Submitted:
27 February 2026
Posted:
27 February 2026
You are already at the latest version
Abstract
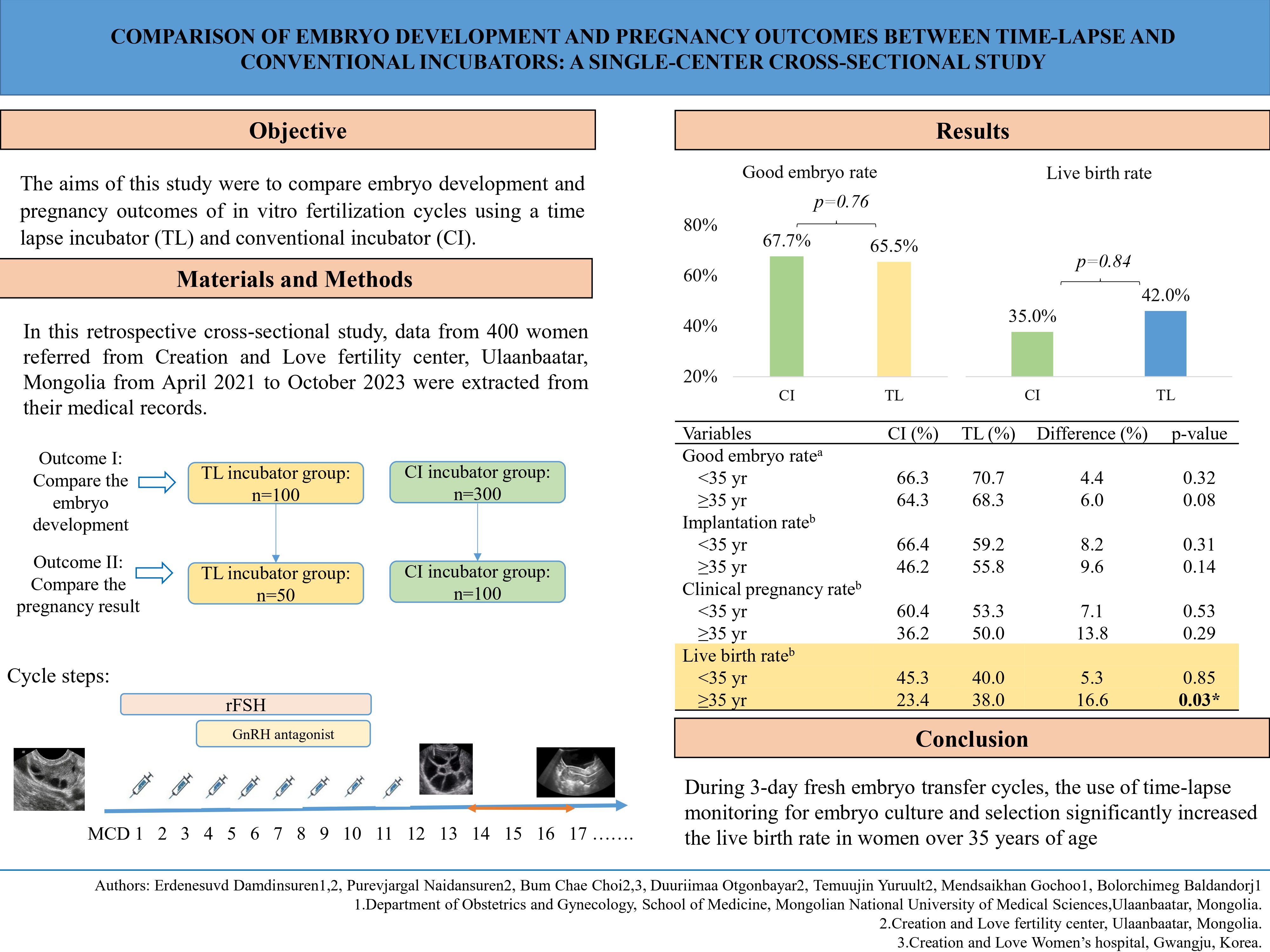
Background: In recent years, time-lapse incubators (TLs) with the ability to maintain a stable culture environment have been developed for in vitro fertilization treatment. Methods: In this retrospective cross-sectional study, data from 1,200 women who visited the Creation and Love fertility center, between April 2021 and October 2023 were reviewed. Among them, electronic medical records of 400 women aged 22-45 who underwent in vitro fertilization treatment were selected and divided into 2 groups according to the type of incubator used: 100 in the TL group and 300 in the CI group to evaluate differences in embryo development. Out of these participants, pregnancy outcomes were compared in 150 who underwent fresh-embryo transfer. Controlled ovarian stimulation was performed by standard antagonist protocol. The primary outcome was live birth rate, and the secondary outcome was good embryo rate. Results: The mean age of the study population was 34.6±5.4. Groups had a similar good embryo rate (67.7% vs. 65.5%, p=0.84), clinical pregnancy rate (49.0% vs. 52.0%, p=0.86) and live birth rate (35.0% vs. 42.0%, p=0.76). Furthermore, subgroup analyses of the live birth rate in women aged >35 was higher in the TL group than the CI group (38.0% vs. 23.4%, p=0.03). Conclusions: Based on the comparative analysis of live birth rates between women cultured using TLs and those using CI during 3-day fresh embryo transfer cycles, our study demonstrated a statistically significant increase in live birth rates among women >35 yr of age in the TL group.
Keywords:
infertility
; reproductive techniques
; fertilization in vitro
; sperm injections
; embryo implantation
1. Introduction
Infertility is defined by the failure to achieve a pregnancy after 1 yr or more of regular unprotected sexual intercourse [1]. Infertility affects approximately 80 million people, and the prevalence of infertility is up to 21.9% in 2002 [2]. In vitro fertilization (IVF) is the preferred treatment for many causes of infertility [3]. The European Society for Human Reproduction and Embryology estimated the population based on demand for IVF to be approximately 3,000 cycles per million people [4]. Since the first successful IVF delivery in 1978, the delivery rate has increased, ranging between 7.1% and 32.1 [5]. Improving clinical outcomes of infertile women undergoing IVF treatment has always been the main concern for infertility specialists. Several factors impact the success rate of IVF cycles, although these predominantly involve embryo quality and endometrial receptivity [6].
One of the several technical innovations proposed over the last 2 decades to improve embryo culture and quality assessment, and subsequently optimize treatment outcome, is time-lapse technology (TLT) [7]. A TLT system consists of an incubator integrated with microscopes and cameras connected to an external computer, enabling continuous embryo monitoring. Continued embryo monitoring has allowed us to identify previously unknown or undetectable aspects of development, to have a significant clinical impact [8]. The improvement of embryo development and clinical outcomes provided by TLT in IVF over conventional incubation remains controversial. Several studies reported significant associations between the time-lapse (TL) incubator and clinical outcomes [9,10]. In addition, these studies have focused more on the outcomes of blastocyst transfer. In particular, the selection of a good-quality embryo that has been monitored in TLT for transfer enhances the implantation rate, increases the cumulative pregnancy rate, decreases early pregnancy loss, and reduces the time to pregnancy [9,11]. Moreover, several studies have found that TLT did not contribute to the improvement of the developmental potential of embryos, especially in couples with a favorable prognosis [12,13].
The use of TL technology may not be beneficial for all IVF cases, but it could be advantageous in certain cases. The use of a TLT during cleavage-stage embryo transfer may be more effective, especially in older women with a low number of retrieved oocytes.
To investigate this, our study included cases of cleavage-stage embryo transfer to compare the effectiveness of the two types of incubators. To enhance the accuracy of the analysis, participants were further stratified by age.
2. Materials and Methods
2.1. Study Design
In this retrospective cross-sectional study, data from 400 women referred from Creation and Love fertility center, Ulaanbaatar, Mongolia, from April 2021 to October 2023 were extracted from their medical records. The study included women aged 22-45 yr who underwent IVF treatment cycles. Cycles involving oocyte donation, oocyte cryopreservation, frozen-thawed embryo transfer cycles, and cycles that used a mix of conventional incubator (CI) and TL incubators were excluded. Study participants were initially divided into two groups to compare embryonic development based on the type of incubator: TL group (n=100) and a CI group (n=300). Due to the smaller number of participants using the TL incubator, the cases were allocated in a 1:3 ratio to compare embryo development between the TL and CI groups. Among these, 150 fresh-embryo transfer cycles were included in the outcome analysis after excluding cycles in which all embryos were frozen, transferred to a surrogate, or did not result in usable embryos.
2.2. Controlled Ovarian Stimulation Protocol
Ovarian reserve was assessed using baseline follicle stimulating hormone (FSH), antimullerian hormone (AMH), and antral follicle count (AFC). Controlled ovarian stimulation followed a gonadotropin-releasing hormone antagonist protocol with recombinant FSH (Gonal-F, 150–300 IU/day). Follicular monitoring was done every 2–3 days via transvaginal ultrasound. When a dominant follicle reached 14 mm, Cetrotide (0.25 mg/day) was initiated and continued until ovulation triggering with human chorionic gonadotropin (Ovidrel, 5000–10000 IU), based on follicle size. Hormone levels (estradiol, luteinizing hormone, and progesterone) were recorded on the trigger day.
2.3. Fertilization
Oocyte retrieval was performed 35–36 hr post human chorionic gonadotropin injection via ultrasound-guided aspiration under general anaesthesia. The collected oocytes were cultured in IVF media (Vitrolife, Gothenburg, Sweden) and incubated at 37oC, under 6% CO2, 5% O2 for 2–3 hours. Based on sperm parameters, fertilization was performed using either intracytoplasmic sperm injection or conventional insemination method. Maturation rate was calculated as the proportion of MII oocytes among all retrieved oocytes. Fertilization rate was defined as two pronuclei zygotes per MII oocyte.
2.4. Embryo Culture and Assessment
In the TL group, morphokinetics and abnormal cleavage were monitored. A primo vision camera was set to take a picture of embryos every 10 minutes. The following abnormal cleavage patterns were analyzed: reverse-cleavage appearance and direct cleavage in which a single blastomere divides directly from one to three cells. In both groups, cleavage-stage embryos were according to Veeck’s criteria [14]: grade I, even and homogeneous blastomeres without cytoplasmic fragmentation; grade II, even and homogeneous blastomeres with ≤25% fragmentation; grade III, uneven and heterogeneous blastomeres with 25–50% fragmentation; and grade IV, uneven and heterogeneous blastomeres with ≥50% fragmentation. At day 3, embryos with more than six cells and grade I–II morphology were classified as good quality, while those with six or fewer cells and grade III–IV morphology were classified as poor quality.
2.5. Embryo Transfer
This study analyzed 150 (50 participants used the TL and 100 participants used CI) fresh embryo transfer cycles for pregnancy outcomes. Fresh embryo transfer was performed on day 3 after oocyte retrieval under ultrasound guidance. Embryo selection using TLT based on standard morphological grading and morphokinetic’s criteria (absence of abnormal cleavage). Embryo selection using a CI based on morphology. The number of cleavage-stage embryos transferred was determined based on the participant’s clinical indications and the guideline of the American Society for Reproduction Medicine: ≤2 embryos for women under 35 years of age and triple embryo transfer for women aged 35 years or older. The quality of transferred embryos was classified as follows: (1) all embryos were grade I, (2) at least one embryo was grade I while the others were grade II, and (3) all embryos were grade II.
Surplus embryos were frozen according to the routines at the hospital. Luteal support was administered in the form of 600 mg/day vaginal progesterone (Yenatron, Acraf S.pA, Roma, Italy) until confirmation of biochemical pregnancy. Blood β human chorionic gonadotropin was tested 9 days after transfer, and a value greater than 10 mIU/ml was considered a positive biochemical pregnancy and luteal support was continued until 10 weeks of gestation. The luteal support will be discontinued if a biochemical pregnancy is not observed. The implantation rate refers to the percentage of transferred embryos that successfully implant and develop into gestational sacs.
2.6. Outcome Measurements
The primary outcomes of this study were the clinical pregnancy rate and live birth rate. Clinical pregnancy was confirmed by the presence of a gestational sac and visible primitive heart tube pulsations on transvaginal ultrasound at week 6 of pregnancy. Clinical pregnancy rate refers to the proportion of clinical pregnancy cycles to the number of transfer cycles. The live birth rate was calculated by dividing the number of women with at least one live birth by the number of women who underwent embryo transfer. The secondary outcome was the rate of good-quality embryos, which was calculated as the number of good-quality embryos divided by the total number of fertilized oocytes.
2.7. Ethical Consideration
This study was approved by the Institutional Review Board of the Mongolian National University of Medical Sciences (No. 2023/03-04). The data collection process was in accordance with the ethical standards of the institutional and national committees, and participants’ data were anonymized to ensure confidentiality.
2.8. Statistical Analysis
Statistical analysis was performed using SPSS for Windows (version 17.0, SPSS Inc., Chicago, IL, USA). The Kolmogorov-Smirnov test was used to assess the normality of data distribution in each group. The variables were assessed using mean±standard deviation, N (%). Chi-square tests were carried out to compare categorical variables. Subgroup analysis was conducted to evaluate primary and secondary outcomes between the two age groups (ie, <35 years and ≥35 years). Independent t-tests were used to compare means of continuous variables between the groups. Statistical significance was determined at a p< 0.05.
3. Results
The baseline characteristics of the participants are demonstrated in Table 1. The mean age of the 400 participants included in this study was 34.6±5.4 yr (range 22-45). The mean body mass index (BMI) was 24.3±3.8. The majority of participants in both groups had a BMI within the normal range (68.0%). The mean duration of infertility was 65.1±43.4 months, with a maximum duration of 156 months.
The ovarian stimulation and embryo development characteristics are presented in Table 2. During this study, a total of 3568 oocytes were retrieved in 400 cycles, of which 2861 (80.2%) were at the MII stage, 275 (7.7%) were at the metaphase I stage, and 432 (12.1%) were germinal vesicle oocytes. The mean number of retrieved oocytes per participant was 8.9±6.4. The mean duration of stimulation, total gonadotropin dose, and the mean number of retrieved oocytes were comparable between the two groups. No significant differences were observed in the fertilization rate (91.5% vs 85.5%, p=0.12) and the good embryo rate (67.7% vs 65.5%, p=0.84) between the two incubator groups.
A total of 150 fresh embryo transfer cycles (37.5% of all cycles) were analyzed during the study (Table 3). The mean AMH level, endometrial thickness and progesterone level was similar in both groups. We compared the number and quality of embryos transferred in each group. There was no statistically significant difference in the transferred embryos between the CI and TL groups. Both groups showed similar implantation rates (58.4% vs. 57.1%, p=0.79). The clinical pregnancy rates (49.0% vs. 52.0%, p=0.86) and live birth rates (35.0% vs. 42.0%, p=0.76) were similar between the groups.
Subgroup analysis results for maturation rate, fertilization rate, good embryo rate, implantation rate, clinical pregnancy rate and live birth rate stratified by age are presented in Table 4. There were 83 embryo transfer cycles in women aged <35 years, and a total of 67 embryo transfer cycles in women aged over 35 years. The live birth rate in women aged 35 and older was significantly higher in the TL incubator group compared to CI group. Specifically, the TL group showed a live birth rate of 38.0% compared to 23.4% in the conventional group (p = 0.03).
4. Discussion
In this study, we divided participants into two age groups, and treatment outcomes were analyzed separately within the TL and CI groups. In this subgroup analysis, women aged > 35 yr had a higher live birth rate in the TL group compared to the CI group. Embryos of good and poor quality, or from younger and older women, are known to behave differently during IVF treatment. The higher incidence of aneuploidy with increasing maternal age is often cited as a major reason for age-dependent success rates in IVF cycles. [15,16]. Several studies have mentioned the advantages of TLT for pregnancy outcomes in advanced-aged women. TL monitoring has been reported to improve live birth rates, implantation rates, and clinical pregnancy rates, particularly in women over 35 years of age [17]. Despite improvements in IVF treatment, live birth rates remain suboptimal, especially in advanced age women. Aneuploidy is closely linked to maternal age, with only a minimal correlation to the morphological characteristics of the embryo [18]. The study of Siristatidis et al, similar to ours, showed a higher live birth rate in the TL incubator group, especially in participants aged >40 yr old [19]. The use of the TL system for embryo selection during fresh embryo transfer cycles enables the consideration of not only the morphological structure, but also morphokinetic parameters and abnormal division [20,21].
During this study, no significant differences were observed in the clinical pregnancy rate or the good embryo rate between the use of TL monitoring and standard care. Therefore, it is important to critically evaluate whether the application of TLT is truly necessary and beneficial in specific clinical scenarios. Our results support the findings of several previous studies that assessed the effect of TL imaging systems [22,23,24]. The Cochrane review reported insufficient evidence for differences in live birth rates, miscarriage rates, and clinical pregnancy rates when comparing TLT combined with embryo selection software versus conventional incubation and assessment. The studies included in the Cochrane review encompassed blastocyst transfer as well as both Day 3 and Day 5 embryo transfer cycles [22]. IVF centers commonly transfer one or several embryos during embryo transfer cycles at one of two stages of embryo development: the cleavage stage or the blastocyst stage [25]. Although there is an increasing preference for blastocyst-stage embryo transfer, cleavage-stage transfer offers a comparable cumulative live birth rate, a higher cryopreservation rate, and a lower embryo transfer cancellation rate [26,27]. Previous studies that included Day 3 embryo transfer cycles found no differences in good embryo rate, implantation rate, and clinical pregnancy rate between the TL monitoring and CI groups [23,28]. In a recent multi-center, randomized study, the use of TL imaging systems for embryo culture and selection was reported not to significantly increase the odds of live birth compared to standard care without TL imaging [29]. During a multicentre, three-parallel group, double-blind, randomised controlled trial, the live birth rates were 33.7% in the TL imaging group, 33.0% in the standard care group. It has been reported that in women undergoing IVF treatment cycles, the use of TL imaging systems for embryo culture and selection does not significantly increase the odds of live birth compared with standard care [29].
While most studies evaluating the difference between TL incubator and CI evaluated blastocyst transfer results, we examined cycles involving 3-day embryo transfers. The combination of standard day 3 morphology with the use of TL technology results for embryo evaluation resulted in a significantly higher live birth rate in advanced aged women who retrieved fewer oocytes. A statistically significant relationship has been demonstrated between the timing of early cell divisions and implantation and pregnancy rate [7]. Automated TL embryo assessment combined with morphologic assessment has been compared with morphologic assessment alone. This report demonstrates improved implantation rates in women receiving day 3 embryo transfers based on the combined use of a TL-test along and traditional morphology [30]. Over the last decade, embryo transfer at the blastocyst stage has been used more frequently, cleavage-stage embryo transfers are still being performed. In previous studies, embryo morphokinetic parameters that were retrospectively extracted from TL videos have consistently shown strong correlations with blastocyst formation, implantation potential [31]. It has been reported that combining TL culture with artificial intelligent scoring may enhance ongoing pregnancy rates in single cleavage-stage fresh transfer cycles [32].
We acknowledge some limitations of this study. First, its retrospective design exposes it to a risk of bias and limited statistical power. Second, the sample size was relatively small, which may limit the generalizability of the findings to the broader population of infertile women.
Our results might not be applicable to frozen-thawed embryo transfer strategies. For these reasons, future studies are needed to validate the findings of the present study. While TL technology is an effective and safe alternative for embryo incubation, more randomized trials with a larger number of women who undergo cleavage-stage embryo transfers are required.
5. Conclusions
This study contributes valuable insights into the potential benefits of TL embryo monitoring technology, particularly for women of advanced maternal age undergoing fresh cleavage-stage embryo transfers. While many factors influence IVF outcomes, our findings highlight that the use of a TL system may enhance live birth rates in women over 35 yr old, a group traditionally facing lower success rates largely due to increased aneuploidy and embryo quality challenges. This suggests that incorporating morphokinetic data alongside conventional morphological assessment can refine embryo selection and improve clinical outcomes in this subgroup. Looking forward, larger randomized controlled trials focusing on cleavage-stage embryo transfers are essential to confirm these preliminary benefits and better define the role of TL monitoring in routine IVF practice. Ultimately, this research supports the evolving landscape of assisted reproductive technologies, where individualized treatment approaches guided by advanced embryo assessment tools may improve outcomes for women facing infertility challenges at older ages.
Author Contributions
Conceptualization, E.D, N.P; methodology, E.D, N.P and C.B.C.; software, E.T and M.G.; validation, B.B.; data curation, E.D, E.T, N.P and D.O.; writing—original draft preparation, E.D, B.B.; writing—review and editing, C.B.C, B.B.; visualization, M.G and B.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Mongolian National University of Medical Sciences (No. 2023/03-04). Ethics approval date 21April 2023.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to thank Dr. Hye Young Park for providing a time-lapse monitoring setting for this research. We would also like to thank Creation and Love fertility center’s doctors and colleagues for supporting us.
Conflicts of Interest
The authors declare that there is no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AFC | Antral Follicle Count |
| AMH | Anti-Mullerian Hormone |
| BMI | Body mass index |
| CI | Conventional Incubator |
| FSH | Follicle Stimulating Hormone |
| IVF | In Vitro Fertilization |
| LH | Luteinizing Hormone |
| MII | Metaphase II |
| TL | Time Lapse |
| TLT | Time Lapse Technology |
References
- Organization WH. Infertility. 2023.
- Organization WH. Infertility prevalence estimates, 1990–2021. 2023.
- Carson, S.A.; Kallen, A.N. Diagnosis and Management of Infertility: A Review. JAMA 2021, 326, 65-76.
- Ferraretti, A.P.; Nygren, K.; Andersen, A.N.; de Mouzon, J.; Kupka, M.; Calhaz-Jorge, C.; Wyns, C.; Gianaroli, L.; Goossens, V. Trends over 15 years in ART in Europe: an analysis of 6 million cycles. Hum Reprod Open 2017, hox012. [CrossRef]
- Dyer, S.; Chambers, G.M.; Jwa, S.C.; Baker, V.L.; Banker, M.; de Mouzon, J.; Elgindy, E.; Fu, B.; Ishihara, O.; Kupka, M.S.; Zegers-Hochschild, F.; Adamson, G.D. International Committee for Monitoring Assisted Reproductive Technologies world report: assisted reproductive technology. Hum Reprod 2021, 36, 2921-2934.
- Lacconi, V.; Massimiani, M.; Carriero, I.; Bianco, C.; Ticconi, C.; Pavone, V.; Alteri, A.; Muzii, L.; Rago, R.; Pisaturo, V.; Campagnolo, L. When the Embryo Meets the Endometrium: Identifying the Features Required for Successful Embryo Implantation. Int J Mol Sci 2024, 25. [CrossRef]
- Gimenez, C.; Conversa, L.; Murria, L.; Meseguer, M. Time-lapse imaging: Morphokinetic analysis of in vitro fertilization outcomes. Fertil Steril 2023, 120, 218-227. [CrossRef]
- Apter, S.; Ebner, T.; Freour, T.; Guns, Y.; Kovacic, B. Good practice recommendations for the use of time-lapse technology. Hum Reprod Open 2020, 2020, hoaa008. [CrossRef]
- Reignier, A.; Lefebvre, T.; Loubersac, S.; Lammers, J.; Barriere, P.; Freour, T. Time-lapse technology improves total cumulative live birth rate and shortens time to live birth as compared to conventional incubation system in couples undergoing ICSI. J Assist Reprod Genet 2021, 38, 917-923. [CrossRef]
- Kieslinger, D.C.V.C.; Ramos, L.; Arends, B.; Curfs, M.H.J.M.; Slappendel, E. Clinical outcomes of uninterrupted embryo culture with or without time-lapse-based embryo selection versus interrupted standard culture (SelecTIMO): a three-armed, multicentre, double-blind, randomised controlled trial. Lancet 2023, 401, 1438-1446. [CrossRef]
- Zhang, X.D.; Zhang, Q.; Han, W.; Liu, W.W.; Shen, X.L.; Yao, G.D.; Shi, S.L.; Hu, L.L.; Wang, S.S.; Wang, J.X.; Zhou, J.J.; Kang, W.W.; Zhang, H.D.; Luo, C.; Yu, Q.; Liu, R.Z.; Sun, Y.P.; Sun, H.X.; Wang, X.H.; Quan, S.; Huang, G.N. Comparison of embryo implantation potential between time-lapse incubators and standard incubators: A randomized controlled study. Reprod Biomed Online 2022, 45, 858-866. [CrossRef]
- Jiang, Y.W.L.; Wang, S.; Shen, H.; Wang, B.; Zheng, J. The effect of embryo selection using time-lapse monitoring on IVF/ICSI outcomes: A systematic review and meta-analysis. J Obstet Gynaecol Res 2023, 49. [CrossRef]
- Bergh, C.; Lundin, K. No benefit to pregnancy or livebirth by time-lapse-based embryo selection in IVF. Lancet 2023, 401, 1401-1403. [CrossRef]
- Cheon, K.W.; Song, S.J.; Choi, B.C.; Lee, S.C.; Lee, H.B.; Yu, S.Y.; Yoo, K.J. Comparison of clinical efficacy between a single administration of long-acting gonadotrophin-releasing hormone agonist (GnRHa) and daily administrations of short-acting GnRHa in in vitro fertilization-embryo transfer cycles. J Korean Med Sci 2008, 23, 662-666. [CrossRef]
- Sahin, G.N.; Yildirim, R.M.; Seli, E. Embryonic arrest: causes and implications. Current Opinion in Obstetrics and Gynecology 2023, 35, 184-192. [CrossRef]
- Elmerdahl Frederiksen, L.; Olgaard, S.M.; Roos, L.; Petersen, O.B.; Rode, L.; Hartwig, T. Maternal age and the risk of fetal aneuploidy: A nationwide cohort study of more than 500 000 singleton pregnancies in Denmark from 2008 to 2017. Acta Obstet Gynecol Scand 2024, 103, 351-359. [CrossRef]
- Chera-Aree, P.; Thanaboonyawat, I.; Thokha, B.; Laokirkkiat, P. Comparison of pregnancy outcomes using a time-lapse monitoring system for embryo incubation versus a conventional incubator in in vitro fertilization: An age-stratification analysis. Clin Exp Reprod Med 2021, 48, 174-183. [CrossRef]
- Franasiak, J.M.; Forman, E.J.; Hong, K.H.; Werner, M.D.; Upham, K.M.; Treff, N.R.; Scott, R.T. Jr. The nature of aneuploidy with increasing age of the female partner: a review of 15,169 consecutive trophectoderm biopsies evaluated with comprehensive chromosomal screening. Fertil Steril 2014, 101, 656-663. [CrossRef]
- Siristatidis, C.; Komitopoulou, M.A.; Makris, A.; Sialakouma, A.; Botzaki, M.; Mastorakos, G.; Salamalekis, G.; Bettocchi, S.; Palmer, G.A. Morphokinetic parameters of early embryo development via time lapse monitoring and their effect on embryo selection and ICSI outcomes: a prospective cohort study. J Assist Reprod Genet 2015, 32, 563-570. [CrossRef]
- McQueen, D.B.; Mazur, J.; Kimelman, D.; Confino, R.; Robins, J.C.; Bernardi, L.A.; Yeh, C.; Zhang, J.; Pavone, M.E. Can embryo morphokinetic parameters predict euploid pregnancy loss? Fertil Steril 2021, 115, 382-388. [CrossRef]
- Coticchio, G.; Pennetta, F.; Rizzo, R.; Tarozzi, N.; Nadalini, M.; Orlando, G.; Centonze, C.; Gioacchini, G.; Borini, A. Embryo morphokinetic score is associated with biomarkers of developmental competence and implantation. J Assist Reprod Genet 2021, 38, 1737-1743. [CrossRef]
- Armstrong, S.; Bhide, P.; Jordan, V.; Pacey, A.; Farquhar, C. Time-lapse systems for embryo incubation and assessment in assisted reproduction. Cochrane Database Syst Rev 2018, 5, CD011320.
- Wu, Y.G.; Lazzaroni-Tealdi, E.; Wang, Q.; Zhang, L.; Barad, D.H.; Kushnir, V.A.; Darmon, S.K.; Albertini, D.F.; Gleicher, N. Different effectiveness of closed embryo culture system with time-lapse imaging (EmbryoScope(TM)) in comparison to standard manual embryology in good and poor prognosis patients: a prospectively randomized pilot study. Reprod Biol Endocrinol 2016, 14, 49-54. [CrossRef]
- Nakahara, T.; Iwase, A.; Goto, M.; Harata, T.; Suzuki, M.; Ienaga, M.; Kobayashi, H.; Takikawa, S.; Manabe, S.; Kikkawa, F.; Ando, H. Evaluation of the safety of time-lapse observations for human embryos. J Assist Reprod Genet 2020, 27, 93-96. [CrossRef]
- Glujovsky, D.; Quinteiro Retamar, A.M.; Alvarez Sedo, C.R.; Ciapponi, A.; Cornelisse, S.; Blake, D. Cleavage-stage versus blastocyst-stage embryo transfer in assisted reproductive technology. Cochrane Database Syst Rev 2022, 5, CD002118. [CrossRef]
- Fernandez-Shaw, S.; Cercas, R.; Brana, C.; Villas, C.; Pons, I.O. Ongoing and cumulative pregnancy rate after cleavage-stage versus blastocyst-stage embryo transfer using vitrification for cryopreservation: Impact of age on the results. J Assist Reprod Genet 2015, 32, 177-184. [CrossRef]
- Giladi Yacobi, E.; Miller, N.; Goren Gepstein, N.; Mashiach, J.; Haikin Herzberger, E.; Levi, M.; Ghetler, Y.; Wiser, A. Does cleavage- versus blastocyst-stage embryo transfer improve fertility rates in women over 38 years of age undergoing assisted reproductive technology? Int J Gynaecol Obstet 2024, 167, 1017-1022. [CrossRef]
- Guo, Y.H.; Liu, Y.; Qi, L.; Song, W.Y.; Jin, H.X. can time-lapse incubation and monitoring be beneficial to assisted reproduction technology outcomes? A randomized controlled trial using day 3 double embryo transfer. Front Physiol 2021, 12, 794601. [CrossRef]
- Bhide, P.; Chan, D.Y.L.; Lanz, D.; Alqawasmeh, O.; Barry, E.; Baxter, D.; Gonzalez Carreras, F.; Choudhury, Y.; Cheong, Y.; Chung, J.P.W.; Collins, B.; Cong, L.; Doidge, S.; Heighway, J.; Patel, D.; Pardo, M.C.; Rattos, A.; Wright, A.; Dodds, J.; Perez, T.; Khan, K.S.; Thangaratinam, S. Clinical effectiveness and safety of time-lapse imaging systems for embryo incubation and selection in in-vitro fertilisation treatment (TILT): A multicentre, three-parallel-group, double-blind, randomised controlled trial. Lancet 2024, 404, 256-265. [CrossRef]
- Adamson, G.D.; Abusief, M.E.; Palao, L.; Witmer, J.; Palao, L.M.; Gvakharia, M. Improved implantation rates of day 3 embryo transfers with the use of an automated time-lapse-enabled test to aid in embryo selection. Fertil Steril 2016, 105, 369-375. [CrossRef]
- Goodman, L.R.; Goldberg, J.; Falcone, T.; Austin, C.; Desai, N. Does the addition of time-lapse morphokinetics in the selection of embryos for transfer improve pregnancy rates? A randomized controlled trial. Fertil Steril 2016, 105, 275-285. [CrossRef]
- Wang, X.; Wei, Q.; Huang, W.; Yin, L.; Ma, T. Can time-lapse culture combined with artificial intelligence improve ongoing pregnancy rates in fresh transfer cycles of single cleavage stage embryos? Front Endocrinol (Lausanne) 2024, 15, 1449035. [CrossRef]

Table 1.
Baseline characteristics of participants compared between TL and CI groups.
| Variables | Total (n=400) | CI group (n=300) | TL group (n=100) | p-Value | |||
|---|---|---|---|---|---|---|---|
| Age (yr)* | 34.62±5.39 | 34.82±5.53 | 34.02±4.92 | 0.17 | |||
| Infertility duration (months)* | 65.12±43.36 | 63.85±43.25 | 69.00±43.71 | 0.34 | |||
| BMI (kg/m2)* | 24.34±3.83 | 24.42±3.94 | 24.13±3.53 | 0.50 | |||
| Causes of infertility** | |||||||
| Female | 135 (33.8) | 106 (35.3) | 29 (29.0) | 0.10 | |||
| Male | 176 (44.0) | 133 (44.4) | 43 (43.0) | ||||
| Combined | 66 (16.5) | 42 (14.0) | 24 (24.0) | ||||
| Idiopathic | 23 (5.7) | 19 (6.3) | 4 (4.0) | ||||
| Ovarian reserve markers | |||||||
| AFC* | 7.66±4.39 | 7.39±4.46 | 8.38±3.85 | 0.06 | |||
| AMH (ng/ml)* | 1.90±1.49 | 1.92±1.49 | 2.12±1.39 | 0.11 | |||
| FSH (mIU/ml)* | 7.88±3.30 | 8.22±3.28 | 7.74±3.30 | 0.22 | |||
| Sperm preparation** | |||||||
| Ejaculated | 355 (88.7) | 272 (90.7) | 83 (83.0) | 0.06 | |||
| Testicular | 45 (11.3) | 28 (9.3) | 17 (17.0) | ||||
| Hormone’s level on trigger day | |||||||
| Estrogen (pg/ml)* | 2042.84±1098.81 | 2049.94±1114.65 | 2008.69±1005.47 | 0.56 | |||
| LH (mIU/ml)* | 4.64±4.17 | 4.51±4.25 | 5.04±3.91 | 0.26 | |||
| Progesterone (ng/ml)* | 1.10±0.86 | 1.13±1.03 | 0.98±0.41 | 0.05 | |||
*Data presented as mean±standard deviation, independent t test. **Data presented as n (%), Chi-square test. TL, time-lapse monitoring system; CI, conventional incubator; BMI, body mass index; AFC: antral follicle count; AMH: antimullerian hormone; FSH: follicle-stimulating hormone; LH: luteinizing hormone.
Table 2.
Controlled ovarian hyperstimulation cycle characteristics in the TL and CI groups.
| Variables | Total (n=400) | CI groups (n=300) | TL groups (n=100) | p-Value |
|---|---|---|---|---|
| Duration of stimulation (days) | 14.29±1.91 | 14.33±1.98 | 14.18±1.65 | 0.45 |
| Total dose of gonadotropin (IU) | 2030.30±792.10 | 2040.83±780.14 | 2288.87±773.01 | 0.08 |
| Number of retrieved oocytes | 8.92±6.37 | 8.62±6.72 | 9.82±5.09 | 0.06 |
| Number of MII oocytes | 7.30±5.38 | 7.09±5.68 | 7.90±4.34 | 0.35 |
| Maturation rate (%) | 81.13±20.45 | 81.73±21.06 | 79.32±18.48 | 0.23 |
| Fertilization rate (%) | 91.99±18.68 | 91.52±15.90 | 85.52±23.71 | 0.12 |
| Good embryo rate (%) | 65.85±28.69 | 67.65±27.84 | 65.47±30.59 | 0.84 |
Data presented as mean±standard deviation, independent t test. TL: Time-lapse monitoring system, CI: Conventional incubator, MII: metaphase II.
Table 3.
Baseline characteristics and clinical outcomes of embryo transfer cycles in the TL and CI groups.
Table 3.
Baseline characteristics and clinical outcomes of embryo transfer cycles in the TL and CI groups.
| Variables | Total (n=150) |
CI group (n=100) | TL group (n=50) | p-Value | |
|---|---|---|---|---|---|
| Age (yr)* | 34.11±4.60 | 34.06±4.57 | 33.62±4.67 | 0.36 | |
| Age of husband (yr)* | 35.02±5.78 | 35.81±5.18 | 34.58±6.17 | 0.45 | |
| BMI (kg/m2)* | 24.72±3.81 | 24.69±3.98 | 24.78±3.52 | 0.90 | |
| AMH (ng/ml)* | 2.13±1.42 | 1.97±1.38 | 2.41±1.46 | 0.09 | |
| Causes of infertility** | |||||
| Female | 48 (32.0) | 30 (30.0) | 18 (36.0) | 0.46 | |
| Male | 67 (44.7) | 44 (44.0) | 23 (46.0) | ||
| Combined | 20 (13.3) | 14 (14.0) | 6 (12.0) | ||
| Idiopathic | 15 (10.0) | 12 (12.0) | 3 (6.0) | ||
| Sperm preparation** | |||||
| Ejaculated | 119 (79.3) | 78 (78.0) | 41 (82.0) | 0.32 | |
| Testicular | 31 (20.7) | 22 (22.0) | 9 (18.0) | ||
| Progesterone level on trigger day (ng/ml)* | 0.87±0.50 | 0.91±0.57 | 0.79±0.34 | 0.11 | |
| Endometrial thickness (mm) on trigger day* | 9.93±2.20 | 10.11±2.60 | 9.65±1.37 | 0.20 | |
| Number of transferred embryos*** | |||||
| Single embryo transfer | 12 (8.0) | 9 (9.0) | 3 (6.0) | 0.82 | |
| Double embryo transfer | 71 (47.3) | 48 (48.0) | 23 (46.0) | ||
| Triple embryo transfer | 67 (44.7) | 43 (43.0) | 24 (48.0) | ||
| Grade of transferred embryo** | |||||
| All embryos were grade I | 103 (68.7) | 68 (68.0) | 35 (70.0) | 0.73 | |
| Grade I+one or two grade II embryo/s | 26 (17.3) | 18 (18.0) | 8 (16.0) | ||
| All embryos were grade II | 21 (14.0) | 14 (14.0) | 7 (14.0) | ||
| Implantation rate (%)** | 196/337 (58.2) | 128/219 (58.4) | 68/118 (57.1) | 0.79 | |
| Clinical pregnancy rate (%)** | 75/150 (50.0) | 49/100 (49.0) | 26/50 (52.0) | 0.86 | |
| Live birth rate (%)** | 56/150 (37.3) | 35/100 (35.0) | 21/50 (42.0) | 0.76 | |
* Data presented as mean±standard deviation, independent t test. **Data presented as n (%), Chi-square test. ***Data presented as n (%), Fisher’s exact test. TL: Time-lapse monitoring system, CI: Conventional incubator, BMI: Body mass index, AMH: Antimullerian hormone.
Table 4.
Embryo development and pregnancy outcomes in subgroup analyses of TL and CI based on women’s age.
Table 4.
Embryo development and pregnancy outcomes in subgroup analyses of TL and CI based on women’s age.
| Variables | CI (%) | TL (%) | Difference (%) | p-value |
|---|---|---|---|---|
| Maturation ratea | ||||
| <35 yr | 81.4 | 80.5 | 0.9 | 0.76 |
| ≥35 yr | 81.3 | 80.4 | 0.9 | 0.79 |
| Fertilization ratea | ||||
| <35 yr | 88.6 | 92.4 | 3.8 | 0.15 |
| ≥35 yr | 89.0 | 91.0 | 2.0 | 0.28 |
| Good embryo ratea | ||||
| <35 yr | 66.3 | 70.7 | 4.4 | 0.32 |
| ≥35 yr | 64.3 | 68.3 | 6.0 | 0.08 |
| Implantation rateb | ||||
| <35 yr | 66.4 | 59.2 | 8.2 | 0.31 |
| ≥35 yr | 46.2 | 55.8 | 9.6 | 0.14 |
| Clinical pregnancy rateb | ||||
| <35 yr | 60.4 | 53.3 | 7.1 | 0.53 |
| ≥35 yr | 36.2 | 50.0 | 13.8 | 0.29 |
| Live birth rateb | ||||
| <35 yr | 45.3 | 40.0 | 5.3 | 0.85 |
| ≥35 yr | 23.4 | 38.0 | 16.6 | 0.03 |
Data presented (%), Chi-square test. aAge: <35 (n=202), ≥35 (n=198), all (n=400); bAge:<35 (n=83), ≥35 (n=67), all (n=150). TL: time-lapse incubator; CI: conventional incubator.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



