistochemistry should be performed, and antibiotic treatment initiated if CE is confirmed [70,93]. For surveillance of recurrence, routine imaging is not required if complete resection has been confirmed; however, repeat TVS or SIS should be performed at 6–12 months if pregnancy has not been achieved or if symptoms recur. Patients with risk factors for recurrence (multiple polyps, metabolic syndrome, chronic anovulation) should be counseled about modifiable risk reduction and may benefit from closer follow-up.
8.5. Expectant Management and Surveillance
For small asymptomatic polyps (<10 mm) in women not immediately pursuing fertility treatment, expectant management with surveillance ultrasound is a reasonable alternative to immediate polypectomy [106]. Spontaneous regression occurs in approximately 25% of small polyps within 12 months [105]. However, if the polyp persists or enlarges, or if the woman subsequently pursues fertility treatment, polypectomy should be performed.
9. Discussion
This review synthesizes current evidence on endometrial polyps and subfertility in women under 40 years of age. The findings consistently support hysteroscopic polypectomy as an effective intervention for improving fertility outcomes across treatment modalities.
9.1. Strengths of Current Evidence
The evidence base has several notable strengths. First, the Pérez-Medina RCT provides Level I evidence demonstrating a clear benefit of polypectomy before IUI, with a relative risk of 2.1 for achieving pregnancy [7]. The consistency of findings across subsequent observational studies strengthens the generalizability of these results. Second, multiple pathophysiological mechanisms have been identified that link polyps to impaired fertility, thereby providing biological plausibility. Third, recent meta-analyses have confirmed and quantified the benefit of polypectomy [38,40]. Fourth, cost-effectiveness analyses support polypectomy as economically rational [41].
9.2. Evidence Gaps and Limitations
Despite the overall strength of evidence, several important gaps warrant acknowledgment. Evidence for polypectomy before IVF is less robust than for IUI, with no large randomized controlled trials directly addressing this question. The management of small polyps (<10 mm) remains uncertain despite recent guideline recommendations. The optimal timing of intervention relative to fertility treatment remains poorly defined.
9.3. Clinical Practice Implications
Routine evaluation for endometrial polyps should be incorporated into the diagnostic workup of subfertile women. When polyps are identified, hysteroscopic polypectomy should be considered, although the evidence for removing small asymptomatic polyps (<10 mm) remains limited[13]. Histopathologic examination should be performed to assess for malignancy and chronic endometritis, with antibiotic therapy if plasma cells are identified.
10. Special Populations
10.1. Advanced Maternal Age
Women of advanced reproductive age (≥35 years) face declining ovarian reserve and potentially increased polyp prevalence. In this population, timely diagnosis and treatment are particularly important. The approach should favor prompt polypectomy with expedited progression to fertility treatment.
10.2. Polycystic Ovary Syndrome
Women with polycystic ovary syndrome (PCOS) may have increased polyp prevalence due to chronic anovulation and unopposed estrogen exposure [42]. Management should address both the polyp and underlying PCOS. Metformin and lifestyle modification may reduce the risk of polyp recurrence.
10.3. Recurrent Pregnancy Loss
Women with recurrent pregnancy loss should be evaluated for endometrial polyps as part of the comprehensive workup. The association between polyps, chronic endometritis, and RPL suggests that polyp removal and treatment of associated inflammation may reduce miscarriage risk [21].
11. Future Directions
Despite substantial progress in understanding the relationship between endometrial polyps and subfertility, several important questions remain unresolved. Not all polyps impair fertility to the same degree. Identification of molecular biomarkers (e.g., specific gene expression signatures, cytokine profiles, or receptivity markers) that predict which polyps are most likely to impair fertility would enable more targeted treatment decisions. The transcriptomic abnormalities identified by Chiu et al. [11] and the HOXA gene dysregulation reviewed by Pîrlog et al. [47] represent promising starting points for such investigations. While most studies suggest waiting 1–2 cycles after polypectomy before embryo transfer, the optimal interval has not been definitively established. Prospective studies comparing immediate versus delayed treatment, with mechanistic endpoints (e.g., endometrial receptivity markers, inflammatory cytokines) in addition to clinical outcomes, would help clarify this question.
Most studies have included heterogeneous populations of subfertile women. Subgroup analyses or dedicated studies in specific populations (e.g., women with recurrent implantation failure, recurrent pregnancy loss, or specific polyp characteristics) would refine treatment recommendations. Most studies report short-term outcomes (pregnancy rate, live birth rate in the first treatment cycle). Long-term outcomes, including cumulative live birth rates over multiple cycles, time to pregnancy, and obstetric complications, are less well characterized.
Polyp recurrence rates after hysteroscopic removal range from 3.7% to 15% [25,64]. Identified risk factors include incomplete base resection (particularly with grasping forceps versus resectoscopy), multiple polyps at initial diagnosis, obesity and metabolic syndrome, chronic endometritis, tamoxifen use, chronic anovulation, and older age [25,64]. Technique-specific data suggest that complete base resection using monopolar or bipolar resectoscopy is associated with lower recurrence than blind curettage or simple avulsion [77]. Recommended post-polypectomy surveillance includes: (1) no routine imaging if complete resection was achieved; (2) repeat TVS or SIS at 6–12 months if pregnancy is not achieved; (3) immediate re-evaluation if symptoms recur (abnormal bleeding); and (4) addressing modifiable risk factors (weight management, CE treatment) in high-risk patients. Strategies to prevent recurrence, including hormonal interventions, warrant further investigation.
12. Conclusions
Endometrial polyps are common in subfertile women and are associated with impaired fertility through multiple mechanisms, including mechanical interference, intrinsic molecular abnormalities, chronic inflammation, altered endometrial receptivity, and disruption of the immune microenvironment. Recent transcriptomic studies have revealed fundamental changes in gene expression in polyp tissue, including dysregulation of Wnt signaling and vascular smooth muscle genes, that may contribute to subfertility even in the absence of significant anatomical distortion.
Current evidence supports hysteroscopic polypectomy as an effective intervention to improve fertility outcomes, particularly in women undergoing intrauterine insemination. Level I evidence from randomized controlled trials demonstrates that polypectomy before IUI more than doubles pregnancy rates. For women undergoing IVF/ICSI, moderate-quality evidence suggests that polypectomy of documented polyps improves clinical pregnancy and live birth rates, though the magnitude of benefit is more variable.
Chronic endometritis frequently coexists with endometrial polyps and independently impairs fertility. Standardized diagnosis using CD138 immunohistochemistry with a threshold of ≥5 plasma cells per high-power field identifies women who benefit from antibiotic treatment. Doxycycline 100 mg orally twice daily for 14 days is the recommended first-line regimen, with test-of-cure biopsy to confirm resolution. Successful treatment of chronic endometritis substantially improves reproductive outcomes.
Clinical decision-making should be individualized based on polyp characteristics, patient age, fertility treatment plan, and patient preferences. Strong evidence supports polypectomy for symptomatic polyps, polyps ≥10 mm, and polyps in women undergoing IUI or IVF/ICSI. For small asymptomatic polyps (<10 mm), individualized decision-making is appropriate, considering the potential for spontaneous regression and the limited direct evidence for benefit of removal.
Future research should focus on identifying molecular predictors of polyp-associated infertility, optimizing the timing of polypectomy relative to fertility treatment, clarifying the role of polypectomy in specific subpopulations, and standardizing the diagnosis and treatment of chronic endometritis. These advances will enable more personalized and effective management of endometrial polyps in subfertile women.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, G.G. and O.B.; Methodology, G.G. and O.B.; Data Curation, G.G.; Writing—Original Draft Preparation, G.G.; Writing—Review and Editing, G.G. and O.B.; Supervision, O.B. All authors have read and agreed to the published version of the manuscript.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Salim, S.; Won, H.; Nesbitt-Hawes, E.; Campbell, N.; Abbott, J. Diagnosis and Management of Endometrial Polyps: A Critical Review of the Literature. J. Minim. Invasive Gynecol. 2011, 18, 569–581. [Google Scholar] [CrossRef]
- Lieng, M.; Istre, O.; Qvigstad, E. Treatment of Endometrial Polyps: A Systematic Review. Acta Obstet. Gynecol. Scand. 2010, 89, 992–1002. [Google Scholar] [CrossRef]
- Pereira, N.; Amrane, S.; Estes, J.L.; Lekovich, J.P.; Elias, R.T.; Spandorfer, S.D. Surgical Management of Endometrial Polyps in Infertile Women: A Comprehensive Review. Surg. Res. Pract. 2015, 2015, 914390. [Google Scholar] [CrossRef] [PubMed]
- Zegers-Hochschild, F.; Adamson, G.D.; Dyer, S.; Racowsky, C.; De Mouzon, J.; Sokol, R.; Rienzi, L.; Sunde, A.; Schmidt, L.; Cooke, I.D.; et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil. Steril. 2017, 108, 393–406. [Google Scholar] [CrossRef]
- Shokeir, T.A.; Shalan, H.M.; El-Shafei, M.M. Significance of Endometrial Polyps Detected Hysteroscopically in Eumenorrheic Infertile Women. J. Obstet. Gynaecol. Res. 2004, 30, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Bettocchi, S.; Nappi, L.; Ceci, O.; Selvaggi, L. Office Hysteroscopy. Obstet. Gynecol. Clin. N. Am. 2004, 31, 641–654. [Google Scholar] [CrossRef]
- Pérez-Medina, T.; Bajo-Arenas, J.; Salazar, F.; Redondo, T.; Sanfrutos, L.; Alvarez, F.; Engels, V. Endometrial Polyps and Their Implication in the Pregnancy Rates of Patients Undergoing Intrauterine Insemination: A Prospective, Randomized Study. Hum. Reprod. 2005, 20, 1632–1635. [Google Scholar] [CrossRef]
- Chambers, G.M.; Sullivan, E.A.; Ishihara, O.; Chapman, M.G.; Adamson, G.D. The Economic Impact of Assisted Reproductive Technology: A Review of Selected Developed Countries. Fertil. Steril. 2009, 91, 2281–2294. [Google Scholar] [CrossRef]
- Varasteh, N.N.; Neuwirth, R.S.; Levin, B.; Keltz, M.D. Pregnancy Rates After Hysteroscopic Polypectomy and Myomectomy in Infertile Women. Obstet. Gynecol. 1999, 94, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Stamatellos, I.; Apostolides, A.; Stamatopoulos, P.; Bontis, J. Pregnancy Rates After Hysteroscopic Polypectomy Depending on the Size or Number of the Polyps. Arch. Gynecol. Obstet. 2008, 277, 395–399. [Google Scholar] [CrossRef]
- Al-Quran, F.; Al-Fayez, N.; Qudah, S.; Shraideh, Z.; O’Moush, R. Spontaneous Pregnancy Rate After Hysteroscopic Removal of Endometrial Polyps in Infertility Patients; Experience at King Hussein Medical Center. J. R. Med. Serv. 2018, 25, 27–31. [Google Scholar] [CrossRef]
- Modesto, W.; Bahamondes, M.V.; Bahamondes, L. Hysteroscopic Polypectomy Versus Expectant Management in Asymptomatic Infertile Women: A Meta-Analysis. Int. J. Reprod. Contracept. Obstet. Gynecol. 2020, 9, 2765–2770. [Google Scholar] [CrossRef]
- Bougie, O.; Randle, E.; Thurston, J.; Black, A.; Bhatt, J.; Glanc, P.; Gonçalves, J.; Guo, Y.; Laberge, P.; Leyland, N.; et al. Guideline No. 447: Diagnosis and Management of Endometrial Polyps. J. Obstet. Gynaecol. Can. 2024, 46, 102402. [Google Scholar] [CrossRef]
- Tuncer, S.F.; Yildiz, G.; Ozcan, A.; Karadeniz, T.; Kilic, F.; Kuru Pekcan, M.; Yildiz, P.; Inal, H.A. Comprehensive Analysis of Risk Factors for Recurrence in Women of Reproductive Age Undergoing Hysteroscopic Polypectomy. Med. Sci. Monit. 2025, 31, e950098. [Google Scholar] [CrossRef]
- Dreisler, E.; Stampe Sorensen, S.; Ibsen, P.H.; Lose, G. Prevalence of Endometrial Polyps and Abnormal Uterine Bleeding in a Danish Population Aged 20–74 Years. Ultrasound Obstet. Gynecol. 2009, 33, 102–108. [Google Scholar] [CrossRef]
- Yanaihara, A.; Yorimitsu, T.; Motoyama, H.; Iwasaki, S.; Kawamura, T. Location of Endometrial Polyp and Pregnancy Rate in Infertility Patients. Fertil. Steril. 2008, 90, 180–182. [Google Scholar] [CrossRef]
- Cicinelli, E.; Resta, L.; Nicoletti, R.; Zappimbulso, V.; Tartagni, M.; Saliani, N. Endometrial Micropolyps at Fluid Hysteroscopy Suggest the Existence of Chronic Endometritis. Hum. Reprod. 2005, 20, 1386–1389. [Google Scholar] [CrossRef]
- Johnston-MacAnanny, E.B.; Hartnett, J.; Engmann, L.L.; Nulsen, J.C.; Sanders, M.M.; Benadiva, C.A. Chronic Endometritis Is a Frequent Finding in Women with Recurrent Implantation Failure After In Vitro Fertilization. Fertil. Steril. 2010, 93, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Kasius, J.C.; Fatemi, H.M.; Bourgain, C.; Sie-Go, D.M.D.S.; Eijkemans, R.J.C.; Fauser, B.C.; Devroey, P.; Broekmans, F.J.M. The Impact of Chronic Endometritis on Reproductive Outcome. Fertil. Steril. 2011, 96, 1451–1456. [Google Scholar] [CrossRef] [PubMed]
- Văduva, C.C.; Stepan, A.E.; Niculescu, M.; Popa, R.G.; Neamțu, S.D.; Florescu, M.M.; Niculescu, C.E. The Association Between Endometrial Polyps, Chronic Endometritis and Endometriosis with Infertility. Rom. J. Morphol. Embryol. 2022, 63, 151–159. [Google Scholar]
- McQueen, D.B.; Bernardi, L.A.; Stephenson, M.D. Chronic Endometritis in Women with Recurrent Early Pregnancy Loss and/or Fetal Demise. Fertil. Steril. 2014, 101, 1026–1030. [Google Scholar] [CrossRef]
- Kitaya, K.; Matsubayashi, H.; Takaya, Y.; Nishiyama, R.; Yamaguchi, K.; Takeuchi, T.; Ishikawa, T. Live Birth Rate Following Oral Antibiotic Treatment for Chronic Endometritis in Infertile Women with Repeated Implantation Failure. Am. J. Reprod. Immunol. 2017, 78, e12719. [Google Scholar] [CrossRef] [PubMed]
- Taylor, H.S.; Arici, A.; Olive, D.; Igarashi, P. HOXA10 Is Expressed in Response to Sex Steroids at the Time of Implantation in the Human Endometrium. J. Clin. Investig. 1998, 101, 1379–1384. [Google Scholar] [CrossRef]
- Ashary, N.; Tiwari, A.; Modi, D. Homeobox Genes in Endometrium: From Development to Decidualization. Int. J. Dev. Biol. 2020, 64, 227–237. [Google Scholar] [CrossRef]
- Marwood, M.; Visser, K.; Salamonsen, L.A.; Dimitriadis, E. Interleukin-11 and Leukemia Inhibitory Factor Regulate the Adhesion of Endometrial Epithelial Cells: Implications in Fertility Regulation. Endocrinology 2009, 150, 2915–2923. [Google Scholar] [CrossRef]
- Richlin, S.S.; Ramachandran, S.; Shanti, A.; Murphy, A.A.; Parthasarathy, S. Glycodelin Levels in Uterine Flushings and in Plasma of Patients with Leiomyomas and Polyps: Implications for Implantation. Hum. Reprod. 2002, 17, 2742–2747. [Google Scholar] [CrossRef] [PubMed]
- Rackow, B.W.; Jorgensen, E.; Taylor, H.S. Endometrial Polyps Affect Uterine Receptivity. Fertil. Steril. 2011, 95, 2690–2692. [Google Scholar] [CrossRef] [PubMed]
- Niknejadi, M.; Haghighi, H.; Ahmadi, F.; Niknejad, F.; Chehrazi, M.; Vosough, A.; Miri, E. Diagnostic Accuracy of Transvaginal Sonography in the Detection of Uterine Abnormalities in Infertile Women. Iran. J. Radiol. 2012, 9, 139–144. [Google Scholar] [CrossRef]
- Sanin-Ramirez, A.; Madrazo-Navarro, M.; Reyna-Villasmil, N.; Reyna-Villasmil, E. Two-Dimensional Transvaginal Sonography vs Saline Contrast Sonohysterography for Diagnosing Endometrial Polyps: Systematic Review and Meta-Analysis. Ultrasound Obstet. Gynecol. 2020, 56, 851–860. [Google Scholar] [CrossRef]
- Güven, M.A.; Bese, T.; Demirkiran, F.; Idil, M.; Mgoyi, A. Hydrosonography in Screening for Intracavitary Pathology in Infertile Women. Int. J. Gynaecol. Obstet. 2004, 86, 377–383. [Google Scholar] [CrossRef]
- Ayida, G.; Chamberlain, P.; Barlow, D.; Kennedy, S. Uterine Cavity Assessment Prior to In Vitro Fertilization: Comparison of Transvaginal Scanning, Saline Contrast Hysterosonography and Hysteroscopy. Ultrasound Obstet. Gynecol. 1997, 10, 59–62. [Google Scholar] [CrossRef]
- Kaveh, M.; Ghajarzadeh, M.; Ghasemi, M.; Nasr, R. Comparison of Diagnostic Accuracy of Saline Infusion Sonohysterography, Transvaginal Sonography, and Hysteroscopy in Evaluating the Endometrial Polyps in Infertile Women. Videosurgery Miniinvasive Tech. 2020, 15, 310–316. [Google Scholar]
- Nishioka, Y.; Morohashi, R.; Kuji, N. Pregnancy Rates After Hysteroscopic Endometrial Polypectomy Versus Endometrial Curettage Polypectomy: A Retrospective Study. Medicina 2023, 59, 1868. [Google Scholar] [CrossRef]
- Wang, C.; Peng, Y.; Wang, Q.; Li, Y.; Liu, X.; Chen, H. No Differences in IVF Pregnancy Outcomes Following Hysteroscopic Polypectomy Using a Manual Hysteroscopic Tissue Removal Device Versus Conventional Resection. BMC Surg. 2025, 25, 128. [Google Scholar] [CrossRef]
- Wang, C.W.; Hsu, W.C.; Chou, C.Y.; Chang, D.Y.; Huang, K.E. Pretreatment with Long-Acting Gonadotropin-Releasing Hormone Agonists Improved Pregnancy Outcomes After Hysteroscopic Multiple Polypectomies: A Retrospective Cohort Study. Taiwan. J. Obstet. Gynecol. 2024, 63, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Triantafyllidou, O.; Korompokis, I.; Chasiakou, S.; Tsonis, O.; Sioutis, D.; Siristatidis, C. Impact of Hysteroscopic Polypectomy on IVF Outcomes in Women with Unexplained Infertility. J. Clin. Med. 2024, 13, 4755. [Google Scholar] [CrossRef]
- Wen, W.; Tu, X.; Ma, Y.; Li, Y. Risk Factors and Assisted Reproductive Outcomes in Infertility Patients with Concomitant Endometrial Polyps. J. Army Med. Univ. 2024, 46, 886–893. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, X.; Chen, H.; Li, Y.; Peng, Y.; Wang, Q. Whether Hysteroscopy Improves Fertility Outcomes in Women Undergoing IVF/ICSI: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2024, 15, 1489783. [Google Scholar] [CrossRef]
- Dunn, R.C.; Lathi, R.B.; Westphal, L.M.; Milki, A.A. Is There Such a Thing as Too Early? Effect of Early Embryo Transfer After Hysteroscopic Polypectomy on Live Birth and Other Pregnancy Outcomes. Fertil. Steril. 2018, 110, 1316–1321. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, Y.; Xue, Q.; Shang, J.; Yang, X.; Shan, C. Hysteroscopic Resection of Endometrial Polyps and Assisted Reproductive Technology Pregnancy Outcomes Compared with No Treatment: A Systematic Review. J. Minim. Invasive Gynecol. 2019, 26, 618–627. [Google Scholar] [CrossRef]
- Mouhayar, Y.; Franasiak, J.M.; Sharara, F.I. Hysteroscopic Polypectomy Prior to Infertility Treatment: A Cost Analysis and Systematic Review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 214, 106–110. [Google Scholar] [CrossRef]
- Bai, F.; Wan, Y.; Deng, Y.; Liu, M.; Chen, X.; Liu, Y.; Guo, Y. Research Progress of Endometrial Receptivity in Patients with Polycystic Ovary Syndrome: A Systematic Review. Reprod. Biol. Endocrinol. 2021, 19, 122. [Google Scholar] [CrossRef]
- Johnston-MacAnanny, E.B.; Hartnett, J.; Engmann, L.L.; Nulsen, J.C.; Sanders, M.M.; Benadiva, C.A. Chronic Endometritis Is a Frequent Finding in Women with Recurrent Implantation Failure After In Vitro Fertilization. Fertil. Steril. 2010, 93, 437–441. [Google Scholar] [CrossRef]
- Lessey, B.A.; Castelbaum, A.J.; Sawin, S.W.; Buck, C.A.; Schinnar, R.; Bilker, W.; Strom, B.L. Aberrant Integrin Expression in the Endometrium of Women with Endometriosis. J. Clin. Endocrinol. Metab. 1994, 79, 643–649. [Google Scholar] [CrossRef]
- Apparao, K.B.; Murray, M.J.; Fritz, M.A.; Meyer, W.R.; Chambers, A.F.; Truong, P.R.; Lessey, B.A. Osteopontin and Its Receptor Alphavbeta(3) Integrin Are Coexpressed in the Human Endometrium During the Menstrual Cycle but Regulated Differentially. J. Clin. Endocrinol. Metab. 2001, 86, 4991–5000. [Google Scholar] [CrossRef]
- Taylor, H.S.; Arici, A.; Olive, D.; Igarashi, P. HOXA10 Is Expressed in Response to Sex Steroids at the Time of Implantation in the Human Endometrium. J. Clin. Invest. 1998, 101, 1379–1384. [Google Scholar] [CrossRef]
- Pîrlog, L.M.; Pătrășcanu, A.A.; Ona, M.D.; Cătană, A.; Rotar, I.C. HOXA10 and HOXA11 in Human Endometrial Benign Disorders: Unraveling Molecular Pathways and Their Impact on Reproduction. Biomolecules 2025, 15, 563. [Google Scholar] [CrossRef] [PubMed]
- Daftary, G.S.; Troy, P.J.; Bagot, C.N.; Young, S.L.; Taylor, H.S. Direct Regulation of Beta3-Integrin Subunit Gene Expression by HOXA10 in Endometrial Cells. Mol. Endocrinol. 2002, 16, 571–579. [Google Scholar] [CrossRef]
- Ruiz-Alonso, M.; Blesa, D.; Díaz-Gimeno, P.; Gómez, E.; Fernández-Sánchez, M.; Carranza, F.; Carrera, J.; Vilella, F.; Pellicer, A.; Simón, C. The Endometrial Receptivity Array (ERA): High Diagnostic Performance in Infertile Patients. Fertil. Steril. 2013, 100, 1332–1339. [Google Scholar] [CrossRef]
- Nikas, G.; Develioglu, O.H.; Toner, J.P.; Jones, H.W. Endometrial Pinopodes Indicate a Shift in the Window of Receptivity in IVF Cycles. Hum. Reprod. 1999, 14, 787–792. [Google Scholar] [CrossRef] [PubMed]
- Maia, H.; Maltez, A.; Studart, E.; Athayde, C.; Coutinho, E.M. Effect of the Levonorgestrel-Releasing Intrauterine System on the Expression of Bcl-2 Family Proteins and Steroid Receptors in Endometrial Polyps. Fertil. Steril. 2008, 89, 1356–1362. [Google Scholar] [CrossRef]
- Gellersen, B.; Brosens, J.J. Cyclic Decidualization of the Human Endometrium in Reproductive Health and Failure. Endocr. Rev. 2014, 35, 851–905. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, T.; Yoshimura, Y. Molecular and Cellular Mechanisms for Differentiation and Regeneration of the Uterine Endometrium. Endocr. J. 2008, 55, 795–810. [Google Scholar] [CrossRef] [PubMed]
- Moffett, A.; Colucci, F. Uterine NK Cells: Active Regulators at the Maternal-Fetal Interface. J. Clin. Invest. 2014, 124, 1872–1879. [Google Scholar] [CrossRef]
- Kitaya, K.; Yasuo, T. Aberrant Expression of Selectin E, CXCL1, and CXCL13 in Chronic Endometritis. Mod. Pathol. 2010, 23, 1136–1146. [Google Scholar] [CrossRef]
- Tuckerman, E.; Mariee, N.; Prakash, A.; Li, T.C.; Laird, S. Uterine Natural Killer Cells in Peri-Implantation Endometrium from Women with Repeated Implantation Failure After IVF. J. Reprod. Immunol. 2010, 87, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Mor, G.; Cardenas, I.; Abrahams, V.; Guller, S. Inflammation and Pregnancy: The Role of the Immune System at the Implantation Site. Ann. N. Y. Acad. Sci. 2011, 1221, 80–87. [Google Scholar] [CrossRef]
- Goldstein, S.R. Saline Infusion Sonohysterography. Clin. Obstet. Gynecol. 1996, 39, 248–258. [Google Scholar] [CrossRef]
- Parsons, A.K.; Lense, J.J. Sonohysterography for Endometrial Abnormalities: Preliminary Results. J. Clin. Ultrasound 1993, 21, 87–95. [Google Scholar] [CrossRef]
- Dijkhuizen, F.P.; Brölmann, H.A.; Potters, A.E.; Bongers, M.Y.; Heinz, A.P. The Accuracy of Transvaginal Ultrasonography in the Diagnosis of Endometrial Abnormalities. Obstet. Gynecol. 1996, 87, 345–349. [Google Scholar] [CrossRef]
- Soares, S.R.; Barbosa dos Reis, M.M.; Camargos, A.F. Diagnostic Accuracy of Sonohysterography, Transvaginal Sonography, and Hysterosalpingography in Patients with Uterine Cavity Diseases. Fertil. Steril. 2000, 73, 406–411. [Google Scholar] [CrossRef]
- Ludwin, A.; Martins, W.P.; Ludwin, I. Evaluation of Uterine Cavity with Saline Contrast Sonohysterography for Diagnosing Endometrial Polyps: Systematic Review and Meta-Analysis. Ultrasound Obstet. Gynecol. 2020, 56, 851–860. [Google Scholar] [CrossRef]
- Salim, R.; Regan, L.; Woelfer, B.; Backos, M.; Jurkovic, D. A Comparative Study of the Morphology of Congenital Uterine Anomalies in Women with and Without a History of Recurrent First Trimester Miscarriage. Hum. Reprod. 2003, 18, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Exacoustos, C.; Zupi, E.; Amadio, A.; Amoroso, C.; Szabolcs, B.; Romanini, M.E.; Arduini, D. Recurrence of Endometrial Polyps After Hysteroscopic Polypectomy: A Long-Term Prospective Study. Am. J. Obstet. Gynecol. 2014, 211, 123.e1–123.e5. [Google Scholar] [CrossRef]
- Bettocchi, S.; Nappi, L.; Ceci, O.; Selvaggi, L. Office Hysteroscopy. Obstet. Gynecol. Clin. North Am. 2004, 31, 641–654. [Google Scholar] [CrossRef]
- Cooper, N.A.; Smith, P.; Khan, K.S.; Clark, T.J. Vaginoscopic Approach to Outpatient Hysteroscopy: A Systematic Review of the Effect on Pain. BJOG 2010, 117, 532–539. [Google Scholar] [CrossRef]
- Bettocchi, S.; Ceci, O.; Di Venere, R.; Pansini, M.V.; Pellegrino, A.; Marello, F.; Nappi, L. Advanced Operative Office Hysteroscopy Without Anaesthesia: Analysis of 501 Cases Treated with a 5 Fr. Bipolar Electrode. Hum. Reprod. 2002, 17, 2435–2438. [Google Scholar] [CrossRef]
- Cicinelli, E.; Parisi, C.; Galantino, P.; Pinto, V.; Barba, B.; Schonauer, S. Reliability, Feasibility, and Safety of Minihysteroscopy with a Vaginoscopic Approach: Experience with 6,000 Cases. Fertil. Steril. 2003, 80, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Cicinelli, E.; De Ziegler, D.; Nicoletti, R.; Colafiglio, G.; Saliani, N.; Resta, L.; Rizzi, D.; De Vito, D. Chronic Endometritis: Correlation Among Hysteroscopic, Histologic, and Bacteriologic Findings in a Prospective Trial with 2190 Consecutive Office Hysteroscopies. Fertil. Steril. 2008, 89, 677–684. [Google Scholar] [CrossRef]
- Cicinelli, E.; Matteo, M.; Tinelli, R.; Lepera, A.; Alfonso, R.; Indraccolo, U.; Marrocchella, S.; Greco, P.; Resta, L. Prevalence of Chronic Endometritis in Repeated Unexplained Implantation Failure and the IVF Success Rate After Antibiotic Therapy. Hum. Reprod. 2015, 30, 323–330. [Google Scholar] [CrossRef]
- Dueholm, M.; Lundorf, E.; Hansen, E.S.; Ledertoug, S.; Olesen, F. Accuracy of Magnetic Resonance Imaging and Transvaginal Ultrasonography in the Diagnosis, Mapping, and Measurement of Uterine Myomas. Am. J. Obstet. Gynecol. 2002, 186, 409–415. [Google Scholar] [CrossRef]
- Güven, M.A.; Bese, T.; Demirkiran, F.; Idil, M.; Mgoyi, A. Hydrosonography in Screening for Intracavitary Pathology in Infertile Women. Int. J. Gynaecol. Obstet. 2004, 86, 377–383. [Google Scholar] [CrossRef]
- Ayida, G.; Chamberlain, P.; Barlow, D.; Kennedy, S. Uterine Cavity Assessment Prior to In Vitro Fertilization: Comparison of Transvaginal Scanning, Saline Contrast Hysterosonography and Hysteroscopy. Ultrasound Obstet. Gynecol. 1997, 10, 59–62. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, Y.; Xue, Q.; Shang, J.; Yang, X.; Shan, C. Hysteroscopic Resection of Endometrial Polyps and Assisted Reproductive Technology Pregnancy Outcomes Compared with No Treatment: A Systematic Review. J. Minim. Invasive Gynecol. 2019, 26, 618–627. [Google Scholar] [CrossRef]
- Kalampokas, T.; Pandian, Z.; Keay, S.D.; Bhattacharya, S. Ultrasound Diagnosis of Endometrial Polyps: A Systematic Review. Ultrasound Obstet. Gynecol. 2012, 39, 630–638. [Google Scholar] [CrossRef]
- Lieng, M.; Qvigstad, E.; Sandvik, L.; Jorgensen, H.; Langebrekke, A.; Istre, O. Hysteroscopic Resection of Symptomatic and Asymptomatic Endometrial Polyps. J. Minim. Invasive Gynecol. 2007, 14, 189–194. [Google Scholar] [CrossRef]
- Nishioka, Y.; Morohashi, R.; Kuji, N. Pregnancy Rates After Hysteroscopic Endometrial Polypectomy Versus Endometrial Curettage Polypectomy: A Retrospective Study. Medicina 2023, 59, 1868. [Google Scholar] [CrossRef] [PubMed]
- Triantafyllidou, O.; Korompokis, I.; Chasiakou, S.; Tsonis, O.; Sioutis, D.; Siristatidis, C. Impact of Hysteroscopic Polypectomy on IVF Outcomes in Women with Unexplained Infertility. J. Clin. Med. 2024, 13, 4755. [Google Scholar] [CrossRef] [PubMed]
- Wen, W.; Tu, X.; Ma, Y.; Li, Y. Risk Factors and Assisted Reproductive Outcomes in Infertility Patients with Concomitant Endometrial Polyps. J. Army Med. Univ. 2024, 46, 886–893. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, X.; Chen, H.; Li, Y.; Peng, Y.; Wang, Q. Whether Hysteroscopy Improves Fertility Outcomes in Women Undergoing IVF/ICSI: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2024, 15, 1489783. [Google Scholar] [CrossRef] [PubMed]
- Dunn, R.C.; Lathi, R.B.; Westphal, L.M.; Milki, A.A. Is There Such a Thing as Too Early? Effect of Early Embryo Transfer After Hysteroscopic Polypectomy on Live Birth and Other Pregnancy Outcomes. Fertil. Steril. 2018, 110, 1316–1321. [Google Scholar] [CrossRef]
- Shohayeb, A.; El-Khayat, W. Does Timing of Frozen Embryo Transfer After Hysteroscopic Polypectomy Affect Pregnancy Outcomes? A Randomized Controlled Trial. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 101888. [Google Scholar] [CrossRef]
- Karayalcin, R.; Ozcan, S.; Moraloglu, O.; Ozyer, S.; Mollamahmutoglu, L.; Batioglu, S. Results of 2500 Office-Based Diagnostic Hysteroscopies Before IVF. Reprod. Biomed. Online 2010, 20, 689–693. [Google Scholar] [CrossRef]
- Wang, C.; Peng, Y.; Wang, Q.; Li, Y.; Liu, X.; Chen, H. No Differences in IVF Pregnancy Outcomes Following Hysteroscopic Polypectomy Using a Manual Hysteroscopic Tissue Removal Device Versus Conventional Resection. BMC Surg. 2025, 25, 128. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.W.; Hsu, W.C.; Chou, C.Y.; Chang, D.Y.; Huang, K.E. Pretreatment with Long-Acting Gonadotropin-Releasing Hormone Agonists Improved Pregnancy Outcomes After Hysteroscopic Multiple Polypectomies: A Retrospective Cohort Study. Taiwan. J. Obstet. Gynecol. 2024, 63, 229–233. [Google Scholar] [CrossRef]
- Mouhayar, Y.; Franasiak, J.M.; Sharara, F.I. Hysteroscopic Polypectomy Prior to Infertility Treatment: A Cost Analysis and Systematic Review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 214, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Kitaya, K.; Matsubayashi, H.; Takaya, Y.; Nishiyama, R.; Yamaguchi, K.; Takeuchi, T.; Ishikawa, T. Live Birth Rate Following Oral Antibiotic Treatment for Chronic Endometritis in Infertile Women with Repeated Implantation Failure. Am. J. Reprod. Immunol. 2017, 78, e12719. [Google Scholar] [CrossRef] [PubMed]
- McQueen, D.B.; Bernardi, L.A.; Stephenson, M.D. Chronic Endometritis in Women with Recurrent Early Pregnancy Loss and/or Fetal Demise. Fertil. Steril. 2014, 101, 1026–1030. [Google Scholar] [CrossRef]
- Crum, C.P.; Hornstein, M.D.; Nucci, M.R.; Mutter, G.L. Hertig and Beyond: A Systematic and Practical Approach to the Endometrial Biopsy. Adv. Anat. Pathol. 2003, 10, 301–318. [Google Scholar] [CrossRef]
- Kasius, J.C.; Fatemi, H.M.; Bourgain, C.; Sie-Go, D.M.; Eijkemans, R.J.; Fauser, B.C.; Devroey, P.; Broekmans, F.J. The Impact of Chronic Endometritis on Reproductive Outcome. Fertil. Steril. 2011, 96, 1451–1456. [Google Scholar] [CrossRef]
- Song, D.; Feng, X.; Zhang, Q.; Xia, E.; Xiao, Y.; Xie, W.; Li, T.C. Prevalence and Confounders of Chronic Endometritis in Premenopausal Women with Abnormal Bleeding or Reproductive Failure. Reprod. Biomed. Online 2018, 36, 78–83. [Google Scholar] [CrossRef]
- Bouet, P.E.; El Hachem, H.; Monceau, E.; Gariépy, G.; Kadoch, I.J.; Sylvestre, C. Chronic Endometritis in Women with Recurrent Pregnancy Loss and Recurrent Implantation Failure: Prevalence and Role of Office Hysteroscopy and Immunohistochemistry in Diagnosis. Fertil. Steril. 2016, 105, 106–110. [Google Scholar] [CrossRef]
- De Smet, S.; Mackens, S.; Blockeel, C.; Tournaye, H.; Forsyth, R. Development of a CD138-Based Histopathological Scoring System to Diagnose Chronic Endometritis. Hum. Reprod. 2024, 39, i687. [Google Scholar] [CrossRef]
- Herlihy, N.S.; Klimczak, A.M.; Titus, S.; Scott, C.; Hanson, B.M. The Role of Endometrial Staining for CD138 as a Marker of Chronic Endometritis in Predicting Live Birth. J. Assist. Reprod. Genet. 2022, 39, 303–309. [Google Scholar] [CrossRef]
- Liu, W.J.; Huang, J.; Sun, L.; Huang, L.; Zhang, Q. Effect of Performing a New Biopsy After Antibiotic Treatment on the Outcomes of Assisted Reproduction in Patients with Infertility and Chronic Endometritis. Reprod. Biomed. Online 2022, 45, 1035–1043. [Google Scholar] [CrossRef]
- Li, Y.; Yu, S.; Huang, C.; Lian, R.; Chen, C.; Liu, S.; Li, L.; Diao, L.; Zeng, Y. Evaluation of Peripheral and Uterine Immune Status of Chronic Endometritis in Patients with Recurrent Reproductive Failure. Fertil. Steril. 2020, 113, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Cicinelli, E.; Matteo, M.; Tinelli, R.; Pinto, V.; Marinaccio, M.; Indraccolo, U.; De Ziegler, D.; Resta, L. Chronic Endometritis Due to Common Bacteria Is Prevalent in Women with Recurrent Miscarriage as Confirmed by Improved Pregnancy Outcome After Antibiotic Treatment. Reprod. Sci. 2014, 21, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Moreno, I.; Cicinelli, E.; Garcia-Grau, I.; Gonzalez-Monfort, M.; Bau, D.; Vilella, F.; De Ziegler, D.; Resta, L.; Valbuena, D.; Simon, C. The Diagnosis of Chronic Endometritis in Infertile Asymptomatic Women: A Comparative Study of Histology, Microbial Cultures, Hysteroscopy, and Molecular Microbiology. Am. J. Obstet. Gynecol. 2018, 218, 602.e1–602.e16. [Google Scholar] [CrossRef] [PubMed]
- Luncan, M.; Huniadi, A.; Bimbo-Szuhai, E.; Botea, M.; Zaha, I. The Effectiveness of Intrauterine Antibiotic Infusion Versus Oral Antibiotic Therapy in the Treatment of Chronic Endometritis in Patients During IVF Procedures. BMC Womens Health 2022, 22, 528. [Google Scholar] [CrossRef]
- Vitagliano, A.; Saccardi, C.; Noventa, M.; Di Spiezio Sardo, A.; Saccone, G.; Cicinelli, E.; Pizzi, S.; Andrisani, A.; Litta, P.S. Effects of Chronic Endometritis Therapy on In Vitro Fertilization Outcome in Women with Repeated Implantation Failure: A Systematic Review and Meta-Analysis. Fertil. Steril. 2018, 110, 103–112. [Google Scholar] [CrossRef]
- Liu, J.; Liu, Z.; Liu, Y.; Cheng, L.; Yan, L. Impact of Antibiotic Treatment for Chronic Endometritis on Pregnancy Outcomes in Women with Reproductive Failures. Front. Med. 2022, 9, 980511. [Google Scholar] [CrossRef]
- Vitagliano, A.; Petre, G.C.; Francini-Pesenti, F.; De Toni, L.; Papaleo, E.; Viganò, P.; Di Nisio, A.; Foresta, C. Chronic Endometritis in Infertile Women: Impact of Untreated Disease, Plasma Cell Count and Antibiotic Therapy on IVF Outcome—A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 2250. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Pan, P.; Chen, X.; Li, L.; Li, Y.; Yang, D. Analysis of Pregnancy Outcomes in Patients with Recurrent Implantation Failure Complicated with Chronic Endometritis. Front. Cell Dev. Biol. 2023, 11, 1088586. [Google Scholar] [CrossRef]
- Zhang, Q.Y.; Yang, G.X.; Tan, J.F.; Xiong, Y.J.; Xu, Y. Antibiotic Cured Chronic Endometritis Remains a Risk Factor for Early Pregnancy Loss in the Subsequent Frozen-Warmed Euploid Embryo Transfer. Reprod. Biomed. Online 2023, 47, 103611. [Google Scholar] [CrossRef]
- DeWaay, D.J.; Syrop, C.H.; Nygaard, I.E.; Davis, W.A.; Van Voorhis, B.J. Natural History of Uterine Polyps and Leiomyomata. Obstet. Gynecol. 2002, 100, 3–7. [Google Scholar] [CrossRef]
- Lieng, M.; Istre, O.; Sandvik, L.; Qvigstad, E. Prevalence, 1-Year Regression Rate, and Clinical Significance of Asymptomatic Endometrial Polyps: Cross-Sectional Study. J. Minim. Invasive Gynecol. 2009, 16, 465–471. [Google Scholar] [CrossRef]
- Bosteels, J.; Weyers, S.; Puttemans, P.; Panayotidis, C.; Van Herendael, B.; Gomel, V.; Mol, B.W.; Mathieu, C.; D’Hooghe, T. The Effectiveness of Hysteroscopy in Improving Pregnancy Rates in Subfertile Women Without Other Gynaecological Symptoms: A Systematic Review. Hum. Reprod. Update 2010, 16, 1–11. [Google Scholar] [CrossRef]
- El-Toukhy, T.; Campo, R.; Khalaf, Y.; Tabanelli, C.; Gianaroli, L.; Gordts, S.S.; Gordts, S.; Mestdagh, G.; Mardesic, T.; Voboril, J.; et al. Hysteroscopy in Recurrent In-Vitro Fertilisation Failure (TROPHY): A Multicentre, Randomised Controlled Trial. Lancet 2016, 387, 2614–2621. [Google Scholar] [CrossRef]
- Jansen, F.W.; Vredevoogd, C.B.; van Ulzen, K.; Hermans, J.; Trimbos, J.B.; Trimbos-Kemper, T.C. Complications of Hysteroscopy: A Prospective, Multicenter Study. Obstet. Gynecol. 2000, 96, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Ben-Arie, A.; Goldchmit, C.; Laviv, Y.; Levy, R.; Caspi, B.; Huszar, M.; Dgani, R.; Hagay, Z. The Malignant Potential of Endometrial Polyps. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 115, 206–210. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Integrated pathophysiological mechanisms linking endometrial polyps to subfertility. The diagram illustrates multiple interconnected pathways by which endometrial polyps impair fertility, including: (1) mechanical interference with sperm transport and embryo implantation; (2) intrinsic molecular abnormalities including dysregulated Wnt signaling and vascular defects; (3) chronic inflammation with altered cytokine profiles; (4) impaired endometrial receptivity and HOXA gene dysregulation; and (5) disruption of the immune microenvironment and decidualization. These mechanisms act synergistically to reduce fertility potential.
Figure 1.
Integrated pathophysiological mechanisms linking endometrial polyps to subfertility. The diagram illustrates multiple interconnected pathways by which endometrial polyps impair fertility, including: (1) mechanical interference with sperm transport and embryo implantation; (2) intrinsic molecular abnormalities including dysregulated Wnt signaling and vascular defects; (3) chronic inflammation with altered cytokine profiles; (4) impaired endometrial receptivity and HOXA gene dysregulation; and (5) disruption of the immune microenvironment and decidualization. These mechanisms act synergistically to reduce fertility potential.

Table 1.
Summary of Key Studies on Endometrial Polyps and Fertility Outcomes.
| Study | Design | N | Intervention | Key Finding |
|---|---|---|---|---|
| Pérez-Medina 2005 [7] | RCT | 215 | Polypectomy vs. observation before IUI | PR 63.4% vs. 28.2% (RR 2.1, p < 0.001) |
| Triantafyllidou 2024 [36] | Retrospective cohort | 40 | Polypectomy in RIF patients | CPR 65% (26/40); total positive 72.5% (29/40) |
| Wang 2024 [38] | Meta-analysis | 11,887 | Hysteroscopy before IVF | CPR RR 1.34 (1.19–1.51); LBR RR 1.43 (1.21–1.69) |
| Nishioka 2023 [33] | Retrospective | 156 | Hysteroscopic vs. curettage polypectomy | PR 68.2% vs. 51.4% (OR 2.03) |
| Bougie 2024 [13] | Guideline (SOGC) | N/A | Polypectomy recommended for infertile women with polyps | Strong recommendation |
| Dunn 2018 [39] | Retrospective | 389 | Early vs. delayed ET after polypectomy | No difference in LBR |
| Tuncer 2025 [14] | Retrospective | 428 | Risk factors for recurrence | Recurrence rate 7.78% |
| Wang 2024 [35] | Retrospective | 186 | GnRH-a pretreatment | LBR 53.3% vs. 43.3% (OR 1.47) |
Abbreviations: RCT, randomized controlled trial; IUI, intrauterine insemination; PR, pregnancy rate; RR, relative risk; RIF, recurrent implantation failure; CPR, clinical pregnancy rate; IVF, in vitro fertilization; LBR, live birth rate; OR, odds ratio; CI, confidence interval; ET, embryo transfer; GnRH-a, gonadotropin-releasing hormone agonist; SOGC, Society of Obstetricians and Gynaecologists of Canada.
Table 2.
Diagnostic Test Characteristics for Endometrial Polyp Detection.
| Modality | Sensitivity (%) | Specificity (%) | Advantages | Limitations |
|---|---|---|---|---|
| 2D-TVS | 55–88 | 65–95 | Non-invasive, widely available, low cost | Operator dependent, limited in thick endometrium |
| 3D-TVS | 85–95 | 90–98 | Better cavity visualization, multiplanar imaging | Requires specialized equipment, higher cost |
| SIS | 87–94 | 81–94 | Improved accuracy over TVS, office-based | Requires fluid instillation, mild discomfort |
| Hysteroscopy | 92–100 | 75–94 | Gold standard, allows simultaneous treatment | Invasive, requires instrumentation |
| MRI | 80–90 | 85–95 | No radiation, excellent soft tissue contrast | High cost, limited availability, not first-line |
Abbreviations: 2D-TVS, two-dimensional transvaginal sonography; 3D-TVS, three-dimensional transvaginal sonography; SIS, saline infusion sonohysterography; MRI, magnetic resonance imaging.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



