Submitted:
25 February 2026
Posted:
28 February 2026
You are already at the latest version
Abstract
Background: Care for knee osteoarthritis (KOA) is frequently fragmented, and pathway-level decisions within Physical Medicine and Rehabilitation (PM&R) are influenced by local organizations. We sought expert consensus on an ideal, function-oriented KOA care itinerary deliverable in PM&R services. Methods: A two-round Real-Time Delphi study was conducted using the SmartDelphi web platform. A steering committee of five PM&R physicians developed a 37-item questionnaire covering referral/access, functional and outcome assessment, conservative management, escalation/referral thresholds, and follow-up/discharge. Round 1 was online (SERMEF osteoarthritis working group; 46 invited, 40 completed; 87.0%) with responses collected until 30 April 2025. Round 2 was an in-person, facilitated validation round on 30 May 2025 at the SERMEF Congress (A Coruña; 85 invited, 70 completed; 82.4%). Items were rated on a 6-point Likert scale; consensus strength was defined by interquartile range (IQR): strong (0–1) vs weak (≥2). No patient-level data were collected; participant characteristics were comparable across rounds, suggesting consensus refinement reflected deliberation rather than panel shifts over time. Results: Consensus supported a longitudinal, function-first pathway structured into five phases: entry/referral to PM&R; comprehensive functional assessment using a minimum outcomes dataset (pain VAS/NRS, WOMAC function, quality-of-life scale); multimodal conservative rehabilitation combining exercise/physiotherapy, education/self-management support, and indicated oral/topical therapies; reassessment-guided escalation in non-responders, reserving interventional PM&R techniques, multidisciplinary musculoskeletal pain-unit management, or orthopaedic evaluation for persistent pain and/or functional limitation; and longitudinal monitoring with defined discharge criteria. Conclusions: SERMEF PM&R experts converged on an implementation-oriented, outcomes-driven KOA itinerary centred on functioning, conservative multimodal care, structured reassessment, and explicit discharge planning.
Keywords:
knee osteoarthritis
; physical medicine and rehabilitation
; Delphi consensus
; real-time Delphi
; care pathway
; rehabilitation itinerary
1. Introduction
Knee osteoarthritis (KOA) is a leading cause of chronic pain, reduced mobility, and years lived with disability, with substantial societal impact through work disability and healthcare utilisation. Recent Global Burden of Disease (GBD) analyses document a sustained increase in OA-related burden since 1990 and project further growth to 2050, driven largely by population ageing and demographic transitions [1]. Given its high prevalence and direct effect on walking capacity and participation, KOA is a key target for pathway-based, high-value care.
Across major clinical practice guidelines, KOA management is consistently anchored in non-pharmacological, person-centred interventions—therapeutic exercise, education and self-management support, weight management when indicated, and biomechanical/assistive strategies—while pharmacological and interventional approaches are positioned as adjuncts within a stepped-care model [2,3,4]. Despite this convergence, real-world delivery remains heterogeneous and frequently fragmented across levels of care and specialties, contributing to unwarranted variation in timing of conservative care, referral thresholds, continuity of follow-up, and alignment with patient priorities. In response, health-system quality initiatives have promoted measurable standards and pathway-based models to reduce variability and ensure timely access to evidence-based conservative management before escalation to specialist referral and surgical consideration [5,6].
Physical Medicine and Rehabilitation (PM&R) is positioned to coordinate a functioning-oriented itinerary for KOA that integrates pain management with disability reduction through personalised exercise prescription, movement and biomechanical optimisation, education, and shared goal-setting. In routine practice, PM&R commonly interfaces primary care, rheumatology/orthopaedics, physiotherapy, and community resources, and can operationalise minimum assessment datasets and longitudinal follow-up models focused on functioning outcomes. However, key pathway decisions—such as sequencing of interventions, criteria and timing for referral, minimum standards for access to structured rehabilitation, and follow-up intensity—are not always fully resolved by comparative evidence and are influenced by local service organisation and practice patterns.
In this context, formal consensus methods can produce implementation-ready recommendations when evidence is incomplete at the care-model level. Real-time digital Delphi approaches enable iterative rating with immediate aggregated feedback, improving efficiency and potentially reducing attrition compared with traditional multi-round designs [7]. For the present project, we used a Real-Time Delphi approach implemented with the SmartDelphi tool (www.smartdelphi.com) [8] a digitally adapted Delphi model designed to support online consensus-building in healthcare with rapid feedback and structured participation.
2. Materials and Methods
2.1. Study Design and Digital Platform
We conducted a two-round modified Real-Time Delphi consensus study to define a function-oriented care itinerary for patients with knee osteoarthritis (KOA) managed within Physical Medicine and Rehabilitation (PM&R) services. The process was implemented using the SmartDelphi web-based platform, which enables structured online participation with real-time aggregation of responses and visual feedback, allowing participants to review collective trends while preserving response anonymity [8]. The study combined an initial asynchronous digital round with a subsequent facilitated validation round conducted in person. This hybrid configuration reflects contemporary adaptations of Delphi methodology that integrate digital real-time feedback mechanisms and controlled panel expansion to enhance representativeness and external validation, while maintaining consistent eligibility criteria and identical questionnaire structure across rounds [7,8].
2.2. Questionnaire Development
The Delphi questionnaire was developed by a steering committee of five PM&R physicians, each with >10 years of experience in the conservative management of knee OA. The committee’s mandate was to define a function-oriented itinerary centered on pathway decision points aligned with functional assessment and longitudinal management. Through iterative meetings and item refinement, the committee finalized 37 items covering the main stages of the KOA itinerary: assessment, conservative management, escalation criteria, referral thresholds, and follow-up. Drafting was conducted between January and February 2025, followed by a technical review and proofreading during the first week of March 2025 to correct minor inconsistencies.
To enhance content validity and ensure comprehensive coverage of relevant clinical domains, questionnaire development followed a structured triangulation approach. The initial item pool was informed by a targeted review of major international clinical practice guidelines for knee osteoarthritis management, including EULAR, OARSI, and NICE recommendations, as well as by previously published care pathway models and rehabilitation-oriented outcome frameworks. Rather than conducting a formal systematic review, the steering committee performed a structured evidence-informed mapping exercise to identify key decision points across the KOA care trajectory, including referral patterns, functional assessment standards, therapeutic sequencing, escalation criteria, and follow-up strategies.
Draft items were iteratively refined through multidisciplinary expert discussion to ensure clinical relevance, clarity, and coverage of the full rehabilitation pathway. Particular attention was paid to capturing both intervention-related and organisational decision nodes, reflecting the real-world coordination role of PM&R services. The final set of 37 items was considered to provide adequate representational coverage of the KOA rehabilitation itinerary while maintaining feasibility for participant completion and response quality, consistent with methodological recommendations for Delphi questionnaire design. Figure 1 shows a screenshot of how the feedback is presented to participants, showing descriptive statistics and options to check any stratification of the answers to the questionnaires.
2.3. Participants, Eligibility, and Recruitment
Eligible participants were PM&R physicians who were members of the Spanish Society of Physical Medicine and Rehabilitation (SERMEF) and had clinical experience in knee OA management. No formal sample size calculation was performed, consistent with Delphi methodology, which prioritizes expertise over statistical representativeness.
Round 1 (online, asynchronous). Participants were recruited from the SERMEF osteoarthritis working group. Invitations were distributed by SERMEF via email, and participants accessed the questionnaire through a web link sent to their email address. Round 1 responses were collected until 30 April 2025. The steering committee reviewed Round 1 outputs to evaluate item clarity and interpretability and to identify domains requiring consolidation prior to the in-person consensus exercise.
Round 2 (in-person, facilitated). Round 2 was conducted on 30 May 2025 during the SERMEF Congress in A Coruña. Participants joined by scanning a QR code displayed on the projection screen, providing direct access to the same online questionnaire.
A total of 46 eligible PM&R physicians from the SERMEF osteoarthritis working group were invited to participate in Round 1 of the Delphi process. Of these, 40 completed the questionnaire, corresponding to a response rate of 87.0%.
Round 2 was conducted during the SERMEF Congress and was designed as an expanded validation round allowing participation from a broader group of clinicians with expertise in knee osteoarthritis management. A total of 85 physicians were invited to participate in this phase, of whom 70 completed the questionnaire, yielding a response rate of 82.4%.
Although Round 2 incorporated additional participants, eligibility criteria and questionnaire structure remained identical across rounds, ensuring methodological consistency. The demographic and professional characteristics of participants were comparable across rounds, suggesting that consensus refinement primarily reflects iterative expert deliberation rather than shifts in panel composition.
To minimise recruitment bias, invitations were distributed centrally by the scientific society rather than by individual investigators. Participation was restricted to PM&R physicians with demonstrated clinical involvement in knee osteoarthritis management. The inclusion of a second round conducted during a national scientific congress increased panel heterogeneity and improved representativeness across different clinical settings and levels of experience.
As participation was voluntary, self-selection bias cannot be fully excluded. However, the high response rates and broad distribution of professional characteristics support the representativeness of the expert panel.
Figure 2 summarizes the tasks done by the research team and participants in the two Delphi rounds.
2.4. Delphi Procedure and Rating Scale
In both rounds, participants rated each item using a 6-point Likert scale (1 = strongly disagree; 6 = strongly agree). The digital platform enabled immediate aggregation and visualization of group responses to support structured consensus-building and facilitate interpretation during the in-person exercise.
2.5. Data Collection
In addition to item ratings, participants reported demographic and professional characteristics including age, gender, geographic region, and years of clinical experience. No patient-level data were collected.
2.6. Consensus Criteria
Consensus strength was assessed using the interquartile range (IQR) of item ratings. Strong consensus was defined as IQR 0–1. Weak consensus was defined as IQR ≥2, indicating heterogeneous ratings and highlighting items requiring further consolidation and discussion in the subsequent consensus step.
2.7. Statistical Analysis
For each item and round, responses were summarized using the median and IQR. Items were classified according to the predefined consensus categories (strong vs. weak) based on IQR thresholds. Where relevant, the proportion of respondents selecting high-agreement categories (ratings 5–6) was also calculated to support interpretability of agreement intensity. Analyses were performed with item-level denominators (i.e., n reported per item), and missing data were handled at the item level (pairwise).
Panel stability and representativeness were descriptively evaluated by comparing aggregated demographic and professional characteristics of participants across rounds.
2.8. Ethical and Data Protection Considerations
Participation was voluntary. All participants received study information and provided electronic informed consent prior to questionnaire access. Data were collected and analyzed in anonymized form, and processing complied with applicable data-protection requirements (GDPR, EU 2016/679).
3. Results
3.1. Delphi participants Rounds 1 and 2
The composition of the expert panel remained stable across rounds. Participants in both rounds shared comparable clinical and professional profiles, including years of experience in musculoskeletal medicine, active clinical practice, and institutional settings. No relevant structural differences were observed between rounds, suggesting that changes in consensus primarily reflect the deliberative effect of the Delphi process rather than shifts in panel composition.
The characteristics of the SERMEF Physical Medicine and Rehabilitation (PM&R) physicians who participated in both Delphi rounds are summarized in Table 1.
3.2. Construction of the Function-Oriented KOA Rehabilitation Pathway
Beyond item-level agreement, the Delphi exercise supported the integration of consensus statements into a coherent, function-oriented rehabilitation pathway for patients with KOA managed within PM&R services. Using items that achieved strong consensus (IQR 0–1) and mapping their logical sequence within routine clinical workflows, we constructed a sequential model of care structured around key decision points and longitudinal management (Table 2; Figure 3).

Table 2.
a. Item-Level Agreement and Consensus Metrics across the Two Delphi Rounds (R1 vs. R2): Pathways.
Table 2.
a. Item-Level Agreement and Consensus Metrics across the Two Delphi Rounds (R1 vs. R2): Pathways.
| # | Item (full text) | Mean | Δ | Median | SD | IQR | ||||
| R1 | R2 | Mean | R1 | R2 | R1 | R2 | R1 | R2 | ||
| Q37 | Ideally, defined discharge criteria should exist. | 5.20 | 5.43 | 0.23 | 5 | 5 | 0.72 | 0.63 | 1 | 1 |
| Q33 | Ideally, outcome measures should include a WOMAC knee functional scale. | 4.88 | 5.15 | 0.27 | 5 | 5 | 1.02 | 0.63 | 2 | 1 |
| Q34 | Ideally, outcome measures should include a quality of life scale. | 4.53 | 4.97 | 0.44 | 5 | 5 | 0.85 | 0.74 | 1 | 0 |
| Q32 | Ideally, outcome measures should include a pain scale (VAS/NRS). | 4.75 | 4.96 | 0.21 | 5 | 5 | 1.06 | 0.83 | 2 | 1 |
| Q28 | In knee osteoarthritis, the therapeutic sequence should include physical therapy in combination with oral and/or topical therapy and/or interventional techniques. | 4.53 | 4.91 | 0.38 | 5 | 5 | 0.93 | 0.79 | 1 | 0 |
| Q27 | In knee osteoarthritis, the therapeutic sequence should be topical therapy, oral therapy, physical therapy, and interventional techniques. | 4.63 | 4.89 | 0.26 | 5 | 5 | 1.08 | 0.99 | 1 | 2 |
| Q24 | Ideally, patients with knee osteoarthritis should be seen in a general rehabilitation outpatient clinic. | 4.35 | 4.72 | 0.37 | 5 | 5 | 1.19 | 1.04 | 1 | 1 |
| Q21 | Ideally, patients with knee osteoarthritis should be referred from primary care or other physicians. | 4.61 | 4.71 | 0.10 | 5 | 5 | 1.14 | 1.00 | 1 | 1 |
| Q23 | Ideally, patients with knee osteoarthritis should be managed in a multidisciplinary musculoskeletal pain unit. | 4.43 | 4.51 | 0.08 | 5 | 5 | 1.47 | 1.17 | 3 | 1 |
| Q25 | Ideally, patients with knee osteoarthritis should be seen in a dedicated osteoarthritis clinic. | 3.95 | 3.81 | 0.14 | 4 | 4 | 1.18 | 1.21 | 2 | 2 |
| Q36 | Ideally, outcome measures should include PROMs (Patient-Reported Outcome Measures). | 4.05 | 3.80 | 0.25 | 4 | 4 | 1.11 | 1.24 | 2 | 2 |
| Q35 | Ideally, outcome measures should include subjective assessment scales (patient and clinician). | 3.85 | 3.66 | 0.19 | 4 | 4 | 1.12 | 1.08 | 2 | 2 |
| Q22 | Ideally, patients with knee osteoarthritis should be referred from rheumatology. | 2.83 | 3.04 | 0.21 | 3 | 3 | 0.83 | 1.12 | 1 | 2 |
| Q31 | Ideally, outcome measures should include a descriptive scale (same/worse/better). | 2.93 | 2.85 | 0.08 | 3 | 3 | 0.92 | 0.97 | 1 | 1 |
| Q20 | Ideally, patients with knee osteoarthritis should be referred from orthopaedics (COT). | 2.15 | 2.38 | 0.23 | 2 | 2 | 0.82 | 0.89 | 1 | 1 |
| Q26 | Ideally, patients with knee osteoarthritis should be seen in a dedicated interventional clinic. | 2.83 | 2.29 | 0.54 | 3 | 2 | 0.98 | 0.89 | 2 | 1 |
| Q30 | Interventional techniques should be used as first-line treatment combined with physical therapy. | 2.08 | 1.82 | 0.26 | 2 | 2 | 0.73 | 0.83 | 0 | 1 |
Table 2.
b. Item-Level Agreement and Consensus Metrics across the Two Delphi Rounds (R1 vs. R2): Treatments.
Table 2.
b. Item-Level Agreement and Consensus Metrics across the Two Delphi Rounds (R1 vs. R2): Treatments.
| Mean | Δ | Median | SD | IQR | ||||||
| # | Item (full text) | R1 | R2 | Mean | R1 | R2 | R1 | R2 | R1 | R2 |
| Q15 | Ideally, treatment should include therapeutic exercise | 5.52 | 5.71 | 0.19 | 6 | 6 | 0.71 | 0.52 | 0 | 0 |
| Q14 | Ideally, treatment should include weight control | 5.41 | 5.65 | 0.24 | 6 | 6 | 0.76 | 0.60 | 0 | 0 |
| Q9 | Ideally, treatment should include oral strong opioids | 2.32 | 2.05 | 0.27 | 2 | 2 | 0.94 | 0.81 | 1 | 1 |
| Q18 | Ideally, treatment should include orthoses | 2.56 | 2.40 | 0.16 | 2 | 2 | 1.01 | 0.95 | 1 | 1 |
| Q17 | Ideally, treatment should include occupational therapy | 2.48 | 2.36 | 0.12 | 2 | 2 | 0.98 | 0.88 | 1 | 1 |
| Q8 | Ideally, treatment should include oral tramadol | 3.21 | 3.10 | 0.11 | 3 | 3 | 1.02 | 0.93 | 1 | 1 |
| Q19 | Ideally, treatment should include heat or cold therapy | 3.98 | 4.07 | 0.09 | 4 | 4 | 1.07 | 1.00 | 2 | 2 |
| Q7 | Ideally, treatment should include oral NSAIDs | 4.02 | 4.18 | 0.16 | 4 | 4 | 1.12 | 1.05 | 2 | 2 |
| Q13 | Ideally, treatment should include topical capsaicin | 3.22 | 3.15 | 0.07 | 3 | 3 | 1.03 | 1.02 | 2 | 2 |
| Q12 | Ideally, treatment should include topical NSAIDs | 4.01 | 3.86 | 0.15 | 4 | 4 | 1.08 | 1.16 | 2 | 2 |
| Q11 | Ideally, treatment should include chondroitin or glucosamine | 3.25 | 3.12 | 0.13 | 3 | 3 | 1.15 | 1.18 | 2 | 2 |
| Q10 | Ideally, treatment should include duloxetine | 3.08 | 3.01 | 0.07 | 3 | 3 | 1.06 | 1.12 | 2 | 2 |
| Q6 | Ideally, treatment should include classical analgesic electrotherapy | 3.11 | 3.02 | 0.09 | 3 | 3 | 1.09 | 1.15 | 2 | 2 |
| Q16 | Ideally, treatment should include physiotherapy | 3.04 | 2.92 | 0.12 | 3 | 3 | 1.14 | 1.19 | 2 | 2 |
Table 2.
c. Item-Level Agreement and Consensus Metrics across the Two Delphi Rounds (R1 vs. R2): Referral criteria.
Table 2.
c. Item-Level Agreement and Consensus Metrics across the Two Delphi Rounds (R1 vs. R2): Referral criteria.
| # | Mean | Δ | Median | SD | IQR | |||||
| # | Item (full text) | R1 | R2 | Mean | R1 | R2 | R1 | R2 | R1 | R2 |
| Q1 | The ideal management of KOA patients should include early evaluation by PM&R specialists | 5.34 | 5.58 | 0.24 | 6 | 6 | 0.81 | 0.63 | 1 | 0 |
| Q2 | KOA management should prioritise functional recovery as a primary clinical objective | 5.46 | 5.69 | 0.23 | 6 | 6 | 0.77 | 0.58 | 1 | 0 |
| Q3 | KOA patient care should be coordinated through multidisciplinary management | 5.12 | 5.41 | 0.29 | 5 | 6 | 0.96 | 0.76 | 1 | 1 |
| Q4 | PM&R services should play a central coordinating role in KOA care pathways | 4.98 | 5.21 | 0.23 | 5 | 5 | 1.01 | 0.88 | 2 | 1 |
| Q5 | KOA clinical management should include structured clinical pathway protocols | 4.86 | 5.03 | 0.17 | 5 | 5 | 1.08 | 0.94 | 2 | 2 |
Figure 3.
Mean Item Ratings across the Two Delphi Rounds (Round 1 vs. Round 2).
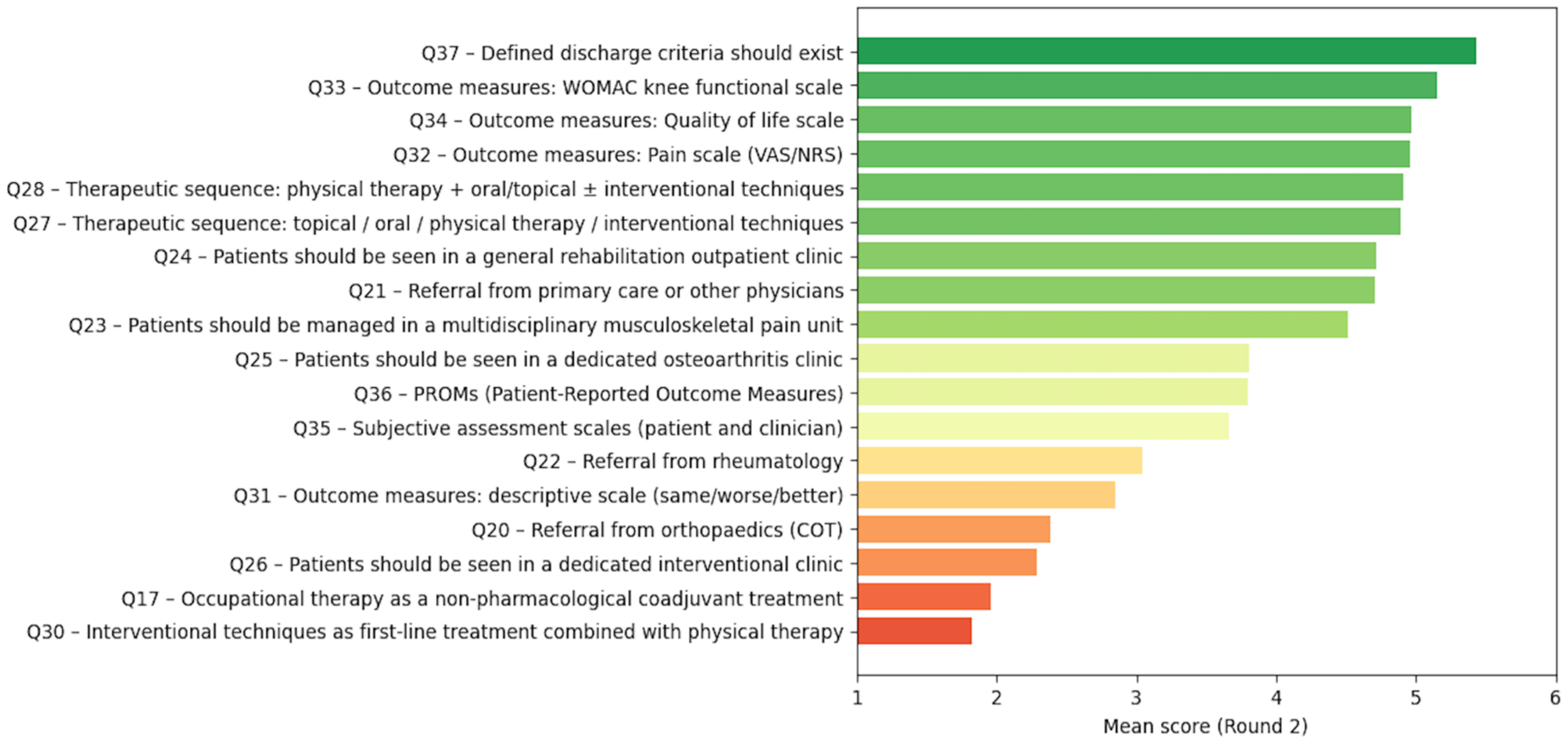
The resulting pathway is organized into five interrelated clinical phases: (1) entry and referral, (2) comprehensive functional assessment, (3) structured conservative intervention, (4) escalation and interventional decision-making, and (5) longitudinal monitoring and discharge planning.
3.2.1. Entry and Referral Phase.
Consensus supported that KOA patients should typically access PM&R through referral from primary care or other physicians and be evaluated within a general rehabilitation outpatient setting (Table 2). The entry phase includes confirmation of the clinical diagnosis, exclusion of alternative causes of knee pain, and identification of factors requiring prioritization or early referral.
3.2.2. Comprehensive Functional Assessment Phase.
Strong consensus emerged for the systematic use of multidimensional outcome measures to guide clinical decision-making, including pain assessment scales (VAS/NRS), disease-specific functional measures such as WOMAC, and quality-of-life scales (Table 2). These measures were incorporated as core components of baseline assessment and subsequent reassessment within the pathway.
3.2.3. Structured Conservative Intervention Phase.
The panel endorsed a multimodal conservative management approach coordinated within PM&R services. Items with higher agreement supported combining physical therapy with oral and/or topical therapies and, when appropriate, interventional techniques as adjuncts rather than standalone strategies (Table 2). Accordingly, the pathway integrates exercise-based therapy and rehabilitation interventions with pharmacological/topical options based on clinical indication and functional status.
3.2.4. Escalation and Interventional Decision-Making Phase.
Consistent with the lowest-rated items, experts did not support the use of interventional techniques as first-line treatment (Table 2). Interventions were positioned in the pathway as escalation options for patients with persistent pain and/or functional limitation despite adequate conservative management, with decision nodes informed by reassessment outcomes.
3.2.5. Longitudinal Monitoring and Discharge Planning Phase.
One of the highest-rated statements in the Delphi process was the need for defined discharge criteria (Table 2). The pathway therefore incorporates periodic follow-up and reassessment using the same validated measures applied at baseline to monitor response and guide continuation, optimization, escalation, or discharge decisions. Discharge is framed as a planned transition following achievement of predefined criteria and functional stabilization.
Taken together, these consensus-derived elements define a structured, function-oriented KOA rehabilitation pathway characterized by standardized assessment, multimodal conservative care as the foundation of management, escalation based on treatment response, and explicit discharge planning supported by repeated outcome measurement (Table 2; Figure 3).
3.3. Mapping of Delphi Consensus Statements to the Rehabilitation Pathway Model
To enhance methodological transparency, the construction of the rehabilitation pathway was based on a structured mapping process linking individual Delphi consensus statements to specific clinical phases and decision nodes within the proposed care model. Items achieving strong consensus (IQR 0–1) were considered core structural components of the pathway, whereas items showing moderate consensus informed supportive or contextual elements.
The mapping process followed three sequential steps. First, consensus items were grouped according to their primary clinical domain, including referral and access to care, functional assessment, therapeutic intervention, escalation criteria, and follow-up strategies. Second, items were organised into a chronological sequence reflecting routine clinical workflows in KOA management. Third, related items were synthesised into decision nodes defining transitions between pathway phases.
For example, items supporting referral from primary care and evaluation within general rehabilitation outpatient clinics were mapped to the entry phase of the pathway. Items demonstrating strong agreement regarding the use of validated outcome measures, including WOMAC, pain scales, and quality-of-life instruments, were incorporated into the comprehensive functional assessment phase. Statements supporting multimodal conservative management informed the intervention phase, whereas items rejecting interventional procedures as first-line treatment contributed to defining escalation criteria. Finally, consensus on the need for explicit discharge criteria was mapped to the longitudinal monitoring and discharge phase.
This structured mapping approach ensured that the final pathway model directly reflects expert consensus rather than post hoc interpretative synthesis, thereby strengthening the conceptual validity of the proposed care itinerary. Table 3 summarizes the mapping of the Delphi items.
Figure 4 shows the algorithm that summarizes the consensus-derived clinical itinerary for patients with symptomatic KOA managed within PM&R.
4. Discussion
This Real-Time Delphi consensus among SERMEF PM&R physicians proposes a structured, function-oriented care itinerary for patients with KOA managed within rehabilitation services. The outputs converge on a longitudinal model centered on standardized outcome assessment, multimodal conservative care as the foundation of management, escalation guided by reassessment, and explicit discharge criteria—elements that are consistent with contemporary international guidance emphasizing exercise, education/self-management support, and person-centered care [2,9,10].
4.1. Function-First Framing and Measurement Strategy
A central implication of the consensus is the prioritization of function as the organizing principle of KOA rehabilitation. The strong endorsement of WOMAC, pain intensity scales, and quality-of-life measures supports a minimum dataset that captures symptom severity, disability, and broader impact. This is aligned with guideline syntheses showing that higher-quality OA recommendations consistently foreground exercise, education, and patient-centered outcomes, and with updated EULAR non-pharmacological core recommendations for hip/knee osteoarthritis [2,10,11].
The more heterogeneous endorsement of broader PROMs and subjective global ratings is plausibly explained by implementation barriers in routine care (time, workflow integration, digital infrastructure, and standardization). Recent evidence syntheses and implementation studies highlight that PROM initiatives can improve care, but successful uptake depends strongly on design and implementation strategies, including co-design with patients and clinicians [12,13].
From a pathway perspective, anchoring decisions to repeated measurement is also clinically meaningful because clinically important change thresholds are heterogeneous across instruments and contexts; contemporary syntheses provide estimates of minimal important change/difference for commonly used KOA outcome tools, supporting interpretability of longitudinal monitoring [14].
4.2. Conservative Multimodal Care as the Backbone
The pathway structure derived from the Delphi aligns with the evidence base positioning exercise therapy and rehabilitation interventions as first-line management in KOA and noting persistent underutilization despite strong evidence [2,15,16].
The panel’s preference for integration over rigid step ordering is also coherent with real-world KOA care, where tailoring is required based on clinical phenotype, comorbidities, symptom drivers, and functional goals. Guideline syntheses further indicate that while core recommendations are consistent, variability persists in adjunctive options and in practical applicability/implementation guidance—an issue that may contribute to heterogeneity for “fixed-sequence” statements [10,11].
4.3. Escalation and Interventional Positioning
A clinically important convergence in this Delphi is the lack of support for interventional techniques as a first-line strategy, with interventional options positioned as escalation tools following inadequate response to conservative management. This pattern is consistent with major guidance that prioritizes conservative interventions and recommends intra-articular therapies selectively (e.g., corticosteroid injections for acute exacerbation—particularly with effusion—rather than as routine first-line treatment) [9,17,18].
This consensus supports an escalation logic based on reassessment and function rather than procedure-led pathways, while still preserving a role for interventions as part of a stepped, individualized plan.
4.4. Service Configuration, Referral Routes, and Multidisciplinary Models
The consensus that KOA can be appropriately managed within general rehabilitation outpatient settings, with frequent referral from primary care, aligns with pragmatic access structures in many systems and with the emphasis on early delivery of non-pharmacological core care [2,10].
The observed convergence toward multidisciplinary musculoskeletal pain-unit models after Round 2 is consistent with emerging literature that argues for integrated, interprofessional care pathways in KOA, even though KOA-specific outcome evidence for collaboration models remains comparatively limited [19].
4.5. Discharge Criteria and Longitudinal Follow-Up as Quality Levers
The strong consensus on explicit discharge criteria is particularly actionable. KOA is a chronic, fluctuating condition; structured discharge criteria can standardize transitions from specialist rehabilitation to supported self-management and community/primary care follow-up, while preserving the capacity to re-enter specialist care when function deteriorates. This emphasis is coherent with guideline calls for sustained self-management strategies and ongoing exercise engagement as core elements of OA management [9,16,17].
4.6. Implications for Implementation
Taken together, the consensus itinerary provides a pragmatic scaffold for reducing unwarranted variability in KOA rehabilitation practice. Near-term implementation priorities supported by both consensus and contemporary guidance include: (i) embedding a minimum dataset (pain, WOMAC/function, QoL) at baseline and follow-up; (ii) ensuring consistent access to multimodal conservative care (exercise-based therapy, education/self-management support, and indicated adjunct therapies); (iii) defining escalation triggers based on reassessment; and (iv) standardizing discharge criteria and transition plans [2,9,12].
4.7. Strengths and Limitations
Several methodological considerations should be acknowledged. The second Delphi round incorporated additional participants recruited during a national congress, which differs from traditional fixed-panel Delphi designs. However, this strategy is consistent with real-time Delphi methodologies aimed at increasing representativeness and validating consensus across a broader expert community. The consistent eligibility criteria, identical questionnaire structure, and comparable participant characteristics between rounds support the robustness of the consensus findings.
Strengths include the Real-Time Delphi approach and the two-round structure (asynchronous followed by in-person), which plausibly promoted convergence for items with initial dispersion. Limitations include restriction to SERMEF PM&R physicians (potentially underrepresenting primary care, rheumatology, orthopaedics, physiotherapy, nursing, and patient perspectives), and the fact that Delphi agreement does not directly establish effectiveness—highlighting the need for prospective implementation evaluation.
4.8. Future Directions
Next steps should include multi-stakeholder co-design (including patients) and implementation studies assessing feasibility, fidelity, functional outcomes, patient-reported outcomes, and resource use. PROM implementation evidence indicates that impact depends on workflow integration and stakeholder engagement, supporting a structured implementation plan alongside the pathway [12,13].
5. Conclusions
This Real-Time Delphi study among SERMEF Physical Medicine and Rehabilitation (PM&R) physicians defines an implementation-oriented, function-centred care itinerary for patients with knee osteoarthritis managed within rehabilitation services. Expert consensus converged on a longitudinal pathway structured around five linked phases: (1) entry and referral to PM&R, typically from primary care; (2) standardized baseline assessment using a minimum dataset that includes pain intensity (VAS/NRS), function (WOMAC), and quality of life; (3) multimodal conservative rehabilitation as the foundation of management (exercise-based therapy/physiotherapy, education and self-management support, and indicated oral/topical therapies); (4) escalation guided by scheduled reassessment, with interventional PM&R techniques, multidisciplinary musculoskeletal pain-unit management, or orthopaedic evaluation reserved for patients with persistent pain and/or functional limitation despite adequate conservative care; and (5) longitudinal follow-up with explicit, predefined discharge criteria supported by repeated outcome measurement.
Overall, the resulting model provides a pragmatic scaffold to reduce unwarranted variability in KOA rehabilitation and to operationalize a stepped, outcomes-driven approach centred on functioning. Future work should focus on multi-stakeholder co-design (including patients and other specialties) and prospective implementation studies to evaluate feasibility, fidelity, patient-reported outcomes, functional impact, and resource use when applying this itinerary in routine care.
Author Contributions
Conceptualization, HB-A, JF-C, CC-G, SF-G, JIC-M and JMM-F; methodology, HB-A, JMM-F, AT-O, MC-P.; software, AT-O, MC-P.; validation, HB-A, JF-C, CC-G, SF-G, JIC-M and MC-P.; formal analysis, AT-O, MC-P and JMM-F.; investigation, HB-A, JF-C, and JMM-F; resources, HB-A and JF-C; data curation, AT-O, MC-P and JMM-F; writing—original draft preparation, HB-A and JMM-F; writing—review and editing, HB-A and JMM-F; visualization, HB-A and JMM-F.; supervision, JF-P, AT-O and MC-P; project administration, HB-A and JMM-F.; funding acquisition JF-C and HB-A. All authors have read and agreed to the published version of the manuscript.
Funding
The authors declare that this research was supported by an unrestricted research grant from Meiji Pharma Spain, S.A., a subsidiary of Meiji Holdings Co., Ltd., which is a diversified company engaged in the manufacture and sale of pharmaceutical products (including antibiotics, hyaluronic acid–based medicines, and other pharmaceutical formulations) and, on a broader group level, food products, nutritional supplements, and consumer goods. Meiji Pharma Spain had no role in the study design; collection, analysis, or interpretation of data; writing of the manuscript; or the decision to publish the results. All opinions, findings, conclusions, and recommendations expressed in this article are solely those of the authors and do not necessarily reflect the views of the sponsor.
Institutional Review Board Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki and complied with applicable Spanish and European regulations on biomedical research and data protection, including the Spanish Biomedical Research Law 14/2007, Royal Decree 1090/2015, and the General Data Protection Regulation (GDPR, EU 2016/679). In accordance with Articles 2 and 3 of Law 14/2007 and Article 2 of Royal Decree 1090/2015, review by a Research Ethics Committee (CEIm) was not required because the study consisted exclusively of an anonymous survey of healthcare professionals, with no intervention, no collection of biological samples, and no collection or processing of personal health data from patients.
Informed Consent Statement
Participation was voluntary. All participants received an online information sheet describing the study objectives, procedures, and data protection safeguards, and provided electronic informed consent prior to accessing the questionnaire. Eligibility was confirmed through screening questions verifying: (i) SERMEF membership; and (ii) for the in-person round, ≥5 years of clinical experience in the conservative management of knee osteoarthritis. Survey data were collected anonymously through the SmartDelphi web platform. No directly identifiable information was collected or stored, and responses were analysed only in aggregated form to preserve confidentiality. During both the asynchronous and face-to-face Real-Time Delphi rounds, feedback was provided exclusively at group level, without any possibility of attributing responses to individual participants. The study protocol was reviewed internally by the coordinating team and endorsed by the Spanish Society of Physical Medicine and Rehabilitation (SERMEF).
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to privacy restrictions.
Acknowledgments
We thank the rehabilitation physicians from the Spanish Society of Physical Medicine and Rehabilitation (SERMEF) who participated in the Delphi process for their time, commitment, and valuable contributions.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| KOA | Knee Osteoarthritis |
| PM&R | Physical Medicine and Rehabilitation |
| MSK | Musculoskeletal |
References
- Steinmetz, J.D.; et al. GBD 2021 Osteoarthritis Collaborators. Global, Regional, and National Burden of Osteoarthritis, 1990–2020 and Projections to 2050: A Systematic Analysis for the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023, 5, e508–e522. [Google Scholar] [CrossRef] [PubMed]
- Moseng, T.; Vliet Vlieland, T.P.M.; Battista, S.; et al. EULAR Recommendations for the Non-Pharmacological Core Management of Hip and Knee Osteoarthritis: 2023 Update. Ann. Rheum. Dis. 2024, 83, 730–740. [Google Scholar] [CrossRef] [PubMed]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; et al. OARSI Guidelines for the Non-Surgical Management of Knee, Hip, and Polyarticular Osteoarthritis. Osteoarthritis Cartilage 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE). Osteoarthritis in Over 16s: Diagnosis and Management (NG226); NICE: London, UK, 2022. [Google Scholar]
- Ackerman, I.N.; Doukas, F.; Buchbinder, R.; et al. Ensuring a Fit-for-Purpose Resource for Consumers, Clinicians and Health Services: The Updated Osteoarthritis of the Knee Clinical Care Standard. Med. J. Aust. 2024, 221, 197–200. [Google Scholar] [CrossRef] [PubMed]
- Australian Commission on Safety and Quality in Health Care (ACSQHC). Osteoarthritis of the Knee Clinical Care Standard; ACSQHC: Sydney, Australia, 2024. [Google Scholar]
- Varndell, W.; Fry, M.; Elliott, D. Applying Real-Time Delphi Methods: Development of a Pain Management Survey in Emergency Nursing. BMC Nurs. 2021, 20, 149. [Google Scholar] [CrossRef] [PubMed]
- Monguet, J.M.; Trejo, A.; Martí, T.; Escarrabill, J. Health Consensus: A Digital Adapted Delphi for Healthcare. Int. J. User-Driven Healthc. 2017, 7, 27–43. [Google Scholar] [CrossRef]
- Brophy, R.H.; Fillingham, Y.A. AAOS Clinical Practice Guideline Summary: Management of Osteoarthritis of the Knee (Nonarthroplasty), Third Edition. J. Am. Acad. Orthop. Surg. 2022, 30, e721–e729. [Google Scholar] [CrossRef] [PubMed]
- Conley, B.; Bunzli, S.; Bullen, J.; O’Brien, P.; Persaud, J.; Gunatillake, T.; Dowsey, M.M.; Choong, P.F.M.; Lin, I. Core Recommendations for Osteoarthritis Care: A Systematic Review of Clinical Practice Guidelines. Arthritis Care Res. (Hoboken) 2023, 75, 1897–1907. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, A.J.; Gray, B.; Wallis, J.A.; Taylor, N.F.; Kemp, J.L.; Hunter, D.J.; Barton, C.J. Recommendations for the Management of Hip and Knee Osteoarthritis: A Systematic Review of Clinical Practice Guidelines. Osteoarthritis Cartilage 2023, 31, 1280–1292. [Google Scholar] [CrossRef] [PubMed]
- Bonsel, J.M.; Itiola, A.J.; Huberts, A.S.; Bonsel, G.J.; Penton, H. The Use of Patient-Reported Outcome Measures to Improve Patient-Related Outcomes—A Systematic Review. Health Qual. Life Outcomes 2024, 22, 101. [Google Scholar] [CrossRef] [PubMed]
- Amat-Fernandez, C.; Pardo, Y.; Bosch, G.; Lizano-Barrantes, C.; Briseño Diaz, R.; Vernet-Tomas, M.; Fumadó, L.; Beisani, M.; Redondo Pachón, D.; Bach Pascual, A.; et al. Evaluating the Implementation of PROMs and PREMs in Routine Clinical Care: Co-Design of Tools from the Perspective of Patients and Healthcare Professionals. Health Qual. Life Outcomes 2025, 23, 15. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.D.C.; Perriman, D.M.; Fearon, A.M.; Couldrick, J.M.; Scarvell, J.M. Minimal Important Change and Difference for Knee Osteoarthritis Outcome Measurement Tools after Non-Surgical Interventions: A Systematic Review. BMJ Open 2023, 13, e063026. [Google Scholar] [CrossRef] [PubMed]
- Young, J.J.; Pedersen, J.R.; Bricca, A. Exercise Therapy for Knee and Hip Osteoarthritis: Is There an Ideal Prescription? Curr. Treatm. Opt. Rheumatol. 2023, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Lawford, B.J.; Hall, M.; Hinman, R.S.; van der Esch, M.; Harmer, A.R.; Spiers, L.; Kimp, A.; Dell’Isola, A.; Bennell, K.L. Exercise for Osteoarthritis of the Knee. Cochrane Database Syst. Rev. 2024, 12, CD004376. [Google Scholar] [CrossRef] [PubMed]
- Uson, J.; Rodriguez-García, S.C.; Castellanos-Moreira, R.; O’Neill, T.W.; Doherty, M.; Boesen, M.; Pandit, H.; Möller Parera, I.; Vardanyan, V.; Terslev, L.; et al. EULAR Recommendations for Intra-Articular Therapies. Ann. Rheum. Dis. 2021, 80, 1299–1305. [Google Scholar] [CrossRef] [PubMed]
- Pereira, T.V.; Saadat, P.; Bobos, P.; Iskander, S.M.; Bodmer, N.S.; Rudnicki, M.; Kiyomoto, H.D.; Montezuma, T.; Almeida, M.O.; Bansal, R.; et al. Effectiveness and Safety of Intra-Articular Interventions for Knee and Hip Osteoarthritis Based on Large Randomized Trials: A Systematic Review and Network Meta-Analysis. Osteoarthritis Cartilage 2025, 33, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Voorn, M.J.J.; Boymans, T.A.E.J.; Köke, A.J.A.; de Mooij, M.A.C.; Rommers, C.G.M.; de Nooijer, J.; Goossens, M.J.E.B.; Huijnen, I.P.J.; Verbunt, J.A.M.C.F. Enhancing Collaboration and Integrated Vision on Health: Key Strategies for Addressing Knee Osteoarthritis. Int. J. Integr. Care 2025, 25, 28. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Sample screen of the Smart Delphi tool used to facilitate consensus in the Real-Time Delphi synchronous focus group.
Figure 1.
Sample screen of the Smart Delphi tool used to facilitate consensus in the Real-Time Delphi synchronous focus group.
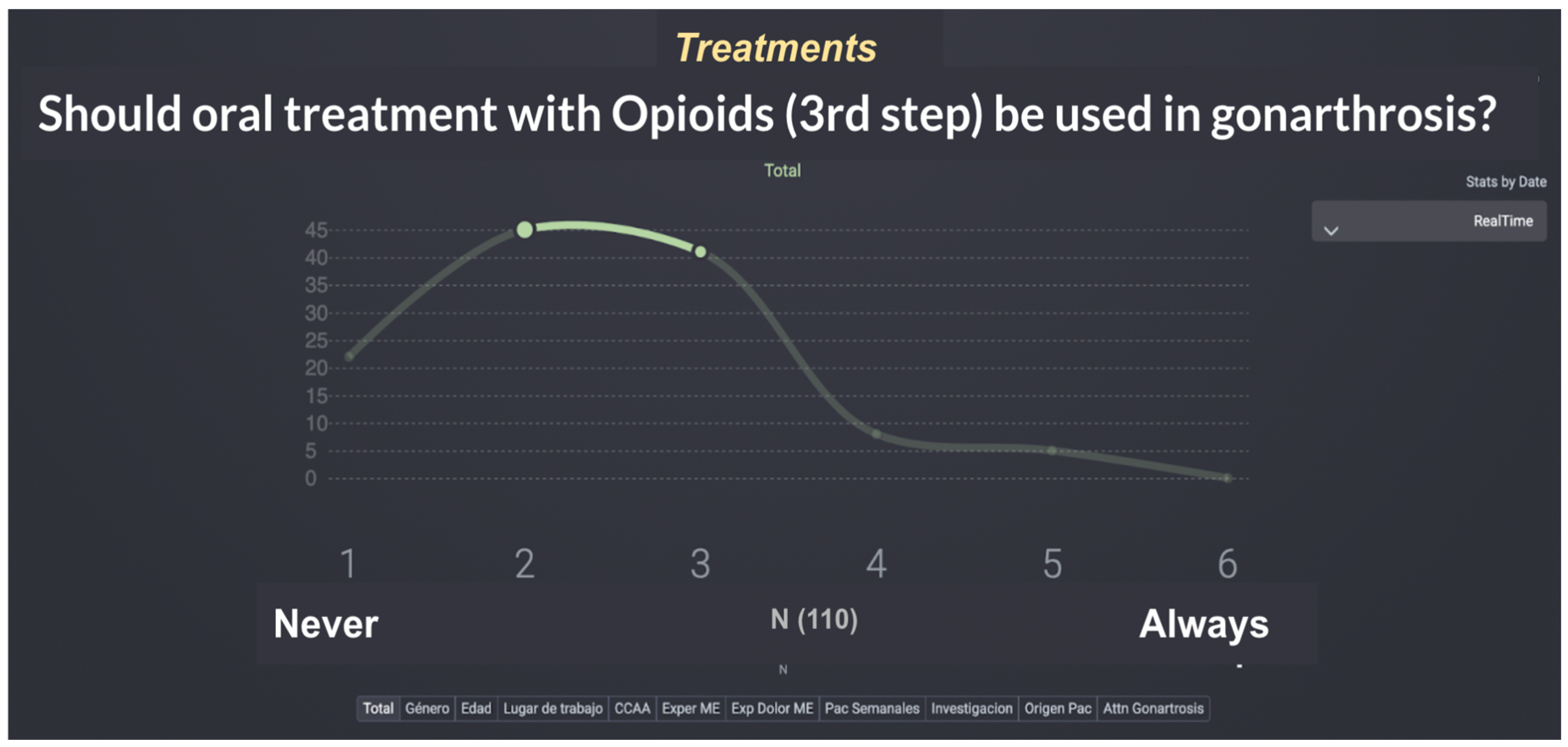
Figure 2.
Tasks done by the research team and participants in the two Delphi rounds.
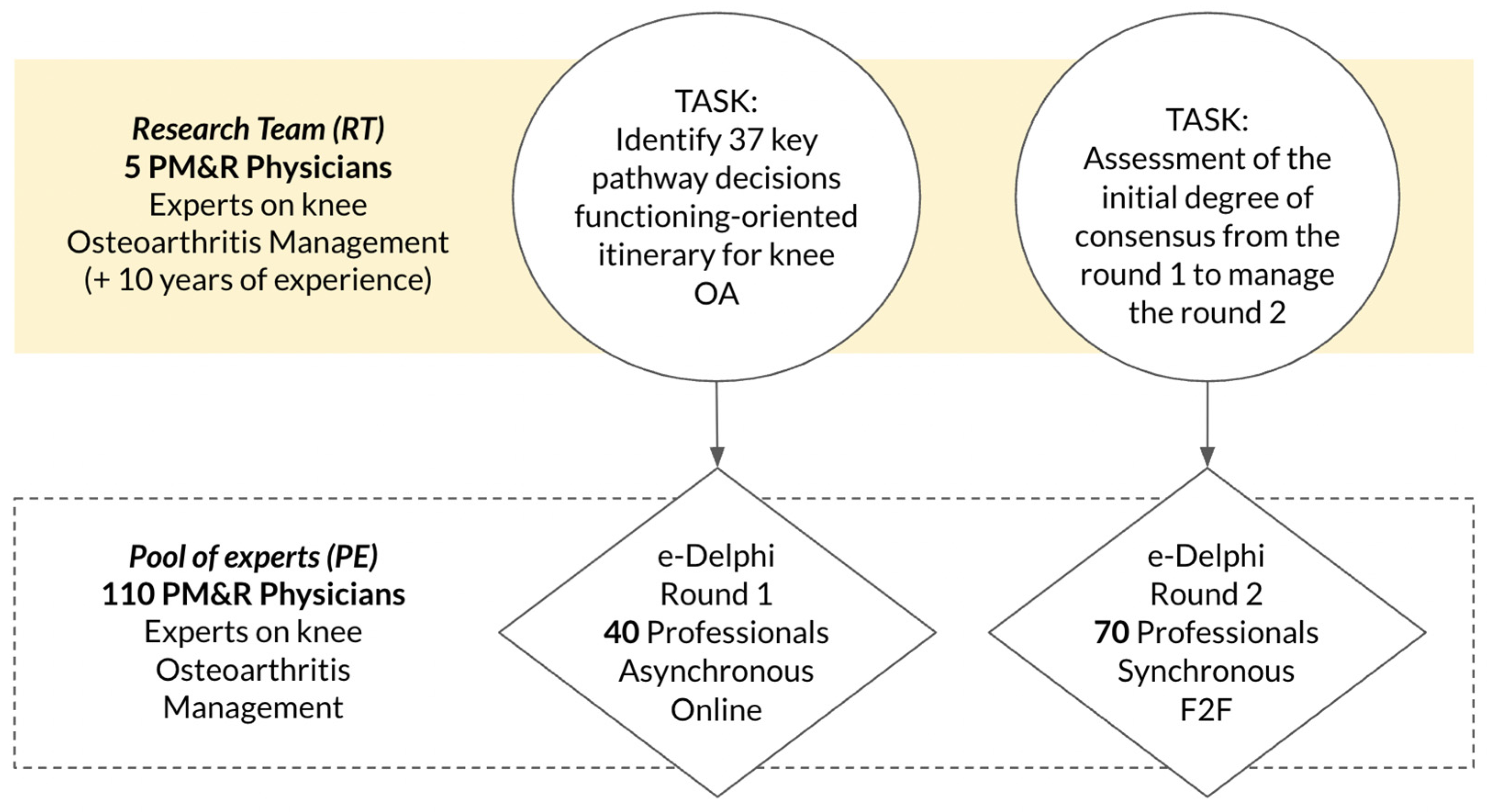
Figure 4.
PM&R-Led Care Pathway for Knee Osteoarthritis (KOA): Baseline Outcomes, Impairment Stratification, Multimodal Conservative Rehabilitation, and Escalation with Longitudinal Follow-Up.
Figure 4.
PM&R-Led Care Pathway for Knee Osteoarthritis (KOA): Baseline Outcomes, Impairment Stratification, Multimodal Conservative Rehabilitation, and Escalation with Longitudinal Follow-Up.
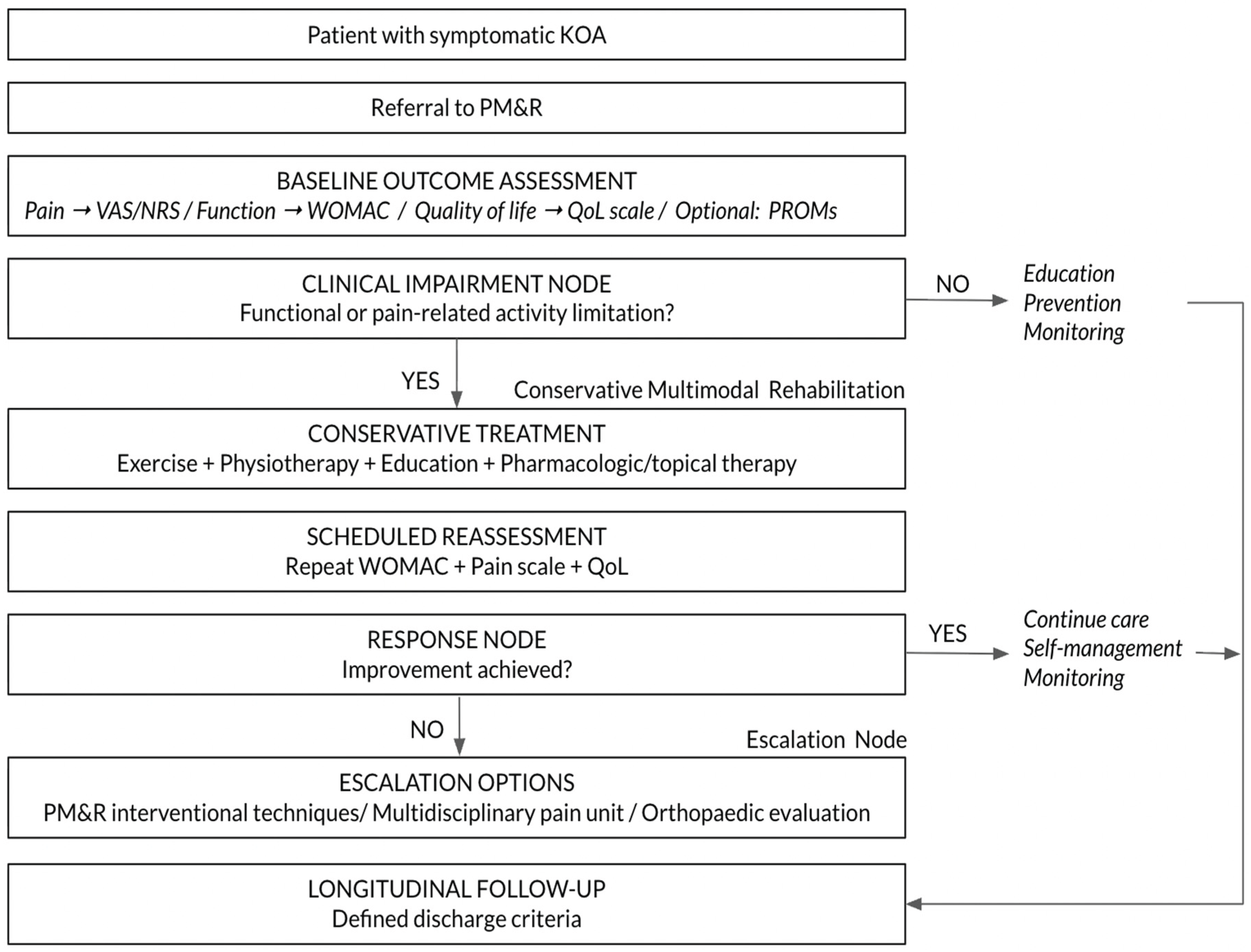
Table 1.
Demographic and Professional Characteristics of SERMEF PM&R Physicians Participating in Both Delphi Rounds.
Table 1.
Demographic and Professional Characteristics of SERMEF PM&R Physicians Participating in Both Delphi Rounds.
| Variable | Category | n | % |
| Sample | Complete respondents | 110 | 100 |
| Gender | |||
| Female | 71 | 64.0 | |
| Male | 39 | 35.1 | |
| Age group | |||
| 20–29 | 13 | 12.6 | |
| 30–39 | 24 | 21.6 | |
| 40–49 | 26 | 23.4 | |
| 50–59 | 31 | 27.9 | |
| 60–69 | 15 | 13.5 | |
| ≥70 | 1 | 0.9 | |
| Work setting | |||
| Tertiary / referral hospital | 57 | 51.4 | |
| Secondary hospital (~400 beds) | 30 | 27.0 | |
| General hospital (~200 beds) | 9 | 8.1 | |
| District hospital (~100 beds) | 9 | 8.1 | |
| Primary care | 2 | 2.7 | |
| Other | 3 | 2.7 | |
| Experience in musculoskeletal Rehabilitation. Medicine | |||
| <5 years | 7 | 7.2 | |
| 5–10 years | 19 | 17.1 | |
| 10–20 years | 38 | 34.2 | |
| >20 years | 46 | 41.4 | |
| Experience with interventional techniques for musculoskeletal pain management | |||
| <5 years | 13 | 12.6 | |
| 5–10 years | 27 | 24.3 | |
| 10–20 years | 43 | 38.7 | |
| >20 years | 27 | 24.3 | |
| Weekly number of patients with knee OA evaluated per physician | |||
| <20 | 15 | 14.4 | |
| 20–50 | 46 | 41.4 | |
| >50 | 49 | 44.1 | |
| Research involvement measured in publications during last 5 years | |||
| None | 35 | 32.4 | |
| <5 studies | 53 | 47.7 | |
| 5–30 studies | 15 | 13.5 | |
| >30 studies | 7 | 6.3 | |
| Where are your patients with knee osteoarthritis generally managed? | |||
| General rehabilitation clinic | 88 | 80.2 | |
| Multidisciplinary MSK pain unit | 16 | 14.4 | |
| Dedicated OA clinic | 1 | 0.9 | |
| Interventional clinic | 1 | 0.9 | |
| Other | 4 | 3.6 | |
Table 3.
Mapping of Delphi Items to the Operational Rehabilitation Pathway Model.
| Pathway Phase | Clinical Purpose | Delphi Items Supporting the Phase |
| Phase 1. Entry and Referral to PM&R | Defines how patients access rehabilitation care and where initial evaluation occurs | Q21 Referral from primary care or other physicians Q24 Evaluation in general rehabilitation outpatient clinic Q20 Possible referral from orthopaedics Q22 Possible referral from rheumatology |
| Phase 2. Functional and Outcome Assessment | Establishes baseline clinical status and enables follow-up comparison using validated outcome measures | Q32 Pain scale (VAS/NRS) Q33 WOMAC functional scale Q34 Quality of life scale Q31 Descriptive global status scale Q35 Subjective clinical and patient assessment Q36 PROMs |
| Phase 3. Conservative Multimodal Treatment | Defines first-line therapeutic management combining rehabilitation and supportive therapies | Q28 Multimodal treatment combining physical therapy and pharmacological/topical therapy Q27 Sequential organisation of treatment components |
| Phase 4. Escalation and Advanced Therapeutic Options | Defines when and how advanced treatments or specialist referrals are considered | Q30 Interventional techniques should not be first-line treatment Q26 Use of interventional techniques when escalation is required Q23 Possible management in multidisciplinary MSK pain unit Q25 Dedicated OA clinics as specialised care setting |
| Phase 5. Longitudinal Monitoring and Discharge | Defines follow-up strategy and criteria for completing rehabilitation care | Q37 Defined discharge criteria |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



