Submitted:
10 March 2026
Posted:
11 March 2026
You are already at the latest version
Abstract
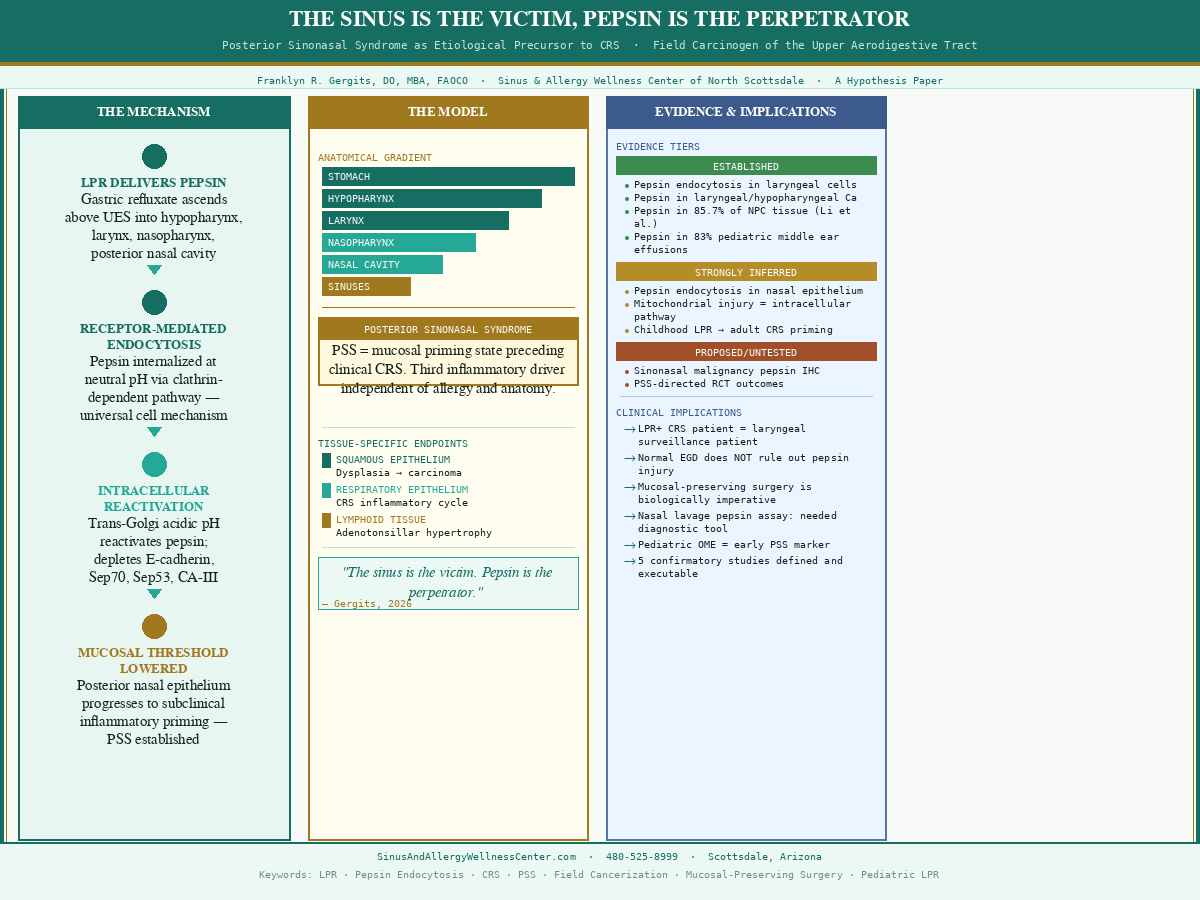
Objective: To propose Posterior Sinonasal Syndrome (PSS) as the etiological precursor to a defined subset of chronic rhinosinusitis (CRS), establish pepsin as a field carcinogen across the upper aerodigestive mucosal surface, and define the biological imperative for mucosal-preserving surgery in PSS-CRS patients. Methods: Synthesis of peer-reviewed evidence across four domains: pepsin endocytosis mechanisms in upper airway epithelium; pepsin detection in sinonasal, nasopharyngeal, and middle ear tissue; epidemiological trends in pediatric upper airway disease; and clinical outcomes in refractory CRS. Evidence is stratified as established, strongly inferred, or proposed requiring confirmatory study. Results: Pepsin, delivered via laryngopharyngeal reflux along a defined anatomical concentration gradient, produces receptor-mediated intracellular injury in posterior nasal epithelium — a mechanism established in laryngeal cells and strongly inferred in nasal cells. This injury lowers the posterior nasal mucosal inflammatory threshold, creating PSS as a priming state preceding clinical CRS. Pepsin has been detected within malignant tissue at two anatomically distinct sites: laryngeal and hypopharyngeal carcinoma, and nasopharyngeal carcinoma in 85.7% of cases versus 17.2% of controls — the two-site molecular fingerprint of a field carcinogen across the full upper aerodigestive surface. Pepsin detection in 83% of pediatric middle ear effusions and its correlation with adenoid hypertrophy grade establish that this process begins in childhood. PSS represents a third inflammatory driver of CRS, independent of allergy and anatomy, unrecognized by the 2025 AAO-HNS guideline. Five confirmatory studies and a nasal lavage pepsin assay validation pathway are defined. Conclusion: PSS is the etiological precursor to a misidentified subset of treatment-resistant CRS. Pepsin is both the primary driver of posterior nasal mucosal priming and a field carcinogen across the upper aerodigestive surface. Aggressive tissue-resecting FESS in this population is biologically counterproductive. The confirmatory studies are named, the clinical tools are within reach, and the patients are in rhinology practices now.
Keywords:
laryngopharyngeal reflux
; pepsin endocytosis
; chronic rhinosinusitis
; posterior sinonasal syndrome
; PSS
; field cancerization
; upper aerodigestive tract
; squamous metaplasia
; mucosalpreserving surgery
; balloon sinuplasty
; posterior nasal nerve neuromodulation
; nasal lavage pepsin assay
; cancer risk stratification
; pediatric LPR
; otitis media with effusion
; adenotonsillar hypertrophy
; FESS
; Setliff small hole surgery
Level of Evidence: 5 — Expert opinion / Hypothesis
1. Introduction
Laryngopharyngeal reflux (LPR) — the retrograde flow of gastric contents above the upper esophageal sphincter into the laryngopharynx and beyond — has become one of the more consequential diagnoses in modern otolaryngology. Prevalence has increased approximately 4% per year since 1976. Otolaryngology visits attributable to LPR rose 500% between 1990 and 2001. A condition that was rarely encountered a generation ago now occupies a substantial portion of a busy ENT practice.[27]
For most of this period, the working model of LPR-driven injury centered on acid. That model was always incomplete. Laryngopharyngeal mucosa is damaged by as few as four acid reflux episodes per day — the esophageal mucosa tolerates fifty without visible injury. Acid suppression with proton pump inhibitors fails to resolve LPR symptoms in a substantial proportion of patients. pH monitoring studies have documented repeatedly that many LPR events occur at weakly acidic or non-acidic pH levels that would never trigger a standard probe event. The acid model explained some of what was observed clinically. It never explained all of it.[17]
The work of Johnston and colleagues, beginning in 2007, reframed the pathophysiology in a way that the acid model could not. Pepsin — the principal proteolytic enzyme of gastric refluxate — is actively internalized by upper airway epithelial cells through receptor-mediated endocytosis at neutral pH, trafficked to the trans-Golgi compartment where the acidic luminal environment reactivates its proteolytic activity, and then depletes the epithelial barrier proteins E-cadherin, carbonic anhydrase isoenzyme III, Sep70, and Sep53. That mechanism, and its extension to sinonasal tissue by Southwood and colleagues in 2015, is described in detail in Section 3 and Section 4.[1,2,3,6]
What the clinical literature has not adequately examined is why this epidemic arrived when it did. Three developments beginning in the mid-twentieth century transformed pepsin from a gastric enzyme with incidental upper airway exposure into a chronic mucosal pathogen delivered at historically unprecedented frequency. The obesity epidemic increased intragastric pressure mechanically, disrupted esophagogastric junction anatomy, and promoted the transient lower esophageal sphincter relaxations that drive refluxate above the upper esophageal sphincter — the GERD rate ratio rising from pre-1995 baseline to 1.51 by 2005–2009, tracking the obesity curve closely. The high-fat Western diet independently relaxed the lower esophageal sphincter through a cholecystokinin-mediated mechanism, adding a pharmacological insult to the mechanical one. Less recognized than either of these, FDA food acidification mandates beginning in the late 1970s ensured that nearly every commercially bottled or canned beverage in the American food supply — with the exception of still water — is acidified to a pH of 2.8–4.4. The esophageal adenocarcinoma incidence data from SEER records the oncologic consequence: a 767% increase from 1973 baseline, averaging 5.1% annual growth, in the cancer that sits at the downstream end of the same reflux-pepsin pathway.[27]
Central to this paper is a clinical argument that has not previously been articulated in the rhinology literature. Posterior sinonasal syndrome (PSS) is the direct upstream precursor to refractory chronic rhinosinusitis in a defined and identifiable patient population. PSS is not a variant of CRS. It is not a comorbidity. It is the mucosal priming condition — created by pepsin endocytosis in posterior nasal columnar epithelium, progressing silently over years — that makes the posterior nasal mucosa susceptible to the inflammatory cascade that produces clinical CRS when any sufficient secondary trigger arrives. The sequence is fixed: pepsin injury first, threshold lowering second, trigger third, clinical CRS fourth. The CRS in the PSS patient is not the primary disease. It is the declared endpoint of a process that began upstream, in the posterior nasal mucosa, years or decades before the patient presented with symptoms that met the diagnostic criteria for sinusitis. Treating CRS without identifying and addressing the PSS that precedes and causes it is treating the consequence while the cause continues to operate. This is why the PSS-CRS patient fails every treatment the guideline recommends: the guideline treats CRS. The patient has PSS. The sinus is the victim. Pepsin is the perpetrator.
This paper proposes a unified model connecting these disparate bodies of evidence. Pepsin endocytosis in upper airway epithelium is not a tissue-specific event limited to the larynx — it is a universal consequence of LPR across the entire upper aerodigestive tract. The clinical manifestation of this injury varies by tissue type and anatomical position within the reflux concentration gradient. Understanding this model has direct implications for the management of refractory CRS, the cancer risk counseling of LPR patients, and the design of the confirmatory studies that could formally establish one of the most clinically significant mechanisms in upper airway medicine.
2. The Anatomical Concentration Gradient: A Foundation for the Model
The path of LPR refluxate follows a defined anatomical sequence. Gastric contents that overcome the lower esophageal sphincter ascend through the esophagus. Those that additionally overcome the upper esophageal sphincter enter the hypopharynx first, contact the laryngeal inlet, ascend to the nasopharynx, and may eventually reach the posterior nasal cavity and paranasal sinuses. At each successive station, the refluxate is progressively diluted by salivary bicarbonate, mucosal secretions, and gravitational dispersion.
This anatomy creates a concentration gradient for pepsin that is highest at the hypopharynx and larynx and lower — but still clinically significant — at the nasopharynx and nasal cavity. The significance of this gradient to the argument that follows cannot be overstated. Pepsin does not travel from the nose downward to the larynx. It travels from the stomach upward, reaching the larynx before the nose. A patient in whom nasal pepsin is detectable at endocytosis-sufficient concentrations is, by anatomical necessity, a patient in whom laryngeal and hypopharyngeal pepsin burden is at least as great and almost certainly greater.
Detection of pepsin in nasal lavage fluid or nasal tissue from a CRS patient is therefore not simply evidence of a sinusitis-LPR association. It is evidence that pepsin endocytosis is occurring throughout that patient’s upper airway, at higher concentrations in the tissues anatomically closer to the source. The nasal cavity is the distal sentinel of a process that is more intense at the larynx and hypopharynx. That framing matters for everything that follows.
3. The Endocytosis Mechanism Is Not Larynx-Specific
Johnston’s foundational 2007 paper established that pepsin uptake by laryngeal epithelial cells is receptor-mediated, using electron microscopy to demonstrate co-localization of pepsin with transferrin — a classical marker of receptor-mediated endocytosis — in intracellular vesicles. Subsequent work confirmed that the internalized pepsin is trafficked to late endosomes and the trans-Golgi network, where acidic luminal pH of approximately 4 to 5 reactivates its proteolytic activity.[1,4]
Johnston’s group noted that it is unlikely there is a specific biologic receptor for pepsin, proposing instead that pepsin exploits or piggybacks another receptor-ligand complex, dysregulating its normal physiological function. The receptor has not been definitively identified in the published literature. What has been established is that the uptake pathway uses clathrin-mediated endocytosis — one of the most universal and fundamental cellular processes in human biology, operating in every nucleated cell for nutrient uptake, growth factor signaling, and membrane recycling. Clathrin-mediated endocytosis is not a larynx-specific mechanism.[1]
Southwood and colleagues extended the pepsin damage story to human nasal epithelial cells in 2015. Using electron microscopy, they demonstrated mitochondrial damage in pepsin-treated nasal epithelial cells that was not present in controls — the same mitochondrial fingerprint documented in pepsin-treated laryngeal cells. Mitochondrial damage at neutral pH, where pepsin is enzymatically inactive on the cell surface, is mechanistically explained only by intracellular reactivation. Surface contact with inactive pepsin at neutral pH does not damage mitochondria. Pepsin must be inside the cell, in an acidic compartment, to produce this pattern.[6]
This inference is further supported by Samuels and colleagues’ counterintuitive finding that pepsin endocytosis is more prominent at neutral pH than at weakly acidic pH. The more alkaline the refluxate, the more efficiently pepsin is internalized. For patients on high-dose PPI therapy, this has a direct and uncomfortable implication: acid suppression that neutralizes refluxate does not suppress pepsin and may optimize the pH conditions for endocytosis rather than preventing it.[7]
Taken together, the available evidence supports the conclusion that pepsin endocytosis is a property of upper airway epithelial cells generally — operating through a universal clathrin-dependent mechanism and producing the same intracellular damage signature, mitochondrial dysfunction, depletion of protective proteins, and activation of inflammatory cytokine pathways, in both laryngeal and nasal cell types.
4. Tissue-Specific Endpoints: Why the Same Injury Produces Different Diseases
If pepsin endocytosis operates in both laryngeal and nasal epithelial cells and produces similar intracellular damage in both, why does the clinical literature describe laryngeal carcinoma as an endpoint of LPR while CRS — not sinonasal malignancy — is the dominant upper airway disease associated with reflux? The answer lies in the fundamental biological differences between the two tissue types.
Laryngeal epithelium is stratified squamous — histologically identical to esophageal and oropharyngeal epithelium. Squamous epithelium’s characteristic response to chronic sublethal injury is dysplasia, and the well-established pathological sequence of chronic irritation to squamous metaplasia to dysplasia to carcinoma in situ to invasive carcinoma is the same pathway observed in Barrett’s esophagus progression, HPV-driven oropharyngeal carcinoma, and tobacco-associated head and neck cancer. Pepsin-driven depletion of E-cadherin, Sep70, and carbonic anhydrase in laryngeal squamous cells creates the compromised cellular environment in which this dysplastic pathway is facilitated. Johnston’s group has demonstrated that pepsin treatment of laryngeal and hypopharyngeal cell lines produces NF-kB activation, upregulation of TRAIL and BCL2A1, promotion of anchorage-independent growth and cell migration, and changes in miRNA profiles identical to those observed in head and neck squamous cell carcinoma — and critically, pepsin has been identified within laryngeal and hypopharyngeal carcinoma tissue itself, establishing its presence not merely as a risk association but as a molecular participant at the tumor site. That same tissue-level detection has been independently confirmed at the proximal end of the reflux gradient: Li et al. identified pepsin in 85.7% of nasopharyngeal carcinoma tissue versus 17.2% of chronic nasopharyngitis controls — the NPC finding that, paired with Johnston’s laryngeal tissue detection, constitutes the two-site molecular fingerprint of pepsin as a field carcinogen operating across the full upper aerodigestive mucosal surface.[5,13,16]
Sinonasal epithelium is pseudostratified ciliated columnar respiratory epithelium — structurally and immunologically distinct. Respiratory epithelium does not characteristically undergo squamous dysplasia under chronic inflammatory stress. Its pathological response to persistent injury is chronic mucosal inflammation, goblet cell hyperplasia, ciliary dysfunction, and the self-perpetuating inflammatory cycle that defines CRS. Southwood’s pepsin-treated nasal epithelial cells produced a pro-inflammatory cytokine signature including IL-8 that overlaps precisely with the CRS inflammatory profile. Sinonasal malignancy is rare not because the posterior nasal mucosa is protected from pepsin, but because respiratory epithelium does not undergo the dysplastic transformation pathway that squamous epithelium follows under the same intracellular insult.[6]
This tissue-type specificity reconciles the epidemiology with the proposed model. CRS affects approximately 30 million Americans — roughly 10% of the adult population. Laryngeal cancer produces approximately 13,000 new cases per year in the United States. The 2,000-fold difference in prevalence does not argue against a shared upstream mechanism. It argues precisely for tissue-specific endpoints from that shared mechanism.
5. The Cofactor Model: Why Not All Patients Progress to Laryngeal Cancer
The proposed model does not claim that LPR causes laryngeal cancer in all exposed patients, or even in most. The meta-analysis by Luo et al. (2018), drawing on 18 case-control studies, found an odds ratio of 2.47 for laryngeal malignancy in patients with reflux disease — elevated, but far from deterministic. In the subset of studies examining LPR specifically rather than GERD broadly, the odds ratio was 3.09. A 3-fold elevation in risk in a disease with a baseline annual incidence of 2.5 per 100,000 still produces a rare outcome in absolute terms.[11]
This pattern — a mechanism present in many, a catastrophic outcome in few — is characteristic of co-carcinogenesis. Tobacco is the strongest established risk factor for laryngeal cancer; the vast majority of smokers never develop it. HPV infects most sexually active adults; oropharyngeal carcinoma remains rare. Hepatitis C virus causes hepatocellular carcinoma in a fraction of chronically infected patients. In each of these cases, the carcinogenic agent is necessary to explain the elevated risk but not sufficient to produce disease on its own.
The cofactors that may determine which LPR patients progress from pepsin-driven squamous cell injury to dysplasia and carcinoma include cumulative lifetime exposure to pepsin endocytosis events — which determines the degree of protective protein depletion — tobacco and alcohol use, individual genetic variation in DNA repair capacity and immune surveillance, and the degree to which the upper esophageal sphincter is incompetent, which determines how consistently refluxate reaches the supraglottic structures.
The Lewin et al. 2003 prospective study is instructive. Eighty-five percent of patients with premalignant or early laryngeal carcinomas had documented LPR on 24-hour pH monitoring, and critically, no significant association was found between the level of LPR and histologic stage or smoking status. Heartburn did not predict LPR. LPR appears to operate as a background facilitator — present across the spectrum from dysplasia to invasive cancer, not correlated with stage because it is a permissive condition rather than a staging variable.[12]
A critical methodological limitation of the Lewin study and of the broader LPR-laryngeal cancer literature deserves explicit acknowledgment. The 24-hour pH monitoring used to identify LPR detects acid — specifically, episodes in which hypopharyngeal or esophageal pH drops below a defined threshold. It does not detect pepsin. A patient whose LPR is predominantly non-acidic would read as LPR-negative on 24-hour pH monitoring despite having active pepsin in their hypopharynx undergoing receptor-mediated internalization into laryngeal squamous cells. The 85% prevalence of LPR in Lewin’s premalignant and early carcinoma population, measured by acid detection, is almost certainly an underestimate of the true pepsin exposure prevalence. The parallel finding at the proximal end of the reflux gradient — Li et al.’s detection of pepsin in 85.7% of NPC tissue — reinforces this conclusion: if pepsin is present in malignant tissue at both the distal high-concentration station (larynx) and the proximal lower-concentration station (nasopharynx), the field carcinogen model predicts that pH-based studies are systematically underestimating pepsin’s carcinogenic role across the entire upper aerodigestive tract.
In summary: pepsin endocytosis in laryngeal squamous cells appears to be necessary but not sufficient for malignant transformation. It creates a compromised intracellular environment in which carcinogenic cofactors can complete the transformation. The low absolute incidence of laryngeal cancer in the LPR population reflects the requirement for multiple cofactors, not the absence of the upstream mechanism.
6. The Developmental Hypothesis: Childhood LPR as the Origin of Adult CRS
The mechanism described in the preceding sections does not begin in adulthood. The evidence suggests it begins in childhood — and that the accumulated subclinical posterior nasal mucosal injury from years of pediatric LPR is the missing etiology of the slow progressive mucosal activation that eventually presents as adult CRS.
The evidentiary anchor for this claim is the landmark 2002 study by Tasker and colleagues, published in The Lancet, which detected pepsin and pepsinogen in 83% of middle ear effusion fluid samples from children undergoing myringotomy for otitis media with effusion. The middle ear communicates with the nasopharynx via the Eustachian tube. Pepsin in the middle ear requires pepsin in the nasopharynx first. The Tasker finding established that in a substantial majority of children with recurrent otitis media with effusion — one of the most common pediatric conditions managed by otolaryngologists — gastric refluxate is routinely reaching the nasopharynx and posterior nasal cavity.[18]
If the pepsin endocytosis mechanism operates in posterior nasal respiratory epithelium as proposed in Section 3 and Section 4, then these children are not merely experiencing episodic surface irritation. They are experiencing receptor-mediated internalization of pepsin into posterior nasal epithelial cells, with the same downstream consequences demonstrated in adult nasal epithelial cells in vitro. The difference is duration: a child with LPR beginning in infancy and persisting through adolescence may accumulate a decade or more of subclinical posterior nasal mucosal injury before any clinical presentation of sinusitis occurs.
This framing resets the natural history of CRS entirely. The current clinical model treats CRS as a disease of adult onset — something that develops in the third, fourth, or fifth decade, typically attributed to a combination of anatomic factors, allergic sensitization, and infectious history. The question clinicians ask is: why does this adult have chronic sinusitis? The developmental hypothesis asks a different question: what was happening in this person’s posterior nasal mucosa at age three, age eight, age fourteen?
The slow, progressive character of CRS development is precisely what one would expect from subclinical cumulative injury spanning years to decades. Posterior nasal mucosal cells damaged by intermittent pepsin endocytosis do not immediately fail — they function in a progressively compromised state, their activation threshold dropping lower until what was subclinical injury crosses into the recognized clinical syndrome of chronic rhinosinusitis.
In my 30 years of rhinologic practice, the most challenging and least understood CRS subset is the patient with severe, progressive posterior mucosal inflammation who has anatomically normal or near-normal sinuses on CT, well-controlled allergic disease, no significant infectious history, and yet fails every intervention offered. These are patients whose disease appears to have no adequate proximate cause in adulthood because the cause is not proximate — it is distal in time, rooted in a childhood of unrecognized and untreated LPR silently injuring the posterior nasal mucosa year after year.
The clinical implications move in two directions. Looking backward at adult CRS patients, a detailed history of childhood ear disease — specifically recurrent otitis media with effusion, which the Tasker data identifies as a surrogate marker for nasopharyngeal pepsin exposure — becomes a potentially informative element of the rhinologic intake. A 45-year-old with refractory posterior CRS who had multiple sets of pressure equalization tubes as a child may be telling you, without knowing it, that their posterior nasal mucosal priming began in kindergarten. Looking forward at pediatric patients, children with LPR and recurrent otitis media with effusion deserve an upstream diagnosis and upstream management — not merely tubes and adenoidectomy for the downstream tissue consequences of a process that is not being addressed at its source.
A second subset of patients appears to follow a distinct course: posterior nasal mucosal injury accumulates at a faster rate, reaching a primed pre-inflammatory state relatively early, then waiting. The threshold is crossed not by slow accumulation but by a discrete precipitating event delivering sufficient additional inflammatory load to a tissue already positioned at the edge of clinical disease. The candidates for that triggering event are familiar to any rhinologist — a first significant allergic sensitization, a severe bacterial sinusitis, an occupational irritant exposure, the immune shifts of early pregnancy. What makes this subset clinically distinctive is not the nature of the trigger. It is the speed and severity of the response. Most patients who sustain a first sinus infection recover. The patient in this subset does not. Their disease goes chronic rapidly, it is immediately posterior-predominant, and they arrive asking why they have not responded to treatments that resolve the condition in everyone else around them. The answer is that their posterior nasal mucosa was not normal at the moment the trigger arrived. It had been subclinically injured for years, its activation threshold already at the edge, and the precipitating event did not cause their CRS — it revealed it.
6.1. The Nasopharyngeal Lymphoid Cascade: Adenotonsillar Inflammation as a Parallel Endpoint
The posterior nasal mucosa is not the only nasopharyngeal tissue exposed to pepsin-laden refluxate in children with LPR. Waldeyer’s ring — the circumferential arrangement of lymphoid tissue comprising the adenoid, the palatine tonsils, and the lingual tonsil — sits at the anatomical crossroads where ascending refluxate, descending nasal secretions, and inspired air all converge. If pepsin reaches the nasopharynx in sufficient concentration to be endocytosed by posterior nasal respiratory epithelial cells, it is simultaneously bathing the adenoid and, via the oropharynx, the palatine tonsils.
This is not inferential. Pepsin has been detected in adenoid and tonsillar tissue in published studies. Ozdek and colleagues demonstrated pepsin and pepsinogen in adenoid tissue from children undergoing adenoidectomy, with significantly higher concentrations in children with recurrent disease than in controls. Agackiran and colleagues found similar findings in tonsillar tissue. The adenoid and tonsils are not passive bystanders — they are repeatedly exposed to a proteolytic enzyme capable of receptor-mediated internalization and progressive depletion of the barrier proteins and stress response proteins that protect mucosal surfaces from chronic inflammatory injury.[19,20]
Chronic pepsin exposure of nasopharyngeal lymphoid tissue, I propose, drives the adenotonsillar hypertrophy and recurrent inflammatory cycles that define the pediatric upper airway surgical patient. Pepsin endocytosis in lymphoid epithelium activates inflammatory cytokine cascades, impairs barrier function, and creates a chronically inflamed tissue that responds to each subsequent viral or bacterial exposure with exaggerated, prolonged inflammation. The clinical result — enlarging adenoids, recurrent tonsillitis, and the hypertrophic adenoid that obstructs the Eustachian tube orifice — is the predictable tissue-level consequence of repeated pepsin-driven intracellular injury in lymphoid epithelium.
The mechanical consequence of adenoid hypertrophy closes the loop with the Tasker middle ear finding. An enlarged, inflamed adenoid physically obstructs the Eustachian tube orifice, impairing middle ear pressure equalization and creating the negative pressure environment that draws nasopharyngeal fluid — including pepsin-containing refluxate — into the middle ear space. Pepsin in the middle ear may therefore arrive via two pathways: direct Eustachian tube reflux of nasopharyngeal pepsin, and passive effusion into a middle ear rendered dysfunctional by pepsin-driven adenoid hypertrophy. Both pathways originate from the same upstream source.
The pediatric upper airway surgical triad — pressure equalization tubes, adenoidectomy, and tonsillectomy — represents three separate surgical responses to what may, in a significant subset of patients, be a single upstream problem: untreated or undertreated LPR driving pepsin-mediated inflammation throughout Waldeyer’s ring and the posterior nasal mucosa. The child who receives a third set of tubes, an adenoidectomy at age seven, and a tonsillectomy at age nine may be a child in whom the surgical interventions are addressing the downstream tissue manifestations of pepsin injury while the upstream pepsin exposure continues uninterrupted. This does not argue against surgical intervention — tubes, adenoidectomy, and tonsillectomy remain appropriate treatments for the immediate problems they address. It argues that surgical intervention without concurrent LPR evaluation may be treating the result while leaving the cause active.
The population-level surgical trend data make this epidemiologically urgent. Erickson and colleagues documented that adenotonsillectomy rates rose from 369 per 100,000 person-years in the early 1970s to 638 per 100,000 by 2000–2005 — a 73% increase over three decades. Parker and Walner’s analysis found the absolute number of children undergoing adenotonsillar surgery increased from approximately 441,870 in 1996 to 695,029 in 2006, a 57% increase in ten years. The indication driving this growth was upper airway obstruction and sleep-disordered breathing, rising from 12% of procedures in 1970 to 77% by 2005. Upper airway obstruction is the clinical endpoint of the hypertrophic adenotonsillar tissue that this model predicts as the downstream consequence of chronic pepsin-driven lymphoid inflammation. Zhou and colleagues found that 69.77% of salivary samples from children with adenoid hypertrophy tested pepsin-positive, with a positive correlation between pepsin intensity and adenoid hypertrophy grade. The mechanistic chain from upstream pepsin exposure to downstream surgical intervention is established in the biology.[29,30,31]
7. Clinical Implications
7.1. The CRS Patient with LPR Is a Laryngeal Surveillance Patient
The most immediately actionable implication of this model is the reframing of the LPR-positive CRS patient. If nasal pepsin detection implies laryngeal pepsin endocytosis at equal or greater concentrations, then a patient presenting with refractory posterior CRS and documented or suspected LPR is a patient in whom intracellular pepsin damage is almost certainly active at the level of the larynx and hypopharynx. This does not mean that patient will develop laryngeal cancer — the cofactor model argues they may well not. It means that careful laryngoscopic evaluation of the supraglottis and posterior commissure is warranted, and that a high index of suspicion for laryngeal dysplasia is appropriate in patients with long-duration refractory LPR, particularly those with tobacco or alcohol history. The anatomical gradient model further demands nasopharyngeal attention: Li et al.’s detection of pepsin in 85.7% of NPC tissue confirms that the proximal end of the reflux gradient carries the same tissue-level pepsin burden as the larynx, and nasopharyngoscopy with attention to the fossa of Rosenmüller should be a standard component of the complete surveillance examination in the high-pepsin-burden patient.
7.2. Surgical and Procedural Management in PSS: An Integrated Framework
The framework proposed in this paper does not challenge the surgical and procedural management of CRS broadly — it argues that the correct surgical approach in the PSS subset is fundamentally different from the aggressive tissue-resecting paradigm that has become the default in tertiary rhinologic practice. This distinction matters because PSS patients are overrepresented in the refractory CRS population that presents for revision surgery. Applying the same surgical approach to PSS-driven posterior CRS that is appropriate for polyp-dominant, anatomically obstructive, or fungal CRS is not neutral — it is actively harmful, for reasons the biology of pepsin-driven posterior mucosal injury makes precise.
When the primary driver of CRS is pepsin-induced intracellular injury that has lowered the posterior nasal mucosal inflammatory threshold, the sinus is a victim of upstream molecular disease. Surgery that removes the mucosal substrate — wide antrostomy creating goblet cell-depleted, mucociliary transport-disrupted maxillary sinuses; middle turbinate resection eliminating structural and physiological baffling; ethmoid marsupializtion creating squamous metaplastic patchwork healing — does not address the intracellular mechanism and destroys the tissue architecture that pepsin-directed treatment requires intact in order to produce mucosal recovery.
The appropriate surgical role in the PSS patient is mucosal preservation: balloon sinuplasty restoring ostial patency without mucosal resection, natural ostium-preserving approaches consistent with Setliff’s small hole surgery principles, and procedures that address anatomic, physiologic, and neural contributors to posterior disease without converting recoverable respiratory epithelium into permanent squamous metaplastic surfaces.
Balloon sinuplasty is the surgical expression of the correct biological logic in the PSS patient. It restores ostial patency through catheter-based dilation of the natural ostium without mucosal resection, without bone removal at the ostium margins, and without disrupting the ciliary continuity that mucociliary transport requires. Goblet cell populations, secretory IgA production, innate immune mucosal coating, and the respiratory columnar epithelial architecture that pepsin-directed treatment depends on are preserved intact. In the PSS patient with ongoing pepsin delivery, balloon sinuplasty leaves the posterior nasal and sinonasal mucosal substrate in a state where — if pepsin burden is simultaneously reduced — it retains the biological capacity to recover.
Functional endoscopic sinus surgery remains appropriate where the primary driver is genuinely anatomical: significant polypoid disease producing mechanical obstruction, anatomic variants generating contact-point inflammation, or fungal disease requiring surgical debridement. In the PSS patient whose posterior CRS is driven by pepsin-induced mucosal priming rather than anatomical obstruction, the indication for aggressive tissue-resecting FESS does not exist.
Turbinate reduction restores nasal airflow and reduces nasal resistance in PSS patients whose turbinate hypertrophy reflects both anatomic predisposition and pepsin-driven posterior mucosal inflammatory burden. The clinical consequences of improved nasal airflow extend substantially beyond sinus symptom scores. Restored nasal breathing improves sleep architecture, reduces sleep-disordered breathing, and addresses the brain fog and sleep disturbance that a significant subset of PSS patients describe as among their most debilitating symptoms.
Eustachian tube balloon dilation addresses the posterior nasopharyngeal inflammatory consequence of pepsin-driven mucosal injury at the Eustachian tube orifice. Chronic nasopharyngeal mucosal inflammation in PSS patients impairs Eustachian tube function, reduces pressure equalization capacity, and contributes to the ear fullness, pressure sensation, and muffled hearing that accompany posterior CRS in a significant proportion of patients. Its durability in PSS patients is optimized when combined with upstream pepsin-directed management.
Neuromodulation of the posterior nasal nerve requires precise anatomical distinction between the currently available procedures. Cryotherapy via ClariFix and radiofrequency neuromodulation via RhinAer both target the posterior nasal nerve at the sphenopalatine foramen region in the posterior lateral nasal wall. Both downregulate posterior nasal nerve activity in the immediate nasal cavity territory. Their treatment zone, however, does not extend to the nasopharynx.
The Neumark procedure delivers radiofrequency neuromodulation at the sphenopalatine foramen region and then extends treatment with two additional delivery points in the nasopharynx that neither ClariFix nor RhinAer reaches. This is the defining clinical distinction of the Neumark procedure: it encompasses the established foraminal treatment zone and expands beyond it into the nasopharyngeal peripheral branch network that innervates the posterior nasal mucosa in its deepest territory, the nasopharynx itself, and the autonomic supply to the Eustachian tube orifice. The result is a substantially greater total surface area of radiofrequency neuromodulation delivered into the posterior nasal and nasopharyngeal nerve field in a single treatment session. The procedure is designed for office-based delivery under local anesthesia, making it accessible to a wider range of providers and facilitating the repeat treatment sessions that a reversible neuromodulatory approach permits.
For the PSS patient, whose disease is concentrated in exactly the nasopharyngeal territory that the Neumark procedure’s additional treatment points specifically reach, Neumark is the neuromodulation procedure whose anatomical coverage matches the PSS disease distribution. Pepsin endocytosis in posterior nasal and nasopharyngeal epithelial cells drives chronic cytokine activation and mucosal inflammation that continuously hyperstimulates the posterior nasal nerve branches distributing through that territory. Neumark, by downregulating those nasopharyngeal nerve branches, may interrupt one of the neural amplification loops that perpetuates PSS independent of ongoing pepsin exposure.
7.3. Pepsin-Directed Medical Management: A Practical Treatment Framework
There is currently no formally established, guideline-endorsed treatment protocol specifically for pepsin-driven CRS or PSS. This absence is a direct consequence of the diagnostic infrastructure gap described in Section 9 — without a validated clinical assay for nasal pepsin, there is no recognized patient population around which to build a treatment protocol. What follows represents the best available evidence-based framework for pepsin-directed management, synthesized from the LPR literature, the Koufman dietary work, the Johnston mechanistic studies, and 30 years of clinical observation in a high-volume rhinology practice.
Dietary modification is the most mechanistically grounded and immediately accessible intervention. The low-acid, low-fat diet developed and refined by Koufman and colleagues reduces both gastric acid production and gastric pepsin secretion at the source. The primary dietary triggers to eliminate are coffee, alcohol, carbonated beverages, citrus, tomatoes, chocolate, mint, and high-fat foods. These do not merely increase reflux frequency — several directly stimulate gastric pepsin secretion and reduce lower esophageal sphincter tone, increasing both the volume and proteolytic activity of the refluxate reaching the upper airway. Dietary modification is the upstream intervention that reduces the pepsin burden available for endocytosis before it reaches the posterior nasal mucosa and larynx. Patient compliance with dietary modification is the single most important determinant of treatment response in pepsin-driven CRS, and the counseling investment required to achieve it is substantially higher than prescribing a medication.[28]
Alkaline water at pH 8.8 or higher is a mechanistically grounded adjunct to dietary modification, but its precise mechanism and anatomical scope require accurate framing to avoid clinical misapplication. Koufman’s group demonstrated that pH 8.8 water irreversibly denatures pepsin — permanently eliminating its proteolytic activity through alkaline hydrolysis. This distinction matters: pepsin remains structurally stable and reactivatable at pH up to 8.0, so only water at or above pH 8.8 achieves irreversible rather than merely reversible inactivation. The observation that endocytosis is maximized at neutral pH 7.0 — when pepsin is enzymatically silent but structurally intact — explains precisely why conventional water and PPI-alkalinized refluxate fail to prevent pepsin injury: they create the neutral pH environment that maximizes cellular uptake without reaching the 8.8 threshold required for irreversible denaturation. High-dose BID proton pump inhibitor therapy similarly fails to solve this problem: PPI-suppressed gastric pH typically reaches 4–6, which renders pepsin inactive but not denatured, and once pepsin is internalized into the late endosomal and trans-Golgi compartment where pH drops to approximately 5.5, it reactivates intracellularly regardless of extracellular acid suppression.[25]
For PSS patients whose primary pepsin burden is posterior nasal and nasopharyngeal, swallowed alkaline water addresses the pharyngeal and laryngeal LPR injury gradient but does not reach the nasal cavity or nasopharynx by the swallowing route. Alkaline saline nasal lavage directed posteriorly toward the choana is the delivery vehicle for the PSS-specific anatomical target. Both interventions are appropriate and complementary in the PSS patient, and both should be prescribed explicitly.
Alginate-based barrier therapy is the most mechanistically targeted anti-pepsin treatment currently available and the most underutilized in United States clinical practice. Sodium alginate preparations form a physical raft on the surface of gastric contents immediately after ingestion, mechanically preventing refluxate from reaching the upper esophageal sphincter and physically trapping pepsin within the gastric compartment before it can reflux into the upper airway. Unlike acid suppression, alginates act on pepsin directly — binding it at the source regardless of refluxate pH. Alginate preparations available in the United States should be used after meals and at bedtime in PSS patients with suspected or confirmed pepsin-driven disease.
Proton pump inhibitors retain a role in PSS management for patients with concurrent acid-driven esophageal disease, where they are appropriate and necessary. However, PPIs do not suppress pepsin and may paradoxically optimize endocytosis conditions by raising refluxate pH toward neutral. PPIs should be used at the lowest effective dose in PSS patients and should never be presented to the patient as the primary treatment for their posterior mucosal disease.
Posterior nasal saline irrigation — high-volume, directed posteriorly toward the nasopharynx — reduces surface pepsin dwell time in the posterior nasal cavity and nasopharynx by mechanical washout. Irrigation technique matters significantly in PSS patients: standard anterior-directed irrigation inadequately reaches the posterior nasal cavity and nasopharynx where pepsin deposition is concentrated. High-volume squeeze bottle or pulsatile irrigation directed toward the posterior choana, performed twice daily, is the appropriate technique.
Head of bed elevation — 6 to 8 inches — reduces nocturnal LPR, which is mechanistically the most damaging reflux pattern in PSS. During sleep, salivary bicarbonate production essentially ceases, swallowing frequency drops dramatically, and refluxate that reaches the upper airway dwells at mucosal surfaces far longer than during waking hours. Gravity elevation of the head of bed — not pillow elevation, which flexes the neck and may worsen reflux — reduces this nocturnal exposure substantially.
7.4. The Limitation of Acid Suppression Alone
Effective LPR management in PSS requires pepsin containment, not just acid suppression. Alginates physically bind pepsin in the refluxate before it reaches the upper airway. Dietary modification eliminates the triggers that stimulate pepsin secretion at the source. PPI therapy addresses a co-traveler, not the driver, and its limitations are mechanistically predictable from the endocytosis model described in Section 3.
7.5. The Pediatric Surgical Patient Deserves an LPR Evaluation
The adenotonsillar cascade described in Section 6.1 has one immediate clinical implication that requires no new research to implement: the child with recurrent, refractory, surgically-resistant upper airway disease deserves a systematic LPR evaluation before additional surgical intervention is planned. Not every child with a first ear infection — the child who needs a third set of tubes, whose adenoid regrows, who returns for a fourth procedure. That child deserves the question: is there an upstream pepsin-driven process that surgery is not reaching?
In my experience, LPR in children is systematically underdiagnosed because its presentation differs from adult reflux disease. Children with LPR rarely complain of heartburn. They present with chronic cough, throat clearing, noisy breathing, and recurrent respiratory infections — the exact upper airway surgical indications described above. The absence of classic GERD symptoms in a child with recurrent otitis, adenoid hypertrophy, and tonsillar disease should not be interpreted as the absence of reflux. It should prompt consideration of LPR as the silent upstream driver.
7.6. PSS and the 2025 AAO-HNS Clinical Practice Guideline: The Missing Inflammatory Driver
The 2025 AAO-HNS clinical practice guideline update on chronic rhinosinusitis represents the most authoritative current statement from the specialty on CRS management. The guideline makes three antibiotic-related recommendations that collectively reframe CRS as primarily inflammatory rather than primarily infectious: watchful waiting is recommended for acute bacterial rhinosinusitis unless symptoms have persisted a minimum of 14 days; when antibiotics are prescribed, a 5 to 7 day course is now recommended; and saline irrigation followed by topical intranasal corticosteroids — not antibiotics — is positioned as the primary first-line treatment for CRS. These recommendations are correct and overdue.[23]
However, the guideline’s inflammation-focused framework reaches a ceiling in the PSS patient that it does not yet have the mechanistic vocabulary to explain. The PSS patient has already been irrigating with saline. They have already been using topical intranasal corticosteroids daily, often for years. Their posterior mucosal inflammation persists despite faithful adherence to exactly the treatment the 2025 guideline recommends — because those treatments, however appropriate, are operating at the wrong level. Saline irrigation mechanically removes surface debris. Topical corticosteroids suppress cytokine signaling at the epithelial surface. Neither penetrates the cell. Neither reverses pepsin-driven mitochondrial damage. Neither restores the E-cadherin, carbonic anhydrase isoenzyme III, and stress proteins that pepsin endocytosis has progressively depleted from posterior nasal epithelial cells over years or decades.
The PSS patient who has exhausted the 2025 guideline’s treatment ladder is the patient for whom the guideline has no remaining answer — because the guideline does not yet recognize pepsin-driven intracellular injury as a distinct inflammatory mechanism in CRS. Allergy and anatomy have long been recognized as the two dominant modifiable contributors to CRS inflammation. Pepsin-driven posterior nasal mucosal injury is the third inflammatory driver — one that operates independently of allergy, independently of anatomy, and independently of infection. PSS is the clinical name for the CRS phenotype in which this third driver is dominant.
8. Gaps in the Evidence and Required Studies
This model is a hypothesis grounded in existing peer-reviewed data. Several confirmatory studies are required before it can be considered established.
The single most immediately practice-changing priority this paper identifies is the development and clinical validation of a quantitative posterior nasal lavage pepsin assay. The technology base exists: the monoclonal antibody platform developed from Johnston’s work and commercialized in the Peptest salivary lateral flow assay could be adapted to nasal lavage matrix with appropriate validation studies. What does not exist is a validated, standardized, clinically accessible office-based tool that a rhinologist could deploy at the time of nasal endoscopy — collecting a posterior nasal aspirate, processing by validated ELISA with established reference ranges, and receiving back a quantitative pepsin concentration result that distinguishes no exposure, low-level exposure, clinically significant PSS-range exposure, and high-burden cancer-risk-stratifying exposure. The validation study is straightforward in design: collect posterior nasal lavage samples prospectively from patients with PSS-pattern posterior CRS, anterior-predominant CRS, LPR without CRS, and normal controls; measure pepsin concentration by validated ELISA; correlate with symptom severity scores, endoscopic findings, and treatment response to pepsin-directed therapy. Without this assay, PSS remains a clinical and inferential diagnosis. With it, PSS becomes a laboratory-confirmable diagnosis with an objective quantitative measure of disease burden.
The following confirmatory studies address the mechanistic and clinical gaps that precede or accompany assay validation, organized by priority tier.
Tier 1 studies are executable in a high-volume rhinology practice without requiring basic science infrastructure. Study 2: Posterior nasal biopsy histopathology and pepsin immunohistochemistry in PSS — the single most critical mechanistic gap in this paper. Design: prospective case series with controls. Posterior nasal mucosal biopsy at time of endoscopy in PSS patients, anterior-predominant CRS patients, and normal controls. Primary outcome: prevalence of intracellular pepsin in posterior nasal columnar epithelium in PSS versus controls. A positive result transforms the PSS mechanism from strongly inferred to established. Study 3: Retrospective surgical history cohort study testing the developmental hypothesis using existing practice records — comparing adult PSS patients, anterior-predominant CRS patients, and normal controls on childhood surgical history including PE tube insertions, adenoidectomy, and tonsillectomy. Study 4: Laryngoscopic survey of PSS patients confirming that posterior nasal mucosal injury in PSS is accompanied by laryngoscopic evidence of pepsin-driven injury at the higher-concentration end of the same reflux gradient. Study 7: Prospective pepsin-directed PSS treatment trial with pre-post comparison and matched controls, measuring symptom severity score change, posterior nasal endoscopic mucosal appearance, and nasal lavage pepsin concentration at six and twelve months.
Tier 2 studies require academic pathology infrastructure or multi-site collaboration. Study 5: Pepsin immunohistochemistry in sinonasal carcinoma tissue — the most important named gap in the field cancerization section, directly testing whether pepsin is present in sinonasal SCC and adenocarcinoma tissue and providing the first direct tissue evidence connecting pepsin to sinonasal malignancy. Study 6: Squamous metaplasia characterization in post-FESS versus post-balloon sinuplasty maxillary sinus mucosa at one year — the direct tissue-level test of the surgical philosophy argument.
Tier 3 studies test the developmental and field cancerization hypotheses at population scale. Study 9: Administrative claims database analysis of pediatric surgical history and adult CRS, testing the developmental hypothesis using existing insurance claims data. Study 10: Longitudinal LPR exposure and CRS incidence cohort following LPR-confirmed adults without baseline CRS for five years, with incident CRS diagnosis compared to matched non-LPR controls.
9. The Diagnostic Infrastructure Gap: Why Clinical Pepsin Detection Must Become Standard of Care
The science described in this paper is not new. Johnston established receptor-mediated pepsin endocytosis in laryngeal epithelial cells in 2007. Southwood demonstrated pepsin-driven mitochondrial damage in human nasal epithelial cells in 2015. Tasker found pepsin in middle ear effusion fluid in 2002. Nearly two decades have elapsed. The reason this mechanism has not changed clinical practice is not scientific — it is infrastructural. The tools required to detect pepsin in clinical specimens do not exist within the standard clinical laboratory and billing framework that governs day-to-day medical care.
As a practicing rhinologist in a private practice setting, I confront this gap daily. I cannot order a nasal secretion pepsin assay the way I order a culture, a complete blood count, or an allergen panel. There is no CPT code for nasal lavage pepsin quantification. There is no insurance reimbursement pathway for salivary or nasal pepsin testing in the context of CRS evaluation. There is no College of American Pathologists-validated protocol that allows a clinical pathology laboratory to process a nasal secretion specimen for pepsin concentration and return a reportable result. The PepTest salivary pepsin assay, commercially available in the United Kingdom, has no equivalent clinical billing infrastructure in the United States.[22]
The wrong diagnostic standard has compounded this problem. Twenty-four hour pH monitoring became the clinical gold standard for LPR diagnosis because it was available, quantifiable, and reimbursable — not because it measured the right molecule. pH monitoring detects acid. It does not detect pepsin. A patient with predominantly non-acidic or weakly acidic LPR will test negative on pH monitoring despite having active pepsin in their hypopharynx at concentrations sufficient for endocytosis. This patient’s LPR will be dismissed, their nasal pepsin burden will go unmeasured, and their refractory posterior CRS will continue to be attributed to causes that surgical and antimicrobial treatment cannot address.
A normal upper endoscopy is routinely interpreted as evidence that reflux is not clinically significant. This interpretation is mechanistically unjustified in the context of LPR and pepsin-driven upper airway injury. The esophagus is the most protected tissue in the reflux pathway. It tolerates fifty acid reflux episodes per day without visible injury, while the laryngeal mucosa is damaged by as few as four. A gastroenterologist performing a normal EGD on a patient with refractory posterior CRS and suspected LPR, and concluding that reflux is not contributing to that patient’s disease, is applying the wrong tissue standard to the wrong question. Until gastroenterology and otolaryngology reach a shared understanding that extra-esophageal pepsin injury operates independently of esophageal mucosal damage, patients with PSS will continue to be reassured by a normal scope result that does not speak to their actual disease.
The clinical infrastructure agenda this paper calls for is specific. Validation of a standardized nasal secretion pepsin assay suitable for clinical pathology laboratories, with defined reference ranges. CPT code development for nasal lavage and salivary pepsin quantification. Insurance coverage pathways for pepsin testing in the diagnostic evaluation of refractory CRS, LPR, recurrent pediatric otitis media with effusion, and laryngeal dysplasia. Development of tissue pepsin immunohistochemistry as a clinical pathology service. And a joint statement from the American Academy of Otolaryngology — Head and Neck Surgery and the American College of Gastroenterology acknowledging that a normal EGD does not rule out clinically significant extra-esophageal pepsin injury and that the appropriate diagnostic standard for LPR-driven upper airway disease requires pepsin detection rather than acid detection alone.
None of these infrastructure items requires new science. The science is done. What is required is the institutional will — in otolaryngology professional societies, in clinical pathology, in payer organizations, and in the gastroenterology community — to translate two decades of peer-reviewed mechanistic research into the clinical tools that practicing physicians need to identify pepsin-driven disease in the patients sitting in front of them.
10. Discussion
What emerges from synthesizing these disparate bodies of literature is a picture of a single enzyme — pepsin — operating through a single cellular mechanism — receptor-mediated endocytosis — across an entire anatomical territory, producing disease that has been described as if it were multiple unrelated conditions. Globus pharyngeus, chronic throat clearing, refractory CRS, posterior sinonasal inflammation, recurrent otitis media with effusion, laryngeal dysplasia, and laryngeal carcinoma have each been separately associated with LPR. The proposed model suggests these are not independent associations but sequential stations on a continuum of pepsin-driven upper airway injury, differentiated by anatomical position within the reflux gradient, by the tissue type encountered, and by the cofactors present in individual patients.
The posterior sinonasal mucosa occupies a particular position in this model. Anatomically, it is the most posterior and superior tissue regularly reached by ascending refluxate — a convergence zone where pepsin-laden refluxate, allergens, bacteria, and inflammatory neural signals all intersect. Clinically, it is the tissue most consistently inflamed in patients with refractory CRS who do not respond to standard treatment. My clinical experience over 30 years of rhinologic practice, including extensive work with balloon sinuplasty and in-office procedures under local anesthesia, suggests that posterior sinonasal mucosal inflammation — not anterior disease, not isolated sinus obstruction — is the distinguishing feature of the most refractory CRS subset. The proposed model provides a molecular substrate for that clinical observation.
10.1. Relationship to Existing Literature
The mechanistic foundation of this model rests on established findings that have not previously been synthesized into a clinical framework for rhinologists. Johnston’s pepsin endocytosis mechanism, Tasker’s detection of pepsin in 83% of pediatric middle ear effusions, Zhou’s correlation between nasopharyngeal pepsin concentration and adenoid hypertrophy grade, Southwood’s in vitro posterior nasal cell mitochondrial injury data, and Ren’s pepsin detection in CRS sinonasal tissue each represent independent lines of evidence pointing toward a shared pathophysiological mechanism. The contribution of this paper is not new laboratory data — it is the clinical synthesis connecting those existing findings into a coherent disease model with diagnostic and therapeutic implications.[1,8,18]
The rhinologic literature has not previously named or characterized PSS as a distinct CRS subtype, and the LPR literature has not extended pepsin’s carcinogenic mechanism superiorly beyond the larynx and hypopharynx into the sinonasal tract. Li et al.’s independent detection of pepsin within nasopharyngeal carcinoma tissue — at the proximal end of the same reflux gradient where Johnston established pepsin’s carcinogenic molecular footprint in laryngeal tissue — provides the two-site tissue-level evidence that elevates the field cancerization argument from mechanistic inference to direct anatomical confirmation across the upper aerodigestive mucosal surface.[13]
10.2. Strengths of the Proposed Model
The model’s primary strength is mechanistic coherence. Each step in the proposed pathophysiological sequence is grounded in a mechanism that has been demonstrated in adjacent tissue types or predicted by in vitro data. The model does not require new biology — it requires extension of established biology into an anatomical territory that has not previously been systematically examined. A second strength is clinical testability: the core predictions of PSS are testable in a high-volume rhinology practice with existing clinical tools. A third strength is the explanatory power of the model for the refractory posterior CRS patient who fails every anatomically and immunologically directed intervention, whose CT and endoscopy are discordant with symptom severity, and whose disease waxes and wanes with dietary and positional factors that modulate pepsin delivery.
10.3. Limitations and What the Model Cannot yet Prove
The central limitation is that this paper is a hypothesis without a prospective clinical trial. No randomized controlled study has tested whether pepsin-directed management produces superior outcomes to standard CRS treatment in a PSS-defined patient population. No longitudinal cohort has confirmed that childhood pepsin burden prospectively predicts adult CRS. No tissue study has demonstrated pepsin endocytosis in posterior nasal respiratory columnar epithelium specifically. The field cancerization model, while mechanistically coherent and supported by Li et al.’s NPC tissue finding and Johnston’s laryngeal tissue detection — together providing the two-site anatomical evidence that a field carcinogen requires — has not been tested with systematic IHC across the full spectrum of sinonasal malignancy specimens.
A second category of limitation is diagnostic. PSS as defined in this paper does not yet have a validated diagnostic instrument. Until the quantitative nasal lavage pepsin assay is validated, PSS diagnosis rests on clinical pattern recognition — posterior-predominant symptoms, treatment resistance, and concordant LPR history — which is subject to ascertainment bias.
A third limitation is the evidentiary basis for the field cancerization and carcinogenic claims. The two-site tissue detection provides the anatomical anchoring the field cancerization claim requires, but the full spectrum of upper aerodigestive malignancy has not been systematically surveyed by pepsin IHC, and the absolute risk elevation the model implies has not been quantified. The surveillance and behavioral modification recommendations for high-pepsin-burden patients are therefore precautionary rather than evidence-based in the strict sense — appropriate given the mechanistic basis and the low harm of the intervention, but requiring explicit acknowledgment that they anticipate rather than reflect confirmatory data.
10.4. Clinical Implications Prior to Confirmatory Evidence
Despite the absence of confirmatory trial data, the PSS model generates several clinical recommendations that are immediately actionable, low-risk, and mechanistically defensible. Recognizing the posterior-predominant symptom pattern and treatment resistance profile of PSS costs nothing and changes how a rhinologist evaluates a refractory CRS patient. Asking about LPR history, dietary acid load, and positional symptoms in every posterior CRS patient is a history-taking change, not an intervention. Defaulting to mucosal-preserving surgical approaches in patients with posterior-predominant disease and LPR history avoids irreversible harm without requiring pepsin confirmation. Initiating pepsin-directed medical management in the patient with confirmed LPR and refractory posterior CRS has a favorable risk-benefit profile at any level of mechanistic certainty. These are not actions that require a randomized controlled trial. They are the rational clinical response to a mechanistically coherent model in a patient population that current standard of care is already failing.
10.5. Origin of the Hypothesis and Its Implications for Interpretation
This hypothesis emerges from 30 years of rhinologic practice rather than from a basic science laboratory. The clinical observations that generated the PSS model — the posterior-predominant presentation, the treatment resistance profile, the dietary and positional modulation of symptoms, the discordance between imaging findings and symptom severity, and the relationship to LPR history — are pattern observations from a high-volume single-practice rhinology experience. They carry the evidentiary weight of extensive clinical observation by an experienced rhinologist, not the statistical power of a prospective multi-site study. The synthesis connecting those observations to Johnston’s molecular biology, Tasker’s middle ear data, Zhou’s adenoid data, and the field cancerization literature is this paper’s original intellectual contribution. The model should be evaluated as a hypothesis that deserves urgent confirmatory investigation — not as a conclusion that the evidence has already established, and not as a speculation that lacks mechanistic grounding.
11. Conclusions
Pepsin-driven receptor-mediated endocytosis is proposed as a universal mechanism of upper airway injury in patients with LPR, operating across the entire aerodigestive tract via a defined concentration gradient, beginning not in adulthood but in childhood. In the pediatric upper airway, pepsin exposure of nasopharyngeal lymphoid tissue drives the chronic adenotonsillar inflammation underlying the pediatric surgical triad — the same triad that may be the earliest clinical expression of a lifelong pepsin-driven disease process. In the posterior nasal mucosa, years of subclinical intracellular injury accumulate silently through childhood and adolescence, lowering the mucosal activation threshold until adult CRS emerges. In the larynx and hypopharynx, the same injury in squamous epithelium creates the compromised cellular environment in which carcinogenic cofactors can complete a malignant transformation — a carcinogenic role confirmed by pepsin’s detection within laryngeal carcinoma tissue itself, and extended across the upper aerodigestive field by Li et al.’s independent detection of pepsin within nasopharyngeal carcinoma tissue at the proximal end of the same reflux gradient.
This framework supports aggressive, pepsin-directed LPR management across the entire lifespan — beginning in children with recurrent otitis media and adenotonsillar disease, continuing in adults with refractory posterior CRS and Posterior Sinonasal Syndrome, and extending to careful laryngoscopic and nasopharyngoscopic surveillance in the LPR-positive rhinology patient. Five specific confirmatory studies and three executable clinical research programs require no laboratory infrastructure to pursue. Chronic rhinosinusitis, long understood as a disease of adult onset with adult causes, belongs in its proper developmental context: the end-stage presentation of a process that began in the nasopharynx of a child, driven by an enzyme that medicine has spent thirty years looking at in the wrong tissue.
Author Contributions
FRG: Conceptualization, hypothesis development, literature synthesis, manuscript preparation.
Funding
No external funding was received for this work.
Acknowledgments
During the preparation of this manuscript, the author used Claude (Anthropic) to assist with literature synthesis, structural organization, and editorial refinement of language and readability. All AI-assisted content was reviewed, revised, and approved by the author. The hypothesis, clinical framework, original observations, and all scientific conclusions are the author’s own. The author takes full responsibility for the accuracy and integrity of all content in this manuscript.
Conflicts of Interest
The author declares no conflicts of interest relevant to this manuscript.
References
- Johnston, N; Wells, CW; Blumin, JH; Toohill, RJ; Merati, AL. Receptor-mediated uptake of pepsin by laryngeal epithelial cells. Ann Otol Rhinol Laryngol. 2007, 116(12), 934–938. [Google Scholar] [CrossRef]
- Johnston, N; Dettmar, PW; Lively, MO; Postma, GN; Belafsky, PC; Birchall, M; Koufman, JA. Effect of pepsin on laryngeal stress protein (Sep70, Sep53, and Hsp70) response: role in laryngopharyngeal reflux disease. Ann Otol Rhinol Laryngol. 2006, 115(1), 47–58. [Google Scholar] [CrossRef] [PubMed]
- Gill, GA; Johnston, N; Buda, A; Pignatelli, M; Pearson, J; Dettmar, PW; Koufman, J. Laryngeal epithelial defenses against laryngopharyngeal reflux: investigations of E-cadherin, carbonic anhydrase isoenzyme III, and pepsin. Ann Otol Rhinol Laryngol. 2005, 114(12), 913–921. [Google Scholar] [CrossRef] [PubMed]
- Johnston, N; Wells, CW; Samuels, TL; Blumin, JH. Rationale for targeting pepsin in the treatment of reflux disease. Ann Otol Rhinol Laryngol. 2010, 119(8), 547–558. [Google Scholar] [CrossRef]
- Johnston, N; Yan, JC; Hoekzema, CR; Samuels, TL; Stoner, GD; Blumin, JH; et al. Pepsin promotes proliferation of laryngeal and pharyngeal epithelial cells. Laryngoscope 2012, 122(6), 1317–1325. [Google Scholar] [CrossRef]
- Southwood, JE; Hoekzema, CR; Samuels, TL; Wells, C; Poetker, DM; Johnston, N; Loehrl, TA. The impact of pepsin on human nasal epithelial cells in vitro: a potential mechanism for extraesophageal reflux induced chronic rhinosinusitis. Otolaryngol Head Neck Surg. 2015, 153(2), 208–215. [Google Scholar] [CrossRef]
- Samuels, TL; Johnston, N. Pepsin as a causal agent of inflammation during nonacidic reflux. Otolaryngol Head Neck Surg. 2009, 141(3), 559–563. [Google Scholar] [CrossRef]
- Ren, JJ; Zhao, Y; Wang, J; Ren, X; Xu, Y; Tang, W; et al. Pepsin as a marker of laryngopharyngeal reflux detected in chronic rhinosinusitis patients. Otolaryngol Head Neck Surg. 2017, 156(5), 893–900. [Google Scholar] [CrossRef]
- Bardhan, KD; Strugala, V; Dettmar, PW. Reflux revisited: advancing the role of pepsin. Int J Otolaryngol. 2012, 2012, 646901. [Google Scholar] [CrossRef] [PubMed]
- Aldajani, A; Alzhrani, F; Alhefdhi, AH; et al. Association between laryngopharyngeal reflux and chronic rhinosinusitis: a systematic review and meta-analysis. Am J Rhinol Allergy 2024, 38(2), 91–99. [Google Scholar] [CrossRef]
- Luo, J; Pan, X; Zhang, C; Wang, S. Gastroesophageal and laryngopharyngeal reflux associated with laryngeal malignancy: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2019, 17(1), 39–46. [Google Scholar]
- Lewin, JS; Gillenwater, AM; Garrett, JD. Characterization of laryngopharyngeal reflux in patients with premalignant or early carcinomas of the larynx. Cancer 2003, 97(4), 1010–1014. [Google Scholar] [CrossRef]
- Li, Y; Chen, J; Zhou, M; et al. Expression of pepsin in nasopharyngeal carcinoma and its correlation with quality of life after radiotherapy. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2022, 57(6), 686–692. [Google Scholar]
- Tae, K; Jin, BJ; Ji, YB; Jeong, JH; Cho, SH. The role of laryngopharyngeal reflux as a risk factor in laryngeal cancer: a preliminary report. Clin Exp Otorhinolaryngol. 2011, 4(2), 101–104. [Google Scholar]
- Blaine-Sauer, S; Samuels, TL; Yan, K; Johnston, N. Amprenavir inhibits pepsin-mediated laryngeal epithelial disruption and E-cadherin cleavage in vitro. Laryngoscope 2023, 133(8), 1940–1948. [Google Scholar]
- Samuels, TL; Johnston, N. Pepsin promotes activation of epidermal growth factor receptor and downstream oncogenic pathways at slightly acidic and neutral pH in exposed hypopharyngeal cells. Cancer Med. 2021, 10(9), 3089–3100. [Google Scholar]
- Koufman, JA. The otolaryngologic manifestations of gastroesophageal reflux disease (GERD): a clinical investigation of 225 patients using ambulatory 24-hour pH monitoring and an experimental investigation of the role of acid and pepsin in the development of laryngeal injury. Laryngoscope 1991, 101 (4 Pt 2 Suppl 53, 1–78. [Google Scholar] [PubMed]
- Tasker, A; Dettmar, PW; Panetti, M; Koufman, JA; Birchall, JP; Pearson, JP. Is gastric reflux a cause of otitis media with effusion in children? Laryngoscope 2002, 112(11), 1930–1934. [Google Scholar] [CrossRef]
- Ozdek, A; Cirak, MY; Samim, E; Bayiz, U; Ozcan, KM; Turet, S. A possible role of Helicobacter pylori in chronic rhinosinusitis: a preliminary report. Laryngoscope 2003, 113(4), 679–682. [Google Scholar] [CrossRef] [PubMed]
- Agackiran, Y; Ozcan, KM; Akdogan, O; Dere, H. Helicobacter pylori reinvestigation in tonsils with updated detection method and literature review. Ann Otol Rhinol Laryngol. 2010, 119(3), 177–181. [Google Scholar]
- Yilmaz, T; Ceylan, M; Akyol, A; Ozcan, M; Gürsel, B. Possible role of gastroesophageal reflux in the etiology of adenoid hypertrophy in pediatric patients. Otolaryngol Head Neck Surg. 2008, 138(5), 561–565. [Google Scholar]
- Hayat, JO; Gabieta-Somnez, S; Yazaki, E; et al. Pepsin in saliva for the diagnosis of gastro-oesophageal reflux disease. Gut 2015, 64(3), 373–380. [Google Scholar]
- Rosenfeld, RM; Piccirillo, JF; Chandrasekhar, SS; et al. Clinical Practice Guideline (Update): Adult Sinusitis. Otolaryngol Head Neck Surg 2025, 173(S1), S1–S56. [Google Scholar]
- Sedaghat, AR; Gray, ST; Chambers, KJ; et al. Clinical Practice Guideline: Acute Rhinosinusitis in Adults. Otolaryngol Head Neck Surg 2025, 172(S2), S1–S47. [Google Scholar]
- Koufman, JA; Johnston, N. Potential benefits of pH 8.8 alkaline drinking water as an adjunct in the treatment of reflux disease. Ann Otol Rhinol Laryngol. 2012, 121(7), 431–434. [Google Scholar]
- Strugala, V; Avis, J; Jolliffe, IG; Johnstone, LM; Dettmar, PW. The role of an alginate suspension on pepsin and bile acids — key aggressors in the gastric refluxate. Does this have implications for the treatment of gastro-oesophageal reflux disease? J Pharm Pharmacol. 2009, 61(8), 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, HB; Sweet, S; Winchester, CC; Dent, J. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut 2014, 63(6), 871–880. [Google Scholar] [CrossRef]
- Koufman, JA. Low-acid diet for recalcitrant laryngopharyngeal reflux: therapeutic benefits and their implications. Ann Otol Rhinol Laryngol. 2011, 120(5), 281–287. [Google Scholar] [CrossRef] [PubMed]
- Erickson, BK; Larson, DR; St Sauver, JL; Meverden, RA; Orvidas, LJ. Changes in incidence and indications of tonsillectomy and adenotonsillectomy, 1970-2005. Otolaryngol Head Neck Surg 2009, 140(6), 894–901. [Google Scholar]
- Parker, NP; Walner, DL. Trends in the indications for pediatric tonsillectomy or adenotonsillectomy. Int J Pediatr Otorhinolaryngol. 2011, 75(2), 282–285. [Google Scholar]
- Zhou, X; Yan, F; Chen, C; et al. Association between laryngopharyngeal reflux and changes in adenoid hypertrophy in children. Evid Based Complement Alternat Med. 2023, 2023, 5531628. [Google Scholar] [CrossRef] [PubMed]
- Maniaci, A; Lavalle, S; Masiello, E; et al. Gene expression biomarkers for personalized treatment of laryngeal cancer. J Pers Med. 2024, 14(2), 175. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



