Submitted:
26 February 2026
Posted:
28 February 2026
You are already at the latest version
Abstract
Background:
Symptomatic supraventricular tachycardia (SVT) in childhood may adversely affect physical, emotional, social, and school functioning during critical developmental periods. Although catheter ablation is an established and effective treatment for pediatric SVT, outcome evaluations have largely focused on rhythm control, with limited attention to neurobehavioral functioning.
Objectives:
To evaluate changes in health-related quality of life (HRQoL) following catheter ablation in children with symptomatic SVT and to characterize post-ablation attention–behavioral outcomes, with particular emphasis on age- and sex-related patterns.
Methods:
This retrospective–prospective observational cohort study included 59 children and adolescents (aged 4–17 years) who underwent successful catheter ablation for symptomatic SVT between January 2022 and December 2025. Pre-ablation HRQoL data were obtained retrospectively, while post-ablation HRQoL, structured psychiatric interviews, and attention–behavioral assessments were conducted approximately six months after ablation. HRQoL was assessed using the Pediatric Quality of Life Inventory (PedsQL™ 4.0). Psychiatric diagnoses were established using the Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version (K-SADS-PL), and attention–behavioral symptoms were evaluated using the DSM-IV Based Disruptive Behavior Disorders Screening and Assessment Scale (DBDS).
Results:
Significant improvements were observed across all HRQoL domains following catheter ablation (physical, emotional, social, and school functioning; all p < 0.001). In contrast, attention–behavioral outcomes demonstrated greater heterogeneity. Boys exhibited higher post-ablation inattention scores than girls, and increasing age was associated with higher inattention and conduct-related problem scores. Although a subset of participants exceeded predefined DBDS cutoff values, mean attention–behavioral scores were generally within non-clinical ranges. Approximately 30% of participants met criteria for at least one psychiatric diagnosis at follow-up, most commonly anxiety disorders.
Conclusions:
Catheter ablation in children with symptomatic SVT is associated with marked improvements in health-related quality of life but does not uniformly normalize attention and behavioral functioning. These findings highlight the importance of incorporating brief neurobehavioral screening into routine post-ablation follow-up and support a more comprehensive, patient-centered approach to pediatric arrhythmia care.
Keywords:
pediatric supraventricular tachycardia
; catheter ablation
; health-related quality of life
; attention and behavioral outcomes
; pediatric arrhythmia
; neurobehavioral functioning
; child and adolescent psychiatry
1. Introduction
Pediatric cardiac arrhythmias, although less prevalent than those observed in adults, may exert a substantial impact on daily functioning during critical periods of physical, cognitive, and psychosocial development. Children affected by symptomatic arrhythmias frequently experience recurrent palpitations, exercise intolerance, anxiety, and school-related difficulties, all of which may contribute to impaired psychosocial well-being and reduced quality of life for both patients and their families [1,2,3]. Among these conditions, supraventricular tachycardia (SVT) represents the most common symptomatic arrhythmia in childhood and has been consistently associated with diminished health-related quality of life (HRQoL) in pediatric populations [2,3].
Catheter ablation is widely accepted as the standard therapeutic approach for children with recurrent or symptomatic arrhythmias. Advances in catheter technology and three-dimensional electroanatomic mapping systems have resulted in high procedural success rates and favorable safety profiles, even in younger pediatric cohorts [4,5,6,7]. Consequently, catheter ablation has become an integral component of contemporary pediatric arrhythmia management, with multiple studies demonstrating significant post-procedural improvements in symptom burden and HRQoL [8,9].
Despite these well-established benefits, outcome assessments following catheter ablation have largely focused on rhythm control and physical functioning. Comparatively little attention has been directed toward cognitive and behavioral domains, which play a central role in academic performance, social adaptation, and long-term developmental outcomes. Children exposed to chronic cardiac symptoms may be particularly vulnerable to attention and behavioral difficulties due to anxiety, sleep disturbances, reduced physical activity, academic stress, and prolonged symptom exposure prior to definitive treatment [10,11,12].
In the contemporary ablation era, multicenter registries have confirmed persistently high success rates and declining complication rates, particularly with the widespread adoption of three-dimensional electroanatomic mapping systems and fluoroscopy-sparing strategies [14,15,16,17]. However, data regarding neurobehavioral outcomes following catheter ablation in pediatric populations remain limited.
Therefore, the present study aimed to evaluate changes in HRQoL before and after catheter ablation in children with symptomatic SVT and to characterize post-ablation attention–behavioral functioning, with particular attention to age- and sex-related patterns. By integrating cardiologic and psychiatric outcome measures, this study seeks to contribute to a more comprehensive understanding of recovery trajectories following pediatric catheter ablation.
2. Materials and Methods
2.1. Study Design, Setting, and Reporting Standard
This study was designed as a retrospective–prospective observational cohort study and was conducted at the Pediatric Cardiology Clinic of Inönü University. Pediatric patients who underwent catheter ablation for symptomatic supraventricular tachycardia (SVT) between January 2022 and December 2025 were retrospectively identified from institutional ablation records.
The study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cohort studies. Patient selection, exclusions, and final inclusion are illustrated using a STROBE-compliant flow diagram (Figure 1).
2.2. Ethical Approval
The study protocol was approved by the Malatya Turgut Özal University Clinical Research Ethics Committee (approval number: 2025/394). Institutional permission was obtained from İnönü University Faculty of Medicine Hospital. Written informed consent was obtained from parents or legal guardians, and assent was obtained from children when developmentally appropriate. All study procedures were conducted in accordance with the principles of the Declaration of Helsinki.
2.3. Study Population and Eligibility Criteria
Eligible participants were children and adolescents aged 4–17 years who underwent catheter ablation for symptomatic SVT during the study period.
2.3.1. Inclusion Criteria
Participants were included if they met all of the following criteria:
(i) age between 4 and 17 years;
(ii) diagnosis of symptomatic SVT;
(iii) successful catheter ablation performed between 2022 and 2025; and
(iv) availability for post-ablation psychiatric evaluation and health-related quality of life (HRQoL) assessment.
2.3.2. Exclusion Criteria
Participants were excluded if they had:
(i) structural or congenital heart disease;
(ii) history of cardiac surgery;
(iii) known neurological or neurodevelopmental disorders;
(iv) known genetic syndromes;
(v) incomplete psychiatric assessment data; or
(vi) refusal to participate.
Patients with asymptomatic pre-excitation (e.g., incidentally detected Wolff–Parkinson–White pattern without documented tachyarrhythmia or clinical symptoms) were not included, as the study focused exclusively on symptomatic SVT with a clear clinical indication for catheter ablation.
2.4. Catheter Ablation and Definition of Procedural Success
All catheter ablation procedures were performed according to contemporary pediatric electrophysiology practice. During the study period, three-dimensional electroanatomic mapping systems were routinely used to guide ablation and to minimize radiation exposure, in line with current recommendations [18,19].
Procedural success was defined as complete elimination of the arrhythmogenic substrate with no acute post-procedural recurrence of tachyarrhythmia. To reduce confounding related to persistent arrhythmia or early recurrence, analyses were restricted to patients with acute procedural success.
Eligible patients were identified from institutional ablation logs and contacted consecutively for follow-up evaluation in chronological order of the index ablation procedure.
2.5. Timing of Outcome Assessments
Baseline (pre-ablation) HRQoL data referred to the month preceding catheter ablation and were obtained retrospectively from routine pre-procedural medical records when available. When documentation was unavailable, standardized caregiver recall referring specifically to the same pre-ablation time window was obtained during follow-up.
Post-ablation HRQoL assessment, structured psychiatric interview, and attention–behavioral symptom assessment were conducted during a single follow-up visit approximately six months after catheter ablation. Psychiatric and behavioral assessments were obtained only at this post-ablation time point; no pre-ablation psychiatric or behavioral assessments were available in routine clinical care records. The study timeline is illustrated in Figure 2.
2.6. Health-Related Quality of Life Assessment
HRQoL was assessed using the Pediatric Quality of Life Inventory (PedsQL™ 4.0). The parent-proxy report form was administered for children aged 4–7 years, while the child self-report form was used for participants aged 8–17 years, in accordance with standard instrument guidelines.
Items were reverse-scored and linearly transformed to a 0–100 scale following the developer’s scoring protocol, with higher scores indicating better HRQoL. Subscale scores (Physical, Emotional, Social, and School Functioning) and total HRQoL scores were calculated as the mean of completed items, provided that at least 50% of items within a subscale were completed. No imputation procedures were applied for missing data.
2.7. Psychiatric Assessment and Diagnostic Interview
Psychiatric evaluation was conducted approximately six months after catheter ablation by a board-certified child and adolescent psychiatrist. Psychiatric diagnoses were established according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), using the Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version (K-SADS-PL).
The interview was administered in a semi-structured format and included both parent and child components when developmentally appropriate. All interviews were conducted by the same clinician using a standardized assessment protocol. Due to the observational nature of the study, blinding to cardiology-related clinical information was not feasible. Previous psychiatric history and current psychotropic medication use were documented through caregiver report and medical record review.
2.8. Attention–Behavioral Symptom Assessment
Attention and behavioral functioning were assessed using the DSM-IV Based Disruptive Behavior Disorders Screening and Assessment Scale (DBDS), a standardized parent-report instrument evaluating symptoms of attention-deficit/hyperactivity disorder (ADHD), oppositional defiant disorder (ODD), and conduct disorder (CD).
The DBDS yields four subscale scores: inattention, hyperactivity, oppositional defiant behaviors, and conduct-related problems, with higher scores indicating greater symptom severity. The DBDS was administered only at the post-ablation follow-up visit; no pre-ablation DBDS assessments were available.
The Turkish version of the DBDS has demonstrated satisfactory validity and reliability, with internal consistency coefficients (Cronbach’s α) exceeding 0.70 across all subscales. For descriptive purposes, predefined cutoff values were applied (inattention ≥ 10, hyperactivity ≥ 10, oppositional defiant behaviors ≥ 6, conduct-related problems ≥ 6). DBDS scores were interpreted as dimensional symptom indicators and were not used to establish psychiatric diagnoses, which were determined exclusively through the K-SADS-PL interview.
2.9. Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics (version 26.0; IBM Corp., Armonk, NY, USA). Continuous variables were summarized as mean ± standard deviation or median (interquartile range), depending on data distribution, and categorical variables were presented as frequencies and percentages.
Sex-based comparisons of DBDS subscale scores were conducted using the Mann–Whitney U test. Associations between age and DBDS subscale scores were assessed using Spearman rank correlation coefficients. Proportions of participants exceeding DBDS clinical cutoff values were compared between sexes using chi-square tests or Fisher’s exact test, as appropriate.
Pre- and post-ablation HRQoL scores were compared using Wilcoxon signed-rank tests. To account for multiple comparisons across the four PedsQL™ subscales, Bonferroni correction was applied, with statistical significance defined as p < 0.0125. All other analyses were conducted using a two-tailed significance threshold of p < 0.05.
3. Results
3.1. Study Population and Clinical Characteristics
A total of 59 pediatric patients (34 girls and 25 boys) were included in the final analysis. The median age of the cohort was 13.0 years (interquartile range: 10.0–15.0). All participants had symptomatic supraventricular tachycardia and underwent successful catheter ablation. None of the patients had structural or congenital heart disease or a history of cardiac surgery.
Follow-up assessments were conducted approximately six months after catheter ablation. Baseline health-related quality of life data referred to the month preceding the procedure, whereas post-ablation evaluations—including HRQoL assessment, structured psychiatric interview, and attention–behavioral assessment—were obtained during a single follow-up visit. Demographic and clinical characteristics of the study population are summarized in Table 1.
3.2. Psychiatric Diagnoses at Post-Ablation Follow-Up
At post-ablation follow-up, 18 participants (30.5%) met DSM-5 criteria for at least one psychiatric diagnosis based on the K-SADS-PL interview. Anxiety disorders were the most frequent diagnosis (n = 9, 15.3%), followed by depressive disorders (n = 4, 6.8%), adjustment disorder (n = 3, 5.1%), and attention-deficit/hyperactivity disorder (n = 2, 3.4%). Some participants met criteria for more than one diagnosis. The distribution of psychiatric diagnoses is presented in Table 6.
3.3. Health-Related Quality of Life Outcomes
Significant improvements were observed across all health-related quality of life domains following catheter ablation. Median PedsQL™ scores increased significantly in physical, emotional, social, and school functioning domains (all p < 0.001). Effect sizes for HRQoL improvements were large across all subscales. No significant sex-based differences were observed in HRQoL change scores. Pre- and post-ablation HRQoL results are presented in Table 2.
3.4. Attention–Behavioral Outcomes
Mean post-ablation DBDS subscale scores were 4.31 ± 3.64 for inattention, 4.05 ± 3.98 for hyperactivity, 4.75 ± 4.32 for oppositional defiant behaviors, and 1.08 ± 2.22 for conduct-related problems. Descriptive statistics for DBDS subscale scores are shown in Table 3A.
Sex-based comparisons demonstrated significantly higher inattention scores among boys compared with girls (p = 0.008). No significant sex-based differences were observed for hyperactivity, oppositional defiant behaviors, or conduct-related problems. Sex-stratified DBDS subscale scores are presented in Table 3B.
3.5. Associations Between Age and Attention–Behavioral Symptoms
Spearman correlation analysis demonstrated a positive association between age and inattention scores (r = 0.373, p = 0.004), as well as between age and conduct-related problem scores (r = 0.301, p = 0.021). No significant associations were observed between age and hyperactivity or oppositional defiant behavior scores. Correlation analyses are summarized in Table 4.
3.6. DBDS Clinical Cutoff Exceedance
A subset of participants exceeded predefined DBDS clinical cutoff values. Cutoff exceedance rates were 13.6% for inattention, 10.2% for hyperactivity, 27.1% for oppositional defiant behaviors, and 10.2% for conduct-related problems. Overall and sex-based distributions of cutoff exceedance are presented in Table 5. No significant sex-based differences were observed across DBDS subscales (all p > 0.05).
4. Discussion
In this prospective observational study, catheter ablation was associated with significant and consistent improvements across all domains of health-related quality of life (HRQoL) in children with symptomatic supraventricular tachycardia. Improvements in physical, emotional, social, and school functioning highlight the central role of effective rhythm control in alleviating symptom burden and restoring daily functioning during critical developmental periods. Although formal diagnostic cutoff values are not defined for PedsQL™ scores, the relatively low pre-ablation HRQoL observed in this cohort suggests clinically meaningful impairment prior to definitive treatment.
These findings are consistent with contemporary pediatric studies demonstrating substantial HRQoL gains following successful catheter ablation. Recent cohorts treated in the modern ablation era—characterized by the widespread adoption of three-dimensional electroanatomic mapping systems and reduced fluoroscopy exposure—have reported sustained improvements in both physical and psychosocial domains of HRQoL [20,21,22]. By confirming these benefits in a recent cohort, the present study extends earlier observations and reinforces the role of catheter ablation as an effective intervention for improving patient-centered outcomes in pediatric supraventricular tachycardia.
In contrast to the uniform improvement observed in HRQoL, attention and behavioral outcomes demonstrated greater heterogeneity. Boys exhibited higher post-ablation inattention scores than girls, and increasing age was associated with higher levels of inattention and conduct-related problems. These findings are consistent with established epidemiological data indicating a higher prevalence of attentional difficulties among male children and adolescents, as well as age-related increases in academic and behavioral demands [23,24]. Importantly, these patterns are unlikely to represent a direct effect of catheter ablation and instead appear to reflect broader developmental, psychosocial, and contextual influences.
Although a subset of participants exceeded predefined DBDS subscale cutoff values, mean attention–behavioral scores remained well below clinical thresholds, and only a small proportion of children met DSM-5 diagnostic criteria for attention-deficit/hyperactivity disorder or other disruptive behavior disorders on structured psychiatric interview. This discrepancy suggests that most observed symptoms were subclinical in nature. Similar patterns have been reported in pediatric populations with chronic medical conditions, where subthreshold behavioral symptoms may persist despite improvement in disease-specific outcomes [25].
Nevertheless, subclinical attention and behavioral difficulties may still have functional relevance, particularly in academic performance and social adaptation. The persistence of such symptoms following successful rhythm control indicates that improvements in cardiac outcomes and HRQoL do not necessarily translate into parallel normalization of neurobehavioral functioning. Prior research in pediatric cardiology and developmental medicine has emphasized that neurobehavioral trajectories are shaped by multiple interacting factors—including illness duration, psychological stress, developmental stage, and environmental context—beyond cardiac rhythm abnormalities alone [26,27].
The strengths of this study include its prospective follow-up design, the use of validated HRQoL and psychiatric assessment instruments, and the integrated evaluation of cardiologic, psychological, and behavioral outcomes in a contemporary pediatric ablation cohort. Several limitations should be acknowledged. The single-center observational design and modest sample size limit causal inference and generalizability. The absence of a healthy control group restricts direct comparison with normative populations, and baseline attention–behavioral assessments were not available, precluding pre–post comparisons in this domain. Additionally, follow-up was limited to approximately six months after ablation, and longer-term studies are needed to assess the persistence or evolution of neurobehavioral findings. Despite these limitations, post-ablation DBDS scores were generally consistent with non-clinical ranges, supporting the robustness of the overall findings.
In summary, while catheter ablation effectively improves health-related quality of life in children with symptomatic supraventricular tachycardia, attention and behavioral outcomes appear more heterogeneous and may follow distinct recovery trajectories. Recognition of these patterns may inform more comprehensive post-ablation follow-up strategies that address both cardiologic and neurobehavioral dimensions of pediatric patient care.
4.1. Clinical Implications
From a clinical perspective, the present findings suggest that procedural success following catheter ablation should not be defined solely by rhythm control and symptom resolution. Although most children experience marked improvements in quality of life, a subset—particularly older children and boys—may continue to exhibit attention-related or behavioral vulnerabilities after successful ablation.
Incorporating brief, developmentally appropriate screening for attention, behavioral regulation, and school functioning into routine post-ablation follow-up may facilitate early identification of children who could benefit from psychological or educational support. Such an approach would complement standard cardiologic care and promote timely referral to multidisciplinary services when indicated, supporting a more holistic and patient-centered model of care in pediatric arrhythmia management.
4.2. Strengths and Limitations
This study has several notable strengths. First, it provides an integrated evaluation of cardiologic, psychiatric, and patient-reported outcomes in a contemporary pediatric cohort undergoing catheter ablation for symptomatic supraventricular tachycardia. By combining health-related quality of life (HRQoL) measures with structured psychiatric interviews and standardized attention–behavioral assessments, the study extends outcome evaluation beyond traditional rhythm- and symptom-based endpoints.
Second, the use of validated instruments—including the Pediatric Quality of Life Inventory (PedsQL™ 4.0), the Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version (K-SADS-PL), and the DSM-IV Based Disruptive Behavior Disorders Screening and Assessment Scale (DBDS)—strengthens the reliability and interpretability of the findings. All psychiatric assessments were conducted by the same board-certified child and adolescent psychiatrist using a standardized protocol, thereby minimizing inter-rater variability.
Third, the study reflects real-world clinical practice in the modern ablation era, characterized by the routine use of three-dimensional electroanatomic mapping systems and fluoroscopy-sparing strategies. This enhances the clinical relevance and generalizability of the findings to contemporary pediatric electrophysiology settings.
Several limitations should also be acknowledged. The observational design and single-center setting limit causal inference and may restrict generalizability to other populations or healthcare systems. The sample size was modest, which may have reduced statistical power to detect smaller associations, particularly in subgroup analyses.
In addition, baseline attention–behavioral assessments were not available, precluding direct pre–post comparisons in this domain. As a result, post-ablation attention and behavioral findings should be interpreted descriptively rather than as treatment-related changes. Pre-ablation HRQoL data were obtained retrospectively in some participants through caregiver recall, which may have introduced recall bias despite the use of standardized instructions and a clearly defined reference period.
The absence of a healthy control group further limits direct comparison with normative populations. Although reference data exist for both HRQoL and attention–behavioral measures, formal statistical comparisons were not performed due to differences in assessment context and informant type. Finally, follow-up was limited to approximately six months after ablation; longer-term studies are needed to determine whether observed neurobehavioral patterns persist, improve, or evolve over time.
4.3. Future Directions
Future research should aim to clarify the longitudinal trajectories of attention and behavioral functioning in children undergoing catheter ablation for supraventricular tachycardia. Prospective studies incorporating standardized pre- and post-ablation neurobehavioral assessments would allow for direct evaluation of treatment-related changes and help disentangle the effects of rhythm control from developmental and psychosocial influences. Inclusion of age-matched healthy control groups or disease-control cohorts could further contextualize observed findings relative to normative developmental patterns.
In addition, longer-term follow-up extending into adolescence and early adulthood may provide valuable insight into whether subclinical attention and behavioral symptoms persist, resolve, or evolve over time. Future studies may also benefit from integrating school-based outcomes, sleep quality measures, and caregiver stress assessments to better capture the multidimensional impact of pediatric arrhythmias and their treatment. Such work would support the development of more comprehensive, multidisciplinary follow-up models that address both cardiac and neurobehavioral aspects of recovery.
5. Conclusions
In children with symptomatic supraventricular tachycardia, catheter ablation is associated with significant and clinically meaningful improvements across all domains of health-related quality of life. These findings reinforce the effectiveness of catheter ablation not only in achieving rhythm control but also in restoring physical, emotional, social, and school functioning during critical developmental periods.
However, attention and behavioral outcomes appear more heterogeneous and do not uniformly parallel improvements in quality of life. A subset of patients—particularly older children and boys—may continue to exhibit subclinical attention-related or behavioral vulnerabilities despite successful ablation. These results highlight the importance of incorporating brief neurobehavioral screening into routine post-ablation follow-up and support a more holistic, patient-centered approach to care in pediatric arrhythmia management.
Author Contributions
Conceptualization, T.D. and Ö.E.; methodology, T.D. and Ö.E.; validation, T.D., S.A.M. and M.Ö.; formal analysis, Ö.D.; investigation, T.D.; resources, S.A.M.; data curation, Ö.D.; writing—original draft preparation, T.D.; writing—review and editing, T.D.; visualization, T.D.; supervision, Ö.E.; project administration, Ö.E. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Clinical Research Ethics Committee of Malatya Turgut Özal University (approval number: 2025/394).
Informed Consent Statement
Written informed consent was obtained from all parents or legal guardians of the participants, and assent was obtained from children when developmentally appropriate.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author. The data are not publicly available due to ethical and privacy considerations.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| ADHD | attention-deficit/hyperactivity disorder |
| CD | conduct disorder |
| DBDS | DSM-IV Based Disruptive Behavior Disorders Screening and Assessment Scale |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition |
| HRQoL | health-related quality of life |
| K-SADS-PL | Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version |
| ODD | oppositional defiant disorder |
| PedsQL™ | Pediatric Quality of Life Inventory |
| SVT | supraventricular tachycardia |
References
- Moak, J.P.; Barron, K.S.; Hougen, T.J.; et al. Supraventricular tachycardia in children: Clinical features, diagnosis, and management. Pediatr. Cardiol. 2001, 22, 303–308. [Google Scholar]
- Uzark, K.; Jones, K.; Slusher, J.; Limbers, C.A.; Burwinkle, T.M.; Varni, J.W. Quality of life in children with heart disease as perceived by children and parents. Pediatrics 2008, 121, e1060–e1067. [Google Scholar] [CrossRef]
- Lawoko, S.; Soares, J.J.F. Quality of life among parents of children with congenital heart disease, parents of children with other diseases, and parents of healthy children. Qual. Life Res. 2003, 12, 655–666. [Google Scholar] [CrossRef] [PubMed]
- Kugler, J.D.; Danford, D.A.; Houston, K.A.; Felix, G. Pediatric radiofrequency catheter ablation registry: Success, complications, and outcomes. J. Cardiovasc. Electrophysiol. 1997, 8, 136–143. [Google Scholar]
- Saul, J.P.; Kanter, R.J.; Abrams, D.; et al. PACES/HRS expert consensus statement on the use of catheter ablation in children and patients with congenital heart disease. Heart Rhythm 2016, 13, e251–e289. [Google Scholar] [CrossRef] [PubMed]
- Blaufox, A.D.; Felix, G.L.; Saul, J.P. Radiofrequency catheter ablation in infants ≤18 months old. J. Cardiovasc. Electrophysiol. 2001, 12, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Papez, A.L.; Al-Ahdab, M.; Dick, M., II. Advances in mapping technologies for pediatric catheter ablation. Pediatr. Cardiol. 2019, 40, 1235–1243. [Google Scholar]
- Pfammatter, J.P.; Paul, T. Quality of life after radiofrequency catheter ablation of supraventricular tachycardia in children. Heart 1999, 82, 58–62. [Google Scholar]
- Janousek, J.; Paul, T.; Gebauer, R.A. Long-term outcome of catheter ablation for supraventricular tachycardia in children. Europace 2004, 6, 372–378. [Google Scholar]
- Jackson, J.L.; Leslie, C.E.; Hondorp, S.N. Depressive and anxiety symptoms in children with arrhythmias. Pediatr. Cardiol. 2012, 33, 1200–1206. [Google Scholar]
- Marino, B.S.; Lipkin, P.H.; Newburger, J.W.; et al. Neurodevelopmental outcomes in children with congenital heart disease: Evaluation and management. Circulation 2012, 126, 1143–1172. [Google Scholar] [CrossRef]
- Mussatto, K.A.; Hoffmann, R.; Hoffman, G.; et al. Risk and prevalence of developmental delay in young children with congenital heart disease. Pediatrics 2014, 133, e570–e577. [Google Scholar] [CrossRef] [PubMed]
- Latal, B. Neurodevelopmental outcomes of the child with congenital heart disease. Clin. Perinatol. 2016, 43, 173–185. [Google Scholar] [CrossRef]
- Van Hare, G.F.; Javitz, H.; Carmelli, D.; et al. Prospective assessment of outcomes after pediatric catheter ablation in a multicenter registry. Heart Rhythm 2020, 17, 1485–1492. [Google Scholar]
- Backhoff, D.; Klehs, S.; Müller, M.J.; et al. Reduction of fluoroscopy exposure in pediatric catheter ablation using three-dimensional electroanatomic mapping systems. Europace 2021, 23, 948–955. [Google Scholar]
- Kaltman, J.R.; Tanel, R.E.; Vetter, V.L.; et al. Contemporary outcomes of catheter ablation for supraventricular tachycardia in children and adolescents. J. Am. Heart Assoc. 2020, 9, e017671. [Google Scholar]
- Papez, A.L.; Dick, M., II; Triedman, J.K. Fluoroless catheter ablation in pediatric electrophysiology: Current practice and outcomes. Heart Rhythm 2021, 18, 1120–1127. [Google Scholar]
- Walsh, E.P. Interventional electrophysiology in patients with congenital heart disease. Circulation 2019, 139, 1152–1164. [Google Scholar] [CrossRef] [PubMed]
- Triedman, J.K.; Bergau, D.M.; Saul, J.P. Radiation exposure in pediatric electrophysiology: Strategies for minimization. Heart Rhythm 2020, 17, 991–997. [Google Scholar]
- Kaltman, J.R.; Tanel, R.E.; Vetter, V.L.; et al. Contemporary outcomes of catheter ablation for supraventricular tachycardia in children and adolescents: A multicenter experience. Heart Rhythm 2020, 17, 1485–1492. [Google Scholar]
- Van Hare, G.F.; Javitz, H.; Carmelli, D.; et al. Prospective assessment after pediatric catheter ablation: Health-related quality of life and functional outcomes in the modern era. J. Am. Heart Assoc. 2021, 10, e018957. [Google Scholar]
- Backhoff, D.; Klehs, S.; Müller, M.J.; et al. Health-related quality of life after radiofrequency catheter ablation in children and adolescents with supraventricular tachycardia. Europace 2022, 24, 790–797. [Google Scholar]
- Willcutt, E.G.; Doyle, A.E.; Nigg, J.T.; Faraone, S.V.; Pennington, B.F. Validity of the executive function theory of attention-deficit/hyperactivity disorder: A meta-analytic review. Biol. Psychiatry 2021, 89, 934–944. [Google Scholar] [CrossRef] [PubMed]
- Polanczyk, G.V.; Salum, G.A.; Sugaya, L.S.; Caye, A.; Rohde, L.A. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child Psychol. Psychiatry 2022, 63, 415–431. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M. Psychosocial adjustment of children with chronic physical illness: A meta-analysis. J. Pediatr. Psychol. 2020, 45, 749–762. [Google Scholar]
- Marino, B.S.; Shera, D.; Wernovsky, G.; et al. The development of executive function in children with heart disease: Neuropsychological and psychosocial considerations. Cardiol. Young 2021, 31, 377–385. [Google Scholar]
- Cassidy, A.R.; Ilardi, D.; Bowen, S.R.; et al. Neurodevelopmental and psychosocial outcomes in pediatric heart disease: Implications for long-term follow-up. Curr. Opin. Cardiol. 2023, 38, 78–84. [Google Scholar]
Figure 1.
STROBE-compliant flow diagram illustrating patient selection, exclusions, and final inclusion. The flow diagram summarizes patient selection, exclusions, and final inclusion according to STROBE guidelines.
Figure 1.
STROBE-compliant flow diagram illustrating patient selection, exclusions, and final inclusion. The flow diagram summarizes patient selection, exclusions, and final inclusion according to STROBE guidelines.
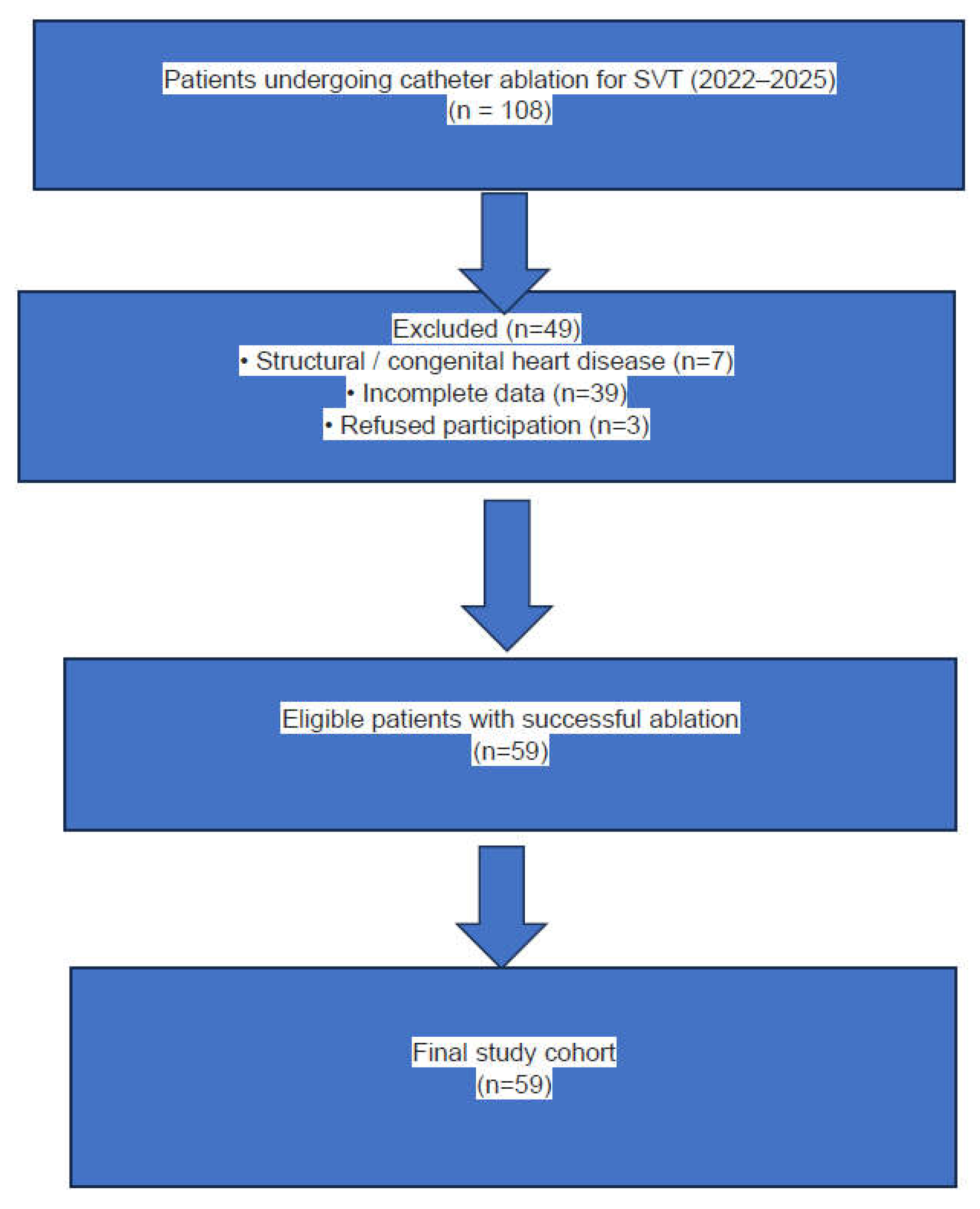
Figure 2.
Timeline of catheter ablation and outcome assessments. Baseline HRQoL data were obtained retrospectively, whereas psychiatric and behavioral assessments were conducted prospectively during a single follow-up visit approximately six months after catheter ablation.
Figure 2.
Timeline of catheter ablation and outcome assessments. Baseline HRQoL data were obtained retrospectively, whereas psychiatric and behavioral assessments were conducted prospectively during a single follow-up visit approximately six months after catheter ablation.
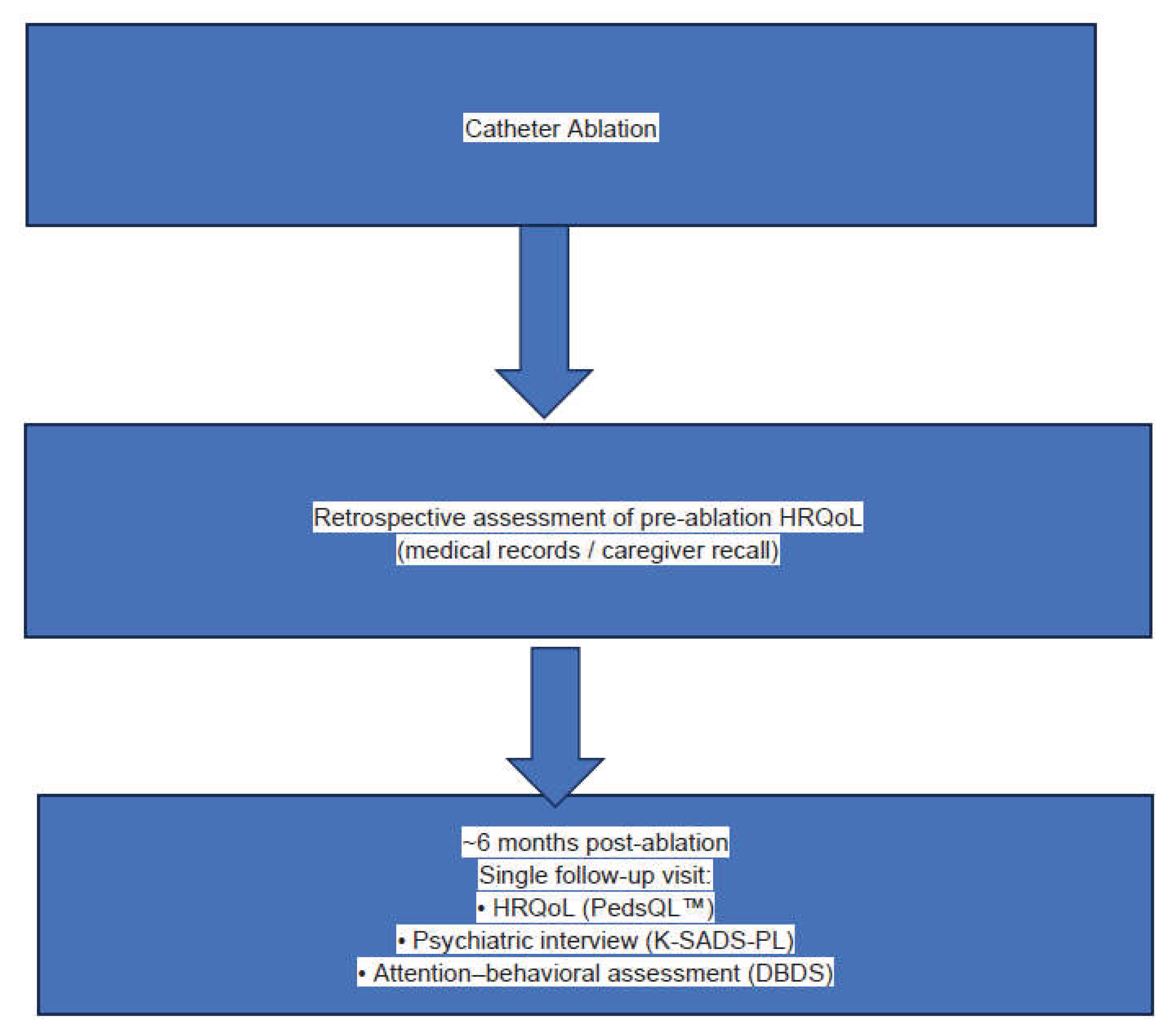

Table 1.
Demographic and Clinical Characteristics of the Study Sample (n = 59).
| Variable | Value |
|---|---|
| Age, median (IQR), years | 13.0 (10.0–15.0) |
| Sex, n (%) | |
| Girls | 34 (57.6) |
| Boys | 25 (42.4) |
| Diagnosis | Supraventricular tachycardia |
| Structural/congenital heart disease | None |
| History of cardiac surgery | None |
| Successful catheter ablation | 59 (100%) |
| Time from ablation to follow-up, months | ~6 |
Values are presented as median (interquartile range, IQR) or number (percentage). Table 1 is descriptive in nature; no statistical comparisons were performed.
Table 2.
Changes in Health-Related Quality of Life (PedsQL™) Before and After Catheter Ablation.
| PedsQL™ Domain | Pre-ablation Median (IQR) | Post-ablation Median (IQR) | Wilcoxon Z | p-value | Effect size (r) |
| Physical functioning | 47.5 (32.5–62.5) | 65.0 (56.3–72.5) | −6.612 | <0.001 | 0.861 |
| Emotional functioning | 32.5 (25.0–45.0) | 42.5 (35.0–47.5) | −6.461 | <0.001 | 0.841 |
| Social functioning | 45.0 (40.0–50.0) | 47.5 (43.8–50.0) | −6.589 | <0.001 | 0.858 |
| School functioning | 32.5 (22.5–41.3) | 40.0(32.5-45.0) | −6.027 | <0.001 | 0.785 |
| PedsQL™ Domain | Pre-ablation Median (IQR) | Post-ablation Median (IQR) | Wilcoxon Z | p-value | Effect size (r) |
| Physical functioning | 47.5 (32.5–62.5) | 65.0 (56.3–72.5) | −6.612 | <0.001 | 0.861 |
| Emotional functioning | 32.5 (25.0–45.0) | 42.5 (35.0–47.5) | −6.461 | <0.001 | 0.841 |
| Social functioning | 45.0 (40.0–50.0) | 47.5 (43.8–50.0) | −6.589 | <0.001 | 0.858 |
| School functioning | 32.5 (22.5–41.3) | 40.0 (32.5–45.0) | −6.027 | <0.001 | 0.785 |
Values are presented as median (interquartile range, IQR). Comparisons were performed using the Wilcoxon signed-rank test. Effect size r was calculated as |Z| / √N.
Table 3.
Attention–Behavioral Outcomes Assessed by DBDS.
| A. Post-Ablation DBDS Subscale Scores. | |||||
| DBDS Subscale | Mean (SD) | Median (IQR) | |||
| Inattention | 4.31 (3.64) | 3.00 (2.00–6.00) | |||
| Hyperactivity | 4.05 (3.98) | 3.00 (1.00–5.00) | |||
| Oppositional defiant behaviors | 4.75 (4.32) | 4.00 (2.00–6.50) | |||
| Conduct-related problems | 1.08 (2.22) | 0.00 (0.00–1.00) | |||
| B. Sex-Based Comparisons of DBDS Subscale Scores. | |||||
| Subscale | Girls Mean (SD) | Boys Mean (SD) | p-value | ||
| Inattention | 3.59 (3.64) | 5.28 (3.46) | 0.008 | ||
| Hyperactivity | 3.68 (3.76) | 4.56 (4.29) | 0.468 | ||
| Oppositional defiant behaviors | 4.68 (3.94) | 4.84 (4.86) | 0.556 | ||
| Conduct-related problems | 0.85 (1.84) | 1.40 (2.65) | 0.314 | ||
Sex-based comparisons were performed using the Mann–Whitney U test. Statistically significant p-values are shown in bold.
Table 4.
Correlation Between Age and Attention–Behavioral Outcomes (DBDS).
| DBDS Subscale | Spearman’s r | p-value |
|---|---|---|
| Inattention | 0.373 | 0.004 |
| Hyperactivity | 0.015 | 0.911 |
| Oppositional defiant behaviors | 0.159 | 0.230 |
| Conduct-related problems | 0.301 | 0.021 |
Spearman rank correlation coefficients were used. Statistically significant correlations are shown in bold.
Table 5.
Proportion of Participants Exceeding DBDS Clinical Cutoff Values.
| A. Overall Distribution. | ||||||
| DBDS Subscale | Clinical Cutoff | n (%) | ||||
| Inattention | ≥10 | 8 (13.6%) | ||||
| Hyperactivity | ≥10 | 6 (10.2%) | ||||
| Oppositional defiant behaviors | ≥6 | 16 (27.1%) | ||||
| Conduct-related problems | ≥6 | 6 (10.2%) | ||||
| B. Sex-Based Distribution of Cutoff Exceedance. | ||||||
| Subscale | Sex | Below Cutoff n (%) | Above Cutoff n (%) | p-value | ||
| Inattention ≥10 | Girls | 30 (88.2) | 4 (11.8) | 0.932 | ||
| Boys | 21 (84.0) | 4 (16.0) | ||||
| Hyperactivity ≥10 | Girls | 32 (94.1) | 2 (5.9) | 0.404 | ||
| Boys | 21 (84.0) | 4 (16.0) | ||||
| Oppositional defiant ≥6 | Girls | 25 (73.5) | 9 (26.5) | 1.000 | ||
| Boys | 18 (72.0) | 7 (28.0) | ||||
| Conduct-related ≥6 | Girls | 31 (91.2) | 3 (8.8) | 1.000 | ||
| Boys | 22 (88.0) | 3 (12.0) | ||||
Chi-square or Fisher’s exact test was used as appropriate. No significant sex-based differences were observed.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



