Submitted:
16 February 2026
Posted:
27 February 2026
You are already at the latest version
Abstract
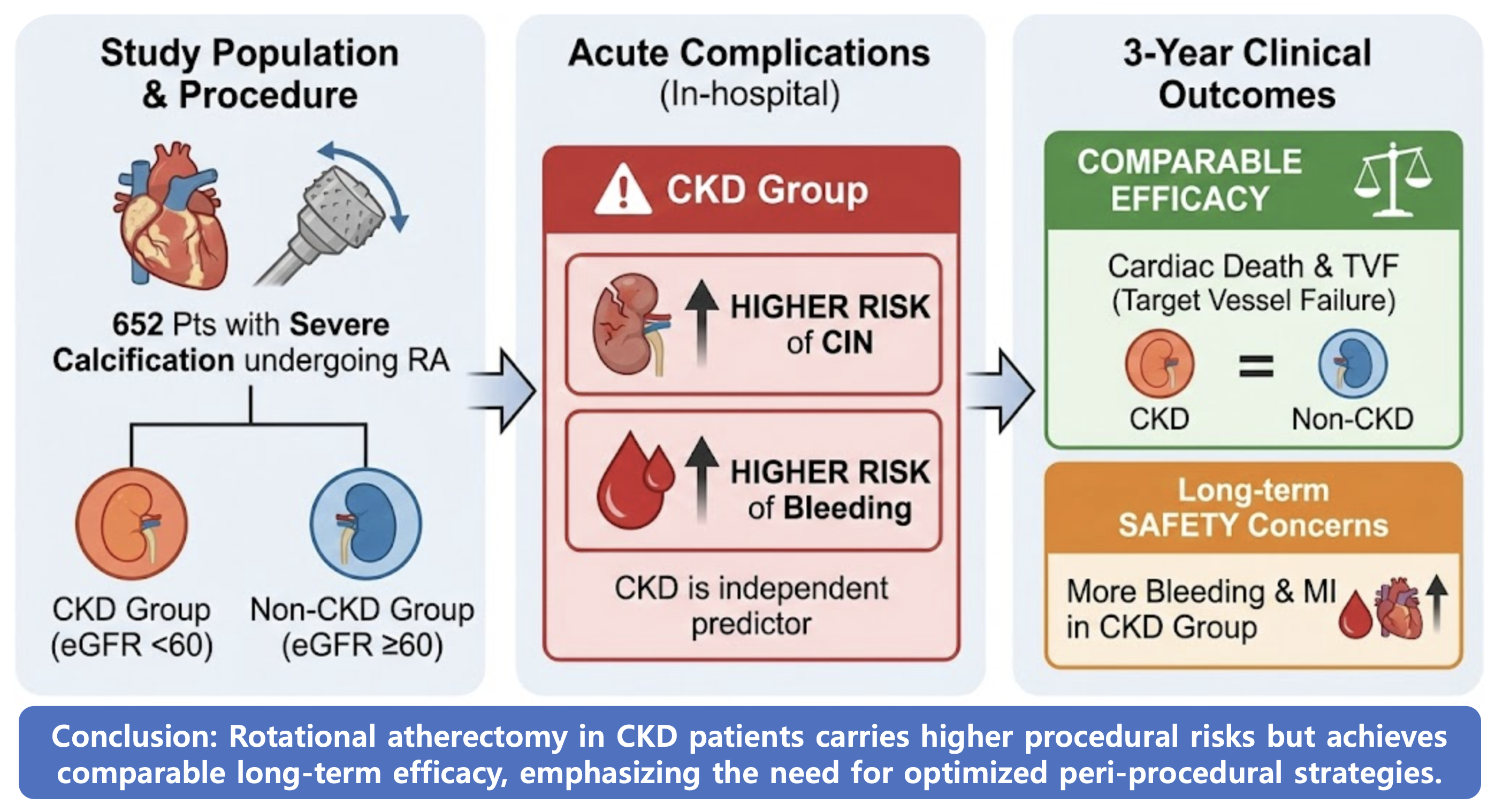
Background and Objectives: Chronic kidney disease (CKD) is associated with severe coronary calcification and increased procedural risks. We aimed to evaluate the impact of CKD on contrast-induced nephropathy (CIN), bleeding, and long-term clinical outcomes in patients undergoing rotational atherectomy (RA). Materials and Methods: This study retrospectively analyzed 652 patients who underwent RA for calcified coronary lesions from the multicenter ROCK registry and a single-center extension between 2010 and 2025. Patients were classified into CKD (eGFR < 60 mL/min/1.73 m², n = 66) and non-CKD (n = 586) groups, excluding those on dialysis. The primary endpoint was a composite of CIN and in-hospital bleeding. Secondary endpoints included 3-year target vessel failure (TVF), myocardial infarction (MI), and total bleeding. Results: The primary composite outcome occurred more frequently in the CKD group (16.7% vs. 5.1%, p = 0.001). Specifically, CIN was significantly higher in CKD patients (15.2% vs. 1.7%, p < 0.001), while in-hospital bleeding did not differ significantly. In multivariate analysis, CKD was an independent predictor of the primary outcome (adjusted OR 3.02; 95% CI 1.36–6.69; p = 0.006). At 3-year follow-up, total bleeding (10.6% vs. 3.9%, p = 0.008) and MI (6.1% vs. 2.1%, p = 0.024) were higher in the CKD group, whereas TVF and cardiac death showed no significant difference. Conclusions: CKD is a robust independent risk factor for CIN and long-term bleeding in patients undergoing RA. However, comparable long-term efficacy outcomes suggest that RA remains a feasible strategy in CKD patients when early complications are carefully managed with contrast-minimizing strategies.
Keywords:
rotational atherectomy (RA)
; chronic kidney disease (CKD)
; contrast-induced nephropathy (CIN)
1. Introduction
Chronic kidney disease (CKD) is associated not only with a higher burden of coronary artery disease but also with a disproportionately high prevalence of severe coronary artery calcification; a meta-analysis reported coronary artery calcification in approximately 60% of CKD patients, and observational data suggest that calcification can be present in up to 90% of patients with more advanced CKD group [1,2,3].
Severe coronary calcification is a well-studied risk factor or procedural complexity and is associated with suboptimal percutaneous coronary intervention (PCI) performance and worse clinical outcomes, including higher rates of repeat revascularization and adverse events after intervention [4,5].
In patients with CKD, contrast using invasive procedures such as coronary angiography and PCI carry a heightened risk of contras-induced nephropathy (CIN) and bleeding complications compared with patients with preserved renal function, reflecting both reduced renal reserve and a CKD-related bleeding diathesis [6]. Consistently, CKD has been linked to increased rates of major adverse cardiovascular events and mortality after PCI, with higher ischemic and hemorrhagic event rates observed in contemporary cohorts [7] and large trial datasets [8].
Rotational atherectomy (RA) is an established strategy for severely calcified, high complexity coronary lesions; however, it is used in a relatively small proportion of PCI procedures worldwide, typically on the order of 1-2% of all PCI cases in national datasets [9,10].
Despite the growing body of RA literature, data specifically evaluating CIN and bleeding, along with long-term clinical outcomes in RA-treated patients, particularly stratified by CKD status remain limited. Therefore, we conducted a retrospective analysis based on a RA registry to compare CIN, bleeding, and long-term outcomes between CKD and non-CKD patients undergoing RA.
2. Materials and Methods
2.1. Study Design and Population
The clinical data of 540 patients with severe calcific coronary artery disease who underwent PCI using RA between January 2010 and October 2019 at 9 tertiary centers from the ‘ROtational atherectomy in Calcified lesions in Korea (ROCK)’ registry and additional 178 patients from Saint Vincent hospital from November 2019 to August 2025 were retrospectively analyzed. Among them, 66 patients under dialysis were excluded since our main outcome, CIN was not able to be evaluated in dialysis patients. The clinical characteristics of total 652 patients were collected from each center using a standardized case report form of procedural details and follow-up data. Follow-up data were obtained from patient medical records or physician/patient interviews were retrospectively analyzed. The local ethics committee of each hospital approved this study. Informed consent to participants was waived because this study was designed as retrospective study. All methods were performed in accordance with the relevant guidelines and regulations. Between 2010 and 2019, consecutive patients with heavily calcific coronary lesions and significant stenosis (stenosis ≥ 70% of vessel diameter) who underwent PCI using RA were retrospectively enrolled from each institutional database. CKD was defined as an estimated glomerular filtration rate <60 mL/min/1.73 m2, as calculated using the Modification of Renal Diet equation from baseline serum creatinine [11]. Study population and flow chart are described in Figure 1.
2.2. RA Procedure
Following the protocol of ROCK Registry, the treatment strategy, including decisions of performing/timing of RA, burr size, and choice of vascular access, was at the discretion of the attending cardiologists with careful consideration of clinical risk factors, anatomical complexity, patients’ conditions. Standard techniques guided all procedures. All RA procedures were performed using the Rotablator TM RA system (Boston Scientific, Marlborough, MA, USA). During RA, pauses in ablation runs and intracoronary nitroglycerin and/or verapamil were used to avoid coronary spasm and slow flow phenomenon. Antiplatelet therapy and peri-procedural anticoagulation were performed following the accepted guidelines [12,13]. Also, direct RA is included in our study defined as the early application of RA (1) before pre-balloon; (2) pre-balloon dilation with balloon size of less than 2.0 mm; (3) judged by tactile sense of balloon passage by operators; or (4) presence severe calcification on imaging modalities. On the other hand, indirect RA was defined as RA after the balloon was expanded to a size greater than 2.0 mm.
2.3. Study Outcomes
The primary endpoint of the study was a composite of CIN and in-hospital bleeding. And the individual outcome was also evaluated. CIN was defined as the impairment of kidney function measured as either a 25% increase in serum creatinine from baseline or a 0.5 mg/dL increase in absolute serum creatinine value within 48–72 h after the procedure. The secondary endpoint were 3-year outcome of target-vessel failure (TVF), defined as cardiac death, target-vessel spontaneous myocardial infarction (TVMI), or target vessel revascularization (TVR), all-cause death, cardiac death (CD), any MI, TVMI, any repeat revascularization (RR), TVR, target-lesion revascularization (TLR), stent thrombosis (ST), cerebrovascular accident (CVA), and bleeding. Technical success was defined as the achievement of residual stenosis < 30% in the presence of grade III Thrombolysis in myocardial infarction flow. Procedural success was defined as achieving technical success without in-hospital major adverse cerebral and cardiac events (MACCEs), including in-hospital death, in-hospital CVA, urgent revascularization (CABG or PCI), peri-procedural MI or ST during the hospitalization period. Procedural complications included cardiac tamponade, coronary perforation, severe coronary dissection, defined from The National Heart, Lung, and Blood Institute classification system as type D, E, and F, temporary pacemaker insertion, CIN, or in-hospital bleeding. We investigated procedure time, radiation dose, and contrast amount to assess procedural efficiency and safety. Death was defined as death from any cause. TVMI was spontaneous MI clearly attributable to the target vessel. Spontaneous MI was defined as any creatine kinase-myocardial band or troponin increase above the upper limit of the normal range with ischemic symptoms or signs during follow-up after discharge. Peri-procedural MI was defined as peak elevations of the creatine kinase-myocardial band of over 10-fold above the upper reference limit within 48 h after the procedure [14]. RR was defined as any percutaneous or surgical revascularization in any vessel. TVR was defined as any percutaneous or surgical revascularization of the treated vessel. TLR was defined as any percutaneous or surgical revascularization of the treated lesion. CVA was defined as a focal neurological deficit of central origin lasting >24 h, confirmed by a neurologist and imaging. All clinical events were confirmed by source documentation collected at each hospital and centrally adjudicated by an independent group of clinicians unaware of the revascularization type.
2.4. Statistical Analyses
Continuous variables were presented as mean ± standard deviation (SD) and compared using the Student t-test or Mann Whitney U test. Categorical variables were presented as counts (percentages) and compared using the chi-square or Fisher exact test, as appropriate. The primary outcomes were analyzed using multivariable logistic regression models. Odds ratios with 95% confidence intervals were calculated to estimate the independent association between CKD status and the occurrence of each outcome after adjustment for predefined covariates. Event rates were estimated on Kaplan–Meier estimates in time-to-first-event analyses, and they were compared using the log-rank test. A univariate Cox regression analysis was performed to obtain the hazard ratio (HR) for clinical outcomes. Then, to find out the independent predictors with the clinical outcomes, a multivariate Cox proportional hazard regression model was performed using important clinical covariates including clinically relevant variables and statistically significant variables with a p-value < 0.05 by univariate analysis. For subgroup analysis, Cox regression analysis was performed and visualized using forest plots. All statistical analyses were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC, USA), and a p-value < 0.05 was considered statistically significant.
3. Results
3.1. Baseline Characteristics
Baseline characteristics are summarized in Table 1, Table 2 and Table 3. A total of 652 patients who underwent ROTA were included in the analysis, of whom 66 (10.1%) were classified as having CKD (eGFR < 60 mL/min/1.73 m²) and 586 (89.9%) as non-CKD. Diabetes mellitus (DM) was higher in the CKD group (78.8% vs. 54.2%, p < 0.001). Regarding cardiovascular history, prior peripheral vascular disease were more frequent in the CKD group (21.2% vs. 6.5%, p < 0.001), whereas prior myocardial infarction and prior coronary artery bypass grafting showed no statistically significant differences between groups. Clinical diagnosis of STEMI/NSTEMI was more included in CKD group (39.4% vs. 26.0%, p = 0.021). Patients with CKD had a lower pre-procedural left ventricular ejection fraction compared with non-CKD patients (48.4 ± 14.0 vs. 54.0 ± 12.9, p = 0.001). Other vessel revascularization was performed more frequently in CKD group (54.6% vs. 41.9, p = 0.049). Lastly, contrast volume was significantly less used in CKD group (189.4 ± 95.6 vs. 214.1 ± 91.9, p = 0.044).
3.2. Primary Outcomes
Primary in-hospital outcomes are presented in Table 4. The composite outcome of CIN or in-hospital bleeding occurred more frequently in the CKD group compared with the non-CKD group (16.7% vs. 5.1%, p = 0.001). After adjustment for age, sex, smoking, hypertension, diabetes, clinical diagnosis of STEMI/NSTEMI, MVD, other-vessel revascularization, procedural approach, and pre-procedural LV ejection fraction, CKD remained independently associated with the composite outcome (adjusted OR, 3.02; 95% CI, 1.36-6.69; p = 0.006). CIN occurred significantly more often in patients with CKD (15.2% vs. 1.7%, p < 0.001). In multivariable analysis using the same adjustment model, CKD was an independent predictor of CIN (adjusted OR, 7.18; 95% CI, 2.32-22.21, p < 0.001). In-hospital bleeding alone did not differ significantly between the non-CKD and CKD groups (3.0% vs. 3.6%, p > 0.999).
3.3. Secondary Outcomes
3-year outcomes are summarized in Table 4. Median follow-up duration was 1.5 (IQR, 0.6-2.9) years. Myocardial infarction occurred more frequently in CKD patients (6.1% vs. 2.1%, log-rank p = 0.024) and CKD was independently associated with an increased risk of myocardial infarction in multivariable analysis (adjusted HR, 4.00; 95% CI, 1.16-13.68, log-rank p = 0.029). However, TVF, CD, TVMI, TVR, CVA, and ST were more common in the CKD group, though this did not reach statistical significance. Total bleeding events during follow-up occurred markedly more often in CKD patients (10.6% vs. 3.9%, log-rank p = 0.008), with CKD showing a strong independent association after multivariable adjustment (adjusted HR, 3.39; 95% CI, 1.37-8.37, log-rank p = 0.008). This association was primarily driven by minor bleeding events (adjusted HR, 7.80; 95% CI, 2.28-26.65, log-rank p = 0.001), whereas major bleeding did not differ significantly between two groups. Kaplan-Meier curves representing 3-year outcomes of TVF, CD, MI, TVMI, TVR, and total bleeding are shown in Figure 2.
3.4. Subgroup Analyses
Subgroup analyses were performed to evaluate whether the association between CKD and the composite primary outcome (CIN or in-hospital bleeding) differed across clinically relevant subgroups, including age (< 70 vs. ≥ 70 years), sex, presence of MVD, other-vessel revascularization, use of a direct RA strategy, and pre-procedural LVEF (Figure 3). CKD was consistently associated with an increased risk of the composite primary outcome across most subgroups. The magnitude of risk associated with CKD was particularly pronounced in patients aged ≥ 70 years (OR, 3.31; 95% CI, 1.44-7.62, p = 0.005) , male patients (OR, 4.51; 95% CI, 1.62-12.55, p = 0.004), those with MVD (OR, 4.46; 95% CI, 1.98-10.03, p < 0.001), patients undergoing other-vessel revascularization (OR, 5.67; 95% CI, 2.01-16.05, p = 0.001),those with direct RA approach (OR, 5.10; 95% CI, 2.14-12.16, p < 0.001), and those with pre-procedural LVEF under 50% (OR, 5.20; 95% CI, 1.92-14.13, p = 0.001) indicating that the adverse effect of CKD on the primary outcome was consistent across these subgroups.
4. Discussion
In this retrospective cohort study, CKD was independently associated with a significantly higher risk of CIN in patients undergoing ROTA. Subgroup analyses demonstrated that this association remained consistent across most clinically relevant strata, including age ≥70 years, sex, MVD, other-vessel revascularization, direct ROTA strategy, and pre-procedural ejection fraction. With respect to 3-year outcomes, myocardial infarction and total bleeding events occurred significantly more frequently in the CKD group, whereas major adverse cardiovascular events (MACE), cerebrovascular accident (CVA), and stent thrombosis (ST) were numerically higher but did not reach statistical significance.
Coronary artery calcification in patients with CKD represents a critical determinant of both treatment strategy and long-term prognosis. Patients with CKD not only have a higher burden of coronary artery disease but also exhibit more advanced vascular calcification, often necessitating coronary intervention. Such interventions inherently require invasive procedures involving antithrombotic therapy with potential bleeding risk, as well as the unavoidable use of iodinated contrast agents, a well-established precipitant of acute kidney injury. In this context, CKD embodies a clinical phenotype intrinsically vulnerable to coronary procedures.
For patients with severe coronary calcification, preparation with RA is often required beyond conventional balloon angioplasty. Several studies have evaluated the clinical outcomes of RA-treated populations. Although not stratifying patients specifically by CKD status, prior investigations have identified low preoperative mean arterial pressure as an important predictor of CIN in RA-treated patients [15]. Moreover, studies examining plaque-modification strategies have shown that patients requiring additional intervention for severe calcification experience higher rates of CIN compared with those undergoing less complex PCI [16]. Conversely, one study comparing RA and non-RA groups reported reduced MACE rates in the RA group during in-hospital and 2-year follow-up, suggesting potential procedural benefits in selected patients [17].
It is well established that CKD patients experience higher rates of CIN and bleeding complications following contrast-based invasive procedures compared with individuals with preserved renal function [18,19]. Several pathophysiological mechanisms may explain these observations. CKD patients are more susceptible to contrast-induced renal injury even at comparable contrast volumes due to impaired renal reserve and altered microvascular autoregulation. Although RA-treated patients are generally expected to require higher contrast volumes than non-RA PCI cases, the contrast volume used in our study was much lower than that reported in prior ROTA versus non-ROTA comparisons [20]. Notably, even with relatively lower contrast exposure in the CKD group, the risk of CIN remained substantially higher than in the non-CKD group, reaffirming CKD itself as a major independent determinant of CIN.
Regarding bleeding risk, despite the interventional complexity associated with RA, in-hospital bleeding did not significantly differ between CKD and non-CKD groups. Although total bleeding events during 3-year follow-up were significantly higher in CKD patients, this difference was primarily driven by minor bleeding events. This observation may be partly explained by the absence of significant differences in vascular access site distribution (radial vs. femoral) and other peri-procedural factors, including procedural time, between the two groups. Nevertheless, given the significantly increased long-term bleeding risk observed in CKD patients, individualized therapeutic planning that incorporates bleeding propensity remains important. The biological basis for increased bleeding in CKD is well recognized. CKD is associated with platelet dysfunction, endothelial abnormalities, and uremia-related coagulopathy, all contributing to an elevated bleeding tendency [21]. Current guidelines also recognize CKD as a major determinant of bleeding risk and recommend consideration of early de-escalation or shortening of dual antiplatelet therapy when clinically appropriate [22,23,24]. Furthermore, the preferential use of polymer-free or bioabsorbable-polymer stents may facilitate shorter durations of dual antiplatelet therapy without compromising ischemic protection in this high-risk population [25].
In subgroup analyses, although post-procedural bleeding complications are generally more common in women [26], the magnitude of risk associated with CKD was higher in male patients in our cohort. In patients with MVD, longer procedural times, higher contrast volumes, and repeated intra-procedural anticoagulation may contribute to increased bleeding and renal stress. Similarly, in cases where direct RA was not performed, the need for additional lesion preparation may increase procedural burden and contrast exposure, potentially explaining the observed increase in risk.
One prior study evaluating ROTA in patients with advanced CKD, including those with end-stage renal disease on dialysis, reported no significant difference in acute procedural complications according to renal function and emphasized the feasibility of RA in advanced CKD [27]. Consistent with our findings, while CKD itself confers an unavoidable increase in acute procedural risk—particularly for CIN—long-term MACE did not significantly differ after 3 years. This suggests that with meticulous peri-procedural management and careful complication control, RA remains a viable therapeutic option in CKD patients.
Taken together, our findings support a more individualized interventional strategy in CKD patients undergoing RA. In those with multivessel disease, early consideration of staged PCI may help reduce contrast burden. In elderly CKD patients, thorough pre-procedural imaging assessment and strategic planning—including contrast minimization and the use of a direct ROTA approach to reduce procedural time—may prevent renal injury. Although acute complications may not be entirely avoidable, appropriate early management may allow CKD patients to achieve long-term outcomes comparable to those without CKD, supporting the feasibility of RA in this high-risk population.
This study has several limitations. First, the retrospective study design precludes causal inference and may allow residual confounding; however, we applied multivariable adjustment and subgroup analyses to strengthen the validity of our findings. Second, though the sample size was not large, the cohort consisted exclusively of patients undergoing RA, making the study adequately powered within this high-risk population. Third, patients with end-stage renal disease on dialysis were excluded because CIN was a primary endpoint, which limits generalizability but was necessary to accurately evaluate contrast-related renal injury. Finally, procedural strategies and contrast use were operator-dependent, and minor bleeding events may have been underreported; though, key clinical variables were incorporated into adjusted analyses.
In patients undergoing RA for severely calcified coronary lesions, CKD independently increases the risk of CIN and long-term bleeding, as well as ischemic events such as MI. However, comparable 3-year major adverse cardiovascular outcomes suggest that RA remains a feasible strategy in CKD when early complications are carefully managed. These findings emphasize the need for contrast-minimizing procedural strategies, thoughtful lesion preparation planning, and tailored antiplatelet regimens in CKD patients undergoing complex coronary intervention.
5. Conclusions
In patients undergoing rotational atherectomy for severely calcified coronary lesions, CKD is a robust independent risk factor for CIN and long-term bleeding complications, particularly minor bleeding. However, the long-term efficacy outcomes, including target vessel failure and cardiac death, were comparable between CKD and non-CKD groups. These findings support the feasibility of rotational atherectomy in CKD patients, emphasizing the importance of optimized peri-procedural strategies to minimize contrast burden and bleeding complications.
Author Contributions
Conceptualization, J.L.,S.-S.C., J.J., K.K., Y.K., K.L. and S.-H.H.; data curation, S.-R.L., W.-Y.J., J.-H.L. (Jang-Hoon Lee), I.-J.C., K.-H.Y., S.-W.L., J.-H.L. (Jae-Hwan Lee), H.-J.L., S. H.H., S.-N.L. and K.L.; formal analysis, S.-H.H.; investigation, J.L., Y.K. and J.J.; methodology, S.-H.H. and K.-D.Y.; project administration, S.-H.H., K.L. and J.J.; resources, K.-W.M., K.-D.Y. and D.M.; software, J.L.,S.-S.C.; supervision, K.-D.Y., S.-H.H. and K.L.; validation, S.-H.H., K.K. and J.J.; visualization, J.L., S. S.C., K.K. and J.J.; writing—original draft preparation, J.L., S.-S.C., J.J. and S.-H.H.; writing—review and editing, S.-H.H., K.-D.Y., S.-R.L. and K.L. Each author has reviewed and consented to the final manuscript as submitted for publication. All authors have read and agreed to the published version of the manuscript.
Funding
This study received no external funding.
Institutional Review Board Statement
The study was executed following the guidelines of the Declaration of Helsinki and authorized by the Institutional Review Board (IRB) of Daejeon St. Mary’s Hospital (approval code: DC19REDI0066, approval date: 30 July 2019).
Informed Consent Statement
All participants in the study provided their informed consent.
Data Availability Statement
The data included in this manuscript cannot be shared publicly, due to the need to protect the privacy of the included subjects. Data may be shared upon reasonable request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CABG | coronary artery bypass graft |
| CD | cardiac death |
| CIN | contrast induced nephropathy |
| CKD | chronic kidney disease |
| CVA | cerebrovascular accident |
| LVEF | left ventricle ejection fraction |
| MVD | multivessel disease |
| PCI | percutaneous coronary intervention |
| RA | rotational atherectomy |
| ST | stent thrombosis |
| RR | repeat revascularization |
| TVF | target vessel failure |
| TVM | target-vessel spontaneous myocardial infarction |
| TVR | target-vessel revascularization |
References
- Russo, D; Palmiero, G; De Blasio, AP; Balletta, MM; Andreucci, VE. Coronary artery calcification in patients with CRF not undergoing dialysis. Am J Kidney Dis. 2004, 44(6), 1024–30. [Google Scholar] [CrossRef]
- Nitta, K; Akiba, T; Suzuki, K; Uchida, K; Ogawa, T; Majima, K; et al. Assessment of coronary artery calcification in hemodialysis patients using multi-detector spiral CT scan. Hypertens Res. 2004, 27(8), 527–33. [Google Scholar] [CrossRef] [PubMed]
- Wang, XR; Zhang, JJ; Xu, XX; Wu, YG. Prevalence of coronary artery calcification and its association with mortality, cardiovascular events in patients with chronic kidney disease: a systematic review and meta-analysis. Ren Fail. 2019, 41(1), 244–56. [Google Scholar] [CrossRef] [PubMed]
- Guedeney, P; Claessen, BE; Mehran, R; Mintz, GS; Liu, M; Sorrentino, S; et al. Coronary Calcification and Long-Term Outcomes According to Drug-Eluting Stent Generation. JACC Cardiovasc Interv. 2020, 13(12), 1417–28. [Google Scholar] [CrossRef] [PubMed]
- Généreux, P; Madhavan, MV; Mintz, GS; Maehara, A; Palmerini, T; Lasalle, L; et al. Ischemic outcomes after coronary intervention of calcified vessels in acute coronary syndromes. Pooled analysis from the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) and ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) TRIALS. J Am Coll Cardiol. 2014, 63(18), 1845–54. [Google Scholar]
- Dangas, G; Iakovou, I; Nikolsky, E; Aymong, ED; Mintz, GS; Kipshidze, NN; et al. Contrast-induced nephropathy after percutaneous coronary interventions in relation to chronic kidney disease and hemodynamic variables. Am J Cardiol. 2005, 95(1), 13–9. [Google Scholar] [CrossRef]
- Saltzman, AJ; Stone, GW; Claessen, BE; Narula, A; Leon-Reyes, S; Weisz, G; et al. Long-term impact of chronic kidney disease in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention: the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) trial. JACC Cardiovasc Interv. 2011, 4(9), 1011–9. [Google Scholar]
- Appleby, CE; Ivanov, J; Lavi, S; Mackie, K; Horlick, EM; Ing, D; et al. The adverse long-term impact of renal impairment in patients undergoing percutaneous coronary intervention in the drug-eluting stent era. Circ Cardiovasc Interv. 2009, 2(4), 309–16. [Google Scholar] [CrossRef]
- Barbato, E; Carrié, D; Dardas, P; Fajadet, J; Gaul, G; Haude, M; et al. European expert consensus on rotational atherectomy. EuroIntervention 2015, 11(1), 30–6. [Google Scholar] [CrossRef]
- Jung, J; Her, S-H. Rotational Atherectomy: A to Z. J Cardiovasc Interv. 2025, 4(1), 29–39. [Google Scholar] [CrossRef]
- Matsuo, S; Imai, E; Horio, M; Yasuda, Y; Tomita, K; Nitta, K; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009, 53(6), 982–92. [Google Scholar] [CrossRef] [PubMed]
- Levine, GN; Bates, ER; Blankenship, JC; Bailey, SR; Bittl, JA; Cercek, B; et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Catheter Cardiovasc Interv. 2013, 82(4), E266–355. [Google Scholar] [CrossRef] [PubMed]
- Levine, GN; Bates, ER; Bittl, JA; Brindis, RG; Fihn, SD; Fleisher, LA; et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines: An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention, 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease, 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction, 2014 AHA/ACC Guideline for the Management of Patients With Non-ST-Elevation Acute Coronary Syndromes, and 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery. Circulation 2016, 134(10), e123–55. [Google Scholar] [PubMed]
- Moussa, ID; Klein, LW; Shah, B; Mehran, R; Mack, MJ; Brilakis, ES; et al. Consideration of a new definition of clinically relevant myocardial infarction after coronary revascularization: an expert consensus document from the Society for Cardiovascular Angiography and Interventions (SCAI). Catheter Cardiovasc Interv. 2014, 83(1), 27–36. [Google Scholar] [CrossRef]
- Liu, X; Wan, L; Wu, X; Gu, Y; Hu, L. Low Preoperative Mean Arterial Pressure as a Risk Factor for Contrast-Induced Nephropathy After Rotational Atherectomy. Rev Cardiovasc Med. 2025, 26(11), 43418. [Google Scholar] [CrossRef]
- Kumar, S; Kearney, KE; Chung, CJ; Elison, D; Steinberg, ZL; Lombardi, WL; et al. Risk of acute kidney injury after percutaneous coronary intervention with plaque modification. Cardiovasc Revasc Med. 2025, 77, 12–9. [Google Scholar] [CrossRef]
- Kawamoto, H; Latib, A; Ruparelia, N; Ielasi, A; D’Ascenzo, F; Pennacchi, M; et al. In-hospital and midterm clinical outcomes of rotational atherectomy followed by stent implantation: the ROTATE multicentre registry. EuroIntervention 2016, 12(12), 1448–56. [Google Scholar] [CrossRef]
- Crimi, G; De Marzo, V; De Marco, F; Conrotto, F; Oreglia, J; D’Ascenzo, F; et al. Acute Kidney Injury After Transcatheter Aortic Valve Replacement Mediates the Effect of Chronic Kidney Disease. J Am Heart Assoc. 2022, 11(19), e024589. [Google Scholar] [CrossRef]
- Li, SX; Patel, NK; Flannery, LD; Cigarroa, RJ; Shaqdan, AW; Erickson, P; et al. Impact of bleeding after transcatheter aortic valve replacement in patients with chronic kidney disease. Catheter Cardiovasc Interv. 2021, 97(1), E172–e8. [Google Scholar] [CrossRef]
- Demir, OM; Poletti, E; Lombardo, F; Laricchia, A; Beneduce, A; Maccagni, D; et al. Rotational atherectomy-based percutaneous coronary intervention and the risk of contrast-induced nephropathy. Minerva Cardioangiol. 2020, 68(2), 137–45. [Google Scholar] [CrossRef]
- Jubelirer, SJ. Hemostatic abnormalities in renal disease. Am J Kidney Dis. 1985, 5(5), 219–25. [Google Scholar] [CrossRef]
- Yeh, RW; Secemsky, EA; Kereiakes, DJ; Normand, SL; Gershlick, AH; Cohen, DJ; et al. Development and Validation of a Prediction Rule for Benefit and Harm of Dual Antiplatelet Therapy Beyond 1 Year After Percutaneous Coronary Intervention. Jama 2016, 315(16), 1735–49. [Google Scholar] [CrossRef]
- Costa, F; van Klaveren, D; James, S; Heg, D; Räber, L; Feres, F; et al. Derivation and validation of the predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy (PRECISE-DAPT) score: a pooled analysis of individual-patient datasets from clinical trials. Lancet 2017, 389(10073), 1025–34. [Google Scholar] [CrossRef]
- Urban, P; Mehran, R; Colleran, R; Angiolillo, DJ; Byrne, RA; Capodanno, D; et al. Defining High Bleeding Risk in Patients Undergoing Percutaneous Coronary Intervention. Circulation 2019, 140(3), 240–61. [Google Scholar] [CrossRef]
- van Geuns, RJ; Chun-Chin, C; McEntegart, MB; Merkulov, E; Kretov, E; Lesiak, M; et al. Bioabsorbable polymer drug-eluting stents with 4-month dual antiplatelet therapy versus durable polymer drug-eluting stents with 12-month dual antiplatelet therapy in patients with left main coronary artery disease: the IDEAL-LM randomised trial. EuroIntervention 2022, 17(18), 1467–76. [Google Scholar] [CrossRef]
- Chiu, JH; Bhatt, DL; Ziada, KM; Chew, DP; Whitlow, PL; Lincoff, AM; et al. Impact of female sex on outcome after percutaneous coronary intervention. Am Heart J. 2004, 148(6), 998–1002. [Google Scholar] [CrossRef]
- Lo, WJ; Chen, WJ; Lai, CH; Chen, YW; Su, CS; Chang, WC; et al. Rotablation in Patients with Advanced Renal Insufficiency through End-Stage Renal Disease: Short- and Intermediate-Term Results. J Interv Cardiol. 2022, 2022, 7884401. [Google Scholar] [CrossRef]
Figure 1.
Study population and flow chart.
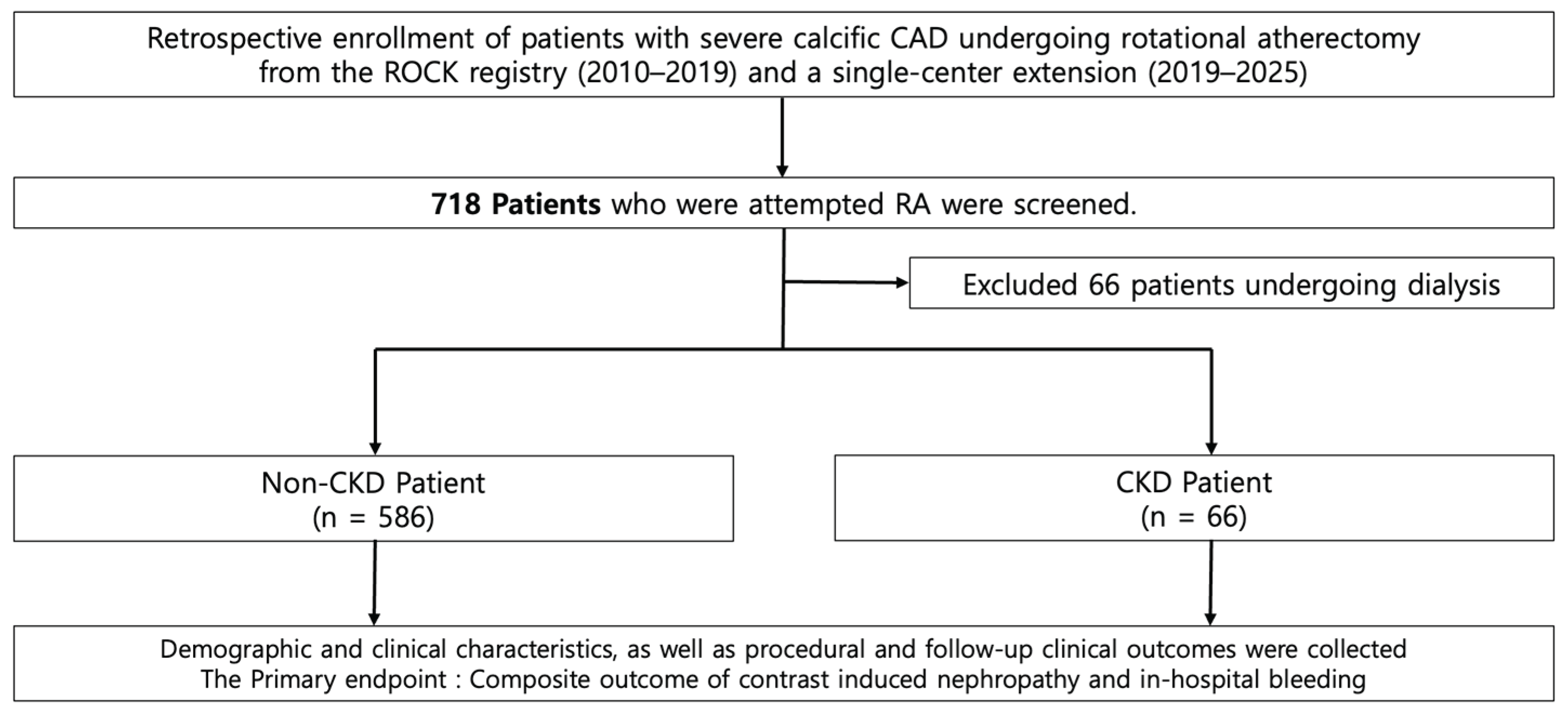
Figure 2.
Kaplan–Meier curves for secondary outcomes during the follow-up period. (A) TVF, target vessel failure; (B) CD, cardiac death; (C) MI, myocardial infarction; (D) TVMI, target vessel myocardial infarction; (E) TVR, target vessel revascularization; (F) Total bleeding.
Figure 2.
Kaplan–Meier curves for secondary outcomes during the follow-up period. (A) TVF, target vessel failure; (B) CD, cardiac death; (C) MI, myocardial infarction; (D) TVMI, target vessel myocardial infarction; (E) TVR, target vessel revascularization; (F) Total bleeding.
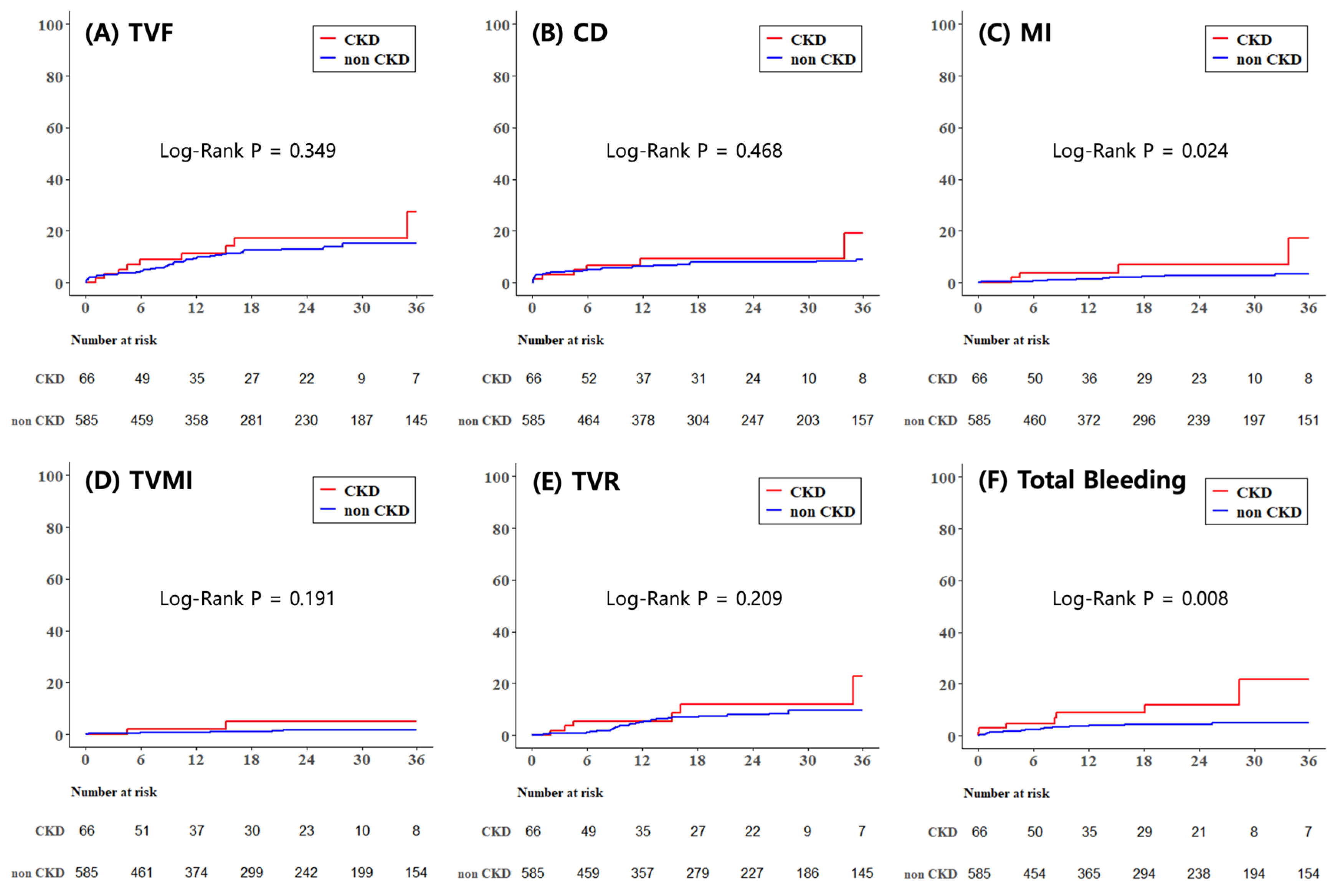
Figure 3.
Forest plot for subgroup analysis comparing the incidence of composite primary outcome between CKD and non-CKD groups.
Figure 3.
Forest plot for subgroup analysis comparing the incidence of composite primary outcome between CKD and non-CKD groups.
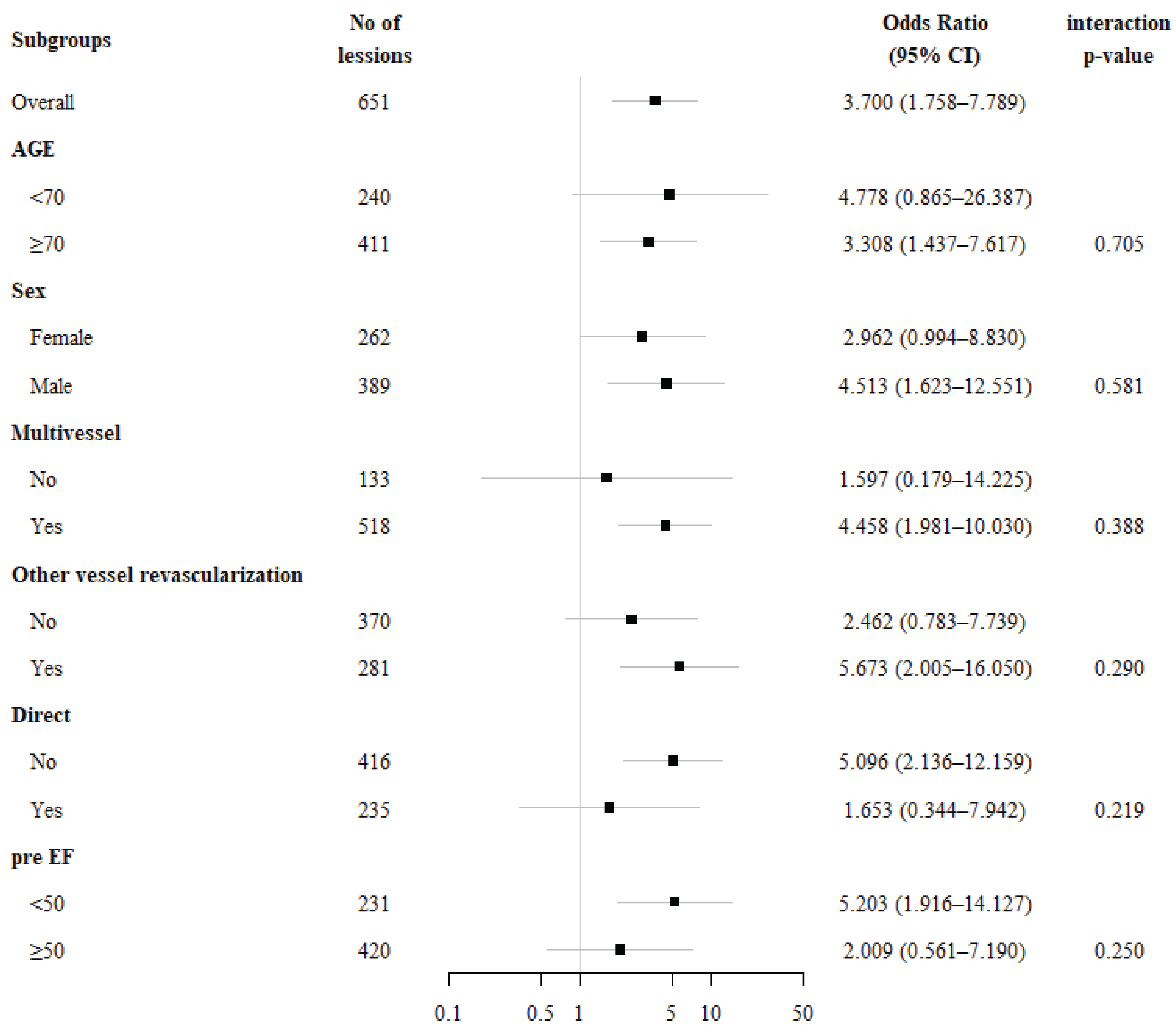

Table 1.
Baseline characteristics.
| non CKD | CKD | ||
| n = 586 | n = 66 | p-value | |
| Age | 72.0±9.6 | 74.3±8.3 | 0.069 |
| Sex | 351(60.0) | 38(57.6) | 0.703 |
| BMI | 24.2±3.9 | 24.1±3.6 | 0.874 |
| Systolic BP | 131.9±24.1 | 133.5±18.2 | 0.581 |
| Diastolic BP | 74.8±12.5 | 74.3±10.9 | 0.737 |
| Smoking | 111(19.0) | 7(10.6) | 0.094 |
| HTN | 446(76.2) | 57(86.4) | 0.063 |
| DM | 317(54.2) | 52(78.8) | <0.001 |
| Dyslipidemia | 301(51.5) | 33(50.0) | 0.823 |
| CKD (no dialysis) | 0(0.0) | 66(100.0) | <0.001 |
| LV Ejection Fraction | 54.0±12.9 | 48.4±14.0 | 0.001 |
| Medical History | |||
| PCI | 136(23.3) | 19(28.8) | 0.317 |
| CABG | 24(4.1) | 4(6.1) | 0.515 |
| MI | 64(10.9) | 9(13.6) | 0.511 |
| CVA | 93(15.9) | 10(15.2) | 0.875 |
| PVD | 38(6.5) | 14(21.2) | <0.001 |
| Chronic lung disease | 34(5.8) | 8(12.1) | 0.061 |
| Heart failure | 73(12.5) | 12(18.2) | 0.192 |
| Atrial fibrillation | 42(7.2) | 10(15.2) | 0.024 |
| Clinical_diagnosis (STEMI/NSTEMI) |
152(26.0) | 26(39.4) | 0.021 |
CKD, chronic kidney disease; BMI, body mass index; BP, blood pressure; HTN, hypertension; DM, diabetes mellitus; CKD, chronic kidney disease; LV, left ventricle; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft; MI, myocardial infarction; CVA, cerebrovascular accident; PVD, peripheral vascular disease; NSTEMI, non-ST segmental elevation myocardial infarction; STEMI, ST segmental elevation myocardial infarction.
Table 2.
Laboratory analyses and medications.
| non CKD | CKD | ||
| n = 586 | n = 66 | p-value | |
| Labaratory analyses | |||
| Hb | 12.6±2.3 | 11.1±1.8 | <0.001 |
| Platelet | 220.8±65.5 | 219.8±93.0 | 0.910 |
| Triglyceride | 119.0±74.2 | 123.1±66.0 | 0.686 |
| Total cholesterol | 146.5±40.1 | 134.6±35.3 | 0.030 |
| LDL cholesterol | 85.2±39.3 | 75.6±31.9 | 0.079 |
| HDL cholesterol | 47.1±14.7 | 40.2±14.3 | <0.001 |
| Hs-CRP | 2.6±10.6 | 2.5±6.8 | 0.971 |
| HbA1c | 6.7±1.6 | 7.4±1.5 | 0.002 |
| Medication | |||
| NOAC | 21(3.6) | 5(7.6) | 0.171 |
| DAPT | 559(95.6) | 61(92.4) | 0.230 |
| Aspirin | 571(97.6) | 62(93.9) | 0.099 |
| P2Y12_inhibitor | 574(98.1) | 66(100.0) | 0.614 |
| Cilostazol | 73(12.5) | 6(9.1) | 0.424 |
| Beta-blocker | 392(67.0) | 45(68.2) | 0.848 |
| ACEi or ARB | 377(64.4) | 39(59.1) | 0.391 |
| Statin | 552(94.4) | 62(93.9) | 0.782 |
Hb, hemoglobin; LDL, low density lipoprotein; HDL, high density lipoprotein; Hs-CRP, high sensitivity C-reactive protein; NOAC, new oral anticoagulant; DAPT, dual antiplatelet therapy; ACEI/ARB, angiotensin converting enzyme inhibitor / angiotensin II receptor blocker.
Table 3.
Lesion and procedural characteristics.
| non CKD | CKD | ||
| n = 586 | n = 66 | p-value | |
| Lesion Classification(B2/C) | 549(93.9) | 62(93.9) | >0.999 |
| Vessel disease | |||
| 1VD | 124(21.2) | 9(13.6) | 0.312 |
| 2VD | 187(32.0) | 25(37.9) | |
| 3VD | 274(46.8) | 32(48.5) | |
| Multivessel disease (MVD) | 461(78.8) | 57(86.4) | 0.149 |
| LM disease | 86(14.7) | 11(16.7) | 0.671 |
| IVUS | 303(51.8) | 37(56.1) | 0.511 |
| Direct | 211(36.1) | 24(36.4) | 0.962 |
| Other vessel revascularization | 245(41.9) | 36(54.6) | 0.049 |
| Procedural approach | |||
| Radial | 291(49.7) | 31(47.0) | 0.669 |
| Femoral | 294(50.3) | 35(53.0) | |
| Procedure success | 555(94.9) | 64(97.0) | 0.762 |
| Technical success | 562(96.1) | 66(100.0) | 0.155 |
| Contrast (mL) | 214.1±91.9 | 189.4±95.6 | 0.044 |
| Procedural time | 78.0±51.4 | 86.5±56.4 | 0.211 |
| Radiation dose | 3,811.6±3,643.3 | 4,354.1±2,684.3 | 0.574 |
| Rotational atherectomy | |||
| Size of burr (start) | 1.5±0.2 | 1.5±0.2 | 0.951 |
| Size of burr (max) | 1.5±0.6 | 1.5±0.2 | 0.795 |
| Number of burr | 1.2±0.4 | 1.2±0.5 | 0.991 |
| Stent | |||
| Stent diameter | 3.0±0.4 | 3.0±0.3 | 0.384 |
| Total number of stent | 2.5±1.3 | 2.6±1.3 | 0.377 |
| Total length of stent | 69.6±37.7 | 74.3±38.4 | 0.343 |
| Peri-procedural complication | |||
| Coronary dissection | 192(32.8) | 19(28.8) | 0.507 |
| Coronary perforation | 21(3.6) | 2(3.0) | >0.999 |
| Urgent intervention for tamponade | 3(0.5) | 0(0.0) | >0.999 |
| Temporary pacemaker | 39(6.7) | 6(9.1) | 0.442 |
| Periprocedural MI | 54(9.2) | 10(15.2) | 0.126 |
| Inhospital outcome | |||
| Inhospital death | 18(3.1) | 2(3.0) | >0.999 |
| Inhospital CVA | 2(0.3) | 0(0.0) | >0.999 |
| Urgent CABG | 2(0.3) | 0(0.0) | >0.999 |
| Urgent PCI | 5(0.9) | 1(1.5) | 0.475 |
LM, left main; IVUS, intravascular ultrasound sonography; MI, myocardial infarction; CVA, cerebrovascular accident; CABG, coronary artery bypass graft; PCI, percutaneous coronary intervention.
Table 4.
Clinical outcomes (Primary and Secondary outcomes).
| non CKD | CKD | univariate | multivariate | |||||||||
| Primary outcome | n = 586 | n = 66 | p-value | OR | 95%CI (lower – upper) |
p-value | OR | 95%CI (lower – upper) |
p-value | |||
| Composite | 30(5.1) | 11(16.7) | 0.001 | 3.700 | 1.758 | 7.789 | <0.001 | 3.019 | 1.363 | 6.685 | 0.006 | |
| CIN | 10(1.7) | 10(15.2) | <0.001 | 10.269 | 4.099 | 25.727 | <0.001 | 7.184 | 2.324 | 22.210 | <0.001 | |
| In-hospital bleeding | 21(3.6) | 2(3.0) | >0.999 | 0.839 | 0.192 | 3.662 | 0.816 | 0.779 | 0.170 | 3.565 | 0.747 | |
| Secondary outcome (3-year outcome) |
n = 586 | n = 66 | p-value | Log-rank p-value |
HR | 95%CI (lower – upper) |
p-value | HR | 95%CI (lower – upper) |
p-value | ||
| TVF | 63(10.8) | 9(13.6) | 0.481 | 0.349 | 1.395 | 0.693 | 2.807 | 0.351 | 1.317 | 0.639 | 2.715 | 0.456 |
| AD | 55(9.4) | 9(13.6) | 0.273 | 0.210 | 1.565 | 0.772 | 3.171 | 0.214 | 1.326 | 0.641 | 2.743 | 0.447 |
| CD | 41(7.0) | 6(9.1) | 0.461 | 0.468 | 1.373 | 0.582 | 3.236 | 0.469 | 1.260 | 0.522 | 3.043 | 0.607 |
| MI | 12(2.1) | 4(6.1) | 0.069 | 0.024 | 3.417 | 1.097 | 10.645 | 0.034 | 3.975 | 1.155 | 13.683 | 0.029 |
| TVMI | 7(1.2) | 2(3.0) | 0.229 | 0.191 | 2.735 | 0.568 | 13.175 | 0.210 | 3.904 | 0.616 | 24.735 | 0.148 |
| RR | 50(8.6) | 6(9.1) | 0.881 | 0.723 | 1.165 | 0.499 | 2.719 | 0.724 | 0.933 | 0.390 | 2.233 | 0.876 |
| TVR | 35(6.0) | 6(9.1) | 0.291 | 0.209 | 1.733 | 0.727 | 4.128 | 0.215 | 1.459 | 0.590 | 3.611 | 0.414 |
| TLR | 31(5.3) | 4(6.1) | 0.772 | 0.632 | 1.289 | 0.454 | 3.660 | 0.633 | 1.091 | 0.370 | 3.216 | 0.875 |
| NLR | 25(4.3) | 3(4.6) | 0.756 | 0.756 | 1.209 | 0.365 | 4.010 | 0.756 | 1.149 | 0.333 | 3.971 | 0.826 |
| CVA | 8(1.4) | 3(4.6) | 0.091 | 0.054 | 3.419 | 0.906 | 12.913 | 0.070 | 3.296 | 0.820 | 13.250 | 0.093 |
| ST | 5(0.9) | 1(1.5) | 0.475 | 0.603 | 1.756 | 0.205 | 15.028 | 0.607 | 1.731 | 0.179 | 16.745 | 0.635 |
| Total bleeding | 23(3.9) | 7(10.6) | 0.025 | 0.008 | 2.983 | 1.275 | 6.978 | 0.012 | 3.392 | 1.374 | 8.370 | 0.008 |
| Minor bleeding | 9(1.5) | 5(7.6) | 0.009 | <0.001 | 5.776 | 1.918 | 17.396 | 0.002 | 7.798 | 2.282 | 26.646 | 0.001 |
| Major bleeding | 9(1.5) | 1(1.5) | >0.999 | 0.940 | 1.082 | 0.137 | 8.577 | 0.940 | 1.336 | 0.151 | 11.854 | 0.795 |
CIN, contrast induced nephropathy; TVF, target-vessel failure; AD, all-cause death; CD, cardiac death; MI, myocardial infarction; TVMI, target-vessel spontaneous MI; RR, repeat revascularization; TVR, target-vessel revascularization; TLR, target-lesion revascularization; NLR, neutrophil to lymphocyte ratio; CVA, cerebrovascular accident; ST, stent thrombosis. TVF is defined as composite of CD, TVMI, TVR.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



