Submitted:
24 February 2026
Posted:
27 February 2026
You are already at the latest version
Abstract
Objective: Pupillometry is a noninvasive method which measures changes in the size of the pupil intending to study cognitive processes and identify networks that are related to specific attentional states such as attention, mental effort, working memory, and many others, through monitoring pupil size. This study aimed to investigate hotspots and global research trends in the field of pupillometry by bibliometric analysis.Methods: Publications from 1999 to 2025 in the Web of Science database were extracted and analyzed using bibliometric methods. This study utilized the R Bibliometrix package, along with the web platforms VOS Viewer and CiteSpace.Results: A total of 2,897 peer-reviewed documents were obtained, and the annual research output from 1999 to 2025 has increased significantly. The role of pupillometry in this research has been investigated by over 11,534 authors coming from 3,019 institutions in 89 countries or regions. According to the report, the United States had the highest number of publications, while Psychophysiology was the most productive journal. Amongst the most active academic institutions, the University of Toronto stood out as the most active, and among the most prolific authors, Olson Daiwai emerged as the most prolific. We found that keywords from pupillometry related including locus-coeruleus (304 occurrences), attention (240 occurrences), pupil (239 occurrences), pupillary light reflex (237 occurrences), and retinal ganglion cells (135 occurrences) had high frequency and among the strongest citation burst keywords, “infrared pupillometer”, “in situ keratomileusis”, “retinal ganglion cells”, and “refractive surgery” showed citation bursts from 1999 to 2025, corresponding with the increase in published documents.Conclusions: It can be noted that this study was the first comprehensive bibliometric study to summarize trends and developments in pupillometry research from a bibliometric perspective. By analyzing bibliometric data on development trends in pupillometry development trends, developers or researchers would be able to propose future research directions as well as pursue further collaborations.
Keywords:
pupillometry
; pupillary light reflex (PLR)
; bibliometrics analysis
; CiteSpace
; VOSviewer
Introduction
Irene Loewenfeld, in her monumental two-volume monograph on pupillometry (1999), noted that there is centuries-old anecdotal and semi-scientific observations have suggested that pupil diameter varies not only in relation to the amount of light entering the eye but also – sometimes visibly – to an individual’s internal states [1]. The pupil, an aperture within the iris, plays a critical role in the ocular system by regulating the entry of light into the eye, thereby enabling vision through its focused projection onto the retina. In humans and many animals, the pupil is typically circular in shape, though exceptions exist, such as in domestic cats. The size of the pupil is controlled by two sets of smooth muscles within the iris: the sphincter (or constrictor) muscles, which reduce its diameter, and the dilator muscles, which increase it. These dynamic changes in diameter serve to regulate the amount of light reaching the retina, thereby optimizing visual perception [2,3]. In relatively low-light conditions, the pupil dilates, while in brighter environments, it constricts. This process, known as the pupillary light reflex (PLR), is clinically utilized to assess the functionality of the visual system and diagnose optic nerve disorders [4]. A common clinical application of this reflex is exemplified when medical personnel use a penlight to evaluate a patient’s pupillary response [5]. The PLR is mediated by afferent input from the retina via the optic nerve to the pretectal nucleus in the midbrain and efferent parasympathetic fibers from the Edinger-Westphal nucleus to the sphincter pupillae muscle via the oculomotor nerve. Dilation, conversely, is governed by sympathetic pathways originating in the hypothalamus, descending to the spinal cord, and then traveling through the superior cervical ganglion to innervate the dilator pupillae muscle. There are, however, significant postgeniculate influences on the pupillary light reflex [6]. A large number of studies reported that patients with post-geniculate lesions had reduced pupillary light reflex in the blind hemifield [7,8,9]. Also, lesions of the visual cortex can produce pupillary hypokinesia, and psychophysical studies indicate that cortical inputs can affect the pupillary light reflex possibly through pretectal projections [10,11]. Disruption at any point in this reflex arc—from the retina and optic nerve to the brainstem and iris—can alter pupillary dynamics [12]. Otto Löwenstein and Irene Loewenfeld inaugurated a new era in pupillary research through the development of infrared video pupillography (IVP) [13]. Building upon Loewenfeld’s seminal contributions and, more recently, the discovery of melanopsin-expressing intrinsically photosensitive retinal ganglion cells (ipRGCs), pupillography has gained renewed interest and broader application in ophthalmology, psychology, and psychiatry [14]. Traditionally, infrared video pupillography was regarded as most effective for detecting moderate to severe optic neuropathies due to variability in pupillary light reflex (PLR) amplitudes. However, recent studies indicate that chromatic pupillometry and advanced analyses of pupillary responses can sensitively detect early dysfunction of retinal ganglion cells and the optic nerve [15,16,17]. Pupillometry, by quantifying these changes, becomes a non-invasive window into both ophthalmic and neurological health.
Pupillometry, the study of changes in pupil diameter as influenced by cognitive processing, has garnered significant attention in recent years. While the investigation of pupil behavior has long been a focus of ophthalmology and optometry research, the field of pupillometry has undergone considerable growth over the past two decades. Initially, assessments involved the use of a flashlight aimed at the pupil to evaluate consciousness impairment [18,19]. However, with advancements in technology, it is now possible to precisely measure pupil diameter and perform more sophisticated assessments. The development of infrared cameras has enabled more precise measurement of the pupillary light reflex (PLR), leading to the emergence of various types of pupillometers, including smartphone pupillometers, portable infrared pupillometers, pupillometers with goggles, eye tracker pupillometers, and expensive desktop pupillometers [20,21,22,23,24]. Most studies employing pupillometry have been conducted in laboratory environments, where participants are dark-adapted and illumination is tightly controlled [25,26,27]. However, given the numerous potential applications of pupillometry, it is desirable to develop instruments suitable for use in applied settings such as the home, workplace, sports field, or roadside. Recently, more affordable and accessible devices have been introduced for PLR measurement [20,21,28,29]. Notably, smartphone-based software applications now utilize the iPhone’s camera to record pupil responses while using its flash to deliver light stimuli. Contemporary studies indicate that the pupillary response to light can assist specialists in diagnosing various conditions [30,31,32]. Abnormalities in pupil size and shape have been correlated with changes in intracranial pressure (ICP) [33,34,35]. Under normal conditions, when the PLR is intact, light exposure across the pupil leads to a reduction in its diameter [36]. The pupillary response is regulated by the autonomic nervous system, with key metrics such as maximum constriction velocity and relative constriction amplitude serving as reliable indicators for detecting parasympathetic dysfunction [37,38,39]. The dynamics of the PLR exhibit a consistent sequence, which can be categorized into four distinct phases based on temporal variations in pupil size: response latency, maximum constriction, pupillary escape, and recovery [40,41]. Automated pupillometry allows for the quantification of three of these phases—latency, constriction velocity (CV), and dilation velocity (DV). The amplitude of contraction, CV, and DV are influenced by the intensity and duration of the applied stimulus [42]. While traditional PLR assessments are dependent on clinician skill and the properties of the light source (intensity and duration), modern pupillometry benefits from technological advancements in high-speed cameras and computational technology, facilitating precise and reproducible measurements [43]. The modern pupillometer, a handheld device, allows for quantitative assessments with exceptional accuracy, and the following eight parameters were automatically quantified: initial pupil diameter (mm), contraction amplitude (mm), contraction latency (ms), contraction duration (ms), contraction velocity (mm/s), dilation latency (ms), dilation duration (ms), and dilation velocity (mm/s) (Figure 1A) [44,45,46].
Since 1999, a significant body of literature has emerged in the field of pupillometry. Bibliometric analysis, which employs statistical and mathematical techniques to examine large volumes of scientific documents, has become an essential tool for tracking the evolution of this field. Mapping knowledge domains (MKD), a method that reveals emerging research areas and knowledge structures, utilizes document analysis software such as VOSviewer and CiteSpace to generate visual representations of scientific trends [47,48,49]. The aim of this bibliometric analysis is to systematically evaluate academic output in the field of pupillometry, providing insights into publication trends from 1999 to 2025. Metrics such as publication volume, source journals, author productivity, co-authorship networks, co-citation patterns, and international collaborations will be analyzed. Additionally, MKD will highlight underexplored domains within pupillometry, offering a comprehensive overview of the field’s development.
Materials and Methods
Data Source
Although several databases can meet the needs of global-level analyses [50], we chose the Science Citation Index Expanded (SCI- Expanded, 1999-present) of the WoS Core Collection (WoSCC) database for our evaluation. The WoSCC database covers more than 12,000 international scientific journals with great impact and quality and is the most applied database for bibliometric analysis [51,52]. Apart from the general literature search, it also possesses an important function of citation index searching, which helps assess the academic performance of literature in a specific field [53].
Search Strategy
The online SCI Expanded database was used as the data source. The search query was designated as pupillometry (Topic) or pupillometer (Topic) or pupillography (Topic) or pupillogram (Topic) or pupillometric (Topic) or pupillographic (Topic) or afferent pupillary defect (Topic) or swinging flashlight test (Topic). The language criterion was restricted to "English," and only "articles or reviews" published between 1999 and 2025 were included, as illustrated in Supplementary Table S1. Scotland, England, Wales, and Northern Ireland were four distinct administrative entities, and papers from these regions were evaluated independently rather than collectively as the United Kingdom. Hong Kong was incorporated into the People's Republic of China (PRC). Our emphasis encompassed publications from 1999 to 2025, with the search conducted on December 01, 2025. The file was exported in "plain text" format, with the option for "full record and cited references" chosen. Essential details of each document, including countries, organizations, authors, title, journal, abstract, keywords, and references, were extracted. The comprehensive data retrieval procedures and inclusion criteria for this investigation are encapsulated in Figure 1B.
Mapping Analysis
In this research, a visualized bibliometric analysis was generated using the VOSviewer software (www.vosviewer.com) version 1.6.17 [49]. This software facilitates the creation of visual bibliometric maps and node-link diagrams, encompassing research trend data, including countries, publications, and researchers, as well as network information from co-cited reference and co-authorship analyses. Keywords articulate the theme of scientific literature, and the clustering of analogous keywords resulted in co-occurrence keyword clusters, which can be utilized to investigate the knowledge structure and hotspots within this research domain.
Full records and cited references of all publications in TXT format were obtained and assembled from WoSCC, subsequently imported into CiteSpace 6.3.3., 64 bits basic (Drexel University, Philadelphia, PA, USA), VOSviewer 1.6.20 (Leiden University, The Netherlands), Microsoft Excel 2019, and one online platform (https://bibliometric.com), according to the software demanded for visual analysis and data analysis.
This study examined country scientific production, three field plots (co-cited references, authors, keywords), author production over time, author impact (H-index), and thematic evolution utilizing the R language-based Bibliometrix Package (version 5.1.0), which can display the publications of the ten most prolific authors over the past 25 years and delineate the evolution of research topics.
In addition to the software referred to above, bibliometric analysis software (https://bibliometric.com/) was applied to study collaboration relationships among countries. Figure 1C summarizes the entire process of bibliometric analysis.
Results
Publication Output and Development Trend
The WOS database comprises 2,897 publications pertaining to pupillometry from 1999 to 2025. The papers were examined based on the year of publication (Table 1). The analysis indicated that between 1999 and 2025, the total number of publications rose from 32 to 257. The number of papers published in 2021 was the highest (9.49%). As shown in Figure 2A, publications and citations have increased annually, indicating that citation changes are approximately in sync with the number of published documents.
Analysis of Leading Countries/Regions
The countries that made the greatest contributions are presented in Table 2. A distribution world map and network map of pupillometry research are shown in Figure 2B, Figure 3A, and Figure 3B, respectively. Among 89 countries and regions that have contributed to the publications in this field, the United States contributed the largest number of publications (1,086 articles, 37.48% of all the articles), followed by Germany (351, 12.11%), England (267, 9.21%), and Netherlands (168, 5.79%). While the United States had the highest number of citations (29,243 citations), followed by those from the Germany (8,482 citations), England (7,380 citations), and Netherlands (6,251 citations), and the rest are all less than 4,000 citations. The USA had the highest centrality (38%), followed by England (30%), Australia (23%), Italy (13%), Germany (12%), and Netherlands (10%). According to the country co-authorship analysis, there was a high degree of communication among countries. Each node represents the influence of a country, with larger nodes representing more influence. The links between nodes indicated the level of cooperation across countries; the distance and strength of links reflect the proximity of collaboration in the field of pupillometry (Figure 3C).
Analysis of Leading Organizations
It has been reported that 3,019 institutions have published articles on using pupillometry in the past 25 years and the top 10 organizations accounted for 13.60% (394 documents) (Table 3). Among 3,019 institutions that appeared at least 5 times, the remaining 306 meet the thresholds (Figure 3D). Four of the top 10 most productive institutions are from the US. The University of Toronto (Canada, 46 articles) was the preeminent university in terms of publication, followed by the, the University of Pennsylvania (USA, 43 articles), University of Tubingen (Germany, 43 articles), University of Oslo (Norway, 41 articles), Johns Hopkins University (USA, 40 articles), the University of Pittsburgh (USA, 40 articles), Australian National University ( Australia, 37 articles), University of Copenhagen (Demark, 36 articles), University of California San Francisco (USA, 35 articles), and Technical University of Denmark (Demark, 33 articles). The distribution links of research organizations were established using VOSviewer to map the network (Figure 3D). The node size indicated the quantity of published documents, while the link strength reflected the degree of collaboration.
Distribution of Journals
A total of 2,897 academic documents originated from 682 journals. Table 5 enumerates the top 10 most prolific journals, accompanied by their impact factors, as well as the top 10 predominant study domains within the leading journals. Of the 682 productive journals published at least five times, the remaining 154 productive journals meet the thresholds. Table 5 presents the ten most prolific journals and co-cited journals in pupillometry research, accounting for 19.22% of all publications in these journals. The top 5 journals in terms of publication volume were Psychophysiology (79 articles, 2.72%), Scientific Reports (74 articles, 2.55%), Plos One (74 articles, 2.55%), Investigative Ophthalmology & Visual Science (69 articles, 2.38%), and Journal of Cataract and Refractive Surgery (53 articles, 1.82%). The H-index of the top 10 most prolific journals indicates that Investigative Ophthalmology & Visual Science possesses the highest impact measures, each with an H-index of 30, followed by Psychophysiology (27), International Journal of Psychophysiology (25), Journal of Cataract and Refractive Surgery (25), Plos One (25), Ophthalmology (22), Graefes Archive for Clinical and Experimental Ophthalmology (18), Frontiers in Neurology (16), Scientific Reports (16), and American Journal of Ophthalmology (15) (Figure 4E).
Distribution of Co-Cited References
A total of 75,461 cited references were retrieved in the co-citation analysis. The ten most co-cited references pertinent to pupillometry study were identified and enumerated in Table 6. Among the 75,461 referenced citations, 80 co-cited references were quoted a minimum of 60 times in the field of pupillometry (Supplementary Table 2). Aston-jones G et al. [62] (2005, 359 citations, 6,684 total link strength), Joshi S et al. [54] (2016, 271 citations, 4,667 total link strength), Beatty J et al. [63] (1982, 263 citations, 4,362 total link strength), and Kahneman D et al. [64] (1996, 260 citations, 4,642 total link strength) were the most selected prolific co-cited references among all 75,461 cited references.
Distribution of Key Words: Hotspots of Pupillometry Study
It is especially important to note that we identified a number of potentially distinctive characteristics of the pupillometry field. We selected significant keywords from the relationships among the top 20 co-cited references, authors, and the evolution of keywords in pupillometry research (Figure 5A). They are almost associated with the top 10 authors and co-cited references (Table 4 and Table 6).
Figure 5B displayed word clouds containing author keywords. The keywords provided by the author gave us additional valuable information. The present writers concentrate on the utilization of the pupillometry techniques (Pupillometry, pupillography, eye tracking, pupillary light reflex, responses, dilation) in potential mechanisms or clinical applications of neuro-ophthalmological diseases, as well as topics in neuropsychology, neuropsychiatry, anesthesiology, and other related fields (Glaucoma, myopia, traumatic brain injury, locus-coeruleus, Alzheimer’s disease, Parkinson’s disease, multiple sclerosis, depression, schizophrenia, pain assessment, and postoperative pain, etc.)
The co-occurrence analysis of high-frequency keywords revealed the research hotspots in pupillometry. The minimum co-occurrence frequency of a keyword was set as 20. Out of the 9,433 retrieved keywords related to pupillometry, 230 keywords satisfied the criteria. Keywords having similarities were clustered based on the network. Table 7 enumerates the top 10 keywords for each cluster. Figure 5C illustrates that 1,000 keywords can be categorized into five research clusters by color.
Co-Evolutionary Pathway in the Study of Pupillometry
The keywords' evolution over time is illustrated in Figure 6A and B. Citespace is utilized to generate co-evolutionary pathways and numerous significant keywords, including “Locus coeruleus”, “Melanopsin”, “Traumatic brain injury”, “Listening effort”, “Autonomic nervous system”, “Refractive surgery”, “Intracranial pressure”, “Ocular trauma”, “Pupillographic sleepiness test”, and “Covert attention”. The top 25 co-occurrence keywords are shown in Supplementary Table 3. Moreover, the top 25 strongest citation burst keywords were identified, and among these keywords, “infrared pupillometer”, “in situ keratomileusis”, “retinal ganglion cells”, and “refractive surgery” showed the most citation bursts from 1999 to 2025, corresponding with the increase in published documents (Figure 6C).
Discussion
General Information
In this analysis, we identified 2,897 publications related to pupillometry in the Web of Science (WOS) database from 1999 to 2025. The number of academic documents serves as a key research indicator, offering valuable insights into the development and emerging trends within a field. The steady increase in the number of articles published over the past 25 years reflects the rapid growth of pupillometry research within the medical domain. The University of Toronto (Canada), the University of Pennsylvania (USA), and the University of Tubingen (Germany) were the most prolific institutions and played significant roles in international collaborations. An analysis of co-authorship patterns and author co-citations can provide a deeper understanding of individual researchers’ contributions and influence, highlighting the importance of collaborative efforts within the pupillometry research community. The United States, Germany, and England were the leading countries and made a great contribution to the publication in pupillometry (Table 2, Figure 3A, B, C) [56,59,62,63,64,65,66,67,68]. The United States is the principal collaborator with Germany, England, the Netherlands, and other nations. In addition, the United States ranks first in both the number of citations and total link strengths within this domain. Furthermore, the centrality and citations of the United States were 0.38 and 29,243, while that of the rest of the countries were less than 0.2 and 8,500 respectively, except for the centrality of England was 0.30 and Australia was 0.23. Geographical distance may not significantly impact international cooperation. The results regarding publication and citation numbers indicate that the pupillometry field is undergoing rapid evolution, generating considerable interest for future research.
The co-citation analysis identified pertinent subjects inside high-quality academic publications. The ten most co-cited references primarily relate to novel methodologies considered pivotal in the evolution of pupillometry. The Psychophysiology has the most publications related to pupillometry (79 publications), yet the journal with the highest impact factor is Investigative Ophthalmology & Visual Science (IF 2024 = 5.0), the only journal in the top 10 with an IF score ≥ 5. The analysis of research hotspots indicated that the domain of pupillometry extends beyond neurology, ophthalmology, suggesting advancements in psychology, anesthesiology, psychiatry, critical care medicine, experimental research medicine, and further fields, as illustrated in Table 5.
From the analysis of authors (Table 4, Figure 4A), Olson Daiwai (Corresponding author) from the Department of Neurology and Neurotherapeutics, University of Texas Southwestern Medical Center was the most prolific author and the longest period in publication. In addition, he and his colleagues (Aiyagari Venkatesh, top 7; Stutzman Sonja E, top 9) contributed to the pupillometry research. In addition, the member of this team was ranked seventh in the top ten of impact measures (Figure 4C). Overall, pupillometry research serves as an advantageous conduit for author collaboration. Additionally, the research team is the primary focus of collaboration, as the most academicians are from different countries. Cooperation among researchers from different countries should be strengthened, and beneficial terraces should be established, substantial advancements can be realized by optimizing the clinical translation of research and facilitating the exchange of technological innovations among scientists investigating disparities within the field of pupillometry.
Clinical Applications of Pupillometry
Ocular Accommodation and Convergence Eye Movements
When transitioning from viewing a distant to a near object, the near reflex is activated, involving ocular accommodation, convergence, and pupil miosis, to ensure clear and single binocular vision. Conversely, when focus shifts back to a distant target, ocular disaccommodation, divergence, and pupil mydriasis occur [69]. It is well established that pupil diameter is influenced by the amount of light reaching the retina. Therefore, controlling light conditions is crucial in pupillometry research. Another potential confounder in pupil response is accommodation, as the pupil constricts during the near reflex when focusing on a nearby object [70].
Ocular accommodation is the process by which the crystalline lens increases its dioptric power to focus on an object of interest, ensuring a high-resolution foveal retinal image. Focusing on a nearby object not only induces accommodation but also neurologically triggers convergence and pupillary constriction, collectively known as the ‘near-triad’ [71]. Recent studies have discussed accommodative infacility in concussion, a condition that reflects impaired accommodation. Accommodative facility indirectly assesses the efficiency of the dynamic accommodative mechanism, including the critical parameter of peak response velocity. Therefore, individuals with slower accommodative responses to positive or negative flipper lenses would exhibit reduced facility [72,73].
In pupillometry research, two accommodation mechanisms are typically considered. First, during mentally demanding tasks, participants may shift their accommodation level. For instance, individuals may struggle to maintain focus on a visually presented problem and inadvertently gaze into the distance. Second, when viewing pictorial stimuli with apparent depth cues, participants may adjust their accommodation level in response to these cues. However, most studies investigating the effect of mental demands on pupil size do not measure accommodation, while those examining the effect of depth cues on accommodation or vergence often omit pupil size measurements [74,75]. Consequently, there is limited understanding of how accommodation functions as a potential confounder in pupillometry research.
The vergence eye movement mechanism is unique in that it is the only visual response that causes the eyes to move arbitrarily. It is crucial for depth perception and eye movement refixation. Both eyes can adapt and quickly alter fixation symmetrically, engaging with the saccadic system. Bifoveal fixation and stereopsis require precise alignment of the visual axes to shift focus between distances, thereby enhancing depth perception and spatial localization [76]. Vergence angle— the inward rotation of the eyes driven by retinal disparity— is another important variable in pupillometry, as vergence is part of the pupillary near reflex. Many studies have shown that pupil constriction is synchronized with vergence, likely occurring via midbrain neurons that project to the Edinger-Westphal nucleus and the oculomotor nucleus [77]. According to the dual interaction model, the pupillary near reflex is not driven solely by accommodation or convergence, but rather as an interactive result of the neural pathways that control both mechanisms [78].
Relative Afferent Pupillary Defect (RAPD)
The swinging flashlight test remains the primary method for assessing relative afferent pupillary defect (RAPD) in patients with unilateral neuro-ophthalmic pathology [79,80]. The RAPD is a hallmark sign of unilateral or asymmetric optic nerve disease, including optic neuritis, glaucoma, ischemic optic neuropathy, and compressive lesions [23,81,82,83]. Traditionally detected by the swinging flashlight test, RAPDs can now be quantified via automated pupillometry with high accuracy. Studies show that automated RAPD detection correlates strongly with visual field defects, retinal nerve fiber layer (RNFL) thinning on OCT, and visual evoked potentials [84,85]. Automating the swinging flashlight test offers several advantages. To obtain a reliable assessment of an afferent pupil defect, it is necessary to simultaneously measure both eyes to account for natural differences in the midbrain decussations of the afferent pathway, asymmetric supranuclear influences on the Edinger-Westphal nucleus, and potential efferent differences in pupil innervation [86,87,88]. A binocular pupillographic device is ideally suited for this purpose. Moreover, the severity of RAPD can be more accurately measured by comparing the pupillary light responses (PLRs) at different light intensities. Studies have shown that the pupil responds not only to changes in light flux but also to variations in pattern, color, and motion, even when light intensity remains constant [89,90]. Objective RAPD measurement aids in early diagnosis and progression monitoring. Optic neuritis, a common manifestation of multiple sclerosis (MS), often results in a relative afferent pupillary defect. Pupillometry is valuable in detecting subclinical optic neuritis in MS [85,91]. Delayed constriction latency and reduced constriction amplitude are frequently observed. Quantitative pupillometry may help identify patients with subclinical visual pathway involvement before symptom onset [92]. Besides, Glaucoma is a leading cause of irreversible blindness and often presents without early symptoms. Functional loss precedes structural changes in some patients. Pupillometry can detect glaucomatous damage by measuring asymmetric pupillary responses. Reduced pupil constriction amplitude and velocity in response to light stimuli have been reported in glaucoma patients, especially with advanced damage [93]. The correlation between pupillometric indices and visual field loss has been established, offering a potential supplementary tool for early detection. Advanced applications include chromatic pupillometry, which uses wavelength-specific stimuli to differentiate rod-, cone-, and melanopsin-mediated responses, thereby enhancing sensitivity to early glaucomatous changes.
Despite its advantages, pupillography has been challenging to incorporate into clinical practice due to its limited availability and lack of portability. Previous work by Nicholas J. Volpe and colleagues demonstrated that a portable monocular pupillometer could record the swinging flashlight test (SFT) and identify RAPDs of 0.9 log units with 80% sensitivity and 92% specificity. However, this device’s sensitivity and specificity were deemed insufficient for clinical use [94]. To address this limitation, Volpe et al. developed a portable pupillometer capable of binocular recordings for up to 20 seconds, which improved sensitivity and specificity. This binocular pupillometer, when used with neutral density filters (NDFs), has shown promise for detecting RAPDs in clinical practice. Their study found that the device could detect RAPDs of ≥0.6 log units with 100% sensitivity and 91% and 95% specificity, respectively, for contraction amplitude (CA) and contraction velocity (CV). Additionally, the use of NDFs in front of the healthy eye allowed for the grading of RAPDs by eliminating baseline measurement differences. Subtle RAPDs can be confirmed by placing 0.3 log unit filters over each eye to accentuate or neutralize any observed differences [95]. However, Dominik Bruegger and colleagues [96] reported higher sensitivity (90.2%) and specificity (82.2%) than those found by Wilhelm [86] who correctly identified only 85% of relative afferent pupillary defects (RAPDs) greater than 0.3 log units. This improvement may be attributed to methodological differences; specifically, Bruegger’s analysis compared device results with the presence of optic neuropathy confirmed by multiple clinical findings, rather than using the clinically measured RAPD as the sole reference standard.
Retinal and Macular Diseases
Principally, Pupillary responses also reflect retinal function, particularly of the photoreceptors and intrinsically photosensitive retinal ganglion cells (ipRGCs). Pupillometry has been used in age-related macular degeneration (AMD), showed as altered constriction amplitude and increased latency; in diabetic retinopathy is reduced PLR amplitude, even in early stages [97]. Additionally, retinitis pigmentosa was found as reduced scotopic response and minimal rod-mediated PLR and central serous chorioretinopathy showed that asymmetric responses with central retinal involvement [98]. Chromatic pupillometry has enabled the assessment of cone- and rod-specific pathways, helping to localize dysfunction in inherited retinal diseases and quantify residual function. Minoru Nakayama and co-workers demonstrated that the error rates for healthy and age-related macular degeneration (AMD)-affected pupils were low when the coefficient combining PLR amplitude and waveform features was optimized at 1.5. However, error rates remained high in patients with age-related ocular changes. Because aging affects the pupil through multiple mechanisms, distinguishing healthy from AMD-affected eyes may be challenging in some cases [99].
Refractive and Cataract Surgery
Procedures such as LASIK and PRK alter corneal optics and can influence visual quality, especially under scotopic conditions. Preoperative assessment of pupil size is crucial for predicting postoperative night vision complaints. Patients with large mesopic pupils may experience increased glare and halos. Pupillometry is used to match ablation zones with pupil diameter and to customize surgical plans. Postoperative changes in pupil dynamics can reflect neural adaptation or altered sensory input. Pupillary responses can help evaluate visual quality after cataract surgery. Differences in PLR dynamics have been observed between multifocal, monofocal, and extended depth of focus (EDOF) intraocular lenses (IOLs) [100]. In patients with posterior capsular opacification or suboptimal outcomes, altered pupillary dynamics may suggest light scatter or neural inefficiency. Furthermore, iris behavior during surgery (intraoperative floppy iris syndrome) can be anticipated by preoperative dynamic pupillometry.
Pediatric and Pharmacologic Ophthalmology
In children, especially those with developmental delays or non-verbal limitations, pupillometry offers objective metrics for visual pathway function. The affected eyes of amblyopic patients often show delayed PLR and reduced amplitude [101]. The affected eyes of patients with congenital glaucoma show abnormal baseline diameters and reduced constriction [102]. The pupillary response of patients with neurodevelopmental disorders to light and cognitive stimuli can reflect abnormal sensory processing. Because children may not cooperate with subjective visual testing, pupillometry becomes especially useful in diagnosis and monitoring.
Furthermore, Pupil responses to pharmacologic agents such as pilocarpine, tropicamide, or apraclonidine aid in diagnosing; Adie’s tonic pupil: Denervation hypersensitivity demonstrated by low-dose pilocarpine; Horner’s syndrome: Dilation lag and apraclonidine-induced reversal; Argyll Robertson pupil: Normal near response but absent light reflex [30,103]. Pharmacological studies of the pupil are extensive in both human and non-human species. The use of pharmacological agents helps elucidate the central neural networks that control pupillary function and provides valuable insights into the drugs themselves by characterizing their effects within a well-defined physiological and pharmacological framework. Drugs can be administered to the ocular surface in various formulations, commonly as aqueous or oily solutions [104]. The specific formulation must be clearly indicated, including whether the compound is used in its base or salt form. The vehicle should also be specified, as corneal penetration is generally superior with oily solutions. Although continuous superfusion of drugs onto the ocular surface has been explored, the application of “blobs” in the form of eye drops remains the standard method [105]. Pupillometry enhances diagnostic confidence by quantifying subtle drug effects that may be difficult to detect visually. Pupil dynamics provide insight into autonomic neuropathies, including those due to diabetes, Parkinson’s disease, and post-viral syndromes. Reduced dark adaptation velocity and smaller scotopic diameters indicate sympathetic dysfunction. These metrics are increasingly used in evaluating systemic disease impacts on ocular health.
Neurological Disorder
Neurological assessments traditionally rely on a combination of clinical examination, neuroimaging, and electrophysiological testing. Among the simplest yet most informative clinical observations is the pupillary response, particularly in assessing consciousness, cranial nerve function, and brainstem activity. The pupil is controlled by a balance between parasympathetic and sympathetic input to two muscles: the sphincter pupillae and the dilator pupillae. The parasympathetic pathway originates in the Edinger-Westphal nucleus, travels with cranial nerve III, and constricts the pupil via acetylcholine release. The sympathetic pathway originates in the hypothalamus, synapses in the cervical ganglion, and mediates dilation via norepinephrine. Neurological damage affecting any part of this complex pathway—from the brainstem to the peripheral ganglia—can manifest as characteristic changes in pupillary reactivity. Importantly, the pupils serve as a proxy for deeper brain function, particularly brainstem integrity and cortical modulation via the locus coeruleus-norepinephrine (LC-NE) system [106]. Manual pupil exams suffer from inter-observer variability and limited precision. In contrast, automated pupillometry offers reproducible, objective data that can detect subtle changes not visible to the naked eye—particularly important in critical care and neurosurgical settings.
The Neurological Pupil index (NPi), a composite score generated by proprietary algorithms (e.g., by Neuroptics), standardizes pupillary reactivity on a scale from 0 to 5, helping clinicians quickly interpret trends and detect abnormalities. Traumatic brain injury (TBI) remains one of the most studied applications of pupillometry in neurology. Brain trauma often causes increased intracranial pressure (ICP), which can compress cranial nerves or the brainstem, leading to pupillary dilation or non-reactivity [107]. Quantitative pupillometry can detect early signs of herniation and guide interventions such as decompressive craniectomy. Studies have shown that declining NPi scores can precede clinical signs of deterioration [68]. In addition, in ischemic stroke or subarachnoid hemorrhage, pupillary changes can signal increased ICP, brainstem involvement, or impending herniation. Pupillometry is useful in serial monitoring of patients to detect secondary neurological decline. In a study of Larson et al. show that abnormal pupillary responses predicted poor neurological outcomes and were independently associated with higher mortality [20]. In the neuro-ICU, continuous or repeated pupillometric assessments allow real-time tracking of neurological status. Non-reactive pupils, especially if bilateral, are a poor prognostic sign, while improvement in NPi scores can indicate recovery of brainstem function.
Alzheimer’s disease (AD) is associated with early degeneration of the LC-NE system. Pupil dilation in response to cognitive tasks (pupillary cognitive response) is reduced in AD patients, reflecting impaired noradrenergic modulation. Romagnoli M et al. [108] demonstrated that pupillary responses during memory tasks can differentiate between healthy controls, patients with mild cognitive impairment (MCI), and those with AD. Autonomic dysfunction in Parkinson’s disease (PD) affects both sympathetic and parasympathetic pathways, often resulting in abnormal pupillary dynamics. Delayed light reflex, reduced amplitude of constriction, and asymmetric dilation velocities are frequently observed [109,110]. Erdinç Bozkurt and colleagues identified statistically significant reductions in contrast sensitivity across all tested spatial frequencies in the Parkinson’s group compared to healthy controls [111]. This result is consistent with previous literature and reinforces the view that contrast sensitivity loss in Parkinson’s disease follows a generalized rather than frequency-specific pattern [112]. Pupillometry can also help distinguish PD from atypical parkinsonian syndromes, such as multiple system atrophy (MSA), which may present with more profound dysautonomia [113]. In patients with Graves’ orbitopathy, static pupillographic parameters remained within normal limits, whereas dynamic measurements revealed delayed constriction and reduced redilation velocity [114,115]. These findings suggest that pupillometry reflects not only the integrity of the afferent visual pathway but also autonomic nervous system function, indicating potential diagnostic value across a range of neuro-ophthalmologic disorders.
Autonomic neuropathies, such as those found in diabetes or autoimmune disorders, can impair both sympathetic and parasympathetic pupillary control. Pupillometric abnormalities in diabetics include smaller baseline diameter, slower dilation velocity, and reduced constriction amplitude. These markers may appear before overt cardiovascular autonomic dysfunction, offering an early diagnostic window [116]. In disorders like pure autonomic failure or postural orthostatic tachycardia syndrome (POTS), pupillometry may be used to assess autonomic integrity. Recent studies suggest potential use in screening for autonomic involvement in long COVID as well. Besides, pupillometry has been used alongside fMRI, EEG, and MEG to study functional brain networks. Because pupil size correlates with LC-NE activity, it serves as a proxy for arousal, attention, and vigilance. For example, simultaneous fMRI-pupillometry studies have shown that pupil dilation precedes increased activity in the salience network, linking peripheral autonomic signals to central attentional systems [56].
The pupil plays a critical role in controlling the amount of light entering the eye, adapting to various luminance levels and focal requirements. Its response to light and near stimuli is governed by a complex interplay of neurological and ocular mechanisms, making it an insightful marker for ocular and systemic health. Historically, clinicians relied on subjective evaluation of pupillary responses. However, modern pupillometry provides high-resolution, quantitative assessments that have transformed the accuracy and consistency of pupil evaluation in ophthalmology. Infrared video-based pupillometers allow real-time tracking of pupil diameter and dynamic reactivity, including constriction latency, velocity, and redilation metrics [57]. These measurements provide vital information about the status of the optic nerve, retina, iris musculature, and autonomic pathways. The integration of pupillometry into ophthalmic evaluations enhances diagnostic sensitivity for detecting afferent pupillary defects (APDs), glaucoma progression, retinal dysfunction, and postoperative complications.
Psychological and Psychiatric Disorders
Pupil dilation correlates with mental effort and decision uncertainty. Pupillary responses are also sensitive to emotional arousal. Emotionally salient stimuli—such as fearful faces or affective sounds—typically elicit greater pupil dilations, even when presented subliminally, implying that pupillometry can reveal unconscious emotional processing [117]. Research by Iain Jackson and colleagues has extended this approach to developmental studies, showing that infants exhibit increased pupil dilation in response to unexpected or novel stimuli, providing insight into early cognitive and predictive mechanisms [118]. Kahneman and Beatty demonstrated that pupil size increases with task difficulty, establishing pupillometry as a proxy for cognitive load. This has since been applied to explore executive function, working memory, and attentional processes in both healthy and clinical populations. Accurate pupillometry requires high-resolution eye-tracking and controlled lighting. Key methodological variables include Baseline correction: Adjusting for individual differences in resting pupil size; Stimulus timing and duration: Standardization is crucial to ensure response validity; Artifact removal: Eye blinks and saccades can distort readings; Psychotropic medication effects: Many psychiatric drugs influence pupil size independently of mental states. Despite these challenges, standardized protocols are emerging, allowing for more reliable cross-study comparisons [64].
Depression is associated with dysregulation in arousal and affective processing. Studies show blunted pupil dilation in response to emotional stimuli, suggesting reduced emotional reactivity [119]. Pupillary responses to negative stimuli have been proposed as predictors of treatment response to cognitive behavioral therapy (CBT) and selective serotonin seuptake inhibitors (SSRIs). In bipolar disorder, pupillometric abnormalities are seen during both manic and depressive episodes, though patterns vary. Some evidence suggests hypersensitivity to reward-related stimuli in mania, reflected in greater pupil dilation [120]. Anxiety involves heightened arousal and threat sensitivity, often reflected in increased tonic pupil dilation and exaggerated responses to threat-related stimuli. Individuals with generalized anxiety disorder (GAD) and post-traumatic stress disorder (PTSD) exhibit larger and prolonged pupillary responses to aversive cues, indicating sustained hypervigilance. Pupillometry has also been used to assess attentional bias in social anxiety disorder, particularly in response to facial expressions [121]. The time course of pupil dilation provides insights into the temporal dynamics of threat processing. In depression, for instance, early changes in pupil responses to emotional stimuli have been proposed as predictors of antidepressant efficacy [122]. Similarly, pupillometry may be useful in studying the cognitive effects of ketamine, antipsychotics, and psychedelics. Emerging studies are exploring the use of pupillometry in brain stimulation contexts such as transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS). Real-time pupillary feedback may help optimize stimulation parameters for individualized treatment. Cognitive training interventions in disorders like Attention-Deficit/Hyperactivity Disorder (ADHD) and anxiety have also used pupillary metrics to assess engagement and cognitive load, providing a physiological validation of task efficacy. More recently, the post-illumination pupil response (PIPR) has been evaluated in individuals with seasonal affective disorder (SAD). Roecklein et al. [123] initially reported a reduced PIPR in participants with SAD compared to nondepressed, nonseasonal controls. Subsequently, Laurenzo et al. [124] observed an attenuation of the PIPR in individuals with nonseasonal major depressive disorder (MDD) relative to nondepressed controls, though this difference was evident only under low-intensity red and blue stimuli, not under higher-intensity chromatic conditions.
Patients with schizophrenia show abnormal pupillary responses to cognitive and emotional stimuli, potentially reflecting disruptions in attentional control and arousal regulation. Reduced task-evoked pupil dilation has been observed during working memory tasks, implicating deficits in executive function [125]. Some findings also suggest that pupillary measures correlate with negative symptoms such as blunted affect and cognitive anhedonia. Early-stage psychosis studies have explored whether pupillometry could serve as a marker for risk or prodromal states. In ADHD, altered pupil dynamics have been linked to attentional dysregulation and arousal abnormalities. Children with ADHD often exhibit lower baseline pupil diameter and reduced dilation during tasks requiring sustained attention [126]. Pupillometry also provides a non-invasive way to monitor medication effects. For example, methylphenidate has been shown to normalize pupil responses in children with ADHD, correlating with improved performance.
Pupillometry has gained traction in autism research, given its potential to reflect sensory sensitivity, emotional reactivity, and social processing deficits. Children with Autism Spectrum Disorder (ASD) often show atypical pupil responses to social stimuli such as faces or eye contact. Reduced or delayed pupillary responses to emotional expressions are interpreted as evidence of reduced social salience. Such findings may aid in early diagnosis or in evaluating intervention outcomes [127]. Pupillometry is sensitive to pharmacological modulation, especially drugs affecting the cholinergic and noradrenergic systems. SSRIs, benzodiazepines, and stimulants all impact pupil size, offering an avenue to monitor treatment effects objectively.
Sleepiness
Changes in pupillary diameter under complete darkness can result only from accommodation or from innervational variations within the central and peripheral sympathetic systems that determine the baseline pupil size. Oscillations in pupil diameter occurring in darkness and associated with sleepiness were first described by Loewenstein et al. [128] , who termed them “fatigue waves.” In contemporary sleep research and sleep medicine, however, a distinction is made between sleepiness and fatigue. Consequently, the terms “sleepiness waves” or “sleepiness-related oscillations” are now preferred, as fatigue does not induce oscillatory changes in pupil diameter. The Pupillographic Sleepiness Test (PST) offers a less time-consuming and less labor-intensive alternative to other objective assessments, such as the Multiple Sleep Latency Test (MSLT). Classical psychometric properties of the PST have been systematically evaluated and found to be adequate. The PST is now well established and widely applied in sleep research, sleep medicine, and psychology [129,130].
H Frohnhofen and colleagues conducted a study comparing scores on the Essener Questionnaire of Age and Sleepiness (EQAS) with pupillometry-derived physiological measures of sleepiness [131]. They selected the Pupillary Unrest Index (PUI) as the primary measurement parameter, given that it is a validated and widely accepted indicator of sleepiness. The study found that an EQAS score above 3 effectively differentiated sleepy from non-sleepy participants according to PUI-based sleepiness criteria. The high negative predictive value (90%) and positive predictive value (75%) of this cut-off suggest that the EQAS may serve as an adequate substitute for pupillometry in assessing sleepiness among older adults. These results demonstrate a significant correlation between EQAS scores and the PUI, supporting the physiological validity of the sleepiness. Furthermore, the observed dose–response relationship highlights a close association between the two measures. In addition, sleep deprivation studies have shown that PUI values increase following sleep loss [132] and correlate well with other physiological indicators of sleepiness across time-of-day variations [133].
Anesthesiology
Anesthesiology demands accurate and real-time monitoring of a patient’s physiological and neurological status. Traditional methods include heart rate, blood pressure, oxygen saturation, and EEG-based systems (e.g., BIS monitoring). However, these do not always reflect the nuanced activity of the central nervous system. Pupillometry has gained attention as a complementary method, providing dynamic information about analgesia, sedation levels, and brainstem integrity [134]. Pupil size is controlled by the autonomic nervous system—sympathetic stimulation causes dilation (mydriasis), while parasympathetic activation causes constriction (miosis). Anesthetic agents such as opioids, sedatives, and inhaled anesthetics affect this balance. Opioids like remifentanil induce miosis due to parasympathetic dominance. Propofol, remifentanil and volatile agents (e.g., sevoflurane) reduce light reflex amplitude and can cause variable pupil changes depending on dose and patient physiology [135,136]. Monitoring these changes provides an indirect but responsive measure of drug effect and autonomic activity during surgery.
Pupillary reflex dilation (PRD) in response to nociceptive stimuli during general anesthesia is a key marker for insufficient analgesia. A PRD ≥13% is considered a reliable indicator of pain-related sympathetic activation [137]. Studies show opioid titration guided by pupillometry reduces intraoperative consumption and improves hemodynamic stability [138]. Pupil diameter and PLR decrease with increasing levels of sedation; Under deep anesthesia, both the PLR amplitude and baseline size diminish. Pupillometric data can supplement Bispectral Index (BIS) to avoid over-sedation or intraoperative awareness. Besides, in pediatric patients, especially neonates, traditional pain scales are unreliable. Pupillometry has been explored for measuring opioid efficacy in neonates undergoing painful procedures and reducing opioid use by guiding dosing with PRD thresholds. Pupillometry has demonstrated an useful method to assess the spinal effects of epidural opioids [139,140].
Critical Care and Emergency Medicine
Pupillary responses can persist even when cortical activity is severely impaired, making pupillometry a vital tool in assessing consciousness in comatose or vegetative patients. The presence of reactive pupils in the first 24 hours post-cardiac arrest is associated with a favorable prognosis. Quantitative measures such as NPi have demonstrated greater prognostic accuracy than traditional manual assessments. A study by Saliman NH et al. [141] found that NPi scores below 3 were significantly associated with poor neurological outcomes and non-survival in ICU patients. Moreover, some researchers have used pupillary response to detect covert consciousness in patients with locked-in syndrome or minimally conscious states. Pupil dilation in response to mental arithmetic or imagery tasks may indicate preserved awareness even in the absence of motor function [142].
In critical care, monitoring a patient’s neurological status is essential for identifying life-threatening conditions early. Pupillometry provides a quantitative, objective assessment of the pupil’s reactivity, which can help detect changes in cerebral perfusion, brain injury, and the effects of drugs or anesthesia. Its ability to track fluctuations in pupil size and reactivity makes it particularly useful in the ICU, where patients may be sedated or unconscious, and traditional methods of neurological assessment may be unreliable. Critical care conditions such as traumatic brain injury (TBI), stroke, sepsis, and cardiac arrest often affect brain function, and pupillometry offers a non-invasive method for assessing these changes in real time. Its ability to detect subtle shifts in pupil dynamics makes it an ideal tool for managing and treating critically ill patients [68,143]. In critical care, where patients often suffer from life-threatening conditions such as traumatic brain injury, stroke, sepsis, or drug overdose, timely and accurate neurological assessment is essential. The ability of pupillometry to offer objective data in these scenarios has made it an increasingly valuable tool in intensive care units (ICUs) worldwide [144]. Moreover, as the push for standardized, data-driven approaches to patient monitoring continues, pupillometry aligns with the broader movement toward precision medicine.
Keyword Analysis of Pupillometry Study
In this field, keyword co-occurrence analysis and the identification of burst keywords effectively illustrate the evolution of research hotspots, reflecting the thematic development of the field. Keyword co-occurrence cluster analysis revealed that the frontier disciplines and internal structure of the pupillometry literature are predominantly organized into five distinct clusters (Table 7), each centered around a specific theme. Cluster 1 is associated with advancements in imaging technologies, such as eye tracking, pupillography, infrared pupillometry, quantitative pupillometry, dynamic pupillometry, chromatic pupillometry, and automated pupillometry [98,145,146,147,148,149,150,151,152,153,154,155,156]. Cluster 2 is linked to ophthalmopathies, including glaucoma and refractive error diseases, with key terms such as glaucoma, retinal nerve fiber layer, photorefractive keratectomy, refractive surgery, and myopia [157,158,159,160,161,162]. Cluster 3 focuses on neuropathological conditions, encompassing terms like locus coeruleus, autonomic nervous system, traumatic brain injury, intracranial pressure, Alzheimer’s disease, Parkinson’s disease, and multiple sclerosis [163,164,165,166,167,168,169]. Cluster 4 is connected with psychological and mental health research, addressing keywords such as cognitive control, depression, stress, schizophrenia, and mind-wandering [170,171,172,173,174]. Finally, Cluster 5 pertains to anesthesiology and critical care, with relevant terms including heart rate variability, analgesia, cardiac arrest, anesthesia, pain assessment, and postoperative pain [175,176,177,178,179,180,181,182,183,184]. These research hotspots primarily center on the mechanisms, pathology, biological assessment, diagnosis, and therapeutic guidance of neuro-ophthalmological diseases, as well as topics in neuropsychology, neuropsychiatry, anesthesiology, and other related fields.
Limitations
It is important to acknowledge certain limitations inherent in this bibliometric analysis. First, a significant constraint of this study is the predominance of English-language publications, which represents a limitation in capturing the full scope of pupillometry research. Many valuable contributions may be published in journals written in other languages, which were not fully represented in this analysis. Second, it is essential to recognize the inherent differences between bibliometric data and real-world research findings. For instance, older articles typically accumulate a greater number of citations, while newer, high-quality articles may not receive the same attention due to their relatively lower citation frequency. Third, while the SCI Expanded database is adequate for conducting bibliometric analyses, the document retrieval counts are only marginally different between SCI Expanded and WoSCC. Since different databases have distinct properties, such as variations in citation frequency counts, document classification, and export formats, combining multiple databases may not always yield optimal results [185]. Finally, some bibliometric experts recommend using the “front page” filter to refine the analysis and exclude unrelated documents, thus improving the relevance and quality of the bibliometric assessment [186].
Conclusions
A total of 2,897 articles on pupillometry research published between 1999 and 2025 were retrieved from the Web of Science Core Collection (WoSCC) SCI-Expanded database. The research in this field has been conducted by over 11,534 authors from 3,019 institutions across 89 countries or regions. Hybrid analysis and visualization tools, namely CiteSpace and VOSviewer, were utilized to systematically analyze key aspects of the literature, including the volume of publications, prominent institutions, countries, journals, leading authors, and collaboration networks. These tools also facilitate the identification of potential collaboration opportunities by analyzing co-occurrence networks. This study provides a comprehensive overview of the current state of pupillometry research, offering valuable insights into the field’s development. The findings and recommendations presented in this study are of particular significance to ophthalmologists, neurologists, neurosurgeons, psychiatrists, psychologists, anesthesiologists, pupillometry technology engineers, and researchers in related disciplines, guiding them in identifying future research directions and fostering collaborative efforts in the field of pupillometry.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Phanna Han had the idea for the study. Phanna Han selected studies for inclusion and abstracted data. Phanna Han and Marady Hun did the statistical analyses. Phanna Han and Fulgencio Nsue Eyene Nfumu interpreted the data. Phanna Han wrote the first draft. Bing Jiang critically revised the paper for important intellectual content. All authors have read and approved the content of the manuscript.
Funding
This work was supported by the Natural Science Foundation of China (NSFC 82070967 and 81770930 to Bing Jiang), China Hunan Provincial Science and Technology Department (No. 2020SK2086), and the Natural Science Foundation of Hunan Province (2020jj4788 to Bing Jiang). The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Data Availability Statement
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Conflicts of Interest
All authors have declared no conflicts of interest.
Ethical Approval
All data for this study were obtained from existing publications and Ethical approval was not required for this research.
References
- Loewenfeld, IE; Lowenstein, O. The Pupil: Anatomy, Physiology, and Clinical Applications; 1999. [Google Scholar]
- Gonzalez, RC WR. Digital Image Processing, 2nd ed.; Prentice-Hall: NJ, 2002. [Google Scholar]
- DC, B. Neuroophthalmology of the pupil and accommodation. In Principles and Practice of Ophthalmology; Albert, DM, Jakobiec, FA, Eds.; W.B. Saunders: Philadelphia, 1994. [Google Scholar]
- Bremner, FD. Pupil assessment in optic nerve disorders. Eye (Lond) 2004, 18(11), 1175–81. [Google Scholar] [CrossRef]
- Sirois, S; Brisson, J. Pupillometry. Wiley Interdiscip Rev Cogn Sci. 2014, 5(6), 679–92. [Google Scholar] [CrossRef]
- Wilhelm, H; Kardon, RH. The pupillary light reflex pathway; Neuro-Ophthalmology, 1997. [Google Scholar]
- Kardon, RH. Pupil perimetry. Curr Opin Ophthalmol. 1992, 3(5), 565–70. [Google Scholar] [CrossRef]
- Yoshitomi, T; Matsui, T; Tanakadate, A; Ishikawa, S. Comparison of threshold visual perimetry and objective pupil perimetry in clinical patients. J Neuroophthalmol. 1999, 19(2), 89–99. [Google Scholar] [CrossRef] [PubMed]
- Tan, L; Kondo, M; Sato, M; Kondo, N; Miyake, Y. Multifocal pupillary light response fields in normal subjects and patients with visual field defects. Vision Res. 2001, 41(8), 1073–84. [Google Scholar] [CrossRef] [PubMed]
- Barbur, JL; Forsyth, PM. Can the pupil response be used as a measure of the visual input associated with the geniculo-striate pathway? 1986. [Google Scholar]
- Gamlin, PD. The pretectum: connections and oculomotor-related roles. Prog Brain Res. 2006, 151, 379–405. [Google Scholar]
- Tekin, K; Sekeroglu, MA; Kiziltoprak, H; Doguizi, S; Inanc, M; Yilmazbas, P. Static and dynamic pupillometry data of healthy individuals. Clin Exp Optom. 2018, 101(5), 659–65. [Google Scholar] [CrossRef]
- Lowenstein, O; Loewenfeld, IE. Electronic pupillography; a new instrument and some clinical applications. AMA Arch Ophthalmol. 1958, 59(3), 352–63. [Google Scholar] [CrossRef]
- Diamond, JP. The Pupil. Anatomy, Physiology and Clinical Applications. Br J Ophthalmol. 2001, 85(1), 121e. [Google Scholar] [CrossRef]
- Maddess, T; Carle, CF; Kolic, M; Saraç, Ö; Essex, RW; Rohan, EMF; et al. Diagnostic Power and Reproducibility of Objective Perimetry in Glaucoma. J Glaucoma 2024, 33(12), 940–50. [Google Scholar] [CrossRef] [PubMed]
- Bayraktar, S; Hondur, G; Şekeroğlu, MA; Şen, E. Evaluation of Static and Dynamic Pupillary Functions in Early-Stage Primary Open Angle Glaucoma. J Glaucoma 2023, 32(7), e90–e4. [Google Scholar] [CrossRef]
- Bhowmik, S; Arjunan, SP; Sarossy, M; Radcliffe, P; Kumar, DK. Pupillometric recordings to detect glaucoma. Physiol Meas. 2021, 42(4). [Google Scholar] [CrossRef] [PubMed]
- Weisberg, LA. Mesencephalic hemorrhages: clinical and computed tomographic correlations. Neurology 1986, 36(5), 713–6. [Google Scholar] [CrossRef]
- Du, R; Meeker, M; Bacchetti, P; Larson, MD; Holland, MC; Manley, GT. Evaluation of the portable infrared pupillometer. Neurosurgery 2005, 57(1), 198-203; discussion 198-203. [Google Scholar] [CrossRef]
- Larson, MD; Behrends, M. Portable infrared pupillometry: a review. Anesth Analg. 2015, 120(6), 1242–53. [Google Scholar] [CrossRef]
- Solyman, O; Abushanab, MMI; Carey, AR; Henderson, AD. Pilot Study of Smartphone Infrared Pupillography and Pupillometry. Clin Ophthalmol. 2022, 16, 303–10. [Google Scholar] [CrossRef]
- Halperin, A; Pajuelo, M; Tornheim, JA; Vu, N; Carnero, AM; Galdos-Cardenas, G; et al. Pupillary Light Reflexes are Associated with Autonomic Dysfunction in Bolivian Diabetics But Not Chagas Disease Patients. Am J Trop Med Hyg. 2016, 94(6), 1290–8. [Google Scholar] [CrossRef]
- Negi, R; Kalivemula, M; Bisht, K; Bhate, M; Sachdeva, V; Bharadwaj, SR. Diagnostic accuracy of a modularized, virtual-reality-based automated pupillometer for detection of relative afferent pupillary defect in unilateral optic neuropathies. Front Ophthalmol (Lausanne) 2024, 4, 1396511. [Google Scholar] [CrossRef]
- Hayes, TR; Petrov, AA. Mapping and correcting the influence of gaze position on pupil size measurements. Behav Res Methods 2016, 48(2), 510–27. [Google Scholar] [CrossRef] [PubMed]
- Holland, E; Karpecki, P; Fingeret, M; Schaeffer, J; Gupta, P; Fram, N; et al. Efficacy and Safety of CSF-1 (0.4% Pilocarpine Hydrochloride) in Presbyopia: Pooled Results of the NEAR Phase 3 Randomized, Clinical Trials. Clin Ther. 2024, 46(2), 104–13. [Google Scholar] [CrossRef]
- Brown, SM; Bradley, JC. Comparison of 2 monocular pupillometers and an autorefractor for measurement of the dark-adapted pupil diameter. J Cataract Refract Surg. 2011, 37(4), 660–4. [Google Scholar] [CrossRef]
- Patwari, PP; Stewart, TM; Rand, CM; Carroll, MS; Kuntz, NL; Kenny, AS; et al. Pupillometry in congenital central hypoventilation syndrome (CCHS): quantitative evidence of autonomic nervous system dysregulation. Pediatr Res. 2012, 71(3), 280–5. [Google Scholar] [CrossRef] [PubMed]
- Muppidi, S; Adams-Huet, B; Tajzoy, E; Scribner, M; Blazek, P; Spaeth, EB; et al. Dynamic pupillometry as an autonomic testing tool. Clin Auton Res. 2013, 23(6), 297–303. [Google Scholar] [CrossRef] [PubMed]
- McAnany, JJ; Smith, BM; Garland, A; Kagen, SL. iPhone-based Pupillometry: A Novel Approach for Assessing the Pupillary Light Reflex. Optom Vis Sci. 2018, 95(10), 953–8. [Google Scholar] [CrossRef] [PubMed]
- Yoo, YJ; Yang, HK; Hwang, JM. Efficacy of digital pupillometry for diagnosis of Horner syndrome. PLoS One 2017, 12(6), e0178361. [Google Scholar] [CrossRef]
- Chang, DS; Arora, KS; Boland, MV; Supakontanasan, W; Friedman, DS. Development and validation of an associative model for the detection of glaucoma using pupillography. Am J Ophthalmol. 2013, 156(6), 1285–96.e2. [Google Scholar] [CrossRef]
- Park, JC; Moss, HE; McAnany, JJ. The Pupillary Light Reflex in Idiopathic Intracranial Hypertension. Invest Ophthalmol Vis Sci. 2016, 57(1), 23–9. [Google Scholar]
- Marshall, LF; Barba, D; Toole, BM; Bowers, SA. The oval pupil: clinical significance and relationship to intracranial hypertension. J Neurosurg. 1983, 58(4), 566–8. [Google Scholar] [CrossRef]
- Mittal, MK; Rabinstein, AA; Wijdicks, EF. Pearls & oy-sters: oval pupil: two observations. Neurology 2013, 81(17), e124-5. [Google Scholar]
- Jefferis, JM; Littlewood, RA; Pepper, IM; Hickman, SJ; Salvi, SM. Optic nerve sheath fenestration via a supero-medial eyelid skin crease approach for the treatment of idiopathic intracranial hypertension in a UK population. Eye (Lond) 2021, 35(5), 1418–26. [Google Scholar] [CrossRef]
- Atchison, DA; Girgenti, CC; Campbell, GM; Dodds, JP; Byrnes, TM; Zele, AJ. Influence of field size on pupil diameter under photopic and mesopic light levels. Clin Exp Optom. 2011, 94(6), 545–8. [Google Scholar] [CrossRef]
- Ferrari, GL; Marques, JL; Gandhi, RA; Heller, SR; Schneider, FK; Tesfaye, S; et al. Using dynamic pupillometry as a simple screening tool to detect autonomic neuropathy in patients with diabetes: a pilot study. Biomed Eng Online 2010, 9, 26. [Google Scholar] [CrossRef]
- Prasad, S; Baccon, J; Galetta, SL. Mydriatic pupil in giant cell arteritis. J Neurol Sci. 2009, 284(1-2), 196–7. [Google Scholar] [CrossRef]
- Wang, Y; Zekveld, AA; Naylor, G; Ohlenforst, B; Jansma, EP; Lorens, A; et al. Parasympathetic Nervous System Dysfunction, as Identified by Pupil Light Reflex, and Its Possible Connection to Hearing Impairment. PLoS One 2016, 11(4), e0153566. [Google Scholar] [CrossRef]
- McCall, WV; Sareddy, S; Youssef, NA; Miller, BJ; Rosenquist, PB. The pupillary light reflex as a point-of-care test for suicide risk: Preliminary results. Psychiatry Res. 2021, 295, 113582. [Google Scholar] [CrossRef] [PubMed]
- Strauch, C; Wang, CA; Einhäuser, W; Van der Stigchel, S; Naber, M. Pupillometry as an integrated readout of distinct attentional networks. Trends Neurosci. 2022, 45(8), 635–47. [Google Scholar] [CrossRef] [PubMed]
- Oster, J; Huang, J; White, BJ; Radach, R; Itti, L; Munoz, DP; et al. Pupillary responses to differences in luminance, color and set size. Exp Brain Res. 2022, 240(6), 1873–85. [Google Scholar] [CrossRef] [PubMed]
- Larson, MD; Singh, V. Portable infrared pupillometry in critical care. Crit Care 2016, 20(1), 161. [Google Scholar] [CrossRef]
- Zhao, W; Stutzman, S; DaiWai, O; Saju, C; Wilson, M; Aiyagari, V. Inter-device reliability of the NPi-100 pupillometer. J Clin Neurosci. 2016, 33, 79–82. [Google Scholar] [CrossRef]
- Anderson, M; Elmer, J; Shutter, L; Puccio, A; Alexander, S. Integrating Quantitative Pupillometry Into Regular Care in a Neurotrauma Intensive Care Unit. J Neurosci Nurs. 2018, 50(1), 30–6. [Google Scholar] [CrossRef]
- Godau, J; Bharad, K; Rösche, J; Nagy, G; Kästner, S; Weber, K; et al. Automated Pupillometry for Assessment of Treatment Success in Nonconvulsive Status Epilepticus. Neurocrit Care 2022, 36(1), 148–56. [Google Scholar] [CrossRef]
- Zyoud, SH; Zyoud, AH. Coronavirus disease-19 in environmental fields: a bibliometric and visualization mapping analysis. Environ Dev Sustain. 2021, 23(6), 8895–923. [Google Scholar] [CrossRef]
- Li, X; Zhang, T; Zhao, L; Liu, Q; Shi, C; Zhang, R. Mapping of Global Research on Electronic Cigarettes: A Bibliometric Analysis. Front Public Health 2022, 10, 856257. [Google Scholar] [CrossRef] [PubMed]
- van Eck, NJ; Waltman, L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics 2010, 84(2), 523–38. [Google Scholar] [CrossRef]
- Kulkarni, AV; Aziz, B; Shams, I; Busse, JW. Comparisons of citations in Web of Science, Scopus, and Google Scholar for articles published in general medical journals. Jama 2009, 302(10), 1092–6. [Google Scholar] [CrossRef]
- Martinez-Pulgarin, DF; Acevedo-Mendoza, WF; Cardona-Ospina, JA; Rodríguez-Morales, AJ; Paniz-Mondolfi, AE. A bibliometric analysis of global Zika research. Travel Med Infect Dis. 2016, 14(1), 55–7. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Calderón, S; Nasner-Posso, KM; Alfaro-Toloza, P; Paniz-Mondolfi, AE; Rodríguez-Morales, AJ. A bibliometric analysis of global Ebola research. Travel Med Infect Dis. 2015, 13(2), 202–4. [Google Scholar] [CrossRef] [PubMed]
- Gao, M; Gao, D; Sun, H; Cheng, X; An, L; Qiao, M. Trends in Research Related to Premenstrual Syndrome and Premenstrual Dysphoric Disorder From 1945 to 2018: A Bibliometric Analysis. Front Public Health 2021, 9, 596128. [Google Scholar] [CrossRef]
- Joshi, S; Li, Y; Kalwani, RM; Gold, JI. Relationships between Pupil Diameter and Neuronal Activity in the Locus Coeruleus, Colliculi, and Cingulate Cortex. Neuron 2016, 89(1), 221–34. [Google Scholar] [CrossRef]
- Joshi, S; Gold, JI. Pupil Size as a Window on Neural Substrates of Cognition. Trends Cogn Sci. 2020, 24(6), 466–80. [Google Scholar] [CrossRef]
- Murphy, PR; O'Connell, RG; O'Sullivan, M; Robertson, IH; Balsters, JH. Pupil diameter covaries with BOLD activity in human locus coeruleus. Hum Brain Mapp. 2014, 35(8), 4140–54. [Google Scholar] [CrossRef] [PubMed]
- Mathôt, S. Pupillometry: Psychology, Physiology, and Function. J Cogn. 2018, 1(1), 16. [Google Scholar] [CrossRef] [PubMed]
- van der Wel, P; van Steenbergen, H. Pupil dilation as an index of effort in cognitive control tasks: A review. Psychon Bull Rev. 2018, 25(6), 2005–15. [Google Scholar] [CrossRef]
- Laeng, B; Sirois, S; Gredebäck, G. Pupillometry: A Window to the Preconscious? Perspect Psychol Sci. 2012, 7(1), 18–27. [Google Scholar] [CrossRef]
- Hall, CA; Chilcott, RP. Eyeing up the Future of the Pupillary Light Reflex in Neurodiagnostics. In Diagnostics (Basel); 2018; 1, p. 8. [Google Scholar]
- Kret, ME; Sjak-Shie, EE. Preprocessing pupil size data: Guidelines and code. Behav Res Methods 2019, 51(3), 1336–42. [Google Scholar] [CrossRef]
- Aston-Jones, G; Cohen, JD. An integrative theory of locus coeruleus-norepinephrine function: adaptive gain and optimal performance. Annu Rev Neurosci. 2005, 28, 403–50. [Google Scholar] [CrossRef]
- Beatty, J. Task-evoked pupillary responses, processing load, and the structure of processing resources. Psychol Bull. 1982, 91(2), 276–92. [Google Scholar] [CrossRef] [PubMed]
- Kahneman, D; Beatty, J. Pupil diameter and load on memory. Science 1966, 154(3756), 1583–5. [Google Scholar] [CrossRef]
- Bradley, MM; Miccoli, L; Escrig, MA; Lang, PJ. The pupil as a measure of emotional arousal and autonomic activation. Psychophysiology 2008, 45(4), 602–7. [Google Scholar] [CrossRef]
- Gilzenrat, MS; Nieuwenhuis, S; Jepma, M; Cohen, JD. Pupil diameter tracks changes in control state predicted by the adaptive gain theory of locus coeruleus function. Cogn Affect Behav Neurosci. 2010, 10(2), 252–69. [Google Scholar] [CrossRef] [PubMed]
- Hess, EH; Polt, JM. Pupil Size in Relation to Mental Activity during Simple Problem-Solving. Science 1964, 143(3611), 1190–2. [Google Scholar] [CrossRef]
- Chen, JW; Gombart, ZJ; Rogers, S; Gardiner, SK; Cecil, S; Bullock, RM. Pupillary reactivity as an early indicator of increased intracranial pressure: The introduction of the Neurological Pupil index. Surg Neurol Int. 2011, 2, 82. [Google Scholar] [CrossRef] [PubMed]
- Redondo, B; Serramito, M; Vera, J; Alguacil-Espejo, M; Rubio-Martínez, M; Molina, R; et al. Diurnal Variation in Accommodation, Binocular Vergence, and Pupil Size. Optom Vis Sci. 2023, 100(12), 847–54. [Google Scholar] [CrossRef] [PubMed]
- Alpern, M; Mason, GL; Jardinico, RE. Vergence and accommodation. V. Pupil size changes associated with changes in accommodative vergence. Am J Ophthalmol. 1961, 52, 762–7. [Google Scholar] [CrossRef]
- Bharadwaj, SR; Roy, S; Satgunam, P. Spasm of Near Reflex: Objective Assessment of the Near-Triad. Invest Ophthalmol Vis Sci. 2020, 61(8), 18. [Google Scholar] [CrossRef]
- Dutta, P; Atiya, A; Vittal, S; Ambika, S; Hussaindeen, JR. Pupillary dynamics and accommodative response in mild traumatic brain injury. Taiwan J Ophthalmol. 2024, 14(2), 248–55. [Google Scholar] [CrossRef]
- Dutta, P. Characteristics of binocular vision and oculomotor function among sports-concussed athletes. Indian J Ophthalmol. 2023, 71(5), 2076–82. [Google Scholar] [CrossRef]
- Busby, A; Ciuffreda, KJ. The effect of apparent depth in pictorial images on accommodation. Ophthalmic Physiol Opt. 2005, 25(4), 320–7. [Google Scholar] [CrossRef]
- Marquart, G; Winter, JCFD. Workload assessment for mental arithmetic tasks using the task-evoked pupillary response. PeerJ 2015. [Google Scholar] [CrossRef]
- Kawata, H; Ohtsuka, K. Dynamic asymmetries in convergence eye movements under natural viewing conditions. Jpn J Ophthalmol. 2001, 45(5), 437–44. [Google Scholar] [CrossRef]
- Balaban, CD; Kiderman, A; Szczupak, M; Ashmore, RC; Hoffer, ME. Patterns of Pupillary Activity During Binocular Disparity Resolution. Front Neurol. 2018, 9, 990. [Google Scholar] [CrossRef]
- McDougal, DH; Gamlin, PD. Autonomic control of the eye. Compr Physiol. 2015, 5(1), 439–73. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, H. Disorders of the pupil. Handb Clin Neurol. 2011, 102, 427–66. [Google Scholar]
- Kawasaki, A. Disorders of the Pupil. Continuum (Minneap Minn) 2025, 31(2), 527–42. [Google Scholar] [CrossRef]
- Koshikawa, Y; Sato, A; Umeda, R; Ichibayashi, R. Diagnosis of Acute Glaucoma Attack Using a Quantitative Pupillometer: A Case Report. Cureus 2024, 16(11), e72850. [Google Scholar] [CrossRef] [PubMed]
- Herbst, K; Sander, B; Lund-Andersen, H; Wegener, M; Hannibal, J; Milea, D. Unilateral anterior ischemic optic neuropathy: chromatic pupillometry in affected, fellow non-affected and healthy control eyes. Front Neurol. 2013, 4, 52. [Google Scholar] [CrossRef] [PubMed]
- Kim, HM; Yang, HK; Hwang, JM. Quantitative analysis of pupillometry in isolated third nerve palsy. PLoS One 2018, 13(11), e0208259. [Google Scholar] [CrossRef]
- Casey, F; Van, HMT; Donovan, J; Nghia, HDT; Oanh, PKN; Thwaites, CL; et al. Automated pupillometry and optic nerve sheath diameter ultrasound to define tuberculous meningitis disease severity and prognosis. J Neurol Sci. 2023, 453, 120808. [Google Scholar] [CrossRef]
- Gil-Casas, A; Piñero, DP; Molina-Martín, A. Dynamic Pupillary Response in Multiple Sclerosis Patients with and without Optic Neuritis. Biomedicines 2023, 11(12). [Google Scholar] [CrossRef]
- Wilhelm, B; Lüdtke, H; Peters, T; Schmid, R; Wilhelm, H; Zrenner, E. Automated swinging flashlight test in patients with optic nerve diseases. Klin Monbl Augenheilkd 2001, 218(1), 21–5. [Google Scholar] [CrossRef]
- Lavertu, G; Tremblay, M; Michael, R; You, E; Chabot, G. Validation of a new cell phone application for quick screening of relative afferent pupillary defect. Can J Ophthalmol. 2025, 60(5), e680–e8. [Google Scholar] [CrossRef] [PubMed]
- Sarker, P; Zaman, N; Ong, J; Paladugu, P; Aldred, M; Waisberg, E; et al. Test-Retest Reliability of Virtual Reality Devices in Quantifying for Relative Afferent Pupillary Defect. Transl Vis Sci Technol. 2023, 12(6), 2. [Google Scholar] [CrossRef] [PubMed]
- Barbur, JL; Harlow, AJ; Sahraie, A. Pupillary responses to stimulus structure, colour and movement. Ophthalmic Physiol Opt. 1992, 12(2), 137–41. [Google Scholar] [CrossRef]
- Gamlin, PD; Zhang, H; Harlow, A; Barbur, JL. Pupil responses to stimulus color, structure and light flux increments in the rhesus monkey. Vision Res. 1998, 38(21), 3353–8. [Google Scholar] [CrossRef] [PubMed]
- Shindler, KS; Revere, K; Dutt, M; Ying, GS; Chung, DC. In vivo detection of experimental optic neuritis by pupillometry. Exp Eye Res. 2012, 100, 1–6. [Google Scholar] [CrossRef]
- Jakobsen, J. Pupillary function in multiple sclerosis. Acta Neurol Scand. 1990, 82(6), 392–5. [Google Scholar] [CrossRef]
- Bhowmik, S; Motin, MA; Sarossy, M; Radcliffe, P; Kumar, D. Sample entropy analysis of pupillary signals in glaucoma patients and control via light-induced pupillometry. Annu Int Conf IEEE Eng Med Biol Soc. 2020, 2020, 280–3. [Google Scholar]
- Volpe, NJ; Plotkin, ES; Maguire, MG; Hariprasad, R; Galetta, SL. Portable pupillography of the swinging flashlight test to detect afferent pupillary defects. Ophthalmology 2000, 107(10), 1913–21; discussion 22. [Google Scholar] [CrossRef]
- Volpe, NJ; Dadvand, L; Kim, SK; Maguire, MG; Ying, GS; Moster, ML; et al. Computerized binocular pupillography of the swinging flashlight test detects afferent pupillary defects. Curr Eye Res. 2009, 34(7), 606–13. [Google Scholar] [CrossRef]
- Bruegger, D; Grabe, HM; Vicini, R; Dysli, M; Lussi, D; Abegg, M. Detection of Relative Afferent Pupillary Defects Using Eye Tracking and a VR Headset. Transl Vis Sci Technol. 2023, 12(6), 22. [Google Scholar] [CrossRef]
- Kelbsch, C; Lange, J; Wilhelm, H; Wilhelm, B; Peters, T; Kempf, M; et al. Chromatic Pupil Campimetry Reveals Functional Defects in Exudative Age-Related Macular Degeneration with Differences Related to Disease Activity. Transl Vis Sci Technol. 2020, 9(6), 5. [Google Scholar] [CrossRef]
- Kardon, R; Anderson, SC; Damarjian, TG; Grace, EM; Stone, E; Kawasaki, A. Chromatic pupillometry in patients with retinitis pigmentosa. Ophthalmology 2011, 118(2), 376–81. [Google Scholar] [CrossRef]
- Nakayama, M; Nowak, W; Ishikawa, H; Asakawa, K; Ichibe, Y. Discovering irregular pupil light responses to chromatic stimuli using waveform shapes of pupillograms. EURASIP J Bioinform Syst Biol. 2014, 2014, 18. [Google Scholar] [CrossRef] [PubMed]
- Xu, W; Jia, F; Liu, J; Li, J; Zhao, J; Lin, S; et al. Digital Pupillometry and Centroid Shift Changes in Dominant and Nondominant Eyes. Klin Monbl Augenheilkd 2025, 242(1), 62–9. [Google Scholar] [CrossRef]
- Kiziltoprak, H; Tekin, K; Yetkin, E; Sekeroglu, MA. Static and Dynamic Pupil Characteristics in Myopic Anisometropic Amblyopia. Beyoglu Eye J. 2020, 5(2), 86–92. [Google Scholar] [CrossRef] [PubMed]
- Tekin, K; Kiziltoprak, H; Sekeroglu, MA; Yetkin, E; Bayraktar, S; Yilmazbas, P. Static and dynamic pupil characteristics in pseudoexfoliation syndrome and glaucoma. Clin Exp Optom. 2020, 103(3), 332–8. [Google Scholar] [CrossRef]
- de Vries, L; Fouquaet, I; Boets, B; Naulaers, G; Steyaert, J. Autism spectrum disorder and pupillometry: A systematic review and meta-analysis. Neurosci Biobehav Rev. 2021, 120, 479–508. [Google Scholar] [CrossRef]
- Baranowski, P; Karolewicz, B; Gajda, M; Pluta, J. Ophthalmic drug dosage forms: characterisation and research methods. ScientificWorldJournal 2014, 2014, 861904. [Google Scholar] [CrossRef]
- Farkouh, A; Frigo, P; Czejka, M. Systemic side effects of eye drops: a pharmacokinetic perspective. Clin Ophthalmol. 2016, 10, 2433–41. [Google Scholar] [CrossRef] [PubMed]
- Oliva, M. Pupil size and search performance in low and high perceptual load. Cogn Affect Behav Neurosci 2019, 19(2), 366–76. [Google Scholar] [CrossRef]
- Traylor, JI; El Ahmadieh, TY; Bedros, NM; Al Adli, N; Stutzman, SE; Venkatachalam, AM; et al. Quantitative pupillometry in patients with traumatic brain injury and loss of consciousness: A prospective pilot study. J Clin Neurosci. 2021, 91, 88–92. [Google Scholar] [CrossRef]
- Romagnoli, M; Stanzani Maserati, M; De Matteis, M; Capellari, S; Carbonelli, M; Amore, G; et al. Chromatic Pupillometry Findings in Alzheimer's Disease. Front Neurosci. 2020, 14, 780. [Google Scholar] [CrossRef]
- Giza, E; Fotiou, D; Bostantjopoulou, S; Katsarou, Z; Karlovasitou, A. Pupil light reflex in Parkinson's disease: evaluation with pupillometry. Int J Neurosci. 2011, 121(1), 37–43. [Google Scholar] [CrossRef] [PubMed]
- İşcan, D; Türkoğlu, C; Arslan, E. Evaluation of autonomic involvement in Parkinson's disease using pupillometry. Neurol Sci. 2025, 46(8), 3685–90. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, E; Muhafız, E; Erdoğan, CE; Nizamoğulları, Ş; Toprak, G; Meydan, B. Pupillographic evaluation accompanying structural and functional assessment of the optic nerve in patients with Parkinson's disease. BMC Ophthalmol. 2025, 25(1), 397. [Google Scholar] [CrossRef]
- Lin, TP; Rigby, H; Adler, JS; Hentz, JG; Balcer, LJ; Galetta, SL; et al. Abnormal visual contrast acuity in Parkinson's disease. J Parkinsons Dis. 2015, 5(1), 125–30. [Google Scholar] [CrossRef]
- Schwartz, R; Rothermich, K; Kotz, SA; Pell, MD. Unaltered emotional experience in Parkinson's disease: Pupillometry and behavioral evidence. J Clin Exp Neuropsychol. 2018, 40(3), 303–16. [Google Scholar] [CrossRef] [PubMed]
- Serbest Ceylanoglu, K; Sen, EM; Sekeroglu, MA. Static and dynamic pupillary features in graves' ophthalmopathy. Clin Exp Optom. 2023, 106(5), 551–5. [Google Scholar] [CrossRef]
- Kuskonmaz, SM; Kocer, AM; Onder, CE; Sekeroglu, MA. Static and dynamic pupillary features in graves disease without orbitopathy. Int Ophthalmol. 2024, 44(1), 428. [Google Scholar] [CrossRef]
- Lerner, AG; Bernabé-Ortiz, A; Ticse, R; Hernandez, A; Huaylinos, Y; Pinto, ME; et al. Type 2 diabetes and cardiac autonomic neuropathy screening using dynamic pupillometry. Diabet Med. 2015, 32(11), 1470–8. [Google Scholar] [CrossRef]
- Nuske, HJ; Vivanti, G; Hudry, K; Dissanayake, C. Pupillometry reveals reduced unconscious emotional reactivity in autism. Biol Psychol. 2014, 101, 24–35. [Google Scholar] [CrossRef]
- Jackson, I; Sirois, S. Infant cognition: going full factorial with pupil dilation. Dev Sci. 2009, 12(4), 670–9. [Google Scholar] [CrossRef]
- Jones, NP; Siegle, GJ; Mandell, D. Motivational and emotional influences on cognitive control in depression: A pupillometry study. Cogn Affect Behav Neurosci. 2015, 15(2), 263–75. [Google Scholar] [CrossRef]
- Yang, X; Fridman, AJ; Unsworth, N; Casement, MD. Pupillary motility responses to affectively salient stimuli in individuals with depression or elevated risk of depression: A systematic review and meta-analysis. Neurosci Biobehav Rev. 2023, 148, 105125. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, AL; Garcia, JB; Viera, EB; Santos, AM; Bertrand, RH. Pupillometry: the influence of gender and anxiety on the pain response. Pain Physician 2013, 16(3), E257-66. [Google Scholar]
- Siegle, GJ; Steinhauer, SR; Friedman, ES; Thompson, WS; Thase, ME. Remission prognosis for cognitive therapy for recurrent depression using the pupil: utility and neural correlates. Biol Psychiatry 2011, 69(8), 726–33. [Google Scholar] [CrossRef]
- Roecklein, K; Wong, P; Ernecoff, N; Miller, M; Donofry, S; Kamarck, M; et al. The post illumination pupil response is reduced in seasonal affective disorder. Psychiatry Res. 2013, 210(1), 150–8. [Google Scholar] [CrossRef]
- Laurenzo, SA; Kardon, R; Ledolter, J; Poolman, P; Schumacher, AM; Potash, JB; et al. Pupillary response abnormalities in depressive disorders. Psychiatry Res. 2016, 246, 492–9. [Google Scholar] [CrossRef] [PubMed]
- Fattal, J; Brascamp, JW; Slate, RE; Lehet, M; Achtyes, ED; Thakkar, KN. Blunted pupil light reflex is associated with negative symptoms and working memory in individuals with schizophrenia. Schizophr Res. 2022, 248, 254–62. [Google Scholar] [CrossRef] [PubMed]
- Aslan, MG; Uzun, F; Fındık, H; Kaçar, M; Okutucu, M; Hocaoğlu, Ç. Pupillometry measurement and its relationship to retinal structural changes in children with attention deficit hyperactivity disorder. Graefes Arch Clin Exp Ophthalmol. 2020, 258(6), 1309–17. [Google Scholar] [CrossRef]
- Segers, M; Bebko, JM; Zapparoli, BL; Stevenson, RA. A pupillometry study of multisensory social and linguistic processing in autism and typical development. Dev Psychol. 2020, 56(11), 2080–94. [Google Scholar] [CrossRef]
- Lowenstein, O; Feinberg, R; Loewenfeld, IE. Pupillary Movements During Acute and Chronic Fatigue A New Test for the Objective Evaluation of Tiredness. In Invest Ophthalmol; 1963. [Google Scholar]
- Regen, F; Dorn, H; Danker-Hopfe, H. Association between pupillary unrest index and waking electroencephalogram activity in sleep-deprived healthy adults. Sleep Med. 2013, 14(9), 902–12. [Google Scholar] [CrossRef]
- Urschitz, MS; Heine, K; Brockmann, PE; Peters, T; Durst, W; Poets, CF; et al. Subjective and objective daytime sleepiness in schoolchildren and adolescents: results of a community-based study. Sleep Med. 2013, 14(10), 1005–12. [Google Scholar] [CrossRef]
- Frohnhofen, H; Fulda, S; Frohnhofen, K; Popp, R. Validation of the Essener Questionnaire of Age and Sleepiness in the elderly using pupillometry. Adv Exp Med Biol. 2013, 755, 125–32. [Google Scholar] [PubMed]
- Wilhelm, B; Giedke, H; Lüdtke, H; Bittner, E; Hofmann, A; Wilhelm, H. Daytime variations in central nervous system activation measured by a pupillographic sleepiness test. J Sleep Res. 2001, 10(1), 1–7. [Google Scholar] [CrossRef] [PubMed]
- Danker-Hopfe, H; Kraemer, S; Dorn, H; Schmidt, A; Ehlert, I; Herrmann, WM. Time-of-day variations in different measures of sleepiness (MSLT, pupillography, and SSS) and their interrelations. Psychophysiology 2001, 38(5), 828–35. [Google Scholar] [CrossRef] [PubMed]
- Li, Z; Cai, J; Li, J; Xu, X; Zheng, L. Comparative evaluation of the bispectral index (BIS) and BISpro during propofol anaesthesia. J Int Med Res. 2021, 49(4), 3000605211001705. [Google Scholar] [CrossRef]
- Vide, S; Kreuzer, M; Ferreira, A; Couto, M; Agustí, M; Jaramillo, S; et al. Cortical, subcortical, brainstem and autonomic responses to nociception under total intravenous anesthesia. J Clin Anesth. 2025, 103, 111825. [Google Scholar] [CrossRef]
- Dallemagne, A; Anderloni, M; Havaux, M; Duranteau, O; Taccone, FS. Influence of Sevoflurane on the Neurological Pupil Index in Surgical and Critically Ill Patients: A Pilot Study. Brain Sci. 2024, 14(3). [Google Scholar] [CrossRef]
- Sabourdin, N; Diarra, C; Wolk, R; Piat, V; Louvet, N; Constant, I. Pupillary Pain Index Changes After a Standardized Bolus of Alfentanil Under Sevoflurane Anesthesia: First Evaluation of a New Pupillometric Index to Assess the Level of Analgesia During General Anesthesia. Anesth Analg. 2019, 128(3), 467–74. [Google Scholar] [CrossRef]
- Barvais, L; Engelman, E; Eba, JM; Coussaert, E; Cantraine, F; Kenny, GN. Effect site concentrations of remifentanil and pupil response to noxious stimulation. Br J Anaesth. 2003, 91(3), 347–52. [Google Scholar] [CrossRef]
- Larson, MD; Berry, PD; May, J; Bjorksten, A; Sessler, DI. Autonomic effects of epidural and intravenous fentanyl. Br J Anaesth. 2007, 98(2), 263–9. [Google Scholar] [CrossRef]
- Guglielminotti, J; Mentré, F; Gaillard, J; Ghalayini, M; Montravers, P; Longrois, D. Assessment of pain during labor with pupillometry: a prospective observational study. Anesth Analg. 2013, 116(5), 1057–62. [Google Scholar] [CrossRef]
- Saliman, NH; Belli, A; Blanch, RJ. Afferent Visual Manifestations of Traumatic Brain Injury. J Neurotrauma 2021, 38(20), 2778–89. [Google Scholar] [CrossRef]
- Stoll, J; Chatelle, C; Carter, O; Koch, C; Laureys, S; Einhäuser, W. Pupil responses allow communication in locked-in syndrome patients. Curr Biol. 2013, 23(15), R647–8. [Google Scholar] [CrossRef] [PubMed]
- Opic, P; Rüegg, S; Marsch, S; Gut, SS; Sutter, R. Automated Quantitative Pupillometry in the Critically Ill: A Systematic Review of the Literature. Neurology 2021, 97(6), e629–e42. [Google Scholar] [CrossRef] [PubMed]
- Jaquet, P; Couffignal, C; Tardivon, C; Godard, V; Bellot, R; Assouline, B; et al. PupillOmetry for preDIction of DeliriUM in ICU (PODIUM): protocol for a prospective multicentre cohort study. BMJ Open. 2023, 13(7), e072095. [Google Scholar] [CrossRef] [PubMed]
- Santini, T; Fuhl, W; Kasneci, E. PuReST: robust pupil tracking for real-time pervasive eye tracking; ACM, 2018. [Google Scholar]
- Villanueva, A; Cabeza, R; Porta, S. Eye tracking: Pupil orientation geometrical modeling. Image & Vision Computing 2006, 24(7), 663–79. [Google Scholar]
- Cavanagh, JF; Wiecki, TV; Kochar, A; Frank, MJ. Eye tracking and pupillometry are indicators of dissociable latent decision processes. J Exp Psychol Gen. 2014, 143(4), 1476–88. [Google Scholar] [CrossRef]
- Fountas, KN; Kapsalaki, EZ; Machinis, TG; Boev, AN; Robinson, JS; Troup, EC. Clinical implications of quantitative infrared pupillometry in neurosurgical patients. Neurocrit Care 2006, 5(1), 55–60. [Google Scholar] [CrossRef]
- Bitirgen, G; Korkmaz, C; Zamani, A; Iyisoy, MS; Kerimoglu, H; Malik, RA. Abnormal quantitative pupillary light responses following COVID-19. Int Ophthalmol. 2022, 42(9), 2847–54. [Google Scholar] [CrossRef]
- Serbest Ceylanoglu, K; Sen, EM; Sekeroglu, MA. Static and dynamic pupillary features in graves' ophthalmopathy. Clin Exp Optom. 2022, 1–5. [Google Scholar] [CrossRef]
- Crippa, SV; Pedrosa Domellöf, F; Kawasaki, A. Chromatic Pupillometry in Children. Front Neurol. 2018, 9, 669. [Google Scholar] [CrossRef] [PubMed]
- Sandroni, C; Citerio, G; Taccone, FS. Automated pupillometry in intensive care. Intensive Care Med 2022. [Google Scholar] [CrossRef] [PubMed]
- Mathôt, S; Vilotijević, A. Methods in cognitive pupillometry: Design, preprocessing, and statistical analysis. Behav Res Methods 2023, 55(6), 3055–77. [Google Scholar] [CrossRef]
- Favre, E; Rahmaty, Z; Ben-Hamouda, N; Miroz, JP; Abed-Maillard, S; Rusca, M; et al. Nociception assessment with videopupillometry in deeply sedated intensive care patients: Discriminative and criterion validations. Aust Crit Care 2024, 37(1), 84–90. [Google Scholar] [CrossRef] [PubMed]
- Fink, L; Simola, J; Tavano, A; Lange, E; Wallot, S; Laeng, B. From pre-processing to advanced dynamic modeling of pupil data. Behav Res Methods 2024, 56(3), 1376–412. [Google Scholar] [CrossRef]
- Mizera, J; Sova, M; Genzor, S; Krejci, T; Vachutka, J; Vanek, J; et al. Pupillography in contemporary sleep medicine - A narrative review. Neuro Endocrinol Lett. 2023, 44(5), 297–308. [Google Scholar]
- Nissen, C; Sander, B; Milea, D; Kolko, M; Herbst, K; Hamard, P; et al. Monochromatic Pupillometry in Unilateral Glaucoma Discloses no Adaptive Changes Subserved by the ipRGCs. Front Neurol 2014, 5, 15. [Google Scholar] [CrossRef]
- Martucci, A; Cesareo, M; Napoli, D; Sorge, RP; Ricci, F; Mancino, R; et al. Evaluation of pupillary response to light in patients with glaucoma: a study using computerized pupillometry. Int Ophthalmol. 2014, 34(6), 1241–7. [Google Scholar] [CrossRef]
- Park, HL; Jung, SH; Park, SH; Park, CK. Detectping autonomic dysfunction in patients with glaucoma using dynamic pupillometry. Medicine (Baltimore) 2019, 98(11), e14658. [Google Scholar] [CrossRef]
- Rukmini, AV; Chew, MC; Finkelstein, MT; Atalay, E; Baskaran, M; Nongpiur, ME; et al. Effects of low and moderate refractive errors on chromatic pupillometry. Sci Rep. 2019, 9(1), 4945. [Google Scholar] [CrossRef] [PubMed]
- Mabed, IS; Saad, A; Guilbert, E; Gatinel, D. Measurement of pupil center shift in refractive surgery candidates with caucasian eyes using infrared pupillometry. J Refract Surg. 2014, 30(10), 694–700. [Google Scholar] [CrossRef]
- Vilotijević, A; Mathôt, S. Functional benefits of cognitively driven pupil-size changes. Wiley Interdiscip Rev Cogn Sci. 2024, 15(3), e1672. [Google Scholar] [CrossRef]
- Murphy, PR; Robertson, IH; Balsters, JH; O'Connell, R G. Pupillometry and P3 index the locus coeruleus-noradrenergic arousal function in humans. Psychophysiology 2011, 48(11), 1532–43. [Google Scholar] [CrossRef] [PubMed]
- Lynch, G. Using Pupillometry to Assess the Atypical Pupillary Light Reflex and LC-NE System in ASD. Behav Sci (Basel) 2018, 8(11). [Google Scholar] [CrossRef] [PubMed]
- Jahns, FP; Miroz, JP; Messerer, M; Daniel, RT; Taccone, FS; Eckert, P; et al. Quantitative pupillometry for the monitoring of intracranial hypertension in patients with severe traumatic brain injury. Crit Care 2019, 23(1), 155. [Google Scholar] [CrossRef]
- El Ahmadieh, TY; Bedros, N; Stutzman, SE; Nyancho, D; Venkatachalam, AM; MacAllister, M; et al. Automated Pupillometry as a Triage and Assessment Tool in Patients with Traumatic Brain Injury. World Neurosurg. 2021, 145, e163–e9. [Google Scholar] [CrossRef]
- Fotiou, DF; Stergiou, V; Tsiptsios, D; Lithari, C; Nakou, M; Karlovasitou, A. Cholinergic deficiency in Alzheimer's and Parkinson's disease: evaluation with pupillometry. Int J Psychophysiol. 2009, 73(2), 143–9. [Google Scholar] [CrossRef]
- El Haj, M; Chapelet, G; Moustafa, AA; Boutoleau-Bretonnière, C. Pupil size as an indicator of cognitive activity in mild Alzheimer's disease. Excli j. 2022, 21, 307–16. [Google Scholar] [PubMed]
- Oddo, M; Taccone, FS; Petrosino, M; Badenes, R; Blandino-Ortiz, A; Bouzat, P; et al. The Neurological Pupil index for outcome prognostication in people with acute brain injury (ORANGE): a prospective, observational, multicentre cohort study. Lancet Neurol. 2023, 22(10), 925–33. [Google Scholar] [CrossRef]
- Choi, J; Corcoran, CM; Fiszdon, JM; Stevens, M; Javitt, DC; Deasy, M; et al. Pupillometer-based neurofeedback cognitive training to improve processing speed and social functioning in individuals at clinical high risk for psychosis. Psychiatr Rehabil J. 2017, 40(1), 33–42. [Google Scholar] [CrossRef] [PubMed]
- Mestanikova, A; Ondrejka, I; Mestanik, M; Cesnekova, D; Visnovcova, Z; Bujnakova, I; et al. Pupillary light reflex is altered in adolescent depression. Physiol Res. 2017, 66 (Suppl 2), S277–s84. [Google Scholar] [CrossRef]
- Berman, G; Muttuvelu, D; Berman, D; Larsen, JI; Licht, RW; Ledolter, J; et al. Decreased retinal sensitivity in depressive disorder: a controlled study. Acta Psychiatr Scand. 2018, 137(3), 231–40. [Google Scholar] [CrossRef]
- Barry, C; Wang, E. Racially fair pupillometry measurements for RGB smartphone cameras using the far red spectrum. Sci Rep. 2023, 13(1), 13841. [Google Scholar] [CrossRef] [PubMed]
- Pelagatti, C; Blini, E; Vannucci, M. Catching Mind Wandering With Pupillometry: Conceptual and Methodological Challenges. Wiley Interdiscip Rev Cogn Sci. 2025, 16(1), e1695. [Google Scholar] [CrossRef]
- Vinclair, M; Schilte, C; Roudaud, F; Lavolaine, J; Francony, G; Bouzat, P; et al. Using Pupillary Pain Index to Assess Nociception in Sedated Critically Ill Patients. Anesth Analg. 2019, 129(6), 1540–6. [Google Scholar] [CrossRef]
- Vide, S; Castro, A; Correia, R; Cabral, T; Lima, D; Nunes, CS; et al. Foreseeing postoperative pain in neurosurgical patients: pupillometry predicts postoperative pain ratings-an observational study. J Clin Monit Comput. 2021, 35(5), 1111–8. [Google Scholar] [CrossRef]
- Zugni, N; Guadrini, L; Rasulo, F. Noninvasive neuromonitoring in the operating room and its role in the prevention of delirium. Best Pract Res Clin Anaesthesiol. 2021, 35(2), 191–206. [Google Scholar] [CrossRef]
- Paramanathan, S; Grejs, AM; Søreide, E; Duez, CHV; Jeppesen, AN; Reinertsen Å, J; et al. Quantitative pupillometry in comatose out-of-hospital cardiac arrest patients: A post-hoc analysis of the TTH48 trial. Acta Anaesthesiol Scand. 2022, 66(7), 880–6. [Google Scholar] [CrossRef]
- Fratino, S; Garré, A; Garufi, A; Hafidi, S; Migliorino, E; Stropeni, S; et al. Evaluation of nociception in unconscious critically ill patients using a multimodal approach. Anaesth Crit Care Pain Med. 2023, 42(2), 101175. [Google Scholar] [CrossRef]
- Kornilov, E; Gehlen, L; Yacobi, D; Soehle, M; Kowark, A; Thudium, M. Pupillary Pain Index Predicts Postoperative Pain but Not the Effect of Peripheral Regional Anaesthesia in Patients Undergoing Total Hip or Total Knee Arthroplasty: An Observational Study. Medicina (Kaunas) 2023, 59(5). [Google Scholar] [CrossRef]
- Singh, A; Akhileshwar; Kumar, N; De, RR; Bahadur, R; Shekhar, S. The Role of Pupillometry in the Assessment of Pain in Children Under General Anesthesia: A Prospective Single-Blinded Observational Study. Cureus 2023, 15(8), e43894. [Google Scholar] [CrossRef]
- Nyholm, B; Grand, J; Obling, LER; Hassager, C; Møller, JE; Schmidt, H; et al. Quantitative pupillometry for neuroprognostication in comatose post-cardiac arrest patients: A protocol for a predefined sub-study of the Blood pressure and Oxygenations Targets after Out-of-Hospital Cardiac Arrest (BOX)-trial. Resusc Plus 2023, 16, 100475. [Google Scholar] [CrossRef] [PubMed]
- Ma, X; Monfared, R; Grant, R; Goh, YM. Determining Cognitive Workload Using Physiological Measurements: Pupillometry and Heart-Rate Variability. Sensors (Basel) 2024, 24(6). [Google Scholar] [CrossRef]
- Krafthöfer, J; Fabig, SC; Baron, R; Gierthmühlen, J. Pupillometry as a Potential Objective Measurement of Pain Assessment in Healthy Volunteers. J Pain Res. 2024, 17, 2037–42. [Google Scholar] [CrossRef]
- Zhang, Y; Lim, D; Yao, Y; Dong, C; Feng, Z. Global Research Trends in Radiotherapy for Gliomas: A Systematic Bibliometric Analysis. World Neurosurg. 2022, 161, e355–e62. [Google Scholar] [CrossRef] [PubMed]
- Fu, HZ; Wang, MH; Ho, YS. The most frequently cited adsorption research articles in the Science Citation Index (Expanded). J Colloid Interface Sci. 2012, 379(1), 148–56. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(A) Key components of the pupillary light reflex. (B) A flowchart representing retrieval strategies for pupillometry articles from the WOS SCI-Expanded database and the inclusion criteria for the study. (C) The whole flow chart of bibliometric analysis for pupillometry in this study.
Figure 1.
(A) Key components of the pupillary light reflex. (B) A flowchart representing retrieval strategies for pupillometry articles from the WOS SCI-Expanded database and the inclusion criteria for the study. (C) The whole flow chart of bibliometric analysis for pupillometry in this study.
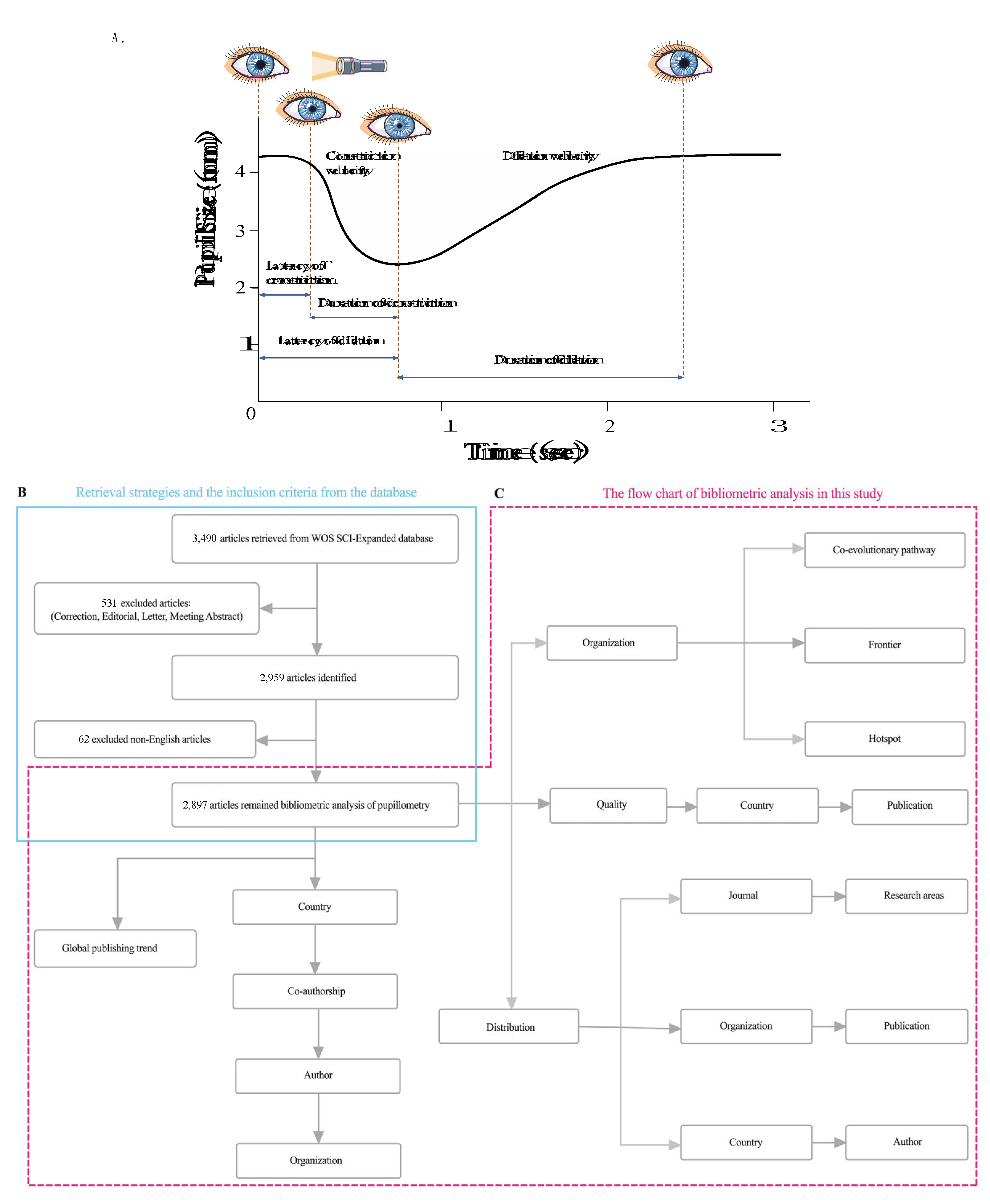
Figure 2.
Trends in the growth of publications and the number of cited articles worldwide from 1999 to 2025. (A) The annual publication, and annual citation. (B) The annual publication in the top 10 countries.
Figure 2.
Trends in the growth of publications and the number of cited articles worldwide from 1999 to 2025. (A) The annual publication, and annual citation. (B) The annual publication in the top 10 countries.
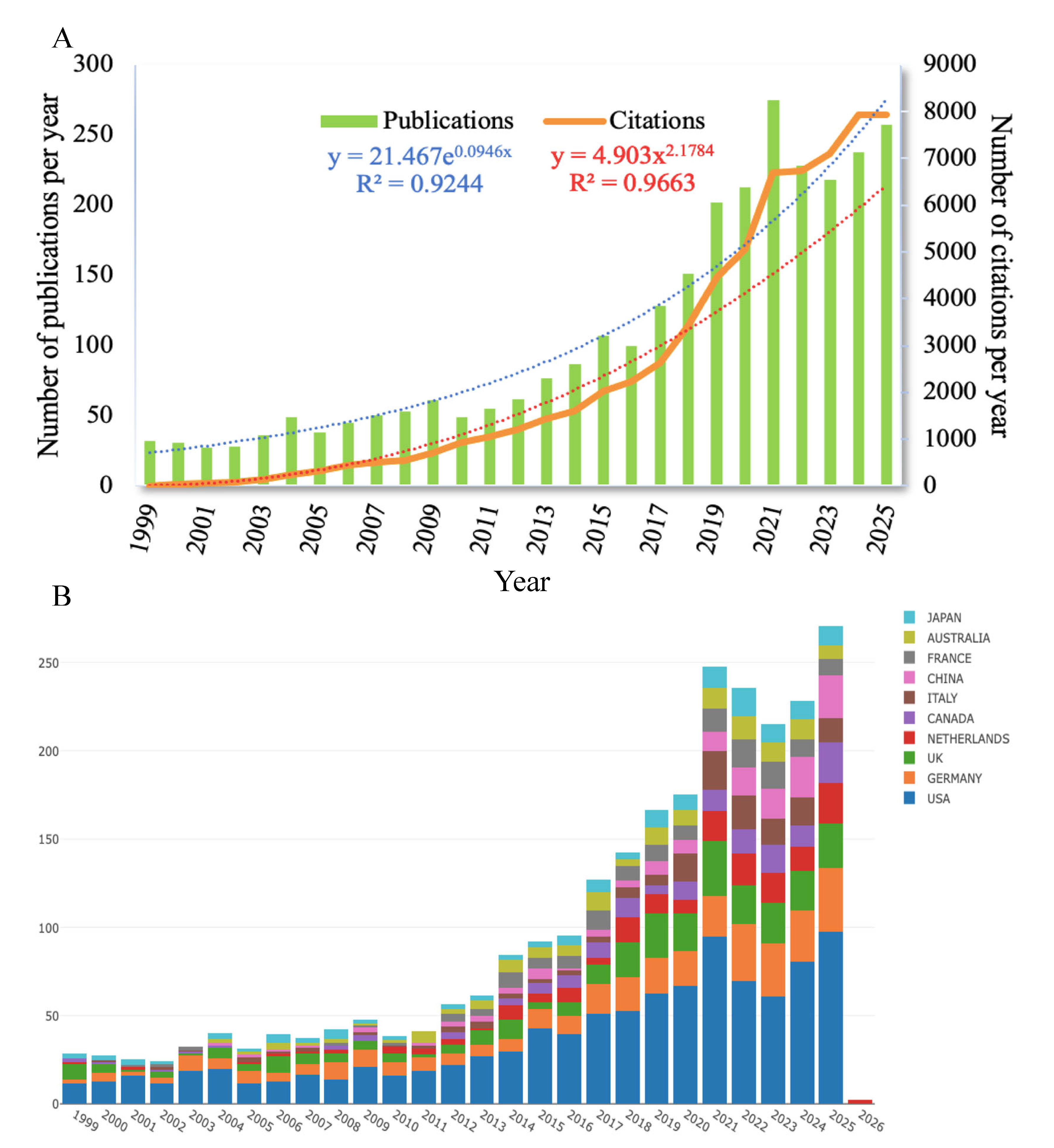
Figure 3.
Countries and institutions related to pupillometry research published worldwide. (A) The distribution world map of pupillometry. (B) Network map of the country distribution for pupillometry. (C) Distribution of main countries from 1999 to 2025 in the pupillometry field. The minimum number of a country’s number was set as 5. A total of 53 countries met the threshold of 89 countries. (D) Cooperation network of main research organizations from 1999 to 2025 in the pupillometry field. The minimum number of documents of an organization was set as 5. A total of 306 organizations of the 3,019 organizations met the threshold.
Figure 3.
Countries and institutions related to pupillometry research published worldwide. (A) The distribution world map of pupillometry. (B) Network map of the country distribution for pupillometry. (C) Distribution of main countries from 1999 to 2025 in the pupillometry field. The minimum number of a country’s number was set as 5. A total of 53 countries met the threshold of 89 countries. (D) Cooperation network of main research organizations from 1999 to 2025 in the pupillometry field. The minimum number of documents of an organization was set as 5. A total of 306 organizations of the 3,019 organizations met the threshold.
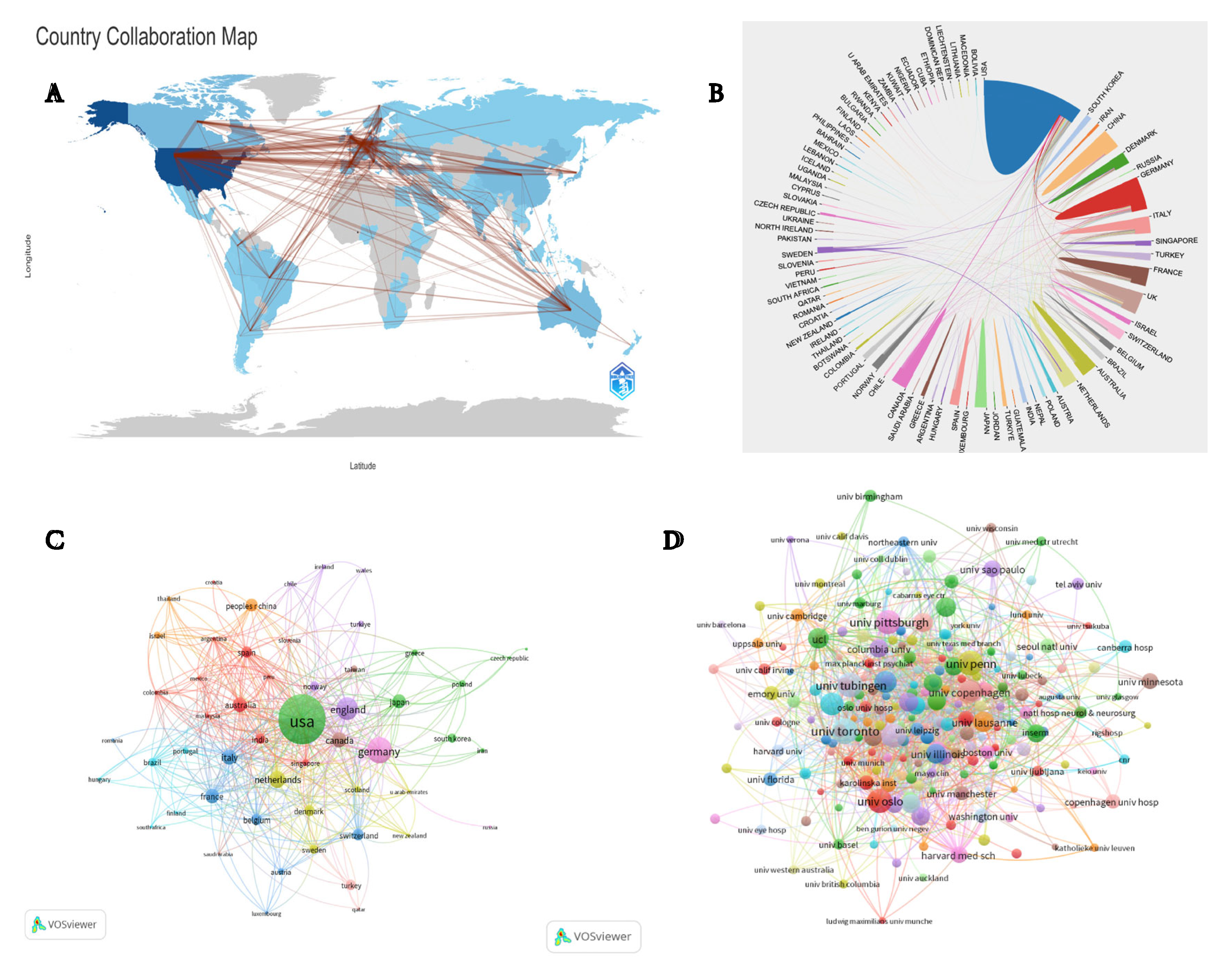
Figure 4.
Analysis of authors, keyword co-occurrence and references involved in pupillometry field. (A) Timeline distribution of publications from the top 10 active authors. (B) Co-authorship network of productive authors from 1999 to 2025 in the pupillometry field. The minimum number of documents of an author was set as 5. A total of 174 authors met the threshold of the 11,534 authors that were involved in this study. (C) Author local impact by H-index. (D) Top 25 references with the strongest citation bursts involved in the pupillometry field. (E) Sources’ local impact by H-index.
Figure 4.
Analysis of authors, keyword co-occurrence and references involved in pupillometry field. (A) Timeline distribution of publications from the top 10 active authors. (B) Co-authorship network of productive authors from 1999 to 2025 in the pupillometry field. The minimum number of documents of an author was set as 5. A total of 174 authors met the threshold of the 11,534 authors that were involved in this study. (C) Author local impact by H-index. (D) Top 25 references with the strongest citation bursts involved in the pupillometry field. (E) Sources’ local impact by H-index.
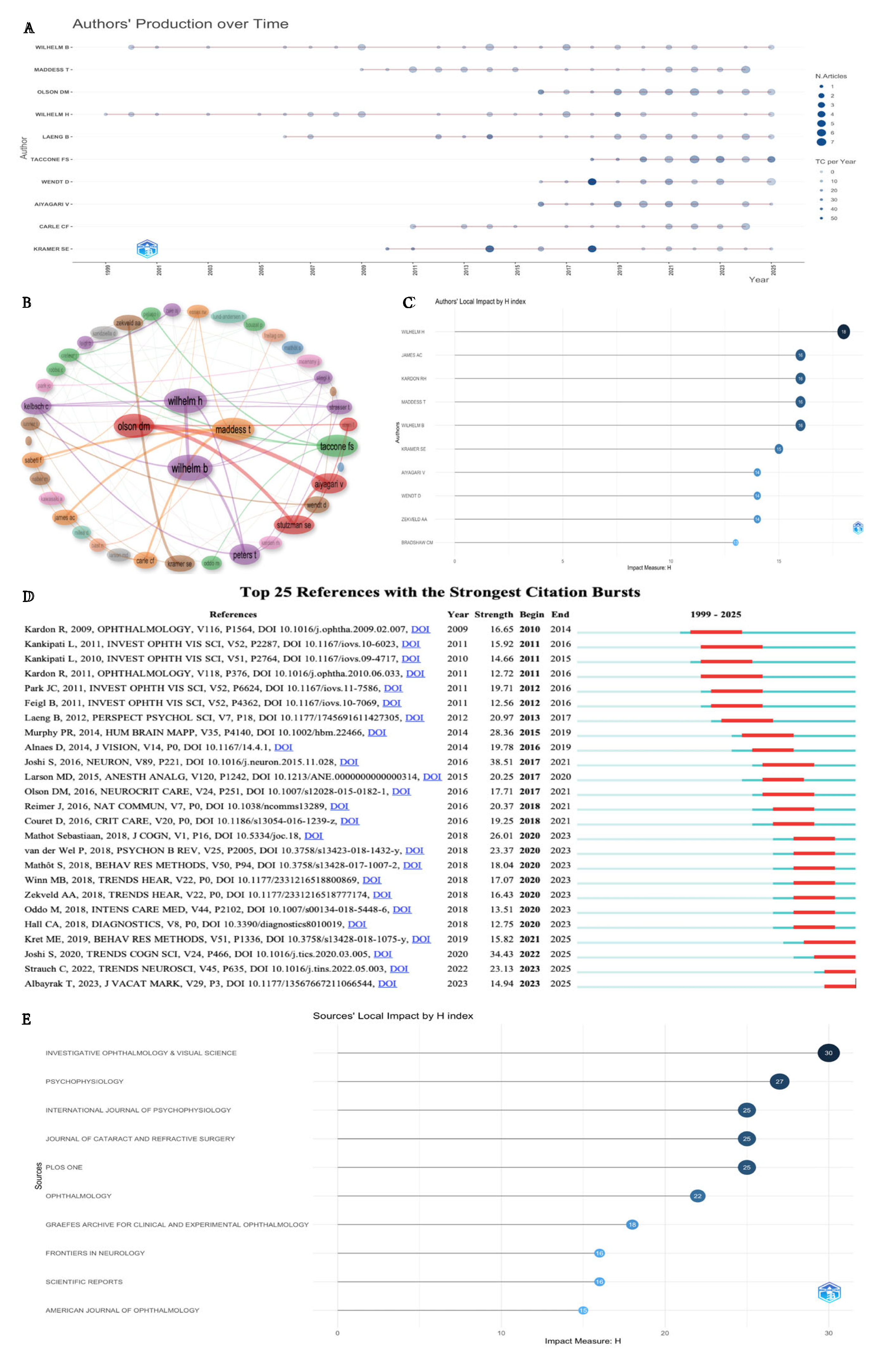
Figure 5.
Keyword-related mapping in studies of the pupillometry. (A) The relationship of the top 20 co-cited references, authors, and keywords evolution based on an alluvial flow map. (B) Visualization based on cloudword for top 50 keyword co-occurrences. (C) Network visualization map of keyword co-occurrence analysis using VOS viewer. All keywords are labeled. The size of the node reflects the occurrence frequency of a certain keyword. The larger the size of the node is, the more frequently the keyword co-occurs. VOS viewer marks keywords with different colors, and the color of the nodes and labels indicates the cluster in which they belong to. Closely related keywords are grouped into one cluster with the same color. The higher the quantity of co-occurrences of two keywords, the closer will they be located in the network.
Figure 5.
Keyword-related mapping in studies of the pupillometry. (A) The relationship of the top 20 co-cited references, authors, and keywords evolution based on an alluvial flow map. (B) Visualization based on cloudword for top 50 keyword co-occurrences. (C) Network visualization map of keyword co-occurrence analysis using VOS viewer. All keywords are labeled. The size of the node reflects the occurrence frequency of a certain keyword. The larger the size of the node is, the more frequently the keyword co-occurs. VOS viewer marks keywords with different colors, and the color of the nodes and labels indicates the cluster in which they belong to. Closely related keywords are grouped into one cluster with the same color. The higher the quantity of co-occurrences of two keywords, the closer will they be located in the network.
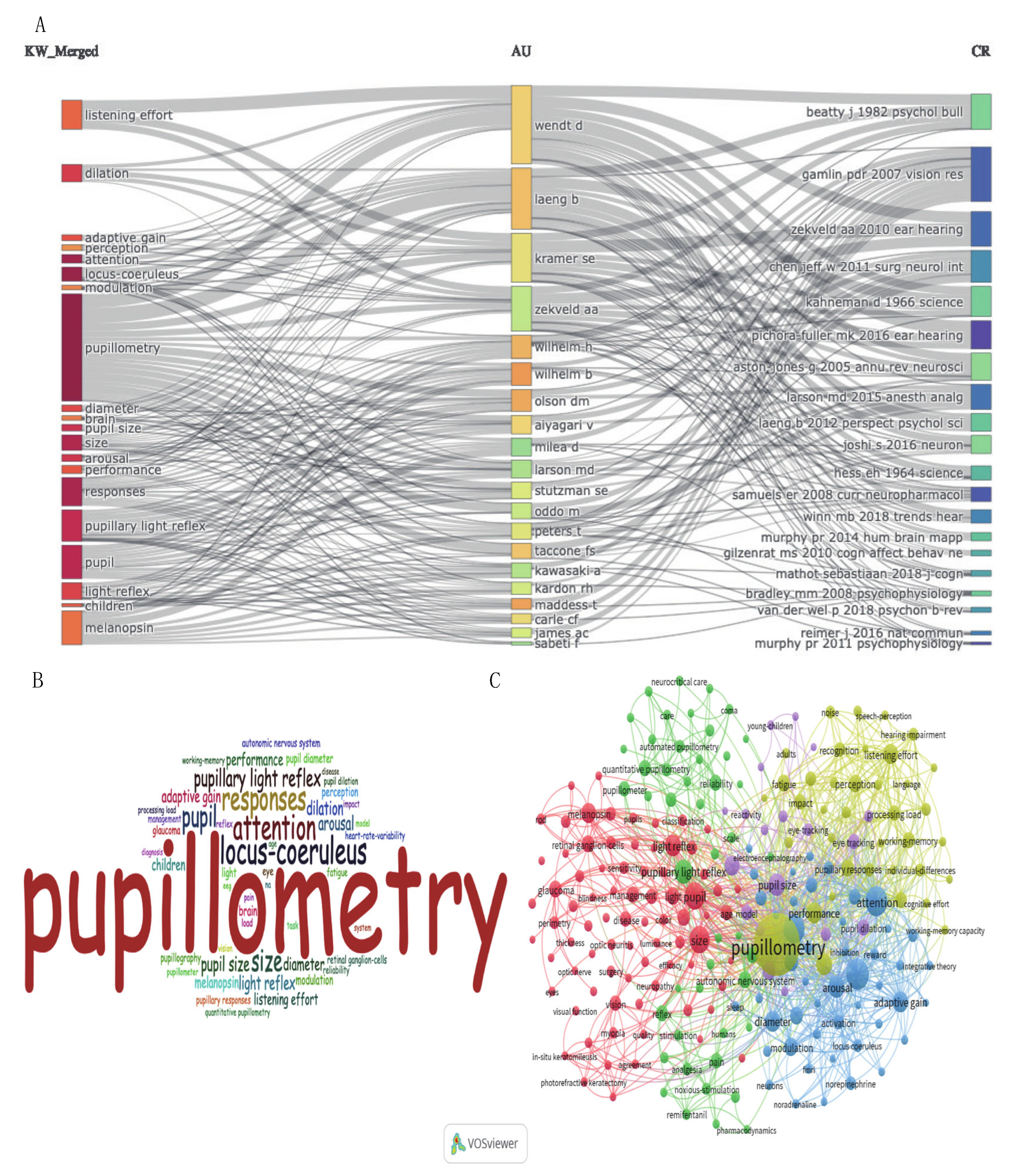
Figure 6.
| Keyword strongest citation burst and evolution in studies of the pupillometry. (A) Major keywords evolution of pupillometry research. (B) Evolutionary pathway in the study of pupillometry: The position of each node represents when it first appeared, and the lines between nodes represent relationships between keywords. The node colors represent different years, from cold to warm means period from 1999 to 2025. Bluish purple indicates the previous keyword, and red indicates the latest keyword. Longer colored segments indicate a larger reference time span. The flow of knowledge between clusters from cool to warm colors can also be observed over time. (C) The top 25 burst keywords from 1999 to 2025 in the pupillometry field.
Figure 6.
| Keyword strongest citation burst and evolution in studies of the pupillometry. (A) Major keywords evolution of pupillometry research. (B) Evolutionary pathway in the study of pupillometry: The position of each node represents when it first appeared, and the lines between nodes represent relationships between keywords. The node colors represent different years, from cold to warm means period from 1999 to 2025. Bluish purple indicates the previous keyword, and red indicates the latest keyword. Longer colored segments indicate a larger reference time span. The flow of knowledge between clusters from cool to warm colors can also be observed over time. (C) The top 25 burst keywords from 1999 to 2025 in the pupillometry field.
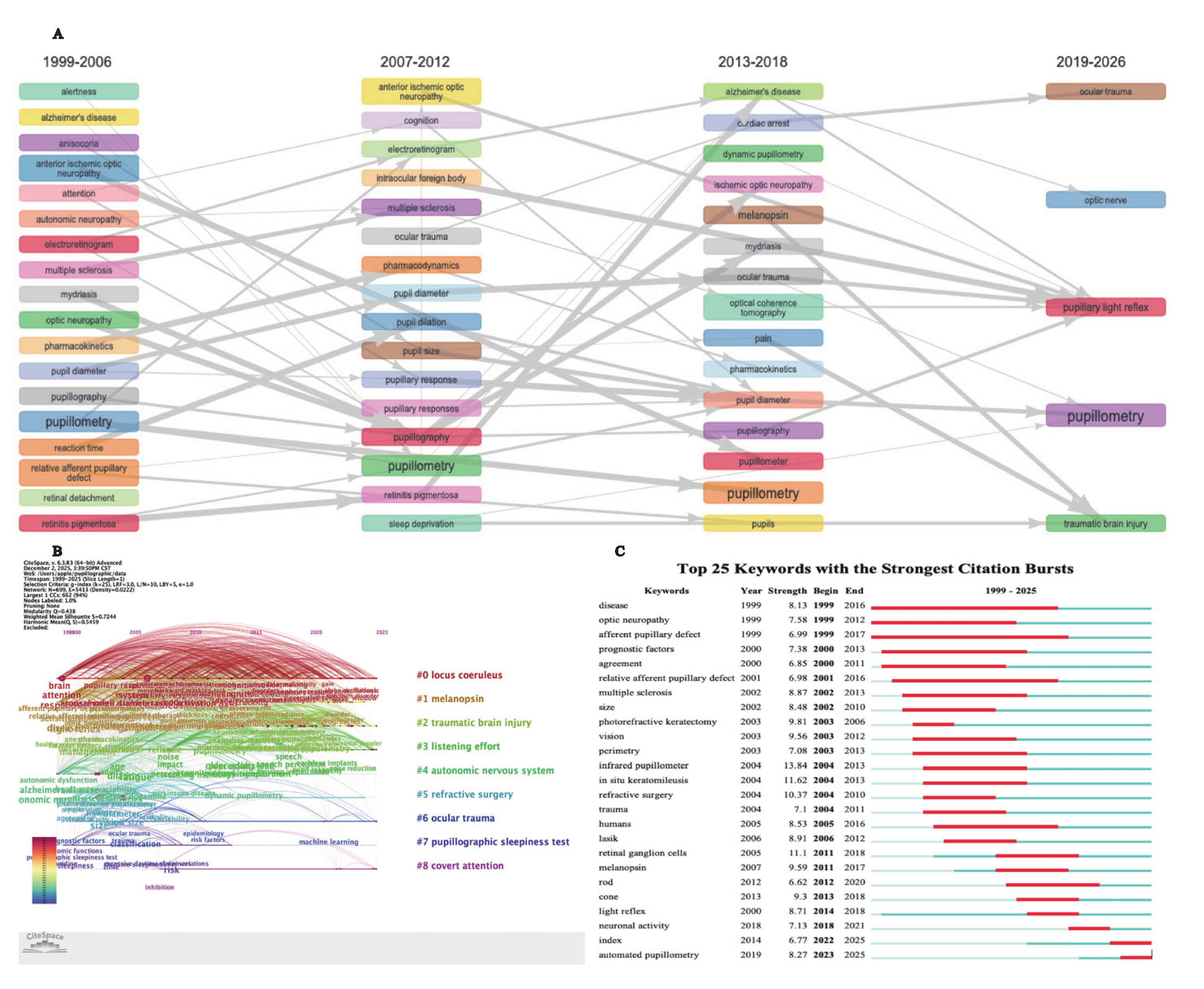

Table 1.
The quantity of pupillometry research in terms of years.
| Year | Publications | Citations |
|---|---|---|
| 1999 | 32 | 6 |
| 2000 | 31 | 32 |
| 2001 | 27 | 60 |
| 2002 | 28 | 86 |
| 2003 | 36 | 147 |
| 2004 | 49 | 249 |
| 2005 | 38 | 331 |
| 2006 | 45 | 452 |
| 2007 | 50 | 501 |
| 2008 | 53 | 548 |
| 2009 | 61 | 704 |
| 2010 | 49 | 931 |
| 2011 | 55 | 1,049 |
| 2012 | 62 | 1,217 |
| 2013 | 77 | 1,434 |
| 2014 | 87 | 1,601 |
| 2015 | 107 | 2,020 |
| 2016 | 100 | 2,230 |
| 2017 | 128 | 2,629 |
| 2018 | 151 | 3,417 |
| 2019 | 202 | 4,453 |
| 2020 | 213 | 5,050 |
| 2021 | 275 | 6,686 |
| 2022 | 228 | 6,732 |
| 2023 | 218 | 7,093 |
| 2024 | 238 | 7,941 |
| 2025 | 257 | 7,923 |
| Total | 2,897 | 65,552 |
Table 2.
The top 10 countries contributed to publications in the pupillometry field.
| Rank | Country | Documents | Citations | Citation/ Document (%) | Centrality | Total link strength |
|---|---|---|---|---|---|---|
| 1 | USA | 1,086 | 29,243 | 26.92 | 0.38 | 440 |
| 2 | Germany | 351 | 8,482 | 24.16 | 0.12 | 274 |
| 3 | England | 267 | 7,380 | 27.64 | 0.30 | 254 |
| 4 | Netherlands | 168 | 6,251 | 37.20 | 0.10 | 211 |
| 5 | Canada | 146 | 3,332 | 22.82 | 0.01 | 127 |
| 6 | Italy | 145 | 3,435 | 23.68 | 0.13 | 192 |
| 7 | France | 136 | 3,483 | 25.61 | 0.07 | 132 |
| 8 | Australia | 135 | 3,784 | 28.02 | 0.23 | 124 |
| 9 | Japan | 122 | 1,703 | 13.95 | 0.04 | 56 |
| 10 | China | 106 | 1,003 | 9.46 | 0.05 | 47 |
Table 3.
Top ten productive organizations from 1999 to 2025 in the pupillometry field.
| Rank | Organization | Country | Documents | Citations | Citation/ Document (%) (%) | Centrality |
|---|---|---|---|---|---|---|
| 1 | University of Toronto | Canada | 46 | 1,134 | 24.65 | 0.05 |
| 2 | University of Pennsylvania | USA | 43 | 2,517 | 58.53 | 0.08 |
| 3 | University of Tubingen | Germany | 43 | 980 | 22,79 | 0.03 |
| 4 | University of Oslo | Norway | 41 | 1,047 | 25.53 | 0.03 |
| 5 | Johns Hopkins University | USA | 40 | 770 | 19.25 | 0.11 |
| 6 | University of Pittsburgh | USA | 40 | 1,099 | 27.47 | 0.05 |
| 7 | Australian National University | Australia | 37 | 580 | 15.67 | 0.01 |
| 8 | University of Copenhagen | Denmark | 36 | 377 | 10.47 | 0.02 |
| 9 | University of California San Francisco | USA | 35 | 1,162 | 33.20 | 0.06 |
| 10 | Technical University of Denmark | Denmark | 33 | 938 | 28.42 | 0.01 |
Table 4.
Top ten productive authors and co-cited authors from 1999 to 2025 in the pupillometry field.
Table 4.
Top ten productive authors and co-cited authors from 1999 to 2025 in the pupillometry field.
| Rank | Author | Documents | Citations | H-index | Co-cited author | Citations | Total link strength |
|---|---|---|---|---|---|---|---|
| 1 | Olson Daiwai M | 34 | 703 | 13 | Beatty J | 527 | 14,690 |
| 2 | Meddess Ted | 33 | 554 | 16 | Kahneman D | 515 | 14,743 |
| 3 | Laeng Bruno | 29 | 956 | 13 | Zekveld AA | 494 | 16,363 |
| 4 | Wilhelm Barbara | 28 | 398 | 16 | Larson MD | 457 | 6,607 |
| 5 | Wihelm Helmut | 27 | 553 | 18 | Aston-jones G | 454 | 13,492 |
| 6 | Wendt Dorothea | 26 | 788 | 14 | Laeng B | 414 | 10,003 |
| 7 | Aiyagari Venkatesh | 25 | 696 | 14 | Joshi S | 412 | 11,224 |
| 8 | Peters Tobias | 22 | 442 | 13 | Murphy PR | 374 | 11,651 |
| 9 | Stutzman Sonja E | 22 | 423 | 12 | Unsworth N | 366 | 12,517 |
| 10 | Kramer Sophia E | 21 | 1,735 | 15 | Mathot S | 340 | 8,967 |
Table 5.
The top 10 journals and research areas in the study of pupillometry.
| Rank | Journal | Country | Documents (%) | Citations | Total link strength | IF (2024) | Co-cited journal | Citations | Total link strength |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Psychophysiology | USA | 79 (2.72) | 3,106 | 913 | 2.9 | IOVS | 3,008 | 150,007 |
| 2 | Scientific Reports | England | 74 (2.55) | 897 | 636 | 2.9 | Psychophysiology | 2,593 | 157,620 |
| 3 | Plos One | USA | 74 (2.55) | 1,993 | 621 | 3.8 | Ophthalmology | 2,045 | 84,424 |
| 4 | IOVS | USA | 69 (2.38) | 2,656 | 940 | 5.0 | Journal of Neuroscience | 1,987 | 135,029 |
| 5 | Journal of Cataract and Refractive Surgery | USA | 53 (1.82) | 1,473 | 358 | 2.6 | Plos One | 1,760 | 108,990 |
| 6 | Graefes Archive for Clinical and Experimental Ophthalmology | USA | 48 (1.65) | 848 | 392 | 2.3 | Science | 1,629 | 96,516 |
| 7 | International Journal of Psychophysiology | Netherlands | 46 (1.58) | 1,714 | 422 | 2.7 | Neuroimage | 1,526 | 102,829 |
| 8 | Frontiers in Neurology | Switzerland | 42 (1.44) | 986 | 602 | 2.9 | American Journal of Ophthalmology | 1,426 | 97,259 |
| 9 | Journal of Neuro-ophthalmology | USA | 37 (1.27) | 721 | 152 | 2.6 | Neuron | 1,414 | 55,775 |
| 10 | Ophthalmic Plastic and Reconstructive Surgery | USA | 35 (1.20) | 330 | 599 | 1.3 | Ear and Hearing | 1,346 | 75,559 |
IOVS, Investigative Ophthalmology & Visual Science; PNAS, Proceedings of the National Academy of Sciences of the United States of America.
Table 6.
Top ten co-cited references in pupillometry research from 1999 to 2025 in the pupillometry field.
Table 6.
Top ten co-cited references in pupillometry research from 1999 to 2025 in the pupillometry field.
| Rank | Cited reference | Title | Citations | Total link strength |
|---|---|---|---|---|
| 1 | aston-jones g, 2005, annu rev neurosci, v28, p403, doi 10.1146/annurev.neuro.28.061604.135709 | An integrative theory of locus coeruleus-norepinephrine function: adaptive gain and optimal performance | 359 | 6,684 |
| 2 | joshi s, 2016, neuron, v89, p221, doi 10.1016/j.neuron.2015.11.028 | Relationships between Pupil Diameter and Neuronal Activity in the Locus Coeruleus, Colliculi, and Cingulate Cortex | 271 | 4,667 |
| 3 | beatty j, 1982, psychol bull, v91, p276, doi 10.1037/0033-2909.91.2.276 | Task-evoked pupillary responses, processing load, and the structure of processing resources | 263 | 4,362 |
| 4 | kahneman d, 1966, science, v154, p1583, doi 10.1126/science.154.3756.1583 | Pupil diameter and load on memory | 260 | 4,642 |
| 5 | bradley mm, 2008, psychophysiology, v45, p602, doi 10.1111/j.1469-8986.2008.00654.x | The pupil as a measure of emotional arousal and autonomic activation | 220 | 3,081 |
| 6 | laeng b, 2012, perspect psychol sci, v7, p18, doi 10.1177/1745691611427305 | Pupillometry: A Window to the Preconscious? | 214 | 3,010 |
| 7 | murphy pr, 2014, hum brain mapp, v35, p4140, doi 10.1002/hbm.22466 | Pupil diameter covaries with BOLD activity in human locus coeruleus | 193 | 3,765 |
| 8 | hess eh, 1964, science, v143, p1190, doi 10.1126/science.143.3611.1190 | Pupil Size in Relation to Mental Activity during Simple Problem-Solving | 179 | 3,302 |
| 9 | gilzenrat ms, 2010, cogn affect behav ne, v10, p252, doi 10.3758/cabn.10.2.252 | Pupil diameter tracks changes in control state predicted by the adaptive gain theory of locus coeruleus function | 169 | 3,530 |
| 10 | Sebastiaan, Mathôt.(2018). Pupillometry: Psychology, Physiology, and Function. J Cogn, 1(1), 16. doi:10.5334/joc.18 | Pupillometry: Psychology, Physiology, and Function | 157 | 2,267 |
Table 7.
Co-occurrence analysis of keywords. Top 10 keywords in the 5 clusters.
| Cluster 1 | Cluster 2 | Cluster 3 | Cluster 4 | Cluster 5 |
|---|---|---|---|---|
| Pupillometry (1069) | Pupil (239) | Locus-coeruleus (304) | Cognition (60) | Heart rate variability (99) |
| Pupillary light reflex (237) | Retinal ganglion cells (135) | Attention (240) | Speech perception (49) | Pain (66) |
| Eye tracking (112) | Eye (113) | Brain (97) | Cognitive control (48) | Analgesia (51) |
| Infrared pupillometry (87) | Melanopsin (111) | Autonomic nervous system (96) | Autism spectrum disorder (46) | Heart rate (46) |
| Pupillography (83) | Glaucoma (83) | Working-memory (96) | Anxiety (45) | Cardiac arrest (41) |
| Quantitative pupillometry (70) | Afferent pupillary defect (73) | Traumatic brain injury (85) | Depression (41) | Anesthesia (36) |
| Pupillometer (68) | Cone (51) | Intracranial pressure (57) | Stress (31) | Morphine (27) |
| Automated pupillometry (61) | Rod (42) | Alzheimer’s disease (53) | Sustained attention (28) | Pain assessment (18) |
| Dynamic pupillometry (41) | Optic neuritis (35) | Multiple sclerosis (53) | Schizophrenia (24) | Postoperative pain (15) |
| Chromatic pupillometry (22) | Myopia (35) | Parkinson's disease (36) | Dementia (18) | Diazepam (9) |
The numbers in brackets represent the frequency of keywords according to the co-occurrence.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



