Submitted:
26 February 2026
Posted:
27 February 2026
You are already at the latest version
Abstract
Introduction: Management of fractures or osteomyelitis with accompanying soft-tissue damage in the lower extremities remains challenging. This study evaluated the effectiveness of a multidisciplinary orthoplastic approach in patients with severe bone and soft-tissue defects of traumatic or infectious origin. Particular attention was given to the role of radiological techniques—Doppler ultrasound and Angio-CT—in preoperative planning. Imaging provided essential information on the number, location, size, and branching patterns of perforators, supporting functional and aesthetic outcomes. Material and Methods: This retrospective case series included 27 patients treated between May 2021 and December 2023. Group A comprised 17 patients with acute post-traumatic bone and soft-tissue loss, and Group B included 10 patients with chronic osteomyelitis, fistula, and soft-tissue defects. Treatment involved multidisciplinary reconstruction using local and free flaps following radiological assessment. Bone stabilization was achieved with low-contact locking plates or intramedullary nails. In osteomyelitis cases, polymethyl methacrylate bone cement served as a filler and local antibiotic carrier. Functional outcomes were assessed using the Lower Limb Functional Index (LLFI). Osteomyelitis and open fractures were classified according to Cierny–Mader and Gustilo–Anderson systems. Fourteen patients undergoing propeller or ALT flaps received preoperative Doppler ultrasound and CT angiography. Results: Mean follow-up was 17.9 months in Group A and 24.4 months in Group B. Doppler ultrasound findings were consistent with Angio CT results, with no false-positive perforators confirmed intraoperatively. Ultrasound additionally provided information on flow velocity and vessel diameter, supporting surgical planning. No infection recurrence was observed, and bone union was achieved in all patients. LLFI scores improved significantly (p<0.05), and all patients reported satisfaction with outcomes. Conclusion: A collaborative orthoplastic approach ensures favorable outcomes in complex lower limb reconstruction. Radiological assessment, particularly Doppler ultrasound, plays a key role in flap planning and may serve as a reliable standalone preoperative tool. Combined radical debridement, stable fixation, flap reconstruction, and local antibiotic therapy effectively manage complex orthoplastic conditions.
Keywords:
bone and implant infections
; bone healing
; orthoplasty
; soft-tissue reconstruction
; flap reconstruction
; perforators ultrasound
; perforators Angio-CT
Introduction
Lower extremity injuries in the type of open fractures is a very complicated and difficult therapeutic issue in orthopedics and traumatology. Simultaneous bone and soft tissue injuries are problems quite common in daily practice [1,2]. The difficulties that come to be confronted are mainly the primary injury extent with open entry points for infection of the traumatic site. The main causes of extremity defects are trauma, tumors and chronic osteomyelitis [2].
Orthoplastic treatment is a multidisciplinary form of treatment that combines orthopedic and plastic surgery, and, with this kind of treatment, it is possible to use microsurgical techniques and local flaps. Combined treatment with specialists, such as radiologists, internal medicine specialists, diabetologists, microbiologists and psychologists, is necessary for therapeutic success. The goal of orthoplasty and reconstructive surgery is to choose the optimal form of treatment that provides the best functional and aesthetic results, provides a quick recovery and limits disability.
Options for lower extremity reconstruction must provide adequate coverage for exposed bone, muscle, joints and tendons while maximizing function and providing acceptable aesthetics [3]. As shown in previous publications, the debridement of infected bones and soft tissues must be as radical as necessary. This procedure seems to be crucial for good clinical outcomes [4], and many different forms of therapy can be used to achieve this goal. The latest research indicates the factors that should be taken into account when choosing the form and method of treatment. The most important prognostic factors are the patient’s condition and the characteristics of the injury [5].
In our clinical practice, we usually use regional flaps, such as propeller flaps (Figure 1) and free flap like antero-lateral thigh flap and also muscle flaps depending on the etiology and the location and size of the defect [2,4,5].
The aim of the study was to evaluate the treatment options for patients with severe bone and soft-tissue defects of a traumatic and infectious etiology of the lower extremities and that allow for improvements to the functionality of the limb and the achievement of a satisfactory aesthetic result.
Materials and Methods
This study was approved by the institutional review board (number: 41/2021), and informed consent was obtained from patients for their participation. Written informed consent for publication of information and photos was obtained from all presented study participants.
A retrospective case series of 27 patients was divided into two groups: (A) acute post-traumatic bone and soft-tissue loss (17 patients) and (B) chronic osteomyelitis with fistula and soft-tissue loss (10 patients). Acute defects are injuries—mainly open, infected fractures—with the time of their surgical supply being up to 3 weeks after the injury. Conversely, chronic defects and chronic osteitis are diseases that last longer than 6 months. We provided multidisciplinary treatment for bone and soft-tissue healing using various local and free flaps from May 2021 to December 2023. Our standard approach to preoperative planning is to use bone segment X-rays and extremity X-rays. For detailed imaging, we used computed tomography (CT) and magnetic resonance imaging (MRI); for vascular imaging, Angiography-Computed Tomography (Angio-CT); for regional flap planning, we used Doppler ultrasound [6]. We based the description of radiological procedures on articles available in the PubMed database between 2003-2024. All published studies that analysed the applicability of doppler ultrasound or Angio-CT, in the evaluation of arterial perforators and used the terms ‘arterial perforators’ OR ‘ultrasound arterial perforators’ OR ‘doppler ultrasound arterial perforators’ OR ‘angio-CT arterial perforators’ AND ‘lower limb flap’ OR ‘propeller flap’ OR ‘ALT flap’ OR ‘distal crus’ were identified and reviewed. The search limits were defined as ‘English’ (language), and ‘the beginning of a given database through to 31 December 2024’. Each patient who underwent propeller flap or Antero-Lateral Thigh flap (ALT flap) (n=14) underwent Doppler ultrasound performed by an experienced radiologist and CT angiography. In group A, 9 patients didn’t have perforators identification in the radiological examination, and they underwent a total of 9 flaps – muscle (n=6), reverse sural (n=1), flag-ship (n=1), cross-leg (n=1). In group B, 4 patients also had no perforators identification in the radiological examination, and these patients underwent a total of 6 flaps – muscle (n=4), reverse sural (n=1), flag-ship (n=1). Clinical assessments were based on the Lower Limb Functional Index [7]. All patients received empirical intravenous broad-spectrum antibiotic therapy immediately after the intraoperative collection of at least five tissue biopsies for microbiological examination (standard culture and sonication). All patients initially received empirical intravenous broad-spectrum antibiotic therapy tailored to cover the most common pathogens associated with bone and soft-tissue infections. This regimen was standardized across cases based on current clinical guidelines. However, once microbiological results were available from intraoperative tissue biopsies, antibiotic treatments were customized to target specific pathogens identified in each patient. Targeted oral antibiotic therapy was continued for 6 weeks, with CRP levels monitored every 2 weeks to assess treatment efficacy and adjust as necessary. This approach ensured both a broad initial coverage and a precise, pathogen-specific treatment strategy. PMMA with antibiotics was used both as a filler for bone infection cavities and to cover the intramedullary nails used to stabilize open fractures and intramedullary infections [8,9]. Cases of acute tibial segment injury were evaluated based on the Gustilo–Anderson classification [10], whereas patients with chronic defects and inflammation were evaluated based on the Cierny–Mader classification [11].
The inclusion criteria were as follows: patients who had simultaneous bone loss or osteomyelitis and soft-tissue defects of an acute or chronic etiology in the lower extremity. The end of the treatment process, as well as the end of the study, was healing in patients that met all three of the following criteria (i.e., healing time): (1) bone union, (2) healing of the inflammatory process and (3) healing of the flap.
Statistical analysis: The data comprised 27 patients divided into two groups: (A) acute post-traumatic bone and soft-tissue loss (17 patients) and (B) chronic osteomyelitis with fistula and soft-tissue loss (10 patients). Due to the small sample size and non-normal distribution of the data, confirmed by Shapiro–Wilk tests, we employed non-parametric statistical methods. Specifically, the Wilcoxon signed-rank test was used to evaluate changes in the Lower Limb Functional Index (LLFI) pre- and post-treatment.
The initial between-group comparisons were found to be inappropriate due to significant differences in age, baseline LLFI scores, and follow-up duration between the acute and chronic groups. These differences violate the assumption of homogeneity necessary for valid comparative analysis. The Minimal Clinically Important Difference (MCID) for LLFI scores was not defined in this study, which limits the interpretation of the practical significance of the improvements observed.
To address this, we conducted within-group analyses using the Wilcoxon signed-rank test for each group separately, focusing on the change in LLFI scores pre- and post-treatment. This approach respects the inherent differences between groups by avoiding direct comparisons and instead evaluates the efficacy of the treatment within each distinct group.
On the basis of the Shapiro–Wilk tests, we did not achieve a normal distribution for all variables; therefore, we used the Wilcoxon signed-rank test. For evaluation of perforator data P-values were calculated using Student’s t-test for continuous variables and the chi-square test for the number of vessels. The analysis of the data included descriptive statistics and was performed with Stata v. 11.0 (StataCorp, USA) and Excel (Microsoft, USA). Statistical significance was set at p < 0.05. These statistical methods were selected to align with the data characteristics, providing a reliable analysis of treatment outcomes.
Radiological Evaluation of Perforators
Doppler Ultrasound was our method of choice and depending on the result we potentially extended the diagnostics with angio-ct or much less frequently angio-mr [12].
Although for the purpose of this research, patients who qualified for propeller and ALT flaps underwent Doppler USG and angio-CT examination. An example of vascular imaging studies is shown in Figure 2.
We used an 11-18 MHz linear transducer, with the majority of examinations on peripheral artery preset. Based on the location of the skin defect in the distal calf, we focused on perforators originating either from an peroneal or tibial artery.
It is important to adjust the flow speed (PRF in cm/s) and gain scales accordingly in the color doppler or power doppler option. Gain and scale should be set so that the color fills the entire lumen of the arterial vessel, "touching" but not exceeding the inner boundary of the intima-media complex (IMT). A symptom of excessive gain is the phenomenon of "blooming" of color outside the vessel wall, into the adjacent tissues. In that case we should either lower the gain or increase the scale (PRF). From our experience, the only exception is when we want to find a perforator with a relatively low velocity and small diameter, then, sensitivity is a greater priority. Increasing gain and decreasing scale will indeed cause the appearance of many blooming artifacts, but will potentially allow identifying a small arterial perforator. Sensitivity also depends on the color box size. The smaller the color box size, the greater the sensitivity.
After determining the site of search for perforators with the orthopedists and after appropriate adjustment of the device, based on experience and data from scientific publications, one should carefully search for arteries branching off the peroneal or posterior tibial artery and visualize in B-mode the pulsating perforator that passes through the deep fascia to the subcutaneous tissue [13]. At the level of the deep fascia puncture, the vessel diameter and flow velocity should be measured. The color Doppler gate should be tilted at an angle of < 60° relative to the long axis of the vessel; it is not recommended to examine the flow spectrum in B-mode. The recommended width of the spectral gate should correspond to 30–70% of the diameter of the analyzed vessel [14]. According to Song et. al. the mean arterial flow velocity of perforators at the level of fascia penetration was 28.06 +/- 7.94 cm/s which matches with other authors with PSV of 21.9 cm/s [15,16].
It is important to document adequate flow from the perforator pedicle to the propeller flap due to the adequate blood supply and consequently nourishment of the flap in order to avoid necrosis, which are the primary reason for flap failure [15,17].
The place where the perforators pass through the deep fascia should be carefully analyzed in at least two planes to be sure that this is the real place of puncture of the fascia. Quite often, the perforating vessel in the proximal section reaches the deep fascia and then continues subfascial, adhering to the fascia, and the real puncture of the fascia occurs even a few centimeters further. It is crucial information, because it is a pivot point on which the propeller flap is rotated around its own axis. The closer the pivot point is to the skin defect, the greater the chance of covering the entire lesion as the larger portion of healthy proximal skin can be mobilized and positioned over the skin defect also the shortest possible arc of rotation can prevent postoperative complications [18,19].
Another important information is the number and direction of the perforator branches in the subcutaneous section [20].
In the distal third of the calf we usually were able to identificate one to three perforators for both medial and lateral side. The fascia puncture locations were marked with a marker on the skin.
Preoperative evaluation of potential perforators using Doppler ultrasound allows for the assessment of key parameters such as their number, location, size, origin, course, and branching patterns. This detailed assessment enables the surgeon/orthopedic to plan the extent of the operation and, in cases where suitable perforators are absent, to consider alternative treatments or extended diagnostic imaging [21,22]. Additionally, the measurement of vessel diameter and flow velocity at the point where the perforator pierces the deep fascia is critical in reducing the risk of postoperative complications, such as flap necrosis, and in selecting the optimal vessel for the procedure [13,15,19,23]. Evaluating the main arterial trunks of the lower limb is also important, it identifies any vascular anomalies as well as peripheral artery disease and potential arteries occlusion[12]. However, assessing the distal third of the lower limb can be challenging due to the progressively smaller diameter of the perforators in this region, which increases the procedure's user dependency [16,21]. According to Jakubietz et al in color doppler ultrasound false positive results were present in 21% of cases, on the other hand Gunnarsson et al showed 0 % false positive cases [13,24].
To minimize intra and postoperative complications, assessing perforators through ultrasound or CT angiography is critical [12,25,26]. Despite preoperative mapping of perforators using Doppler ultrasound, their exact location where they penetrate the fascia may differ in practice. This sometimes necessitates intraoperative adjustments to the flap design to match the actual location of the perforator [21].
Angio-CT
We used the angio-ct (CTA) method when Doppler ultrasound provided insufficient data, i.e. comprehensive assessment of the limb vascularization and simultaneous assessment of the condition of bone structures (extent of defects, presence of sequestra), vascular anomalies were visible, obstruction of the main arterial trunks, no perforators were detected or they were not suitable for propeller flap.
Performing angio-ct is associated with obvious limitations such as allergy to contrast agents or renal failure. An additional potential problem is insufficient filling of the vascular bed with a contrast agent, which makes it difficult and sometimes impossible to detect perforators in a particular area of intrest. Another limitation is the inability to determine the flow rate in the perforator, and its precise course in the subcutaneous tissue. However, it should be remembered that after performing CTA and locating the appropriate perforator, the Doppler USG examination can be repeated to assess the quality of the vessel.
Feng et al conducted a direct comparative analysis between CTA and Doppler ultrasound in terms of the usefulness and sensitivity of both examinations in the context of the evaluation of lower limb perforators. He concluded that doppler ultrasound shows a mean error of 1.11 ± 1.29 mm and CTA shows a mean error of 2.55 ± 2.63 mm in the context of the demonstrated site of deep fascia penetration and its actual location during the surgery. The success of color Doppler ultrasound has been directly related to the experience of radiologists; however, the same has not been true for CT angiography [30].
What is more, Color Doppler ultrasound is capable of detecting small perforators with a caliber up to 0.5 mm [31].
Results
This retrospective study group consisted of 27 patients. The mean age in group A was 46,9 years, and that in group B was 66,7 years (p<0,05). The mean time to healing was 8,2 in group A and 5,9 in group B (p<0,05). The mean follow-up time was 17,87 months in group A and 24,4 months in group B (p<0,05). The most common location of defects and soft-tissue- and bone-healing problems was in the lower extremity of our material, which is the distal third of the tibia segment, as recorded for 17 patients (62%) (Table 1). All patients with defects in the lower extremity qualified for surgery. During surgery, six types of flaps were used. Overall, we used a propeller flap in eleven patients (39%), a medial gastrocnemius muscle flap in six patients (21%), a soleus muscle flap in four patients (14%), ALT flap in three (10%) a retrograde sural three times (10%), flagship flap in two patients (7%) and one cross-leg flap (3%). All patients in group A required bone stabilization. In group B, eight patients required bone stabilization, and one patient required a knee endoprosthesis. We mainly used LCPs for bone stabilization, that is, 7 in group A and 4 in group B, and intramedullary nails, that is, 10 in group A and 4 in group B.
The Doppler ultrasound scan was consistent with the angio-CT scan results, confirmed intraoperatively. We did not have false positive cases. 1-2 perforators were identified in the calf Doppler ultrasound. For the propeller flap, one perforator located closest to the skin defect was used, allowing for optimal skin coverage of the defect and with appropriate morphological values. The average velocity at the level of fascia perforation was 27,89 cm/s (n=18) and the average artery diameter at the same level was 1,55 mm (n=18) (Table 2). A high standard deviation (SD) indicates substantial variability within the groups. None of the comparisons show a significant difference (p>0.05), suggesting that arterial flow velocity and vessel diameter are similar in both acute and chronic injury groups.
Twelve patients were treated with PMMA-supported antibiotics for osteomyelitis. We used gentamicin–clindamycin–vancomycin for all of these patients. During surgery, material was collected for microbiological examinations (sonication and standard culture) [32]. In most patients, more than one type of bacteria was found in the collected material. The most common pathogens were Enterococcus faecalis and methicillin-resistant coagulase-negative staphylococci (MRCNS). Mixed bacterial flora was more common in group A.
We observed no difference in the length of surgery, with the mean time in Group A was 324.3 minutes and in Group B it was 362.2 minutes (p=0.32). The length of stay in hospital averaged 4.12 weeks in group A and 3.44 weeks in group B (p=0.21). In four group A and three group B patients, we were forced to perform a flap revision, mainly because of venous congestion. For the first few cases, we used hirudin therapy, but in time, we abandoned this treatment due to Pseudomonas infection (two cases in group A). We treated subsequent cases of venous congestion with punctures and injections of heparin and intravenous dextran and dexaven. If the venous congestion persisted despite interim treatment, we performed revision surgery. (Table 3).
No major complications such as flap failure, wound dehiscence, or infection recurrence were observed during the follow-up period. Patient satisfaction was assessed through structured interviews and visual analog scales, with all patients reporting high levels of satisfaction regarding both the functional and aesthetic results of their treatment. These data underscore the effectiveness of combining radiologically guided flap planning and multidisciplinary care in achieving favorable clinical outcomes.
The LLFI was used to assess patients’ quality of life and satisfaction before surgery and at the end of treatment (healing time) during follow-up in the ambulatory clinic. The LLFI was significantly (p<0.05) higher after surgery, with a mean preoperative score of 9.53 (±6.09) in group A and 27.0 (±12.08) in group B, and 66.26 (±8.09) and 69.6 (±9.02) for the postoperative groups, respectively. A statistically significant (p<0,05) difference was observed in the level of the LLFI scale before reconstructive surgery, where the LLFI was 9.53 (±6.09) in group A and 27.0 (±12.08) in group B. The difference was 17.47. This result is, one might say, obvious because of the comparison of an acute and sudden traumatic loss of limb function and experiencing a state of chronic limited functioning in which certain compensatory systems (“habituation”, bracing and the acceptance of the disease) have already taken effect. After orthoplastic treatment, there was no statistically significant difference in the LLFI scales for the two groups (Table 4).
Discussion
As highlighted, the treatment of patients with bone and soft-tissue defects is very difficult. Good qualifications and properly performed operations are crucial. Many flap-based surgical techniques are described in the literature, and each has its advantages and disadvantages. There are three permanent perforators on the lower extremity that allow for the proper realization of the propeller flap. The perforating vessel should be as close as possible to the beginning of the skin defect. The flap must be at least 1 cm longer and at least 0.5 cm wider than the defect. It is very important to cut the perforator to a sufficient length past the fascia to avoid twist points [6]. Song et al. showed how significant the direction of the rotation of a flap is. The correct direction of rotation can reduce the risk of flap loss, especially with large flaps [33]. The other options are free flaps, for example, an ALT. Wong et al. evaluated an anterolateral thigh flap. In their opinion, an ALT can reliably and safely be harvested in most patients [34]. The purported difficulty with the use of this flap lies in the anatomical variations that may render this flap unreliable. Despite anatomic inconstancy, an anterolateral thigh free flap is relatively easy to harvest and utilize. Its pedicle can be used to bridge a vascular defect in the extremity [35]. Other free flaps are latissimus dorsi muscle flaps and dorsali pedis artery-based flaps. These are very good flaps, but our experience with cases of infectious and post-traumatic tissue changes speaks for the use of local flaps in the first place due to their easy availability, low cost and shorter operating time and, perhaps, a lack of experience in making free microsurgical flaps. Innocenti et al. compared the costs and efficiency of free and propeller flaps. Complications arose for 6% of the free flaps and 3.7% of the propeller flaps. The average cost of a free flap is EUR 5077.5 per patient, and the cost of a propeller flap is EUR 1595.6 per patient. The choice of surgical option should only be made after a careful evaluation of the soft tissue surrounding the defect. For small and medium defects in healthy extremities, a propeller flap should be used. Free flaps should be chosen for large defects caused by trauma or vascular disease [36]. Propeller flaps have one more limitation. They should be avoided if underlying metalwork is required for bony fixation [37]. Furthermore, as our results show, local flaps are a very good solution for the complex treatment of soft-tissue damage and defects of various etiologies. A distal-based sural flap is a useful alternative to free tissue transfer for simple and complex defects in the lower third tibia segment, foot and ankle. This procedure includes the lesser saphenous vein, used to augment venous drainage. The flap should be used with caution in elderly patients and those with venous insufficiency. Patients with venous insufficiency have been found to have a nine times greater risk of complications [38]. A gastrocnemius flap is widely used to reconstruct the knee and upper tibia segment, whereas a soleus flap is used to cover middle and lower tibia segment defects. The soleus muscle can be divided longitudinally and used as a hemisoleus flap. Muscle flaps fill defects with a significant soft-tissue thickness; however, they show scarring, contractures and complications at the donor site [39]. Al-Mugaren et al. published an algorithm of their approach to lower extremity defects and the selection of appropriate flaps for reconstruction [40]. They consider the propeller blade and keystone as “new trends” in reconstructive surgery. Nevertheless, classic flaps, such as gastrocnemius flaps, soleus flaps and inverted calf flaps, as well as free microsurgical flaps, also have their advantages and are used in severe defects of the lower extremity. In the end, flap choice should be made depending on the defect’s etiology, resources available, surgeon’s experience and the patients’ comorbidities and expectations [41]. There are also treatments that do not require the use of microsurgery. In the absence of appropriate equipment, experienced surgeons use external fixators, and bone transport and soft-tissue distraction can also be used, although they have no advantages over microvascular techniques [42].
Orthoplasty combines orthopedic treatment (bone loss and osteomyelitis) and plastic treatment (soft-tissue loss). In cases of patients with osteomyelitis, antibiotic cement-coated interlocking nails seem to be the best option for treatment. They are advantageous over external fixators, as they eliminate the complications of external fixators and have good patient compliance [43]. The antibiotics that are used should be heat-stable, exhibit broad-spectrum activity, have good elution properties from the cement and have low allergenicity [44]. In our study, we used gentamycin–clindamycin–vancomycin and a PMMA as a donor. The use of antibiotic-impregnated cement-coated intramedullary nails for the infected non-union of tibia and femur fractures has been well documented in the literature. It may also reduce the morbidity of the two surgical procedures and inpatient admissions required for the two-stage procedures or for the application and removal of external fixators to that of a single procedure and inpatient admission [45]. Lan et al. reported that patients with a Gustilo–Anderson III open tibia fracture treated with the Masquelet technique have a shorter average union time and a lower risk of infection than patients treated with a vascularized bone graft [46]. Sometimes, because of the removal of a large amount of tissue, it is necessary to perform massive reconstructive surgery [4]. In difficult cases that do not respond to treatment or in departments without an experienced flap surgeon, other methods of therapy should be considered, one of which is bone transport with the Ilizarov technique. Bone transport treatment with a soft-tissue transport technique can provide satisfactory clinical results in most cases [47]. Novel treatment methods, such as an osteoinductive autologous bone graft substitute, are described. The aim of this method is to accelerate bone regeneration [48]. The clinical evidence regarding the use of bone morphogenetic proteins in the treatment of fractures, non-unions and osteonecrosis is still controversial, and there are not enough clinical reports [49]. In our material, there were no complications of non-union, so we did not have to use another form of treatment.
Various methods of delivering antibiotics have been investigated. Patel et. al. showed that PMMA beads with antibiotics are very effective in the treatment of chronic osteomyelitis and in preventing infection recurrence [50]. The sonication of material collected during an operation is a well-known technique used for implant-associated infection. This method, which is based on the application of long-wave ultrasounds radiating in a liquid medium, has been recently validated for the diagnosis of prosthetic joint infections [32]. The treatment of patients with reconstructions because of extremity fractures is a long-term process. After their first operation, patients often require revision. Aydogan et. al. showed that, after revision, patients had poor outcomes, had a low quality of life and needed a long time to go back to work. Patients suffering from flap ischemia have worse outcomes than those without flap ischemia [51]. In our study, the complications that occurred after primary surgeries were due to venous congestion, which remains a major postoperative complication [52]. Venous congestion can cause necrosis of the distal flap. In the first few cases, we used hirudin therapy according to a study conducted by de Chalain. Later, we switched from the use of hirudinotherapy to injections with heparin and an intravenous supply of dextran and dexaven.
Radiology plays a crucial role in lower leg microsurgery by providing essential imaging support that enhances surgical planning, execution, and postoperative evaluation. Radiological imaging assists in mapping the vascular supply to the lower leg. Techniques like Doppler ultrasound and angiography allow surgeons to visualize blood vessels, ensuring that the surgical site will receive adequate blood supply post-surgery. The anatomical study of lateral lower leg perforators provides significant insights into their distribution, characteristics, and clinical applications. The study revealed that 73.1% of the perforators had a septocutaneous course, while 26.9% were musculocutaneous. This suggests that septocutaneous perforators may be more prevalent in the lateral lower leg, which could influence surgical approaches for flap harvesting. The anterior tibial artery was identified as the primary source of perforators (53.0%), followed by the peroneal artery (41.6%) and the popliteal artery (5.1%). Notably, popliteal artery perforators were significantly larger than those from the other arteries, indicating their potential utility in reconstructive procedures. Perforators in the proximal third were significantly longer and larger compared to those in the distal third. Musculocutaneous perforators were found to be longer and wider than septocutaneous ones, which may influence the choice of perforator for different types of tissue transfer.[53]
The article by Lichte et al. discusses the use of routine preoperative color Doppler duplex ultrasound scanning to localize perforators in ALT flaps. The study found a strong correlation between the accuracy of identification and the patients' body mass index (BMI), but not with age or sex. The authors conclude that color Doppler ultrasound is a reliable and effective method for identifying perforators in ALT flaps, suggesting it could become a standard procedure in preoperative planning. The method is non-invasive, cost-effective, and avoids radiation exposure, making it favorable compared to other imaging techniques. [54] The use of Color Duplex Sonography (CDS) for preoperative localization of perforator arteries improved surgical accuracy and facilitated the design and execution of the flap procedures. Liu et al. investigates the clinical efficacy of using bilateral anterolateral thigh perforator (ALTP) flaps for repairing large skin and soft tissue defects in the extremities. Twelve patients with defects ranging from 18.0×11.0 cm² to 38.0×15.0 cm², caused by various injuries, underwent this surgical procedure. The study employed CDS to accurately locate perforator arteries preoperatively, which improved surgical outcomes. [55] The study by Tang et al. focuses on improving the localization of perforators in the ALT for soft tissue reconstructive surgery using augmented reality (AR) combined with CTA. The research involved 14 patients who underwent CTA mapping of their lateral circumflex femoral artery (LCFA) and its perforators, which were then projected onto the skin surface during surgery for accurate flap harvesting. The combined CTA and AR technique achieved a 90.2% accuracy rate and a 97.4% sensitivity in identifying perforators, significantly outperforming handheld Doppler ultrasound, which had an accuracy of 82.4%. [56] The study conducted by Ahmad Alwi et al. provides valuable insights into the feasibility of using the medial plantar artery flap for diabetic patients with suspected vascular insufficiency. The study found that more than 50% of the lower limbs in diabetic patients with vascular compromise still exhibited a patent medial plantar artery. This suggests that the medial plantar artery flap may be a viable option for reconstructive procedures in this patient population. The findings highlight the necessity of conducting a CTA prior to surgical intervention to accurately assess the patency of the medial plantar artery. The study demonstrated that bedside clinical assessments, such as palpation and hand-held Doppler evaluations of the posterior tibial artery, were inadequate predictors of medial plantar artery patency. [57]
Each department should develop a scheme for the prevention and treatment of venous congestion after reconstructive surgery. This study has some limitations, such as a retrospective design and a small and heterogeneous group of patients.
Our findings highlight the critical role of Doppler ultrasound and Angio-CT in enhancing surgical precision and reducing intraoperative uncertainty. The high concordance between preoperative Doppler ultrasound and intraoperative findings (with no false positives confirmed intraoperatively) suggests that these imaging modalities can serve as reliable tools for perforator localization, thereby minimizing operative time and optimizing flap success rates. In our study, we observed no false positive cases in the preoperative identification of arterial perforators using both color Doppler ultrasound and CT angiography. This result contrasts with the findings of Jakubietz et al., who reported a 21% false positive rate with Doppler ultrasound [13]. Several factors may explain this discrepancy. First, the accuracy of Doppler imaging is highly dependent on operator skill and technique; in our study, all examinations were performed by experienced sonographers using standardized, multi-planar protocols. Additionally, technological advances since the time of Jakubietz et al.'s publication such as improved probe resolution and Doppler sensitivity likely contributed to enhanced detection accuracy. Our findings are consistent with those of Gunnarsson et al., who similarly reported a 0% false positive rate, suggesting that with current imaging standards and experienced operators CDU is a highly reliable tool for preoperative perforator mapping [24].
Furthermore, the consistent application of these assessments facilitated ongoing outcome monitoring and improvements in surgical planning, aligning with the continuous quality improvement framework. This approach underscores the importance of multidisciplinary collaboration and data-driven decision-making in advancing the quality of complex orthoplastic reconstructions.
Conclusions
Orthoplastic treatment is a challenging process for the surgeon. On the one hand, there is chronically infected bone with fistula and, on the other hand, acute high-energy trauma with soft-tissue and bone loss. Either case requires the major involvement of a multidisciplinary team and adequate preparation of the patient for a very complex and sometimes lengthy treatment process fraught with a number of possible complications. The end result is always a cure and the best long-term good functional and aesthetic outcomes. Local flaps combined with modern bone fixation and local antibiotic supports such as PMMA have proven to be excellent in treating complex cases of orthoplasty patients. The orthoplastic approach is therefore an effective and efficient but very challenging process for treating both acute and chronic soft-tissue defects and bone infections. The radiological findings were combined with clinical evaluations, including microbiological assessments and functional outcomes measured by the Lower Limb Functional Index (LLFI). This multidisciplinary approach not only facilitated surgical planning but also contributed to the overall treatment strategy, ensuring that both functional and aesthetic outcomes were prioritized. For preoperative evaluation, propeller flap ultrasound is sufficient in preoperative scanning, and in doubtful cases, evaluation in angio-CT is sometimes necessary. Systematic and integrated approach to imaging that plays a pivotal role in the management of complex lower extremity injuries. The use of various imaging modalities allows for a comprehensive understanding of the anatomical and pathological features, which is crucial for optimizing surgical outcomes in orthoplastic treatment. Of course, high-quality controlled studies in larger groups of patients are needed to assess its long-term safety and efficacy.
To enhance the evaluation of treatment effectiveness, future studies should integrate a broader range of Patient Reported Outcomes (PROs). These could include measures such as pain levels, mobility, daily activity limitations, and psychological well-being.
Understanding these dimensions would provide valuable insights into the real-world effectiveness of the interventions and help tailor treatments to better meet patient needs. Gathering detailed PROs can also guide improvements in clinical practice and patient care strategies, ensuring a more patient-centered approach to treatment.
While our study demonstrates promising results regarding the role of radiological assessments, such as Doppler ultrasound and Angio-CT, in preoperative planning for complex lower limb reconstructions, certain limitations must be acknowledged. The retrospective design of this case series introduces potential selection bias and limits causal inferences. The heterogeneity of the patient cohort varying injury severity, defect size, and comorbidities may affect the generalizability of our findings. Additionally, in some cases, the radiological identification of perforators was unsuccessful, necessitating alternative intraoperative strategies.
These limitations highlight the need for prospective, controlled studies to validate the efficacy of standardized radiological assessment protocols. Future research should aim to develop and implement standardized criteria for perforator identification and flap planning, which could improve preoperative accuracy and operative outcomes. Incorporating continuous quality monitoring tools will also be essential to track process efficiencies and patient outcomes over time, improvement quality in orthoplastic surgical practice.
Author Contributions
Conceptualization, K.K. and M.S.; data curation, K.K., M.S. and R.G.; formal analysis, K.K., M.S., R.G., K.CH, Ż.N. and M.Z.; investigation, K.K., M.S. and R.G.; methodology, K.K. and M.S.; project administration, K.K., M.S., R.G., M.Z. and J.Cz.; resources, K.K., M.S. and R.G.; software, K.K., K.CH, Ż.N and M.S.; supervision, R.G., M.Z. and J.Cz.; validation, M.Z. and J.Cz.; visualization, K.K. and M.S.; writing—original draft, K.K., K.CH, Ż.N and M.S.; writing—review and editing, K.K., M.S., R.G., M.Z., K.CH, Ż.N and J.Cz. All authors have read and agreed to the published version of the manuscript.
Funding
No external funding contributed to this work.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the Medical Centre of Postgraduate Education (41/2021, 21.05.2021, Warsaw).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The underlying data from the electronic data base is available on demand.
Conflicts of interest
The authors declare no conflict of interest.
References
- Nelson J, Fischer J, Brazio P, Kovach S, Rosson G, Rad A. A review of propeller flaps for distal lower extermity soft tissue recostruction: Is flap loss too high? Microsurgery 2013 Oct; 33(7):578-86.
- Soltanian H, Garcia R, Hollenbeck S. Current Concepts in Lower Extremity Reconstruction. Plast reconstr Surg. 2015 Dec;136(6):815e-829e.
- Mastroianni M, Leto Barone AA, Shanmugarajah K, Leonard DA, Di Rosa L, Feingold RS et al. Lower extremity soft tissue defect reconstruction with the serratus anterior flap. Microsurgery 2014 Mar;34(3):183-7.
- Sambri A, Pignatti M, Tedeschi S, Lozano Miralles ME, Giannini C, Fiore M, Filippini M, Cipriani R, Viale P, De Paolis M. Combined Orthoplastic Approach in Fracture-Related Infections of the Distal Tibia. Microorganisms. 2022 Aug 12;10(8):1640.
- Battiston B, Cristina Castrogiovanni M, Beltramo Ch. The orthoplastic approach in the mangled lower limb. Lo Scalpello Journal. 2023. Apr; 37:4-8.
- Ibrahim RM, Gunnarsson GL, Akram J, Sørensen JA, Thomsen JB. Color Doppler ultrasonography targeted reconstruction using pedicled perforator flaps—a systematic review and meta-analysis. European Journal of Plastic Surgery 2018;41(5):495-504.
- Bejer A. et al. Polish Cross-Cultural Adaptation of the Lower Limb Functional Index (LLFI) Demonstrates a Valid Outcome Measure for the Lower Limb Region and Joints. Int. J. Environ. Res. Public Health 2021, 18(18), 9894; [CrossRef]
- Kalbas Y, Klingebiel F, Pape H-Ch. Antibiotic coated nails: Rationale, development, indications and outcomes. Journal of Orthopaedic Surgery 2022;30(3) 1–7;. [CrossRef]
- Walter N, Rupp M, Krückel J, Alt V. Individual and commercially available antimicrobial coatings for intramedullary nails for the treatment of infected long bone non-unions: a systematic review. Injury 2022; 53S3 S74–S80.
- Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 1976;58:453–458.
- Cierny, G.; Mader, J.T.; Penninck, J.J. A clinical staging system for adult osteomyelitis. Clin. Orthop. Relat. Res. 2003, 10, 7–24.
- Gravvanis A, Petrocheilou G, Tsoutsos D, Delikonstantinou I, Karakitsos D. Integrating imaging techniques in lower limb microsurgical reconstruction: focusing on ultrasonography versus computed tomography angiography. In Vivo. 2013 May-Jun;27(3):371-5. PMID: 23606693.
- Gunnarsson GL, Tei T, Thomsen JB (2016) Color Doppler ultrasonography–targeted perforator mapping and angiosome-based flap reconstruction. Ann Plast Surg 77:464–468.
- Zubair A, Lotfollahzadeh S. Peripheral Arterial Duplex Assessment, Protocols, and Interpretation. PMID: 35015455.
- Song S, Jeong HH, Lee Y, Powers H, Suh YC, Christoffi P, Suh HP, Hong JPJ. Direction of Flap Rotation in Propeller Flaps: Does It Really Matter? J Reconstr Microsurg. 2019 Oct;35(8):549-556. Epub 2019 May 10. PMID: 31075803. [CrossRef]
- Lovětínská, Vanesa & Sukop, Andrej & Sulženko, Jakub & Hora, Adam & Patzelt, Matej & Kožnar, Boris & Kovačič, Karol & Kamenistý, Michal & Kučerák, Jozef. (2024). Stable Arterial Perforators Mapping in Lower Leg Using Color-Coded Doppler Sonography, Acoustic Doppler, and Thermal Imaging Camera in Patients Undergoing Digital Subtraction Angiography. Journal of Reconstructive Microsurgery Open. 00. 10.1055/a-2241-2323.5381852.
- Ozdemir R, Kocer U, Sahin B, Oruc M, Kilinc H, Tekdemir I. Examination of the skin perforators of the posterior tibial artery on the leg and the ankle region and their clinical use. Plast Reconstr Surg. 2006 Apr 15;117(5):1619-30. PMID: 16641734. [CrossRef]
- Teo TC. The propeller flap concept. ClinPlast Surg 2010; 37: 615–626.
- Ibrahim RM, Gunnarsson GL, Akram J, Sørensen JA, Thomsen JB. Color Doppler ultrasonography targeted reconstruction using pedicled perforator flaps-a systematic review and meta-analysis. Eur J Plast Surg. 2018;41(5):495-504. Epub 2018 Jun 29. PMID: 30294069; PMCID: PMC6153870. [CrossRef]
- Yu D, Hou Q, Liu A, Tang H, Fang G, Zhai X, Jiang H, Cao X. Delineation the anatomy of posterior tibial artery perforator flaps using human cadavers with a modified technique. Surg Radiol Anat. 2016 Nov;38(9):1075-1081. Epub 2016 Apr 15. PMID: 27083588. [CrossRef]
- Shen L, Liu Y, Zhang C, Guo Q, Huang W, Wong KKL, Chang S. Peroneal perforator pedicle propeller flap for lower leg soft tissue defect reconstruction: Clinical applications and treatment of venous congestion. J Int Med Res. 2017 Jun;45(3):1074-1089. Epub 2017 Mar 27. PMID: 28345420; PMCID: PMC5536429. [CrossRef]
- Bhattacharya V, Deshpande SB, Watts RK, Reddy GR, Singh SK, Goyal S. Measurement of perfusion pressure of perforators and its correlation with their internal diameter. Br J Plast Surg 2005;58 (06):759–764.
- Gravvanis A, Karakitsos D, Dimitriou V, Zogogiannis I, Katsikeris N, Karabinis A and Tsoutsos D: Portable duplex ultrasonography: A diagnostic and decision-making tool in reconstructive microsurgery. Microsurgery 30: 348-353, 2010.
- Jakubietz RG, Jakubietz MG, Grünert JG, et al. [Propeller flaps: the reliability of preoperative, unidirectional Doppler sonography]. Handchir Mikrochir Plast Chir. 2011;43:76–80.
- Evaluation of the vessels of the lower leg before microsurgical fibular transfer. Part I: anatomical variations in the arteries of the lower leg; Frank Hölzle.
- Tsukino A, Kurachi K, Inamiya T and Tanigaki T: Preoperative color Doppler assessment in planning of anterolateral thigh flaps. Plast Reconstr Surg 113: 241-246, 2004.
- Higueras Sun ̃e ́ MC, Lo ́pez Ojeda A, Narva ́ez Garcı ́a JA, et al. Use of angioscanning in the surgical planning of perforator flaps in the lower extremities. J Plast Reconstr Aesthet Surg 2011; 64: 1207–1213.
- Ribuffo D, Atzeni M, Saba L, et al. Clinical study of peroneal artery perforators with computed tomographic angiography: implications for fibular flap harvest. Surg Radiol Anat 2010; 32: 329–334.
- Fukaya E, Saloner D, Leon P, et al. Magnetic resonance angiography to evaluate septocutaneous perforators in free fibula flap transfer. J Plast Reconstr Aesthet Surg 2010; 63: 1099–1104.
- Tenekeci, G. (2018). Perforator Flaps: Principles and Techniques. InTech. [CrossRef]
- Feng S, Min P, Grassetti L, Lazzeri D, Sadigh P, Nicoli F, Torresetti M, Gao W, di Benedetto G, Zhang W, Zhang YX. A Prospective Head-to-Head Comparison of Color Doppler Ultrasound and Computed Tomographic Angiography in the Preoperative Planning of Lower Extremity Perforator Flaps. Plast Reconstr Surg. 2016 Jan;137(1):335-347. PMID: 26710036. [CrossRef]
- Oliva A, Pavone P, D'Abramo A, Iannetta M, Mastroianni CM, Vullo V. Role of Sonication in the Microbiological Diagnosis of Implant-Associated Infections: Beyond the Orthopedic Prosthesis. Adv Exp Med Biol. 2016;897:85-102.
- Song S, Jeong HH, Lee Y, Powers H, Suh YC, Christoffi P et al. Direction of Flap Rotation in Propeller Flaps: Does It Really Matter? J Reconstr Microsurg. 2019 Oct;35(8):549-556.
- Wong C, Wei F. Anterolateral Tigh Flap. Head Neck. 2010 Apr;32(4):529-40.
- Lim J, Kwon H, Lee K, Pak C. Immediate Lower Extremity Reconstruction Using an Anterolateral Thigh Free Flap With Simultaneous Interposition Graft of Descending Branches of Lateral Circumflex Femoral Vessels. Int J Low Extrem Wounds. 2019 Mar;18(1):89-93.
- Innocenti M, Dell’Acqua I, Famiglietti M, Vignini L, Menichini G. Free perforator flaps vs propeller flaps in lower extremity reconstruction: A cost/effectiveness analysis on a series of 179 cases. Injury. 2019 Dec;50 Suppl 5:S11-S16.
- Guillier D, Sapino G, Schaffer C, Borens O ,Thein E, Bramhall RJ, et al. Lower extremity reconstruction involving osteosynthesis material: A retrospective study on propeller flaps outcomes, Injury. 2021 Oct;52(10):3117-3123.
- de Blacam C, Colakoglu S, Ogunleye AA, Nguyen JT, Ibrahim AM, Lin SJ et al. Risk factors associated with complications in lower-extremity reconstruction with the distally based sural flap: a systematic review and pooled analysis. J Plast Reconstr Aesthet Surg. 2014 May;67(5):607-16.
- Pu LLQ. Further experience with the medial hemisoleus muscle flap for soft-tissue coverage of a tibial wound in the distal third of the leg. Plast Reconstr Surg. 2008 Jun;121(6):2024-2028.
- AlMugaren FM, Pak CJ, Suh HP, Hong JP. Best Local Flaps for Lower Extremity Reconstruction. Plast Reconstr Surg Glob Open. 2020 Apr; 8(4): e2774.
- Scampa M, Mégevand V, Suva D, Kalbermatten DF, Oranges CM. Free versus Pedicled Flaps for Lower Extremity Reconstruction: A Meta-Analysis of Comparative Studies. J Clin 2022 Jun 25;11(13):3672.
- Xu Y-Q, Fan X-Y, He X-Q, Wen H-J. Reconstruction of massive tibial bone and soft tissue defects by trifocal bone transport combined with soft tissue distraction: experience from 31 cases. BMC Musculoskeletal Disorders. 2021 Jan 7;22(1):34.
- Bhatia C, Tiwari AK, Sharma SB, Thalanki S, Rai A. Role of Antibiotic Cement Coated Nailing in Infected Nonunion of Tibia. Malays Orthop J. 2017 Mar;11(1):6-11.
- van Vugt TAG, Arts JJ, Geurts JAP. Antibiotic-Loaded Polymethylmethacrylate Beads and Spacers in Treatment of Orthopedic Infections and the Role of Biofilm Formation. Front Microbiol. 2019 Jul 25;10:1626.
- Thonse R, Conway J. Antibiotic cement-coated interlocking nail for the treatment of infected nonunions and segmental bone defects. J Orthop Trauma. 2007 Apr;21(4):258-68.
- Lan C-Y, Lien P-H, Lien Y-T, Lin C-H, Hsu C-C, Lin C-H et al. Comparison of the clinical outcomes between vascularized bone graft and the Masquelet technique for the reconstruction of Gustilo type III openvtibial fractures. BMC Musculoskeletal Disorders. 2022 Dec 1;23(1):1036.
- Xu YQ, Fan XY, He XQ, Wen HJ. Reconstruction of massive tibial bone and soft tissue defects by trifocal bone transport combined with soft tissue distraction: experience from 31 cases. BMC Musculoskelet Disord. 2021 Jan 7;22(1):34. Erratum in: BMC Musculoskelet Disord. 2021 Feb 2;22(1):130. [CrossRef]
- Dumic-Cule I, Peric M, Kucko L, Grgurevic L, Pecina M, Vukicevic S. Bone morphogenetic proteins in fracture repair. Int Orthop. 2018 Nov;42(11):2619-2626. [CrossRef]
- Krishnakumar GS, Roffi A, Reale D, Kon E, Filardo G. Clinical application of bone morphogenetic proteins for bone healing: a systematic review. Int Orthop. 2017 Jun;41(6):1073-1083. [CrossRef]
- Patel KH, Bhat SN, H M. Outcome analysis of antibiotic-loaded poly methyl methacrylate (PMMA) beads in musculoskeletal infections. J Taibah Univ Med Sci. 2020 Nov 19;16(2):177-183.
- Aydogan E, Langer S, Josten C, Fakler J, Henkalmann R. Outcomes of tissue reconstruction in distal lower leg fractures: a retrospective cohort study. BMC Musculoskeletal Disorders. 2020 Dec 1;21(1):799.
- Shen L, Liu Y, Zhang Ch, Guo Q, Huang W, Loong Wong KK et al. Peroneal perforator pedicle propeller flap for lower leg soft tissue defect reconstruction: Clinical applications and treatment of venous congestion. Journal of International Medical Research 2017 Jun; 45(3): 1074–1089.
- Hupkens P, Schijns W, Van Abeelen M, Kooloos JG, Slater NJ, Ulrich DJ. Lateral lower leg perforator flaps: an anatomical study to localize and classify lateral lower leg perforators. Microsurgery. 2015 Feb;35(2):140-7. Epub 2014 Sep 15. PMID: 25219380. [CrossRef]
- Lichte J, Teichmann J, Loberg C, Kloss-Brandstätter A, Bartella A, Steiner T, Modabber A, Hölzle F, Lethaus B. Routine preoperative colour Doppler duplex ultrasound scanning in anterolateral thigh flaps. Br J Oral Maxillofac Surg. 2016 Oct;54(8):909-913. Epub 2016 Jun 25. PMID: 27349963. [CrossRef]
- Liu C, Gao F, Liu XL, Wu GZ. A clinical study of ultrasonic localization-assisted combined transplantation of a bilateral anterolateral thigh perforator flap for the repair of large-area skin and soft tissue defects of the extremities. Eur Rev Med Pharmacol Sci. 2023 Apr;27(7):2871-2880. PMID: 37070887. [CrossRef]
- Tang Y, Guo Q, Li X, Huang Y, Kuang W, Luo L. Augmented reality-assisted systematic mapping of anterolateral thigh perforators. BMC Musculoskelet Disord. 2022 Dec 2;23(1):1047. PMID: 36457082; PMCID: PMC9716696. [CrossRef]
- Ahmad Alwi AA, Low CL, Kow RY, Tajudin FA, Lim BC, Halim Lim AA, Md Ralib Md Raghib AR. Evaluation of Feasibility of Medial Plantar Artery Flap With Computed Tomography Angiography in Diabetic Patients: A Pilot Radioanatomic Study. Cureus. 2023 Oct 31;15(10):e48067. PMID: 38046487; PMCID: PMC10689118. [CrossRef]
Figure 1.
A 41-year-old man suffered a factory accident, resulting in an open fracture Gustilo–Anderson IIIb of the right distal tibia segment, treated with ex-fix: (a) proeprative condition of the skin and surrounding tissues, clinical soft-tissue defect with an open, infected tibia bone (b) intraoperative view of the propellar flap with prepared perforator; (c) healed propellar flap with good coverage. The time to follow-up was 16 months.
Figure 1.
A 41-year-old man suffered a factory accident, resulting in an open fracture Gustilo–Anderson IIIb of the right distal tibia segment, treated with ex-fix: (a) proeprative condition of the skin and surrounding tissues, clinical soft-tissue defect with an open, infected tibia bone (b) intraoperative view of the propellar flap with prepared perforator; (c) healed propellar flap with good coverage. The time to follow-up was 16 months.
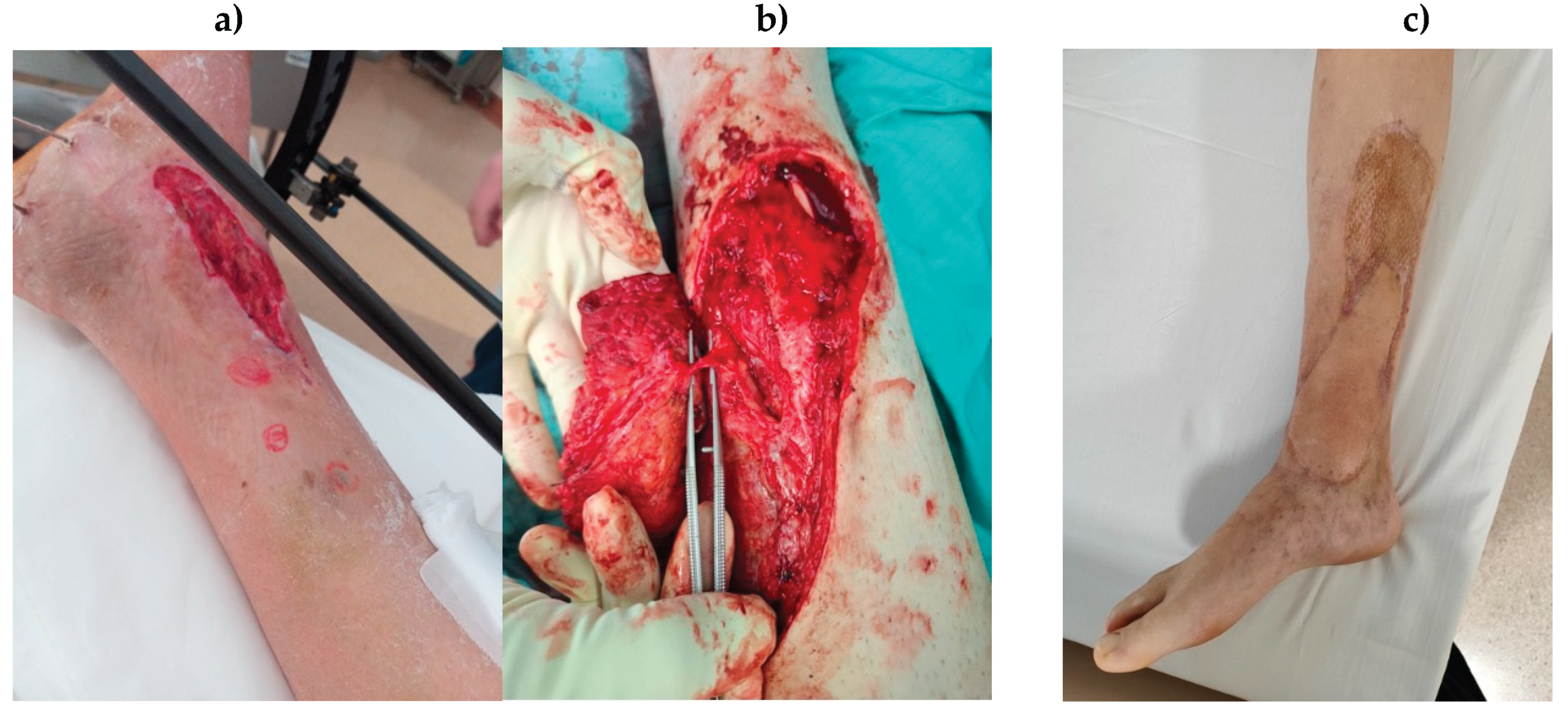
Figure 2.
A 49-year-old male with acute osteomyelitis of distal tibia: (a) Doppler ultrasound examination of distal crus perforator branching from posterior tibial artery. Evaluation of perforator diameter at the level of fascia penetration; (b) evaluation of velocity and flow spectrum at the level of fascia penetration; (c) same perforator seen on angio-CT with accompanying vein (arrow).
Figure 2.
A 49-year-old male with acute osteomyelitis of distal tibia: (a) Doppler ultrasound examination of distal crus perforator branching from posterior tibial artery. Evaluation of perforator diameter at the level of fascia penetration; (b) evaluation of velocity and flow spectrum at the level of fascia penetration; (c) same perforator seen on angio-CT with accompanying vein (arrow).
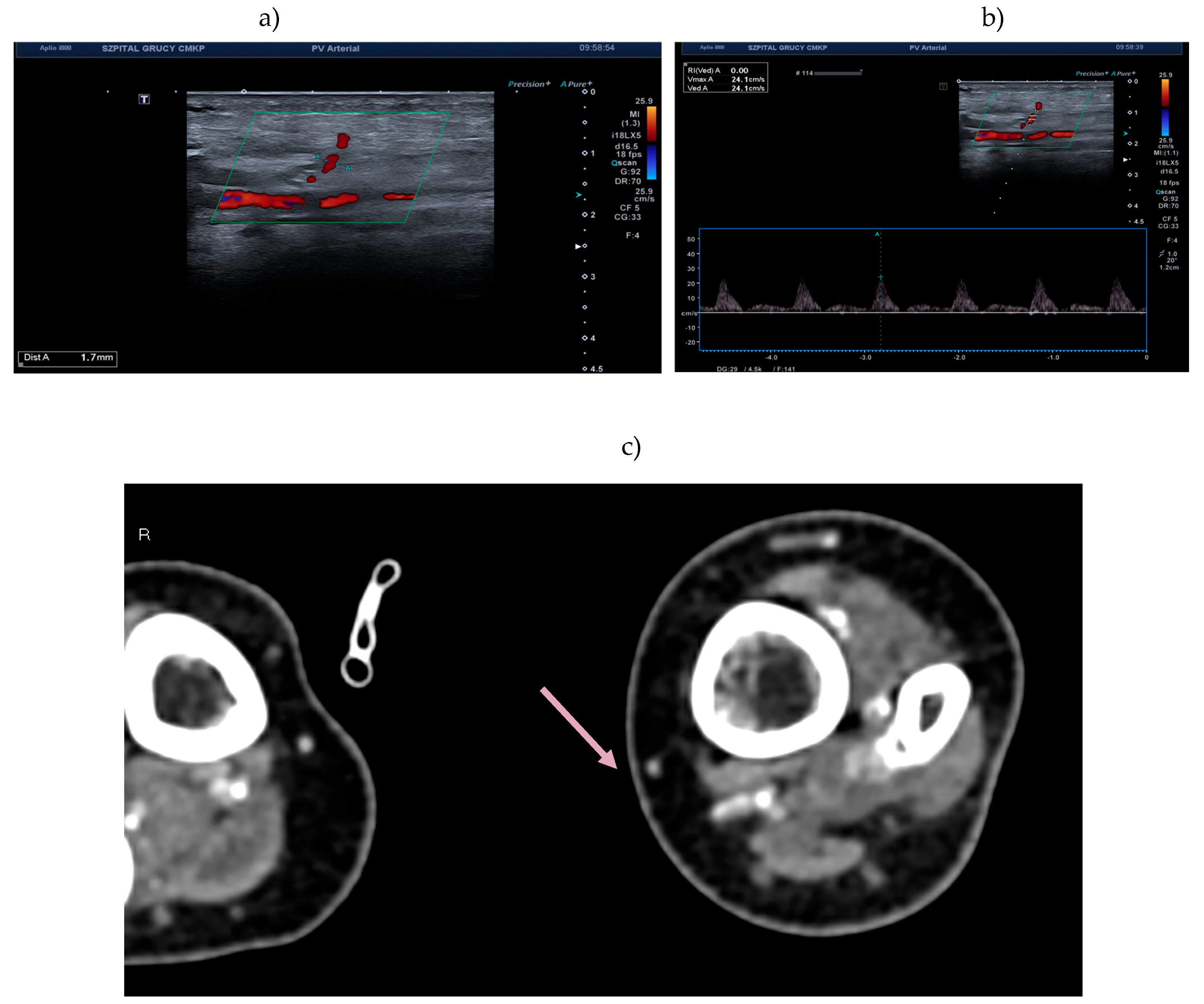

Table 1.
Demographic data of patients who underwent lower extremity reconstruction.
| Group A (Acute Damage) n=17 |
Group B (Chronic Damage) n=10 |
p-Value | |
|---|---|---|---|
| Mean age; years (SD) | 46,9 (±13,25) | 66,7 (±15,06) | 0,0056 |
| Sex | Female: 2 Male: 15 |
Female: 5 Male: 5 |
n/a |
| Side | Right: 12 Left: 5 |
Right: 6 Left: 4 |
n/a |
| Drug/disease | Nicotine: 9 | Nicotine: 3 RZS: 1 |
n/a |
| Classification | Gustilo–Anderson: II – 5 IIIa – 1 IIIb – 8 IIIc - 3 |
Cierny–Mader: II – 2 III – 5 IV - 3 |
n/a |
| Localization Mean time to healing; mth (SD) |
Proximal tibia seg.: 3 Central tibia seg.: 2 Distal tibia seg.: 12 8,2 (±6,89) |
Proximal tibia seg.: 3 Central tibia seg.: 2 Distal tibia seg.: 5 5,9 (±4,81) |
n/a 0,04 |
| Mean time to follow-up; mth (SD) | 17,87 (±8,46) | 24,4 (±9,36) | 0,043 |
mth, month; RZS, rheumatoid disease; seg., segment; n/a, not applicable; p-value, Wilcoxon signed-rank test; SD, standard deviation.
Table 2.
Doppler Ultrasound Analysis of Arterial Flow and Vessel Diameter in Patients Undergoing Propeller and ALT Flap Reconstruction.
Table 2.
Doppler Ultrasound Analysis of Arterial Flow and Vessel Diameter in Patients Undergoing Propeller and ALT Flap Reconstruction.
| Parameter | Group A (Acute Damage) n=8 |
Group B (Chronic Damage) n=6 |
P-Value |
|---|---|---|---|
| Number of perforators detected | 11 |
7 |
0,346 |
| Flap | Propeller: 7 ALT: 1 |
Propeller: 4 ALT: 2 |
n/a |
| Mean velocity; cm/s (SD) | 29 (±13,74) | 26,14 (±6,20) | 0,557 |
| Mean diameter; mm (SD) | 1,56 (±0,65) | 1,53 (±0,61) | 0,909 |
| False positive cases | 0 | 0 | n/a |
n/a, not applicable; p-value, flow velocity and vessel diameter: Unpaired two-sample t-test (Welch’s t-test) was used to compare the means between the two groups. Number of vessels: Chi-square test was applied to assess differences between groups.; SD, standard deviation.
Table 3.
Analysis of the operation and hospitalization data of patients who underwent lower extremity reconstruction.
Table 3.
Analysis of the operation and hospitalization data of patients who underwent lower extremity reconstruction.
| Group A (Acute Damage) n=17 |
Group B (Chronic Damage) n=10 |
p-Value | |
|---|---|---|---|
| Bone fixation | LCP: 7 Nail: 10 ---- ---- |
LCP: 4 Nail: 4 Endoprothesis: 1 Non: 1 |
n/a |
| Flap | M. gastrocnemius: 3 M. soleus: 3 Propeller: 7 Reverse sural: 1 Flag-ship: 1 Cross-leg: 1 ALT: 1 |
M. gastrocnemius: 3 M. soleus: 1 Propeller: 4 Reverse sural: 1 Flag-ship: 1 ------ ALT: 2 |
n/a |
| Bacteria | E. faecalis: 9 MRCNS: 7 MRSA: 2 MSSA: 3 E. coli: 4 P. Mirabilis 1 |
E. faecalis: 2 MRCNS: 4 MRSA: 5 ---- E. Coli: 2 P. Mirabilis: 1 |
n/a |
| Mean operation time; min. (SD) | 324,3 (±112,6) | 362,2 (±50,9) | 0,32 |
| Mean hospitalization time; week (SD) | 4,12 (±2,65) | 3,44 (±1,5) | 0,21 |
| Extra procedures/ complication |
4 (21%) | 3 (30%) | n/a |
min., minutes; LCP, low-contact locking plate; PMMA, polymethylmethacrylate cement; MSSA, methicillin-sensitive Staphylococcus aureus; MRCNS, methicillin-resistant coagulase-negative Staphylococcus; MRSA, methicillin-resistant Staphylococcus aureus; n/a, not applicable; p-value, Wilcoxon signed-rank test; SD, standard deviation.
Table 4.
Functional and clinical outcomes: LLFI pre- and post-operation for lower extremity reconstruction.
Table 4.
Functional and clinical outcomes: LLFI pre- and post-operation for lower extremity reconstruction.
| LLFI | Group A (Acute Damage) n=17 |
Group B (Chronic Damage) n=10 |
p-Value |
|---|---|---|---|
| Preoperation (SD) | 9,53 (±6,09) | 27,0 (±12,08) | 0,001 |
| Postoperation (SD) | 66,26 (±8,09) | 69,6 (±9,02) | 0,22 |
LLFI, Lower Limb Functional Index; p-value, Wilcoxon signed-rank test; SD, standard deviation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



