Submitted:
04 March 2026
Posted:
05 March 2026
You are already at the latest version
Abstract
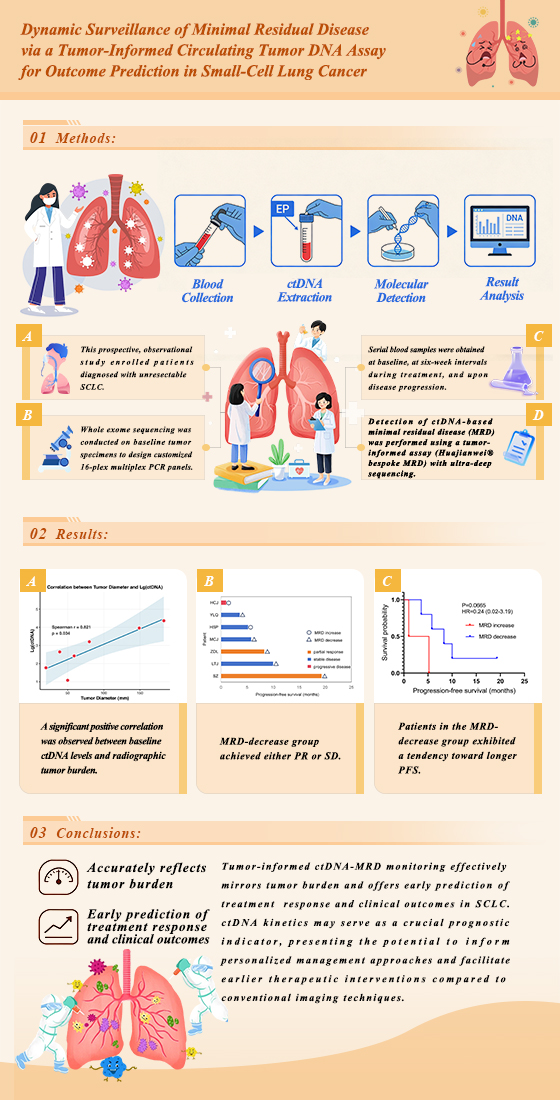
Background: Small-cell lung cancer (SCLC) represents an aggressive malignancy associated with a poor prognosis, underscoring the critical demand for enhanced monitoring methodologies. Circulating tumor DNA (ctDNA) constitutes a promising non-invasive biomarker; however, reports employing highly sensitive, tumor-informed assays in SCLC remain scarce. This investigation aimed to assess the clinical utility of a personalized ctDNA monitoring strategy for predicting therapeutic outcomes and resistance in SCLC patients. Methods: This prospective, observational study enrolled patients diagnosed with unresectable SCLC. Whole exome sequencing was conducted on baseline tumor specimens to design customized 16-plex multiplex PCR panels. Serial blood samples were obtained at baseline, at six-week intervals during treatment, and upon disease progression. Detection of ctDNA-based minimal residual disease (MRD) was performed using a tumor-informed assay (Huajianwei® bespoke MRD) with ultra-deep sequencing. Results: Among seven evaluable patients, the baseline ctDNA-MRD positivity rate was 100%. A significant positive correlation was observed between baseline ctDNA levels and radiographic tumor burden (r = 0.821, P = 0.034). Longitudinal analysis indicated that patients exhibiting an early decline in MRD levels (n=5) demonstrated a trend toward superior progression-free survival (PFS) compared to those with an MRD increase (n=2) (P = 0.0665, hazard ratio (HR) = 0.24 (95% CI: 0.02 - 3.19)). Notably, elevation in MRD preceded radiographic progression by as much as 135 days in certain instances. Conclusions: Tumor-informed ctDNA-MRD monitoring effectively mirrors tumor burden and offers early prediction of treatment response and clinical outcomes in SCLC. ctDNA kinetics may serve as a crucial prognostic indicator, presenting the potential to inform personalized management approaches and facilitate earlier therapeutic interventions compared to conventional imaging techniques.
Keywords:
small-cell lung cancer
; circulating tumor DNA
; minimal residual disease
; liquid biopsy
; tumor-informed
1. Introduction
Lung cancer remains the foremost cause of cancer-associated mortality globally [1]. Primary lung cancer is primarily categorized into two major pathological subtypes: non-small cell lung cancer (NSCLC) and small-cell lung cancer (SCLC). Although SCLC constitutes only 15% to 20% of all primary lung cancer cases [2], it is distinguished by a high degree of malignancy, poor differentiation, and rapid proliferation, contributing to an exceptionally poor prognosis with a five-year survival rate below 5% [3,4]. Given its aggressive characteristics, there exists a pressing and substantial clinical requirement for effective strategies for early disease detection, real-time assessment of therapeutic response, and accurate prognostic forecasting.
Circulating tumor DNA (ctDNA) has emerged as a precise, non-invasive predictive biomarker with considerable potential across the spectrum of cancer management, encompassing early screening, diagnosis, prognostic assessment, and treatment monitoring [5,6,7]. In SCLC, dynamic alterations in ctDNA levels function as a sensitive metric for evaluating therapeutic response and forecasting survival outcomes. For example, an early reduction in ctDNA levels exceeding two-fold during chemotherapy is significantly correlated with extended progression-free survival (PFS) and overall survival (OS) [8]. Similarly, patients who achieve clearance of the molecular tumor burden index (mTBI) following induction chemotherapy demonstrate prolonged OS [9]. Moreover, ctDNA status can aid in identifying patients most likely to respond to immunotherapy. An integrated algorithm that incorporates serial ctDNA measurements during chemoradiotherapy, prophylactic cranial irradiation, and radiographic regression has been demonstrated to effectively predict progression risk and pinpoint high-risk limited-stage (LS)-SCLC populations who would derive maximal benefit from consolidation immunotherapy [10].
Research has established that the molecular response of ctDNA, characterized by the clearance of mutations and copy number variations, can predict clinical outcomes approximately four weeks earlier than conventional imaging modalities on average; patients exhibiting a molecular response demonstrate significantly improved PFS and OS [11]. Conversely, elevated baseline ctDNA levels and the persistence of ctDNA positivity following consolidation immunotherapy are associated with an unfavorable prognosis [10,12,13]. Extensive evidence underscores the critical role of minimal residual disease (MRD) in predicting outcomes for patients with locally advanced or advanced lung cancer [14,15]. Next-generation sequencing (NGS)-based ctDNA detection serves as the primary methodology for MRD monitoring [16]. In solid tumors, two principal strategies are employed for MRD detection: tumor-informed and tumor-agnostic analysis. The tumor-informed approach represents a highly sensitive and specific technique [17]. It involves performing NGS on blood samples using a predefined panel of oncogenic mutations or employing machine learning algorithms to identify potential tumor-derived ctDNA variants. Furthermore, by conducting comparative analyses between tumor and normal tissues and utilizing small, targeted panels (typically spanning a few kilobases) sequenced to ultra-high depth (often exceeding 100,000x coverage) [18], the tumor-informed method effectively distinguishes ctDNA signals of tumor origin from background noise, such as clonal hematopoiesis or germline variants. This significantly enhances both the sensitivity and specificity of detection.
Overall, the tumor-informed approach is supported by more robust and extensive clinical validation, whereas the tumor-agnostic method requires further evidentiary support. Although prior studies have demonstrated correlations between ctDNA levels and treatment efficacy or prognosis in SCLC patients [9,11,13], reports utilizing the highly sensitive tumor-informed methodology remain limited. In this study, we performed whole exome sequencing (WES) on SCLC tissue samples to design and synthesize customized panels. This enabled personalized and dynamic monitoring of MRD in peripheral blood samples throughout the treatment course. The objective was to investigate the clinical utility of this customized plasma ctDNA-based MRD monitoring approach in SCLC patients and its significance in predicting therapeutic outcomes and the emergence of resistance.
2. Materials and Methods
2.1. Study Design and Patients
This was a prospective, observational, single-cohort study. The research flowchart is shown in Figure 1 (Created with BioGDP.com [19]). Inclusion criteria were: (1) age ≥ 18 years; (2) histopathologically confirmed unresectable SCLC; (3) a life expectancy exceeding three months; (4) availability of sufficient tumor tissue for WES; (5) ability to provide adequate peripheral blood samples for ctDNA-based MRD detection during treatment; and (6) presence of at least one measurable lesion according to Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. The primary endpoint was the correlation between ctDNA-based MRD status and radiologically assessed PFS.
2.2. Sample Collection
Baseline tumor formalin-fixed paraffin-embedded (FFPE) samples were collected (consisting of 15-20 sections, each 5 µm thick). A total of 20 mL of peripheral venous blood was collected in Streck tubes at baseline, every six weeks during treatment, and at the time of disease progression. These samples were transported to the BGI Tianjin Specimen Center within 72 hours of collection.
2.3. Efficacy Evaluation
Computed tomography (CT) and/or magnetic resonance imaging (MRI) was performed every six weeks (± seven days) during treatment. Therapeutic efficacy was evaluated according to RECIST version 1.1. PFS was defined as the time from treatment initiation to the first documentation of objective tumor progression or death from any cause, whichever occurred first. OS was defined as the time from pathological diagnosis to death from any cause. Patients who were lost to follow-up were censored at the date of their last known contact. For those who remained alive at the study cutoff date, survival data were censored on that date.
2.4. Extraction of Cell-Free DNA (cfDNA)
CfDNA, including ctDNA, was isolated from human plasma using the QIAamp Circulating Nucleic Acid Kit (QIAGEN, Hilden, Germany) according to the manufacturer’s instructions. Briefly, the plasma samples were subjected to enzymatic lysis with QIAGEN Proteinase K and Buffer ACL (supplemented with carrier RNA) at 60°C for 30 minutes to ensure the complete release of nucleic acids from proteins and vesicles. Binding conditions were adjusted by the addition of Buffer ACB, and the resulting lysate was drawn through a QIAamp Mini column using the QIAvac 24 Plus vacuum manifold. The silica membrane was sequentially washed with Buffers ACW1, ACW2, and 96 - 100% ethanol to efficiently remove residual contaminants and inhibitors. Finally, the purified nucleic acids were eluted in the Buffer AVE. The extracted DNA was either used immediately for downstream applications or stored at -20°C for long-term stability.
2.5. WES at Baseline
Fresh tumor tissue samples were FFPE, stained with hematoxylin and eosin (H&E), and subjected to pathological review to confirm a tumor content of at least 30%. Genomic DNA (gDNA) was extracted from tumor tissue using the QIAamp DNA FFPE Tissue Kit and from matched whole blood samples using the MagPure Buffy Coat DNA Midi KF Kit, followed by quantification with a Qubit 3.0 fluorometer.
For library preparation, approximately 400 ng of tumor gDNA and 200 ng of germline DNA underwent fragmentation, end repair, 3'-adenylation, and adapter ligation. The resulting libraries were pooled and hybridized to the Quanxi® pan-cancer whole exome panel. Sequencing was performed on the MGISEQ-2000 platform, achieving a mean coverage depth of 500× for tumor samples and 200× for normal controls. In addition to identifying single nucleotide variants (SNVs), insertions/deletions (indels), copy number variations (CNVs), and rearrangements, the analysis included evaluations of tumor mutational burden (TMB) and microsatellite instability (MSI). To facilitate personalized monitoring, sequencing data were processed through the Signatera™ WES pipeline to select 16 prioritized SNVs per patient. Based on these variants, 16 specific multiplex PCR primer pairs were optimized, designed, and synthesized at BGI Tech Solutions for subsequent ctDNA detection.
2.6. Personalized Tumor-Informed ctDNA Detection
At each monitoring time point, 20 mL of peripheral blood was collected in cfDNA BCT® tubes (Streck) and processed using the Huajianwei® bespoke MRD assay (BGI Genomics), a tumor-informed approach based on the Signatera™ platform as previously described [20,21]. cfDNA was extracted from a median plasma volume of 8 mL using the QIAamp Circulating Nucleic Acid Kit (Qiagen). Subsequently, 10 - 66 ng of cfDNA was used for library preparation with patient-specific primer sets. In this method, the 16 prioritized SNVs previously identified via WES were targeted. Personalized 16-plex primer pairs were employed to amplify universal cfDNA libraries, which were then sequenced on the MGISEQ-2000 platform to a median depth exceeding 110,000× per amplicon. Data analysis was performed using the Signatera™ plasma pipeline (Natera), and MRD positivity was defined by the detection of at least two patient-specific variants. ctDNA burden was quantified as mean tumor molecules per milliliter of plasma (MTM/mL). The assay demonstrates a sensitivity of >95% for detecting variants at a 0.03% variant allele frequency (VAF).
2.7. Statistic Analysis
Survival analysis was conducted using the Kaplan-Meier method, and differences between groups were compared with the log-rank test. The correlation between ctDNA levels and the sum of diameters of target lesions was analyzed using Spearman's rank correlation coefficient. All statistical tests were two-sided, and a P-value < 0.05 was considered statistically significant. Data analysis was performed using R software (version 4.1).
3. Results
3.1. Patient Characteristics
A total of 20 patients were enrolled in this study. However, personalized panels were successfully designed from WES data for only seven participants, whose clinical data are summarized in Table 1. The cohort was predominantly male, with a median age of 60 years (range: 58 to 74 years). All participants had a documented smoking history, with substantial cumulative exposure ranging from 15 to 122 pack-years. Regarding disease severity at baseline, two patients presented with limited-stage disease, while the remaining five had extensive-stage disease. The majority of the cohort was diagnosed with pure SCLC; one patient was diagnosed with combined SCLC (C-SCLC).
The treatment administered varied across different lines of therapy. Six patients received platinum-based combination chemotherapy, frequently combined with thoracic radiotherapy, programmed cell death ligand-1 (PD-L1) inhibitors, or PD-1 inhibitors. One patient was administered anti-angiogenesis monotherapy as a fifth-line treatment. Clinical outcomes exhibited variability, with PFS durations spanning from 1.0 to 19.3 months. The best overall responses comprised partial response (PR) in two patients, stable disease (SD) in three patients, and progressive disease (PD) in two patients. TMB also demonstrated considerable heterogeneity, ranging from 4.81 to 61.8 mutations per megabase. PD-L1 expression levels were predominantly low or not assessed, with documented Tumor Proportion Scores (TPS) of either 0% or less than 1%.
3.2. Clinical Relevance of Baseline WES and ctDNA Analysis
WES was conducted to delineate the baseline genomic profile of the enrolled patients. Evaluation of mutation frequency identified TP53 and RB1 as the most commonly altered genes, present in 100% and 85.7% of the cohort, respectively (Figure 2). Other frequently observed mutations included RYR2 (approximately 80%), LRP1B (approximately 70%), and ZFHX4 (approximately 60%). The gene mutation waterfall plot revealed a predominance of missense mutations among the detected genes, accompanied by frameshift, nonsense, and splice-site variants. Notably, the baseline positivity rate for ctDNA-based MRD detection was 100%, as ctDNA was successfully detected in all seven patients prior to the commencement of study treatment.
Beyond genomic characterization, we further examined the association between ctDNA levels and physical tumor burden. Spearman's rank correlation analysis indicated a significant positive linear relationship between baseline ctDNA quantification and the sum of the longest diameters of target lesions, producing a correlation coefficient of 0.821 (P = 0.034). These results, depicted in a scatter plot (Figure 3), imply that ctDNA can effectively function as a molecular proxy for overall tumor volume.
3.3. Longitudinal Assessment of ctDNA-MRD During Treatment
Longitudinal monitoring of MRD was performed for all seven patients to assess the predictive utility of ctDNA dynamics. A total of 23 blood samples were collected for analysis. Based on MRD trends observed at the second monitoring time point (the first on-treatment evaluation), patients were categorized into two distinct groups: the MRD-decrease group (n=5) and the MRD-increase group (n=2), as shown in the swimmer plot (Figure 4). Patients in the MRD-decrease group achieved either PR or SD as their best response, with a tendency toward longer PFS, extending up to 19.3 months. Although the limited cohort size yielded a P-value of 0.0665, the hazard ratio (HR) of 0.24 (95% confidence interval: 0.02 - 3.19) suggests a pronounced trend toward a reduced risk of disease progression in patients with declining ctDNA levels (Figure 5). Remarkably, one patient attained sustained MRD clearance after three cycles of sequential chemoradiotherapy; this individual remains alive with an OS currently surpassing 30 months. In contrast, the two patients demonstrating an early increase in MRD experienced rapid disease progression, with PFS durations of only 5.2 and 1.0 months, respectively. These findings underscore that early on-treatment ctDNA-MRD kinetics may constitute a crucial indicator of therapeutic response and long-term prognosis in SCLC patients. Moreover, our longitudinal data suggest that MRD elevation can act as an early warning signal, preceding radiographic disease progression by up to 135 days.
4. Discussion
This study represents an innovative application of a tumor-informed methodology for dynamic MRD monitoring in SCLC patients, offering a preliminary investigation into the relationship between ctDNA-MRD kinetics and clinical efficacy. Despite the inherent constraints of a limited sample size, our findings reveal a distinct clinical signal: patients achieving a significant reduction or clearance of MRD during treatment demonstrated a marked trend toward superior PFS. This was exemplified most strikingly by a single patient who achieved MRD clearance after only three cycles of chemotherapy and subsequently attained an OS exceeding 30 months. This case strongly suggests that MRD clearance could serve as a surrogate marker for "molecular complete response", potentially offering prognostic insights as significant as radiographic complete response. Furthermore, the positive correlation identified between ctDNA and tumor burden provides empirical support for ctDNA as a quantitative surrogate in SCLC management.
From a mechanistic perspective, the dynamic fluctuations of MRD likely reflect the differential sensitivity of specific tumor clones to cytotoxic agents. Given that SCLC is characterized by high proliferative activity and a propensity for early systemic dissemination, traditional imaging often fails to capture micro-residual disease or occult metastases. As genetic fragments released into the bloodstream via apoptosis or necrosis, ctDNA may serve as a more sensitive indicator, capable of reflecting the evolution of total tumor burden earlier and more accurately than conventional methods. The observed correlation between ctDNA levels and the sum of target lesion diameters validates this biological rationale and provides a theoretical foundation for future trials exploring whether ctDNA-MRD status could justify extending intervals between radiographic evaluations.
When compared with existing literature, our results align with several prospective cohorts in both non-small-cell lung cancer (NSCLC) and SCLC. For instance, previous research by Chaudhuri et al. noted that post-treatment ctDNA status was highly associated with recurrence risk in LS-SCLC [6]. Similarly, research by Moding et al. confirmed that long-term survival rates for patients achieving MRD clearance were significantly higher than for those who do not [22]. By replicating these findings, our study suggests that the prognostic stratification value of dynamic MRD monitoring may be a universal feature that transcends specific disease stages and is applicable across the SCLC spectrum.
We must acknowledge that the small sample size is the primary limitation of this study. Additionally, the optimal timing and thresholds for MRD monitoring remain unstandardized; the trend-based classification at the second monitoring point used in this study remains exploratory. However, despite these limitations, the high degree of data integrity and the biological consistency of our results underscore the value of this work as early exploratory evidence.
Future research should pivot toward several key directions to build upon these preliminary findings. First, the initiation of prospective, multicenter cohorts is necessary to systematically evaluate the predictive efficacy of MRD kinetics at various clinical milestones. Second, there is a clear need to explore MRD-driven adaptive therapeutic strategies, such as treatment de-escalation for those with durable MRD clearance or treatment intensification for those with persistent molecular positivity. Finally, researchers should focus on integrated modeling that combines genomic features with MRD dynamics to enhance personalized prognostic precision. It is worth noting that while the prospects are broad, ctDNA detection in SCLC still faces challenges. For example, TP53 mutations can be detected in the cfDNA of non-cancerous populations due to clonal hematopoiesis of indeterminate potential [23], limiting its use in early screening. Additionally, in heavily pre-treated patients, ctDNA dynamics may show a poor correlation with radiographic responses under certain combination therapies [23], suggesting its value may vary by treatment regimen and clinical context. Future studies are needed to further standardize detection protocols and validate clinical utility in large-scale trials across diverse therapeutic scenarios.
5. Conclusions
This investigation demonstrates that dynamic MRD monitoring via ctDNA effectively mirrors fluctuations in tumor burden and is associated with clinical outcomes in SCLC patients. As a convenient and efficient liquid biopsy approach, ctDNA analysis offers significant utility for real-time disease surveillance and prognostic stratification. These findings support the potential of ctDNA to enhance precision and personalized treatment strategies for SCLC.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: Raw data of the Spearman's rank correlation coefficient; Figure S2: Data of the PFS and ctDNA-MRD levels. Figure S3: Raw data of WES.
Author Contributions
Conceptualization, J.C.; methodology, Q.Z and D.D.; software, Q.Z., J.S. and D.D; validation, J.C.; formal analysis, M.Z.; investigation, X.X.; data curation, Y.Y., L.G, S.H. and S.L.; writing—original draft preparation, Q.Z.; writing—review and editing, D.D.; supervision, J.C.; project administration, J.C. and Q.Z.; funding acquisition, J.C and Q.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Sanming Project of Medicine in Shenzhen (SZSM202211012 and SZSM202411002), the National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital & Shenzhen Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Shenzhen (E010324012).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Cancer Hospital Chinese Academy of Medical Sciense, Shenzhen (YLQX2023-1-2; October 23, 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the supplementary material. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| SCLC | Small-cell lung cancer |
| ctDNA | circulating tumor DNA |
| PFS | progression-free survival |
| OS | overall survival |
| mTBI | molecular tumor burden index |
| LS-SCLC | limited-stage small-cell lung cancer |
| MRD | minimal residual disease |
| NGS | next-generation sequencing |
| WES | whole exome sequencing |
| RECIST | Response Evaluation Criteria in Solid Tumors |
| FFPE | formalin-fixed paraffin-embedded |
| CT | computed tomography |
| MRI | magnetic resonance imaging |
| cfDNA | cell-free DNA |
| H&E | hematoxylin and eosin |
| gDNA | genomic DNA |
| SNVs | single nucleotide variants |
| indels | insertions/deletions |
| CNVs | copy number variations |
| TMB | tumor mutational burden |
| MSI | microsatellite instability |
| MTM/mL | mean tumor molecules per milliliter |
| VAF | variant allele frequency |
| PD-(L)1 | programmed cell death (ligand) -1 |
| PR | partial response |
| SD | stable disease |
| PD | progressive disease |
| TPS | Tumor Proportion Scores |
| HR | hazard ratio |
| NSCLC | non-small-cell lung cancer |
References
- Sung, H.; Ferlay, J.; Siegel, R. L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA-Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Wood, D. E.; Kazerooni, E. A.; Aberle, D.; Berman, A.; Brown, L. M.; Eapen, G. A.; Ettinger, D. S.; Ferguson, J. S.; Hou, L.; Kadaria, D.; et al. NCCN Guidelines® Insights: Lung Cancer Screening, Version 1.2022. J. Natl. Compr. Cancer Netw. 2022, 20, 754–764. [Google Scholar] [CrossRef]
- Ganti, A. K. P.; Loo, B. W.; Bassetti, M.; Blakely, C.; Chiang, A.; D’Amico, T. A.; D’Avella, C.; Dowlati, A.; Downey, R. J.; Edelman, M. J.; et al. Small Cell Lung Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 1441–1464. [Google Scholar] [CrossRef]
- Zugazagoitia, J.; Paz-Ares, L. Extensive-Stage Small-Cell Lung Cancer: First-Line and Second-Line Treatment Options. J. Clin. Oncol. 2022, 40, 671–680. [Google Scholar] [CrossRef]
- Abbosh, C.; Birkbak, N. J.; Wilson, G. A.; Jamal-Hanjani, M.; Constantin, T.; Salari, R.; Le Quesne, J.; Moore, D. A.; Veeriah, S.; Rosenthal, R.; et al. Phylogenetic ctDNA Analysis Depicts Early-Stage Lung Cancer Evolution. Nature 2017, 545, 446–451. [Google Scholar] [CrossRef]
- Chaudhuri, A. A.; Chabon, J. J.; Lovejoy, A. F.; Newman, A. M.; Stehr, H.; Azad, T. D.; Khodadoust, M. S.; Esfahani, M. S.; Liu, C. L.; Zhou, L.; et al. Early Detection of Molecular Residual Disease in Localized Lung Cancer by Circulating Tumor DNA Profiling. Cancer Discov. 2017, 7, 1394–1403. [Google Scholar] [CrossRef]
- Newman, A. M.; Bratman, S. V.; To, J.; Wynne, J. F.; Eclov, N. C. W.; Modlin, L. A.; Liu, C. L.; Neal, J. W.; Wakelee, H. A.; Merritt, R. E.; et al. An Ultrasensitive Method for Quantitating Circulating Tumor DNA with Broad Patient Coverage. Nat. Med. 2014, 20, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Heeke, S.; Gay, C. M.; Estecio, M. R.; Tran, H.; Morris, B. B.; Zhang, B.; Tang, X.; Raso, M. G.; Rocha, P.; Lai, S.; et al. Tumor- and Circulating-Free DNA Methylation Identifies Clinically Relevant Small Cell Lung Cancer Subtypes. Cancer Cell 2024, 42, 225–237.e5. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Liu, Y.; Yuan, M.; Dong, G.; Zhang, H.; Zhang, T.; Chang, L.; Xia, X.; Li, L.; Zhu, H.; et al. The Feasibility of Using Biomarkers Derived from Circulating Tumor DNA Sequencing as Predictive Classifiers in Patients with Small-Cell Lung Cancer. Cancer Res. Treat. 2022, 54, 753–766. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Wu, Y.; Zhao, J.; Zhang, T.; Fei, K.; Zhao, X.; Deng, L.; Zhang, Z.; Jiang, Y.; Wang, J.; et al. Circulating Tumor DNA Refines Consolidation Immunotherapy for Limited-Stage Small Cell Lung Cancer Patients. Signal Transduct. Target. Ther. 2025, 10, 347. [Google Scholar] [CrossRef]
- Sivapalan, L.; Iams, W. T.; Belcaid, Z.; Scott, S. C.; Niknafs, N.; Balan, A.; White, J. R.; Kopparapu, P.; Cann, C.; Landon, B. V.; et al. Dynamics of Sequence and Structural Cell-Free DNA Landscapes in Small-Cell Lung Cancer. Clin. Cancer Res. 2023, 29, 2310–2323. [Google Scholar] [CrossRef]
- Herbreteau, G.; Langlais, A.; Greillier, L.; Audigier-Valette, C.; Uwer, L.; Hureaux, J.; Moro-Sibilot, D.; Guisier, F.; Carmier, D.; Madelaine, J.; et al. Circulating Tumor DNA as a Prognostic Determinant in Small Cell Lung Cancer Patients Receiving Atezolizumab. J. Clin. Med. 2020, 9, 3861. [Google Scholar] [CrossRef]
- Li, J.; Wang, L.; Dong, Z.; Song, Q.; Wang, Z. A Meta-Analysis of Circulating Tumor DNA as a Survival Indicator in Small Cell Lung Cancer Patients. Clin. Exp. Med. 2023, 23, 3935–3945. [Google Scholar] [CrossRef]
- Pan, Y.; Zhang, J. T.; Gao, X.; Chen, Z. Y.; Yan, B.; Tan, P. X.; Yang, X. R.; Gao, W.; Gong, Y.; Tian, Z.; et al. Dynamic Circulating Tumor DNA during Chemoradiotherapy Predicts Clinical Outcomes for Locally Advanced Non-Small Cell Lung Cancer Patients. Cancer Cell 2023, 41, 1763–1773.e4. [Google Scholar] [CrossRef]
- Dong, S.; Wang, Z.; Zhang, J. T.; Yan, B.; Zhang, C.; Gao, X.; Sun, H.; Li, Y. S.; Yan, H. H.; Tu, H. Y.; et al. Circulating Tumor DNA-Guided De-Escalation Targeted Therapy for Advanced Non-Small Cell Lung Cancer: A Nonrandomized Controlled Trial. JAMA Oncol. 2024, 10, 932–940. [Google Scholar] [CrossRef] [PubMed]
- Dong, Q.; Chen, C.; Hu, Y.; Zhang, W.; Yang, X.; Qi, Y.; Zhu, C.; Chen, X.; Shen, X.; Ji, W.; et al. Clinical Application of Molecular Residual Disease Detection by Circulation Tumor DNA in Solid Cancers and a Comparison of Technologies: Review Article. Cancer Biol. Ther. 2023, 24, 2274123. [Google Scholar] [CrossRef]
- Martínez-Castedo, B.; Camblor, D. G.; Martín-Arana, J.; Carbonell-Asins, J. A.; García-Micó, B.; Gambardella, V.; Huerta, M.; Roselló, S.; Roda, D.; Gimeno-Valiente, F.; et al. Minimal Residual Disease in Colorectal Cancer. Tumor-Informed versus Tumor-Agnostic Approaches: Unraveling the Optimal Strategy. Ann. Oncol. 2025, 36, 263–276. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Shields, M. D.; Chauhan, P. S.; Ramirez, R. J.; Harris, P. K.; Reimers, M. A.; Zevallos, J. P.; Davis, A. A.; Pellini, B.; Chaudhuri, A. A. Commercial ctDNA Assays for Minimal Residual Disease Detection of Solid Tumors. Mol. Diagn. Ther. 2021, 25, 757–774. [Google Scholar] [CrossRef]
- Jiang, S; Li, H; Zhang, L; Mu, W; Zhang, Y; Chen, T; Wu, J; Tang, H; Zheng, S; Liu, Y; Wu, Y; Luo, X; Xie, Y; Ren, J. Generic Diagramming Platform (GDP): a comprehensive database of high-quality biomedical graphics. Nucleic Acids Res. 2025, 53, D1670–D1676. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Abbosh, C.; Birkbak, N. J.; Wilson, G. A.; Jamal-Hanjani, M.; Constantin, T.; Salari, R.; Le Quesne, J.; Moore, D. A.; Veeriah, S.; Rosenthal, R.; et al. Phylogenetic ctDNA Analysis Depicts Early-Stage Lung Cancer Evolution. Nature 2017, 545, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Reinert, T.; Henriksen, T. V.; Christensen, E.; Sharma, S.; Salari, R.; Sethi, H.; Knudsen, M.; Nordentoft, I.; Wu, H. T.; Tin, A. S.; et al. Analysis of Plasma Cell-Free DNA by Ultradeep Sequencing in Patients with Stages I to III Colorectal Cancer. JAMA Oncol. 2019, 5, 1124–1131. [Google Scholar] [CrossRef]
- Moding, E. J.; Liu, Y.; Nabet, B. Y.; Chabon, J. J.; Chaudhuri, A. A.; Hui, A. B.; Bonilla, R. F.; Ko, R. B.; Yoo, C. H.; Gojenola, L.; et al. Circulating Tumor DNA Dynamics Predict Benefit from Consolidation Immunotherapy in Locally Advanced Non-Small Cell Lung Cancer. Nat. Cancer 2020, 1, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Cuesta, L.; Perdomo, S.; Avogbe, P. H.; Leblay, N.; Delhomme, T. M.; Gaborieau, V.; Abedi-Ardekani, B.; Chanudet, E.; Olivier, M.; Zaridze, D.; et al. Identification of Circulating Tumor DNA for the Early Detection of Small-Cell Lung Cancer. EBioMedicine 2016, 10, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Narayan, A.; Xu, Y.; Wolfe, J.; Vu, D.; Trinh, T.; Kantak, C.; Ivy, S. P.; Eder, J. P.; Deng, Y.; et al. Circulating Tumor DNA Dynamics Fail to Predict Efficacy of Poly(ADP-ribose) Polymerase/VEGFR Inhibition in Patients with Heavily Pretreated Advanced Solid Tumors. JCO Precis. Oncol. 2024, 8, e2300289. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The flowchart of this study. Whole exome sequencing from 20 participants was conducted on baseline tumor specimens. Ultimately, personalized panels were successfully customized for seven patients. Serial peripheral blood samples from these patients were collected at baseline, every six weeks, and upon disease progression. Detection of ctDNA-based MRD was performed via a tumor-informed assay with ultra-deep sequencing. The trends in these measurements were then analyzed in relation to clinical efficacy and outcomes. SCLC, small-cell lung cancer; cfDNA, cell-free DNA; FFPE, formalin-fixed paraffin-embedded; WES, whole exome sequencing. MRD, minimal residual disease.
Figure 1.
The flowchart of this study. Whole exome sequencing from 20 participants was conducted on baseline tumor specimens. Ultimately, personalized panels were successfully customized for seven patients. Serial peripheral blood samples from these patients were collected at baseline, every six weeks, and upon disease progression. Detection of ctDNA-based MRD was performed via a tumor-informed assay with ultra-deep sequencing. The trends in these measurements were then analyzed in relation to clinical efficacy and outcomes. SCLC, small-cell lung cancer; cfDNA, cell-free DNA; FFPE, formalin-fixed paraffin-embedded; WES, whole exome sequencing. MRD, minimal residual disease.

Figure 2.
Genomic profile of the enrolled patients by WES (n=7). TP53 and RB1 were the most commonly altered genes, present in 100% and 85.7% of the cohort, respectively. Other frequently observed mutations included RYR2, LRP1B, and ZFHX4. WES, whole exome sequencing.
Figure 2.
Genomic profile of the enrolled patients by WES (n=7). TP53 and RB1 were the most commonly altered genes, present in 100% and 85.7% of the cohort, respectively. Other frequently observed mutations included RYR2, LRP1B, and ZFHX4. WES, whole exome sequencing.

Figure 3.
Spearman's rank correlation between baseline ctDNA levels and the longest diameters of target lesions.
Figure 3.
Spearman's rank correlation between baseline ctDNA levels and the longest diameters of target lesions.

Figure 4.
Swimmer plot of the participants. MRD, minimal residual disease.

Figure 5.
Kaplan–Meier survival curves of the MRD increase and decrease cohorts. Patients in the MRD-decrease exhibited a tendency toward longer PFS. MRD, minimal residual disease; PFS, progression-free survival.
Figure 5.
Kaplan–Meier survival curves of the MRD increase and decrease cohorts. Patients in the MRD-decrease exhibited a tendency toward longer PFS. MRD, minimal residual disease; PFS, progression-free survival.


Table 1.
Patient characteristics.
| Patient | Age | Sex | Smoking, pack-years | Pathological diagnosis | Tumor stage | Treatment | Lines | PFS (months) | Tumor response | TMB (Muts/Mb) |
PD-L1 (TPS) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| LTJ | 58 | Male | 80 | SCLC | LS | platinum-etoposide with thoracic radiotherapy | 1st | 10.0 | SD | 7.97 | NA |
| MCJ | 60 | Male | 40 | SCLC | ES | platinum-etoposide with PD-L1 inhibitor | 1st | 5.8 | SD | 5.19 | 0% |
| ZDL | 59 | Male | 40 | SCLC | ES | platinum-etoposide with thoracic radiotherapy | 2nd | 8.3 | PR | 5.01 | NA |
| HSP | 60 | Male | 122 | SCLC | ES | platinum-etoposide with PD-1 inhibitor | 3rd | 5.2 | SD | 61.8 | NA |
| YLQ | 61 | Male | 60 | SCLC | ES | anlotinib | 5th | 3.6 | PD | 4.81 | <1% |
| HCJ | 60 | Male | 15 | C-SCLC | ES | platinum-etoposide | 3rd | 1.0 | PD | 8.25 | <1% |
| SZ | 74 | Male | 30 | SCLC | LS | platinum-etoposide with thoracic radiotherapy | 1st | 19.3 | PR | 11.17 | NA |
Abbreviations: SCLC, small-cell lung cancer; C-SCLC, combined small cell lung cancer; LS, limited stage; ES, extensive stage; PFS, progression-free survival; SD, stable disease; PD, progressive disease; PR, partial response. TMB, tumor mutational burden; PD- (L) 1, programmed cell death (ligand) -1; TPS, Tumor Proportion Scores; NR, not reached. NA, not available.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



