Submitted:
24 March 2026
Posted:
25 March 2026
You are already at the latest version
Abstract
Cancer-related pain remains one of the most prevalent and distressing symptoms across the disease trajectory, significantly impairing function and quality of life. This narrative review examines contemporary approaches to cancer pain management within a palliative care framework, emphasizing the transition from opioid-centric strategies toward multimodal, patient-centered care. Although opioids remain essential for moderate to severe pain, their use is limited by adverse effects, dependence risk, and increasing regulatory and societal concerns. Cancer pain is heterogeneous, arising from tumor progression and treatment-related injury, underscoring the need for mechanism-based assessment to guide therapy. This review highlights the expanding role of adjuvant analgesics, including antidepressants, anticonvulsants, corticosteroids, bisphosphonates, and topical agents, within multimodal regimens designed to optimize analgesia while minimizing opioid exposure. Non-pharmacological and interdisciplinary interventions are emphasized as integral components of supportive and palliative care, addressing both physical and psychosocial suffering. Emerging therapies, including cannabinoids and gene-targeted approaches, are discussed in the context of evolving evidence and personalized medicine. A multidisciplinary, patient-centered framework that integrates pharmacologic and non-pharmacologic strategies is essential for improving symptom control, functional outcomes, and quality of life in patients with cancer.
Keywords:
cancer pain
; palliative care
; multimodal analgesia
; opioids
; adjuvant analgesics
; supportive oncology
; personalized medicine
1. Introduction
With a steadily increasing global incidence, cancer remains a leading cause of mortality worldwide. Among its many associated challenges, chronic pain is one of the most prevalent and debilitating symptoms, significantly impairing quality of life and potentially affecting treatment adherence and outcomes. Despite advances in oncology and pain management, cancer-related pain remains complex and often inadequately controlled. An estimated 51.9% of individuals with advanced or metastatic cancer experience moderate to severe pain [1]. Cancer-related pain arises from heterogeneous mechanisms, including tumor progression and treatment-induced neuropathies. Many patients rely on opioids, raising concerns regarding adverse effects and dependence [2]. These challenges underscore the need for more individualized, mechanism-based approaches to pain management.
This review offers a novel synthesis of cancer pain management by integrating mechanism-based pain classification with a multimodal, patient-centered treatment framework grounded in palliative care principles. Unlike traditional approaches that emphasize opioid-based algorithms, we highlight the transition toward individualized strategies that incorporate adjuvant pharmacologic therapies, non-pharmacologic interventions, and interdisciplinary care. In addition, this review uniquely contextualizes cancer pain management within the evolving landscape of the opioid crisis, healthcare disparities, and emerging precision medicine approaches, including pharmacogenomics and gene-targeted therapies. By bridging current clinical practice with future therapeutic directions, this work provides a comprehensive and forward-looking framework for optimizing pain control and quality of life in patients with cancer.
2. Common Cancers Associated with Pain
Cancer progression is frequently associated with the development of chronic pain, though its prevalence and characteristics vary by malignancy. Patients with lung cancer, breast cancer, and hematologic malignancies demonstrate particularly high pain burdens [3].
2.1. Lung Cancer
Lung cancer is among the most prevalent malignancies and a leading cause of cancer-related mortality [4]. Individuals with advanced-stage lung cancer often necessitate palliative care due to metastatic spread or progression of the primary tumor. Despite the utilization of diverse therapeutic modalities, opioid administration remains prevalent due to the inherent complexities of adequate pain control. In a cohort study by Potter et al. involving 32 lung cancer patients, 73% reported cancer-induced pain. In contrast, 11% attributed their pain to cancer treatment [5]. Cancer-related pain in lung cancer manifests as both acute pain and chronic pain syndromes, arising from several mechanisms. These include tumor infiltration into the chest wall and pleura, nerve compression resulting from tumor impingement on structures such as the brachial plexus, and skeletal pain secondary to bone metastases.
2.2. Breast Cancer
Although lung cancer is frequently linked to elevated incidences of chronic pain, patients with breast cancer also experience substantial pain attributable to malignancy and its associated therapeutic interventions. Multiple studies have investigated the prevalence and intensity of pain experienced by breast cancer survivors. For instance, a survey conducted by Hamood et al. with 305 breast cancer survivors found that 84% of participants reported experiencing moderate pain, while 97% experienced pain on one to three days per week or more. Furthermore, a significant proportion of patients reported pain-associated symptoms such as paresthesia, allodynia, and phantom sensations, underscoring the persistent and multifaceted nature of pain in breast cancer survivors [6]. Pain mechanisms in breast cancer include tumor infiltration into the chest wall, nerves, and lymph nodes, which can cause localized and neuropathic pain. Post-mastectomy pain syndrome, a common consequence of breast surgery, is characterized by chronic, burning pain localized to the chest or axillary region, attributed to nerve injury [7]. Additionally, bone metastases frequently contribute to skeletal pain, particularly in the spine, ribs, and pelvis, further complicating pain management in these patients [8].
2.3. Leukemia and Lymphoma
Pain has long been a neglected aspect in malignant hematology [9,10]. Most patients with hematologic malignancies experience a significant symptom burden, frequently including severe pain, typically present at disease onset. As Niscola et al. explained in their study, some patients report pain relief following the initiation of chemotherapeutic agents; however, survivors or those in advanced disease stages commonly complain of chronic pain due to treatment-related complications and the disease itself [11]. In patients with leukemia, bone pain may result from the expansion of bone marrow caused by the accumulation of abnormal white blood cells. Depending on the affected site, it can manifest as either sharp or dull discomfort [12]. The long bones of the legs and arms are common sites of this pain. Conversely, lymphoma typically presents as painless lymphadenopathy. In advanced stages, B symptoms, such as unexplained fever, significant weight loss, and drenching night sweats, may occur, mediated by pro-inflammatory cytokines [13]. Patients experience diverse pain types, including neuropathic, visceral, and somatic pain, which are crucial for effective management.
3. Pain Presentations
Cancer-related pain is typically classified into neuropathic, visceral, and somatic types, often coexisting within the same patient (Table 1). Gaining insight into how pain presents across various cancers is essential for developing effective pain management strategies.
Pain subtypes vary by cancer and may arise from tumor progression, metastasis, or treatment-related effects.
3.1. Neuropathic Pain
Neuropathic pain results from injury to the somatosensory system [14]. Most patients present with sensory deficits, burning sensations, allodynia, and spontaneous pain attacks [15]. Neuropathic pain can be either central or peripheral, depending on the origin of the neural lesion. Central neuropathic pain originates from disorders within the central nervous system, including the brain and spinal cord in conditions like stroke and Parkinson’s disease [16]. Conversely, the peripheral neuropathic pain predominantly involves abnormalities in peripheral afferent fibers, specifically small, unmyelinated C-fibers and myelinated A-fibers (Aβ and Aδ) [17]. Peripheral neuropathic pain is expected to become more prevalent due to the aging global population, rising cancer incidence, and the effects of chemotherapy, which impact various sensory nerve fibers (Aβ, Aδ, and C fibers) [18].
In cancer patients, the etiology of neuropathic pain is multifactorial: approximately two-thirds are directly tumor-related, 20% are treatment-induced, and 10-15% are attributable to comorbidities [19]. Neuropathic cancer pain can arise from direct infiltration of the peripheral or central nervous system by primary tumors or metastases. Examples of peripheral nervous system involvement include brachial plexus invasion by thoracic tumors and lumbosacral plexus invasion by abdominal or pelvic malignancies [20]. Radiation-induced neuropathy represents another significant pathway to chronic neuropathic pain, although its precise mechanisms remain incompletely elucidated. Proposed etiologies include nerve compression secondary to radiation-induced fibrosis and direct neural and microvascular injury resulting from alterations in the vasculature [21]. Radiation-induced neuropathy is classically exemplified by brachial plexopathy that develops after thoracic irradiation, often for lung or breast cancer [22].
3.2. Visceral Pain
Visceral pain arises when internal organs within the gastrointestinal or genitourinary systems are affected, including hollow organs, solid organs, the peritoneum, or tissues in the retroperitoneal space. It is commonly triggered by blockages in structures like the intestines, bile ducts, or ureters, leading to often diffuse pain. In women, reproductive physiology contributes to the addition of visceral pain throughout life [23]. Visceral pain in cancer presents with characteristics distinct from neuropathic pain. Tumor growth can generate multiple nociceptive stimuli that contribute to pain. These include the release of chemical substances by cancer and immune cells, physical pressure from tumor growth, blockages in hollow organs, and nerve-related changes such as loss of nerve supply, abnormal nerve growth, and altered nerve activity [23]. In hematologic malignancies, visceral compression due to enlarged lymph nodes and organomegaly, most commonly involving the spleen and/or liver, can lead to increased intra-abdominal pressure and associated discomfort [11].
3.3. Somatic Pain
Somatic pain is the most common type of pain observed in cancer patients, presenting as a dull, gnawing, pounding, or gripping discomfort [24]. Cutaneous somatic pain is typically sharp or burning and well-localized from lacerations. Conversely, deep somatic pain originates from joints, tendons, and bone metastasis, tends to be more diffuse, and is commonly characterized as throbbing or aching [23,25,26,27,28]. Somatic pain is the dominant pain subtype for lung and breast cancers due to bone metastasis. Hematologic malignancies present unique pain profiles due to bone marrow infiltration, skeletal involvement, and systemic symptoms. Among patients with hematological cancers, bone pain is one of the most significant forms of disease-related pain. It primarily arises from two key pathological mechanisms: the formation of osteolytic lesions and the infiltration of malignant cells into the bone marrow [9]. These bone lesions can cause constant nociceptive pain that may be localized or radiate to other areas, even during rest. The pain is often intensified by movement (incident pain) and may also include neuropathic characteristics, resulting in a mixed pain profile [11]. Currently, a hematologist in clinical practice can anticipate that chronic pain will be mentioned in approximately one out of every five patients [29]. Among patients undergoing active treatment, ongoing pain is observed in approximately 60%, and even during survivorship, persistent pain affects roughly 33% of individuals [30]. Importantly, pain in these patients may also be treatment-related, emerging postoperatively or as a side effect of chemotherapy or radiation therapy. Considering the substantial burden of chronic pain in cancer patients, particularly those with lung, breast, and hematological cancers, implementing effective pain management strategies is vital in optimizing clinical results and enhancing overall well-being.
4. Pain Therapies
4.1. Non-Pharmacological Approaches
Non-pharmacological interventions are essential in addressing the multidimensional nature of cancer-related pain. While chemotherapy, surgery, and radiation therapy are pivotal for cancer eradication, their capacity to improve a patient’s quality of life is frequently constrained. Cognitive behavioral therapy (CBT) is the most utilized psychological approach for managing chronic pain. This therapy emphasizes the interplay between psychological state, behaviors, and pain awareness. Patients are guided to explore their emotional responses to pain, develop methods for managing stress and calming practices, and build decision-making skills, and to practice these regularly. CBT highlights the impact of patients’ reactions to pain on how they perceive it and acknowledges the importance of their coping mechanisms in managing pain [31]. CBT specifically targets maladaptive beliefs surrounding pain and cancer, often leading to improved pain tolerance and emotional resilience [32]. CBT that incorporates imagery and hypnosis has shown the greatest potential to date in managing chronic pain associated with cancer. Patients are taught to use guided imagery to focus on a relaxing scene, diverting attention from pain. This intervention has displayed significant effectiveness in pediatric patients undergoing invasive procedures, including lumbar punctures and bone marrow aspirations [33], and has also been shown to aid in managing discomfort among females with advanced-stage breast cancer and individuals receiving stem cell transplants [34]. A randomized controlled trial (RCT) further supports the utility of CBT, imagery, and relaxation techniques in mitigating chemotherapy-associated side effects and pain [35].
Beyond established non-pharmacological interventions such as CBT and physical therapy, acupuncture has garnered increasing attention as a valuable complementary modality for managing cancer-related pain. Although many different studies have shown controversy towards this non-pharmacological method, several meta-analyses have demonstrated reductions in pain among patients receiving acupuncture. A meta-analysis evaluating acupuncture’s efficacy for various chronic pain conditions demonstrated statistically significant pain relief compared to both sham and no-acupuncture controls. Against sham acupuncture, reductions in pain scores were observed across several conditions, specifically: back and neck pain (0.23 SDs; 95% CI, 0.13-0.33), osteoarthritis (0.16 SDs; 95% CI, 0.07-0.25), and chronic headache (0.15 SDs; 95% CI, 0.07-0.24). When compared to no-acupuncture controls, the effect sizes were substantially larger: 0.55 SDs (95% CI, 0.51-0.58) for back and neck pain, 0.57 SDs (95% CI, 0.50-0.64) for osteoarthritis, and 0.42 SDs (95% CI, 0.37-0.46) for chronic headaches. These findings underscore acupuncture’s potential as a therapeutic intervention for chronic pain management [36]. These findings propose that acupuncture could function as a valuable adjunctive therapy to conventional analgesics, potentially contributing to enhanced symptom control and improved patient well-being for cancer patients.
4.2. Pharmacological Approaches
Pharmacological approaches represent the most widely adopted strategy for managing cancer-related pain. This method advocates for the judicious use of nonopioid, opioid, and adjuvant analgesics, which can be administered as monotherapy or in combination. Dosing regimens are carefully titrated to each patient’s individual needs to optimize efficacy while minimizing adverse effects [37]. Opioids remain central to the management of moderate to severe cancer pain due to their potent analgesic effects. Common agents include morphine, oxycodone, fentanyl, methadone, and hydromorphone [38,39,40]. However, their use is limited by adverse effects, including gastrointestinal, neurological, and respiratory complications [41]. Long-term opioid therapy is associated with risks such as dependence, overdose, and opioid-induced hyperalgesia, necessitating careful patient selection and monitoring. These risks are dose-dependent, with higher doses associated with increased morbidity [42]. Despite these concerns, opioids remain appropriate, particularly in advanced disease, where the primary goal is symptom relief and quality of life. In this context, the focus shifts from long-term risk mitigation to effective pain control and patient comfort.
Heightened awareness of opioid misuse, coupled with public scrutiny, social stigma, and increased regulatory oversight, has created substantial barriers for patients who legitimately require opioids for cancer-related pain. Investigations consistently reveal patients’ narratives detailing the adverse effects of the opioid crisis on their capacity to manage pain effectively. The prevailing media representation, in conjunction with personal and collective experiences, has engendered significant stigma, apprehension, and self-reproach concerning opioid utilization. As a result, numerous individuals postpone the initiation of opioid regimens and perceive the choice to commence opioid pharmacotherapy as a profound personal or ethical shortcoming, frequently expressing this as “caving in”[43]. Other challenges in opioid utilization and effective cancer pain management include a desire to avoid potential side effects, fatalistic attitudes regarding pain control, fear of addiction, and existing informational deficits concerning appropriate opioid therapy [44].
Not only is prescribing controversy a considerable issue, but studies have also shown that disparities in pain treatment persist across racial and socioeconomic lines. In a survey by Ezenwa et. al., the Pain Management Composite Score and Health Surveys were used. A statistically significant difference emerged in pain management composite scores between African American and Caucasian patients. After accounting for age, gender, income, education, and disability, African Americans reported notably worse pain management outcomes than Caucasians on pain management composite scores SHARP [X2(1, N = 890) = 38.94, p < .001, Squared Partial Correlation Coefficient = .04]. This disparity suggests that African Americans reported less effective pain management compared to Caucasians [45]. African American patients not only reported worse pain management experiences but also had lower overall quality of life scores, underscoring the urgent need to address systemic inequities in cancer care.
5. Adjuvant Analgesics and Multimodal Strategies in Cancer Pain Management
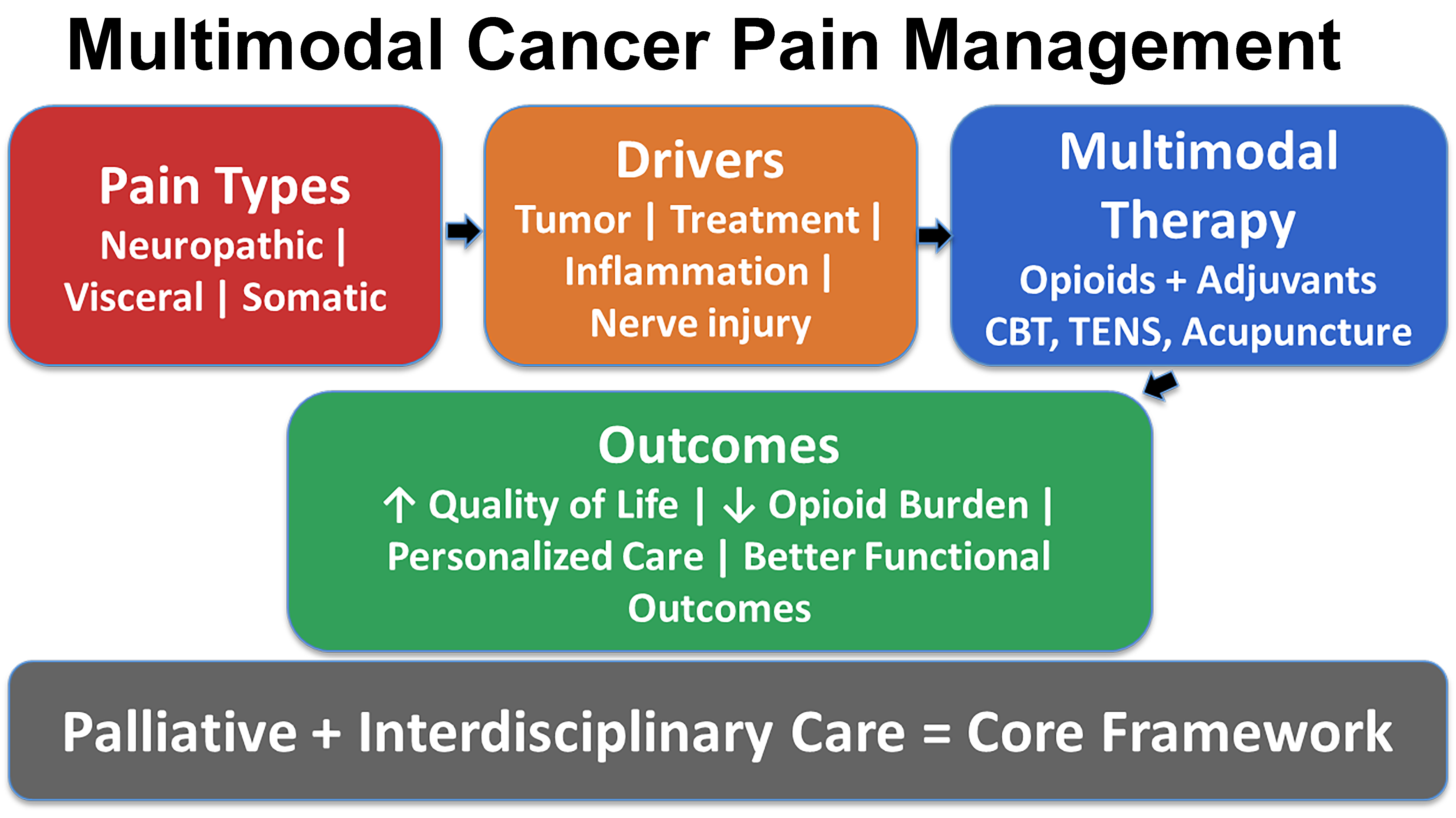
In the last couple of years, the incorporation of adjuvant analgesics and multimodal techniques has emerged as a potential approach to enhance pain control, reduce opioid dependency, and tailor treatment to neuropathic, bone, or inflammatory pain syndromes. (Figure 1)
In the context of cancer, where pain often arises from multifactorial causes, targeted pharmacologic approaches are crucial in managing diverse pain syndromes. Adjuvant analgesics are medications that were not initially developed to treat pain, but they have been shown to possess pain-relieving properties in certain conditions [46]. When administered alone, these agents typically exhibit little or no analgesic activity but can significantly enhance their effects when combined with conventional analgesics [47]. These medications are generally used when pain does not respond to standard treatments. However, in particular chronic pain conditions, they may be considered as an initial treatment option [48]. The role of adjuvant analgesics is multifaceted. They can increase the therapeutic index of opioids by enabling lower dosing, providing analgesic effects where opioids are insufficient, and mitigating some opioid-related side effects. Due to these benefits, they’re often an important part of personalized pain management, especially in patients who can’t tolerate high doses of opioids or in whom opioids are not the best option [49]. The World Health Organization’s (WHO) guidelines on cancer pain management recommend the use of adjuvant medicines, including steroids, antidepressants, and anticonvulsants, to heighten the impact of opioids and NSAIDs and to manage specific pain syndromes [50]. These adjuvant therapeutic analgesics can alleviate bone-related, inflammatory-related, and neuropathic pain states.
5.1. Anticonvulsants
Neuropathic pain, regardless of the origin, is best described due to increased nerve activity in injured neural circuits. This hyperexcitability and the associated molecular changes closely resemble those observed in particular types of epilepsy, which has prompted the repurposing of anticonvulsant medications for neuropathic pain management [51]. Drugs such as gabapentin and pregabalin are commonly prescribed to manage neuropathic pain, especially when it results from nerve compression or side effects of chemotherapy [52]. Gabapentin is particularly effective in relieving neuropathic pain, especially in cases such as painful diabetic neuropathy and postherpetic neuralgia. Given its proven efficacy and favorable side effect profile, it is often regarded as a first-line treatment option for managing neuropathic pain [53]. The gabapentinoids, initially developed as analogs of GABA, bind to the α2δ-1 and α2δ-2 auxiliary subunits of calcium channels [54], therefore leading to a decrease in the release of stimulating neurotransmitters, and helps calm overactive nerve activity. These drugs are usually well tolerated, with dizziness and drowsiness being the most frequently reported side effects.
5.2. Antidepressants
Tricyclic antidepressants (TCAs), such as imipramine, amitriptyline, and clomipramine, are especially effective in neuropathic pain due to their dual inhibition of serotonin and norepinephrine reuptake. Their serotonin reuptake inhibition is primarily due to the parent compounds, while the norepinephrine reuptake effects are largely mediated by their active metabolites, nortriptyline, desipramine, and desmethylclomipramine. Notably, nortriptyline and desipramine are also used independently as TCAs, and along with maprotiline, they primarily target norepinephrine reuptake [55]. Evidence supports the efficacy of TCAs in treating a variety of peripheral pain syndromes involving nerve damage, including painful diabetic and non-diabetic polyneuropathies, postherpetic neuralgia, and postmastectomy pain syndrome [55]. Additionally, serotonin-norepinephrine reuptake inhibitors (SNRI) like duloxetine are commonly used for chemotherapy-induced peripheral neuropathy and are often preferred because they tend to cause fewer or milder side effects than tricyclic antidepressants [52]. Given their well-established efficacy in treating various neuropathic pain syndromes, both TCA and SNRIs remain valuable components of cancer pain management, particularly in patients experiencing nerve damage from chemotherapy, surgery, or tumor infiltration.
5.3. Corticosteroids
Corticosteroids are frequently prescribed in palliative care settings for individuals with cancer [56]. In a Canadian study involving outpatient palliative care cancer patients, 40% were found to be using corticosteroids, with dexamethasone being the most frequently prescribed by palliative care providers [57]. By interfering with key biochemical and cellular pathways involved in inflammation and immune responses, corticosteroids (CS) exert anti-inflammatory, anticancer, and immunosuppressive effects. One of their actions includes increasing annexin A1 levels, which leads to suppression of phospholipase A2 (PLA2) activity and a reduction in prostaglandin and leukotriene production. They also help control inflammation by lowering cyclooxygenase-2 (COX-2) expression and restricting neutrophil movement to inflamed tissues [58]. The most common types of corticosteroids are dexamethasone and prednisone, which are broadly used in cancer pain for their anti-inflammatory and edema-reducing effects. Corticosteroids help control pain resulting from tumor-induced inflammation due to their anti-inflammatory action. They are also utilized in treating cancer-related conditions such as spinal cord compression and metastases to the brain [59]. Corticosteroids have other beneficial effects, such as increased appetite, general well-being, and social interaction [60]. While effective for systemic inflammation and deep tissue pain, corticosteroids may be less suitable for localized pain, such as that affecting the skin or peripheral nerves, where topical agents can offer more targeted relief with fewer systemic effects.
5.4. Topical Agents
Topical analgesics offer a localized approach to pain management, which is particularly useful for patients experiencing focal neuropathic pain where systemic medication may not be necessary or tolerated. Survey data indicate that over a quarter of physicians utilize compounded topical formulations as pain management strategies. Notably, approximately 43% of patients demonstrated favorable outcomes with these treatments, which were associated with a low incidence of adverse effects [61]. When applied to the skin, topical agents can achieve adequate drug levels in the targeted tissues while minimizing systemic absorption, resulting in relatively low plasma concentrations [62]. Keratinocytes, making up approximately 90% of the epidermal cell population, represent a primary target for topical pain-relieving agents. Although typically classified as non-excitable cells, keratinocytes play a significant role in mediating cutaneous responses. Keratinocytes play a key role by releasing substances that activate pain nerves when injured. Injury to peripheral tissues stimulates keratinocytes and dermal blood vessels to release excitatory mediators, such as substance P, calcitonin gene-related peptide (CGRP), and prostaglandins, which interact with receptors on nociceptive neurons, leading to their depolarization [63].
Lidocaine acts as a non-selective blocker of voltage-gated sodium channels, interfering with the initiation and transmission of nerve signals. It stabilizes neuronal membranes, helping suppress abnormal activity in damaged sensory neurons. Its analgesic effects may also involve modulation of keratinocytes and immune cells and interaction with irritant receptors such as TRPV1 and TRPA1 [64]. In addition to lidocaine patches, capsaicin-based treatments are also utilized for managing localized pain. Low-concentration capsaicin creams, which require regular daily application, have demonstrated modest yet reproducible analgesic benefits, as supported by multiple meta-analyses. More recently, a high-concentration capsaicin 8% patch, Qutenza™, has gained approval in both the United States and the European Union. This formulation offers several advantages, including a longer-lasting analgesic effect, improved patient adherence, and a low likelihood of causing widespread side effects or interacting with other medications. The analgesic mechanism of capsaicin is primarily attributed to the depletion of substance P, a neuropeptide integral to the transmission of nociceptive signals, within primary afferent neurons [65]. In cancer patients, topical agents may be particularly valuable for managing focal pain syndromes such as post-surgical neuropathy or chemotherapy-induced dermal pain, offering relief without the burden of systemic side effects.
6. Multimodal Pain Management
Multimodal pain management integrates therapies targeting different biological pathways to enhance analgesic efficacy. Combining pharmacologic agents, such as opioids with antidepressants or anticonvulsants, with non-pharmacological interventions can produce synergistic effects while reducing opioid requirements.[66]. For example, pairing a low-dose opioid with a TCA or anticonvulsant could create an intense relief that specific cancer pains give, more potent than with one drug alone, while also achieving it with a lower opioid dose. This strategy has significantly improved contemporary cancer pain management by enhancing analgesia while reducing opioid requirements.
In addition to pharmacologic strategies, non-pharmacologic interventions, such as CBT and various other techniques, are integral to multimodal pain management. Non-invasive, non-drug interventions (NINPT) provide effective and safe methods for managing chronic pain, minimizing tissue damage, and reducing the risk of major side effects [67]. Techniques such as transcutaneous electrical nerve stimulation (TENS), thermal therapies including heat and cold applications, and massage are designed to influence chronic pain signaling by engaging underlying physiological processes [68,69]. Interventions grounded in psychological frameworks, including mindfulness-based stress reduction and CBT, have demonstrated effectiveness in reducing pain perception and improving coping mechanisms in patients with chronic conditions [70,71]. Collectively, these multimodal strategies not only address physical pain but also help manage the emotional and psychosocial dimensions of suffering. The multimodal approach allows for a customized approach that aligns with the individual’s specific pain patterns and the nature of their illness.
6.1. Palliative Care and Interdisciplinary Approaches to Cancer Pain
An essential yet sometimes underutilized component of multimodal cancer pain management is the early integration of palliative care. Palliative care aims to enhance a patient’s overall well-being by alleviating distressing symptoms, providing psychosocial support, and facilitating goal-oriented communication. Pain is often the most distressing symptom managed by palliative teams, and their involvement has been associated with improved symptom control, reduced hospital admissions, and even increased survival in some cases [72,73]. The interdisciplinary nature of palliative care teams, typically comprising physicians, nurses, psychologists, social workers, chaplains, and pharmacists, allows for a multidimensional approach to pain management. This team-based structure is particularly beneficial in addressing the complex interaction between emotional, physical, spiritual, and societal aspects of cancer-related pain [74].
Despite these benefits, significant gaps remain in the consistent and timely delivery of palliative care services. The American Society of Clinical Oncology (ASCO) has released guidelines that underscore the value of a multidisciplinary palliative care approach in advanced cancer, highlighting its contributions to effective pain management, enhanced quality of life, and comprehensive symptom control [75]. Moreover, hospice services, which fall under the broader umbrella of palliative care, play a critical role in managing refractory pain at the end of life. Hospice services frequently employ individualized pain management plans and continuous infusions to ensure optimal comfort during the final stages of illness [76]. Incorporating palliative care into cancer pain management enhances patient-centered outcomes and exemplifies a shift toward a holistic, multidisciplinary approach that prioritizes both longevity and quality of life.
7. Controversies and Evolving Paradigms in Cancer Pain Management
Cancer pain management, while guided by established protocols, is a dynamic field marked by ongoing debates and evolving perspectives. These controversies have a significant impact on contemporary clinical practice and research directions. The most prominent and enduring controversy in cancer pain management centers on the use of opioids. While these agents have historically been considered the “gold standard” for moderate to severe cancer pain due to their unparalleled efficacy, the broader opioid crisis has profoundly reshaped prescribing behaviors within oncology [77,78]. A significant concern is the societal stigma associated with opioid use, which creates substantial barriers for cancer patients who genuinely require these medications. Patients often express apprehension about initiating opioid regimens, viewing the decision to start opioid pharmacotherapy as a personal or ethical failing. This stigma, exacerbated by media portrayals and personal experiences, can lead to self-reproach and a reluctance to seek adequate pain relief [79,80]. Clinicians, in turn, frequently navigate an ethical tension between their duty to alleviate suffering and the imperative for cautious prescribing [81,82,83]. Furthermore, while the therapeutic goal in advanced or terminal disease stages often shifts towards prioritizing symptom control and maximizing patient comfort, the dose-response relationship with adverse outcomes, including overdose and substance use disorder, necessitates careful titration [84,85]. Compounding these issues are persistent disparities in pain treatment across racial and socioeconomic lines. Studies indicate that minority patients, such as African Americans and Hispanics, are less likely to receive appropriate opioid therapy and specialist referrals compared to White patients, highlighting a systemic inequity that complicates the ethical landscape of pain management [86,87].
Beyond pharmacological interventions, the role and integration of non-pharmacological approaches also present areas of discussion. There is a growing consensus that pharmacological analgesia alone is often insufficient, with debilitating adverse effects frequently hindering patient tolerance and adherence [88]. This limitation underscores the critical need for effective non-pharmacological alternatives. While CBT is widely accepted and well-supported by evidence for managing chronic pain in cancer patients, the efficacy and widespread acceptance of other complementary modalities, such as acupuncture, can be more controversial. Although some systematic reviews and meta-analyses suggest that acupuncture can significantly reduce cancer-related pain and decrease analgesic intake [89,90], its integration into mainstream oncology practice varies. This variability is often influenced by factors such as the specific needling technique, the number of needles used, the duration of sessions, and patient-specific psychological factors [89].
The development of novel and emerging therapies introduces new schools of thought and practical considerations. Cannabinoid-based therapies have garnered increasing interest for their potential role in cancer-related pain management, with some cannabinoid receptor agonists already approved for specific cancer-related symptoms [91]. However, their broader application for pain management remains a subject of debate, with a recognized need for expanded evidence from robust, long-term clinical studies to establish optimal dosing, effectiveness, and safety profiles in oncology populations [91,92]. Similarly, gene-targeted therapies represent a promising future direction, aiming for more precise and individualized pain management by targeting specific pain pathways and considering genetic variations [93]. These therapies offer the potential to overcome limitations of traditional agents, such as a lack of anatomical specificity and off-target effects. Nevertheless, these approaches are essentially in preclinical stages, and significant challenges related to safety, tissue-targeted delivery, and immunogenicity must be addressed before they can achieve widespread clinical feasibility, positioning their current role as more aspirational than immediately practical.
8. Emerging Therapies and Future Directions in the Field
Several promising developments in oncology and pain management research aim to enhance analgesic effectiveness, reduce the risk of opioid-related complications, and offer new hope for patients with treatment-resistant cancer pain. These future directions have the potential to significantly improve cancer pain management and patient quality of life, driven by advancements in personalized medicine, innovative pharmacological targets, and integrated models.
8.1. Cannabinoids
Cannabinoid-based therapies, particularly those involving tetrahydrocannabinol (THC), have garnered increasing interest in their role in cancer-related pain management. A growing proportion of patients are using cannabis and cannabinoid-based therapies to address both palliative and non-palliative cancer-related pain, as well as other associated symptoms [94]. The endogenous cannabinoid system (ECS), which regulates various physiological processes, including pain perception, inflammatory responses, appetite control, energy regulation, cognitive functions like memory and attention, and reward pathways, is the primary mechanism through which THC produces its effects [95]. Currently, two cannabinoid receptor agonists, THC and nabilone, are approved for clinical use in managing chemotherapy-induced nausea and vomiting in cancer patients, and for increasing appetite in individuals with AIDS-related cachexia [95]. Recent studies have suggested that standardized, pharmaceutical-grade formulations could be integrated into cancer pain protocols, offering potential opioid sparing effects and addressing symptoms beyond pain, such as nausea and cachexia [131,13]. Clinical trials that rigorously assess long-term efficacy, optimal dosing, and safety profiles are essential for facilitating wider acceptance in oncology practice.
8.2. Gene-Targeted Therapies
Gene-targeted therapies represent a long-anticipated advancement in cancer pain control. As genomic medicine advances, its promise to transform the understanding and management of cancer-associated pain is becoming increasingly recognized. Traditional pharmacological agents often lack anatomical specificity and can cause off-target effects, sometimes creating new sources of discomfort for patients [96]. These challenges underscore the pressing demand for more precise and individualized treatment modalities. A primary focus of innovation is the advancement of precision pain management strategies. Advancements in genomics and molecular profiling are anticipated to allow clinicians to predict opioid responsiveness, individual pain susceptibility, and risks of adverse events, thereby creating a personalized analgesic regimen [97]. Various gene delivery systems have been investigated in preclinical models for targeting pain pathways. Gene delivery to sensory neurons implicated in pain transmission has shown potential using viral vectors such as adenovirus (Ad), adeno-associated virus (AAV), lentivirus, and herpes simplex virus (HSV) [96]. Non-viral methods are also being explored, including lipid nanoparticles, polymer carriers, and other nanotechnologies. Each platform offers distinct advantages and challenges in terms of safety, tissue-targeted delivery, immunogenicity, and clinical feasibility [98]. Concurrently, advances in gene-based research have enabled a more individualized approach to pain management by investigating SNPs linked to the metabolic processing of opioids (e.g., CYP2D6), pain sensitivity (e.g., COMT), and inflammatory responses. Pharmacogenomic markers, such as CYP2D6 and COMT polymorphisms, have already demonstrated significant potential for guiding dosing and selection; however, additional validation through large-scale studies is necessary before their broad clinical implementation [99]. This expanding study area allows for the development of personalized analgesic regimens tailored to a patient’s genetic makeup. In the future, identifying such genetic profiles may help clinicians predict treatment response, minimize adverse effects, and optimize pain control strategies [98].
8.3. Novel Non-Opioid Analgesics and Molecular Targets
Several novel non-opioid analgesics targeting alternative molecular pathways, including transient receptor potential (TRP) channels, neuroimmune interactions, and sodium channels, are currently in preclinical and early clinical development [100]. Early research efforts primarily centered on TRP channels found in pain-sensing neurons. Several potent small-molecule inhibitors targeting TRPV1, TRPV3, and TRPA1 have already advanced into clinical trials as potential new analgesics. More recently, there has been a notable increase in research expanding TRP channel-targeted therapies to additional conditions, including cancer, asthma, metabolic disorders, and many more. Gaining deeper insights into the roles of TRP channels in both normal physiology and disease states may ultimately enable the development of groundbreaking drugs for these challenging medical conditions [101].
8.4. Integrative and Technological Approaches to Cancer Pain Care
Future models of cancer pain care will increasingly emphasize comprehensive multimodal approaches that integrate rehabilitative, pharmacological, and psychological interventions. The utilization of telemedicine platforms, digital health tools, and wearable biosensors is expected to improve real-time symptom monitoring, enhance patient engagement and adherence, and facilitate individualized treatment adjustments [102,103]. All of these advancements, combined with the early and systematic integration of palliative care, point to a transformative shift toward more precise, equitable, and holistic cancer pain management strategies, with the potential for significantly improved quality of life and patient-centered outcomes.
9. Current Research Gaps
Despite significant advancements in cancer pain management, there are still critical research gaps that limit the optimal, personalized care that patients desire. First, the understanding of the mechanisms behind cancer pain subcategories, such as neuropathic, visceral, and somatic pain, is still insufficient. Moreover, the interaction between tumor-related, treatment-induced, and patient-specific genetic variables remains incompletely understood. The variability of pain sensations among individuals suffering from similar malignancies suggests underlying molecular and neuroimmune variations that warrant further exploration [19,20,96].
Although emerging therapies such as cannabinoid-based treatments and gene-targeted approaches are promising [92,93], there has not been enough clinical evidence to support the long-term effectiveness, optimal dosing, and safety profiles of these innovative treatments [104]. There is also a lack of standardized methodology that needs to be addressed. Rigorous clinical trials are essential for developing standardized, evidence-based protocols tailored to specific pain mechanisms and individual patient profiles. Many patients getting care outside of specialist cancer clinics continue to experience insufficient pain control, and a large number do not obtain appropriate analgesics while enduring moderate to severe pain [105]. The lack of standardized, widely accepted pain assessment tools hampers pain management, making it difficult to establish consistent, evidence-based guidelines across different care environments [106]. Addressing these barriers will require enhanced resources, improved communication technologies, and better assessment methods to support equitable and effective pain management.
Finally, numerous advances in genomics and molecular profiling have identified genetic polymorphisms associated with opioid metabolism and pain sensitivity (e.g., CYP2D6 and COMT); however, these findings have yet to be fully integrated into clinical practice. This rapidly expanding field calls for careful consideration and monitoring by clinicians to ensure that key findings with clinical implications are accessible, interpretable, and effectively communicated. Additional translational research is required to confirm these markers and establish practical guidelines for individualized pain management [38,98].
10. Conclusions
Cancer-related pain remains one of the most complex and burdensome symptoms experienced by patients, often significantly diminishing quality of life. Malignancies such as lung cancer, breast cancer, and hematologic cancers are frequently associated with substantial pain burden arising from both disease progression and treatment-related complications. These conditions often present with neuropathic, visceral, and somatic pain phenotypes, each requiring mechanism-specific management. While opioids remain a cornerstone of treatment, their limitations, including adverse effects, misuse potential, and societal stigma, underscore the need for broader, individualized strategies. Adjuvant analgesics, topical agents, and non-pharmacological interventions expand the therapeutic landscape, enabling more precise and multimodal approaches to pain control.
Emerging therapies, including cannabinoid-based treatments and gene-targeted strategies, offer promise for more personalized and effective pain management, particularly in refractory cases. Advancing cancer pain management will require continued integration of multidisciplinary care, evidence-based innovation, and patient-centered approaches. Addressing pain as a central component of oncology care is essential to improving both clinical outcomes and quality of life.
Funding
This work was supported by the National Institute of Drug Abuse (primary), National Institute of Allergy and Infectious Diseases, National Institute of Dental & Craniofacial Research, National Institute of Neurological Disorders and Stroke, and National Institute of Aging to SA (R01DA049657).
Conflicts of Interest statement
The authors have declared no conflict of interest.
References
- Colosia, A., et al., The Burden of Metastatic Cancer-Induced Bone Pain: A Narrative Review. J Pain Res, 2022. 15: p. 3399-3412. [CrossRef]
- Kaye, A.D., et al., Prescription Opioid Abuse in Chronic Pain: An Updated Review of Opioid Abuse Predictors and Strategies to Curb Opioid Abuse: Part 1. Pain Physician, 2017. 20(2S): p. S93-S109.
- Gallaway, M.S., et al., Pain Among Cancer Survivors. Prev Chronic Dis, 2020. 17: p. E54. [CrossRef]
- Marchevsky, A.M., et al., The differential diagnosis between pleural sarcomatoid mesothelioma and spindle cell/pleomorphic (sarcomatoid) carcinomas of the lung: evidence-based guidelines from the International Mesothelioma Panel and the MESOPATH National Reference Center. Hum Pathol, 2017. 67: p. 160-168. [CrossRef]
- Potter, J. and I.J. Higginson, Pain experienced by lung cancer patients: a review of prevalence, causes and pathophysiology. Lung Cancer, 2004. 43(3): p. 247-57. [CrossRef]
- Hamood, R., et al., Chronic pain and other symptoms among breast cancer survivors: prevalence, predictors, and effects on quality of life. Breast Cancer Res Treat, 2018. 167(1): p. 157-169. [CrossRef]
- Smith, W.C., et al., A retrospective cohort study of post mastectomy pain syndrome. Pain, 1999. 83(1): p. 91-5.
- Parkes, A., et al., Prognostic Factors in Patients with Metastatic Breast Cancer with Bone-Only Metastases. Oncologist, 2018. 23(11): p. 1282-1288. [CrossRef]
- Niscola, P., et al., Pain syndromes in haematological malignancies: an overview. Hematol J, 2004. 5(4): p. 293-303. [CrossRef]
- Niscola, P., Effective pain management in hematological malignancies. Expert Rev Hematol, 2009. 2(3): p. 219-22. [CrossRef]
- Niscola, P., et al., Pain in blood cancers. Indian J Palliat Care, 2011. 17(3): p. 175-83. [CrossRef]
- Maman, E., et al., Acute lymphoblastic leukemia in children: correlation of musculoskeletal manifestations and immunophenotypes. J Child Orthop, 2007. 1(1): p. 63-8. [CrossRef]
- Lewis, W.D., S. Lilly, and K.L. Jones, Lymphoma: Diagnosis and Treatment. Am Fam Physician, 2020. 101(1): p. 34-41.
- Finnerup, N.B., R. Kuner, and T.S. Jensen, Neuropathic Pain: From Mechanisms to Treatment. Physiol Rev, 2021. 101(1): p. 259-301.
- Campbell, J.N. and R.A. Meyer, Mechanisms of neuropathic pain. Neuron, 2006. 52(1): p. 77-92.
- Borsook, D., Neurological diseases and pain. Brain, 2012. 135(Pt 2): p. 320-44. [CrossRef]
- Finnerup, N.B., et al., Neuropathic pain: an updated grading system for research and clinical practice. Pain, 2016. 157(8): p. 1599-1606. [CrossRef]
- Colloca, L., et al., Neuropathic pain. Nat Rev Dis Primers, 2017. 3: p. 17002.
- Bennett, M.I., et al., Prevalence and aetiology of neuropathic pain in cancer patients: a systematic review. Pain, 2012. 153(2): p. 359-365. [CrossRef]
- Edwards, H.L., M.R. Mulvey, and M.I. Bennett, Cancer-Related Neuropathic Pain. Cancers (Basel), 2019. 11(3).
- Delanian, S., J.L. Lefaix, and P.F. Pradat, Radiation-induced neuropathy in cancer survivors. Radiother Oncol, 2012. 105(3): p. 273-82. [CrossRef]
- Fathers, E., et al., Radiation-induced brachial plexopathy in women treated for carcinoma of the breast. Clin Rehabil, 2002. 16(2): p. 160-5. [CrossRef]
- Sikandar, S. and A.H. Dickenson, Visceral pain: the ins and outs, the ups and downs. Curr Opin Support Palliat Care, 2012. 6(1): p. 17-26.
- AC., C. and F. KM., Types of Pain. 6th edition ed. Holland-Frei Cancer Medicine, ed. K. DW, et al. 2003, Hamilton (ON): BC Decker.
- Raffaeli, W. and E. Arnaudo, Pain as a disease: an overview. J Pain Res, 2017. 10: p. 2003-2008. [CrossRef]
- Loeser, J.D. and R. Melzack, Pain: an overview. Lancet, 1999. 353(9164): p. 1607-9.
- Basbaum, A.I., et al., Cellular and molecular mechanisms of pain. Cell, 2009. 139(2): p. 267-84.
- Venkatachalam, K. and C. Montell, TRP channels. Annu Rev Biochem, 2007. 76: p. 387-417.
- Dahlhamer, J., et al., Prevalence of Chronic Pain and High-Impact Chronic Pain Among Adults—United States, 2016. MMWR Morb Mortal Wkly Rep, 2018. 67(36): p. 1001-1006. [CrossRef]
- van den Beuken-van Everdingen, M.H., et al., Prevalence of pain in patients with cancer: a systematic review of the past 40 years. Ann Oncol, 2007. 18(9): p. 1437-49. [CrossRef]
- Singh, P. and A. Chaturvedi, Complementary and alternative medicine in cancer pain management: a systematic review. Indian J Palliat Care, 2015. 21(1): p. 105-15. [CrossRef]
- Keefe, F.J., A.P. Abernethy, and L. C Campbell, Psychological approaches to understanding and treating disease-related pain. Annu Rev Psychol, 2005. 56: p. 601-30. [CrossRef]
- Zeltzer, L. and S. LeBaron, Hypnosis and nonhypnotic techniques for reduction of pain and anxiety during painful procedures in children and adolescents with cancer. J Pediatr, 1982. 101(6): p. 1032-5. [CrossRef]
- Spiegel, D. and J.R. Bloom, Group therapy and hypnosis reduce metastatic breast carcinoma pain. Psychosom Med, 1983. 45(4): p. 333-9. [CrossRef]
- Syrjala, K.L., et al., Relaxation and imagery and cognitive-behavioral training reduce pain during cancer treatment: a controlled clinical trial. Pain, 1995. 63(2): p. 189-198. [CrossRef]
- Vickers, A.J., et al., Acupuncture for Chronic Pain: Update of an Individual Patient Data Meta-Analysis. J Pain, 2018. 19(5): p. 455-474. [CrossRef]
- AC, C. and F. KM., Therapeutic Approaches to Cancer Pain., in Holland-Frei Cancer Medicine. 2003, BC Decker: Hamilton (ON).
- Klepstad, P., et al., Influence from genetic variability on opioid use for cancer pain: a European genetic association study of 2294 cancer pain patients. Pain, 2011. 152(5): p. 1139-1145. [CrossRef]
- Bennett, M., J.A. Paice, and M. Wallace, Pain and Opioids in Cancer Care: Benefits, Risks, and Alternatives. Am Soc Clin Oncol Educ Book, 2017. 37: p. 705-713.
- Boland, J.W. and A.G. Pockley, Clinically relevant concentrations of opioids for in vitro studies. J Opioid Manag, 2016. 12(5): p. 313-321.
- Boland, J.W., Effect of Opioids on Survival in Patients with Cancer. Cancers (Basel), 2022. 14(22). [CrossRef]
- Bedson, J., et al., Risk of adverse events in patients prescribed long-term opioids: A cohort study in the UK Clinical Practice Research Datalink. Eur J Pain, 2019. 23(5): p. 908-922. [CrossRef]
- Azizoddin, D.R., et al., Cancer pain self-management in the context of a national opioid epidemic: Experiences of patients with advanced cancer using opioids. Cancer, 2021. 127(17): p. 3239-3245. [CrossRef]
- Kwon, J.H., Overcoming barriers in cancer pain management. J Clin Oncol, 2014. 32(16): p. 1727-33. [CrossRef]
- Ezenwa, M.O. and M.F. Fleming, Racial Disparities in Pain Management in Primary Care. J Health Dispar Res Pract, 2012. 5(3): p. 12-26.
- Mitra, R. and S. Jones, Adjuvant analgesics in cancer pain: a review. Am J Hosp Palliat Care, 2012. 29(1): p. 70-9. [CrossRef]
- Lussier, D., A.G. Huskey, and R.K. Portenoy, Adjuvant analgesics in cancer pain management. Oncologist, 2004. 9(5): p. 571-91. [CrossRef]
- Lamont, L.A., W.J. Tranquilli, and K.A. Mathews, Adjunctive analgesic therapy. Vet Clin North Am Small Anim Pract, 2000. 30(4): p. 805-13, vii. [CrossRef]
- Khan, M.I., D. Walsh, and N. Brito-Dellan, Opioid and adjuvant analgesics: compared and contrasted. Am J Hosp Palliat Care, 2011. 28(5): p. 378-83. [CrossRef]
- Organization, W.H., WHO Guidelines for the pharmacological and radiotherapeutic management of cancer pain in adults and adolescents. 2019. p. 138.
- Jensen, T.S., Anticonvulsants in neuropathic pain: rationale and clinical evidence. Eur J Pain, 2002. 6 Suppl A: p. 61-8. [CrossRef]
- Mezzanotte, J.N., et al., Updates in the Treatment of Chemotherapy-Induced Peripheral Neuropathy. Curr Treat Options Oncol, 2022. 23(1): p. 29-42. [CrossRef]
- Tremont-Lukats, I.W., C. Megeff, and M.M. Backonja, Anticonvulsants for neuropathic pain syndromes: mechanisms of action and place in therapy. Drugs, 2000. 60(5): p. 1029-52.
- Patel, R. and A.H. Dickenson, Mechanisms of the gabapentinoids and α 2 δ-1 calcium channel subunit in neuropathic pain. Pharmacol Res Perspect, 2016. 4(2): p. e00205. [CrossRef]
- Sindrup, S.H., et al., Antidepressants in the treatment of neuropathic pain. Basic Clin Pharmacol Toxicol, 2005. 96(6): p. 399-409. [CrossRef]
- Vyvey, M., Steroids as pain relief adjuvants. Can Fam Physician, 2010. 56(12): p. 1295-7, e415.
- Riechelmann, R.P., et al., Symptom and medication profiles among cancer patients attending a palliative care clinic. Support Care Cancer, 2007. 15(12): p. 1407-12. [CrossRef]
- Ayyar, V.S. and W.J. Jusko, Transitioning from Basic toward Systems Pharmacodynamic Models: Lessons from Corticosteroids. Pharmacol Rev, 2020. 72(2): p. 414-438. [CrossRef]
- Haywood, A., et al., Corticosteroids for the management of cancer-related pain in adults. Cochrane Database Syst Rev, 2015. 2015(4): p. CD010756. [CrossRef]
- Yennurajalingam, S., et al., Impact of a palliative care consultation team on cancer-related symptoms in advanced cancer patients referred to an outpatient supportive care clinic. J Pain Symptom Manage, 2011. 41(1): p. 49-56. [CrossRef]
- Ness, T.J., L. Jones, and H. Smith, Use of compounded topical analgesics--results of an Internet survey. Reg Anesth Pain Med, 2002. 27(3): p. 309-12.
- Stanos, S.P. and K.E. Galluzzi, Topical therapies in the management of chronic pain. Postgrad Med, 2013. 125(4 Suppl 1): p. 25-33. [CrossRef]
- Choi, E., et al., Topical agents: a thoughtful choice for multimodal analgesia. Korean J Anesthesiol, 2020. 73(5): p. 384-393. [CrossRef]
- Sawynok, J., Topical analgesics for neuropathic pain: preclinical exploration, clinical validation, future development. Eur J Pain, 2014. 18(4): p. 465-81. [CrossRef]
- Anand, P. and K. Bley, Topical capsaicin for pain management: therapeutic potential and mechanisms of action of the new high-concentration capsaicin 8% patch. Br J Anaesth, 2011. 107(4): p. 490-502. [CrossRef]
- Raffa, R.B., Pharmacology of oral combination analgesics: rational therapy for pain. J Clin Pharm Ther, 2001. 26(4): p. 257-64. [CrossRef]
- Vijan, S., S. Manaker, and A. Qaseem, Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain. Ann Intern Med, 2017. 167(11): p. 835-836. [CrossRef]
- Johnson, M.I., et al., Efficacy and safety of transcutaneous electrical nerve stimulation (TENS) for acute and chronic pain in adults: a systematic review and meta-analysis of 381 studies (the meta-TENS study). BMJ Open, 2022. 12(2): p. e051073. [CrossRef]
- Field, T., Massage therapy research review. Complement Ther Clin Pract, 2014. 20(4): p. 224-9. [CrossRef]
- Ehde, D.M., T.M. Dillworth, and J.A. Turner, Cognitive-behavioral therapy for individuals with chronic pain: efficacy, innovations, and directions for research. Am Psychol, 2014. 69(2): p. 153-66. [CrossRef]
- Shi, Y., et al., Brain Network to Placebo and Nocebo Responses in Acute Experimental Lower Back Pain: A Multivariate Granger Causality Analysis of fMRI Data. Front Behav Neurosci, 2021. 15: p. 696577. [CrossRef]
- Temel, J.S., et al., Early Palliative Care for Patients with Metastatic Non–Small-Cell Lung Cancer. New England Journal of Medicine, 2010. 363(8): p. 733-742. [CrossRef]
- Bakitas, M., et al., Effects of a Palliative Care Intervention on Clinical Outcomes in Patients With Advanced Cancer: The Project ENABLE II Randomized Controlled Trial. JAMA, 2009. 302(7): p. 741-749.
- Paice, J.A., Cancer pain management and the opioid crisis in America: How to preserve hard-earned gains in improving the quality of cancer pain management. Cancer, 2018. 124(12): p. 2491-2497. [CrossRef]
- Bucklar, N., et al., Early integration or last consultation: in-house palliative care involvement for hospitalized patients in tertiary medicine—a retrospective analysis. Supportive Care in Cancer, 2025. 33(4): p. 251.
- Schaefer, K.G., et al., Raising the bar for the care of seriously ill patients: results of a national survey to define essential palliative care competencies for medical students and residents. Acad Med, 2014. 89(7): p. 1024-31.
- Reed, M.K., et al., Sorting through life: evaluating patient-important measures of success in a medication for opioid use disorder (MOUD) treatment program. Substance Abuse Treatment, Prevention, and Policy, 2023. 18(1): p. 4. [CrossRef]
- Trang, T., et al., Pain and Poppies: The Good, the Bad, and the Ugly of Opioid Analgesics. J Neurosci, 2015. 35(41): p. 13879-88. [CrossRef]
- Harsanyi, H., C. Cuthbert, and F. Schulte, The Stigma Surrounding Opioid Use as a Barrier to Cancer-Pain Management: An Overview of Experiences with Fear, Shame, and Poorly Controlled Pain in the Context of Advanced Cancer. Curr Oncol, 2023. 30(6): p. 5835-5848. [CrossRef]
- Bulls, H.W., et al., Framework for opioid stigma in cancer pain. Pain, 2022. 163(2): p. e182-e189. [CrossRef]
- Carnago, L., M.R. Knisely, and J. Malek, Ethical considerations and decision making in opioid prescribing for chronic pain: A case study in rheumatology practice. J Am Assoc Nurse Pract, 2024. 36(5): p. 300-306. [CrossRef]
- Kotalik, J., Controlling pain and reducing misuse of opioids: ethical considerations. Can Fam Physician, 2012. 58(4): p. 381-5, e190-5.
- Smeltzer, K.E., G.J. Desai, and B. Johnson, Ethical considerations in prescribing or withholding opioids for chronic pain. Osteopathic Family Physician, 2017. 9: p. 26-29.
- Salins, N., et al., Definition of Terms Used in Limitation of Treatment and Providing Palliative Care at the End of Life: The Indian Council of Medical Research Commission Report. Indian J Crit Care Med, 2018. 22(4): p. 249-262. [CrossRef]
- Bhyan, P., et al., Palliative Sedation in Patients With Terminal Illness, in StatPearls. 2025, StatPearls Publishing Copyright © 2025, StatPearls Publishing LLC.: Treasure Island (FL).
- Vargas, A.J., et al., Exploring Racial Disparities in Chronic Pain Management. J Pain Res, 2025. 18: p. 2901-2908. [CrossRef]
- Enzinger, A.C., et al., Racial and Ethnic Disparities in Opioid Access and Urine Drug Screening Among Older Patients With Poor-Prognosis Cancer Near the End of Life. Journal of Clinical Oncology, 2023. 41(14): p. 2511-2522. [CrossRef]
- Baryakova, T.H., et al., Overcoming barriers to patient adherence: the case for developing innovative drug delivery systems. Nat Rev Drug Discov, 2023. 22(5): p. 387-409. [CrossRef]
- Krukowska, K., et al., The effectiveness of acupuncture in cancer pain treatment. Frontiers in Oncology, 2024. Volume 14-2024. [CrossRef]
- Yang, J., et al., Acupuncture for chronic cancer-related pain: a systematic review and network meta-analysis protocol. BMJ Open, 2020. 10(10): p. e039087. [CrossRef]
- Vučković, S., et al., Cannabinoids and Pain: New Insights From Old Molecules. Front Pharmacol, 2018. 9: p. 1259. [CrossRef]
- Boland, E.G., et al., Cannabinoids for adult cancer-related pain: systematic review and meta-analysis. BMJ Supportive & Palliative Care, 2020. 10(1): p. 14. [CrossRef]
- Qie, B., et al., Gene therapy for genetic diseases: challenges and future directions. MedComm (2020), 2025. 6(2): p. e70091. [CrossRef]
- Meng, H., et al., Cannabis and cannabinoids in cancer pain management. Curr Opin Support Palliat Care, 2020. 14(2): p. 87-93. [CrossRef]
- Gamage, T.F. and A.H. Lichtman, The endocannabinoid system: role in energy regulation. Pediatr Blood Cancer, 2012. 58(1): p. 144-8. [CrossRef]
- Handy, C.R., C. Krudy, and N. Boulis, Gene therapy: a potential approach for cancer pain. Pain Res Treat, 2011. 2011: p. 987597. [CrossRef]
- Kaye, A.D., et al., Update on the pharmacogenomics of pain management. Pharmgenomics Pers Med, 2019. 12: p. 125-143. [CrossRef]
- Raguram, A., S. Banskota, and D.R. Liu, Therapeutic in vivo delivery of gene editing agents. Cell, 2022. 185(15): p. 2806-2827. [CrossRef]
- Agulló, L., et al., Pharmacogenetic Guided Opioid Therapy Improves Chronic Pain Outcomes and Comorbid Mental Health: A Randomized, Double-Blind, Controlled Study. Int J Mol Sci, 2023. 24(13). [CrossRef]
- Pulskamp, T.G., L.M. Johnson, and D.J. Berlau, Novel non-opioid analgesics in pain management. Pain Manag, 2024. 14(12): p. 641-651. [CrossRef]
- Kaneko, Y. and A. Szallasi, Transient receptor potential (TRP) channels: a clinical perspective. Br J Pharmacol, 2014. 171(10): p. 2474-507. [CrossRef]
- Basch, E., A.B. Leahy, and A.C. Dueck, Benefits of Digital Symptom Monitoring With Patient-Reported Outcomes During Adjuvant Cancer Treatment. J Clin Oncol, 2021. 39(7): p. 701-703. [CrossRef]
- Blake, H., W.J. Chaplin, and A. Gupta, The effectiveness of digital interventions for self-management of chronic pain in employment settings: a systematic review. Br Med Bull, 2024. 151(1): p. 36-48. [CrossRef]
- Orujlu, S., et al., Barriers to cancer pain management from the perspective of patients: A qualitative study. Nurs Open, 2022. 9(1): p. 541-549. [CrossRef]
- Cluxton, C., The Challenge of Cancer Pain Assessment. Ulster Med J, 2019. 88(1): p. 43-46.
- Hjermstad, M.J., et al., Pain assessment tools in palliative care: an urgent need for consensus. Palliat Med, 2008. 22(8): p. 895-903. [CrossRef]
Figure 1.
Multimodal approach to chronic cancer pain management. Pharmacologic and Non-pharmacologic strategies converge into an integrated plan, aiming to improve pain control, reduce opioid reliance, and enhance quality of life.
Figure 1.
Multimodal approach to chronic cancer pain management. Pharmacologic and Non-pharmacologic strategies converge into an integrated plan, aiming to improve pain control, reduce opioid reliance, and enhance quality of life.


Table 1.
Common cancer types associated with chronic pain and their dominant mechanisms.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



