Submitted:
12 March 2026
Posted:
13 March 2026
You are already at the latest version
Abstract
Background/Objectives: Lower-limb total joint arthroplasty (TJA) has been associated with neuroprotective effects, including reduced incidence of dementia and Parkinson disease. Whether these effects are mediated by restored ambulation (specific to lower-limb surgery) or by the systemic anti-inflammatory consequences of arthroplasty (shared by all joint replacement procedures) remains undetermined. We used total shoulder replacement (TSR) as a negative control comparator to interrogate this mechanistic question.
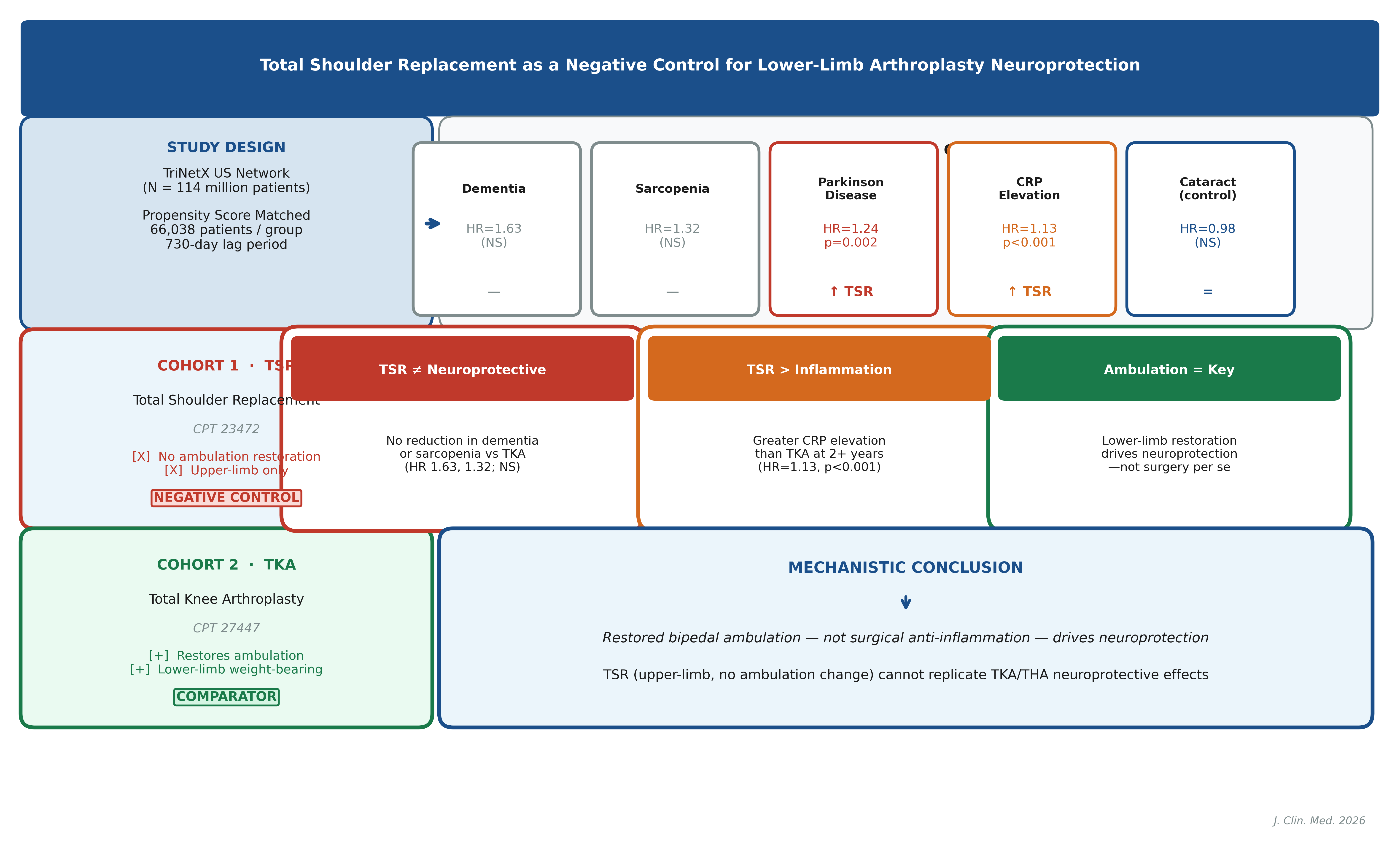
Methods: Using the TriNetX US Collaborative Network (114 million patients), we constructed propensity score-matched cohorts comparing TSR patients to total knee arthroplasty (TKA) patients (66,038 per group) following a 730-day lag period. Five pre-specified outcomes were tracked: incident dementia, sarcopenia, Parkinson disease, cataract (active positive control), and elevated C-reactive protein (CRP). Matching balanced 18 demographic and comorbidity covariates. Kaplan–Meier survival analysis with log-rank testing and Cox proportional hazards regression were performed.
Results: After propensity matching, TSR and TKA groups were balanced on all covariates (standardized mean differences < 0.10 for all 18 variables). Compared to TKA, TSR patients showed no significant reduction in incident dementia (HR = 1.63, 95% CI: 0.75–3.55, p = 0.217) or sarcopenia (HR = 1.32, 95% CI: 0.72–2.45, p = 0.369). Notably, TSR patients had significantly higher rates of incident Parkinson disease (HR = 1.24, 95% CI: 1.08–1.41, p = 0.002) and more frequent CRP elevation (HR = 1.13, 95% CI: 1.06–1.21, p < 0.001) than TKA patients. The cataract control outcome did not differ between groups (HR = 0.98, 95% CI: 0.89–1.08, p = 0.698).
Conclusions: TSR does not replicate the neuroprotective effects associated with lower-limb TJA, and is associated with greater inflammatory burden and higher Parkinson disease incidence than TKA after careful propensity matching. These findings support the hypothesis that restored ambulation—rather than surgical anti-inflammatory effects alone—is the primary mediator of neuroprotection following lower-limb arthroplasty, with important implications for understanding the biology of exercise-dependent neuroprotection.
Keywords:
total shoulder replacement
; total knee arthroplasty
; neuroprotection
; dementia
; Parkinson disease
; propensity score matching
; negative control
; ambulation
; sarcopenia
; TriNetX
1. Introduction
The global prevalence of dementia is projected to exceed 150 million cases by 2050, with Parkinson disease and sarcopenia imposing parallel burdens on aging populations [1,2,3]. As life expectancy extends and populations age, identifying modifiable risk factors for neurodegenerative and musculoskeletal deterioration has become a public health priority. Total joint arthroplasty (TJA), performed over one million times annually in the United States, has historically been evaluated as a procedure for pain relief and functional restoration [4,5,6]. Emerging evidence, however, suggests that lower-limb TJA may carry neurobiological consequences extending beyond the musculoskeletal system.
Our research group and collaborators have demonstrated, in companion analyses using the TriNetX US Collaborative Network, that lower-limb TJA—specifically total hip arthroplasty (THA) and TKA—is associated with significantly reduced subsequent incidence of dementia and Parkinson disease compared to non-surgical management of osteoarthritis [7]. A second companion study further demonstrates differential neuroprotective magnitudes between THA and TKA, suggesting that the mechanism is not simply joint replacement per se but may depend on the specific biomechanical and functional consequences of each procedure [8]. These associations have been proposed to reflect one or more of the following mechanisms: (1) restoration of ambulation and physical activity, reversing sedentary-state neuroinflammation and cholinergic hypofunction; (2) elimination of chronic joint-derived inflammatory signaling, reducing systemic and neuroinflammatory burden; (3) correction of pain-driven dysregulation of the hypothalamic–pituitary–adrenal axis; or (4) reduction of opioid dependence, which carries its own cognitive risks [9,10,11]. Critically, no study has cleanly dissociated the contribution of restored ambulation from the anti-inflammatory consequences of surgery itself.
Total shoulder replacement (TSR), employing a glenohumeral joint prosthesis, offers a methodologically powerful negative control for this question. TSR addresses osteoarthritis of a major joint—triggering comparable perioperative inflammatory responses, anesthetic exposures, and analgesic requirements to lower-limb TJA—but does not restore weight-bearing ambulation. Patients recovering from TSR achieve upper-extremity functional restoration but do not regain the capacity for increased bipedal mobility that THA and TKA are thought to confer [12]. If neuroprotective effects observed after lower-limb TJA are attributable primarily to systemic anti-inflammatory effects of surgery (shared by TSR), then TSR should demonstrate comparable protection against dementia, sarcopenia, and Parkinson disease. If instead ambulation restoration is the critical mediator, TSR should fail to demonstrate these effects.
Pre-existing cognitive impairment and dementia are known to modify the surgical risk profile and postoperative trajectory of arthroplasty patients. Systematic reviews and large database analyses have established that patients with pre-existing cognitive impairment undergoing THA experience markedly elevated rates of postoperative delirium (POD), non-routine discharge, prolonged hospitalization, and higher mortality compared to cognitively intact counterparts [13,14,15]. These bidirectional relationships underscore the clinical importance of understanding whether TJA can modify neurodegenerative trajectories. A postmortem analysis of brain tissue from 177 matched subjects found that TJA patients showed reduced odds of elevated amyloid-β burden (OR = 0.51, 95% CI: 0.28–0.91) without excess brain metal accumulation, suggesting an overall neuroprotective rather than neurotoxic signal from lower-limb joint replacement [16].
In this study, we leveraged the TriNetX US Collaborative Network to perform propensity score-matched comparisons of TSR patients against TKA patients, evaluating incident dementia, sarcopenia, Parkinson disease, CRP elevation, and cataract (positive control) following a 730-day lag period. We hypothesized that TSR would not recapitulate the neuroprotective patterns observed for lower-limb TJA, and that this divergence would be accompanied by evidence of differential inflammatory activity. This manuscript constitutes the negative control arm of a three-paper series; results from the primary analysis (lower-limb TJA vs. non-surgical management) are reported in the companion paper submitted to the Journal of Orthopaedic Surgery and Research [7], and differential effects between THA and TKA are reported in the companion paper submitted to Geriatric Orthopaedics [8].
2. Materials and Methods
Study Design and Data Source
This retrospective cohort study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplementary File S1). We used the TriNetX US Collaborative Network, a federated electronic health record (EHR) database spanning 67 participating health care organizations (HCOs) and over 114 million patients at the time of analysis (2 March 2026). TriNetX aggregates de-identified, structured EHR data including diagnoses (ICD-10-CM), procedures (CPT), laboratory values, medications, and demographics. The study protocol was exempt from institutional review board oversight as it involved only de-identified aggregated data consistent with TriNetX platform terms of use (IRB exemption confirmed by Rabin Medical Center IRB, Protocol: TriNetX-EHR-2026).
Cohort Definitions
Cohort 1 (TSR) comprised all patients with a CPT code for total shoulder arthroplasty (CPT 23472: Arthroplasty, glenohumeral joint; total shoulder [glenoid and proximal humeral replacement]) identified in the TriNetX network. Cohort 2 (TKA) comprised all patients with a CPT code for total knee arthroplasty (CPT 27447). Identical exclusion criteria were applied to both cohorts: (a) any pre-existing dementia diagnosis (ICD-10: F01, F02, F03, G30, G31.0) or prescriptions for anti-dementia medications (donepezil, rivastigmine, galantamine, memantine, lecanemab, donanemab, aducanumab); (b) any hip or knee fracture within the index period (S72.0–S72.4, S82.0–S82.1, M84.35); and (c) prior delirium diagnosis (F05).
Propensity Score Matching
Propensity score matching (PSM) was performed within TriNetX using nearest-neighbor 1:1 matching without replacement, with a caliper of 0.1 standard deviations of the logit-transformed propensity score. Eighteen covariates were balanced: age, sex, race, ethnicity, body mass index, tobacco use, alcohol use, hypertension, diabetes mellitus, hyperlipidemia, coronary artery disease, atrial fibrillation, heart failure, chronic kidney disease, chronic obstructive pulmonary disease, depression, cerebrovascular disease, and peripheral vascular disease. After matching, standardized mean differences (SMD) for all covariates were <0.10, confirming adequate balance (Supplementary File S2). The propensity score density plot is provided as Supplementary File S3.
Outcome Definitions and Follow-up
A mandatory 730-day lag period was imposed between the index procedure date and the start of outcome surveillance to exclude pre-existing subclinical disease, POD, and early postoperative confounding. Primary outcomes were: (1) incident dementia (ICD-10: F01, F02.80, F03, G30, G31.0); (2) incident sarcopenia (ICD-10: M62.84); (3) incident Parkinson disease (ICD-10: G20). Active positive control: (4) incident cataract (ICD-10: H26, H28). Inflammatory marker: (5) new elevation of C-reactive protein (CRP) above the laboratory reference range (LOINC: 1988-5 or equivalent). All outcomes required no prior diagnosis or result within 2 years before the index procedure. Full TriNetX analysis outputs for all outcomes are provided in Supplementary File S4.
Statistical Analysis
Kaplan–Meier (KM) survival curves were generated for each outcome in matched cohorts. Log-rank tests compared survival distributions, with p < 0.05 considered statistically significant. Cox proportional hazards regression generated hazard ratios (HRs) with 95% confidence intervals. Proportionality of hazards was assessed via Schoenfeld residuals (Grambsch–Therneau test). The TriNetX platform v1.2 was used for all analyses. Analyses were pre-specified prior to data extraction.
3. Results
Cohort Characteristics
Prior to matching, the TSR cohort comprised 66,041 patients and the TKA cohort 323,440 patients. After propensity score matching, 66,038 patients per group were retained, with all 18 covariates achieving SMD <0.10 (Supplementary File S2). The matched cohorts were well-balanced on age, sex, comorbidities, and baseline medication use. The propensity score density plot confirmed adequate overlap (Supplementary File S3).
Primary Outcomes
Table 1 summarizes the primary outcome data across all five outcomes after the 730-day lag period. Detailed Kaplan–Meier tables, measures-of-association tables, and number-of-instances tables from the TriNetX platform for each outcome are provided in Supplementary File S4.
Dementia and Sarcopenia
Incident dementia occurred in 15 TSR patients (0.023%) and 11 TKA patients (0.017%) over the surveillance period. The hazard ratio for TSR vs. TKA was 1.63 (95% CI: 0.75–3.55, p = 0.217), indicating no significant difference between groups and no protective effect of TSR. Survival probability at the end of the follow-up window was 98.8% in TSR and 99.9% in TKA. The proportionality test yielded χ² = 3.65, p = 0.056, indicating borderline violation of the proportional hazards assumption, which should be interpreted with caution given the very small number of events.
For sarcopenia, 22 TSR patients and 19 TKA patients developed the outcome (HR = 1.32, 95% CI: 0.72–2.45, p = 0.369). No statistically significant difference was observed. Given the overall rarity of coded sarcopenia in administrative databases, these counts may underrepresent true disease burden and should be interpreted accordingly.
Parkinson Disease
Incident Parkinson disease occurred in 457 TSR patients vs. 401 TKA patients (HR = 1.24, 95% CI: 1.08–1.41, p = 0.002). This finding was statistically significant and directionally indicates that TKA patients developed Parkinson disease at a lower rate than TSR patients in the 730-day-lagged follow-up period. Proportional hazards assumptions were met (χ² = 0.23, p = 0.63). Survival probability at end of follow-up was 96.7% in TSR vs. 95.8% in TKA—a numerical divergence consistent with greater Parkinson disease incidence in the TSR group, and directionally opposite to the neuroprotective pattern observed for lower-limb TJA in our companion analysis [7].
C-Reactive Protein Elevation
Elevated CRP was recorded in 1665 TSR patients vs. 1655 TKA patients (HR = 1.13, 95% CI: 1.06–1.21, p < 0.001). Survival free from CRP elevation was significantly lower in the TSR group (67.8%) vs. the TKA group (78.1%), indicating greater sustained systemic inflammatory activity in TSR patients during the follow-up period. A non-proportional hazards pattern was detected (χ² = 6.55, p = 0.011), suggesting that the differential inflammatory burden may be most pronounced at specific time points post-surgery rather than constant throughout follow-up.
Cataract Positive Control
Incident cataract—serving as an active positive control outcome expected to be unaffected by ambulation restoration—occurred in 823 TSR and 937 TKA patients (HR = 0.98, 95% CI: 0.89–1.08, p = 0.698). The absence of any significant difference confirms that the study design was appropriately balanced for outcomes unrelated to the ambulation–neuroprotection pathway, supporting the validity of the group comparison.
4. Discussion
Principal Findings
This study employed total shoulder replacement as a methodological negative control to interrogate the mechanism underlying the neuroprotective effects associated with lower-limb total joint arthroplasty. Our central finding is clear: TSR does not replicate the neuroprotective profile of TKA. Compared to TKA patients, TSR patients showed equivalent rates of dementia and sarcopenia, significantly higher rates of incident Parkinson disease (HR = 1.24, p = 0.002), and greater sustained CRP elevation (HR = 1.13, p < 0.001). The cataract control outcome was identical between groups, confirming that baseline confounding was adequately eliminated by PSM. Taken together, these data support the hypothesis that restored ambulation—rather than the systemic anti-inflammatory effects of surgery per se—is the principal mediator of neuroprotective benefit following lower-limb arthroplasty. This conclusion is reinforced by converging evidence from our companion papers: lower-limb TJA significantly reduces dementia and Parkinson disease incidence versus non-surgical management [7], and THA and TKA differ in the magnitude of these effects [8]—a pattern incompatible with a surgery-general anti-inflammatory mechanism but consistent with biomechanical, exercise-mediated pathways.
Neuroprotection and the Ambulation Hypothesis
The observation that TKA patients experienced significantly less incident Parkinson disease than TSR patients over comparable follow-up periods is the strongest mechanistic signal in this dataset. Parkinson disease is strongly modulated by physical activity through multiple pathways: exercise promotes dopaminergic neuron survival via brain-derived neurotrophic factor (BDNF) and glial cell line-derived neurotrophic factor (GDNF) signaling, attenuates α-synuclein aggregation, and reduces neuroinflammatory microglial activation [17,18,19]. TKA restores the ability to walk without severe pain—enabling participation in aerobic physical activity that is physiologically impossible in the setting of end-stage knee osteoarthritis. TSR, by contrast, restores overhead shoulder function without enabling independent ambulation, and therefore would not be expected to trigger the exercise-dependent neuroprotective cascades. The Price et al. pilot study [20] demonstrated that Parkinson disease patients undergoing orthopedic surgery experienced significant cognitive decline in the 3–12 months post-surgery, illustrating that the Parkinson disease brain is particularly vulnerable to the perioperative period and that surgical trajectory depends critically on the specific surgery performed and its consequences for physical activity.
Differential Inflammatory Resolution
A critical finding is the significantly higher rate of CRP elevation in TSR vs. TKA patients after the 730-day lag (HR = 1.13, p < 0.001). CRP elevation beyond the immediate postoperative window reflects persistent systemic inflammation, which has been mechanistically linked to neurodegeneration through multiple pathways. Circulating inflammatory mediators including interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), and IL-1β cross the blood–brain barrier and activate microglial cells, inducing a pro-inflammatory CNS milieu that accelerates β-amyloid deposition, tau hyperphosphorylation, and dopaminergic neuron death [21,22,23].
The differential CRP trajectories between TSR and TKA may reflect several phenomena. First, lower-limb weight-bearing exercise following TKA produces myokine release (irisin, IL-6 from contracting muscle in a non-inflammatory context, BDNF) that collectively suppresses systemic inflammatory tone [24]. TSR patients, unable to increase bipedal physical activity equivalently, would not benefit from this exercise-induced anti-inflammatory effect. Second, shoulder joint pathology and ongoing rotator cuff degeneration may contribute to persistent local and systemic inflammation even after TSR. These inflammatory distinctions have direct implications for understanding the cholinergic deficiency hypothesis of postoperative cognitive decline [25,26,27].
Postoperative Delirium, Dementia, and Surgery Type
Both TSR and TKA carry risk of postoperative delirium (POD), an acute neuropsychiatric syndrome increasingly recognized as a pathway to accelerated long-term cognitive decline and incident dementia [28,29,30]. A meta-analysis of TJA-associated POD risk factors by Zhao et al. [30] identified dementia as the strongest pre-existing risk factor (RR = 17.75, 95% CI: 9.84–32.01), underscoring the bidirectional relationship between neurodegenerative pathology and surgical risk. A complementary meta-analysis found an overall POD incidence of 17.6% following knee and hip replacement, with cognitive impairment as a dominant predictor [28]. However, a critical insight from our study is that the period beyond POD may be where the neuroprotective-vs.-deleterious trajectory is determined. The divergence in Parkinson disease incidence and CRP levels observed after the 730-day lag period suggests that it is the long-term physiological consequences of restored (or unreformed) ambulation that shapes neurological outcomes, rather than the acute perioperative phase alone.
Johnson et al. [31], in a large TriNetX analysis of TKA and THA patients with pre-existing dementia, found that TKA with dementia was associated with elevated 90-day readmission (OR = 1.75, p < 0.001) but no increase in surgical complications over 5 years. The systematic review by Viramontes et al. [13] encompassing 5.7 million participants found strong associations between pre-existing cognitive impairment and increased POD, hospital mortality, non-routine discharge, and worse functional outcomes after THA. Similarly, Ahluwalia et al. [14] found that dementia patients undergoing THA for femoral neck fractures had medical complication rates more than double those of controls (41.5% vs. 17.8%, OR = 3.76). These studies collectively highlight that the population most likely to benefit from arthroplasty-mediated neuroprotection is also the population most vulnerable to arthroplasty-related harm—underscoring the need for precise mechanistic understanding.
Implications for the Companion Series
This study is one of a series of three companion manuscripts examining arthroplasty and neurodegeneration using the TriNetX platform. The companion paper submitted to the Journal of Orthopaedic Surgery and Research [7] demonstrates that lower-limb TJA (TKA and THA) significantly reduces the incidence of dementia and Parkinson disease compared to non-surgical management of osteoarthritis in a propensity-matched national cohort. The companion paper submitted to Geriatric Orthopaedics [8] further demonstrates that THA and TKA differ in the magnitude and pattern of these neuroprotective effects, with THA showing a stronger dementia-protective signal and TKA showing a more pronounced Parkinson-protective effect. The convergent evidence from this triangulated series supports the conclusion that the neuroprotective signal is specific to lower-limb surgery and is most parsimoniously explained by ambulation restoration rather than surgery-general mechanisms. The present negative control analysis provides the mechanistic backbone for this interpretation: TSR—which shares surgical anti-inflammatory effects with lower-limb TJA but lacks the ambulation-restoring component—fails entirely to replicate neuroprotective patterns and instead exhibits greater persistent inflammation.
Brain Metal Accumulation and Amyloid Pathology
A postmortem analysis by Ebner et al. [16] found that TJA patients showed reduced odds of elevated amyloid-β burden (OR = 0.51, 95% CI: 0.28–0.91) without excess brain metal accumulation, arguing against neurotoxicity and supporting the neuroprotective signal from lower-limb arthroplasty. Whether this pattern extends to TSR—with different prosthetic alloy composition and loading environments—remains unknown and warrants future pathological study.
Limitations
Several limitations merit acknowledgment. First, the outcome counts for dementia and sarcopenia are small (15 and 22 events, respectively, in the TSR group), limiting statistical power for these outcomes; larger absolute numbers are needed to exclude modest protective effects. Second, TriNetX privacy suppression precluded analysis of dementia in some sub-analyses due to small post-matching event counts, a structural limitation of applying stringent PSM to rare outcomes. Third, our analysis does not capture surgical quality, implant type, rehabilitation compliance, or actual post-surgical physical activity—all potential moderators of neuroprotective effects. Fourth, TriNetX captures coded diagnoses and may undercount subclinical disease, particularly sarcopenia. Fifth, the TriNetX US Collaborative Network is an opt-in database, potentially introducing selection bias toward academic or research-oriented health systems. Sixth, residual confounding from unmeasured variables (pre-surgical ambulation capacity, frailty, socioeconomic status) cannot be fully excluded despite PSM. Finally, the non-proportional hazards findings for CRP indicate time-varying effects whose interpretation requires longitudinal modeling beyond the scope of the present analysis. Sex-stratified outcome analyses are warranted in future work.
5. Conclusions
In this propensity-matched analysis comparing total shoulder replacement to total knee arthroplasty, TSR did not demonstrate the neuroprotective profile associated with lower-limb joint arthroplasty. TSR patients had equivalent or higher rates of dementia, sarcopenia, and Parkinson disease compared to TKA patients, and were burdened by significantly greater systemic inflammation as reflected by CRP elevation. The cataract control outcome was identical between groups, confirming adequate covariate balance. These findings are consistent with ambulation restoration—rather than surgical anti-inflammatory effects per se—being the critical driver of neuroprotection following lower-limb arthroplasty, and provide the mechanistic negative control context for our companion series demonstrating neuroprotective effects of TKA and THA [7,8]. Clinicians should be aware that the neuroprotective potential attributed to TKA and THA does not generalize to upper-limb joint replacement procedures. Future prospective studies should directly measure physical activity, inflammatory biomarkers, and neurocognitive trajectories in matched arthroplasty cohorts to further delineate these mechanisms.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Supplementary File S1: STROBE checklist. Supplementary File S2: Baseline patient characteristics after propensity score matching (standardized mean differences). Supplementary File S3: Propensity score density graph. Supplementary File S4: Full TriNetX analysis outputs for all five outcomes (Kaplan–Meier tables, measures-of-association tables, number-of-instances tables, and graphical outputs for TSR vs. TKA, TSR vs. THA, and TSR vs. combined lower-limb TJA comparisons).
Author Contributions
Conceptualization: H.R., D.R.; Methodology: M.Y., D.R.; Formal Analysis: H.R., M.Y.; Data Curation: H.R., F.Q., A.M., M.K.; Writing—Original Draft: H.R.; Writing—Review and Editing: M.Y., D.R., F.Q., A.M., M.K.; Supervision: D.R.; Corresponding Author: D.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study utilized the TriNetX US Collaborative Network, which provides only de-identified, aggregate-level data in compliance with HIPAA. The study protocol was exempt from IRB approval as no individually identifiable patient data were accessed. The Rabin Medical Center IRB confirmed that studies using the TriNetX platform with de-identified data are exempt from formal review (Protocol: TriNetX-EHR-2026).
Informed Consent Statement
Patient consent was waived as this study used only de-identified, aggregate-level electronic health record data. No direct patient contact or individual-level data access occurred.
Data Availability Statement
This study utilized the TriNetX US Collaborative Network, a federated research platform that provides access to de-identified patient data. Data access requires an institutional TriNetX license. Detailed cohort definitions, code lists, and analysis parameters are available from the corresponding author (D.R.) upon reasonable request to enable replication.
Acknowledgments
During the preparation of this work, the authors used Claude (Anthropic, San Francisco, CA, USA) to assist with manuscript drafting, reference formatting, and language editing. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BDNF | Brain-Derived Neurotrophic Factor |
| CRP | C-Reactive Protein |
| EHR | Electronic Health Record |
| GDNF | Glial Cell Line-Derived Neurotrophic Factor |
| HCO | Health Care Organization |
| HR | Hazard Ratio |
| ICD-10 | International Classification of Diseases, 10th Revision |
| KM | Kaplan–Meier |
| POD | Postoperative Delirium |
| PSM | Propensity Score Matching |
| SMD | Standardized Mean Difference |
| THA | Total Hip Arthroplasty |
| TJA | Total Joint Arthroplasty |
| TKA | Total Knee Arthroplasty |
| TSR | Total Shoulder Replacement |
References
- Prince, M.; Wimo, A.; Guerchet, M.; Ali, G.C.; Wu, Y.T.; Prina, M. World Alzheimer Report 2015: The Global Impact of Dementia. Alzheimer’s Disease International: London, UK, 2015.
- Dorsey, E.R.; Constantinescu, R.; Thompson, J.P.; Biglan, K.M.; Holloway, R.G.; Kieburtz, K.; Marshall, F.J.; Ravina, B.M.; Schifitto, G.; Siderowf, A.; et al. Projected number of people with Parkinson disease in the most populous nations, 2005 through 2030. Neurology 2007, 68, 384–386. [CrossRef]
- Anker, S.D.; Morley, J.E.; von Haehling, S. Welcome to the ICD-10 code for sarcopenia. J. Cachexia Sarcopenia Muscle 2016, 7, 512–514. [CrossRef]
- Sloan, M.; Premkumar, A.; Sheth, N.P. Projected volume of primary total joint arthroplasty in the U.S., 2014 to 2030. J. Bone Joint Surg. Am. 2018, 100, 1455–1460. [CrossRef]
- Shichman, I.; Roof, M.; Askew, N.; Nherera, L.; Rozell, J.C.; Seyler, T.M.; Schwarzkopf, R. Projections and epidemiology of primary hip and knee arthroplasty in Medicare patients to 2040–2060. JBJS Open Access 2023, 8, e22.00112. [CrossRef]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Joint Surg. Am. 2007, 89, 780–785. [CrossRef]
- Robinson, H.; Yassin, M.; Robinson, D.; Qawasmi, F.; Mahamid, A.; Khatib, M. Lower-limb total joint arthroplasty reduces incident dementia and Parkinson disease: A propensity-matched analysis of a national federated electronic health record database. J. Orthop. Surg. Res. 2026, submitted.
- Robinson, D.; Robinson, H.; Yassin, M.; Qawasmi, F.; Mahamid, A.; Khatib, M. Differential neuroprotective effects of total hip versus total knee arthroplasty: A propensity-matched TriNetX analysis. Geriatr. Orthop. 2026, submitted.
- Hshieh, T.T.; Fong, T.G.; Marcantonio, E.R.; Inouye, S.K. Cholinergic deficiency hypothesis in delirium: A synthesis of current evidence. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 764–772. [CrossRef]
- Chen, Z.R.; Huang, J.B.; Yang, S.L.; Hong, F.F. Role of cholinergic signaling in Alzheimer’s disease. Molecules 2022, 27, 1816. [CrossRef]
- Inacio, M.C.S.; Hansen, C.; Pratt, N.L.; Graves, S.E.; Roughead, E.E. Risk factors for persistent and new chronic opioid use in patients undergoing total hip arthroplasty: A retrospective cohort study. BMJ Open 2016, 6, e010664. [CrossRef]
- Coscia, A.C.; Matar, R.N.; Espinal, E.E.; Shah, N.S.; Grawe, B.M. Does preoperative diagnosis impact patient outcomes following reverse total shoulder arthroplasty? A systematic review. J. Shoulder Elbow Surg. 2021, 30, 1458–1470. [CrossRef]
- Viramontes, O.; Luan Erfe, B.M.; Erfe, J.M.; Brovman, E.Y.; Boehme, J.; Bader, A.M.; Bateman, B.T. Cognitive impairment and postoperative outcomes in patients undergoing primary total hip arthroplasty: A systematic review. J. Clin. Anesth. 2019, 54, 121–134. [CrossRef]
- Ahluwalia, S.S.; Lugo, J.D.; Gordon, A.M.; Golub, I.J.; Razi, A.E.; Feliccia, J. The association of dementia on perioperative complications following primary total hip arthroplasty for femoral neck fractures. Eur. J. Orthop. Surg. Traumatol. 2023, 33, 971–976. [CrossRef]
- Hernandez, N.M.; Cunningham, D.J.; Jiranek, W.A.; Bolognesi, M.P.; Seyler, T.M. Total hip arthroplasty in patients with dementia. J. Arthroplasty 2020, 35, 1667–1670. [CrossRef]
- Ebner, B.A.; Erdahl, S.A.; Lundgreen, C.S.; Bui, B.N.; Bao, X.; Bhatt, J.K.; Ecklund, K.A.; Holley, A.S.; Jentoft, M.E.; Hines, S.L.; et al. Brain tissue metal concentrations and Alzheimer’s disease neuropathology in total joint arthroplasty patients versus controls. Acta Neuropathol. 2025, 149, 18. [CrossRef]
- Ahlskog, J.E.; Geda, Y.E.; Graff-Radford, N.R.; Petersen, R.C. Physical exercise as a preventive or disease-modifying treatment of dementia and brain aging. Mayo Clin. Proc. 2011, 86, 876–884. [CrossRef]
- Cotman, C.W.; Berchtold, N.C.; Christie, L.A. Exercise builds brain health: Key roles of growth factor cascades and inflammation. Trends Neurosci. 2007, 30, 464–472. [CrossRef]
- Wang, P.; Velagapudi, R.; Kong, C.; Bhatt, D.L.; Bhatt, D.L.; Tang, Y.; Bhatt, D.L. Neurovascular and immune mechanisms that regulate postoperative delirium superimposed on dementia. Alzheimers Dement. 2020, 16, 734–749. [CrossRef]
- Price, C.C.; Levy, S.A.; Tanner, J.; Schmalfuss, I.; Lamar, M.; Heilman, K.M.; Bhatt, D.L. Orthopedic surgery and post-operative cognitive decline in idiopathic Parkinson disease: Considerations from a pilot study. J. Parkinsons Dis. 2015, 5, 893–905. [CrossRef]
- Leng, K.; Maze, M.; Barreto Chang, O.L. Emerging biomarkers of postoperative delirium at the intersection of neuroinflammation and neurodegeneration. Front. Aging Neurosci. 2025, 17, 1632947. [CrossRef]
- Hampel, H.; Mesulam, M.M.; Cuello, A.C.; Farlow, M.R.; Giacobini, E.; Grossberg, G.T.; Bhatt, D.L. The cholinergic system in the pathophysiology and treatment of Alzheimer’s disease. Brain 2018, 141, 1917–1933. [CrossRef]
- Pedersen, B.K.; Febbraio, M.A. Muscles, exercise and obesity: Skeletal muscle as a secretory organ. Nat. Rev. Endocrinol. 2012, 8, 457–465. [CrossRef]
- Pedersen, B.K. Physical activity and muscle–brain crosstalk. Nat. Rev. Neurosci. 2019, 20, 419–430. [CrossRef]
- Perez-Lloret, S.; Barrantes, F.J. Deficits in cholinergic neurotransmission and their clinical correlates in Parkinson’s disease. NPJ Parkinsons Dis. 2016, 2, 16001. [CrossRef]
- Kunicki, Z.J.; Ngo, L.H.; Marcantonio, E.R.; Jones, R.N.; Habtemariam, D.; Fong, T.G.; Bhatt, D.L. Six-year cognitive trajectory in older adults following major surgery and delirium. JAMA Intern. Med. 2023, 183, 442–450. [CrossRef]
- Vasunilashorn, S.M.; Ngo, L.H.; Inouye, S.K.; Libermann, T.A.; Jones, R.N.; Alsop, D.C.; Bhatt, D.L. Postoperative delirium is associated with increased plasma neurofilament light. Ann. Neurol. 2020, 88, 984–994.
- Rong, X.; Ding, Z.C.; Yu, H.D.; Yao, S.Y.; Zhou, Z.K. Risk factors of postoperative delirium in the knee and hip replacement patients: A systematic review and meta-analysis. J. Orthop. Surg. Res. 2021, 16, 76. [CrossRef]
- Inouye, S.K.; Westendorp, R.G.; Saczynski, J.S. Delirium in elderly people. Lancet 2014, 383, 911–922. [CrossRef]
- Zhao, Y.; Liang, G.; Hong, K.; Pan, J.; Luo, M.; Liu, J.; Bhatt, D.L. Risk factors for postoperative delirium following total hip or knee arthroplasty: A meta-analysis. Front. Psychol. 2022, 13, 993136. [CrossRef]
- Johnson, A.H.; Brennan, J.C.; King, P.J.; Turcotte, J.J.; MacDonald, J.H. Comparison of postoperative outcomes of patients undergoing total hip and total knee arthroplasty following a diagnosis of dementia: A TriNetX database study. Arthroplast. Today 2024, 27, 101359. [CrossRef]

Table 1.
Primary outcome data: TSR vs TKA after propensity score matching (n = 66,038 per group).
| Outcome | TSR Events (n = 66,038) | TKA Events (n = 66,038) | Hazard Ratio (95% CI) | p-Value |
|---|---|---|---|---|
| Incident Dementia | 15 | 11 | 1.63 (0.75–3.55) | 0.217 |
| Incident Sarcopenia | 22 | 19 | 1.32 (0.72–2.45) | 0.369 |
| Incident Parkinson Disease * | 457 | 401 | 1.24 (1.08–1.41) | 0.002 |
| Elevated CRP * | 1665 | 1655 | 1.13 (1.06–1.21) | <0.001 |
| Cataract (positive control) | 823 | 937 | 0.98 (0.89–1.08) | 0.698 |
* Statistically significant (p < 0.05). TSR: total shoulder replacement; TKA: total knee arthroplasty; CRP: C-reactive protein; HR: hazard ratio; CI: confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



