Submitted:
24 March 2026
Posted:
25 March 2026
You are already at the latest version
Abstract
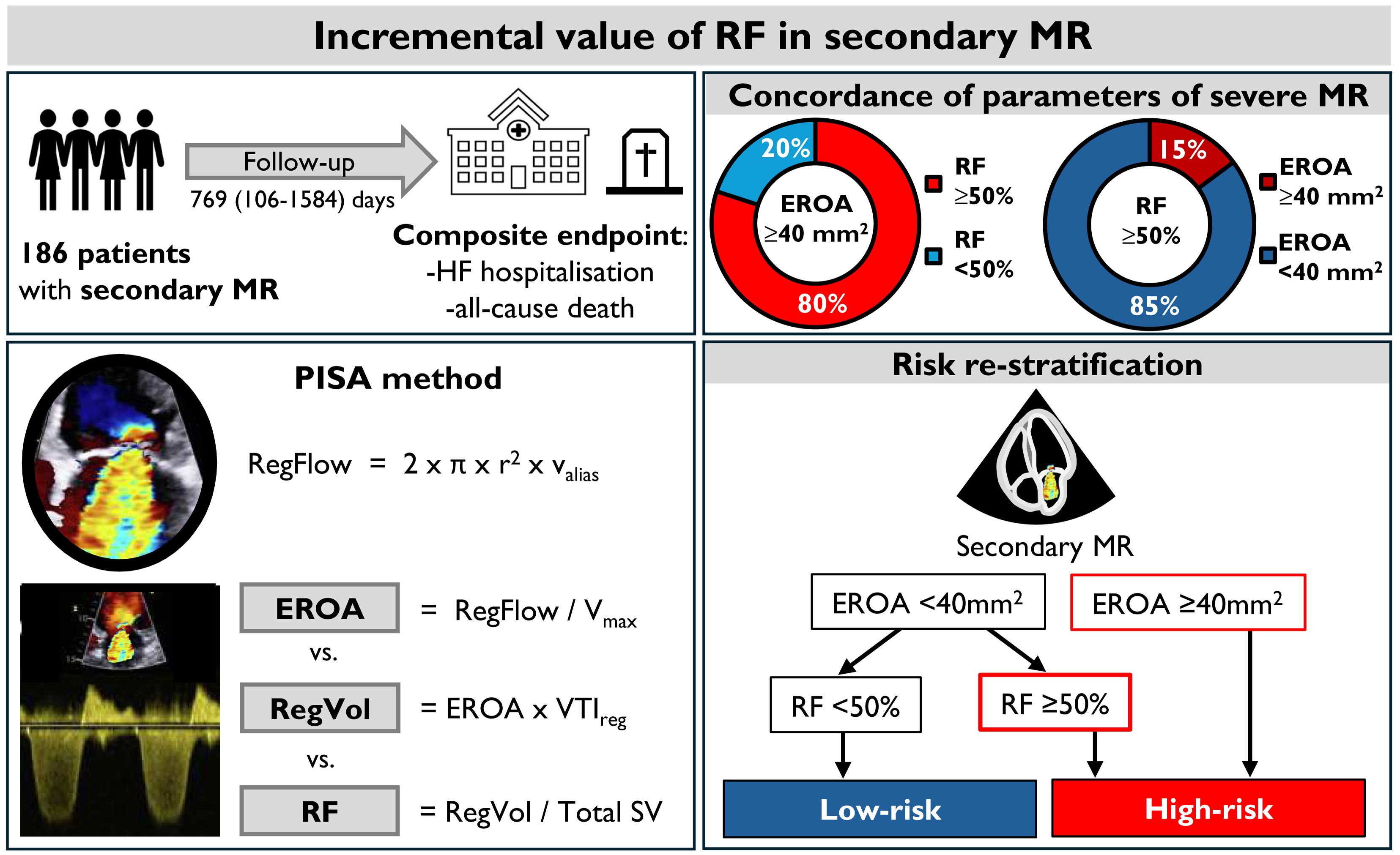
Objectives: Quantifying ventricular secondary mitral regurgitation (MR) remains challenging, and the prognostic value of echocardiographic parameters is uncertain. This study aimed to assess the concordance of parameters of MR severity and determine the added value of regurgitant fraction (RF) in predicting outcomes. Methods and results: We retrospectively analysed 186 patients with ventricular secondary MR who underwent echocardiography with MR assessment, evaluating effective regurgitant orifice area (EROA), regurgitant volume (RegVol) and RF. The primary endpoint was a composite of all-cause death or heart failure hospitalisation. Quantitative parameters of MR severity were frequently discordant. Using the guideline-recommended cut-offs for EROA (≥ 40 mm2), RegVol (≥ 60 ml) and RF (≥ 50%), severe MR was present in 5.4%, 3.3%, and 29.5% of patients, respectively. Both RF ≥ 50% and EROA ≥ 40 mm² were independently associated with clinical outcomes in multivariable Cox models. Combining RF and EROA provided incremental prognostic value over either parameter alone (p < 0.05). Kaplan-Meier curves showed that patients with EROA < 40 mm² and RF ≥ 50% had similar outcomes to those with EROA ≥ 40 mm² (p = 0.055), whereas patients with both EROA < 40 mm² and RF < 50% had significantly better outcomes (p = 0.002). Conclusions: Substantial discordance between quantitative parameters of severe MR was observed in ventricular secondary MR. RF is a strong, underutilised marker of MR severity, reflecting haemodynamic burden beyond EROA and RegVol. Patients with EROA < 40 mm2 and RF > 50% had outcomes comparable to those who met guideline-based threshold for severe MR, defined as EROA ≥ 40 mm2. Our results demonstrate that routine RF assessment enhances risk stratification and enables identification of a high-risk subgroup of patients with EROA < 40 mm2.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Echocardiographic Assessment
2.3. Outcome
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. Comparison of Parameters of MR Severity
3.3. Association of MR Severity with Clinical Outcomes
3.4. Added Value of Combining EROA and RF for the Composite Endpoint
4. Discussion
4.1. Concordance of Quantitative Parameters of MR Severity
4.2. Association of MR Grading with Clinical Outcome
4.3. Clinical Implications
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Acknowledgments
References
- Rossi A.; Dini F.L.; Faggiano P.; Agricola E.; Cicoira M.; Frattini S.; et al. Independent prognostic value of functional mitral regurgitation in patients with heart failure. A quantitative analysis of 1256 patients with ischaemic and non-ischaemic dilated cardiomyopathy. Heart. 2011, 97 :1675-1680.
- Grigioni F.; Enriquez-Sarano M.; Zehr K.J.; Bailey K.R.; Tajik A.J. Ischemic mitral regurgitation: long-term outcome and prognostic implications with quantitative Doppler assessment. Circulation. 2001, 103, 1759-1764.
- Tomaselli M.; Badano L.P.; Oliverio G.; Curti E.; Pece C.; Springhetti P.; et al. Clinical Impact of the Volumetric Quantification of Ventricular Secondary Mitral Regurgitation by Three-Dimensional Echocardiography. J. Am. Soc. Echocardiogr. 2024, 37, 408-419.
- Murata A.; Kaneko T.; Amano M.; Sato Y.; Ohno Y.; Obokata M.; et al. Qualitative and quantitative assessment of atrial functional mitral regurgitation: analysis from the REVEAL-AFMR registry. Eur. Heart. J. Cardiovasc. Imaging. 2025, 26, 299-306.
- Benfari G.; Antoine C.; Essayagh B.; Batista R.; Maalouf J.; Rossi A.; et al. Functional Mitral Regurgitation Outcome and Grading in Heart Failure With Reduced Ejection Fraction. JACC. Cardiovasc. Imaging. 2021, 14, 2303-2315.
- Grayburn P.A.; Carabello B.; Hung J.; Gillam L.D.; Liang D.; Mack M.J.; et al. Defining "severe" secondary mitral regurgitation: emphasizing an integrated approach. J. Am. Coll. Cardiol. 2014, 64, 2792-2801.
- Bartko P.E.; Arfsten H.; Heitzinger G.; Pavo N.; Toma A.; Strunk G.; et al. A Unifying Concept for the Quantitative Assessment of Secondary Mitral Regurgitation. J. Am. Coll. Cardiol. 2019, 73, 2506-2517.
- Lang R.M.; Badano L.P.; Mor-Avi V.; Afilalo J.; Armstrong A.; Ernande L.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart. J. Cardiovasc. Imaging. 2015, 16, 233-70.
- Lancellotti P.; Pibarot P.; Chambers J.; et al. Multi-modality imaging assessment of native valvular regurgitation: an EACVI and ESC council of valvular heart disease position paper. Eur. Heart. J. Cardiovasc. Imaging. 2022, 23, e171-e232.
- Zoghbi W.A.; Adams D.; Bonow R.O.; La Canna G.; Pepi M.; Dulgheru R.; et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2017, 30, 303-371.
- Mukherjee M.; Rudski L.G.; Addetia K.; Afilalo J.; D'Alto M.; Freed B.H.; et al. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults and Special Considerations in Pulmonary Hypertension: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2025, 38, 141-186.
- Pavlou M.; Ambler G.; Seaman S.R.; Guttmann O.; Elliott P.; King M.; et al. How to develop a more accurate risk prediction model when there are few events. BMJ. 2015, 351, h3868.
- Uretsky S.; Aldaia L.; Marcoff L.; Koulogiannis K.; Argulian E.; Lasam G.; et al. Concordance and Discordance of Echocardiographic Parameters Recommended for Assessing the Severity of Mitral Regurgitation. Circ. Cardiovasc. Imaging. 2020, 13, e010278.
- Ambrožič J.; Rauber M.; Berlot B.; Škofic N.; Toplišek J.; Bervar M.; et al. Challenges and pitfalls in classification of disproportionate mitral regurgitation. Int. J. Cardiovasc. Imaging. 2024, 40, 757-767.
- Buck T.; Plicht B.; Kahlert P.; Schenk I.M.; Hunold P.; Erbel R. Effect of dynamic flow rate and orifice area on mitral regurgitant stroke volume quantification using the proximal isovelocity surface area method. J. Am. Coll. Cardiol. 2008, 52, 767-778.
- Schwammenthal E.; Chen C.; Benning F.; Block M.; Breithardt G.; Levine R.A. Dynamics of mitral regurgitant flow and orifice area. Physiologic application of the proximal flow convergence method: clinical data and experimental testing. Circulation. 1994, 90, 307-322.
- Vahanian A.; Beyersdorf F.; Praz F.; Milojevic M.; Baldus S.; Bauersachs J.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart. J. 2022, 43, 561-632.
- Otto C.M.; Nishimura R.A.; Bonow R.O.; Carabello B.A.; Erwin J.P. 3rd; Gentile F.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021, 143, e35-e71.
- O'Gara P.T.; Grayburn P.A.; Badhwar V.; Afonso L.C.; Carroll J.D.; Elmariah S.; et al. 2017 ACC Expert Consensus Decision Pathway on the Management of Mitral Regurgitation: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J. Am. Coll. Cardiol. 2017, 70, 2421-2449.
- Pibarot P.; Dumesnil J.G. Low-flow, low-gradient aortic stenosis with normal and depressed left ventricular ejection fraction. J. Am. Coll. Cardiol. 2012, 60, 1845-1853.
- Goliasch G.; Bartko P.E.; Pavo N.; Neuhold S.; Wurm R.; Mascherbauer J.; et al. Refining the prognostic impact of functional mitral regurgitation in chronic heart failure. Eur. Heart. J. 2018, 39, 39-46.
- Patel J.B.; Borgeson D.D.; Barnes M.E.; Rihal C.S.; Daly R.C.; Redfield M.M. Mitral regurgitation in patients with advanced systolic heart failure. J. Card. Fail. 2004, 10, 285-291.
- Naser J.A.; Rahme S.J.; Ibrahim H.; Scott C.G.; Michelena H.I.; Borlaug B.A.; et al. Role of Quantitative Assessment of Atrial Functional Mitral Regurgitation. J. Am. Soc. Echocardiogr. 2025, 38, 353-355.
- Sannino A.; Smith R.L. 2nd; Schiattarella G.G.; Trimarco B.; Esposito G.; Grayburn P.A. Survival and Cardiovascular Outcomes of Patients With Secondary Mitral Regurgitation: A Systematic Review and Meta-analysis. JAMA. Cardiol. 2017, 2, 1130-1139.
- Gaasch W.H.; Meyer T.E. Secondary mitral regurgitation (part 1): volumetric quantification and analysis. Heart. 2018, 104, 634-638.
- Aurich M.; André F.; Keller M.; Greiner S.; Hess A.; Buss S.J.; et al. Assessment of Left Ventricular Volumes with Echocardiography and Cardiac Magnetic Resonance Imaging: Real-Life Evaluation of Standard versus New Semiautomatic Methods. J. Am. Soc. Echocardiogr. 2014, 27, 1017–1024.






| All patients (n=186) | No events (n= 79) | Events (n=107) | P-value | |
| Clinical characteristics | ||||
| Age (years) | 69±12 | 65±13 | 72±10 | 0.001 |
| Gender (male) | 129 (69) | 56 (71) | 73 (68) | 0.697 |
| BMI (kg/m2) | 27±5 | 28±4 | 27±5 | 0.299 |
| Systolic blood pressure (mmHg) | 122±20 | 125±19 | 119±20 | 0.106 |
| Heart rate (bpm) | 77±19 | 76±22 | 77±17 | 0.700 |
| Atrial fibrillation (%) | 50 (27) | 18 (23) | 32 (27) | 0.279 |
| Ischemic cardiomyopathy (%) | 101 (54) | 41 (52) | 60 (56) | 0.572 |
| Echocardiographic characteristics | ||||
| LVEDD (mm) | 62±10 | 62±9 | 62±11 | 0.990 |
| LVESD (mm) | 51±12 | 50±11 | 51±12 | 0.414 |
| LVEDV index (ml) | 100 (79-124) | 95 (77-119) | 107 (83-126) | 0.109 |
| LVESV index (ml) | 64 (44-84) | 58 836-76) | 69 (49-88) | 0.017 |
| LVEF (%) | 35 (29-45) | 41 (32-42) | 34 (27-42) | 0.001 |
| Stroke volume index (ml/m2) | 31±11 | 33±13 | 29±8 | 0.028 |
| CO (l/min) | 4.2 (3.4-5.0) | 4.1 (3.4-5.4) | 4.2 (3.2-4.8) | 0.199 |
| RV basal diameter (mm) | 41±8 | 39±7 | 42±8 | 0.001 |
| TAPSE (mm) | 18±5 | 19±5 | 18±4 | 0.009 |
| PASP (mmHg) | 48±13 | 46±14 | 50±12 | 0.068 |
| EROA (mm2) | 19 (14-25) | 17 (12-23) | 19 (14-25) | 0.140 |
| RegVol (ml) | 27 (19-37) | 26 (20-33) | 27 (19-37) | 0.640 |
| RF (%) | 39 (29-54) | 36 (25-46) | 40 (30-59) | 0.017 |
| HR (95% CI) | P-value | |
| Age (years) | 1.032 (1.016-1.050) | <0.001 |
| Male sex | 0.985 (0.655-1.450) | 0.941 |
| BMI (kg/m2) | 0.962 (0.919-1.007) | 0.099 |
| Heart rate (bpm) | 1.004 (0.996-1.013) | 0.330 |
| Atrial fibrillation (%) | 1.236 (0.817-1.870 | 0.317 |
| Ischemic cardiomyopathy (%) | 1.183 (0.807-1.734) | 0.389 |
| LVEDD (mm) | 1.004 (0.984-1.024) | 0.706 |
| LVESD (mm) | 1.011 (0.994-1.029) | 0.199 |
| LVEDV index (ml) | 1.004 (0.999-1.008) | 0.098 |
| LVESV index (ml) | 1.007 (1.002-1.011) | 0.007 |
| LVEF (%) | 0.967 (0.951-0.984) | <0.001 |
| Stroke volume index (ml/m2) | 0.976 (0.957-0.995) | 0.012 |
| RV basal (mm) | 1.768 (1.349-2.317) | <0.001 |
| TAPSE (mm) | 0.520 (0.338-0.800) | 0.003 |
| PASP (mmHg) | 1.024 (1.009-1.039) | 0.001 |
| EROA (≥40mm2) | 3.794 81.728-8.330) | 0.001 |
| RegVol (≥60ml) | 0.806 (0.199-3.268) | 0.762 |
| RF (≥50%) | 2.073 (1.385-3.103) | <0.001 |
| Model 1 | Model 2 | Model 3 | ||||
| HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value | |
| Age (years) | 1.036 (1.015-1.058) | 0.001 | 1.041 (1.020-1.063) | <0.001 | 1.037 (1.016-1.059) | 0.001 |
| LVESV index (ml) | 1.007 (1.001-1.012) | 0.016 | 1.006 (1.000-1.011) | 0.049 | 1.008 (1.002-1.013) | 0.006 |
| SV index (ml/m2) | 0.975 (0.954-0.996) | 0.022 | 0.976 (0.955-0.998) | 0.033 | 0.978 (0.957-0.999) | 0.039 |
| RV basal (mm) | 1.627 (1.197-2.212) | 0.002 | 1.577 (1.158-2.147) | 0.004 | 1.592 (1.184-2.142) | 0.002 |
| PASP (mmHg) | 1.007 (0.990-1.025) | 0.401 | 1.005 (0.988-1.022) | 0.576 | 1.004 (0.987-1.021) | 0.643 |
| RegVol (≥60ml) | 0.523 (0.121-2.255) | 0.385 | ||||
| EROA (≥40mm2) | 2.811 (1.211-6.526) | 0.016 | ||||
| RF (≥50%) | 1.757 (1.141-2.704) | 0.010 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



