Submitted:
26 February 2026
Posted:
02 March 2026
You are already at the latest version
Abstract
Background/Objectives: Abnormalities in the partial pressure of carbon dioxide (PCO₂) can occur during respiratory support and may contribute to adverse neonatal outcomes. This study aimed to assess the incidence of early hypocapnia and hypercapnia in mechanically ventilated preterm infants and their major associated outcomes.
Methods: A single-center retrospective cohort study (2017–2024) was conducted in preterm infants < 32 weeks’ gestation who required >24 hours of invasive ventilation within the first 3 days of life. Perinatal-neonatal data were retrieved from the medical database. Admission blood gas values (arterial and capillary-venous) and the maximum and minimum PCO₂ in the first 72 hours were evaluated. Normocapnia was defined as PCO₂ 35–45 mmHg, hypocapnia 45 mmHg. Primary outcomes were the incidence of PCO₂ abnormalities; secondary outcomes included death or severe brain injury (SBI), SBI alone, and bronchopulmonary dysplasia (BPD) among survivors. Logistic regression identified independent predictors of the secondary outcomes.
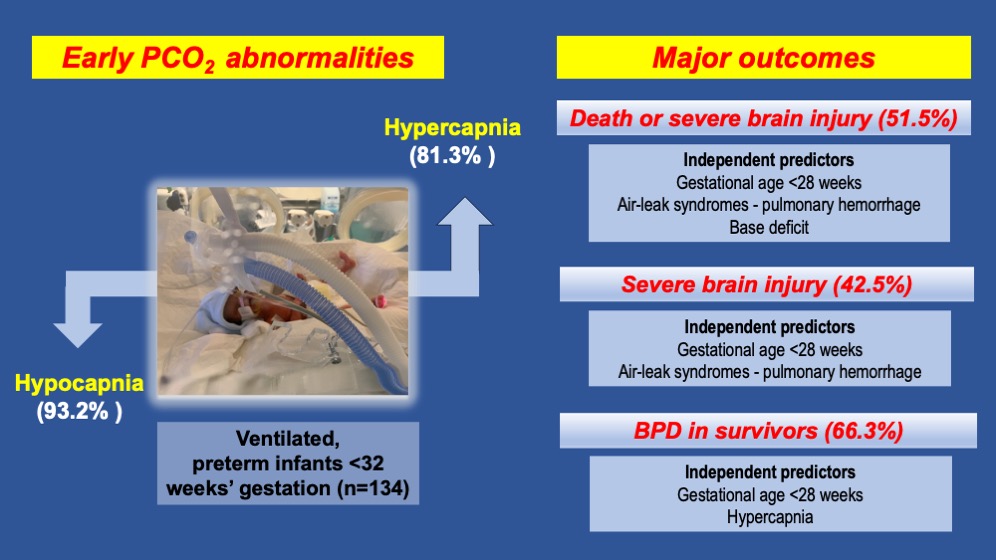
Results: Among the 134 infants evaluated, most experienced both hypercapnia and hypocapnia. Hypercapnia occurred in 81.3% of infants, and hypocapnia in 93.2%. Death or SBI was observed in 51.5%, and SBI alone in 42.5%. Gestational age < 28 weeks, air-leak syndromes, and pulmonary hemorrhage were independent predictors of death or SBI. Among survivors, hypercapnia and gestational age < 28 weeks independently predicted BPD. Infants with adverse outcomes had higher maximum PCO₂ values and greater PCO₂ variability, although these were not independent predictors of SBI or death.
Conclusions: PCO₂ instability is highly prevalent in ventilated preterm infants necessitating personalized ventilation management. Extreme prematurity remains the strongest risk factor for adverse outcomes, while hypercapnia independently predicts BPD.
Keywords:
carbon dioxide
; hypercapnia
; hypocapnia
; mechanical ventilation
1. Introduction
Over the past decades, survival rates for preterm infants have improved markedly [1]. Additionally, modern practice emphasizes non-invasive respiratory support to reduce complications associated with mechanical ventilation. Nevertheless, many preterm infants with respiratory distress syndrome still require invasive ventilation [1,2,3]. In this context, maintaining a normal partial pressure of carbon dioxide (PCO₂) in the blood is essential for preserving acid–base balance, yet optimal PCO₂ targets remain unclear [4].
Hypocapnia and hypercapnia are common in the neonatal intensive care unit (NICU) [5], and often reflect underlying illness or aspects of respiratory management, such as inappropriate iatrogenic hyperventilation [6] or intentional permissive hypercapnia [7].
Accumulating evidence, however, suggests that avoiding both hypocapnia and hypercapnia is crucial, as extreme deviations and wide fluctuations in PCO₂ levels are well recognized risk factors for serious complications—particularly neurological injuries including intraventricular hemorrhage (IVH) and periventricular leukomalacia (PVL) [8,9,10], as well as are potential contributors to bronchopulmonary dysplasia (BPD) [11]. Notably, permissive hypercapnia, aimed at minimizing ventilator-induced lung injury, has been suggested as a promising neonatal ventilation strategy [7]. However, recent literature shows no significant differences in BPD or death with permissive hypercapnia, while a potential association with an increased risk of necrotizing enterocolitis (NEC) remains a concern [12,13].
Τhe objective of the present cohort study in ventilated preterm infants was twofold: (a) to determine the incidence and patterns of PCO₂ abnormalities (hypocapnia, hypercapnia, and variability) during the first 72 hours of life, and (b) to evaluate the associations between these PCO₂ deviations and major neonatal outcomes, including survival, severe brain injury (SBI) and BPD. By investigating early PCO₂ disturbances and their associations with key neonatal outcomes, clinically relevant insights may be gained that support optimal neonatal medical care and promote a personalized medicine approach, enabling ventilation strategies to be individually tailored to the specific condition and medical needs of each preterm infant.
2. Materials and Methods
2.1. Patients and Data Collection
We conducted a single-center retrospective cohort study (2017–2024) of preterm infants (<32 weeks’ gestational age [GA]) who required invasive ventilation for >24 hours within the first 3 days of life. Perinatal and neonatal data were obtained from our center’s medical database. This allowed for the evaluation of blood gas values (pH, PCO₂, base deficit) at NICU admission, as well as the maximum and minimum PCO₂ values during the first three days. The difference between these two values was calculated as an indicator of fluctuation. As in other studies [13,14], arterial and capillary-venous samples were not distinguished because many infants lacked arterial access. Exclusion criteria included major congenital anomalies, advanced resuscitation at birth, death within 24 hours, and insufficient clinical data.
2.2. Outcomes and Definitions
Primarily, we aimed to evaluate the incidence of normocapnia, hypocapnia, and hypercapnia. Secondarily, we aimed to identify any associations between these PCO₂ abnormalities and important neonatal outcomes, including the combined outcome of death prior to NICU discharge or SBI (defined as IVH grades III–IV or cystic PVL), SBI alone, and BPD among survivors with or without SBI.
Normocapnia was defined as a PCO₂ of 35–45 mmHg, hypocapnia as a PCO₂ <35 mmHg, and hypercapnia as a PCO₂ >45 mmHg, in accordance with thresholds commonly used in neonatal research [4]. SBI was defined as the presence of IVH grades III–IV or cystic PVL according to specific ultrasound diagnostic criteria [15,16] and BPD was defined as the need for oxygen therapy or mechanical ventilation at 36 weeks’ postmenstrual age [17].
2.3. Respiratory Management
Although significant changes in respiratory management occurred in our NICU during the study period, we have typically prioritized non-invasive ventilation and less invasive surfactant administration in infants ≥24 weeks’ gestation. When invasive mechanical ventilation was required, exogenous surfactant was administered via the endotracheal tube. Starting in 2020 we implemented synchronized positive pressure ventilation with volume guarantee (VG) as the primary mode of invasive ventilation for preterm neonates. Respiratory care was escalated to rescue high-frequency oscillatory ventilation (HFOV) after failure of conventional ventilation. During the acute phase of respiratory distress syndrome, we targeted blood gas PCO₂ values of 35–50 mmHg and pH ≥7.2 and attempted to maintain oxygen saturation between 90–95%.
2.4. Statistical Analysis
Continuous variables were summarized as mean ± standard deviation when approximately normally distributed, or as median with first and third quartiles (Q1, Q3) otherwise. Categorical variables were summarized as counts and percentages. Normality was assessed using the Shapiro–Wilk and Q–Q plots. For group comparisons we used either Student’s t-test or Mann–Whitney as appropriate in each case for continuous variables, and Chi-square test or Fisher’s exact test when cell counts were <5 for categorical variables.
To describe the associations for each of the outcomes (death or SBI, SBI and BPD for survivors) with the possible predictors, we fitted 3 logistic regression models. Final models are presented as odds ratios (ORs) with 95% confidence intervals and p-values. Log-likelihood test and Akaike Information Criterion (AIC) values were used for comparison and selection between models. Model performance was evaluated using the area under the ROC curve with 95% confidence intervals. Significance level was set at 0.05 for all tests. Statistical analysis was performed using the statistical program R 4.4.1.
3. Results
During the study period, 351 neonates <32 weeks gestation were admitted to our NICU, of whom 169 required intubation and mechanical ventilation for more than 24 hours during the first 3 days of life. After applying exclusion criteria, 134 infants were included in the final analysis.
3.1. Study Population Characteristics
The median GA of the study population was 28 weeks (IQR 25–29) and the median birth weight was 950 g (IQR 700g–1230g). Of the studied neonates, 62 (46.3%) were born at <28 weeks’ gestation while 31 (23.1%) were born at 22-24 weeks. Rescue HFOV was applied in 69 (51.5%) infants. The median duration of invasive mechanical ventilation was 5 days (IQR 2–11), and the median length of NICU stay was 51 days (IQR 11–85). Survival to discharge was 61.9% (n = 83). Major morbidities of the study population included SBI in 42.5% of infants, with severe IVH (grades III-IV) occurring in 29.1%. Additional data on perinatal and neonatal characteristics of the study population are provided in Table 1 along with important clinical outcomes involving survivors only, such as BPD and retinopathy of prematurity (ROP). The following values were observed at NICU admission: pH 7.30 (7.20–7.40), maximum PCO₂ 55.6±13.4 mmHg, minimum PCO₂ 28.0±5.2 mmHg, PCO₂ difference 24.5 (16.4–33.4) mmHg, and base deficit (absolute value) 6.8 (5.2–9.2) mmol/L.
3.2. Variability in PCO₂ During the First 72 Hours
In our cohort, most infants experienced both hypercapnia and hypocapnia (Table 2), reflecting wide intra-individual variability in PCO₂ values. Hypercapnia occurred in 109 infants (81.3%), while the PCO₂ remained 45 mmHg or less in 25 infants (18.7%). Hypocapnia was even more common, and was observed in 125 infants (93.2%), with 87 (64.9%) developing severe hypocapnia (PCO₂ <30 mmHg). Notably, severe hypocapnia was often associated with concurrent episodes of moderate-to-severe hypercapnia (PCO₂ >55 mmHg).
3.3. Outcomes
3.3.1. Death or Severe Brain Injury
As shown in Table 3, infants who survived without SBI had significantly higher GA and birth weight than those who died or developed SBI (29 [28,29,30] vs. 25 [24,25,26,27] weeks; 1170 [1020–1380] vs. 710 [595–960] g; both p<0.001). Infants who died or had SBI were more frequently born <28 weeks (76.8% vs. 13.8%; p<0.001). Survivors had higher 5-min Apgar scores (8 [7,8,9] vs. 7 [7,8]; p=0.006). Pulmonary hemorrhage, air-leak syndromes, treated PDA, and NEC grade II–III were all more common among infants with death or SBI (all p≤0.037). Infants with death or SBI received rescue HFOV significantly more often compared to survivors without SBI (72.5% vs. 29.2%; p<0.001). Moreover, infants with death or SBI had higher base deficit values, greater maximum and fluctuating PCO₂ levels, and a higher incidence of hypercapnia (all p≤0.009).
3.3.2. Severe Brain Injury
Infants without SBI were more mature and had higher birth weights than those with SBI (29 [28,29,30] vs. 25 [24,25,26] weeks; 1130 [880–1350] vs. 710 [610–960] g; both p<0.001). Male sex was more common among infants with SBI (p=0.030). Infants with SBI had significantly higher rates of pulmonary hemorrhage, air-leak syndromes, and treated PDA (all p≤0.016) and were more frequently exposed to sedatives (p=0.048). Moreover, HFOV was used significantly more often in infants with SBI than in those without SBI (68.4% vs. 39%; p=0.001). Survival was markedly lower in the SBI group (31.6% vs. 84.4%; p<0.001). Additionally, infants with SBI exhibited higher maximum PCO₂ levels and greater PCO₂ fluctuations (p≤0 .01) (Online Supplementary Material Table S1).
3.3.3. Survivors with and Without BPD
Among 83 survivors, 55 (66.3%) developed BPD. These infants were significantly more premature and had lower birth weights than those without BPD (28 [26,27,28,29] vs. 30 [29,30,31] weeks; 1070 [852–1205] vs. 1318 [1122–1615] g; both p<0.001). Extremely preterm birth (<28 weeks) was much more common among infants with BPD (38.2% vs. 3.6%; p<0.001). Infants with BPD had higher rates of treated PDA (p=0.001), treated ROP (p=0.028), and sedative exposure (p=0.007). They also required rescue HFOV more often (p=0.013), had a longer duration of invasive ventilation (p<0.001), and had a longer hospital stay (p<0.001). Additionally, infants with BPD exhibited higher maximum PCO₂ levels (p=0.006) and more frequent hypercapnia (p=0.028), whereas other blood gas parameters were comparable between groups (Online Supplementary Material Table S2).
3.4. Multivariable Analyses
We constructed three multiple logistic regression models to evaluate risk factors for (1) death or SBI, (2) SBI independent of death, and (3) BPD among survivors, in very preterm neonates (Table 4). GA was included as a binary variable (<28 weeks vs. ≥28 weeks).
Model 1: GA <28 weeks was associated with higher odds of death or SBI (OR 22.5, 95% CI 8.5–68.7; p<0.001). Higher odds of death or SBI was associated with respiratory complications, including air-leak syndromes (OR 4.6, 95% CI 1.3–17.3; p=0.018) and pulmonary hemorrhage (OR 3.8, 95% CI 1.1–15.8; p=0.046). Absolute base deficit was the last predictor included in the model (OR 1.2 per unit increase, 95% CI 1.0–1.4; p=0.022). The area under the ROC curve (AUC) was 0.895 (95% CI 0.840–0.949).
Model 2: When SBI independent of death was set as the outcome, results were similar to Model 1, with male sex replacing base deficit as a significant predictor. Extremely preterm neonates had 20.6 times higher odds of SBI (OR 20.6, 95% CI 7.7–63.7; p<0.001). Air-leak syndromes (OR 6.2, 95% CI 1.8–23.8; p=0.005) and pulmonary hemorrhage (OR 4.5, 95% CI 1.4–15.8; p=0.012) remained significantly associated with SBI. Male infants were also more likely to develop SBI compared to females (OR 2.6, 95% CI 1.0–7.1; p=0.052). The AUC was 0.895 (95% CI 0.840–0.948).
Model 3: Among survivors, gestational age <28 weeks was associated with increased odds of BPD (OR 9.2, 95% CI 1.4–182.1; p=0.043). PDA requiring treatment showed a trend toward higher BPD risk (OR 5.5, 95% CI 1.2–39.9; p=0.066). Hypercapnia was independently associated with BPD (OR 3.4, 95% CI 1.1–11.5; p=0.025). The AUC was 0.808 (95% CI 0.718–0.897).
4. Discussion
In this cohort, PCO₂ instability was widespread among preterm infants requiring early mechanical ventilation, and although strongly linked to adverse outcomes, hypercapnia independently predicted only the development of BPD.
Few studies have examined the combined incidence of hypocapnia and hypercapnia in mechanically ventilated infants. In the large European Neovent cohort (2013), 4% of infants receiving invasive respiratory support had hypocapnia (PCO₂ <30 mmHg) and 31% had hypercapnia (PCO₂ >52 mmHg). Moreover, hypocapnia occurred most often during the first three days of life, whereas hypercapnia became more prevalent after one week [5]. Later research in ventilated very low birth weight infants also revealed frequent episodes of both PCO₂ abnormalities, with inadequate staffing linked to higher rates of BPD [18]. In addition, even after the implementation of a neuroprotection care bundle which included interventions aimed at optimal respiratory management, the incidence of hypocapnia (<35 mmHg), although reduced from 43.9% to 34.6%, remained common during the first 72 hours, while hypercapnia (>60 mmHg) changed little (38.5% vs. 34.1%) [19]. Another cohort of infants <32 weeks reported <2% hypocapnia and mild, moderate, and severe hypercapnia in 26.5%, 13%, and 6.5%, respectively [8]. Finally, a single-center study of 100 ventilated neonates documented hypocapnia in 82% and hypercapnia in 77%, although overlap within individual infants was not assessed [6]. These studies demonstrate the difficulty with maintaining normocapnia and are consistent with the PCO₂ variability also observed in our study.
Both hypocapnia and hypercapnia have been associated with increased mortality and significant morbidities, with invasive respiratory support being a significant contributing factor. In an exploratory analysis of a randomized trial, hypercapnic extremely low birth weight infants were found to have significantly increased mortality and required higher respiratory support, each reflecting disease severity [20]. A single-center study reported 82% of mechanically ventilated neonates experienced hypocapnia, with mortality reaching 67.1% [6]. Hypocapnia has long been recognized to induce cerebral vasoconstriction and decreased cerebral blood flow, increasing the risk of cerebral palsy and long-term neurodevelopmental impairment [21]. Conversely, hypercapnia causes cerebral vasodilation and hyperperfusion, increasing the risk of cerebral edema, IVH, and, at very high levels (>60 mmHg), seizures and decreased consciousness [22].
The recent (2022) systematic review by Wong SK et al. summarized the accumulated evidence on PCO₂ levels in preterm infants. Hypocapnia was consistently associated with adverse neurological outcomes, with greater or more prolonged exposure to low PCO₂ conferring a higher risk of poor outcomes, predominantly neurological, and in some settings, increased mortality or severe disability. Hypercapnia, on the other hand, apart from the adverse neurological outcomes (IVH), was associated with other important morbidities of prematurity such as BPD, NEC, and ROP [4].
Large database studies offer valuable context for neonatal outcomes, but they rarely focus solely on preterm infants receiving invasive respiratory support [23,24,25]. In contrast, we analyzed only mechanically ventilated infants and assessed PCO₂ in relation to death or SBI. As expected, extreme prematurity (23.1% born at 22–24 weeks) was the strongest independent predictor of death or SBI alongside pulmonary complications (air-leak, pulmonary hemorrhage), and metabolic acidosis (as indicated by base deficit). These findings support the hypothesis that fluctuations in cerebral perfusion and PCO₂ impair autoregulation and heighten vulnerability to hemorrhagic and ischemic brain injury, even though maximum PCO₂ and variability were not independent predictors in our multivariable analysis. Overall, our study showed that individual infant vulnerability early after birth, driven by extreme prematurity and its complications, was a more important contributor to death or SBI than single PCO₂ derangements.
BPD remains a major complication of prematurity. In our cohort, survival with BPD was associated with extreme prematurity, prolonged ventilation, and complications such as hemodynamically significant PDA requiring treatment. Moreover, infants with BPD exhibited higher maximum PCO₂, greater variability, and more frequent hypercapnia. Multivariable analysis confirmed that both gestational age <28 weeks and hypercapnia independently predicted BPD in survivors. Previous studies similarly implicated hypercapnia and wide CO₂ fluctuations as potential contributors to BPD [11,26], though the association may reflect disease severity, permissive hypercapnia, or intrinsic immature lung characteristics [27].
Ventilation mode is well recognized to influence PCO₂ control. In the Neovent cohort study, infants receiving pressure-limited ventilation had lower PCO₂ compared with those receiving volume-targeted or high-frequency ventilation [5]. VG -a mode of volume-targeted ventilation that automatically adjusts peak inspiratory pressure to deliver a consistent tidal volume- is considered helpful in preventing both hyperventilation and hypoventilation, thereby reducing the risk of lung and brain injury. Several meta-analyses have shown that, compared with conventional ventilation, volume-targeted modes significantly reduce BPD, duration of mechanical ventilation, pneumothorax, the combined outcome of death/BPD, and SBI [3]. As VG was widely implemented in our NICU only from 2020 onward, an earlier adoption might have reduced PCO₂ abnormalities observed in our cohort. Additionally, half of the neonates in our study received rescue HFOV. However, HFOV was in most cases not combined with VG, the use of which might have resulted not only in improved oxygenation but also in fewer PCO₂ abnormalities and survival with less severe BPD [28].
This study contributes to the limited evidence on the early incidence of hypocapnia and hypercapnia in ventilated preterm infants and their relationship with severe complications. Quantifying PCO₂ abnormalities underscores the challenges of maintaining ventilation and oxygenation targets in sick neonates receiving invasive respiratory support [29,30].
Although our retrospective design limited serial blood gas monitoring (including pH recording) and differentiation between arterial and capillary-venous samples, the first three days of life remain a critical period before physiological compensation, making PCO₂ a meaningful marker of early ventilatory status. Moreover, the availability of only a single minimum and maximum PCO₂ value may have led to an overestimation of the incidence of hypocapnia and hypercapnia, and may have captured transient changes rather than sustained exposure. NICU-specific practices may also have influenced the results, limiting generalizability to other settings. Data were collected over seven years, during which ongoing efforts to implement evidence-based practices aimed at reducing brain [31] and lung injury [32,33] were underway. These efforts included strategies for optimal PCO₂ control (e.g., use of VG in conventional ventilation), enhanced monitoring such as continuous end-tidal CO₂ and near-infrared spectroscopy to assess brain oxygenation and perfusion. In general, neonatal care bundles have been associated with reduced SBI [19,34], though their impact may be diminished as more extremely preterm infants, with an inherently high risk for IVH, receive intensive care [35]. Further research is needed to establish safe PCO₂ ranges for different gestational ages, investigate long-term neurodevelopmental outcomes, and develop strategies to minimize PCO₂ variability.
5. Conclusions
Early PCO₂ instability is highly prevalent among mechanically ventilated preterm infants, with many experiencing both hypocapnia and hypercapnia during the first three days of life. Although extreme prematurity was a major contributor to adverse outcomes -including death, SBI, and BPD- and PCO₂ abnormalities were more common in infants with adverse outcomes, hypercapnia emerged as an independent predictor only for BPD. Together, these findings highlight the importance of close CO₂ monitoring to protect the vulnerable preterm brain and lungs, while supporting a personalized approach to neonatal ventilatory care in which CO₂ management and targets are tailored to each infant’s gestational age, physiologic stability, and risk of adverse outcomes.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Perinatal and neonatal characteristics in infants with and without SBI; Table S2: Perinatal and neonatal characteristics in survivors with and without any BPD.
Author Contributions
Conceptualization, I.C. and K.S.; Methodology, I.C., A.K., C.P. and K.S.; Formal Analysis, I.C., C.P., E.A. and K.S.; Data I.C., A.K, E.A., T.S., K.T., and C.P.; Writing – Original Draft Preparation, I.C., A.K, E.A., C.P., W.C. and K.S.; Writing – Review & Editing, I.C., A.K, W.C. and K.S.; Visualization, S.T.; Supervision, K.S.; Funding Acquisition, K.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding, except for article processing charges, which were covered by the Research Committee (Eidikos Logariasmos Kondylion Erevnas) of Aristotle University of Thessaloniki. The funders had no role in the study design, data collection and analysis, decision to publish, or the preparation of the manuscript.
Institutional Review Board Statement
The study protocol was reviewed and approved by the Scientific Committee of the Hippokrateio General Hospital of Thessaloniki (Ref. number 12st/13-10- 2025). All work was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Due to the retrospective nature of the study, the parents or legal guardians of the included neonates were not available at the time the records were reviewed; therefore, written informed consent was waived.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Conflicts of Interest Statement
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript: PCO₂: partial pressure of carbon dioxide; PVL: periventricular leukomalacia; GA: gestational age; VG: volume guarantee; HFOV: high-frequency oscillatory ventilation; BPD: bronchopulmonary dysplasia; CS: caesarean section; HFOV: High frequency oscillatory ventilation; IVH: Intra-ventricular hemorrhage; NEC: necrotizing enterocolitis; NICU: neonatal intensive care unit; Mg: magnesium; PDA: patent ductus arteriosus; PPROM: preterm premature rupture of membranes; RDS: respiratory distress syndrome; ROP: retinopathy of prematurity; SBI: severe brain injury; SGA: small for gestational age; AIC: Akaike Information Criterion.
References
- Norman, M; Jonsson, B; Söderling, J; Björklund, LJ; Håkansson, S. Patterns of Respiratory Support by Gestational Age in Very Preterm Infants. Neonatology 2023, 120, 142–52. [Google Scholar] [CrossRef]
- Mukerji, A; Shah, PS; Kadam, M; Borhan, S; Razak, A. Non-invasive respiratory support in preterm infants as primary mode: a network meta-analysis. Cochrane Database Syst Rev. 2025, 7, CD014895. [Google Scholar]
- Sarafidis, K; Chotas, W; Agakidou, E; Karagianni, P; Drossou, V. The Intertemporal Role of Respiratory Support in Improving Neonatal Outcomes: A Narrative Review. Child Basel Switz. 2021, 8, 883. [Google Scholar] [CrossRef] [PubMed]
- Wong, SK; Chim, M; Allen, J; Butler, A; Tyrrell, J; Hurley, T; et al. Carbon dioxide levels in neonates: what are safe parameters? Pediatr Res. 2022, 91, 1049–56. [Google Scholar] [CrossRef] [PubMed]
- van Kaam, AH; De Jaegere, AP; Rimensberger, PC; Neovent Study Group. Incidence of hypo- and hyper-capnia in a cross-sectional European cohort of ventilated newborn infants. Arch Dis Child Fetal Neonatal Ed. 2013, 98, F323–326. [Google Scholar] [CrossRef] [PubMed]
- Bayoumi El Sebaie, D; Alsharany Abuelhamd, W; Mohamed Abdelmomen, A; Fawzy Kamal, A. Is hyperventilation a common iatrogenic problem in the neonatal intensive care unit? CHILDS Health 2024, 19, 362–7. [Google Scholar] [CrossRef]
- Thome, UH; Ambalavanan, N. Permissive hypercapnia to decrease lung injury in ventilated preterm neonates. Semin Fetal Neonatal Med. 2009, 14, 21–7. [Google Scholar] [CrossRef]
- Brown, MK; Poeltler, DM; Hassen, KO; Lazarus, DV; Brown, VK; Stout, JJ; et al. Incidence of Hypocapnia, Hypercapnia, and Acidosis and the Associated Risk of Adverse Events in Preterm Neonates. Respir Care 2018, 63, 943–9. [Google Scholar] [CrossRef]
- Kaiser, JR; Gauss, CH; Pont, MM; Williams, DK. Hypercapnia during the first 3 days of life is associated with severe intraventricular hemorrhage in very low birth weight infants. J Perinatol Off J Calif Perinat Assoc. 2006, 26, 279–85. [Google Scholar] [CrossRef]
- Fabres, J; Carlo, WA; Phillips, V; Howard, G; Ambalavanan, N. Both extremes of arterial carbon dioxide pressure and the magnitude of fluctuations in arterial carbon dioxide pressure are associated with severe intraventricular hemorrhage in preterm infants. Pediatrics 2007, 119, 299–305. [Google Scholar] [CrossRef]
- Erickson, SJ; Grauaug, A; Gurrin, L; Swaminathan, M. Hypocarbia in the ventilated preterm infant and its effect on intraventricular haemorrhage and bronchopulmonary dysplasia. J Paediatr Child Health 2002, 38, 560–2. [Google Scholar] [CrossRef] [PubMed]
- Ozawa, Y; Miyake, F; Isayama, T. Efficacy and safety of permissive hypercapnia in preterm infants: A systematic review. Pediatr Pulmonol. 2022, 57, 2603–13. [Google Scholar] [CrossRef] [PubMed]
- Travers, CP; Gentle, SJ; Shukla, VV; Aban, I; Yee, AJ; Armstead, KM; et al. Late Permissive Hypercapnia for Mechanically Ventilated Preterm Infants: A Randomized Trial. Pediatr Pulmonol. 2025, 60, e71165. [Google Scholar] [CrossRef]
- Altaany, D; Natarajan, G; Gupta, D; Zidan, M; Chawla, S. Severe Intraventricular Hemorrhage in Extremely Premature Infants: Are high Carbon Dioxide Pressure or Fluctuations the Culprit? Am J Perinatol. 2015, 32, 839–44. [Google Scholar] [CrossRef]
- Pierrat, V; Duquennoy, C; van Haastert, IC; Ernst, M; Guilley, N; de Vries, LS. Ultrasound diagnosis and neurodevelopmental outcome of localised and extensive cystic periventricular leucomalacia. Arch Dis Child Fetal Neonatal Ed. 2001, 84, F151–156. [Google Scholar] [CrossRef]
- Papile, LA; Burstein, J; Burstein, R; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. 1978, 92, 529–34. [Google Scholar] [CrossRef]
- Jobe, AH; Bancalari, E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2001, 163, 1723–9. [Google Scholar] [CrossRef] [PubMed]
- Röhr, M; Poryo, M; Bay, J; Gortner, L; Meyer, S. Episodes of hypo- and hypercapnia in a cohort of mechanically ventilated VLBW infants: the role of adequate staffing. Wien Med Wochenschr 1946 2017, 167, 256–8. [Google Scholar] [CrossRef]
- Murthy, P; Zein, H; Thomas, S; Scott, JN; Abou Mehrem, A; Esser, MJ; et al. Neuroprotection Care Bundle Implementation to Decrease Acute Brain Injury in Preterm Infants. Pediatr Neurol. 2020, 110, 42–8. [Google Scholar] [CrossRef]
- Thome, UH; Dreyhaupt, J; Genzel-Boroviczeny, O; Bohnhorst, B; Schmid, M; Fuchs, H; et al. Influence of PCO2 Control on Clinical and Neurodevelopmental Outcomes of Extremely Low Birth Weight Infants. Neonatology 2018, 113, 221–30. [Google Scholar] [CrossRef] [PubMed]
- Levene, M. Minimising neonatal brain injury: how research in the past five years has changed my clinical practice. Arch Dis Child. 2007, 92, 261–5. [Google Scholar] [CrossRef]
- Zhou, W; Liu, W. Hypercapnia and hypocapnia in neonates. World J Pediatr WJP 2008, 4, 192–6. [Google Scholar] [CrossRef] [PubMed]
- Shah, PS; Lui, K; Sjörs, G; Mirea, L; Reichman, B; Adams, M; et al. Neonatal Outcomes of Very Low Birth Weight and Very Preterm Neonates: An International Comparison. J Pediatr. 2016, 177, 144–152.e6. [Google Scholar] [CrossRef]
- Razak, A; Johnston, E; Stewart, A; Clark, MAT; Stevens, P; Charlton, M; et al. Temporal Trends in Severe Brain Injury and Associated Outcomes in Very Preterm Infants. Neonatology 2024, 121, 440–9. [Google Scholar] [CrossRef] [PubMed]
- Lee, J; Lee, CYM; Naiduvaje, K; Wong, Y; Bhatia, A; Ereno, IL; et al. Trends in neonatal mortality and morbidity in very-low-birth-weight (VLBW) infants over a decade: Singapore national cohort study. Pediatr Neonatol. 2023, 64, 585–95. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, S; El-Mohandes, A; Dhanireddy, R; Koch, MA. Association of bronchopulmonary dysplasia and hypercarbia in ventilated infants with birth weights of 500-1,499 g. Matern Child Health J. 2011, 15, S17–26. [Google Scholar] [CrossRef]
- Dassios, T. On carbon dioxide and bronchopulmonary dysplasia. Acta Paediatr Oslo Nor 1992 2023, 112, 2248–9. [Google Scholar] [CrossRef]
- Liu, W; Zong, H; Jiang, J; Yang, C; Li, F. High-frequency oscillatory ventilation with volume guarantee in infants: a systematic review. Pediatr Res. 2025, 98, 470–8. [Google Scholar] [CrossRef]
- Solberg, MT; Bjørk, IT; Hansen, TWR. Adherence to oxygenation and ventilation targets in mechanically ventilated premature and sick newborns: a retrospective study. BMC Pediatr. 2013, 13, 126. [Google Scholar] [CrossRef]
- Nadeem, M; Murray, D; Boylan, G; Dempsey, EM; Ryan, CA. Blood carbon dioxide levels and adverse outcome in neonatal hypoxic-ischemic encephalopathy. Am J Perinatol. 2010, 27, 361–5. [Google Scholar] [CrossRef]
- Society, CP. Neuroprotection from acute brain injury in preterm infants | Canadian Paediatric Society [Internet]. 11 Nov 2025. Available online: https://cps.ca/en/documents/position/neuroprotection.
- Sweet, DG; Carnielli, VP; Greisen, G; Hallman, M; Klebermass-Schrehof, K; Ozek, E; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome: 2022 Update. Neonatology 2023, 120, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Sweet, DG; Carnielli, V; Greisen, G; Hallman, M; Ozek, E; te Pas, A; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome – 2019 Update. Neonatology 2019, 115, 432–50. [Google Scholar] [CrossRef] [PubMed]
- de Bijl-Marcus, K; Brouwer, AJ; De Vries, LS; Groenendaal, F; Wezel-Meijler, G; van. Neonatal care bundles are associated with a reduction in the incidence of intraventricular haemorrhage in preterm infants: a multicentre cohort study. Arch Dis Child Fetal Neonatal Ed. 2020, 105, 419–24. [Google Scholar] [CrossRef]
- Erni, I; Bassler, D; Glauser, D; Wolff, M; Grass, B; Adams, M. Quality improvement project to reduce intraventricular haemorrhage in very preterm infants failed due to increased life-sustaining intensive care at low gestational age. BMJ Open Qual. 2025, 14, e003325. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Perinatal and neonatal characteristics of the study population.
| Variable | Descriptive statistics |
|---|---|
| (n=134) | |
| Gestational age (weeks) | 28 (25; 29) |
| Gestational age < 28 (weeks) | 62 (46.3%) |
| Birth weight (g) | 950 (700; 1230) |
| 5-min Apgar score | 8 (7; 8) |
| Male sex | 63 (47.0%) |
| SGA | 20 (14.9%) |
| Maternal hypertension | 22 (16.4%) |
| Chorioamnionitis | 28 (20.9%) |
| PPROM | 35 (26.1%) |
| Prenatal steroids | 116 (86.6%) |
| Mg administration | 76 (56.7%) |
| Caesarean section | 114 (85.1%) |
| Inborn | 120 (89.6%) |
| Surfactant for RDS | 123 (91.8%) |
| Pulmonary hemorrhage | 31 (23.1%) |
| Air-leak syndromes | 25 (18.7%) |
| PDA | 66 (49.3%) |
| Treated PDA | 54 (40.3%) |
| Severe IVH | 39 (29.1%) |
| SBI | 57 (42.5%) |
| Sepsis (Culture-positive; early/late) | 69 (51.5%) |
| Fentanyl or sedative | 69 (51.5%) |
| NEC (grade II, III) | 17 (12.7%) |
| Rescue HFOV | 69 (51.5%) |
| Duration of invasive ventilation (days) | 5.0 (2.0; 11.0) |
| Survival | 83 (61.9%) |
| Death or SBI | 69 (51.5%) |
| Length of stay (days) | 51 (11; 85) |
| At NICU admission | |
| pH | 7.3 (7.2; 7.4) |
| PCO2 | 36.8 (30.1; 44.0) |
| Base Deficit (absolute value) | 6.8 (5.2; 9.2) |
| During the first 3 days of life | |
| Min PCO2 | 28.0 (± 5.2) |
| Max PCO2 | 55.6 (±13.4) |
| Max-min PCO2 | 24.5 (16.4; 33.4) |
| Clinical outcomes in survivors (n=83) | |
| Any BPD | 54 (65.9%) |
| ROP | 33 (40.2%) |
| Treated ROP | 13 (15.9%) |
| Length of stay (days) | 75 (54; 115) |
Data are presented as mean (SD), median (Q1, Q3) or counts (%). BPD: bronchopulmonary dysplasia; CS: caesarean section; HFOV: High frequency oscillatory ventilation; IVH: Intraventricular hemorrhage; NEC: necrotizing enterocolitis; NICU: neonatal intensive care unit; Mg: magnesium; PDA: patent ductus arteriosus; PPROM: preterm premature rupture of membranes; RDS: respiratory distress syndrome; ROP: retinopathy of prematurity; SBI: severe brain injury; SGA: small for gestational age.
Table 2.
Cross-tabulation of min and max PCO2 (mmHg) of the study population.
| Max PCO2 group | ||||
|---|---|---|---|---|
| Min PCO2 group | 35-45 | 46-55 | 56-65 | >65 |
| <30 | 21 (15.7%) | 27 (20.1%) | 17 (12.7%) | 22 (16.4%) |
| 30-34 | 4 (3%) | 19 (14.2%) | 11 (8.2%) | 4 (3%) |
| 35-45 | 0 (0%) | 5 (3.7%) | 4 (3%) | 0 (0%) |
Values represent the number and percentage of participants within each PCO₂ group.
Table 3.
Perinatal and neonatal characteristics of infants who survived without SBI and in those with the combined outcome of death or SBI.
Table 3.
Perinatal and neonatal characteristics of infants who survived without SBI and in those with the combined outcome of death or SBI.
| Variable | Survival without SBI (n=65) | Death or SBI (n=69) | p-value |
|---|---|---|---|
| Gestational age (weeks) | 29 (28; 30) | 25 (24; 27) | <0.001 |
| Gestational age < 28 weeks | 9 (13.8%) | 53 (76.8%) | <0.001 |
| Birth weight (g) | 1170 (1020; 1380) | 710 (595; 960) | <0.001 |
| 5-min Apgar score | 8 (7; 9) | 7 (7; 8) | 0.006 |
| Male sex | 25 (38.5%) | 38 (55.1%) | 0.054 |
| SGA | 9 (13.8%) | 11 (15.9%) | 0.734 |
| Maternal hypertension | 14 (21.5%) | 8 (11.6%) | 0.120 |
| Chorioamnionitis | 10 (15.4%) | 18 (26.1%) | 0.128 |
| PPROM | 12 (18.5%) | 23 (33.3%) | 0.050 |
| Prenatal steroids | 55 (84.6%) | 61 (88.4%) | 0.520 |
| Mg administration | 35 (53.8%) | 41 (59.4%) | 0.515 |
| Caesarean section | 60 (92.3%) | 54 (78.3%) | 0.029 |
| Inborn | 60 (92.3%) | 60 (87.0%) | 0.401 |
| Surfactant for RDS | 58 (89.2%) | 65 (94.2%) | 0.356 |
| Pulmonary hemorrhage | 5 (7.7%) | 26 (37.7%) | <0.001 |
| Air-leak syndromes | 7 (10.8%) | 18 (26.1%) | 0.023 |
| Treated PDA | 15 (23.1%) | 39 (56.5%) | <0.001 |
| Sepsis (Culture positive; early/late) | 31 (47.7%) | 38 (55.1%) | 0.393 |
| Fentanyl or sedative | 29 (44.6%) | 40 (58.0%) | 0.122 |
| NEC (grade II, III) | 4 (6.2%) | 13 (18.8%) | 0.037 |
| Rescue HFOV | 19 (29.2%) | 50 (72.5%) | <0.001 |
| Duration of invasive ventilation | 4 (1; 9) | 7 (4; 15) | 0.005 |
| At NICU admission | |||
| pH | 7.3 (7.3; 7.4) | 7.3 (7.2; 7.4) | 0.540 |
| PCO2 | 37.4 (31.3; 47.0) | 36.5 (29.4; 42.6) | 0.223 |
| Base Deficit (absolute value) | 5.9 (4.4; 8.5) | 7.4 (5.9; 9.8) | 0.005 |
| During the first 3 days of life | |||
| Min PCO2 | 28.8 (± 5.3) | 27.3 (± 5.0) | 0.116 |
| Max PCO2 | 51.2 (± 10.8) | 59.8 (± 14.3) | <0.001 |
| Max-min PCO2 difference | 20.7 (13.4; 28.1) | 29.1 (22.4; 40.2) | <0.001 |
| Hypercapnia | 47 (72.3%) | 62 (89.9%) | 0.009 |
| Hypocapnia | 60 (92.3%) | 65 (94.2%) | 0.739 |
Data are presented as mean (SD), median (Q1, Q3) or counts (%). BPD: bronchopulmonary dysplasia; CS: caesarean section; HFOV: High frequency oscillatory ventilation; IVH: Intraventricular hemorrhage; NEC: necrotizing enterocolitis; NIC: neonatal intensive care unit; Mg: magnesium; PDA: patent ductus arteriosus; PPROM: preterm premature rupture of membranes; RDS: respiratory distress syndrome; ROP: retinopathy of prematurity; SBI: severe brain injury; SGA: small for gestational age.
Table 4.
Multiple logistic regression models.
| Death or Severe brain injury model | ||
| Predictor | OR (95%) | p-value |
| Gestational age < 28 weeks | 22.5 (8.5-68.7) | <0.001 |
| Air-leak syndromes | 4.6 (1.3-17.3) | 0.018 |
| Pulmonary hemorrhage | 3.8 (1.1-15.8) | 0.046 |
| Base Deficit (absolute value) | 1.2 (1-1.4) | 0.022 |
| Severe brain injury model | ||
| Predictor | OR (95%) | p-value |
| Gestational age < 28 weeks | 20.6 (7.7-63.7) | <0.001 |
| Air-leak syndromes | 6.2 (1.8-23.8) | 0.005 |
| Pulmonary hemorrhage | 4.5 (1.4-15.8) | 0.012 |
| Male sex | 2.6 (1-7.1) | 0.052 |
| BPD model for survivors | ||
| Predictor | OR (95%) | p-value |
| Gestational age < 28 weeks | 9.2 (1.4-182.1) | 0.043 |
| Treated PDA | 5.5 (1.2-39.9) | 0.066 |
| Hypercapnia | 3.4 (1.1-11.5) | 0.025 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



