Submitted:
25 February 2026
Posted:
26 February 2026
You are already at the latest version
Abstract
Background/Objectives: Constipation is a common gastrointestinal problem in older adults and is associated with impaired quality of life, decline in activities of daily living, frailty, and increased risk of delirium and cognitive decline. Its pathogenesis involves age-related changes in gastrointestinal motility, neural regulation, comorbidities, and polypharmacy. This narrative review aims to summarize recent literature on the pathophysiology, contributing factors, and management of constipation in older adults, emphasizing its characterization as a systemic geriatric syndrome. Methods: A narrative literature search was conducted using PubMed for articles published between January 1, 2023, and December 31, 2025. MeSH terms included “Constipation” [Major Topic] and “Aged” [MeSH Terms]. English-language original studies, systematic reviews, and clinical or epidemiological studies involving adults aged ≥65 years were included. Results: Diagnosis in older adults is often complicated by secondary causes such as medications and neurological disorders, as well as atypical presentations in those with cognitive impairment. Constipation prevalence increases markedly with age. Pathophysiological mechanisms include reduced interstitial cells of Cajal, impaired smooth muscle contractility, enteric and autonomic nervous system dysfunction, and gut microbiota dysbiosis, which may promote low-grade inflammation. Major contributing factors include physical inactivity, sarcopenia, dehydration, inappropriate defecation posture, and polypharmacy, particularly opioids and anticholinergic agents. Management should be stepwise, prioritizing non-pharmacological interventions, followed by pharmacological and microbiota-targeted therapies when necessary. Conclusions: Constipation in older adults should be recognized as a systemic geriatric syndrome rather than a localized gastrointestinal disorder. Comprehensive, individualized management beyond simple laxative use is essential to reduce complications and preserve functional health in aging populations.
Keywords:
constipation
; older adults
; geriatric syndrome
; central and autonomic dysregulation
; brain–gut axis
; frailty
; healthcare burden
1. Introduction
Constipation is one of the most prevalent gastrointestinal symptoms among older adults, with an estimated prevalence of approximately 10–30% in community-dwelling elderly populations [1] and as high as 40–60% among residents of long-term care facilities [2]. Age-related decline in gastrointestinal motility, alterations in neural regulatory mechanisms, the presence of multiple comorbidities, and polypharmacy nteract to create a characteristic pathophysiological profile in older adults [3].
With the rapid progression of population aging, constipation has become a major contributor to healthcare utilization, including outpatient visits, laxative prescriptions, emergency department presentations, and hospital admissions [4]. In addition, constipation-related complications such as fecal impaction, bowel obstruction, and delirium are associated with increased medical costs and caregiving burden, making constipation an important issue from a socioeconomic perspective.
Constipation in older adults extends beyond a mere reduction in bowel movement frequency. Accumulating evidence indicates that it is closely associated with impaired quality of life (QOL), decline in activities of daily living (ADL), and progression of frailty [5]. Moreover, constipation has been identified as a risk factor for delirium and cognitive decline [6], underscoring its clinical relevance within the framework of comprehensive geriatric assessment.
The aim of this narrative review is to systematically summarize studies indexed in PubMed between 2023 and 2025 in which constipation and older adults were designated as major topics using Medical Subject Headings (MeSH). This review focuses on the pathophysiology, associated factors, clinical consequences, and management strategies of constipation in older adults. Particular emphasis is placed on its multifactorial nature and systemic functional impact, with the goal of providing insights to inform future research directions and clinical practice.
2. Methods
2.1. Study Design
This study was conducted as a narrative review with the aim of systematically organizing recent knowledge on constipation in older adults. The review focused on changes in diagnostic criteria, epidemiological characteristics, pathophysiological mechanisms, and clinical significance, providing an integrated overview of recent research trends. Systematic review methodology and meta-analysis were not performed; instead, a descriptive synthesis was adopted, prioritizing clinical relevance and interpretability of the available evidence.
2.2. Search Strategy
A literature search was performed using the PubMed database. The search period was defined from January 1, 2023, to December 31, 2025. The following Medical Subject Headings (MeSH) terms and keywords were used, and only studies in which the topic was designated as a major focus were included.
Search terms:
- “Constipation” [Major Topic]
- “Aged” [MeSH Terms]
Search strategy:
(Constipation[Majr] AND Aged[MeSH Terms]) AND (2023:2025[pdat])
When appropriate, additional articles related to diagnostic criteria (Rome criteria), epidemiology, pathophysiology, caregiving environments, and cognitive function were reviewed to supplement the primary search. Only articles published in English were considered.
2.3. Eligibility Criteria
Inclusion Criteria
Studies meeting all of the following criteria were included:
- Studies involving older adults (generally defined as ≥65 years of age)
- Constipation addressed as a primary research topic and designated as a MeSH Major Topic
- Original research articles, systematic reviews, epidemiological studies, or clinical studies
- Availability of an abstract
- Articles published from 2023 onward
Exclusion Criteria
Studies were excluded if they met any of the following criteria:
- Studies limited to pediatric or young adult populations
- Studies in which constipation was evaluated only as a secondary outcome
- Case reports, editorials, or studies available only as conference abstracts
- Animal studies or basic experimental research without clinical data
2.4. Data Extraction and Synthesis
From the selected studies, the following information was extracted:
- Author names, year of publication, and study design
- Study population (e.g., community-dwelling older adults, residents of long-term care facilities, home care patients)
- Definition and diagnostic criteria of constipation (e.g., Rome III, Rome IV, Rome IV-TR)
- Prevalence, associated factors, and clinical outcomes
- Diagnostic and management challenges specific to older adults
The extracted data were organized according to thematic categories. Quantitative synthesis was not performed; instead, findings were descriptively integrated and interpreted. Differences among studies were carefully evaluated with consideration of heterogeneity in study populations, assessment methods, and diagnostic criteria.
2.5. Figure Design and Source Attribution
All figures were created by the authors using Adobe Illustrator for the purpose of conceptual illustration. No copyrighted materials or previously published content were used.
3. Definition of Constipation and Diagnostic Challenges in Older Adults
According to the Rome IV criteria, the diagnosis of functional constipation requires the presence of symptoms during the preceding three months, with symptom onset at least six months before diagnosis. At least two of the following symptoms must be present in ≥25% of defecations: fewer than three spontaneous bowel movements per week, straining during defecation, hard or lumpy stools, sensation of difficult evacuation, or sensation of incomplete evacuation [7].
In older adults, however, secondary causes such as medication-induced constipation, neurological disorders, and metabolic abnormalities frequently coexist. As a result, strict differentiation between functional constipation and chronic constipation is often challenging in this population. Consequently, in routine clinical practice, constipation in older adults is commonly evaluated and managed comprehensively under the broader category of “chronic constipation” [3].
In addition, chronicity of constipation in older adults often leads to symptom adaptation, whereby patients may no longer perceive or report defecatory difficulty or discomfort as explicit complaints [8]. Assessment strategies based solely on bowel movement frequency may therefore underestimate the true burden of constipation. Among older adults with cognitive decline or mild cognitive impairment, self-reporting of constipation-related symptoms is particularly difficult, and symptoms may instead manifest atypically as abdominal discomfort, reduced appetite, or behavioral changes rather than as direct complaints of constipation [1]. 4. Epidemiology of Constipation in Older Adults
4. Epidemiology of Constipation in Older Adults
4.1. Prevalence and Age-Specific Patterns
Numerous studies have demonstrated that the prevalence of constipation increases with advancing age [9]. While the global prevalence of constipation in the general adult population is estimated to be approximately 14% [10], rates among community-dwelling adults aged 60 years and older have been reported to reach as high as 33.5% [11]. A particularly pronounced increase in prevalence has been observed between the ages of 75 and 79 years [12], suggesting a critical age window during which age-related physiological and functional changes may substantially influence bowel function.
4.2. Differences Between Community-Dwelling and Institutionalized Older Adults
Living environment plays a significant role in the risk of constipation among older adults. Compared with community-dwelling older individuals, residents of long-term care facilities consistently exhibit a higher prevalence of constipation [2]. In institutionalized settings, age-related physiological changes are compounded by reduced physical activity, polypharmacy, insufficient intake of dietary fiber and fluids, as well as cognitive impairment and psychological factors, all of which interact in a complex manner to exacerbate constipation [8].
4.3. Female Predominance and Age-Related Changes
One of the most prominent epidemiological features of constipation is its sex-related difference. Across most age groups, the prevalence of constipation in women is approximately twice that observed in men [13]. This disparity has been attributed to the effects of sex hormones, including progesterone and estrogen, which are known to slow gastrointestinal transit, as well as to anatomical and functional differences in the pelvic floor musculature [18]. While female predominance is evident in younger and middle-aged populations, the sex gap appears to narrow in older age groups. These observations suggest that sex hormones play an important role in both the development of constipation and its age-related epidemiological patterns [14].
4.4. Geographic and Socioeconomic Factors
Although geographic variation in constipation prevalence has been reported, findings are not entirely consistent, likely reflecting differences in cultural context, dietary habits, and study methodologies [15]. Socioeconomic factors such as lower socioeconomic status, lower educational attainment, and specific dietary patterns, particularly low-fiber diets, have been identified as common risk factors for constipation [13]. Prevalence rates also vary across regions, ranging from approximately 16% in the United States to 8–26% in European countries [16]. These variations may be influenced by regional differences in dietary composition, physical activity levels, and cultural perceptions of what constitutes constipation.
5. Pathophysiology
5.1. Peripheral Mechanisms (Smooth Muscle, ICC, Anorectal Function)
One of the core pathophysiological mechanisms underlying constipation in older adults is age-related structural degeneration of the gastrointestinal tract, accompanied by impaired neuromuscular control of motility. Aging is associated with a reduction in the density and contractile capacity of colonic smooth muscle cells. In addition, decreased elasticity of intestinal vasculature leads to reduced blood supply, resulting in attenuation of colonic peristalsis and absorptive function [17].
Beyond smooth muscle alterations, aging is also associated with a decline in the number of interstitial cells of Cajal (ICCs), which serve as pacemaker cells regulating gastrointestinal motility [18]. A reduction in ICCs disrupts the synchronization of peristaltic activity and weakens propulsive contractions, directly contributing to prolonged colonic transit time in older adults [18].
Anorectal functional changes further exacerbate constipation in the elderly. Compared with younger individuals, older adults exhibit significantly lower mean anal resting pressure (MARP/MERP) and maximum squeeze pressure (MSP) [14]. These changes are attributed to age-related atrophy of the external anal sphincter, loss of muscle fibers, and increased connective tissue and collagen deposition, all of which reduce sphincter tone and contractile strength [19]. Age-related neuronal loss also leads to diminished rectal sensitivity, resulting in an elevated sensory threshold for the urge to defecate and blunting of the defecation reflex [20].
In addition, age-related weakening and impaired coordination of the pelvic floor musculature become increasingly apparent with advancing age. These alterations contribute to rectoanal dyssynergia during defecation and represent a major pathophysiological component of defecatory disorders and outlet-type constipation in older adults [21].
5.2. Central and Autonomic Dysregulation (CNS–ENS–ANS)
Constipation in older adults reflects dysfunction of the integrated regulatory network linking the central nervous system (CNS), enteric nervous system (ENS), and autonomic nervous system (ANS), collectively referred to as the central–enteric–autonomic axis. Unlike peripheral motility impairment alone, age-related constipation arises from multilevel neural dysregulation affecting both motor and sensory components of defecation [22].
Within the intestinal wall, the Auerbach’s (myenteric) plexus, located between the longitudinal and circular smooth muscle layers, functions as the “second brain” by directly regulating peristalsis. However, aging is associated with structural and functional degeneration of the ENS [23].
Specifically, older adults exhibit a reduction in enteric neurons and decreased expression of connexin 43, a key gap-junction protein essential for intercellular signal transmission [24]. These degenerative changes disrupt the coordination of intestinal contraction and relaxation, leading directly to prolonged colonic transit time (CTT) [23].
The autonomic nervous system serves as the primary conduit transmitting central signals to the gut and plays a critical role in maintaining gastrointestinal homeostasis. Sympathetic overactivity, often driven by anxiety or psychological stress, suppresses gastrointestinal motility and exacerbates constipation [25]. In contrast, the vagus nerve, the principal parasympathetic pathway, promotes gut motility, sensory processing, and anti-inflammatory responses. In older adults and patients with chronic constipation, autonomic dysregulation—characterized by reduced heart rate variability and diminished vagal tone—is frequently observed [26].
Dysfunction of the neural axis affects not only motor function but also sensory processing. Rectal hyposensitivity—defined as reduced perception of rectal distension—is observed in approximately 25–56% of older patients with chronic constipation [27]. When rectal sensory signals fail to reach the brain accurately, the urge to defecate diminishes. This sensory–motor mismatch promotes fecal retention and progressive rectal dilation, further worsening rectal sensitivity and establishing a self-perpetuating neuro-mechanical vicious cycle [27].
Thus, constipation in older adults is fundamentally rooted in multilayered dysfunction of the neural axis, spanning from peripheral enteric degeneration to impaired central defecation control. This neural disintegration provides a critical pathophysiological framework for understanding age-related constipation and underscores the need for integrative therapeutic strategies targeting the brain–gut–autonomic network.
5.3. Gut Microbiota and Inflammaging
In recent years, increasing attention has been directed toward the role of gut microbiota alterations in the pathophysiology of constipation in older adults. Studies using 16S rRNA sequencing have demonstrated that older adults with functional constipation exhibit significant differences in gut microbiota composition compared with healthy controls, characterized by reduced microbial diversity [28]. Specifically, decreases in Firmicutes and Proteobacteria and relative increases in genera such as Bacteroides, Prevotella, and Ruminococcus have been reported [28]. This microbial profile is considered characteristic of constipation-associated dysbiosis.
Aging itself is associated with a decline in microbial diversity and a reduction in beneficial short-chain fatty acid (SCFA)-producing bacteria, such as Faecalibacterium prausnitzii, which play a crucial role in maintaining intestinal and metabolic health [29]. Age-related alterations in gut microbiota influence host immune function and mucosal immune responses. Dysbiosis may promote intestinal barrier dysfunction, chronic low-grade inflammation, and breakdown of immune tolerance, thereby contributing to systemic inflammation associated with aging (“inflammaging”). These processes have been implicated in the development of geriatric syndromes, including constipation [30].
6. Risk Factors
6.1. Physical and Nutritional Factors
Restricted physical activity and a sedentary lifestyle represent major multifactorial contributors to constipation in older adults [8]. Prolonged bed rest, particularly immobilization lasting longer than 48 hours, has been identified as an independent risk factor for the development of constipation, with an odds ratio of 5.244 [31]. Reduced physical activity diminishes the contractile force of intestinal smooth muscle, resulting in delayed colonic transit [31]. In addition, loss of skeletal muscle mass (sarcopenia) contributes to reduced intra-abdominal pressure during defecation, further impairing effective bowel evacuation [32].
Older adults are also predisposed to dehydration due to a diminished perception of thirst, the frequent use of diuretics for conditions such as heart failure, and intentional fluid restriction. Insufficient intraluminal water content leads to hard stools and increased difficulty with defecation [33]. Inadequate intake of dietary fiber and fluids is common in this population and represents a modifiable risk factor for constipation [34]. Furthermore, chronic malnutrition, exemplified by hypoalbuminemia, induces atrophy of the intestinal mucosa and neuromuscular degeneration, resulting in impaired gastrointestinal motility [20].
6.2. Medication-Related Factors
6.2.1. Opioid Analgesics
Older adults frequently suffer from multiple chronic conditions, leading to widespread polypharmacy, which is a major modifiable contributor to constipation in this population [35]. Drug-induced constipation occurs through suppression of gastrointestinal motility or alteration of stool consistency and represents one of the most important reversible causes of constipation in older adults [35].
Opioids are indispensable for pain management but are associated with a very high incidence of opioid-induced constipation (OIC) [36]. Opioids bind not only to central nervous system receptors but also to μ-opioid receptors in the enteric nervous system, resulting in inhibition of peristalsis and increased intestinal water absorption. These effects lead to harder stools and impaired stool passage [37].
The risk of constipation varies according to opioid type and dosage. Compared with codeine, the use of morphine (hazard ratio [HR] 1.59), oxycodone (HR 1.46), and fentanyl (HR 1.37) has been associated with a significantly increased risk of severe constipation [37]. In contrast, tramadol, which exerts serotonin and norepinephrine reuptake inhibition in addition to opioid receptor activity, has been associated with a lower risk of constipation (HR 0.80) compared with other opioids [37]. Daily opioid doses exceeding 50 morphine milligram equivalents (MME) further amplify constipation risk [37].
6.2.2. Anticholinergic Medications
Anticholinergic agents suppress parasympathetic activity and reduce gastrointestinal motility, thereby promoting constipation. Antimuscarinic drugs used to treat urinary frequency or incontinence inhibit bladder contraction but also suppress intestinal motility, exacerbating constipation [38]. Many psychotropic medications, including antipsychotics and antidepressants, possess secondary anticholinergic properties and increase the risk of chronic constipation with long-term use [36]. In patients with Parkinson’s disease, antiparkinsonian medications may further complicate constipation by interacting with underlying enteric neurodegeneration and altering gut microbiota composition and gastrointestinal motility [39].
6.2.3. Other Medications and Effects on the Gastrointestinal Environment
Long-term use of proton pump inhibitors (PPIs) may indirectly contribute to constipation through alterations in the gut environment. PPI use is associated with a significant increase in intestinal permeability markers, such as α1-antitrypsin (AAT), with reported elevations of up to 151%, suggesting impaired intestinal barrier function [40]. Increased gastric pH facilitates fungal overgrowth within the gastrointestinal tract, promoting dysbiosis [40]. This dysbiotic state may induce chronic low-grade inflammation (“inflammaging”) and disrupt gastrointestinal motility [40]. Calcium channel blockers, commonly prescribed for hypertension, also suppress smooth muscle contraction and are recognized risk factors for constipation [16].
Even stimulant laxatives used for constipation treatment can contribute to disease perpetuation when used long term. Chronic use may lead to tolerance and dependence, impairing intrinsic defecatory function and creating a vicious cycle [41]. Continuous laxative use reduces the colon’s autonomous motility, resulting in dependence on pharmacological stimulation for bowel movements [42]. Tolerance necessitates escalating doses to achieve the same effect, further complicating constipation management [8]. Long-term use of anthraquinone-containing laxatives (e.g., senna, aloe, rhubarb) may induce colonic melanosis, which affects the enteric nervous plexus and significantly reduces colonic contractility [34]. Laxative use may also alter gut microbiota composition, reducing microbial diversity and depleting beneficial bacteria essential for stool hydration and motility regulation, thereby exacerbating chronic constipation [8].
6.3. Environmental and Social Factors
Environmental and social factors substantially modulate constipation risk in older adults, particularly through restricted toileting access, loss of independence, and inadequate defecation posture. These factors interact with physical decline to exacerbate functional constipation [43]. In patients with chronic obstructive pulmonary disease (COPD), reduced physical activity compared with age-matched healthy individuals is associated with constipation prevalence rates of approximately 40% [44].
Physiologically optimal defecation postures include a seated or squatting position [27]. Squatting relaxes the puborectalis and pelvic floor muscles and straightens the anorectal angle, facilitating stool passage [27]. In contrast, non-physiological postures, such as lateral decubitus positioning during bedpan use, make regulation of anal pressure difficult and increase the risk of defecatory dysfunction [27].
Increasing care dependency and loss of independence are closely associated with constipation in older adults [45]. Studies have shown that older individuals requiring partial or full assistance with eating or toileting have a higher prevalence of functional constipation compared with independent counterparts [45]. Limited access to toilets or situations requiring voluntary suppression of defecation weaken the defecation reflex and promote chronic constipation [46]. Increased dependency often restricts physical activity and free toilet access. Increasing dependency often restricts mobility and timely toilet access. These functional limitations interact with underlying physical decline to exacerbate constipation [46]. Notably, a prospective study of community-dwelling adults aged 75 years and older demonstrated that sarcopenia is an independent risk factor for incident constipation, underscoring the critical importance of maintaining muscle strength and physical function for constipation prevention in later life [24]. To conceptualize constipation in older adults as a systemic geriatric syndrome, we propose an integrated framework summarizing its multifactorial determinants (Figure 1).
7. Clinical Impact
7.1. Cognitive, Psychological, and Systemic Outcomes
Recent studies have demonstrated that constipation is closely associated not only with physical health but also with brain function and mental status in older adults. Large-scale epidemiological investigations have shown a strong association between constipation and cognitive impairment. In the context of dementia and mild cognitive impairment (MCI), particularly non-amnestic MCI, the “body-first” hypothesis has been proposed, suggesting that constipation may represent one of the earliest prodromal symptoms of neurodegenerative disorders [1]. Chronic constipation, characterized by reduced bowel movement frequency, has also been independently associated with an increased risk of incident MCI in older adults [1].
These associations are thought to be mediated, at least in part, by disruption of the brain–gut–microbiota axis, linking chronic constipation to neuroinflammation and cognitive vulnerability in later life [47]. Constipation-associated dysbiosis disrupts intestinal barrier function, leading to increased intestinal permeability (“leaky gut”). As a result, bacterial metabolites and endotoxins may enter the systemic circulation and exert deleterious effects on the central nervous system via increased permeability of the blood–brain barrier [48]. This dysbiotic state promotes systemic low-grade inflammation (“inflammaging”), which may contribute to neuroinflammatory vulnerability in older adults [49].
Furthermore, patients with constipation exhibit reduced production of beneficial microbial metabolites, including short-chain fatty acids (SCFAs). SCFAs play essential roles in maintaining intestinal and blood–brain barrier integrity, suppressing inflammation, and exerting neuroprotective effects. Decreased SCFA production may therefore enhance neuroinflammation and oxidative stress, accelerating cognitive deterioration in older adults [50].
A strong bidirectional relationship has also been reported between chronic constipation and depressive symptoms [51]. Among patients with obstructed defecation disorder, depressive symptoms have been observed in approximately 82.5% and anxiety symptoms in 55.6%, with greater severity of defecatory symptoms correlating with increased psychological distress [52]. In hospitalized or postoperative older adults, constipation has gained clinical attention as a secondary precipitating factor for delirium, alongside urinary retention and pain [31].
Severe complications such as fecal impaction, bowel obstruction (ileus), rectal ulcers, and even life-threatening stercoral perforation may occur if constipation remains untreated [42]. Collectively, constipation, gut dysbiosis, barrier dysfunction, systemic and neuroinflammation, and neuropsychiatric impairment interact to form a vicious cycle driven by disruption of the brain–gut axis. Therefore, management of constipation in older adults should extend beyond bowel regulation and be positioned as a comprehensive intervention aimed at preventing delirium, preserving cognitive function, and improving mental health.
In addition, among patients with acute heart failure or following myocardial infarction, the coexistence of constipation has been strongly associated with increased risks of rehospitalization and mortality [53]. Excessive straining during defecation can induce acute elevations in blood pressure, potentially triggering adverse cardiovascular events in vulnerable individuals [53].
7.2. Prognosis and Healthcare Burden
If inadequately managed, chronic constipation in older adults may lead to serious complications and substantially increase the burden on healthcare systems. Untreated constipation can result in fecal impaction, stercoral ulcers, diverticulitis, and even intestinal perforation, all of which represent major causes of hospitalization in older populations [51]. Among hospitalized older patients, constipation has been associated with increased risks of delirium, intensive care unit (ICU) admission, and cardiopulmonary arrest [54]. Furthermore, patients with constipation have been reported to have significantly higher rates of readmission within 90 days after discharge, highlighting the importance of constipation management in long-term prognostic care [54].
The socioeconomic burden associated with constipation is considerable and contributes to escalating healthcare costs [44]. In the United States, the annual healthcare expenditure per patient with chronic constipation has been estimated at approximately USD 11,991, including outpatient visits, hospitalizations, and additional costs resulting from treatment failure [43]. Another report indicated that constipation-related medical consultations account for approximately 2.5 million visits annually, with an average cost of USD 2,752 per patient [55].
Constipation also impairs activities of daily living (ADL) and social functioning, thereby increasing dependence on caregiving. Fecal incontinence associated with constipation is one of the primary reasons older adults abandon independent living and transition to long-term care facilities or nursing homes [56]. In cases of severe constipation or fecal impaction, conventional treatments such as laxatives or enemas may be ineffective, necessitating manual disimpaction, an intervention that imposes significant physical and psychological burden on both patients and caregivers [57].
8. Management Strategies
8.1. Non-Pharmacological Interventions
8.1.1. Lifestyle and Dietary Modification
Management of constipation in older adults requires a multidimensional approach that extends beyond symptom relief and takes into account physical function, cognitive status, nutritional condition, and quality of life (QOL) [42]. Because non-pharmacological interventions carry a low risk of adverse effects and promote patient autonomy, they are considered the first-line strategy for constipation management in older adults [42].
Dietary fiber increases stool bulk and improves bowel movement frequency [55]. An intake of 25–35 g of dietary fiber per day is generally recommended [58]. Among fiber-rich foods, prunes (dried plums) are particularly effective, as they contain both dietary fiber and sorbitol. In older women, prune consumption has been shown to improve bowel movement frequency and significantly enhance QOL and subjective satisfaction [8]. According to the recently proposed Dietary Index for Gut Microbiota (DI-GM), increased consumption of whole grains, fermented dairy products, vegetables (e.g., broccoli), coffee, and green tea, along with reduced intake of red meat and high-fat foods, is associated with greater gut microbiota diversity and a significantly lower risk of constipation [59]. In addition, deficiencies in micronutrients such as vitamin B1 and copper have been associated with constipation, highlighting the importance of a nutritionally balanced diet [43].
Decline in chewing ability, assessed by the number of functional tooth units (FTUs), contributes to insufficient fiber intake and reduced digestive efficiency, thereby increasing constipation risk [60]. Chewing dysfunction accompanied by depressive symptoms further amplifies this risk, underscoring the importance of dental rehabilitation as part of comprehensive constipation management [60]. Collectively, these non-pharmacological strategies address modifiable contributors to constipation and should be prioritized before pharmacological escalation.
8.1.2. Physical Activity and Mechanical Stimulation
Physical activity, particularly walking, promotes gastrointestinal motility. In older adults, walking more than 5,500 steps per day has been linked to improved stool quality [61]. Non-invasive interventions combining abdominal vibration with walking exercise (AVCWE) have also been shown to safely and effectively stimulate intestinal motility and facilitate defecation [61]. Abdominal massage and thermal therapy have been reported to significantly improve bowel movement frequency and stool consistency in older adults [62,63]. New non-drug devices, including vibration capsules, are gaining attention as ways to reduce reliance on medications [64].
8.1.3. Toileting Environment, Posture, and Daily Rhythm
Environmental factors play a critical role in successful defecation, especially in older adults with cognitive impairment [2]. Establishing a regular morning defecation routine leverages the gastrocolic reflex and has been identified as an independent protective factor against functional constipation [45]. Using a footstool to elevate the knees above hip level—adopting a semi-squatting forward-leaning posture (“Rodin posture”)—widens the anorectal angle and enables smoother stool evacuation while reducing excessive straining [65]. Sleep deprivation and irregular sleep patterns negatively affect gut microbiota and autonomic nervous system function, thereby exacerbating constipation [66]. Individualized toileting assistance aligned with the patient’s daily rhythm, together with a relaxed and private environment, helps reduce psychological barriers to defecation [16].
8.2. Pharmacological Therapy
8.2.1. Conventional Laxatives: Benefits and Limitations
Although several new pharmacological agents for chronic constipation have been introduced in recent years, more than 60% of patients continue to experience persistent symptoms despite laxative use [44]. Osmotic laxatives include magnesium oxide, sorbitol, and polyethylene glycol (PEG) [67], which soften stools by retaining water within the intestinal lumen [68]. Magnesium oxide is inexpensive and widely used; however, in older adults and patients with renal dysfunction, it carries a risk of hypermagnesemia, which may adversely affect cardiac function [33].
Stimulant laxatives, such as bisacodyl, senna, and rhubarb, directly stimulate intestinal peristalsis [36,67]. Although effective in the short term, long-term use may induce dependence, tolerance, and colonic melanosis, potentially worsening constipation. Therefore, stimulant laxatives should be reserved for intermittent or short-term use [42].
8.2.2. Novel Secretagogues and Prokinetic Agents
Elobixibat inhibits bile acid reabsorption in the ileum, increasing bile acid delivery to the colon and thereby promoting water secretion and colonic motility [69]. In Japanese health economic models, elobixibat has demonstrated favorable cost-effectiveness compared with other novel constipation treatments [69]. Lubiprostone activates ClC-2 chloride channels in the small intestine, enhancing intestinal fluid secretion [70]. However, adverse effects such as nausea and, rarely, serious gastrointestinal events including ischemic colitis have been reported, necessitating careful monitoring [70]. Guanylate cyclase-C (GC-C) agonists, such as linaclotide, improve bowel movements by enhancing intestinal secretion and reducing visceral hypersensitivity [69].
8.2.3. Management of Secondary Constipation in Older Adults
Opioid use is common in older adults for chronic pain management, making opioid-induced constipation (OIC) a major clinical concern. Peripherally acting μ-opioid receptor antagonists (PAMORAs), such as naldemedine and methylnaltrexone, effectively improve bowel function without compromising analgesic efficacy [36].
Prucalopride, a selective 5-hydroxytryptamine (5-HT4) receptor agonist, correlates with higher treatment persistence and adherence in real-world settings compared with other therapies for chronic idiopathic constipation (CIC) [71]. This advantage is likely attributable to its once-daily dosing and high receptor selectivity, which reduce adverse effects [71].
8.3. Microbiota-targeted therapy
8.3.1. Mechanistic Rationale for Microbiota-Based Therapy
In the management of constipation in older adults, probiotics (live beneficial microorganisms) and synbiotics (combinations of probiotics and prebiotics) have attracted attention as effective interventions with a low risk of adverse effects [72]. Their benefits are mediated through multiple biological mechanisms. First, enhancement of short-chain fatty acid (SCFA) production plays a central role [72]. Beneficial bacteria ferment dietary fiber and oligosaccharides to produce SCFAs such as propionate and butyrate, which stimulate the enteric nervous system, enhance colonic motility, and serve as energy sources for intestinal epithelial cells [73].
Second, probiotics and synbiotics contribute to reconstruction of the gut microbiota and correction of dysbiosis [74]. Constipated patients often exhibit increased methanogenic bacteria that suppress intestinal motility, along with reduced beneficial bacterial populations [74]. Supplementation increases beneficial genera such as Bifidobacterium, thereby restoring microbial balance and normalizing intestinal transit [74].
Third, these microbial therapies exert anti-inflammatory effects by strengthening intestinal barrier function and reducing intestinal permeability, which mitigates chronic low-grade inflammation (“inflammaging”) [39]. Suppression of inflammatory cytokines protects enteric neural function and slows the progression of motility impairment [39].
8.3.2. Clinical Evidence in Older Adults
Specific probiotic strains have demonstrated efficacy in older populations. In adults aged 50–85 years, an 84-day intervention with Lactiplantibacillus plantarum strains KABP031/032 significantly improved bowel movement frequency and stool consistency [72], while also reducing perceived stress [72]. In institutionalized older adults, consumption of beverages containing Bifidobacterium longum and Bifidobacterium lactis Bb12 significantly increased the proportion of normal bowel movements [2]. Supplementation with Weizmannia coagulans (formerly Bacillus coagulans) BC01 for 21 days improved stool consistency (Bristol Stool Scale) and QOL scores while increasing SCFA production, particularly acetate [74]. Lactobacillus rhamnosus JYLR-127 has been shown to improve bowel frequency and alleviate abdominal symptoms in older patients following fracture surgery [73].
Synbiotics aim to achieve synergistic effects by combining probiotics with prebiotics such as oligosaccharides [46]. In adults aged 60 years and older, a 4-week intervention with Bifidobacterium animalis subsp. lactis BL-99 combined with fructooligosaccharides (FOS) significantly increased weekly spontaneous bowel movements (SBMs) and shortened whole-gut transit time (WGTT) [75]. Notably, these benefits persisted for two weeks after discontinuation, suggesting sustained improvement in the gut environment [75].
8.3.3. Toward Personalized Microbiota Modulation
Probiotics may also benefit constipation associated with neurological disorders through modulation of the brain–gut axis. In patients with Parkinson’s disease, a 12-week intervention with a probiotic formulation containing L. rhamnosus, L. acidophilus, L. plantarum, and Enterococcus faecium not only alleviated constipation but also reduced systemic inflammatory markers (TNF-α) and shortened the time to onset of levodopa efficacy [39]. In older adults with cognitive impairment, probiotics and synbiotics represent valuable care strategies for constipation prevention and QOL improvement [2]. However, variability in individual responses, strain-specific effects, and placebo influences necessitate personalized approaches tailored to functional status and lifestyle rather than uniform treatment strategies [76]. Table 1 provides a comparative overview of major therapeutic modalities for constipation in older adults, focusing on their mechanisms of action, elderly-specific benefits, risks, and clinical considerations.
Rather than proposing a rigid treatment algorithm, we present a conceptual framework that organizes current evidence into a stepwise clinical approach for constipation management in older adults (Figure 2).
9. Conclusions
Constipation in older adults is not merely a gastrointestinal complaint but a systemic geriatric syndrome. Rather, it represents a systemic syndrome arising from the complex interplay of multiple factors, including age-related changes in neuromuscular function, alterations in the gut microbiota, lifestyle and environmental factors, and medication use. The recent literature highlights that constipation in older adults is closely linked to frailty, cognitive decline, depressive symptoms, and increased healthcare burden, positioning it as a core component of geriatric syndromes.
In particular, neuroinflammation and systemic low-grade inflammation (inflammaging) mediated through disruption of the brain–gut–microbiota axis represent key concepts in positioning constipation as a component of geriatric syndromes. Emerging evidence suggests that constipation may serve as a prodromal symptom of dementia and neurodegenerative disorders, underscoring its substantial clinical importance as a target for early assessment and intervention.
From a therapeutic perspective, management should not rely solely on symptomatic treatment with laxatives. Instead, a comprehensive and individualized approach is essential, with non-pharmacological interventions—such as physical activity, nutritional optimization, bowel habit training, environmental modification, and medication review—forming the foundation of care. In addition, newer pharmacological agents, including bile acid transporter inhibitors, guanylate cyclase-C (GC-C) agonists, 5-HT4 receptor agonists, and peripherally acting μ-opioid receptor antagonists (PAMORAs), may represent effective treatment options for older adults when appropriately selected and carefully monitored. Furthermore, probiotics and synbiotics hold promise as disease-modifying interventions through modulation of the gut environment, and further accumulation of high-quality evidence is anticipated.
Future challenges include the establishment of diagnostic criteria and outcome measures that reflect the unique pathophysiology of constipation in older adults, prospective studies evaluating long-term outcomes including cognitive function and frailty, and validation of multidisciplinary intervention models. Appropriate understanding and management of constipation in older adults extend beyond symptom control and are directly linked to the maintenance of independence, preservation of cognitive function, and reduction of healthcare and caregiving burdens. Continued cross-disciplinary research and clinical practice in both geriatric medicine and gastroenterology are therefore strongly warranted.
Author Contributions
Conceptualization, S.M and A.M.; methodology, S.M.; validation, S.M.; investigation, all authors; data curation, all authors; writing—original draft preparation, all authors; writing—review and editing, S.M.; supervision, H.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
During the preparation of this manuscript, the authors used ChatGPT (OpenAI,GPT-5.2) on 20 February 2026 to improve grammar, formality, and linguistic clarity. No AI system was used to generate scientific ideas, analyze data, or interpret results. All AI-assisted text was reviewed, edited, and validated by the authors. Figures were created with Adobe Illustrator for conceptual illustration. The authors take full responsibility for the content and scientific integrity of the final manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wang, F.; Fei, M.; Hu, W.Z.; Wang, X.D.; Liu, S.; Zeng, Y.; Zhang, J.H.; Lv, Y.; Niu, J.P.; Meng, X.L.; et al. Prevalence of Constipation in Elderly and Its Association With Dementia and Mild Cognitive Impairment: A Cross-Sectional Study. Front. Neurosci. 2022, 15, 821654. [Google Scholar] [CrossRef] [PubMed]
- Schnitker, L.M.; Alrababah, S.; Young, A.; Selby, Z.; Meyer, C.; Lowthian, J.A. Best Practice to Prevent Constipation in People Living With Dementia: A Scoping Review. Int. J. Older People Nurs. 2025, 20. [Google Scholar] [CrossRef]
- Yun, Q.; Wang, S.; Li, B.; Yang, Z.; Wei, C.; Yuan, J.; Hu, J.; Li, Y.; Yang, Z.; Sha, F.; et al. Constipation Preceding Stroke, Dementia and Parkinson’s Disease in Middle-Aged and Older Adults: A Population-Based Cohort Study. Age Ageing 2025, 54. [Google Scholar] [CrossRef]
- Sommers, T.; Corban, C.; Sengupta, N.; Jones, M.; Cheng, V.; Bollom, A.; Nurko, S.; Kelley, J.; Lembo, A. Emergency Department Burden of Constipation in the United States from 2006 to 2011. American Journal of Gastroenterology 2015, 110, 572–579. [Google Scholar] [CrossRef]
- An, J.; Jiao, C.; Guo, J.; Zhang, L.; Li, Z.; Liu, G.; Zhang, Y.; Liu, W. The Association of ZJU Index with Bowel Health in US Participants: A Cross-Sectional Study. Eur. J. Med. Res. 2025, 30, 1165. [Google Scholar] [CrossRef]
- Purayil, S.; Yi, J.; Fletcher, D.; Denke, L.; Atem, F.D.; Zhang, Y.; Wingfield, S. Exploring the Correlation between Constipation and Delirium among Hospitalized Patients Aged 65 Years and Older. Geriatr. Nurs. (Minneap) 2025, 67, 103724. [Google Scholar] [CrossRef]
- Aziz, I.; Whitehead, W.E.; Palsson, O.S.; Törnblom, H.; Simrén, M. An Approach to the Diagnosis and Management of Rome IV Functional Disorders of Chronic Constipation. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Assadollahzadeh, A.; Ravari, A.; Assadollahi, Z.; Mirzaei, T. Comparative Effects of Traditional Thai Abdominal Massage versus Prune Consumption on Constipation and Quality of Life in Elderly Women: A Randomized Controlled Trial. Aging Clin. Exp. Res. 2025, 37. [Google Scholar] [CrossRef] [PubMed]
- Suares, N.C.; Ford, A.C. Prevalence of, and Risk Factors for, Chronic Idiopathic Constipation in the Community: Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2011, 106, 1582–1591. [Google Scholar] [CrossRef] [PubMed]
- Bytzer, P.; Howell, S.; Leemon, M.; Young, L.J.; Jones, M.P.; Talley, N.J. Low Socioeconomic Class Is a Risk Factor for Upper and Lower Gastrointestinal Symptoms: A Population Based Study in 15 000 Australian Adults. Gut 2001, 49, 66. [Google Scholar] [CrossRef]
- Bharucha, A.E.; Pemberton, J.H.; Locke, G.R. American Gastroenterological Association Technical Review on Constipation. Gastroenterology 2013, 144, 218–238. [Google Scholar] [CrossRef]
- Liu, R.; Chao, A.; Wang, K.; Wu, J. Incidence and Risk Factors of Medical Complications and Direct Medical Costs after Osteoporotic Fracture among Patients in China. Arch. Osteoporos. 2018, 13. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, H.; Guo, Z.; Li, S.; Fu, Q. Inverse Association of Alcohol Consumption Patterns with Constipation and Diarrhea: A Population-Based Cross-Sectional Study. BMC Gastroenterol. 2025, 25, 865. [Google Scholar] [CrossRef]
- Zhu, H.T.; Wang, H.F.; Zhang, Q.; Bai, J.F.; Wang, M.; Du, S.Y.; Zhang, Y.L. Comprehensive Microbial and Clinical Profiling of Functional Constipation: A Stratified Comparative Study of Age and Constipation Subtype. World J. Gastroenterol. 2025, 31. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Yang, X.J.; Zhu, H.M.; Tang, Z.; Li, B.Y.; Zhao, D.D. Epidemiological Study of Elderly Constipation in Beijing. World J. Gastroenterol. 2015, 21, 13368. [Google Scholar] [CrossRef] [PubMed]
- Segura-Bayona, C.; Vidal-Alaball, J.; Ramírez-Morros, A.; Miró-Catalina, Q.; Ruiz-Comellas, A. A Primary Care Program Based on Behavioral Reeducation and Abdominal Massage for Improving the Symptoms of Chronic Constipation: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2025, 14. [Google Scholar] [CrossRef]
- Kilgore, A.; Khlevner, J. Functional Constipation: Pathophysiology, Evaluation, and Management. Aliment. Pharmacol. Ther. 2024, 60 Suppl 1, S20–S29. [Google Scholar] [CrossRef]
- Tian, Y.; Li, Y.; Yi, T.; Wang, Q.; Jiang, X.; He, Z.X. Comparison of Tc-99 m Scintigraphic Method and Radiological Method for Colon Transmit Assessment in Patients with Functional Constipation. BMC Gastroenterol 2025, 25. [Google Scholar] [CrossRef]
- Rajasekaran, M.R.; Kanoo, S.; Fu, J.; Nguyen, M.U.L.; Bhargava, V.; Mittal, R.K. Age-Related External Anal Sphincter Muscle Dysfunction and Fibrosis: Possible Role of Wnt/β-Catenin Signaling Pathways. Am. J. Physiol. Gastrointest. Liver Physiol. 2017, 313, G581–G588. [Google Scholar] [CrossRef]
- Yang, X.; Li, W.; Xiao, Q.; Du, S.; Wang, X.; Zhang, Y.; Li, S. Predicting the Risk of Postoperative Constipation in Middle-Aged and Elderly Patients with Lower Limb Fractures Using Machine Learning Algorithms. PLoS One 2025, 20, e0336466. [Google Scholar] [CrossRef]
- Sadeghi, A.; Akbarpour, E.; Majidirad, F.; Bor, S.; Forootan, M.; Hadian, M.R.; Adibi, P. Dyssynergic Defecation: A Comprehensive Review on Diagnosis and Management. The Turkish Journal of Gastroenterology 2023, 34, 182. [Google Scholar] [CrossRef]
- Zhao, X.; Wang, X.; Quan, L. Association between Dietary Inflammatory Index and Energy-Adjusted Dietary Inflammatory Index and Constipation in US Adults. BMC Gastroenterol. 2024, 24. [Google Scholar] [CrossRef] [PubMed]
- Tazaki, T.; Yamada, H.; Sato, R.; Ishii, H.; Sugita, S.; Yanagihara, H.; Nakamura, D.; Takashio, O.; Inamoto, A.; Iwanami, A. Constipation-Associated Factors in Outpatients with Schizophrenia: A Multicenter Questionnaire Survey. Neuropsychopharmacol. Rep. 2024, 44, 604–613. [Google Scholar] [CrossRef]
- Nakagawa, H.; Takeshima, T.; Ozaka, A.; Sasaki, S.; Hamaguchi, S.; Fukuhara, S. The Association between Sarcopenia and Constipation Onset in Community-Dwelling Older Adults in Japan. Intern. Med. 2025, 64, 1965–1970. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.Y.; Lo, S.C.; Beckstead, J.W.; Yang, C.Y. Associations between Constipation Risk and Lifestyle, Medication Use, and Affective Symptoms in Patients with Schizophrenia: A Multicenter Cross-Sectional Study. Soc. Psychiatry Psychiatr. Epidemiol. 2025, 60, 427–440. [Google Scholar] [CrossRef]
- Zheng, T.; Tavares, L.C.; D’Amato, M.; Marques, F.Z. Constipation Is Associated with an Increased Risk of Major Adverse Cardiac Events in a UK Population. Am. J. Physiol. Heart Circ. Physiol. 2024, 327, H956–H964. [Google Scholar] [CrossRef]
- Xiao, C.F.; Li, Y.F.; Sun, Y.Y.; Meng, L.Y.; Wu, J.W.; Wang, M.; Cao, Y.Q.; Wang, C.; Yao, Y.B. Influence of the Examination Position and Distension Medium on the Rectal Sensory Test in Patients with Functional Constipation. BMC Gastroenterol. 2024, 24. [Google Scholar] [CrossRef]
- Guo, M.; Yao, J.; Yang, F.; Liu, W.; Bai, H.; Ma, J.; Ma, X.; Zhang, J.; Fang, Y.; Miao, Y.; et al. The Composition of Intestinal Microbiota and Its Association with Functional Constipation of the Elderly Patients. In Future Microbiol.; REQUESTEDJOURNAL:JOURNAL:IFMB20; WGROUP:STRING:PUBLICATION, 2020; Volume 15, pp. 163–175. [Google Scholar] [CrossRef]
- Strasser, B.; Ticinesi, A. Intestinal Microbiome in Normal Ageing, Frailty and Cognition Decline. Curr. Opin. Clin. Nutr. Metab. Care 2023, 26, 8–16. [Google Scholar] [CrossRef]
- Zhang, Z.J.; Gao, R.; Lu, Y.T.; Zuo, Z.L.; Li, Y.H.; Liu, S.; Song, S.Y.; Wang, Y.; Lai, H. Factors Affecting Dysbiosis of the Gut Microbiota in the Elderly and the Progress of Interventions in Traditional Chinese and Western Medicine. Front. Cell. Infect. Microbiol. 2025, 15, 1529347. [Google Scholar] [CrossRef]
- Zou, L.; da Zheng, X.; Wang, C.G.; Ma, T. Factors Associated with Constipation after Total Hip Arthroplasty and Nursing Countermeasures. Medicine 2025, 104, e45226. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Lim, J.; Baek, J.Y.; Lee, E.; Jung, H.W.; Jang, I.Y. Status of Constipation and Its Association with Sarcopenia in Older Adults: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2021, 18. [Google Scholar] [CrossRef]
- Ishida, T.; Kawada, K.; Jobu, K.; Hamada, T.; Kubo, T.; Fukuda, H.; Hyohdoh, Y.; Kawai, K.; Nakaoka, Y.; Yabe, T.; et al. Impact of Non-cardiovascular Factors on Cardiovascular Death in Acute Decompensated Heart Failure: Enhancing Predictive Models with Frailty and Comorbid Constipation—the Constipation and Frailty Augmented AHEAD Score. Geriatr. Gerontol. Int. 2025, 25, 1341. [Google Scholar] [CrossRef]
- Qi, R.; Zhai, H.; Xu, D.; Wen, Y.; Xu, S. Association between the Planetary Health Diet Index and Chronic Constipation and Diarrhea Risk in General Population: A Cross-Sectional Analysis of NHANES. Medicine 2025, 104, e45468. [Google Scholar] [CrossRef] [PubMed]
- Hamano, J.; Higashibata, T.; Kessoku, T.; Kajiura, S.; Hirakawa, M.; Oyamada, S.; Ariyoshi, K.; Yamada, T.; Yamamoto, Y.; Takashima, Y.; et al. Naldemedine for Opioid-Induced Constipation in Patients With Cancer: A Multicenter, Double-Blind, Randomized, Placebo-Controlled Trial. J. Clin. Oncol. 2024, 42. [Google Scholar] [CrossRef]
- Liu, K.; Chen, A.; Rajaram, P.; Buning, G.; Lee, A.A.; Singh, P. PAMORAs in Opioid-Induced Constipation: Are We Following the Guidelines? Clin. Transl. Gastroenterol. 2025, 16, e00876. [Google Scholar] [CrossRef]
- Yimer, B.B.; Soomro, M.; McBeth, J.; Medina, C.R.R.; Lunt, M.; Dixon, W.G.; Jani, M. Comparative Risk of Severe Constipation in Patients Treated with Opioids for Non-Cancer Pain: A Retrospective Cohort Study in Northwest England. BMC Med. 2025, 23. [Google Scholar] [CrossRef]
- Thomé, B.I.; Scharan, K.O.; Assis, G.M.; Moser, A.D. de L. Unraveling the Frequency of Intestinal Constipation in Woman with Urinary Incontinence: A Descriptive Observational Study. Rev. Bras. Ginecol. Obstet. 2025, 47. [Google Scholar] [CrossRef] [PubMed]
- Leta, V.; Zinzalias, P.; Batzu, L.; Mandal, G.; Staunton, J.; Jernstedt, F.; Rosqvist, K.; Timpka, J.; van Vliet, T.; Trivedi, D.; et al. Effects of a Four-Strain Probiotic on Gut Microbiota, Inflammation, and Symptoms in Parkinson’s Disease: A Randomized Clinical Trial. Mov. Disord. 2025, 40, 2710–2721. [Google Scholar] [CrossRef]
- Umamahesan, C.; Pilcicka, A.; Yick, J.; Baker, K.; Smith, M.; Taylor, D.; Ma, Y.; Mullish, B.H.; Marchesi, J.R.; Gilbert, S.; et al. Interplay of Constipation, Intestinal Barrier Dysfunction and Fungal Exposome in Aetiopathogenesis of Parkinson’s Disease: Hypothesis with Supportive Data. Biochem. J. 2025, 482, 807–821. [Google Scholar] [CrossRef] [PubMed]
- Kutsuna, A.; Nishiyama, Y.; Sakamoto, Y.; Suzuki, F.; Hayashi, T.; Fujisawa, Y.; Suzuki, K.; Aoki, J.; Kimura, K. Constipation in Patients with Acute Ischemic Stroke: A Single-Center Retrospective Analysis. J. Nippon Med. Sch. 2025, 92, 154–162. [Google Scholar] [CrossRef]
- Li, M. qi; Li, Y.; Lam, W.; Yeung, W.F.; Ho, Y.S.; Li, J. ying; Sun, T.C.; Yuen, S.; Hu, Y. le; Yorke, J. Home-Based Acupressure for Managing Constipation and Subjective Well-Being in Spinal Cord Injury Survivors: A Randomized Controlled Trial. J. Integr. Med. 2025, 23, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Du, W.; Lu, L.; Liu, Y.; Yan, Y.; La, R.; Wu, Q.; Xu, J.; Zhou, X. The Association between Dietary Vitamin B1 Intake and Constipation: A Population-Based Study. BMC Gastroenterol. 2024, 24. [Google Scholar] [CrossRef]
- Komori, S.; Akiyama, J.; Tatsuno, N.; Yamada, E.; Izumi, A.; Hamada, M.; Seto, K.; Nishiie, Y.; Suzuki, K.; Hisada, Y.; et al. Prevalence and Risk Factors of Constipation Symptoms among Patients Undergoing Colonoscopy: A Single-Center Cross-Sectional Study. Digestion 2024, 105, 299–309. [Google Scholar] [CrossRef]
- Xian, X.; Wang, X.; Liu, J.; Yang, H. Investigation of Functional Constipation in Elderly Inpatients and Analysis of Its Influencing Factors: A Cross-Sectional Study. Medicine 2024, 103, e39624. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Chen, S.; Zhu, Y.; Wu, M.; Lu, B.; Zhou, X.; Zhu, Y.; Xu, X.; Liu, H.; Zhu, F.; et al. Intestinal Microbiome Changes and Mechanisms of Maintenance Hemodialysis Patients with Constipation. Front. Cell. Infect. Microbiol. 2024, 14. [Google Scholar] [CrossRef]
- Huang, K.Y.; Yu, Z.Z.; Tu, J.J.; Tang, X.Y.; Huang, J.M.; Lu, T.M.; Lu, Y.Q.; Huang, M.C.; Zhou, J.; Maier, A.B.; et al. Positive Association between Constipation and Mild Cognitive Impairment in Elders: A Cross-Sectional Study. Medicine 2024, 103, e39943. [Google Scholar] [CrossRef]
- Martin, C.R.; Osadchiy, V.; Kalani, A.; Mayer, E.A. The Brain-Gut-Microbiome Axis. Cell. Mol. Gastroenterol. Hepatol. 2018, 6, 133. [Google Scholar] [CrossRef]
- Yuan, C.; He, Y.; Xie, K.; Feng, L.; Gao, S.; Cai, L. Review of Microbiota Gut Brain Axis and Innate Immunity in Inflammatory and Infective Diseases. Front. Cell. Infect. Microbiol. 2023, 13. [Google Scholar] [CrossRef]
- Xie, J.; Bruggeman, A.; De Nolf, C.; Vandendriessche, C.; Van Imschoot, G.; Van Wonterghem, E.; Vereecke, L.; Vandenbroucke, R.E. Gut Microbiota Regulates Blood-Cerebrospinal Fluid Barrier Function and Aβ Pathology. EMBO J 2023, 42. [Google Scholar] [CrossRef] [PubMed]
- Esra Bozkurt, M.; Erdogan, T.; Fetullahoglu, Z.; Ozkok, S.; Kilic, C.; Bahat, G.; Akif Karan, M. Investigation of the Prevalence of Functional Constipation and Its Related Factors for in Older Outpatients. Acta Gastroenterol. Belg 2024, 87, 361–365. [Google Scholar] [CrossRef]
- Rudroff, C.; Madukkakuzhy, J.; Otten, J.; Schroer, J.; Richards, D.; Ludwig, S.; Henning, M. Improvement in Functional and Mental Outcomes after Resection Rectopexy for Obstructive Defecation Syndrome ODS. Sci. Rep. 2025, 15. [Google Scholar] [CrossRef]
- Namiuchi, S.; Sunamura, S.; Tanita, A.; Ogata, T.; Noda, K.; Takii, T.; Nitta, Y.; Yoshida, S. Effect of Constipation on Hospitalization Due to Heart Failure in Patients after Myocardial Infarction: A Retrospective Cohort Study. BMC Cardiovasc. Disord. 2025, 25. [Google Scholar] [CrossRef] [PubMed]
- Al Alawi, A.M.; Al Nou’mani, J.; Al Abri, N.; Al Sabbri, M.; Al-Maqbali, J.S. Impact of Constipation on Health Outcomes in Medically Hospitalized Patients: A Prospective Study on Laxative Use and Health Care Outcomes. Medicina (Kaunas) 2024, 60. [Google Scholar] [CrossRef]
- Xu, Y.; Xue, Z. The Relationship between Food Components and Constipation: A Cross-Sectional Study. BMC Gastroenterol 2024, 24. [Google Scholar] [CrossRef]
- Yu, Z.; Guo, M.; Bai, X.; Ruan, G.; Sun, Y.; Han, W.; Yang, H. Exploring the Association between Cardiovascular Health and Bowel Health. Sci. Rep. 2024, 14. [Google Scholar] [CrossRef] [PubMed]
- Kido, M.; Inoue, K.; Kobayashi, R.; Takashima, N.; Shoda, K.; Sugino, S.; Kato, R.; Itoh, Y. Seasonal Variations and a Demographic Analysis of Digital Evacuation Incidence for Constipation Management: A Japanese Population-Based Cohort Study. Intern. Med. 2025, 64, 1623–1632. [Google Scholar] [CrossRef]
- Li, S.; Wang, S.; Li, S.; Liu, C.; Sun, J.; Cao, J.; Cui, X.; Han, Q.; Li, Z.; Wu, F. Brain–Gut–Microbiota Axis: An Effective Target of Abdominal Acupuncture Therapy for Post-Stroke Functional Constipation. Complement. Ther. Med. 2025, 95, 103286. [Google Scholar] [CrossRef]
- Shen, S.; Feng, H.; Wang, C.; Yang, Y.; Chen, Z.; Wang, X.; Li, J. Association between the Dietary Index of Gut Microbiota and Abnormal Bowel Symptoms in U.S. Adults: A Cross-Sectional Study Based on NHANES 2007-2010. BMC Gastroenterol 2025, 25. [Google Scholar] [CrossRef]
- Huang, J.F.; Xiong, Y.J.; Da Meng, X.; Lv, T. Combined Association of Chewing Capacity and Depression with Constipation: A Cross-Sectional Study. BMC Gastroenterol 2025, 25. [Google Scholar] [CrossRef]
- Zhang, Y.Y.; Vimala, R.; Chui, P.L.; Hilmi, I.N. An Abdominal Vibration Combined with Walking Exercise (AVCWE) Program for Older Patients with Constipation: Development and Feasibility Study. Saudi J. Gastroenterol. 2024, 30, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.; Qin, W.; Liao, J.; Liu, Y.; Yan, L. Application of Traditional Chinese Medicine Nursing Technology: Traditional Chinese Medicine Ironing Combined with Traditional Chinese Medicine Massage in Improving Functional Constipation in Elderly Patients. Medicine 2024, 103, e39863. [Google Scholar] [CrossRef]
- Boangmanalu, E.S.; Masfuri, M.; Adam, M.; Nining, S.; Banna, T.; Pulungan, I.M. Swedish Abdominal Massage against Warm Water Therapy on Postoperative Orthopaedic Surgery Constipation: A Comparison Quasi-Experimental Study. F1000Res 2025, 13. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.M.; Rao, S.S.C.; Curtin, B.; Quigley, E. Real-World Evidence of the Long-Term Clinical Utility of a Vibrating Capsule in the Management of Chronic Idiopathic Constipation. Clin. Transl. Gastroenterol. 2025, 16. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xue, Y.; Chen, Q.; Ling, Y.; Zhou, H.; Li, M.; Xu, X.; Zeng, Y. Clinical Relevance of Transperineal Ultrasound Compared with Anorectal Manometry for the Evaluation of Female Patients with Obstructive Defecation Syndrome. BMC Gastroenterol. 2025, 25. [Google Scholar] [CrossRef]
- Zhang, G.; Wang, S.; Ma, P.; Wang, T.; Sun, X.; Zhang, X.; Li, H.; Pan, J. Association of Habitual Sleep Duration with Abnormal Bowel Symptoms: A Cross-Sectional Study of the 2005-2010 National Health and Nutrition Examination Survey. J. Health Popul. Nutr. 2024, 43. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, G.B.; Han, K.; Jung, E.J.; Suh, H.J.; Jo, K. Efficacy and Safety of Galacto-Oligosaccharide in the Treatment of Functional Constipation: Randomized Clinical Trial. Food Funct. 2024, 15, 6374–6382. [Google Scholar] [CrossRef]
- Suzuki, N.; Takeda, Y.; Kabuto, A.; Konishi, T.; Konishi, T.; Sumino, F.; Iwata, H.; Iwagami, M.; Kouchi, Y.; Hitomi, Y.; et al. Efficacy of Tenapanor in Managing Hyperphosphatemia and Constipation in Hemodialysis Patients: A Randomized Controlled Trial. PLoS One 2025, 20. [Google Scholar] [CrossRef]
- Nakajima, A.; Unno, A.; Ota, T.; Shoji, A.; Uenishi, T.; Igarashi, A. Socioeconomic Value of Treatments for Chronic Idiopathic Constipation in Japan. BMC Gastroenterol 2025, 25. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Zhang, J.; Yang, C.; Dong, X.; Wang, Y. Evaluation of Post-Market Adverse Events of Lubiprostone: A Real-World Adverse Event Analysis from the FAERS Database. BMC Gastroenterol 2025, 25. [Google Scholar] [CrossRef]
- Cash, B.D.; Lu, M.; Lembo, A.; Feuerstadt, P.; Nguyen, L.; Terasawa, E.; Ayyagari, R.; Du, S.; Pi, S.; Westermeyer, B.; et al. A Real-World Study of Persistence and Adherence to Prescription Medications in Patients with Chronic Idiopathic Constipation in the United States. J. Manag. Care Spec. Pharm. 2024, 30, 1136–1148. [Google Scholar] [CrossRef]
- Singh, R.G.; Aoki, F.; Rodriguez-Palmero Seuma, M.; Aguilo, M.; Washida, M.; Espadaler-Mazo, J.; Al-Wahsh, H.; Crowley, D.C.; Guthrie, N.; Evans, M.; et al. Efficacy of Probiotic Supplementation with Lactiplantibacillus Plantarum Strains on Gastrointestinal Tract Function - A Randomized Controlled Trial. J. Diet. Suppl. 2025, 22, 549–570. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Zhou, Y.; Xu, X.; Chen, S.; Zhang, S.; Jiang, N.; Liu, Z.; Zhang, J.; Luo, Z.; Zhang, X.; et al. Improvement of Post-Surgery Constipation in Patients with Fractures by Lactobacillus Rhamnosus JYLR-127: A Single-Blind Randomized Controlled Trial. Nutrients 2024, 16. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Zhang, Y.; Yue, F.; Yu, X.; Chen, Y.; Ma, X. Weizmannia Coagulans BC01 Supplementation Improved Functional Constipation by Regulating Gut Microbiota: A Randomized, Placebo-Controlled, Clinical Study. Medicine 2025, 104, e46861. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhang, Q.; Zhao, W.; Chen, J.; Liu, Y.; Zhou, L.; Liu, Y.; Wang, L.; Guan, Y.; He, J.; et al. Effects and Persistence of Bifidobacterium Animalis Subsp. Lactis BL-99 and Fructooligosaccharides on Older Adults with Functional Constipation: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Nutr. Health Aging 2025, 29. [Google Scholar] [CrossRef]
- Luk-In, S.; Leepiyasakulchai, C.; Saelee, C.; Keeratichamroen, A.; Srisangwan, N.; Ponprachanuvut, P.; Chammari, K.; Chatsuwan, T.; Wannigama, D.L.; Shein, A.M.S.; et al. Impact of Resistant Starch Type 3 on Fecal Microbiota and Stool Frequency in Thai Adults with Chronic Constipation Randomized Clinical Trial. Sci. Rep. 2024, 14. [Google Scholar] [CrossRef]
Figure 1.
Constipation as a Multifactorial Geriatric Syndrome.
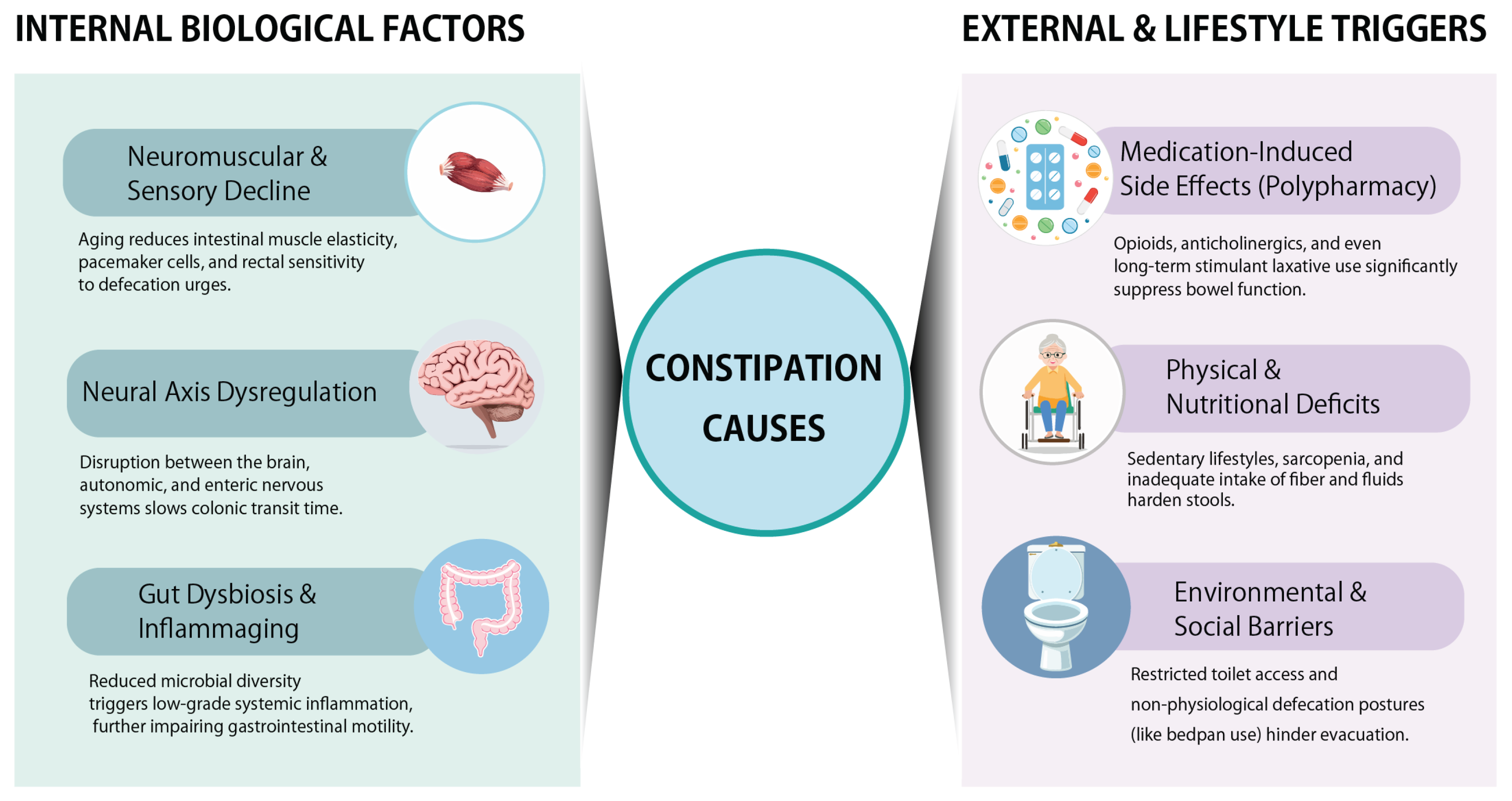
Figure 2.
Conceptual framework for the management of constipation in older adults.
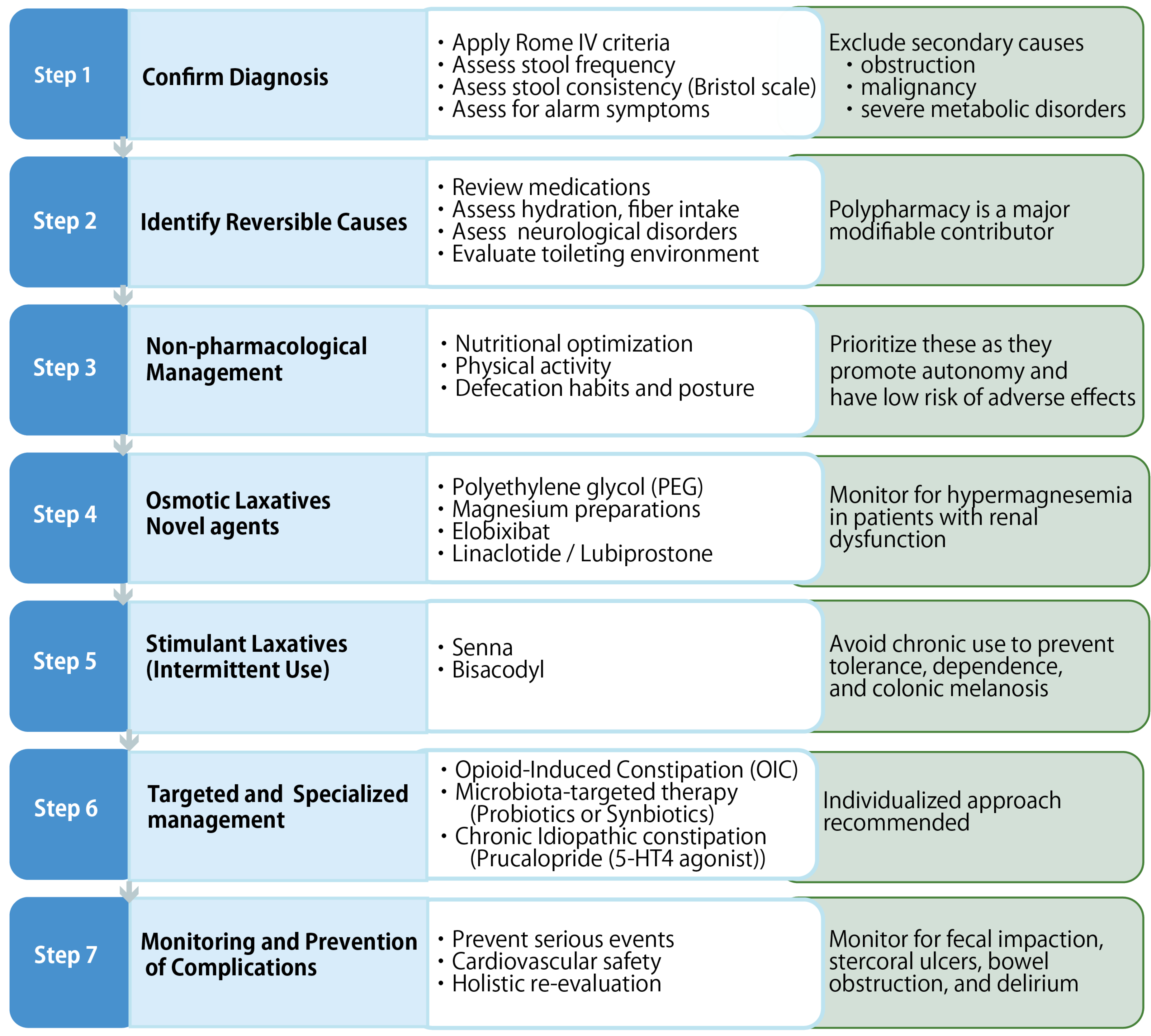

Table 1.
This is a figure. Schemes follow the same formatting.
| Aspect | Non-Pharmacological Interventions | Pharmacological Therapy | Microbiota-Targeted Therapy |
| Primary Methods | Dietary fiber and fluid intake, abdominal massage (Thai, Swedish), postural adjustment, and vibrating capsules [8]. | Osmotic laxatives (Mg Oxide, PEG), stimulants (Senna), prosecretory agents (Elobixibat, Lubiprostone, Linaclotide), and PAMORAs (Naldemedine) [70]. | Probiotics (L. plantarum, W. coagulans) and synbiotics (Bifidobacteria + FOS) [72]. |
| Mechanism of action | Mechanical stimulation of colonic motility, induction of the gastrocolic reflex, and optimization of the anorectal angle [63]. | Increases intestinal fluid secretion via ion channels or triggers direct peristaltic stimulation via enteric nerves [70]. | Reshaping gut microbiota, producing Short-Chain Fatty Acids (SCFAs), and strengthening the intestinal barrier [72]. |
| Elderly-Specific Benefits | Enhances patient autonomy, reduces psychological distress (anxiety/depression), and provides sensory stimulation [8]. | Provides rapid symptom relief; specific agents like PAMORAs are highly effective for opioid-induced constipation (OIC) [36]. | Improves stool consistency and frequency sustainably while positively influencing the brain-gut-microbiota axis to reduce stress [72]. |
| Risks & Side Effects | Requires caregiver training for massage; effectiveness of exercise/diet alone can be limited by immobility [2]. | Risk of dependence, tolerance, electrolyte imbalance, and hypermagnesemia in patients with renal impairment [8]. | Generally safe and well-tolerated; however, some patients may experience transient diarrhea during the early evacuation of accumulated stool [68]. |
| Economic & Clinical Utility | Offers low-cost interventions that can be integrated into primary care to reduce pharmacological dependence [8]. | Elobixibat is associated with lower total costs and better QoL in Japan; productivity loss is a major indirect cost [69]. | Requires additional supplement costs but can contribute to long-term health maintenance and reduced medication burden [72]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



