Submitted:
26 February 2026
Posted:
27 February 2026
You are already at the latest version
Abstract
Purpose: Physical activity levels tend to be lower in Parkinson’s disease (PD) than in healthy age-matched controls, largely because of substantial gait impairment. Remarkably, individuals with PD often retain a remarkable ability to cycle. However, so far, no evidence exists regarding the safety of patients when cycling outdoors in daily life. Therefore, the aim of this review is threefold: 1) to compare the mechanisms of cycling to those of walking, 2) to examine the symptomatic effects of stationary cycling, and 3) to highlight the challenges and opportunities to ensure safe outdoor cycling in PD.Major findings: Compared to walking, making cycling movements likely engages alternative neural circuits that largely bypass the most affected parts of the striatum in PD. Stationary cycling programs are therefore feasible and consistently improve physical fitness and motor symptom severity. Outdoor cycling may further increase physical activity levels, social participation and mobility in PD. However, its feasibility and safety are poorly studied, while there exist significant safety concerns linked primarily to poor balance, but also axial rotation, motor initiation and cognitive impairments. The present review discusses these challenges and considers which may be modifiable through future cycling-rehabilitation interventions.Conclusion: The relatively preserved ability to make cycling movements in PD makes outdoor cycling an attractive form of physical activity and promising strategy to enhance quality of life. However, further research is needed to assess outdoor cycling skills and inform rehabilitation interventions to ensure safe participation in a population for whom maintaining physical activity is essential.
Keywords:
Parkinson’s disease
; cycling
; bicycling
; rehabilitation
; physical activity
; exercise
; neurophysiology
Introduction
Parkinson’s disease (PD) is the second-most common neurodegenerative disorder worldwide[1]. It has a progressive disease course that leads to worsening motor and non-motor symptoms and causes significant burden to patients, their families and society[1,2,3]. The pathophysiology of PD is mainly characterized by the progressive degeneration of dopaminergic neurons in the substantia nigra pars compacta. The resulting dopaminergic denervation affects basal ganglia processing, especially in the sensorimotor striatum, which is associated with increased motor inhibition and impaired automaticity of motor performance[1,4,5]. The cardinal signs of PD include bradykinesia, muscle rigidity and resting tremor, but are also expressed in complex motor signs, such as reduced trunk mobility, postural instability and gait impairment[1,4,6]. To compensate for de-automaticity, PD patients become increasingly reliant on sensory (visual, parietal) and attentional (prefrontal) circuits to facilitate goal-directed motor control[4,5,7]. This explains why during performance of a dual-task the competition between compensatory circuits may be increased, further compromising motor performance[4,5,7]. Inevitably, and with time, both the basal ganglia and the compensatory circuits become increasingly affected causing severe motor and non-motor disability[8] and functional dependence[9].
The primary therapy of PD aims to reduce motor inhibition through dopamine-replacement pharmacotherapy or deep brain stimulation, the latter most often applied to the subthalamic nucleus (STN)[6,8]. Despite strong symptomatic effects[6,8,10], gait impairments are among the most disabling refractory symptoms, significantly affecting daily life mobility[10]. Physical therapy has been shown an effective adjunct strategy to help patients manage their activities of daily living and to keep them mobile and independent for as long as possible[11,12]. Besides motor learning and exercise, one of the critical components of physical therapy comprises of promoting everyday physical activity, defined by any bodily movement produced by skeletal muscles that results in energy expentditure[13] and this in the most safe manner possible[14].
A recent qualitative study identified everyday mobility as an important treatment target for patients with PD[15]. However, in the later stages, mobility becomes severe restricted by gait impairment and freezing of gait (FOG), putting patients at a higher risk of falls [8,16]. Hence, considering other forms of physical activity and exercise than those involving walking seems indicated. Cycling lends itself particularly well as an alternative[17,18,19]. More and more nations are increasing their cycling infrastructure. Cycling is indeed a sustainable and healthy form of mobility and transport that is key for social inclusion and economic development, as postulated by the European declaration on cycling[20,21,22,23]. What is more, the portion of older adults that adopt outdoor cycling has risen substantially since the introduction of electronically-supported bicycles[24]. However, little is known about the difficulties PD patients experience when cycling outdoor without clinical supervision. In this position paper, we therefore address 3 critical aims. First, we describe the mechanisms underlying cycling and present conceptual evidence for why severely affected patients may still be able to cycle[25]. Second, we synthesize the effects of controlled cycling exercises in PD. Third, we critically reflect on the barriers for safe cycling in uncontrolled environments and whether outdoor cycling could feasibly serve as an alternative form of physical activity in PD. Finally, we provide future research directions to promote safe cycling in PD patients’ daily life.
1) Underlying mechanisms of cycling and why people with PD may cycle better than walking.
Several studies have explored the neurophysiological and biomechanical mechanisms underlying cycling following the observation that individuals with PD often experience less motor impairments during cycling movements compared to walking[25]. Although we do not yet have a precise understanding of this phenomenon, multiple plausible and non-exclusive hypotheses have been proposed, each focused on the rotational cycling movements that may engage neural pathways or motor control strategies that are less affected by PD than those controlling gait. However, other differences should also be considered when comparing walking and cycling outdoors.
i) Walking versus rotational cycling movements
Several theories have been put forward to explain the compelling evidence that PD patients have a preserved ability to perform rotational cycling movements in the face of severe gait impairment[25,26,27,28]. A first possible explanation relates to the degree of automaticity. Activities of daily living range from highly automated (i.e. habitual) to more goal-directed actions, depending on the context and need for motor precision[4]. Habitual motor patterns, such as walking, are performed frequently in everyday life from an early age and therefore become highly automated, whereas cycling is typically learned later in development and practiced with a lower frequency, possibly resulting in a lower degree of automatization. Figure 1 presents some of the hypothesized differences between walking and cycling movements in people with and without PD. In healthy people, motor automatization is associated with a shift in neural activation from the anterior associative fronto-striatal circuit to the posterior sensorimotor striatum[4,5], along with reduced attentional cortical demands[4,17]. Simultaneously, neural connectivity increases between the sensorimotor striatum and key components of the motor circuit, including the primary motor cortex (M1), central pattern generators, and the cerebellum, leading to efficient motor execution when precision is less critical, such as in walking (see figure 1, upper left)[4]. In people with PD, the sensorimotor striatum is more severely affected than the anterior striatum, explaining why automated movements are particularly disrupted in PD, and why patients revert to a goal-directed mode of gait control visualized by the bold black lines in Figure 1 (lower left)[4,5]. Cycling movements, considered to be less automated than walking[25], rely more on relatively spared associative neural circuits for goal-directed motor control, even in healthy individuals (Figure 1, upper right)[4,5]. The use of these alternative pathways may underlie the relative preservation of cycling ability in PD (Figure 1, lower right)[25], albeit that this circuit may be over-relied upon (bold arrows) in the PD population.
Storzer et al. (2017) were the first to demonstrate that pathological beta-power in the Subthalamic Nucleus (STN) is significantly attenuated during cycling movements compared to over-ground walking[27], which may indicate that there is less pathological signaling to the STN during cycling (see also Box 1). Bougou et al. (2023) found a similar suppression of beta-activity through local field potential recording in the STN, but only compared active versus passive cycling. Interestingly, low frequency beta was most predominantly suppressed during passive cycling, and particularly in people with PD and FOG. These finding suggest that the somatosensory input of lower limb movements play a key compensatory role during cycling[28].
Box 1: Beta-band oscillatory activity
The primary pathophysiology of motor function in PD has been associated with over-activity in the indirect cortico-striatal-thalamo-cortical loop of the sensorimotor striatum leading to an over-inhibition of the striatal output structures and brainstem locomotor centers[29]. This over-inhibition has also been associated with alterations in beta-band oscillatory neural activity. Under physiological conditions, beta-oscillations help suppress unwanted movements and competing motor programs[30]. When a voluntary movement is initiated, beta power selectively decreases, thereby restricting the inhibitory striatal output and allowing selective movement generation. As such, beta-activity functions as both a neural “handbrake” by limiting unnecessary actions, and a funnel by appropriately initiating intended motor action[27,30]. Excessive and prolonged beta oscillations within the cortico-basal ganglia circuits, particularly in the STN and Globus Pallidus internus (GPi) correlate with bradykinesia, and gait impairment[26,27,30]. A lowering of beta activation as seen during cycling movements is therefore typically interpreted as a favorable outcome in PD[27,28].
It has further been suggested that the pedals of a bicycle act as external tactile cues and also facilitate goal-directed motor control[25]. Cues are external or internal stimuli to direct attention towards the execution of a specific movement[31]. Cueing has been extensively documented as an effective approach to temporarily improve movement initiation and execution in PD, alleviating gait impairments and FOG in particular[31,32,33,34,35]. We propose that bike pedals may serve as external cues in two distinct ways. First, for the pushing leg, the pedal may function as a proprioceptive target to guide foot placement and force direction. Second, for the non-pushing leg, the passive motion of the pedal may facilitate advancement through the movement cycle. Subsequently, the upward force generated beneath this foot may serve as ‘guidance’ to push the opposite pedal[25], thereby enabling movement continuation. As such, bradykinesia is counteracted during cycling and, on a moving bike, this will still contribute to meaningful forward progression.
Although gait patterns in themselves are run automatically[36], actual overground walking in daily life requires constant sensorimotor feedback to navigate and adapt gait parameters in an ever-changing environment with constant gravitational pertubations[37,38]. This imposes substantial load on the motor and cognitive circuits, as well as, requiring basal ganglia involvement, explaining why gait impairments are so prominent in PD[39,40,41]. Given the more constrained movement pattern of rotational cycling movements, these demands are likely to be lower[25]. During cycling, the feet remain fixed on the pedals and move along a fixed path length. Coordination between the pushing and non-pushing leg is also predetermined, occurring in a 360° phasic motion with a 180° delay between the legs. Gravitational perturbations are probably less prominent when seated in the absence of a swing phase[42,43]. Thus, cycling reduces the degrees of freedom and lowers the need for sensorimotor feedback. Rotational cycling movements are also substantially governed by feedforward movement generation[25](see Box 2), relying on predictive motor commands present at movement initiation, rather than by on-line adaptation. Feedforward control is mainly coordinated by the cortico-cerebellar circuit[39,44], which remains relatively intact in PD[39,45].
Box 2: Feedback versus feed-forward motor control
A feedback-regulated movement depends on afferent somatosensory input originating from internal and peripheral receptors, such as Golgi tendon organs and muscle spindles[38]. First, a motor plan is generated and executed in order to produce the intended movement. The somatosensory organs will continuously provide afferent information – reflecting both internal bodily state and external environmental conditions – of the performed movement to the central nervous system. The basal ganglia are involved in selecting, modulating and fine-tuning the motor responses whereafter the outcome is projected to the motor cortex[39,41,45]. Based on the incoming information, the motor system will refine subsequent motor commands to further optimize the next movement[37,38]. In PD, feedback -based processing is mostly affected, leaving a negative imprint on movement adaptation[37,39,40,41,45,46]. Feedforward movements, supported by consistent and predictable movement patterns, are primarily processed through cerebellar-thalamic pathways. In PD, these circuits remain relatively spared[25,39]. Because rotational cycling movements rely more on feedforward control than gait does, it may remain spared even in patients with severe gait impairments, including those experiencing FOG[25].
ii) Balance control differences between walking and cycling outdoors
A key distinction between walking and cycling outdoors relates to the mode of balance control. Walking predominantly relies on anterior-posterior balance control[47]. In contrast, cycling depends largely on mediolateral balance control, which is affected to a lesser degree in PD[25]. What is more, during walking, balance control is largely dependent on step width modulation in the same effectors that also produce the forward stepping motion (i.e. the legs). This regulation is impaired in PD, who typically adopt a maladaptive narrow base of support that increases risk for falls[48]. On the contrary, whilst the forward motion during cycling is also produced by the legs, balance control is regulated mainly by the upper body effectors through leaning and steering. This might allow PD patients to utilize different or more distributed neural circuits, thereby putting less strain on the already impaired control of the lower limbs. What is more, walking requires constant anticipatory postural adjustments (APA’s), i.e., multidirectional weight shifts that underpin appropriate loading and unloading of the legs. Individuals with PD experience abnormally small APA’s, leading to impairments in both gait initiation and continuation[49,50,51]. The rhythmic leg motions and upper-body balance corrections during cycling similarly demand a degree of APA’s to ensure that he body remains balanced on the bicycle frame during movement[25]. However, the mechanical support of the frame and rotational movement of the pedals is likely to facilitate such mediolateral APA’s and allow for greater gravitational control, also in PD[52]. Furthermore, turning during cycling is initiated by steering and leaning without requiring an asymmetric stepping pattern, known to worsen FOG and falls in PD[53,54,55]. Overall, current evidence indicates that several complementary mechanisms may underlie the relative preservation of cycling ability in people with PD.
Symptomatic Effects of Stationary Cycling Exercise in PD
The rationale to recommend cycling for PD is corroborated by converging evidence that cycling exercises result in symptomatic benefits. Unlike physical activity, exercise is defined as planned, structured and repetitive motor practice with a final or intermediate objective to improve or maintain specific outcomes of physical or mental fitness[13]. Mostly based on in-vivo animal studies, and to a lesser degree supported by human work in PD, exercise has been shown to stimulate neuroprotective mechanisms, as derived from brain-derived neurotrophic factor (BDNF), dendritic spine formation and metabolic pathway optimization for striatal dopamine release[56,57,58,59,60]. Exercise has also been demonstrated to induce neurostructural changes and strengthened connectivity between cortico-striatal networks, thought to support the slowing of disease progression[61,62]. However, the precise role of exercise as a potential disease modifier is still under ongoing investigation[63]. So far, aerobic exercise has shown the strongest potential to slow down motor symptom progression[60,61,64]. Various other exercise programs have been found to acutely improve aerobic capacity and muscular strength[60,61,65], motor symptoms[58,60,61,65] and generally enhancing the body’s resilience and ability to compensate[60,61]. Hence, exercise has now become integrated into overall disease management.
Cycling on a stationary indoor bicycle is a popular exercise mode for PD, because of the seated stationary position that results in a low risk of falling. Indeed, indoor bicycles typically provide robust structural support and stability during mounting, dismounting and exercising, offering a means for safe home-based interventions too, whereby training parameters (e.g. speed, resistance, training duration) can be carefully controlled through therapist supervision or mobile health (M-health) technology[66]. A systematic review by Tiihonen et al. (2021) revealed consistent positive effects of indoor cycling on motor symptom severity, self-reported quality of life[67] and reduced symptom progression after 6 months[64,68]. Alberts et al. (2025, ClinicalTrials.gov ID: NCT04000360)[19] published a study protocol, which is investigating the impact of a 12-month cycling exercise program (the CYCLE-II study) on symptom progression based on the OFF-medication MDS-UPDRS III score[69] compared with usual care. Unpublished trial data indicate a mean change of -1.4 points in the cycling group versus +3.6 points in controls, suggesting a clinically meaningful benefit is likely[19]. The program was also safe and feasible with adherence exceeding 87% and few reports of serious (10/129), and non-serious (27/129) adverse events in the cycling group[70].
The scoping review of Palmieri et al. (2024)[71] further highlighted that positive effects of stationary cycling may translate to other activities, even if inconsistently, as one well-controlled RCT did not show any transfer[64]. Generally, clinically meaningful improvements of gait parameters were reported in 69% of the reviewed studies, while 60% demonstrated statistically significant improvements in balance-related outcomes which, however, did not surpass the corresponding minimal detectable change thresholds. Of note, a 6-week backwards cycling program resulted in transferable improvements in backward walking speed, backward reactive balance and overall postural stability[72]. The potential for transfer of cycling-related benefits may be attributable to the fact that individuals with low baseline physical fitness profiles[71] are particularly responsive to any form of exercise. In such individuals, even moderate increases in physical capacity can yield meaningful improvements in functional abilities, including walking[71]. Collectively, these findings indicate that stationary cycling-based exercise programs are safe, feasible, and effective within the broader menu of evidence-based rehabilitation option for people with PD.
Outdoor Cycling Challenges as Alternative form of Physical Activity?
Regular physical activity is linked to broad health benefits[73], which have likewise been observed in the PD population as along with improvements in gait, postural stability and cognitive functioning[14,74]. However, gait disturbances also form a major barrier for engaging in physical activity, as they put patients at a higher risk for falls[75]. Consequently, patients tend to adopt a sedentary lifestyle[76,77], setting off a detrimental spiral of secondary complications, and eventually increasing morbidity[14,78]. To counteract this vicious cycle, cycling can serve as a viable exercise modality, but also as a means to increase daily physical activity when used for transportation or recreation. Recreational cycling enables individuals to travel longer distances, enjoy natural environments, and participate more fully in community life, for example, by visiting family and friends and running routine errands, such as going to the bakery or grocery store. Through cycling, people with PD can substantially expand their social mobility, while simultaneously benefiting from regular physical activity. Moreover, cycling can be preserved in people with severe gait impairment, as illustrated by the video-supported case report of Snijders and Bloem (2011) displaying a gentleman with severe freezing but who could still ride a bicycle (figure 2)[25].
On the down side, outdoor cycling comes with its own risks and difficulties. First and foremost, compared to walking at a slow pace, a fall or collision at a higher speed may give rise to more severe consequences, such as bleeds, fractures, concussions and worse. Besides an advice to wear a safety helmet75, patients must be able to safely execute cycling-specific tasks when navigating in traffic to avoid falls and accidents. This is not self-evident, as outdoor cycling introduces multiple challenges for people with PD. Some of these challenges are evident in the previously referenced case-report video.
Figure 2 displays six screenshots taken from the video illustrating the various egocentric difficulties. First, the initiation of the first cycling movements can be challenging (Figure 2A: note, the pushing of two people to advance the bike). Poor initiation of movement is a hallmark of PD that can be made worse by freezing[49,51,55]. Second, the patient does not fully look over his shoulder (Figure 2B). This might be the result of axial rigidity and poor axial rotation[79,80,81]. The shoulder check serves as a preparatory action for successive traffic maneuvers to determine whether it is safe to proceed and is therefore crucial for navigation in real-world traffic. Figure 2C shows difficulty with making tight turns within the border of a double-laned street, deviating into the parking space of cars. Making exaggerated wide turns may indicate deficits in balance[16,82], turning mobility and axial rotational control, known to be affected in PD[79,80]. It may increase fall and collision risks during public cycling. Figure 2D shows difficulty with making sharp-angled maneuvers and a near collision with a parked car. In figure 2E, the patient swiftly hops off the bike by jumping from the pedals. Intentionally or not, it could indicate a compensatory strategy to overcome difficulties with controlled disembarking.
After dismounting, the participant walks while holding the bicycle, but is restricted because of FOG (Figure 2F). Walking while maneuvering an object is a motor dual task with high balance requirement and a known trigger of FOG[4,5].The same difficulty is shown in another case video by the same group[83]. During traffic, prior to turning one should put out an arm to signal the intended travel direction. The gentleman in the video does not perform this maneuver. Such an action requires mediolateral balance control and single-handed steering, which the patient may have avoided as well.
Figure 3 provides an overview of envisioned difficulties that people with PD may experience with handling a bicycle, including some of those shown in figure 2. The mechanisms that can possibly explain the depicted difficulties are indicated in writing under each subfigure. Figure 3A represents various egocentric problems that likely challenge people with PD given their dual-tasking, balance, transfer, axial rigidity, and motor initiation, some of which (Figure3A: panels 1-6) were also identified in the video of Snijders[25]. The other difficulties depicted include upper-limb motor skills needed for using the breaks and (un)locking a bike (panel 7)[84]; parking a bike on a kickstand involving unipedal balancing and unracking and unparking a bike, demanding retropulsion, a common difficulty in PD (panel 8)[85]; and recalling one’s route, which requires spatial memory (panel 9)[86]. As for allocentric difficulties, figure 3B shows that navigating through traffic is likely to be challenging in the face of reduced cognitive ability and cognitive-motor dual tasking in PD[87,88]. Cycling outdoors indeed requires faster visual scanning of the environment and spatial awareness compared to walking. In conjunction, there is also a great demand on executive functioning to correctly apply the traffic rules, pay attention to other road-users and pedestrians, adapt one’s movements and behavior to an ever-changing environment, and generate responses timely for (emergency) breaking (Figure 3B). Finally, figure 3C shows the primary concerns of outdoor cycling, namely the risk of falling, suffering an accident and the ensuing demotivation to engage in cycling. In conclusion, although cycling may offer a valuable form of physical activity in PD, safety remains the most important challenge.
Gaps and Future Directions
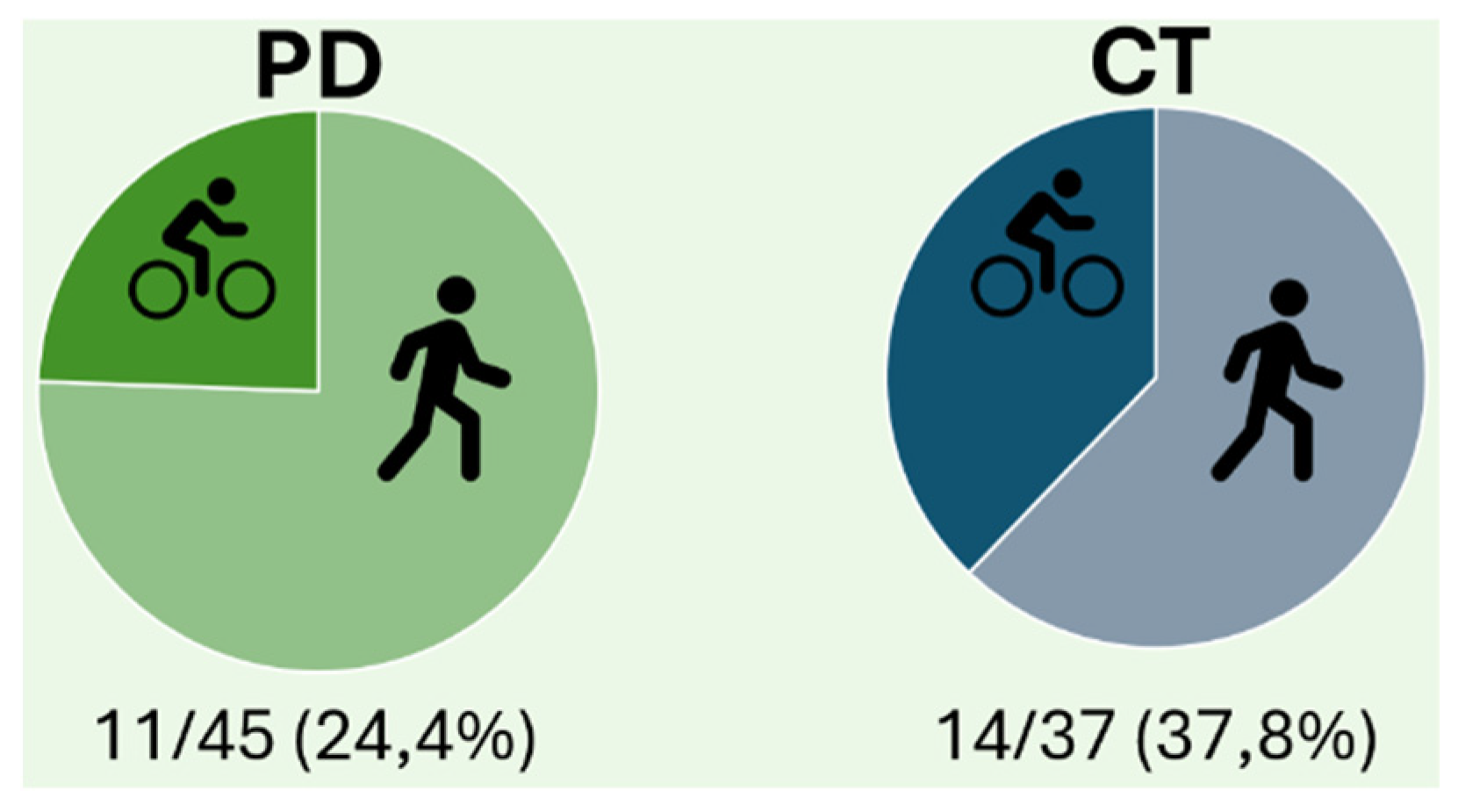
In some countries, such as Belgium and The Netherlands, cycling is integrated in everyday life and cycling paths are widely available. However, even in these ‘cycling nations’, there are no studies on cycling uptake in people with PD specifically. A retrospective evaluation of spontaneous physical activity and exercise as reported on a diary as part of another study[89] in our group, showed that only one in four patients with mild-to-moderate PD cycled outdoor on a weekly basis, which was slightly lower than in healthy older adults living in the same area of Flanders, albeit not statistically significant (see Figure 4). Moreover, a recent survey (G-sport Vlaanderen (2024) of the Flanders regional sport association for persons with a disability[90] indicated that only 54% of people with chronic disease are weekly active. Within this group, seven out of 15 persons with PD reported to participate in weekly physical activity. Interestingly, cycling was listed as the fourth most popular sport in this group, after walking, swimming, and strength exercises.
This begs the question of how can we promote safe cycling in PD? First, the most important motivators and barriers for engaging in cycling must be identified. Next, a training program teaching cycling skills should be developed to enhance road safety and confidence. Multiple studies[91,92,93] already identified a diverse set of motivators and barriers to engage in physical activity and exercise in PD. Barriers included: 1) PD-symptoms and their resulting discomforts, 2) low baseline activity levels, 3) personal factors such as limited self-efficacy, fear of falling, depressive mood or lack of time, and 4) environmental obstacles (insufficient social support, unfavorable weather conditions, poor accessibility and financial burden). Factors that helped engagement were: 1) the perceived health benefits of exercise especially when indicated by health-care professionals, 2) tailoring an exercise program to the individual’s schedule, 3) education about exercise and 4) providing adequate feedback and reward. However, it remains unclear whether the same barriers and motivators apply to outdoor cycling. As for feedback and reward, mobile health (Mhealth) technology emerges as a valuable adjunct for optimizing adherence to exercise through monitoring tools, motivational features and low-threshold goal-setting strategies[91]. Future research should evaluate if Mhealth technology also benefits adherence to and clinical effectiveness of cycling interventions.
In this opinion paper, we identified important gaps in the literature to determine the exact difficulties that patients experience during real-life cycling. More specifically, which cycling tasks are particularly impaired in PD compared to their healthy peers? This understanding will aid in informing future training programs for increasing cycling skills.
Earlier, we espoused that the lack of balance, strength, cognition and fear of falling may impact on cycling proficiency. Equally, external factors, such as the amount of daylight, the weather, the bike type (e-bike versus conventional) and the bike’s size and weight, could also be important. Finally, intrinsic factors, including previous cycling experience and the person’s general agility and speed[94], could be important determinants of cycling ability. Adaptive forms of cycling can also be considered. While, two-wheeled bicycles are agile and appropriate for patients in the early to mid-stages, tricycles may be better suited for the later stages when balance control becomes markedly impaired. Tandem bicycles can also be considered given the potential benefits of (semi-)passive cycling movements. More research is needed to inform and advise patients and healthcare providers appropriately about which bike is best, as well as, on when to discourage cycling in traffic in the light of motor and cognitive deficits.
At present, we are conducting a cross-sectional observational study, the so-called MaestroPD study, to address some of these knowledge gaps (MaestroPD-preregistration)[95]. Using a standardized outdoor assessment, we will compare cycling skills between PD and healthy older adults during different cycling-specific tasks. Performance outcomes will be evaluated based on inertial measurement units and video footage of the bike’s and the cyclist’s movements. In the second phase of the study, we will be able to evaluate which clinical and personal determinants of the participants predict better outdoor cycling performance. Lastly, cycling-specific motivators and barriers will be rated through qualitative analysis of a population-wide survey to identify the key elements that could be addressed in future training programs and outdoor cycling promotion materials.
Conclusion
Given the relative preserved ability to perform rotational cycling movements in PD, it seems compelling to recommend outdoor cycling as an alternative form of physical activity. However, in contrast to the extensive gait-oriented literature, much less is known about outdoor cycling performance and safety in PD, despite the many anticipated challenges. These knowledge gaps must now be addressed to inform the development of cycling-specific rehabilitation programs and to optimize safe and sustainable cycling uptake in people with PD.
Author contributions
TM: main author, AN: Review, FDG: co-supervision, JJODX: co-supervision, MG. main supervisor.
Funding statements
This work was supported by an internal fund of KU Leuven (C+ 24014, “MAESTRO-PD”).
Data availability
Not applicable
Acknowledgements
The authors thank Heleen Deboutte for co-creating the figures.
Statements and declarations
Ethical considerations: There are no human participants in this article and informed consent is not required., Consent for publication: written consent was obtained from NEJM for reusing images of the cycling participant originating from the article of Snijders et al. (2011)., Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Kalia L V., Lang AE. Parkinson’s disease. Lancet 2015; 386: 896–912.
- Dorsey ER, Sherer T, Okun MS, et al. The Emerging Evidence of the Parkinson Pandemic. J Parkinsons Dis 2018; 8: S3–S8.
- Wang S, Che Y, Lin Y, et al. Epidemiology of Parkinson’s disease – Global burden of disease research from 1990 to 2021 and future trend predictions. Clin Park Relat Disord 2026; 14: 100421.
- Wu T, Hallett M, Chan P. Motor automaticity in Parkinson’s disease. Neurobiol Dis 2015; 82: 226–234.
- Gilat M, Bell PT, Ehgoetz Martens KA, et al. Dopamine depletion impairs gait automaticity by altering cortico-striatal and cerebellar processing in Parkinson’s disease. Neuroimage 2017; 152: 207–220.
- Bloem BR, Okun MS, Klein C. Parkinson’s disease. The Lancet 2021; 397: 2284–2303.
- Redgrave P, Rodriguez M, Smith Y, et al. Goal-directed and habitual control in the basal ganglia: implications for Parkinson’s disease. Nat Rev Neurosci 2010; 11: 760–772.
- Tosserams A, Fasano A, Gilat M, et al. Management of freezing of gait — mechanism-based practical recommendations. Nature Reviews Neurology 2025 21:6 2025; 21: 327–344.
- Hassan A, Wu SS, Schmidt P, et al. The Profile of Long-term Parkinson’s Disease Survivors with 20 Years of Disease Duration and Beyond. J Parkinsons Dis 2015; 5: 313–319.
- Mirelman A, Bonato P, Camicioli R, et al. Gait impairments in Parkinson’s disease. Lancet Neurol 2019; 18: 697–708.
- Radder DLM, Lígia Silva de Lima A, Domingos J, et al. Physiotherapy in Parkinson’s Disease: A Meta-Analysis of Present Treatment Modalities. Neurorehabil Neural Repair 2020; 34: 871–880.
- Osborne JA, Botkin R, Colon-Semenza C, et al. Physical Therapist Management of Parkinson Disease: A Clinical Practice Guideline From the American Physical Therapy Association. Phys Ther; 102. Epub ahead of print 1 April 2022. [CrossRef]
- Caspersen C, Powell K, Gregory C. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Reports 1985; 100: 126.
- Speelman AD, Van De Warrenburg BP, Van Nimwegen M, et al. How might physical activity benefit patients with Parkinson disease? Nat Rev Neurol 2011; 7: 528–534.
- Mammen JR, Tyo M, Cadorette J, et al. Understanding what aspects of Parkinson’s disease matter most to patients and families. Scientific Reports 2024 14:1 2024; 14: 21171-.
- Hulbert S, Chivers-Seymour K, Summers R, et al. ‘PDSAFE’ - a multi-dimensional model of falls-rehabilitation for people with Parkinson’s. A mixed methods analysis of therapists’ delivery and experience. Physiotherapy 2021; 110: 77–84.
- Linder SM, Baron E, Learman K, et al. An 8-week aerobic cycling intervention elicits improved gait velocity and biomechanics in persons with Parkinson’s disease. Gait Posture 2022; 98: 313–315.
- Rosenfeldt AB, Koop MM, Penko AL, et al. Components of a successful community-based exercise program for individuals with Parkinson’s disease: Results from a participant survey. Complement Ther Med; 70. Epub ahead of print 1 November 2022. [CrossRef]
- Alberts JL, Rosenfeldt AB, Lopez-Lennon C, et al. Effectiveness of a Long-Term, Home-Based Aerobic Exercise Intervention on Slowing the Progression of Parkinson Disease: Design of the Cyclical Lower Extremity Exercise for Parkinson Disease II (CYCLE-II) Study. Phys Ther; 101. Epub ahead of print 1 November 2021. [CrossRef]
- Makahleh HY, Taamneh MM, Dissanayake D. Promoting Sustainable Transport: A Systematic Review of Walking and Cycling Adoption Using the COM-B Model. Future Transportation 2025; 5: 79.
- Foley L, O’Mahony S, Ryan-Fogarty Y, et al. Cycling among people experiencing socio-economic disadvantage: a scoping review protocol [version 1; peer review: 2 approved]. HRB Open Res; 8. Epub ahead of print 1 January 2025. [CrossRef]
- Logan G, Somers C, Baker G, et al. Benefits, risks, barriers, and facilitators to cycling: a narrative review. Front Sports Act Living 2023; 5: 1168357.
- EUR-Lex - 32024C02377 - EN - EUR-Lex, https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=OJ%3AC_202402377 (accessed 26 February 2026).
- Huang B, Wüst H, de Haas M. Assessing the E-bike trends and impact on sustainable mobility: A national-level study in the Netherlands. Journal of Cycling and Micromobility Research 2024; 2: 100027.
- Snijders AH, Toni I, Ružička E, et al. Bicycling breaks the ice for freezers of gait. Mov Disord 2011; 26: 367–371.
- Licen T, Rakusa M, Bohnen NI, et al. Brain Dynamics Underlying Preserved Cycling Ability in Patients With Parkinson’s Disease and Freezing of Gait. Front Psychol 2022; 13: 847703.
- Storzer L, Butz M, Hirschmann J, et al. Bicycling suppresses abnormal beta synchrony in the Parkinsonian basal ganglia. Ann Neurol 2017; 82: 592–601.
- Bougou V, Vanhoyland M, Decramer T, et al. Active and Passive Cycling Decrease Subthalamic β Oscillations in Parkinson’s Disease. Mov Disord 2024; 39: 85–93.
- Bohnen NI, Jahn K. Imaging: what can it tell us about parkinsonian gait? Mov Disord 2013; 28: 1492.
- Engel AK, Fries P. Beta-band oscillations — signalling the status quo? Curr Opin Neurobiol 2010; 20: 156–165.
- Nieuwboer A. Cueing for freezing of gait in patients with Parkinson’s disease: A rehabilitation perspective. Movement Disorders 2008; 23: S475–S481.
- Zoetewei D, Herman T, Ginis P, et al. On-Demand Cueing for Freezing of Gait in Parkinson’s Disease: A Randomized Controlled Trial. Movement Disorders 2024; 39: 876–886.
- Canning CG. The effect of directing attention during walking under dual-task conditions in Parkinson’s disease. Parkinsonism Relat Disord 2005; 11: 95–99.
- Rutz DG, Benninger DH. Physical Therapy for Freezing of Gait and Gait Impairments in Parkinson Disease: A Systematic Review. PM R 2020; 12: 1140–1156.
- Cosentino C, Putzolu M, Mezzarobba S, et al. One cue does not fit all: A systematic review with meta-analysis of the effectiveness of cueing on freezing of gait in Parkinson’s disease. Neurosci Biobehav Rev; 150. Epub ahead of print 1 July 2023. [CrossRef]
- Dubuc R, Cabelguen JM, Ryczko D. Locomotor pattern generation and descending control: a historical perspective. 2023; 130: 401–416. [CrossRef]
- Wolpert DM, Landy MS. Motor control is decision-making. Curr Opin Neurobiol 2012; 22: 996–1003.
- Ijspeert AJ, Daley MA. Integration of feedforward and feedback control in the neuromechanics of vertebrate locomotion: a review of experimental, simulation and robotic studies. Journal of Experimental Biology; 226. Epub ahead of print 1 August 2023. [CrossRef]
- Gilat M, Hall JM, Ehgoetz Martens KA, et al. Staircase climbing is not solely a visual compensation strategy to alleviate freezing of gait in Parkinson’s disease. J Neurol 2017; 264: 174–176.
- Ehgoetz Martens KA, Pieruccini-Faria F, Almeida QJ. Could Sensory Mechanisms Be a Core Factor That Underlies Freezing of Gait in Parkinson’s Disease? PLoS One 2013; 8: e62602.
- Keijsers NLW, Admiraal MA, Cools AR, et al. Differential progression of proprioceptive and visual information processing deficits in Parkinson’s disease. European Journal of Neuroscience 2005; 21: 239–248.
- Alshehri MA, Alzahrani H, van den Hoorn W, et al. Trunk postural control during unstable sitting among individuals with and without low back pain: A systematic review with an individual participant data meta-analysis. PLoS One 2024; 19: e0296968.
- Reeves NP, Sal y Rosas Celi VG, Ramadan A, et al. Quantifying trunk neuromuscular control using seated balancing and stability threshold. J Biomech 2020; 112: 110038.
- Nguyen KP, Person AL. Cerebellar circuit computations for predictive motor control. Nature Reviews Neuroscience 2025 26:9 2025; 26: 538–553.
- Maschke M, Gomez CM, Tuite PJ, et al. Dysfunction of the basal ganglia, but not the cerebellum, impairs kinaesthesia. Brain 2003; 126: 2312–2322.
- Arber S, Costa RM. Networking brainstem and basal ganglia circuits for movement. Nature Reviews Neuroscience 2022 23:6 2022; 23: 342–360.
- Carpenter MG, Allum JHJ, Honegger F, et al. Postural abnormalities to multidirectional stance perturbations in Parkinson’s disease. J Neurol Neurosurg Psychiatry 2004; 75: 1245–1254.
- Bekkers EMJ, Dijkstra BW, Heremans E, et al. Balancing between the two: Are freezing of gait and postural instability in Parkinson’s disease connected? Neurosci Biobehav Rev 2018; 94: 113–125.
- Jacobs J V., Nutt JG, Carlson-Kuhta P, et al. Knee trembling during freezing of gait represents multiple anticipatory postural adjustments. Exp Neurol 2009; 215: 334–341.
- Rocchi L, Chiari L, Mancini M, et al. Step initiation in Parkinson’s disease: Influence of initial stance conditions. Neurosci Lett 2006; 406: 128–132.
- Salamci M, Guclu-Gunduz A. Anticipatory postural adjustments during gait initiation in people with parkinson’s disease: a systematic review. Acta Neurol Belg. Epub ahead of print 2025. [CrossRef]
- Kang S, Park JW, Kim Y, et al. Biomechanical analysis of patients with mild Parkinson’s disease during indoor cycling training. J Neuroeng Rehabil; 22. Epub ahead of print 1 December 2025. [CrossRef]
- D’Cruz N, Seuthe J, De Somer C, et al. Dual Task Turning in Place: A Reliable, Valid, and Responsive Outcome Measure of Freezing of Gait. Mov Disord 2022; 37: 269–278.
- Goris M, Ginis P, Hansen C, et al. Is the freezing index a valid outcome to assess freezing of gait during turning in Parkinson’s disease? Front Neurol 2024; 15: 1508800.
- Zoetewei D, Ginis P, Goris M, et al. Which Gait Tasks Produce Reliable Outcome Measures of Freezing of Gait in Parkinson’s Disease? J Parkinsons Dis 2024; 14: 1163–1174.
- Cefis M, Chaney R, Wirtz J, et al. Molecular mechanisms underlying physical exercise-induced brain BDNF overproduction. Front Mol Neurosci 2023; 16: 1275924.
- Mahalakshmi B, Maurya N, Lee S Da, et al. Possible Neuroprotective Mechanisms of Physical Exercise in Neurodegeneration. Int J Mol Sci 2020; 21: 1–17.
- Mansoor M, Ibrahim A, Hamide A, et al. Exercise-Induced Neuroplasticity: Adaptive Mechanisms and Preventive Potential in Neurodegenerative Disorders. Physiologia 2025, Vol 5, Page 13 2025; 5: 13.
- Petzinger GM, Fisher BE, McEwen S, et al. Exercise-enhanced Neuroplasticity Targeting Motor and Cognitive Circuitry in Parkinson’s Disease. Lancet neurology 2013; 12: 716.
- Ellis T, Rochester L. Mobilizing Parkinson’s Disease: The Future of Exercise. J Parkinsons Dis 2018; 8: S95–S100.
- Langeskov-Christensen M, Franzén E, Hvid LG, et al. Exercise as medicine in Parkinson’s disease Movement disorders. J Neurol Neurosurg Psychiatry 2024; 95: 1077–1088.
- Kaagman DGM, van Wegen EEH, Cignetti N, et al. Effects and Mechanisms of Exercise on Brain-Derived Neurotrophic Factor (BDNF) Levels and Clinical Outcomes in People with Parkinson’s Disease: A Systematic Review and Meta-Analysis. Brain Sci 2024; 14: 194.
- Patterson CG, Joslin E, Gil AB, et al. Study in Parkinson’s disease of exercise phase 3 (SPARX3): study protocol for a randomized controlled trial. Trials 2022; 23: 855.
- van der Kolk NM, de Vries NM, Kessels RPC, et al. Effectiveness of home-based and remotely supervised aerobic exercise in Parkinson’s disease: a double-blind, randomised controlled trial. Lancet Neurol 2019; 18: 998–1008.
- Schootemeijer S, van der Kolk NM, Bloem BR, et al. Current Perspectives on Aerobic Exercise in People with Parkinson’s Disease. Neurotherapeutics 2020; 17: 1418–1433.
- Alberts JL, Rosenfeldt AB. The Universal Prescription for Parkinson’s Disease: Exercise. J Parkinsons Dis 2020; 10: S21–S27.
- Tiihonen M, Westner BU, Butz M, et al. Parkinson’s disease patients benefit from bicycling - a systematic review and meta-analysis. NPJ Parkinsons Dis; 7. Epub ahead of print 1 December 2021. [CrossRef]
- Schootemeijer S, Darweesh SKL, De Vries NM. Clinical Trial Highlights - Aerobic Exercise for Parkinson’s Disease. J Parkinsons Dis 2022; 12: 2297–2306.
- Goetz CG, Tilley BC, Shaftman SR, et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord 2008; 23: 2129–2170.
- Rosenfeldt AB, Lopez-Lennon C, Suttman E, et al. Use of a Home-Based, Commercial Exercise Platform to Remotely Monitor Aerobic Exercise Adherence and Intensity in People With Parkinson Disease. Phys Ther 2024; 104: 1–11.
- Palmieri JL, Jones L, Schenkman M, et al. Bicycling for Rehabilitation of Persons With Parkinson Disease: A Scoping Review. J Neurol Phys Ther 2024; 48: 125–139.
- O’neal SK, Miller SA, Eikenberry MC, et al. A BACKWARD CYCLING PROGRAMME FOR PEOPLE WITH PARKINSON’S DISEASE: A FEASIBILITY AND PRELIMINARY RESULTS STUDY. J Rehabil Med 2024; 56: 17738.
- Warburton DER, Nicol CW, Bredin SSD. Health benefits of physical activity: the evidence. CMAJ : Canadian Medical Association Journal 2006; 174: 801.
- Tsukita K, Sakamaki-Tsukita H, Takahashi R. Long-term Effect of Regular Physical Activity and Exercise Habits in Patients With Early Parkinson Disease. Neurology 2022; 98: e859.
- Paul SS, Allen NE, Sherrington C, et al. Risk Factors for Frequent Falls in People with Parkinson’s Disease. J Parkinsons Dis 2014; 4: 699–703.
- Oguh O, Eisenstein A, Kwasny M, et al. Back to the basics: Regular exercise matters in Parkinson’s disease: Results from the National Parkinson Foundation QII Registry study. Parkinsonism Relat Disord 2014; 20: 1221–1225.
- Wallén MB, Franzén E, Nero H, et al. Levels and Patterns of Physical Activity and Sedentary Behavior in Elderly People With Mild to Moderate Parkinson Disease. Phys Ther 2015; 95: 1135–1141.
- Nimwegen M Van, Speelman AD, Hofman-Van Rossum EJM, et al. Physical inactivity in Parkinson’s disease. J Neurol 2011; 258: 2214.
- Vaugoyeau M, Viallet F, Aurenty R, et al. Axial rotation in Parkinson’s disease. J Neurol Neurosurg Psychiatry 2006; 77: 815–821.
- Korkmaz B, Yaşa ME, Sonkaya R. Upper extremity functions, spinal posture, and axial rigidity in patients with parkinson’s disease. Acta Neurol Belg. Epub ahead of print 2024. [CrossRef]
- Maarten Afschrift •, Matthijs A, De Ryck T, et al. Turning the head while biking makes older people lose cycling direction and balance. bioRxiv 2022; 2022.03.01.481993.
- Park J-H, Kang Y-J, Horak FB. What Is Wrong with Balance in Parkinson’s Disease? J Mov Disord 2015; 8: 109.
- Snijders AH, Toni I, Ružička E, et al. Bicycling breaks the ice for freezers of gait. Movement Disorders 2011; 26: 367–371.
- Gebhardt A, Vanbellingen T, Baronti F, et al. Poor dopaminergic response of impaired dexterity in Parkinson’s disease: Bradykinesia or limb kinetic apraxia? Movement Disorders 2008; 23: 1701–1706.
- Horak FB, Dimitrova D, Nutt JG. Direction-specific postural instability in subjects with Parkinson’s disease. Exp Neurol 2005; 193: 504–521.
- García-Navarra S, Llana T, Méndez M. Spatial memory deficits in Parkinson’s disease: neural mechanisms and assessment. Am J Neurodegener Dis 2025; 14: 67.
- Burgos PI, Silva-Batista C, Ragothaman A, et al. Cognition is associated with daily-life mobility in people with Parkinson’s disease. Clin Park Relat Disord 2025; 13: 100393.
- Aarsland D, Batzu L, Halliday GM, et al. Parkinson disease-associated cognitive impairment. Nature Reviews Disease Primers 2021 7:1 2021; 7: 1–21.
- Micca L, Albouy G, King BR, et al. The Effect of a Post-Learning Nap on Motor Memory Consolidation in People With Parkinson’s Disease: A Randomised Controlled Trial. J Sleep Res 2025; e70203.
- Van Biesen D, Pineda RC, Scheerder J, et al. Het Vlaamse G-sportlandschap anno 2024. 2024.
- Schootemeijer S, Van Der Kolk NM, Ellis T, et al. Barriers and Motivators to Engage in Exercise for Persons with Parkinson’s Disease. 2020; 10: 1293–1299. [CrossRef]
- Kim M, Kim E, Kim M, et al. Motivators and Barriers Affecting Exercise in Patients With Parkinson’s Disease. Journal of Clinical Neurology 2025; 21: 13–20.
- Mak MK, Wong-Yu IS, Shen X, et al. Exploring behavior, motivation, and barriers to exercise in Parkinson disease. Clin Park Relat Disord 2025; 13: 100362.
- Kovácsová N, de Winter JCF, Schwab AL, et al. Riding performance on a conventional bicycle and a pedelec in low speed exercises: Objective and subjective evaluation of middle-aged and older persons. Transp Res Part F Traffic Psychol Behav 2016; 42: 28–43.
- Maurissens T, Orban De Xivry J-J, De Groote F, et al. MaestroPD: Sensorimotor assessment of (e-)cycling in people with Parkinson’s disease. Epub ahead of print 7 August 2025. [CrossRef]
Figure 1.
schematic models of hypothesized differences in sensorimotor pathways between walking and cycling in healthy persons (HC) and persons with PD (PD). Brain regions are indicated in different colors: frontal area (dark blue); motor cortex (red) including premotor cortex and primary motor cortex; somatosensory cortex (yellow); cerebellum (purple); basal ganglia (green), which are affected in PD (hatched); and central pattern generators (light blue). Black double arrows indicate involved network connections. The thickness of the lines indicate connectivity strength. The red arrow indicates motor efferent output. Dashed lines suggest impaired pathways. When comparing HC and PD during walking, sensory processing (basal ganglia) and thus motor output are impaired. Patients therefore rely on compensatory networks, more involved in attentional motor generation. During cycling, people rely less on sensory information processing and more on feedforward movement prediction (cerebellum). The connection between cerebellum and basal ganglia is likely less engaged while cycling, and may contribute to preserved motor output during cycling.
Figure 1.
schematic models of hypothesized differences in sensorimotor pathways between walking and cycling in healthy persons (HC) and persons with PD (PD). Brain regions are indicated in different colors: frontal area (dark blue); motor cortex (red) including premotor cortex and primary motor cortex; somatosensory cortex (yellow); cerebellum (purple); basal ganglia (green), which are affected in PD (hatched); and central pattern generators (light blue). Black double arrows indicate involved network connections. The thickness of the lines indicate connectivity strength. The red arrow indicates motor efferent output. Dashed lines suggest impaired pathways. When comparing HC and PD during walking, sensory processing (basal ganglia) and thus motor output are impaired. Patients therefore rely on compensatory networks, more involved in attentional motor generation. During cycling, people rely less on sensory information processing and more on feedforward movement prediction (cerebellum). The connection between cerebellum and basal ganglia is likely less engaged while cycling, and may contribute to preserved motor output during cycling.
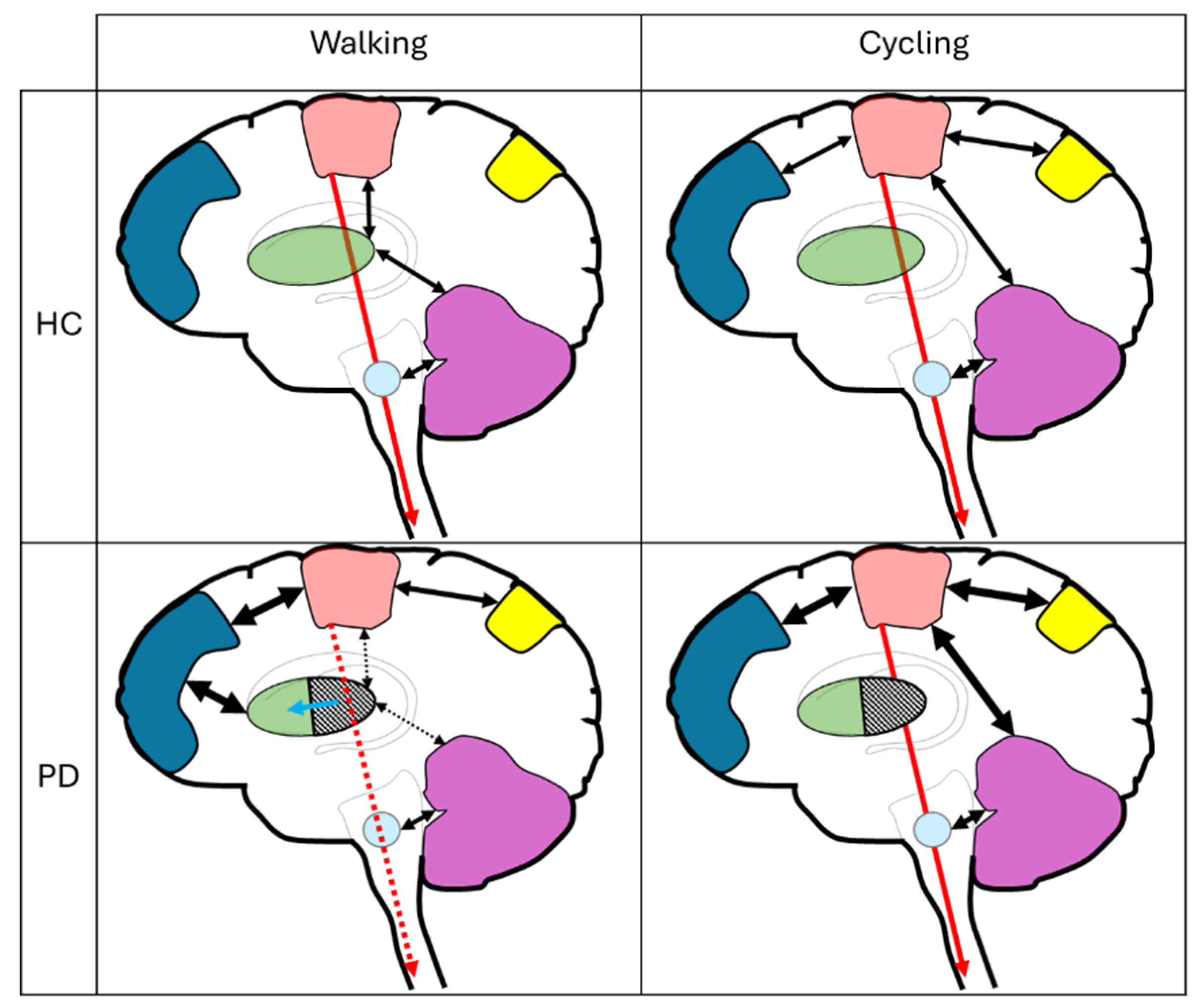
Figure 2.
Screenshots from the case-report video of Snijders and Bloem (2011) entitled “kinesia paroxia”, illustrating six challenges the gentleman faced when cycling outdoors, namely: A) cycling initiation; B) performing a shoulder check; C) turning; D) making sharp-angled maneuvers; E) disembarking from the bicycle; D) difficulty walking with the bicycle. Embarking the bicycle and hand raising are other challenges this gentleman might have experienced, but which is not shown on the video. Permission was obtained by the editor of the New England Journal of Medicine for re-use of the images following a face blurring de-identification procedure.
Figure 2.
Screenshots from the case-report video of Snijders and Bloem (2011) entitled “kinesia paroxia”, illustrating six challenges the gentleman faced when cycling outdoors, namely: A) cycling initiation; B) performing a shoulder check; C) turning; D) making sharp-angled maneuvers; E) disembarking from the bicycle; D) difficulty walking with the bicycle. Embarking the bicycle and hand raising are other challenges this gentleman might have experienced, but which is not shown on the video. Permission was obtained by the editor of the New England Journal of Medicine for re-use of the images following a face blurring de-identification procedure.
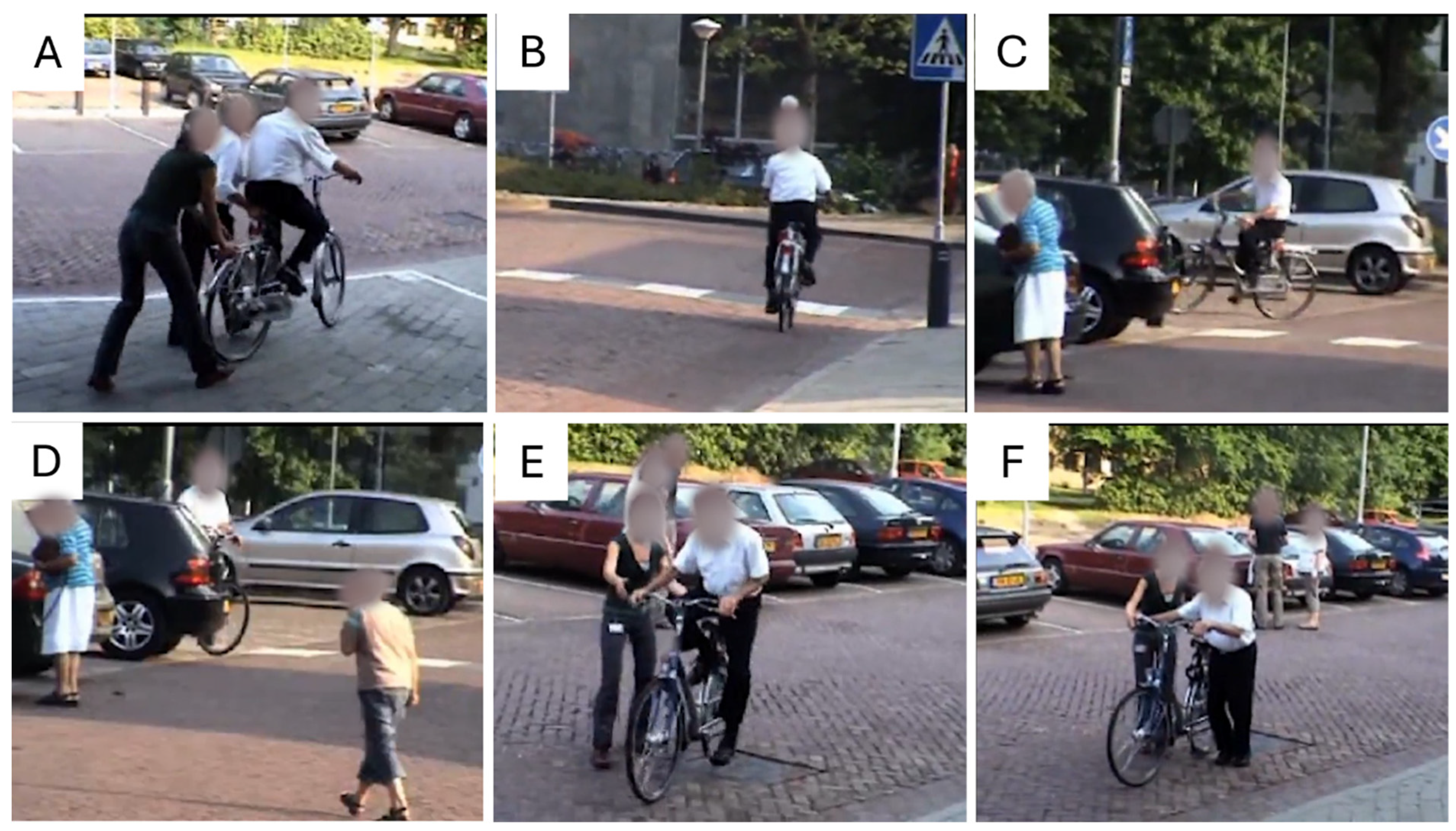
Figure 3.
Envisioned challenges during cycling and primary concerns for cycling participation and safety. The challenges are divided in egocentric and allocentric categories. Egocentric challenges refer to an individual’s level of both motor and cognitive functioning. Allocentric challenges reflect difficulties brought to the cyclist by the traffic and the environment, which includes predictable road changes, uneven surfaces and weather conditions. The primary concerns of outdoor cycling include falls, collisions and low cycling participation.
Figure 3.
Envisioned challenges during cycling and primary concerns for cycling participation and safety. The challenges are divided in egocentric and allocentric categories. Egocentric challenges refer to an individual’s level of both motor and cognitive functioning. Allocentric challenges reflect difficulties brought to the cyclist by the traffic and the environment, which includes predictable road changes, uneven surfaces and weather conditions. The primary concerns of outdoor cycling include falls, collisions and low cycling participation.
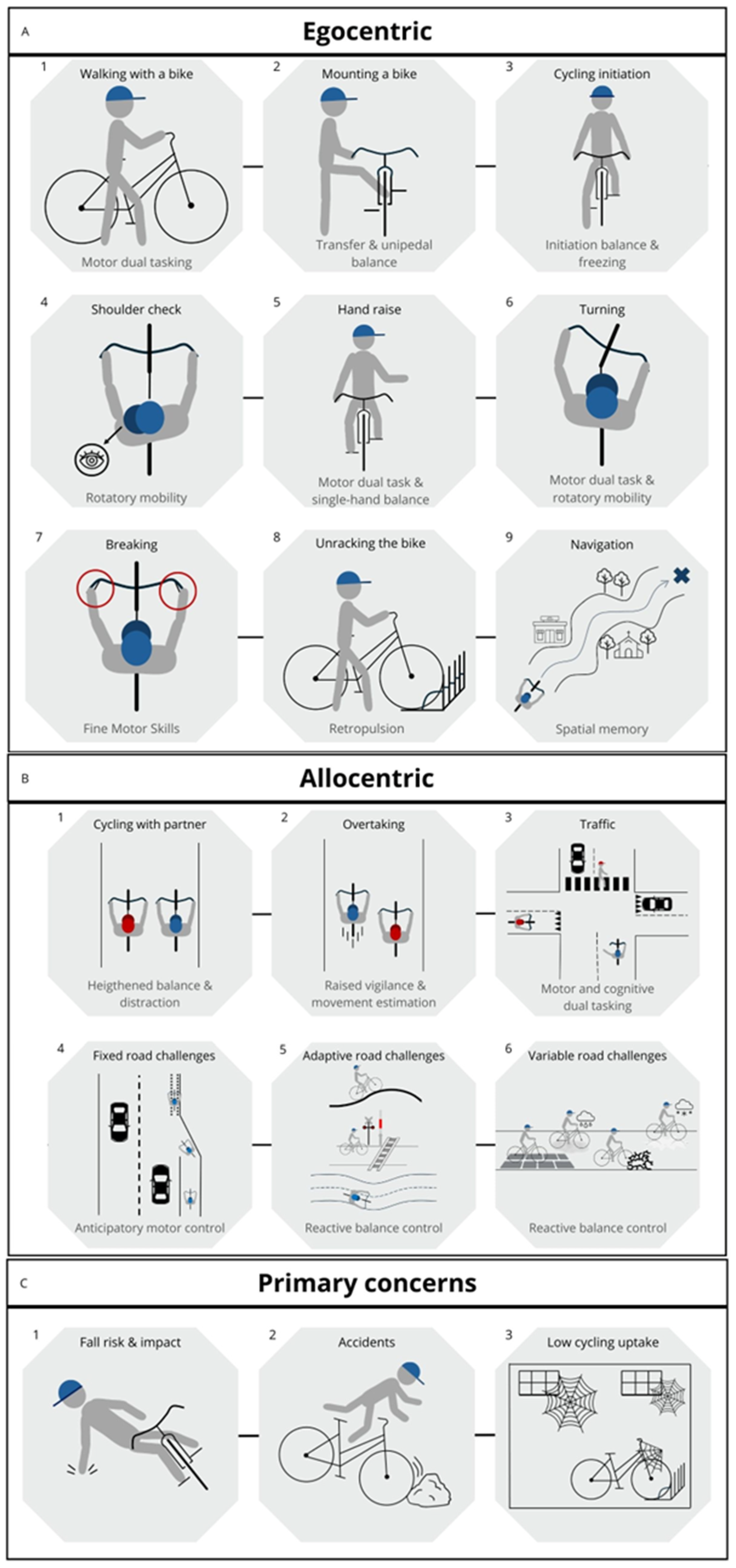
Figure 4.
weekly cycling uptake in persons with PD and age-matched controls. Roughly one in four PD participants report to cycle at least once per week compared to a third in the control group. The difference between both groups was not significant (p=0.19). Ethical approval was obtained from the Medical Ethical Committee for this retrospective evaluation (ID: S70945).
Figure 4.
weekly cycling uptake in persons with PD and age-matched controls. Roughly one in four PD participants report to cycle at least once per week compared to a third in the control group. The difference between both groups was not significant (p=0.19). Ethical approval was obtained from the Medical Ethical Committee for this retrospective evaluation (ID: S70945).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



