Submitted:
16 March 2026
Posted:
17 March 2026
You are already at the latest version
Abstract
Background: Atrial fibrillation (AF) frequently coexists with heart failure (HF) and worsens clinical outcomes. However, predictors of AF in HF with preserved (HFpEF) and mildly reduced ejection fraction (HFmrEF) remain poorly defined. This study aimed to identify clinical, laboratory, and echocardiographic predictors of AF in these HF phe-notypes. Methods: This retrospective single-center observational study included 700 consecutive patients with HF hospitalized between January 2018 and December 2023. The median age was 74 years (IQR 66–80). Women predominated in the cohort (55.3% vs. 44.7%, p < 0.001). Based on echocardiographically assessed left ventricular ejection fraction, patients were stratified into groups with preserved (≥50%), mildly reduced (41–49%) and reduced (≤40%) ejection fraction. Predictors of AF were evaluated using univariate and multivariate lo-gistic regression analyses, and model discrimination was assessed using ROC analysis. Results: Strongest predictors of AF in our patients with HFpEF and HFmrEF were left atrial size (OR 1.114 per mm increase; 95% CI 1.054–1.177; p < 0.001), moderate and severe tricuspid regurgitation (OR 4.092; 95% CI 1.977–8.466; p < 0.001 and OR 6.957; 95% CI 2.482–19.499; p < 0.001), male gender (OR 1.680; 95% CI 1.076–2.621; p = 0.022) and advanced age (OR 1.070 per year; 95% CI 1.032–1.109; p < 0.001). Conclusions: In patients with HFpEF and HFmrEF, AF is strongly associated with atrial remodeling, with left atrial enlargement as the key structural predictor. Identification of high-risk patients using clinical and echocardiographic parameters may facilitate earlier AF detection and improved risk stratification.
Keywords:
atrial fibrillation
; heart failure
; HFpEF
; HFmrEF
; echocardiography
; risk prediction
1. Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia worldwide, affecting approximately 2–3% of the general population, with prevalence increasing markedly with age [1,2,3,4,5]. Epidemiological studies indicate that the lifetime risk of AF exceeds 30% in individuals older than 55 years [1,2,3]. According to data from the Global Burden of Disease project, more than 59 million people worldwide are currently living with AF, and its prevalence is expected to continue rising due to population ageing, improved survival from cardiovascular diseases, and enhanced detection of asymptomatic cases [3,6]. AF carries substantial clinical significance, as it is associated with an increased risk of ischemic stroke, systemic thromboembolism, heart failure (HF), cognitive impairment, and cardiovascular mortality [1,3,7].
Heart failure represents another major global health challenge, characterized by high morbidity, mortality, and healthcare burden [8,9,10,11]. The prevalence of HF is estimated at approximately 1–2% in the adult population and exceeds 10% among individuals older than 70 years [8,9,10,11].
AF and HF frequently coexist and share complex bidirectional interactions [12,13,14]. AF may precipitate or worsen HF through loss of atrial contribution to ventricular filling, irregular ventricular rhythm, and tachycardia-induced cardiomyopathy [1,12,14,15]. Conversely, structural and hemodynamic changes associated with HF—including elevated filling pressures, atrial dilation, myocardial fibrosis, and neurohormonal activation—create a substrate that promotes atrial electrical instability and facilitates the development and maintenance of AF [12,13,14,15].
Particular interest has recently focused on patients with HF with preserved (HFpEF) and mildly reduced ejection fraction (HFmrEF), which represent a rapidly expanding and heterogeneous HF population [9,16,17,18]. In these phenotypes, AF is the most common arrhythmia, with reported prevalence ranging between 15% and 40% in various clinical studies and registries [13,19,20,21,22]. The coexistence of AF and HFpEF/HFmrEF is associated with more severe symptoms, higher rates of hospitalization, and worse long-term prognosis compared with patients in sinus rhythm [13,19,20,21,22].
Multiple factors have been implicated as potential predictors of AF in patients with HF, including advanced age, male sex, hypertension, obesity, diabetes mellitus, chronic kidney disease, and structural heart disease [23,24,25,26,27]. In addition, electrocardiographic abnormalities and echocardiographic markers of atrial remodeling—particularly left atrial (LA) enlargement—have been consistently associated with increased AF risk [23,24,27,28]. Biomarkers reflecting myocardial stress, inflammation, and neurohormonal activation have also been proposed as potential predictors [29,30,31,32]. However, available data remain heterogeneous, and many studies have focused predominantly on HF with reduced ejection fraction (HFrEF), leaving important gaps in the understanding of AF predictors specifically in HFpEF and HFmrEF populations [13,21,28,32].
Identification of reliable predictors of AF in patients with HFpEF and HFmrEF is therefore of considerable clinical importance. Early recognition of individuals at increased risk may facilitate targeted screening strategies, earlier diagnosis of AF, and more effective risk stratification and management. Therefore, the aim of the present study was to identify clinical, laboratory and echocardiographic predictors associated with AF in patients with HFpEF and HFmrEF.
2. Materials and Methods
2.1. Study Design and Population
This retrospective single-center observational study included 700 consecutive patients with chronic HF hospitalized in a tertiary cardiology clinic between January 2018 and December 2023. The diagnosis of chronic HF was established according to the recommendations of the European Society of Cardiology (ESC) based on clinical, laboratory, and echocardiographic criteria [8,9].
The median age of the study population was 74 years (interquartile range [IQR] 66–80 years), and women predominated (55.3% vs. 44.7%, p < 0.001).
Patients were stratified according to left ventricular ejection fraction (LVEF), assessed by transthoracic echocardiography, into the following HF phenotypes: HF with preserved ejection fraction (HFpEF, LVEF ≥50%), HF with mildly reduced ejection fraction (HFmrEF, LVEF 41–49%) and HF with reduced ejection fraction (HFrEF, LVEF ≤40%), in accordance with the current ESC guidelines on HF [8,9]. HFpEF was the most prevalent phenotype (487 patients, 69.6%), followed by HFrEF (107 patients, 15.3%) and HFmrEF (106 patients, 15.1%), p < 0.001.
For the purposes of the study, patients were further classified according to cardiac rhythm into two groups: sinus rhythm (n = 317, 45.3%) and AF (n = 383, 54.7%), encompassing all clinical phenotypes of this arrhythmia as defined by the current ESC guidelines [1]. AF was significantly more prevalent in the study population (p = 0.013).
Clinical data including demographic characteristics, comorbidities, cardiovascular risk factors, medication history, physical examination findings, laboratory results, and instrumental investigations were collected retrospectively from hospital discharge summaries and available medical records and entered into a standardized data collection form.
2.2. Inclusion and Exclusion Criteria
Patients were eligible for inclusion if they met the following criteria:
- age ≥18 years;
- instrumental assessment of LVEF within the previous 12 months;
- documented cardiac rhythm (sinus rhythm, AF, or other rhythm) confirmed by electrocardiography (ECG) or Holter ECG monitoring;
- availability of sufficiently complete clinical, laboratory, and imaging data required for the analysis.
Patients were excluded if they had:
- an acute cardiovascular event (myocardial infarction, ischemic or hemorrhagic stroke, acute peripheral arterial incident, or other) ≤90 days prior to the time of assessment;
- implanted rhythm-modifying cardiac devices (e.g., permanent pacemakers, implantable cardioverter-defibrillators, or cardiac resynchronization therapy devices);
- significant uncontrolled comorbidities that could influence the analyzed parameters (e.g., active malignancy, severe renal failure, uncontrolled endocrine disorders);
- incomplete medical documentation preventing adequate analysis.
2.3. Electrocardiography and Holter ECG Monitoring
A standard 12-lead ECG was performed in all patients using a Mortara ELI 280c electrocardiograph. ECG recordings were analyzed for heart rhythm, heart rate, electrical axis, P-wave morphology, PR interval, QRS duration and morphology, as well as ST-segment and T-wave abnormalities.
When clinically indicated, 24–72-hour Holter ECG monitoring was performed using 3-channel (Contec V5.5.2.3) or 7-channel (Medilog Darwin V2, Schiller Ltd) devices to detect rhythm disturbances and confirm the presence of AF. The diagnosis of this rhythm disorder was established based on electrocardiographic findings in accordance with current ESC guidelines [1]. Both previously diagnosed AF and AF detected during hospitalization were included in the analysis.
2.4. Echocardiographic Assessment
All patients underwent transthoracic echocardiography performed by experienced cardiologists using standard imaging protocols. Examinations were performed using a General Electric Vivid E95 ultrasound system equipped with a 4Vc matrix-array sector transducer and were conducted in accordance with the recommendations of the European Association of Cardiovascular Imaging [33].
Standard M-mode and two-dimensional imaging were used for cardiac structural assessment. Left ventricular systolic function was evaluated by calculating LVEF using the biplane Simpson method.
Cardiac chamber dimensions and geometry were assessed by measuring LA size in the parasternal long-axis view and LA longitudinal diameter in the apical four-chamber view, as well as interventricular septal thickness and posterior left ventricular wall thickness. LV size was further characterized by measuring end-diastolic and end-systolic diameters in the parasternal long-axis view and LV end-diastolic and end-systolic volumes in the apical four-chamber view.
2.5. Laboratory Investigations
Laboratory analyses were performed at the central clinical laboratory of the hospital where our study was conducted. The analyzed variables included potassium, sodium, hemoglobin, hematocrit, C-reactive protein (CRP), N-terminal pro-B-type natriuretic peptide (NT-proBNP), uric acid, serum creatinine, and estimated glomerular filtration rate (eGFR) calculated using the CKD-EPI 2021 formula [34].
2.6. Ethical Considerations
The study protocol was registered in the ClinicalTrials.gov Protocol Registration and Results System (PRS), National Library of Medicine, under the unique protocol ID PK36-3117-27/04/22. It was conducted in accordance with the ethical principles of the Declaration of Helsinki and the principles of Good Clinical Practice. Due to the retrospective and non-interventional design of the study and the use of fully anonymized clinical data, the requirement for informed consent was waived in accordance with applicable national regulations and institutional policies.
2.7. Statistical Analysis
All statistical analyses were performed using SPSS software (IBM SPSS Statistics, version 19.0, IBM Corp., Armonk, NY, USA). Continuous variables are presented as median values with interquartile ranges (IQR), while categorical variables are expressed as absolute numbers and percentages. Categorical variables were compared using the χ² test, while continuous variables were compared using the Kruskal–Wallis test or Mann–Whitney U test as appropriate.
Potential predictors of AF were initially evaluated using univariate logistic regression analysis. Variables showing statistical significance were subsequently included in a multivariate logistic regression model to identify independent predictors of AF.
The predictive performance of the model was assessed using receiver operating characteristic (ROC) curve analysis with calculation of the area under the curve (AUC). Calibration of the model was assessed by comparing the observed prevalence of AF across tertiles of predicted risk.
A p-value <0.05 was considered statistically significant.
3. Results
3.1. Baseline Characteristics of the Study Population
Table 1 summarizes the demographic and epidemiological characteristics of patients according to HF phenotype. HFpEF was the predominant phenotype (69.6%). A significant difference in sex distribution was observed, with male predominance in the HFmrEF and HFrEF groups (p < 0.001). Age and age distribution did not differ significantly between phenotypes (p = 0.738 and p = 0.051), with patients aged ≥70 years constituting the majority of the cohort. The distribution of cases before and after the COVID-19 pandemic was similar across HF phenotypes and did not reach statistical significance.
Table 2 summarizes the clinical profile of the study population, including HF duration, NYHA functional class, and the prevalence and forms of AF according to HF phenotype.
HF duration did not differ significantly between groups (p = 0.077).
NYHA class distribution differed significantly (p < 0.001), with NYHA III predominating across all phenotypes and NYHA IV being more frequent in HFrEF. The predominance of NYHA III likely reflects the hospitalized nature of the study population, in which patients are typically admitted due to symptomatic decompensation or worsening HF.
Heart rhythm distribution also differed significantly (p < 0.001), with sinus rhythm more common in HFpEF, whereas permanent AF predominated in HFmrEF and HFrEF.
Table 3 summarizes the comorbidity profile of HF patients according to HF phenotype. Most cardiovascular and non-cardiovascular comorbidities and cardiometabolic risk factors were similarly distributed across phenotypes. However, coronary artery disease (p = 0.009), chronic kidney disease (p = 0.015), peripheral arterial disease (p = 0.004), and prior cardiac surgery (p < 0.001) were significantly more frequent among patients with HFmrEF and HFrEF.
Table 4 presents the distribution of the CHA₂DS₂-VA score according to HF phenotype and cardiac rhythm. In patients with HFpEF, the median score ranged from 3 to 4 points across different rhythm categories. Comparable values were observed in patients with HFmrEF and HFrEF. Overall, the CHA₂DS₂-VA score showed similar distributions across HF phenotypes, with no statistically significant differences between groups (p = 0.568).
Table 5 presents the distribution of the HAS-BLED score according to HF phenotype and cardiac rhythm. Median HAS-BLED values were 2 points across all HF phenotypes, with largely overlapping interquartile ranges. Accordingly, no statistically significant differences were observed between groups (p = 0.523).
Table 6 summarizes the hemodynamic and anthropometric characteristics of the study population according to HF phenotype. Office systolic blood pressure (BP) differed significantly between groups (p = 0.002), with higher values observed in patients with HFpEF. Heart rate also showed significant differences across phenotypes (p < 0.001), with higher values in HFmrEF and HFrEF. No significant differences were observed in diastolic BP or body mass index (BMI).
Table 7 presents selected laboratory parameters of the study population according to HF phenotype. Serum sodium levels and eGFR differed significantly between groups (p = 0.038 and p = 0.037, respectively). In contrast, potassium levels, hemoglobin concentration, and serum creatinine values were comparable across HF phenotypes.
Table 8 summarizes the echocardiographic characteristics of the study population according to HF phenotype. Significant differences were observed in LA size and multiple LV structural and functional parameters across HF phenotypes (all p < 0.01). Patients with HFrEF exhibited larger LV dimensions and volumes, whereas HFpEF was characterized by smaller ventricular size. A progressive increase in LA dimensions was also observed across HF phenotypes, with the largest values detected in patients with HFrEF. These findings reflect distinct patterns of cardiac remodeling across HF phenotypes, with more pronounced ventricular dilation in HFrEF and relatively preserved ventricular geometry in HFpEF.
To identify factors associated with AF across different HF phenotypes, univariate binary logistic regression analyses were performed separately for each subgroup (Table 9, Table 10, Table 11, Table 12, Table 13 and Table 14). In HFpEF, AF was associated with the broadest range of demographic, clinical, laboratory, echocardiographic, valvular, and treatment-related variables. In HFmrEF, the spectrum of significant associations was more limited and mainly included age, heart rate, and LA size. In HFrEF, AF was associated predominantly with age, hemodynamic parameters, and indices of left ventricular geometry. Multivariate logistic regression further identified distinct phenotype-specific independent predictors of AF.
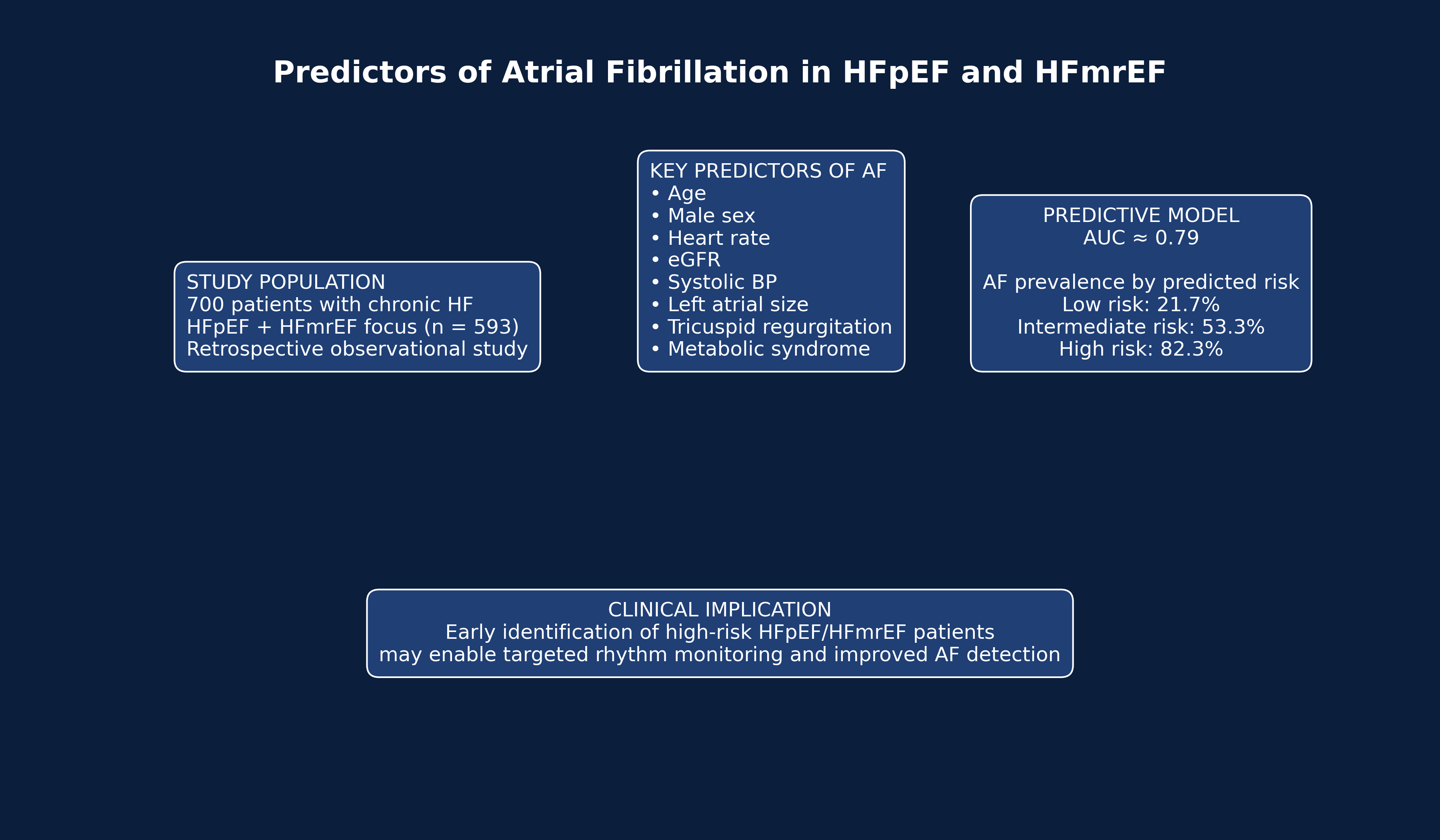
Based on the identified predictors, a prognostic model for AF was developed in the pooled HFpEF/HFmrEF population (n = 593). The model incorporated age, sex, heart rate, office systolic BP, eGFR, LA size measured in the parasternal long-axis view, the presence and severity of tricuspid regurgitation, metabolic syndrome, and an indicator variable for HF phenotype.
The model demonstrated good discriminative ability, with an area under the ROC curve (AUC) of 0.789 in the combined cohort. When stratified by HF phenotype, the model maintained good and comparable discrimination: AUC 0.795 (95% CI 0.756–0.834) in HFpEF and AUC 0.818 (95% CI 0.727–0.897) in HFmrEF. The difference in discriminative performance between phenotypes was not statistically significant (ΔAUC = 0.023, 95% CI −0.074–0.111; p = 0.598), indicating stable predictive performance of the model across both HF phenotypes.
Figure 2 illustrates the observed prevalence of AF across tertiles of predicted risk derived from the multivariable model in patients with HFpEF and HFmrEF. Patients were stratified into three categories according to predicted probability: low risk (<0.33), intermediate risk (0.33–0.66), and high risk (>0.66). The observed prevalence of AF increased progressively across these groups, from 21.7% in the low-risk category to 53.3% in the intermediate-risk category and 82.3% in the high-risk category, demonstrating good discriminatory performance of the model.
Figure 1.
ROC curve of the predictive model for AF in patients with HFpEF and HFmrEF. AUC – area under the curve.
Figure 1.
ROC curve of the predictive model for AF in patients with HFpEF and HFmrEF. AUC – area under the curve.

Figure 2.
Observed AF prevalence according to predicted risk categories. AF – atrial fibrillation.

4. Discussion
4.1. Main Findings of the Study
The present study provides a comprehensive evaluation of clinical, laboratory and echocardiographic predictors of AF in patients with HF across different phenotypes. The main findings can be summarized as follows. First, patients with HFpEF demonstrated the broadest spectrum of factors associated with AF, including demographic characteristics, renal function parameters, hemodynamic variables, and markers of atrial remodeling. Second, in HFmrEF the risk profile was more limited and mainly related to age, heart rate, and LA enlargement. Third, in HFrEF the determinants of AF were predominantly associated with indices of ventricular geometry rather than atrial parameters. Finally, multivariate analysis confirmed that the predictors of AF differ substantially between HF phenotypes, suggesting distinct pathophysiological mechanisms underlying the development of AF in these patient populations.
Although the main focus of the present study was on HFpEF and HFmrEF, HFrEF was included in the analysis as a clinically relevant comparative phenotype rather than as the primary target population. The use of HFrEF as a comparator was considered methodologically more appropriate than the inclusion of healthy controls, since both HF and AF represent complex clinical syndromes that arise in the context of aging, cardiovascular remodeling, and multimorbidity. In this setting, comparison with another HF phenotype provides a more meaningful pathophysiological reference than comparison with individuals without structural heart disease.
Importantly, this approach allowed us to demonstrate that patients with HFpEF and HFmrEF carry a substantial burden of comorbidities and thromboembolic and bleeding risk markers, as reflected by elevated CHA₂DS₂-VA and HAS-BLED scores. These findings suggest that patients with HFpEF and HFmrEF should not be considered clinically lower-risk populations, as their risk profile may be comparable to that observed in HFrEF. At the same time, the determinants of AF appear to vary across HF phenotypes, underscoring the importance of phenotype-specific risk assessment.
For this reason, the predictive modeling in the present study was intentionally focused on HFpEF and HFmrEF. These phenotypes remain less well characterized with regard to AF prediction despite their rapidly increasing prevalence in contemporary clinical practice, their older age profile, and their high burden of multimorbidity. Furthermore, AF in HFpEF and HFmrEF appears to be more closely related to atrial remodeling, diastolic dysfunction, and systemic comorbidities, whereas in HFrEF the arrhythmic substrate may be influenced more strongly by ventricular remodeling and advanced systolic dysfunction. Focusing the predictive analysis on HFpEF and HFmrEF therefore addresses an important knowledge gap and may facilitate earlier identification of patients who could benefit from intensified rhythm monitoring.
4.2. Interpretation of Predictors in HFpEF
In the present study, HFpEF was characterized by the most complex pattern of associations with AF. Several demographic, clinical, and echocardiographic parameters were identified as independent predictors, including age, male sex, heart rate, reduced renal function, lower systolic BP, and LA enlargement, as well as the presence of moderate or severe tricuspid regurgitation. Among these variables, LA size emerged as one of the most consistent predictors, which is in line with the well-established role of atrial structural remodeling in the pathogenesis of AF.
The strong association between tricuspid regurgitation and AF observed in our cohort may reflect the combined effects of atrial dilation, pulmonary hypertension, and right-sided cardiac remodeling, which are frequently encountered in patients with HFpEF. Similarly, impaired renal function and increased heart rate may represent markers of systemic disease burden and neurohormonal activation, both of which are known contributors to arrhythmogenesis.
Interestingly, metabolic syndrome demonstrated an inverse independent association with AF in our model. Although metabolic abnormalities are generally considered pro-arrhythmic, similar paradoxical associations have been reported in some observational studies, potentially reflecting reverse epidemiology phenomena described in cardiometabolic disease [35,36,37,38]. One possible explanation is that differences in body composition, metabolic reserve, and systemic inflammatory profiles may influence atrial structural remodeling and electrophysiological substrate in a phenotype-dependent manner. In addition, residual confounding, competing risks, and heterogeneity within metabolic syndrome components may partly account for these unexpected associations.
4.3. Predictors of AF in HFmrEF
In patients with HFmrEF, the spectrum of predictors associated with AF was more limited compared with HFpEF. In both univariate and multivariate analyses, LA size emerged as the only independent predictor of AF. This finding suggests that atrial structural remodeling plays a particularly central role in the development of AF in this intermediate HF phenotype.
HFmrEF is increasingly recognized as a transitional phenotype between HFpEF and HFrEF, characterized by a heterogeneous pathophysiological background. In this context, LA enlargement may represent an integrative marker reflecting the cumulative impact of chronic diastolic dysfunction, elevated filling pressures, and systemic comorbidity burden. The strong association between atrial size and AF observed in this subgroup supports the concept that atrial remodeling is a key determinant of arrhythmogenesis in patients with HFmrEF.
4.4. Predictors of AF in HFrEF
In contrast to HFpEF and HFmrEF, the determinants of AF in HFrEF were primarily related to indices of ventricular geometry rather than atrial parameters. In multivariate analysis, left ventricular end-diastolic volume emerged as the only independent predictor of AF. This observation suggests that ventricular remodeling and advanced systolic dysfunction may play a dominant role in the arrhythmic substrate of AF in this phenotype.
These findings are consistent with the well-established pathophysiological model of AF development in HFrEF, where ventricular dilation, elevated filling pressures, and neurohormonal activation contribute to progressive atrial structural and electrical remodeling. In this setting, ventricular parameters may indirectly reflect the severity of myocardial disease and its impact on atrial hemodynamics.
4.5. Comparison with Previous Studies
The results of the present study are broadly consistent with previous investigations demonstrating a strong relationship between atrial remodeling and the occurrence of AF in HF patients. LA enlargement has repeatedly been identified as one of the most robust predictors of AF across different cardiovascular populations, including patients with HFpEF and HFmrEF.
Several studies have highlighted the role of advanced age and systemic comorbidities as important contributors to AF development in patients with HF [1,39,40,41]. In particular, data from the CHART-2 registry demonstrated that advanced age is a strong independent predictor of incident AF and its progression in patients with HFpEF [42]. Our findings are consistent with these observations, showing that older age, reduced renal function and higher heart rate were independently associated with AF in this population. These factors may collectively reflect a more advanced stage of systemic and cardiac remodeling, characterized by increased atrial pressure and volume overload, neurohormonal activation and progressive atrial structural changes that facilitate atrial arrhythmogenesis, particularly in the HFpEF phenotype [1,39,40,41,42].
At the same time, the phenotype-specific differences observed in our analysis suggest that the mechanisms underlying AF may vary substantially across HF phenotypes. Previous studies have shown that in HFpEF and HFmrEF the development of AF is largely driven by atrial remodeling associated with chronically elevated filling pressures, atrial dilation and myocardial fibrosis [13,17,27,43]. In contrast, in HFrEF the arrhythmogenic substrate may be more closely related to advanced ventricular remodeling and systolic dysfunction, which secondarily contribute to atrial dilation and electrical instability [13,28,44]. Our findings are consistent with these observations and further support the concept that the determinants of AF may differ between HF phenotypes, emphasizing the importance of considering HF phenotype when evaluating AF risk and when developing predictive models.
4.6. Clinical Implications
The identification of phenotype-specific predictors of AF has several potential clinical implications. Early identification of patients at increased risk of AF may facilitate more targeted rhythm monitoring strategies, particularly in populations where AF may remain clinically silent for prolonged periods.
In patients with HFpEF and HFmrEF, the strong association between AF and left atrial enlargement suggests that echocardiographic assessment of atrial size may serve as a practical tool for risk stratification in routine clinical practice. Similarly, readily available clinical variables such as age, heart rate, renal function, and blood pressure may help identify patients who could benefit from intensified electrocardiographic surveillance.
Importantly, the predictive model developed in the present study demonstrated good discriminative ability, with an AUC approaching 0.8 in the combined HFpEF/HFmrEF cohort. The ability of the model to stratify patients into distinct risk categories further supports its potential clinical utility. Patients classified as high risk may benefit from closer rhythm monitoring, prolonged ambulatory ECG monitoring, and earlier consideration of anticoagulation therapy once AF is documented.
Based on the developed multivariable model, a pragmatic clinical algorithm for AF (AF) risk stratification in patients with HFpEF and HFmrEF was proposed (Figure 3). The model demonstrated good discriminative performance (AUC = 0.789) and allows practical classification of patients into three risk categories: low, intermediate, and high risk. The proposed surveillance intervals represent a pragmatic protocol aligned with current recommendations for AF screening and with the available modalities for ambulatory ECG rhythm monitoring.
In patients with a low a priori probability of AF, routine prolonged monitoring has limited diagnostic yield; therefore, an opportunistic screening approach based on periodic 12-lead ECG and symptom-triggered Holter monitoring appears methodologically justified. In patients with intermediate risk, more frequent ECG assessment and periodic ambulatory ECG monitoring are appropriate, as current recommendations allow Holter monitoring ranging from 24 hours to several days. In the high-risk group, the main objective is to reduce the time to detection of paroxysmal or subclinical AF. Prolonged ambulatory rhythm monitoring increases the probability of detecting arrhythmic episodes, while contemporary guidelines recognize extended monitoring strategies, including patch monitoring up to 14 days, as valid screening tools. Regardless of risk category, ambulatory rhythm monitoring should be performed immediately in the presence of symptoms or clinical suspicion of AF.
4.7. Highlights
Phenotype-specific predictors of AF differ across HF phenotypes.
- HFpEF demonstrates the most complex network of clinical and echocardiographic determinants of AF.
- LA enlargement is the most consistent predictor of AF in HFpEF and HFmrEF.
- A multivariable model combining clinical and echocardiographic parameters showed good predictive performance (AUC ≈ 0.79).
- Risk stratification based on predicted probability effectively discriminated low-, intermediate-, and high-risk groups for AF.
4.8. Strengths and Limitations
Several strengths of the present study should be acknowledged. First, the analysis was based on a relatively large real-world cohort of hospitalized patients with chronic HF. Second, the study included a comprehensive evaluation of demographic, clinical, laboratory, echocardiographic, and therapeutic variables, allowing for a detailed assessment of potential predictors of AF. Third, the analysis was performed separately for different HF phenotypes, which enabled the identification of phenotype-specific predictors and improved the clinical interpretability of the findings.
However, several limitations should also be considered. The retrospective and single-center design of the study may limit the generalizability of the results. In addition, the diagnosis of AF was based on electrocardiographic documentation during hospitalization or available clinical records, which may have led to underdetection of asymptomatic or paroxysmal AF episodes. Furthermore, external validation of the predictive model in independent cohorts would be necessary before its broader clinical implementation.
5. Conclusions
In patients with HF, the predictors of AF differ substantially across HF phenotypes. In the present study, HFpEF was characterized by the most complex pattern of clinical and echocardiographic determinants, including advanced age, male sex, higher heart rate, reduced renal function, lower systolic BP, LA enlargement, and significant tricuspid regurgitation. In contrast, AF in HFmrEF was primarily associated with LA remodeling, whereas in HFrEF ventricular geometry emerged as the main determinant.
These findings suggest that the mechanisms underlying AF differ between HF phenotypes and highlight the importance of phenotype-specific risk assessment. The predictive model developed for patients with HFpEF and HFmrEF demonstrated good discriminative ability and allowed stratification of patients into clinically meaningful AF risk categories. Early identification of patients at increased risk of AF using readily available clinical and echocardiographic parameters may facilitate more targeted rhythm monitoring and improve risk stratification in these increasingly prevalent HF populations.
Author Contributions
Conceptualization, M.M., I.G. and S.N.; methodology, M.M. and S.N; validation, I.G. and S.N., formal analysis, M.M. and S.N; investigation, M.M., I.G. and S.N.; resources, M.M., I.G. and S.N.; data curation, S.N.; writing—original draft preparation, M.M.; writing—review and editing, S.N.; visualization, S.N.; supervision, I.G.; project administration, S.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Ethical review and approval were waived due to the retrospective and non-interventional nature of the study and the use of fully anonymized clinical data, in accordance with applicable national regulations and institutional policies.
Informed Consent Statement
The requirement for informed patient consent was waived due to the retrospective and non-interventional design of the study and the use of fully anonymized clinical data, in accordance with applicable national regulations and institutional policies governing research involving human participants.
Data Availability Statement
The data supporting the results of this study are available from Stefan Naydenov (snaydenov@gmail.com) upon reasonable request, subject to applicable ethical and privacy restrictions.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AF | Atrial fibrillation |
| BP | Blood pressure |
| eGFR | Estimated glomerular filtration rate |
| ECG | Electrocardiography |
| ESC | European Society of Cardiology |
| HF | Heart failure |
| HFmrEF | Heart failure with mildly reduced ejection fraction |
| HFpEF | Heart failure with preserved ejection fraction |
| HFrEF | Heart failure with reduced ejection fraction |
| LA | Left atrial |
| LV | Left ventricular |
| LVEF | Left ventricular ejection fraction |
References
- Van Gelder IC, Rienstra M, Bunting KV, Casado-Arroyo R, Caso V, Crijns HJGM; et al. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). European Heart Journal. 2024 Sep 29;45(36):3314–414. [CrossRef]
- Joglar JA, Chung MK, Armbruster AL, Benjamin EJ, Chyou JY, Cronin EM; et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024 Jan 2;149(1). [CrossRef]
- Karatela MF, Calkins H. The Global Impact of Atrial Fibrillation. Arrhythm Electrophysiol Rev. 2025 Nov 8;14:e28. [CrossRef]
- Alexander B, Tse G, Martinez-Selles M, Baranchuk A. Atrial Conduction Disorders. CCR. 2021 Jan;17(1):68–73. [CrossRef]
- Lippi G, Sanchis-Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: An increasing epidemic and public health challenge. International Journal of Stroke. 2021 Feb;16(2):217–21. [CrossRef]
- Zhang X, Chen Y, Hu W, Lu S, Yu H, Sun Y. Global burden of atrial fibrillation/atrial flutter and its attributable risk factors in adolescents and young adults, 1990–2021: Insights from the global burden of disease study. Annals of Medicine. 2025 Dec 31;57(1):2543524. [CrossRef]
- Bassand JP, Apenteng PN, Atar D, Camm AJ, Cools F, Corbalan R; et al. GARFIELD-AF: A Worldwide Prospective Registry of Patients With Atrial Fibrillation at Risk of Stroke. Future Cardiol. 2021 Jan;17(1):19–38. [CrossRef]
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European Heart Journal. 2021 Sep 21;42(36):3599–726. [CrossRef]
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M; et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European Heart Journal. 2023 Oct 1;44(37):3627–39. [CrossRef]
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022 May 3;145(18). [CrossRef]
- Jia Z, Du X. Epidemiology and Burden of Heart Failure. Cardiology Discovery. 2025 Dec;5(4):281–4. [CrossRef]
- Bidaoui G, Assaf A, Marrouche N. Atrial Fibrillation in Heart Failure: Novel Insights, Challenges, and Treatment Opportunities. Curr Heart Fail Rep. 2025 Dec;22(1):3. [CrossRef]
- Gorczyca-Głowacka I, Galas A, Tymińska A, Byczkowska K, Furman-Niedziejko A, Tkaczyszyn M; et al. Atrial fibrillation in patients with heart failure with reduced, mildly reduced, and preserved ejection fraction: A report from the HEart failuRe ObsErvational Study (HEROES). Pol Heart J. 2025 Jun 30;83(6):701–8. [CrossRef]
- Corica B, Romiti GF, Proietti M, Boriani G, Olshansky B, Huisman MV; et al. Heart failure in patients with recently diagnosed atrial fibrillation: Findings from the GLORIA-AF Registry Phase III. European Journal of Preventive Cardiology. 2025 Sep 1;zwaf485. [CrossRef]
- Xia Y, Jiang J, Fan F, Pan Y, Zhou J, Zhang Y; et al. Prevalence, Characteristics, and Treatment Strategy of Different Types of Heart Failure in Patients With Nonvalvular Atrial Fibrillation. JAHA. 2024 Oct;13(19):e033941. [CrossRef]
- Bozkurt B, Ahmad T, Alexander K, Baker WL, Bosak K, Breathett K; et al. HF STATS 2024: Heart Failure Epidemiology and Outcomes Statistics An Updated 2024 Report from the Heart Failure Society of America. Journal of Cardiac Failure. 2025 Jan;31(1):66–116. [CrossRef]
- Gori M, Iacovoni A, Senni M. Haemodynamics of Heart Failure With Preserved Ejection Fraction: A Clinical Perspective. Cardiac Failure Review. 2016. [CrossRef]
- Savarese G, Stolfo D, Sinagra G, Lund LH. Heart failure with mid-range or mildly reduced ejection fraction. Nat Rev Cardiol. 2022 Feb;19(2):100–16. [CrossRef]
- Saksena S, Slee A, Nagarakanti R, Atul Prakash. Atrial Fibrillation (AF) and Heart Failure With Preserved Ejection Fraction (HFpEF): Advances and Challenges. Cardiovasc electrophysiol. 2025 Oct;36(10):2720–45. [CrossRef]
- Ariyaratnam JP, Elliott AD, Mishima RS, Gallagher C, Lau DH, Sanders P. Heart failure with preserved ejection fraction: An alternative paradigm to explain the clinical implications of atrial fibrillation. Heart Rhythm O2. 2021 Dec;2(6):771–83. [CrossRef]
- Gorter TM, Van Veldhuisen DJ, Mulder BA, Artola Arita VA, Van Empel VPM, Manintveld OC; et al. Prevalence and Incidence of Atrial Fibrillation in Heart Failure with Mildly Reduced or Preserved Ejection Fraction: (Additive) Value of Implantable Loop Recorders. JCM. 2023 May 26;12(11):3682. [CrossRef]
- Patel RB, Greene SJ, Xu H, Alhanti B, Peterson P, Yancy CW; et al. Intersection of Atrial Fibrillation and Heart Failure with Mildly Reduced and Preserved Ejection Fraction in >400 000 Participants in the Get With The Guidelines-Heart Failure Registry. European Journal of Heart Failure. 2023 Jan 1;25(1):63–73. [CrossRef]
- Chousou PA, Chattopadhyay R, Tsampasian V, Vassiliou VS, Pugh PJ. Electrocardiographic Predictors of Atrial Fibrillation. Medical Sciences. 2023 Apr 7;11(2):30. [CrossRef]
- Nguyen KT, Vittinghoff E, Dewland TA, Mandyam MC, Stein PK, Soliman EZ; et al. Electrocardiographic Predictors of Incident Atrial Fibrillation. The American Journal of Cardiology. 2016 Sep;118(5):714–9. [CrossRef]
- Atabekov T, Batalov R, Archakov E, Silivanova I, Khlynin M, Kisteneva I; et al. Predictors of Atrial Fibrillation in Heart Failure Patients with Indications for ICD Implantation. JCM. 2025 Jun 18;14(12):4358. [CrossRef]
- Park JJ, Park JH, Hwang IC, Park JB, Cho GY, Marwick TH. Left Atrial Strain as a Predictor of New-Onset Atrial Fibrillation in Patients With Heart Failure. JACC: Cardiovascular Imaging. 2020 Oct;13(10):2071–81. [CrossRef]
- O’Neal WT, Sandesara P, Patel N, Venkatesh S, Samman-Tahhan A, Hammadah M; et al. Echocardiographic predictors of atrial fibrillation in patients with heart failure with preserved ejection fraction. European Heart Journal - Cardiovascular Imaging. 2017 Jul 1;18(7):725–9. [CrossRef]
- Boehmer AA, Ehrlich JR, Nattel S. Atrial Fibrillation and Heart Failure With Reduced Ejection Fraction. JACC: Clinical Electrophysiology. 2025 Dec;11(12):2774–90. [CrossRef]
- A. Al-Shoaibi N, Y. Ashram W, T. Mokhtar A, K. Arfaj Y, G. Alnahari D, S. Ibrahim R; et al. Non-genetic Risk Factors for Atrial Fibrillation in Individuals Aged 60 and Above. J Pioneering Med Sci. 2025 Oct 5;14(09):1–5. [CrossRef]
- Chen M, Ding N, Mok Y, Mathews L, Hoogeveen RC, Ballantyne CM; et al. Growth Differentiation Factor 15 and the Subsequent Risk of Atrial Fibrillation: The Atherosclerosis Risk in Communities Study. Clinical Chemistry. 2022 Jul 27;68(8):1084–93. [CrossRef]
- Bertoni M1*, Traini AM2, Celli A3, Bini C1, Bracciali A1, Foretic M1 and Di Natale ME. Galectin-3 in Heart Failure with Preserved Ejection Fraction and Persistent Atrial Fibrillation Versus Sinus Rhythm. Correlation with Left Atrial Volume and N-Terminal Pro B-Type Natriuretic Peptide [Internet]. Available from: https://austinpublishinggroup.com/cardiovascular-disorders/fulltext/jcd-v7-id1043.php.
- Ianos RD, Iancu M, Pop C, Lucaciu RL, Hangan AC, Rahaian R; et al. Predictive Value of NT-proBNP, FGF21, Galectin-3 and Copeptin in Advanced Heart Failure in Patients with Preserved and Mildly Reduced Ejection Fraction and Type 2 Diabetes Mellitus. Medicina. 2024 Nov 8;60(11):1841. [CrossRef]
- Lancellotti P, Cosyns B, editors. Examination. In: The EACVI Echo Handbook [Internet]. 1st ed. Oxford University PressOxford; 2015 [cited 2026 Mar 8]. p. 1–14. Available from: https://academic.oup.com/esc/book/40751/chapter/348644852. [CrossRef]
- Stevens PE, Ahmed SB, Carrero JJ, Foster B, Francis A, Hall RK; et al. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International. 2024 Apr;105(4):S117–314. [CrossRef]
- Sagris D, Harrison SL, Lip GYH. Lipids and atrial fibrillation: New insights into a paradox. PLoS Med. 2022 Aug 11;19(8):e1004067. [CrossRef]
- Wang TJ. Obesity and the Risk of New-Onset Atrial Fibrillation. JAMA. 2004 Nov 24;292(20):2471. [CrossRef]
- Sandhu RK, Ezekowitz J, Andersson U, Alexander JH, Granger CB, Halvorsen S; et al. The ‘obesity paradox’ in atrial fibrillation: Observations from the ARISTOTLE (Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation) trial. Eur Heart J. 2016 Oct 7;37(38):2869–78. [CrossRef]
- Carbone S, Canada JM, Billingsley HE, Siddiqui MS, Elagizi A, Lavie CJ. Obesity paradox in cardiovascular disease: Where do we stand? VHRM. 2019 May;Volume 15:89–100. [CrossRef]
- Cheng Y, Deng H, Wei H, Lin W, Liang Z, Chen Y; et al. Association Between Age at Diagnosis of Atrial Fibrillation and Subsequent Risk of Ischemic Stroke. JAHA. 2025 Feb 18;14(4):e038367. [CrossRef]
- Nieuwlaat R, Eurlings LW, Cleland JG, Cobbe SM, Vardas PE, Capucci A; et al. Atrial Fibrillation and Heart Failure in Cardiology Practice: Reciprocal Impact and Combined Management From the Perspective of Atrial Fibrillation. Journal of the American College of Cardiology. 2009 May;53(18):1690–8. [CrossRef]
- Zafrir B, Lund LH, Laroche C, Ruschitzka F, Crespo-Leiro MG, Coats AJS; et al. Prognostic implications of atrial fibrillation in heart failure with reduced, mid-range, and preserved ejection fraction: A report from 14 964 patients in the European Society of Cardiology Heart Failure Long-Term Registry. European Heart Journal. 2018 Dec 21;39(48):4277–84. [CrossRef]
- Ito T, Noda T, Nochioka K, Shiroto T, Yamamoto N, Sato H; et al. Clinical impact of atrial fibrillation progression in patients with heart failure with preserved ejection fraction: A report from the CHART-2 Study. Europace. 2024 Aug 30;26(9):euae218. [CrossRef]
- Chen P, Yin X, Ren L. Construction and validation of a predictive model for the risk of atrial fibrillation in patients with heart failure with preserved ejection fraction: A single-center retrospective analysis. BMC Cardiovasc Disord. 2025 Dec 23;25(1):873. [CrossRef]
- Gopinathannair R, Chen LY, Chung MK, Cornwell WK, Furie KL, Lakkireddy DR; et al. Managing Atrial Fibrillation in Patients With Heart Failure and Reduced Ejection Fraction: A Scientific Statement From the American Heart Association. Circ: Arrhythmia and Electrophysiology. 2021 Jul;14(7). [CrossRef]
Figure 3.
Proposed clinical algorithm for AF risk prediction and rhythm surveillance in patients with HFpEF and HFmrEF. The algorithm is derived from a multivariable predictive model incorporating clinical and echocardiographic parameters associated with AF in the studied population. Based on the estimated individual probability of AF, patients are stratified into three risk categories (low, intermediate, and high risk), which guide the recommended intensity and frequency of electrocardiographic and ambulatory rhythm monitoring. This pragmatic framework illustrates a potential clinical application of the proposed model and may serve as a basis for future external validation and implementation in routine practice.
Figure 3.
Proposed clinical algorithm for AF risk prediction and rhythm surveillance in patients with HFpEF and HFmrEF. The algorithm is derived from a multivariable predictive model incorporating clinical and echocardiographic parameters associated with AF in the studied population. Based on the estimated individual probability of AF, patients are stratified into three risk categories (low, intermediate, and high risk), which guide the recommended intensity and frequency of electrocardiographic and ambulatory rhythm monitoring. This pragmatic framework illustrates a potential clinical application of the proposed model and may serve as a basis for future external validation and implementation in routine practice.


Table 1.
Demographic and epidemiological characteristics of the study population according to HF phenotype.
Table 1.
Demographic and epidemiological characteristics of the study population according to HF phenotype.
| Variable | HFpEF (n = 487; 69.6%) | HFmrEF (n = 106; 15.1%) | HFrEF (n = 107; 15.3%) | Total (n = 700) | p-value |
|---|---|---|---|---|---|
| Sex, n (%) | |||||
| Male | 179 (36.7%) | 64 (60.4%) | 70 (65.4%) | 313 (44.7%) | <0.001 |
| Female | 308 (63.3%) | 42 (39.6%) | 37 (34.6%) | 387 (55.3%) | |
| Age, median (IQR), years | 73 (67–80) | 73 (67–78) | 74 (65–83) | 74 (66–80) | 0.738 |
| Age group, n (%) | |||||
| <40 years | 0 (0%) | 0 (0%) | 1 (0.9%) | 2 (0.3%) | |
| 40–49 years | 0 (0%) | 0 (0%) | 1 (0.9%) | 15 (2.1%) | |
| 50–59 years | 9 (1.8%) | 3 (2.8%) | 3 (2.8%) | 65 (9.3%) | 0.051 |
| 60–69 years | 45 (9.2%) | 8 (7.5%) | 12 (11.2%) | 177 (25.3%) | |
| 70–79 years | 120 (24.6%) | 28 (26.4%) | 29 (27.1%) | 277 (39.6%) | |
| ≥80 years | 196 (40.2%) | 50 (47.2%) | 31 (29.0%) | 164 (23.4%) | |
| COVID-19 period, n (%) | |||||
| Before the pandemic | 210 (43.1%) | 54 (50.9%) | 40 (37.4%) | 304 (43.4%) | 0.132 |
| After the pandemic | 277 (56.9%) | 52 (49.1%) | 67 (62.6%) | 396 (56.6%) |
HFpEF—heart failure with preserved ejection fraction; HFmrEF—heart failure with mildly reduced ejection fraction; HFrEF—heart failure with reduced ejection fraction; IQR—interquartile range.
Table 2.
Clinical characteristics of the study population according to HF phenotype.
| Variable | HFpEF (n = 487; 69.6%) | HFmrEF (n = 106; 15.1%) | HFrEF (n = 107; 15.3%) | Total (n = 700) | p-value |
|---|---|---|---|---|---|
| HF duration before study inclusion, median (IQR), years | 1 (1–2) | 1 (1–4) | 1 (1–4) | 1 (1–3) | 0.077 |
| NYHA functional class, n (%) | |||||
| NYHA II | 12 (2.5%) | 1 (0.9%) | 0 (0.0%) | 13 (1.9%) | <0.001 |
| NYHA III | 474 (97.3%) | 105 (99.1%) | 101 (94.4%) | 680 (97.1%) | |
| NYHA IV | 1 (0.2%) | 0 (0%) | 6 (5.6%) | 7 (1.0%) | |
| Heart rhythm, n (%) | |||||
| Sinus rhythm | 249 (51.1%) | 33 (31.1%) | 35 (32.7%) | 317 (45.3%) | |
| Paroxysmal AF | 50 (10.3%) | 10 (9.4%) | 6 (5.6%) | 66 (9.4%) | |
| Persistent AF | 91 (18.7%) | 27 (25.5%) | 23 (21.5%) | 141 (20.1%) | <0.001 |
| Long-standing persistent AF | 1 (0.2%) | 0 (0%) | 0 (0%) | 1 (0.1%) | |
| Permanent AF | 96 (19.7%) | 36 (34.0%) | 43 (40.2%) | 175 (25.0%) |
HFpEF—heart failure with preserved ejection fraction; HFmrEF—heart failure with mildly reduced ejection fraction; HFrEF—heart failure with reduced ejection fraction; NYHA—New York Heart Association; AF—atrial fibrillation; IQR—interquartile range.
Table 3.
Comorbidity profile and cardiovascular risk factors according to HF phenotype.
| Variable | HFpEF (n = 487; 69.6%) | HFmrEF (n = 106; 15.1%) | HFrEF (n = 107; 15.3%) | Total (n = 700) | p-value |
|---|---|---|---|---|---|
| Arterial hypertension | 476 (97.7%) | 102 (96.2%) | 97 (90.7%) | 675 (96.4%) | 0.596 |
| Dyslipidemia | 163 (33.5%) | 33 (31.1%) | 39 (36.8%) | 235 (33.6%) | 0.678 |
| Impaired glucose metabolism | 8 (1.6%) | 1 (0.9%) | 0 (0%) | 9 (1.3%) | 0.834 |
| Impaired glucose tolerance/ impaired fasting glucose | |||||
| Type 2 diabetes mellitus | 142 (29.2%) | 34 (32.1%) | 26 (24.3%) | 202 (28.9%) | |
| Type 1 diabetes mellitus | 5 (1.0%) | 3 (2.8%) | 1 (0.9%) | 9 (1.3%) | |
| Metabolic syndrome | 27 (5.5%) | 2 (1.9%) | 3 (2.8%) | 32 (4.6%) | 0.167 |
| Weight disorders* | |||||
| Overweight | 14 (2.9%) | 1 (0.9%) | 1 (0.9%) | 16 (2.3%) | 0.330 |
| Obesity | 78 (16.0%) | 13 (12.3%) | 14 (13.1%) | 105 (15.0%) | |
| Coronary artery disease | 144 (29.6%) | 45 (42.5%) | 43 (40.2%) | 232 (30.1%) | 0.009 |
| Valvular heart disease# | 468 (96.3%) | 104 (98.1%) | 105 (98.1%) | 677 (96.9%) | 0.455 |
| Congenital heart disease | 2 (0.4%) | 1 (0.9%) | 0 (0%) | 3 (0.4%) | 0.572 |
| Chronic kidney disease | 93 (19.1%) | 23 (21.7%) | 34 (31.8%) | 150 (21.6%) | 0.015 |
| Cerebrovascular disease | 105 (21.6%) | 22 (20.8%) | 31 (29.0%) | 158 (22.6%) | 0.224 |
| Peripheral arterial disease | 0 (0%) | 0 (0%) | 2 (1.9%) | 2 (0.3%) | 0.004 |
| Prior cardiac surgery | 74 (15.2%) | 26 (24.5%) | 33 (30.8%) | 133 (19.0%) | <0.001 |
| Thyroid disease | 84 (17.3%) | 17 (16.0%) | 20 (18.7%) | 121 (17.3%) | 0.876 |
| Chronic pulmonary disease^ | 111 (22.8%) | 25 (23.6%) | 25 (23.4%) | 161 (23.0%) | 0.998 |
| Obstructive sleep apnea | 16 (3.3%) | 6 (5.7%) | 5 (4.7%) | 27 (3.9%) | 0.700 |
| Smoking status | |||||
| Active smoker | 63 (12.9%) | 21 (19.8%) | 19 (17.8%) | 103 (14.7%) | |
| Former smoker | 59 (12.1%) | 20 (18.9%) | 15 (14.0%) | 94 (13.4%) | 0.060 |
HFpEF—heart failure with preserved ejection fraction; HFmrEF—heart failure with mildly reduced ejection fraction; HFrEF—heart failure with reduced ejection fraction; * obesity — BMI ≥30.0 kg/m², overweight — BMI 25.0–29.9 kg/m²; # moderate or severe valvular lesions; ^ chronic obstructive pulmonary disease and other chronic pulmonary disorders.
Table 4.
Distribution of the CHA₂DS₂-VA score according to HF phenotype and cardiac rhythm.
| HF Phenotype | Cardiac Rhythm | n (%) | CHA₂DS₂-VA score, median (IQR), points |
p-value |
|---|---|---|---|---|
| HFpEF (≥50%) | Paroxysmal AF | 50 (10.3%) | 4 (3–5) | |
| Persistent AF | 91 (18.7%) | 3 (3–5) | ||
| Long-standing persistent AF | 1 (0.2%) | 4 (4–4) | ||
| Permanent AF | 96 (19.7%) | 4 (3–5) | ||
| HFmrEF (41–49%) | Paroxysmal AF | 10 (9.4%) | 3 (2.8–5) | 0.568 |
| Persistent AF | 27 (25.5%) | 4 (2–5) | ||
| Permanent AF | 36 (34.0%) | 4 (3–5) | ||
| HFrEF (≤40%) | Paroxysmal AF | 6 (5.6%) | 2.5 (1.5–4) | |
| Persistent AF | 23 (21.5%) | 3 (2–5) | ||
| Permanent AF | 43 (40.2%) | 4 (3–5) |
HFpEF—heart failure with preserved ejection fraction; HFmrEF—heart failure with mildly reduced ejection fraction; HFrEF—heart failure with reduced ejection fraction; AF—atrial fibrillation; IQR—interquartile range.
Table 5.
Distribution of the HAS-BLED score according to HF phenotype and cardiac rhythm.
| HF Phenotype | Cardiac Rhythm | n (%) | HAS-BLED score, median (IQR), points |
p-value |
|---|---|---|---|---|
| HFpEF (≥50%) | Paroxysmal AF | 50 (10.3%) | 2 (2–2) | |
| Persistent AF | 91 (18.7%) | 2 (1–2) | ||
| Long-standing persistent AF | 1 (0.2%) | 1 (1–1) | ||
| Permanent AF | 96 (19.7%) | 2 (2–3) | ||
| HFmrEF (41–49%) | Paroxysmal AF | 10 (9.4%) | 2 (1–2.25) | 0.523 |
| Persistent AF | 27 (25.5%) | 2 (2–2) | ||
| Permanent AF | 36 (34.0%) | 2 (2–3) | ||
| HFrEF (≤40%) | Paroxysmal AF | 6 (5.6%) | 1.5 (0.75–2.75) | |
| Persistent AF | 23 (21.5%) | 2 (1–3) | ||
| Permanent AF | 43 (40.2%) | 2 (2–2) |
HFpEF—heart failure with preserved ejection fraction; HFmrEF—heart failure with mildly reduced ejection fraction; HFrEF—heart failure with reduced ejection fraction; AF—atrial fibrillation; IQR—interquartile range.
Table 6.
Hemodynamic and anthropometric characteristics of the study population according to HF phenotype.
Table 6.
Hemodynamic and anthropometric characteristics of the study population according to HF phenotype.
| Variable | HFpEF (n = 487) | HFmrEF (n = 106) | HFrEF (n = 107) | Total | p-value |
|---|---|---|---|---|---|
| Office systolic BP, median (IQR), mmHg | 135 (120–150) | 130 (120–150) | 125 (110.5–140) | 130 (120–150) | 0.002 |
| Office diastolic BP, median (IQR), mmHg | 80 (75–90) | 80 (75–90) | 80 (70–90) | 80 (75–90) | 0.530 |
| Body mass index, median (IQR), kg/m² | 31 (28–33.75) | 30 (29.25–30.75) | 37 (24.5–41.7) | 31 (28–35) | 0.525 |
| Heart rate, mean ± SD, bpm | 78.3 ± 17.6 | 85.1 ± 20.4 | 89.3 ± 22.9 | 81.0 ± 19.4 | <0.001 |
BP – blood pressure; HFpEF—heart failure with preserved ejection fraction; HFmrEF—heart failure with mildly reduced ejection fraction; HFrEF—heart failure with reduced ejection fraction; IQR—interquartile range; SD—standard deviation; bpm—beats per minute.
Table 7.
Laboratory characteristics of the study population according to HF phenotype.
| Variable | HFpEF (n = 487) | HFmrEF (n = 106) | HFrEF (n = 107) | Total (n = 700) | p-value |
|---|---|---|---|---|---|
| Potassium (K), mmol/L, median (IQR) | 4.00 (4.00–4.91) | 4.00 (4.00–4.75) | 4.00 (4.00–5.00) | 4.00 (4.00–4.97) | 0.691 |
| Sodium (Na), mmol/L, median (IQR) | 141 (138–143) | 141 (138–143) | 140 (138–143) | 141 (138–143) | 0.038 |
| Hemoglobin (Hb), g/L, median (IQR) | 137 (123–147) | 134 (121–148) | 134 (120–146) | 136 (122–147) | 0.673 |
| Creatinine, µmol/L, median (IQR) | 90 (74–112) | 100 (81.5–131) | 108 (86–156) | 93 (77–117) | 0.341 |
| eGFR, mL/min/1.73 m², median (IQR) | 65 (50–85) | 57 (43–85) | 56 (34–73.3) | 62 (45–84) | 0.037 |
eGFR — estimated glomerular filtration rate calculated using the CKD-EPI equation [34]; HFpEF—heart failure with preserved ejection fraction; HFmrEF—heart failure with mildly reduced ejection fraction; HFrEF—heart failure with reduced ejection fraction; IQR—interquartile range;.
Table 8.
Echocardiographic characteristics of the study population according to heart failure phenotype.
Table 8.
Echocardiographic characteristics of the study population according to heart failure phenotype.
| Variable | HFpEF (n = 487) | HFmrEF (n = 106) | HFrEF (n = 107) | p-value |
|---|---|---|---|---|
| LA size, parasternal long-axis view (mm), median (IQR) | 42 (38–47) | 45 (41.5–50) | 48 (43.5–53.5) | <0.001 |
| LA longitudinal diameter, apical four-chamber view (mm), median (IQR) | 54 (50–62) | 59 (53–63.5) | 62 (55.25–69) | <0.001 |
| Interventricular septal thickness, parasternal long-axis view (mm), median (IQR) | 12 (11–13) | 12 (11–13) | 12 (11–13) | 0.003 |
| Posterior LV wall thickness, parasternal long-axis view (mm), median (IQR) | 12 (11–12) | 12 (11–12) | 11 (10–12) | 0.005 |
| LV end-diastolic diameter, parasternal long-axis view (mm), median (IQR) | 48 (44–52) | 52 (46–59) | 57 (51–62) | <0.001 |
| LV end-systolic diameter, parasternal long-axis view (mm), median (IQR) | 31 (28–35) | 38 (32–42.5) | 45 (39–52) | <0.001 |
| LV end-diastolic volume, apical four-chamber view (mL), median (IQR) | 94 (78.25–119) | 116 (81–150) | 137 (102–177.5) | <0.001 |
| LV end-systolic volume, apical four-chamber view (mL), median (IQR) | 35 (27–48.5) | 59.5 (40–85) | 83 (59.5–128.5) | <0.001 |
| LV ejection fraction (%), Simpson method, median (IQR) | 62 (57–67) | 46 (42–48) | 34 (28–39) | <0.001 |
HFpEF—heart failure with preserved ejection fraction; HFmrEF—heart failure with mildly reduced ejection fraction; HFrEF—heart failure with reduced ejection fraction; IQR—interquartile range; LA — left atrial; LV — left ventricular.
Table 9.
Significant univariate predictors of AF in patients with HFpEF.
| Variable | OR | 95% CI | p-value |
|---|---|---|---|
| HAS-BLED score (per 1-point increase) | 1.419 | 1.120–1.797 | 0.004 |
| CHA₂DS₂-VA score (per 1-point increase) | 1.324 | 1.161–1.509 | <0.001 |
| HF duration (per 1-year increase) | 1.134 | 1.044–1.231 | 0.003 |
| Age (per 1-year increase) | 1.064 | 1.043–1.086 | <0.001 |
| Heart rate (per 1 bpm increase) | 1.022 | 1.011–1.033 | <0.001 |
| Serum creatinine (per 1 µmol/L increase) | 1.005 | 1.001–1.010 | 0.015 |
| Hemoglobin (per 1 g/L increase) | 0.988 | 0.979–0.997 | 0.010 |
| Office diastolic BP (per 1 mmHg increase) | 0.982 | 0.967–0.998 | 0.028 |
| Office systolic BP (per 1 mmHg increase) | 0.985 | 0.977–0.993 | <0.001 |
| eGFR (per 1 mL/min/1.73 m² increase) | 0.975 | 0.966–0.984 | <0.001 |
| Severe tricuspid regurgitation | 8.936 | 3.296–24.226 | <0.001 |
| Moderate tricuspid regurgitation | 4.516 | 2.263–9.009 | <0.001 |
| Moderate mitral regurgitation | 3.879 | 1.778–8.460 | 0.001 |
| Severe mitral regurgitation | 3.733 | 1.136–12.272 | 0.030 |
| Concomitant CKD | 3.097 | 1.332–7.199 | 0.009 |
| Moderate aortic regurgitation | 2.514 | 1.263–5.003 | 0.009 |
| Mild aortic regurgitation | 1.774 | 1.177–2.673 | 0.006 |
| LA size, parasternal long-axis view (per mm increase) | 1.123 | 1.088–1.159 | <0.001 |
| RA size, apical four-chamber view (per mm increase) | 1.073 | 1.038–1.109 | <0.001 |
| LA longitudinal size, apical four-chamber view (per mm increase) | 1.056 | 1.021–1.092 | 0.001 |
| Mitral inflow E-wave velocity (per 1 m/s increase) | 1.023 | 1.013–1.033 | <0.001 |
| Deceleration time of mitral E-wave (per 1-unit increase) | 0.994 | 0.990–0.999 | 0.013 |
| LV ejection fraction, Simpson method (per 1% increase) | 0.964 | 0.940–0.988 | 0.003 |
| Mineralocorticoid receptor antagonist therapy | 2.204 | 1.282–3.790 | 0.004 |
| Prior cardiac surgery | 2.167 | 1.295–3.626 | 0.003 |
| Angiotensin II receptor blocker therapy | 0.649 | 0.446–0.944 | 0.024 |
| Dihydropyridine calcium channel blocker therapy | 0.599 | 0.414–0.868 | 0.007 |
| Centrally acting antihypertensive therapy | 0.495 | 0.264–0.929 | 0.029 |
BP — blood pressure; CHA₂DS₂-VA — Congestive heart failure, Hypertension, Age ≥75 years, Diabetes mellitus, Stroke/transient ischemic attack/thromboembolism, Vascular disease, Age 65–74 years; CI—confidence interval; CKD — chronic kidney disease; eGFR — estimated glomerular filtration rate calculated using the CKD-EPI equation [34]; HAS-BLED - Hypertension, Abnormal renal and/or liver function, Stroke, Bleeding history or predisposition, Labile international normalized ratio, Elderly age >65 years, Drugs and/or alcohol use; HF – heart failure; LA — left atrial; LV — left ventricular; OR—odds ratio; RA — right atrial.
Table 10.
Independent multivariate predictors of AF in patients with HFpEF.
| Variable | Adjusted OR | 95% CI | p-value |
|---|---|---|---|
| Severe tricuspid regurgitation | 6.957 | 2.482–19.499 | <0.001 |
| Moderate tricuspid regurgitation | 4.092 | 1.977–8.466 | <0.001 |
| LA size, parasternal long-axis view (per mm increase) | 1.114 | 1.054–1.177 | <0.001 |
| Age (per 1-year increase) | 1.070 | 1.032–1.109 | <0.001 |
| Male sex | 1.680 | 1.076–2.621 | 0.022 |
| Heart rate (per 1 bpm increase) | 1.026 | 1.012–1.039 | <0.001 |
| Metabolic syndrome | 0.358 | 0.130–0.984 | 0.046 |
| eGFR (per 1 mL/min/1.73 m² increase) | 0.983 | 0.973–0.993 | 0.001 |
| Office systolic BP (per 1 mmHg increase) | 0.985 | 0.977–0.993 | <0.001 |
BP — blood pressure; CI—confidence interval; eGFR — estimated glomerular filtration rate calculated using the CKD-EPI equation [34]; LA — left atrial; OR—odds ratio.
Table 11.
Significant univariate predictors of AF in patients with HFmrEF.
| Variable | OR | 95% CI | p-value |
|---|---|---|---|
| LA size, parasternal long-axis view (per mm increase) | 1.114 | 1.030–1.206 | 0.007 |
| Age (per 1-year increase) | 1.049 | 1.002–1.097 | 0.040 |
| Heart rate (per 1 bpm increase) | 1.030 | 1.005–1.055 | 0.019 |
CI—confidence interval; LA — left atrial; OR—odds ratio.
Table 12.
Independent multivariate predictors of AF in patients with HFmrEF.
| Variable | Adjusted OR | 95% CI | p-value |
|---|---|---|---|
| LA size, parasternal long-axis view (per mm increase) | 1.142 | 1.011–1.291 | 0.033 |
CI—confidence interval; LA — left atrial; OR—odds ratio.
Table 13.
Significant univariate predictors of AF in patients with HFrEF.
| Variable | OR | 95% CI | p-value |
|---|---|---|---|
| Posterior LV wall thickness, parasternal long-axis view (per mm increase) | 1.546 | 1.118–2.138 | 0.008 |
| Age (per 1-year increase) | 1.035 | 1.002–1.070 | 0.035 |
| Heart rate (per 1 bpm increase) | 1.032 | 1.009–1.056 | 0.006 |
| LV end-diastolic volume, apical four-chamber view (per 1 mL increase) | 0.986 | 0.975–0.998 | 0.020 |
| LV end-systolic volume, apical four-chamber view (per 1 mL increase) | 0.983 | 0.969–0.997 | 0.017 |
| Office diastolic BP (per 1 mmHg increase) | 0.952 | 0.917–0.987 | 0.009 |
BP — blood pressure; CI—confidence interval; OR—odds ratio; LV — left ventricular.
Table 14.
Independent multivariate predictors of AF in patients with HFrEF.
| Variable | Adjusted OR | 95% CI | p-value |
|---|---|---|---|
| LV end-diastolic volume, apical four-chamber view (per 1 mL increase) | 0.981 | 0.964–0.998 | 0.033 |
CI—confidence interval; LV — left ventricular; OR—odds ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



