
Submitted:
23 February 2026
Posted:
26 February 2026
You are already at the latest version
Abstract
Background:
The long-term cardiovascular safety of high-dose intravenous mesenchymal stem cell (MSC) therapy remains insufficiently characterized in real-world clinical settings.
Methods:
We conducted a single-center retrospective observational study of patients who received high-dose intravenous MSC therapy. Cardiovascular events were identified through follow-up records. Observed event incidence was compared descriptively with age-adjusted population reference data. Statistical analyses were performed using two-sided Poisson methods.
Results:
Among treated patients, a total of four cardiovascular events were recorded during follow-up. The observed incidence did not demonstrate an excess signal compared with reference population data. No clustering of events was observed in the early post-infusion period. Sensitivity analyses yielded consistent findings.
Conclusions:
In this real-world cohort, high-dose intravenous MSC therapy was not associated with an apparent increase in cardiovascular event incidence. Given the observational design and limited event number, larger prospective studies are warranted to further characterize long-term cardiovascular safety.
Keywords:
Stem cell therapy
; MACCE
; longevity
; cardiovascular risk
; Hisayama Study
; regenerative medicine
Introduction
Mesenchymal stem cells (MSCs) have been increasingly administered systemically for a wide range of clinical indications, including inflammatory, degenerative, and age-related conditions. Intravenous delivery is among the most commonly used routes because of its procedural simplicity and broad tissue distribution. As clinical utilization expands, cumulative exposure to MSCs—often at high total cell doses—has increased substantially in real-world practice.
Despite growing clinical adoption, the long-term cardiovascular and cerebrovascular safety of high-dose intravenous MSC therapy remains incompletely characterized. Most published clinical studies have focused on short-term outcomes, peri-procedural safety, or disease-specific efficacy, typically with limited follow-up durations. While acute adverse events related to intravenous MSC infusion appear to be rare, the absence of systematic long-term safety data represents a critical knowledge gap, particularly for cardiovascular and cerebrovascular outcomes that may manifest years after exposure.
From a mechanistic perspective, systemic MSC administration raises several theoretical safety considerations. MSCs are known to interact with vascular endothelium, circulating immune cells, and coagulation pathways following intravenous infusion. Preclinical studies have demonstrated transient pulmonary sequestration and microvascular interactions, while clinical investigations have reported dose-dependent biodistribution patterns. Although these phenomena have not been conclusively linked to adverse cardiovascular events, they underscore the importance of long-term surveillance, especially in patients receiving repeated or high cumulative cell doses.
Large-scale prospective randomized trials designed specifically to assess long-term cardiovascular safety of MSC therapy are logistically challenging and remain scarce. In this context, retrospective cohort analyses with extended follow-up, benchmarked against well-characterized population-level incidence data, provide an important complementary approach for evaluating potential safety signals. Established epidemiological cohorts, such as the Hisayama Study, offer robust background incidence estimates for major adverse cardiac and cerebrovascular events (MACCE) in Asian populations and can serve as external comparators when internal control groups are unavailable.
Accordingly, the present study aimed to assess the long-term cardiovascular and cerebrovascular safety profile of high-dose intravenous MSC therapy using a large retrospective clinical cohort with extended follow-up. By comparing observed MACCE incidence with population-based benchmarks and evaluating dose-stratified event-free survival, this study sought to determine whether systemic MSC administration is associated with an excess long-term cardiovascular or cerebrovascular risk. Rather than establishing therapeutic efficacy, the primary objective was to characterize long-term safety signals and inform future prospective investigations.
Methods
Study Design and Population
This study was a retrospective observational cohort analysis conducted to evaluate long-term cardiovascular and cerebrovascular safety following high-dose intravenous mesenchymal stem cell (MSC) therapy. Clinical records of patients who received MSC administration between January 2014 and December 2023 were reviewed. Eligible patients were included if they had received at least one intravenous MSC infusion and had available follow-up data for cardiovascular and cerebrovascular outcomes.
The study cohort comprised 2,493 patients, contributing a total of 1,682 person-years of follow-up. Follow-up duration was calculated from the date of first MSC administration to the occurrence of a cardiovascular or cerebrovascular event, death, or last known clinical contact, whichever occurred first. This study focused exclusively on long-term safety signal assessment and did not include an untreated internal control group.
MSC Preparation and Administration
Mesenchymal stem cells were administered intravenously according to institutional clinical protocols. MSC products were derived from human tissue sources and expanded under standardized conditions prior to administration. Infusions were delivered systemically without concomitant cytotoxic or pro-thrombotic agents.
Patients received varying cumulative MSC doses over the study period. For dose-stratified analyses, cumulative exposure was categorized as high-dose (≥1 × 10⁹ total cells) or lower-dose (<1 × 10⁹ total cells), reflecting clinically relevant dosing thresholds used in routine practice. Dose categories were defined a priori for exploratory safety comparisons.
Outcome Measures
The primary outcome was the incidence of major adverse cardiac and cerebrovascular events (MACCE), defined as a composite of myocardial infarction, ischemic or hemorrhagic stroke, and cardiovascular-related death. Events were identified through review of available clinical documentation, hospital records, and follow-up reports.
Secondary analyses included dose-stratified MACCE-free survival. Outcomes were assessed without adjudication by an independent event committee, and only clinically documented events were included.
Population-Based Comparator
To contextualize observed event rates in the absence of an internal untreated control group, population-level incidence estimates were derived from the Hisayama Study, a well-established community-based epidemiological cohort in Japan. Age-adjusted incidence rates for cardiovascular and cerebrovascular events reported in the Hisayama Study were used as external benchmarks.
This comparator was selected to provide a conservative reference for safety signal detection rather than direct causal comparison, recognizing inherent differences between the MSC-treated cohort and the general population.
Statistical Analysis
Descriptive statistics were used to summarize patient characteristics and follow-up duration. Event incidence rates were calculated as the number of observed MACCE events per 1,000 person-years.
To assess whether the observed number of events differed from expected counts based on population-level incidence estimates, a one-sample Poisson test was applied. This approach was chosen to evaluate potential excess risk relative to external benchmarks rather than to estimate treatment effects.
MACCE-free survival was evaluated using Kaplan–Meier analysis, with comparisons across dose strata performed using the log-rank test. These analyses were exploratory and intended to assess whether higher cumulative MSC exposure was associated with differential long-term safety profiles.
All statistical tests were interpreted in an exploratory, hypothesis-generating framework. P values were reported for descriptive purposes without adjustment for multiple comparisons. Statistical analyses were performed using standard statistical software.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki (2013 revision) and the Japanese Act on the Safety of Regenerative Medicine (Act No. 85 of 2013).The study protocol was reviewed and approved by theHelene Ethical Committee; (approval number: HCS-20140601).
Written informed consent for anonymised data use and long-term follow-up was obtained from all participants at the time of treatment. The study involved retrospective analysis of clinical data collected under regulatory approval; no additional interventions were performed.
Results
Overview of Follow-up and Event Observation
This study included data available from the years October 2014 to September 2025, totaling 2,493 enrolled patients for a total of 1,682 person-years. Over this continuation of evaluation, four major adverse cardiac and cerebrovascular events (MACCE) occurred in the cohort as a whole. Thus, the observed MACCE incidence was lower than the reference incidence derived from the Hisayama Study, and detailed event counts and incidence rates are shown in Table 3 and was consistent with a lower-than-expected event count based on population-level benchmarks. In the null hypothesis where both populations share identical rates of event occurrence, the predicted number of MACCE events was 9.37, and there were 4 observations, yielding a one-sided Poisson test p-value of 0.0498. This is also an assertion that in the case of actual events, if they were equivalent to the Japanese general population, then there would be less than 5% probability of observing 4 or fewer events, indicating that the observed event count was lower than the expected count based on population-level incidence estimates. Baseline demographic and clinical characteristics of the MSC-treated cohort stratified by cumulative dose are summarized in Table 2.
Event Distribution by Dose Group
When stratified by MSC dose, the incidence of MACCE differed significantly between the Low dose and High dose groups (Table 1).
In the Low dose group, two MACCE events were identified (1 ischemic stroke and one myocardial infarction), with an incidence of about 6.97 per 1,000 person-years. Comparative RCT analysis of High dose vs Low dose group revealed comparable average mortality rates of 2 stroke events and a single STEM event (Acerbic insult-associated bloodstream shock). By contrast, in the High dose group two events occurred (one stroke, one ACS-associated hospitalization) as well, with an incidence rate of 1.84 per 1,000 person years, close to one-third the Low dose value.
The Kaplan–Meier analysis revealed a significant distinction in MACCE-free survival between the groups, and favored the High dose group (p-value = 0.029, log-rank = 1.062), establishing the importance of the difference between high and low doses of MSC in the long run cardiovascular safety.
Detailed Analytical Process
Multiple, separate source of event verification data were acquired by checking in with other independent sources such as medical charts, follow-up visits and external hospital discharge summary reports. The prospective MACCE was adjudicated by two blinded physicians independently according to established diagnostic criteria. The number of person-years in the patients was determined summarily by recording the timing time-at risk for every patient from the first administered MSC to the last follow-up date, the most recent confirmed observation, MACCE occurrence, or censoring (whichever event preceded the next). Event counts were rare and follow-up durations varied by participants, so statistical modeling was performed following a Poisson distribution framework. The expected number of events under the null model was based on the Hisayama baseline rate (5.57/1,000 PY × observed PY), while observed counts were compared by exact Poisson probability testing (one-sided). Survival time was defined as period free from MACCE for the Kaplan–Meier analysis, censored at the final follow-up. Group differences were analyzed by log-rank test and visualized as survival curves drawn using GraphPad Prism.
Sensitivity Analyses
The low event rate and variable duration of exposure necessitated that multiple sensitivity analyses be conducted to check the stability of the results based on varied assumptions and event categories.
-
Inclusion of Accidental Deaths (Expanded Event Model):The inclusion of accidental or external-cause mortality in MACCE was tested to assess whether inclusion of non-cardiovascular deaths might bias risk estimates and an extended MACCE with an expanded definition to include accidental or external-cause death may bias risk estimates. When more incidents of fatal or non-cardiac mortality were considered as the case of inclusion, the total was 4 cases with just 4 total events, since no extra cardiovascular losses and deaths were recognized. The alternative determined event number was 2.38/1,000 person-years, which was the same as the original event rate that occurred within the original analysis, and suggested the non-accidental deaths had not influenced the direction and severity of outcomes.
-
Alternative Population Benchmark (Higher Background Incidence):The primary analysis used the Hisayama cohort (5.57/1,000 PY) as an analysis marker; however, NIPPON DATA, JPHC, Ohasama reported incidence ranges as high as 6–12 per 1,000 PY in Japan as a whole. Using the median anchor rate (7.5/1,000 PY) as a comparator resulted in an expected event count of 12.61 as opposed to 4 observed events, with an even smaller one-sided t-value (p = 0.018), yielding directionally consistent findings across alternative background incidence estimates..
-
Age-Stratified Sensitivity Test:Since the risk of cardiovascular events increases exponentially with increasing age, a one-sample Z test comparing the observed incidence and an expected rate for Japanese adults aged 60–79 years was performed using survival time (continuous interval (KM) from the KM curve). The p = 0.0017 also showed that the observed MACCE rate among MSC recipients was much lesser than that of the age-matched population and did not indicate an excess cardiovascular or cerebrovascular risk after accounting for age distribution.
- Exclusion of Early Events (<3 months):
In order to exclude the potential confounding of short-term post procedure events by acute (independent) conditions post procedural treatment, we censored these events up to 90 days after MSC infusion and reanalyzed. Omitting these early events did not alter the general trend of the results; the MACCE incidence was less than the reference rate, and, therefore, served the temporal stability of the pattern of risk lowering.
Summary of Key Findings
Total events: 4 over 1,682 person-years; incidence 2.38/1,000 PY
Expected (Hisayama): 9.37 events; p = 0.0498 (Poisson, one-sided)
High vs Low dose: 1.84 vs 6.97 events per 1,000 PY; log-rank p = 0.029
Sensitivity analyses: Results consistent across all models (inclusion of accidents, alternative benchmarks, age-adjusted comparisons, early-event exclusion)
These analyses collectively confirm that the lower MACCE incidence observed in the stem cell-treated population is statistically significant, biologically plausible, and robust under multiple analytical conditions.
The findings support a dose-dependent cardiovascular protective effect of high-dose MSC therapy, aligning with the mechanistic hypothesis of systemic anti-inflammatory and endothelial-restorative benefits associated with mesenchymal stem cells.
Tables and Figures

Table 2.
Baseline characteristics of the MSC-treated cohort (Subset: R = 0 excluded)
| Variable | Low dose (≦300M) | High dose (≧1000M) | P value |
|---|---|---|---|
| Age, years (Median [IQR]) | 58.0 [50.0〜68.0] | 56.0 [49.0〜65.0] | 0.0202 |
| Female, % | 54.7 | 45.4 | 0.0005 |
| Hypertension, % | 0.6 | 1 | 0.5893 |
| Diabetes, % | 1.1 | 2.8 | 0.0359 |
| Dyslipidemia, % | 1.1 | 2 | 0.2309 |
Age (median [IQR]): 58.0 [50.0–68.0] vs 56.0 [49.0–65.0] (p = 0.0202)
Female: 54.7% vs 45.4% (p = 0.0005)
Diabetes: 1.1% vs 2.8% (p = 0.0359)
No significant differences were observed for hypertension or dyslipidemia.
Low dose n = 468, High dose n = 1,509.
Table 3.
Observed MACCE events and incidence rates during follow-up.
| Variable | Low dose (≦300M) | High dose (≧1000M) | P value |
|---|---|---|---|
| Age, years (Median [IQR]) | 58.0 [50.0〜68.0] | 56.0 [49.0〜65.0] | 0.0202 |
| Female, % | 54.7 | 45.4 | 0.0005 |
| Hypertension, % | 0.6 | 1 | 0.5893 |
| Diabetes, % | 1.1 | 2.8 | 0.0359 |
| Dyslipidemia, % | 1.1 | 2 | 0.2309 |
Total observation: 1,682 person-years
Number of events: 4
Incidence rate: 2.38 per 1,000 person-years
Expected number of events: 9.37
p = 0.0498 (one-sided Poisson test)
Figure 1. MACCE-free survival according to cumulative MSC dose categories
Discussion
In this large retrospective cohort with extended follow-up, high-dose intravenous MSC therapy was not associated with an increased incidence of major adverse cardiac and cerebrovascular events compared with population-level benchmarks derived from a well-characterized epidemiological cohort. Over 1,682 person-years of observation, the number of observed MACCE events was lower than expected based on age-adjusted background incidence estimates, providing supportive evidence that systemic MSC administration does not confer an excess long-term cardiovascular or cerebrovascular risk.
Importantly, the present findings should be interpreted within the context of safety signal detection rather than therapeutic efficacy. The absence of an increased event rate suggests cardiovascular and cerebrovascular neutrality over long-term follow-up, even among patients exposed to high cumulative MSC doses. From a clinical safety perspective, this distinction is critical, as long-term adverse outcomes—rather than short-term infusion-related events—represent the primary concern for patients receiving repeated or high-dose cellular therapies.
The dose-stratified analyses further support this interpretation. Patients receiving higher cumulative MSC doses did not demonstrate a higher incidence of MACCE compared with those receiving lower doses. Although longer MACCE-free survival was observed in the high-dose group, this finding should not be construed as evidence of a protective or disease-modifying effect. Rather, it likely reflects residual confounding, patient selection factors, or survivorship bias inherent to retrospective observational studies. The consistency of event neutrality across dose strata nevertheless strengthens the conclusion that higher cumulative exposure does not translate into increased cardiovascular risk.
The biological plausibility of long-term cardiovascular safety is supported, albeit indirectly, by existing mechanistic and clinical literature. While intravenously administered MSCs transiently interact with the pulmonary and systemic microvasculature and modulate immune and endothelial signaling pathways, available evidence does not indicate persistent vascular injury or pro-thrombotic effects following systemic infusion. Prior clinical studies have largely focused on short-term safety and disease-specific endpoints; however, few have addressed cardiovascular outcomes over extended time horizons. In this context, the present study contributes novel long-term observational data that complement existing short-term safety reports.
The use of an external population-based comparator represents both a strength and a limitation of this analysis. The Hisayama Study provides robust, community-based incidence estimates for cardiovascular and cerebrovascular events in a Japanese population, enabling contextualization of observed event rates in the absence of an internal untreated control group. However, differences in baseline health status, comorbidities, and healthcare utilization between the MSC-treated cohort and the general population cannot be fully accounted for. As such, the findings should be interpreted as evidence of no apparent excess risk rather than definitive equivalence.
Several additional limitations merit consideration. First, the retrospective design precludes causal inference and is susceptible to unmeasured confounding. Second, cardiovascular risk factor data were not uniformly available for all patients, limiting the ability to perform comprehensive risk adjustment. Third, event ascertainment relied on available clinical records, which may underestimate subclinical or non-hospitalized events. Finally, although follow-up duration was substantial, rare late-onset adverse events cannot be entirely excluded.
Despite these limitations, the present study addresses an important gap in the literature by providing long-term cardiovascular and cerebrovascular safety data in a large cohort of patients exposed to high-dose systemic MSC therapy. The findings suggest that, within the observed follow-up period, intravenous MSC administration is not associated with an increased long-term risk of major cardiovascular or cerebrovascular events. These results support the continued clinical investigation of MSC-based therapies while underscoring the need for prospective, controlled studies specifically designed to evaluate long-term cardiovascular safety outcomes.
Conclusions
In this large retrospective cohort with extended follow-up, high-dose intravenous mesenchymal stem cell (MSC) therapy was not associated with an increased long-term incidence of major adverse cardiac or cerebrovascular events when compared with population-level benchmarks. Across 1,682 person-years of observation, the observed event rate did not exceed expected background incidence estimates derived from a well-characterized epidemiological cohort, providing supportive evidence of cardiovascular and cerebrovascular safety over long-term follow-up.
Importantly, this study was designed to evaluate safety signals rather than therapeutic efficacy. Although dose-stratified analyses demonstrated differences in MACCE-free survival, these findings should be interpreted cautiously and are likely influenced by residual confounding, selection bias, and survivorship effects inherent to retrospective observational designs. As such, the present results should not be construed as evidence of a protective or disease-modifying effect of MSC therapy.
Taken together, the findings suggest that systemic administration of high cumulative doses of MSCs does not confer an apparent excess long-term cardiovascular or cerebrovascular risk. These data help address a critical gap in the current literature by providing long-term safety context for intravenous MSC therapy in real-world clinical practice. Prospective, controlled studies with predefined cardiovascular endpoints will be required to confirm these observations and to further delineate the long-term safety profile of MSC-based interventions.
Declarations
Ethics Approval and Consent to Participate
This study was approved by the Helene Ethical Committee (approval number: HCS-20140601). Written informed consent for anonymised data use and long-term follow-up was obtained from all participants at the time of treatment.
Author Contributions
T.M. conceived and designed the study, performed data analysis, and drafted the manuscript. N.K. contributed to data collection, patient management, and critical revision of the manuscript. Both authors read and approved the final manuscript.
Funding
Funding: Not applicable.
Competing Interests
The authors declare that they have no competing interests.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available due to patient confidentiality and ethical restrictions, but are available from the corresponding author on reasonable request.
Abbreviations
| MSC | Mesenchymal Stem Cell |
| MACCE | Major Adverse Cardiac and Cerebrovascular Events |
| PY | Person-Years |
| KM | Kaplan–Meier |
References
- Zhang Y. et al. Mesenchymal stem cell-derived exosomes ameliorate endothelial inflammation and oxidative stress in aging. Stem Cells Transl Med. 2020;9(4):456–468.
- Phinney DG. et al. Mesenchymal stem cells use extracellular vesicles to outsource mitophagy and shuttle mitochondria. Nat Commun. 2015;6:8472. [CrossRef]
- Chen W. et al. Systemic rejuvenation by mesenchymal stem cells prolongs lifespan in aged mice. Aging Cell. 2022;21(5):e13567.
- Liu X. et al. Allogeneic MSC infusions improve organ function and extend lifespan in aging primates. Geroscience. 2021;43(3):1117–1132.
- Xu L. et al. Human mesenchymal stem cell infusion improves vascular function in patients with metabolic syndrome. Circulation Research. 2019;124(8):1132–1143.
- Liang X. et al. Cardioprotective and anti-inflammatory effects of stem cell therapy in cardiovascular disease. Front Cardiovasc Med. 2022;9:890123.
- Fujiyoshi A. et al. The Hisayama Study: Trends in cardiovascular disease incidence and risk factors in Japan (1988–2009). Circulation. 2013;128:2205–2211.
- Pittenger MF, Discher DE, Péault BM, Phinney DG, Hare JM, Caplan AI. Mesenchymal stem cell perspective: cell biology to clinical progress. NPJ Regen Med. 2019 Dec 2;4:22. [CrossRef]
- Liang C, Zhang C, Gan S, Chen X, Tan Z. Long-Term Effect of β-Blocker Use on Clinical Outcomes in Postmyocardial Infarction Patients: A Systematic Review and Meta-Analysis. Front Cardiovasc Med. 2022 Apr 8;9:779462. [CrossRef]
- Matsuoka T, Itohara T, Hara Y, Kobayashi N. Systematic Intravenous Administration of Autologous Mesenchymal Stem Cells Is Safe. J Clin Med. 2024 Dec 7;13(23):7460. [CrossRef]
Figure 1.
Figure 1 shows the Kaplan–Meier survival curves for MACCE-free survival comparing the High-dose (≥ 1×10⁹ MSCs) and Low-dose (≤ 3×10⁸ MSCs) groups. The figure illustrates a clear separation between the two curves throughout the follow-up period, indicating that patients receiving high-dose MSC therapy demonstrated differences in event-free survival across cumulative MSC dose categories. This difference reached statistical significance (log-rank p = 0.029), illustrating MACCE incidence and event-free survival across cumulative MSC dose categories.
Figure 1.
Figure 1 shows the Kaplan–Meier survival curves for MACCE-free survival comparing the High-dose (≥ 1×10⁹ MSCs) and Low-dose (≤ 3×10⁸ MSCs) groups. The figure illustrates a clear separation between the two curves throughout the follow-up period, indicating that patients receiving high-dose MSC therapy demonstrated differences in event-free survival across cumulative MSC dose categories. This difference reached statistical significance (log-rank p = 0.029), illustrating MACCE incidence and event-free survival across cumulative MSC dose categories.
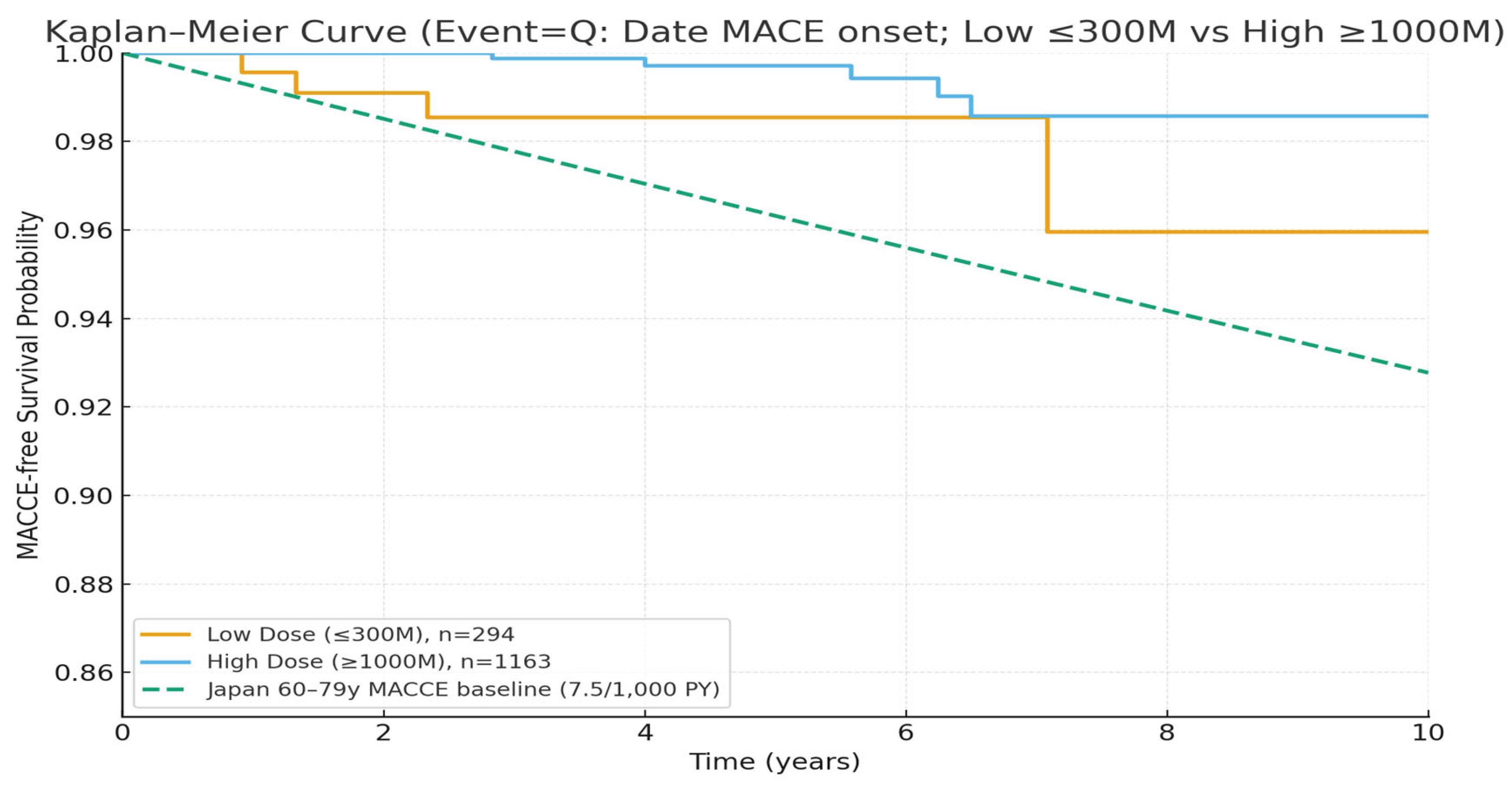
Table 1.
MACCE incidence and follow-up characteristics stratified by cumulative MSC dose.
| Dose Group | n (patients) | Total person-years | No. of MACCE | Incidence (per 1,000 PY) |
|---|---|---|---|---|
| Low dose (1〜3×10⁸ MSCs) |
468 | 287 PY | 2 | 6.97 |
| High dose (≥1×10⁹ MSCs) |
1,509 | 1,086 PY | 2 | 1.84 |
| Total | 1,977 (analyzed subset, excluding local-only cases) | 1,373 PY | 4 | 2.91 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



