Submitted:
24 February 2026
Posted:
26 February 2026
You are already at the latest version
Abstract
Background/Objectives:
Desmoid-type fibromatosis (DT) is a rare, locally aggressive soft tissue tumor with a frequently chronic course and substantial impact on health-related quality of life (HRQoL). While international studies have demonstrated considerable symptom burden and psychosocial impairment, data from Germany are lacking. This study aimed to assess HRQoL in German patients and to identify factors associated with HRQoL.
Methods:
In this cross-sectional analysis adult patients with histologically confirmed DT completed the EORTC QLQ-C30 and the disease-specific Desmoid-Type Fibromatosis Quality of Life Questionnaire (DTF-QoL). HRQoL scores were compared with reference data from the German general population, German sarcoma patients, and international DT cohorts. Sociodemographic, disease-, tumor-, and treatment-related factors associated with HRQoL were examined using multivariate linear regression analyses.
Results:
A total of 155 patients were included (69.7% female; mean age 45.0 years). Compared with the German general population, DT patients reported clinically relevant impairments in role, social, and emotional functioning and higher symptom burden, particularly pain, fatigue, and insomnia. Compared with sarcoma patients, DT patients showed better physical, role, and social functioning, while emotional functioning and symptom burden were largely comparable. German DT patients reported consistently worse HRQoL than Dutch/UK cohorts and moderately worse outcomes than Indian cohorts. Female gender, unemployment or disability pension, intensive multimodal treatment, multiple lines of systemic therapy, and tumor location in the lower extremities were independently associated with poorer HRQoL.
Conclusions:
DT is associated with sustained and clinically meaningful HRQoL impairment. HRQoL is driven primarily by psychosocial and treatment-related factors rather than disease duration, supporting the concept of DT as a chronic condition requiring long-term, multidisciplinary supportive care.
Keywords:
desmoid tumors
; health-related quality of life
; EORTC QLQ C30
; DTF QoL
1. Introduction
Desmoid-type fibromatosis (DT) is a rare, locally aggressive, and non-metastasizing soft tissue tumor that predominantly affects young adults, especially women. At the ICD-10 coding system DTs are classified with D48.1 (tumors of uncertain behavior). The disease is defined as a clonal fibroblastic proliferation that can arise in every part of the body with a significant subgroup arising at the site of prior trauma [1].
Two subgroups of the disease should be recognized particularly with respect to different morbidity features and co-morbidities. Sporadic desmoids develop due to a point mutation in the CTNNB1 gene coding for β-catenin [2,3], whereas patients with familial adenomatosis polyposis (FAP) suffer from FAP-associated Gardner syndrome. The latter group typically develops DTs at the mesentery after restorative colectomy and the mechanism is based on a mutation in the APC gene [4]. Due to its infiltrative growth, DT can cause considerable morbidity due to its infiltrative growth and high risk of local recurrence after surgery [5].
International studies have shown that DT patients experience a broad spectrum of symptoms and psychosocial challenges, including pain, fatigue, functional impairments, and fear of disease progression. These factors can substantially affect key domains of daily life, such as employment, family planning, and social participation [6,7]. However, systematic investigations of health-related quality of life (HRQoL) in DT remain scarce. The development of disease-specific instruments such as the Desmoid-Type Fibromatosis Quality of Life Questionnaire (DTF-QoL) [8] and the Global Desmoid Symptom Scale (GODDESS) [9,10] has enabled a more detailed assessment of symptom burden and functional limitations in this patient group.
Existing evidence indicates that DT patients report markedly lower HRQoL than the general population, with pronounced deficits in physical, role, and social functioning, and elevated levels of pain and fatigue [11,12]. Schut et al. (2022) demonstrated substantial symptom burden and reduced HRQoL among Dutch and United Kingdom (UK) DT patients [13], while Garg et al. (2022) reported similarly low HRQoL scores and high psychosocial distress in an Indian cohort of DT patients [14].
To date, no corresponding data are available from Germany. Against this background, the present study had two objectives:
(a) to evaluate HRQoL in German DT patients in context by comparing their outcomes with those of the general population, sarcoma patients, and international DT cohorts, and
(b) to identify sociodemographic and clinical factors associated with variations in HRQoL.
2. Methods
2.1. Study Design and Cohorts
This analysis uses cross-sectional data from the PROSa-DES study (Burden of Disease and Living Situation in Desmoid Patients) and the PROSa study (Burden and Medical Care of Sarcoma in Germany: Nationwide Cohort Study Focusing on Modifiable Determinants of Patient-Reported Outcome Measures in Sarcoma Patients).
PROSa-DES and PROSa were questionnaire-based, observational studies. In PROSa-DES, patients were recruited between November 2023 and June 2024. Desmoid-type fibromatosis (DT) patients included within the PROSa study were recruited between September 2017 and November 2020. The two datasets were combined for the present analysis, as recruitment of DT patients within the original PROSa framework had been interrupted by the COVID-19 pandemic.
Eligible participants were adults (≥ 18 years) with histologically confirmed sporadic desmoid-type fibromatosis, sufficient cognitive and linguistic ability to provide written informed consent, and the capacity to complete German study questionnaires. Patients with familial adenomatous polyposis (FAP)-associated DT were excluded.
The PROSa-DES study was approved by the Ethics Committee of the Technical University Dresden (EK489112023) and registered at ClinicalTrials.gov (NCT06258421). The PROSa study was approved by the Ethics Committee of the Technical University Dresden (EK1790422017) and registered at ClinicalTrials.gov (NCT03521531).
2.2. Data Collection and Variables
PROSa-DES participants were recruited through two pathways. a) Patients were identified from medical records at the University Hospital Mannheim. b) Additionally, patients were recruited via convenience sampling, using public calls for participation disseminated via the SOS Desmoid patient organization (sos-desmoid.de) and the German Sarcoma Foundation (sarkome.de).
In the PROSa study, participants were approached at one of 39 referral centers across Germany during outpatient visits, and in some cases by phone or letter [15].
In PROSa-DES, questionnaires were distributed, completed at home and returned by mail, whereas in PROSa they could be completed by mail or online. Clinical data were extracted from medical records for patients recruited through hospital sites. For participants enrolled via convenience sampling (PROSa-DES), relevant clinical information was obtained from recent physician letters submitted by the participants themselves or—after written consent—directly from the treating physicians.
2.3. Patient-Reported Outcomes
Health-related quality of life (HRQoL) was assessed using two validated instruments.
First, the European Organisation for Research and Treatment of Cancer Quality of Life Core Questionnaire (EORTC QLQ-C30) [16] was applied to measure global health status, functional domains (physical, role, emotional, cognitive, and social functioning), and symptom scales (e.g., pain, fatigue, nausea/vomiting).
Second, the Desmoid-Type Fibromatosis Quality of Life Questionnaire (DTF-QoL) [8], was used as a disease-specific measure, capturing desmoid-related symptoms across four symptom scales and the psychosocial impact across eleven impact scales.
Both instruments were scored according to their respective scoring manuals. Higher scores in global health status and functioning domains indicate better HRQoL, whereas higher scores in symptom or impact scales reflect greater symptom burden or psychosocial impairment.
2.4. Model Variables
Sociodemographic and clinical characteristics included age at diagnosis (18–35 / 36–55 / > 55 years; PROSa, PROSa-DES), gender (male / female / diverse; PROSa, PROSa-DES), employment status (employed / unemployed / disability pension / retirement pension / other; PROSa, PROSa-DES), and educational level (low / medium / high; PROSa, PROSa-DES).
Disease- and treatment-related variables comprised time since diagnosis (0–< 5 / 5–< 10 / > 10 years; PROSa, PROSa-DES), time since treatment (in treatment / 0–< 5 / 5–< 10 / > 10 years; PROSa-DES), number of systemic therapy lines (0–1 vs. ≥ 2; PROSa-DES), recurrence status (no / yes / no surgery; PROSa, PROSa-DES), received treatments (surgery only / systemic therapy only / chemotherapy + surgery / chemotherapy + surgery + radiotherapy / none [watch & wait] / other; simplified for regression: surgery ± systemic therapy / chemotherapy + surgery + radiotherapy / other; PROSa-DES), and tumor localization (lower extremity (incl. hip/pelvis)/ upper extremity (incl. shoulder)/ trunk / abdominal wall / intra-abdominal / head & neck / not defined or multifocal; PROSa, PROSa-DES).
2.5. Statistical Analysis
Descriptive statistics were calculated to characterize the study sample. Frequencies, proportions, means, and standard deviations (SD) were reported for all model variables. For each domain of the EORTC QLQ-C30 and the DTF-QoL, mean values and standard deviations were computed.
Mean scores were compared with reference data from four external sources:
(a) a German general population sample with reference data for the EORTC QLQ-C30 [17],
(b) a German sarcoma cohort from the PROSa study with EORTC QLQ-C30 data [18].
(c) a Dutch/UK desmoid tumor cohort with available data for both the DTF-QoL and the EORTC QLQ-C30 [13], and
(d) an Indian desmoid tumor cohort with EORTC QLQ-C30 data [14].
For visualization, radar plots were used to display functional and symptom scales (C30), while bar charts with error bars (mean ± SD) depicted DTF-QoL domains.
Univariate and multivariate linear regression analyses were conducted for all 15 QLQ-C30 and 14 DTF-QoL scales. The analysis of DTF-QoL scales was restricted to the PROSa-DES population. For univariate analyses associations between each HRQoL scale and independent variables (as defined above) were examined using t-tests or ANOVA for categorical predictors. Results of univariate analyses are presented in the supplementary n. For multivariate analyses variables with p < 0.10 in univariate testing were entered into generalized linear regression models. A backward selection procedure was applied, retaining variables with p < 0.20 in intermediate steps. All analyses were performed using IBM SPSS Statistics V.30 (Armonk, NY, USA). Due to the exploratory nature of the analysis no corrections for multiple testing were applied. A two-sided p-value < 0.05 was considered statistically significant.
3. Results
3.1. Patient Characteristics
A total of 155 participants were included in the combined analysis, comprising 109 patients from the PROSa-DES cohort (70.3%) and 46 patients from the PROSa cohort (29.7%).
The majority of participants were female (69.7%), with comparable proportions across cohorts (PROSa-DES 69.7%; PROSa 69.6%). The mean age of the total sample was 45.0 years (SD = 14.3), with 45.7 years (SD = 14.1) in PROSa-DES and 43.4 years (SD = 14.8) in PROSa.
Regarding disease duration, 41.6% of all participants had been diagnosed within the past 5 years (PROSa-DES 26.6%, PROSa 77.8%), 28.4% between 5 and 10 years, and 30.0% more than 10 years prior to the survey. The mean time since diagnosis was 7.9 years (SD = 6.4) overall, 9.5 years (SD = 6.1) in PROSa-DES, and 4.0 years (SD = 5.4) in PROSa.
Nearly two thirds of all participants had completed secondary education (62.3%), and 73.5% were employed at the time of survey (62.4%). The most frequent tumor locations were the lower extremities (31.0%) and the intra-abdominal region (23.2%). Further sociodemographic and clinical variables are provided in Table 1.
3.2. Quality of Life of Desmoid Patients in Context
To contextualize the HRQoL results, mean scores of the EORTC QLQ-C30 were compared with four reference populations: the German general population [17], German sarcoma patients [19], a Dutch/ UK DT cohort [13] and an Indian DT cohort [14] (Figure 1). Mean scores of the DTF-QoL sores were compared with the Dutch/ UK DT cohort [13] (Figure 2). Numeric results are presented in Supplementary Tables S1 and S2.
Compared to the German general population, global health status of DT patients was approximately 5 points lower. The largest differences in functional domains were observed in role, social, and emotional functioning (15–20 points below population norms). In the symptom scales, the most pronounced deviations were seen for pain, insomnia, and financial difficulties, with scores 10–15 points higher than population averages.
When compared with the German sarcoma cohort, desmoid patients reported slightly better global health (about 5 points higher), as well as higher physical, role, and social functioning (by 8–12 points). They were also less affected by dyspnea and appetite loss (≈9 points difference). Symptom burdens for fatigue, pain, and insomnia were largely comparable (differences ≤ 4 points).
Relative to the Dutch/UK desmoid cohort, German patients reported consistently higher burden and lower HRQoL, with differences of 15–23 points in role, social, and emotional functioning as well as global health, and of 10–17 points in fatigue, pain, insomnia, and financial difficulties.
Compared with the Indian desmoid cohort, German patients also showed higher impairments, although differences were less pronounced. HRQoL was particularly reduced in role, social, cognitive, and emotional functioning (7–11 points difference). Regarding symptoms, German patients reported markedly higher insomnia (17 points), and higher fatigue and dyspnea (9–10 points). In contrast, Indian patients experienced greater financial difficulties (9 points higher).
On the disease-specific level, DTF-QoL scores of German patients were higher across all domains, indicating greater burden. The most pronounced differences (≥ 20 points) were found for parenting and fertility (31 points), concerns about condition (23 points), and diagnostic and treatment trajectory (23 points).
3.3. Factors Associated with HRQoL
Results of the univariate analyses for all model variables and HRQoL domains (EORTC QLQ-C30 and DTF-QoL) are presented in the Supplementary Tables S1 and S2. Factors with p < 0.1 in univariate testing were included in the generalized linear regression models. Multivariate results are summarized in Table 2 (DTF-QoL) and Table 3 (EORTC QLQ-C30).
3.4. Sociodemographic Factors
Gender. Male participants reported a consistently lower burden and better HRQoL than female participants across almost all DTF-QoL domains. The largest differences were observed in parenting and fertility (B = −26.6, p < 0.001), effect on relationships (B = −19.2, p < 0.001), doctor–patient relationship (B = −17.6, p < 0.001), supportive care (B = −16.3, p < 0.001), and pain/discomfort (B = −15.7, p < 0.001). Similarly, on the EORTC QLQ-C30, men reported significantly better physical functioning (B = 13.1, p < 0.001) and emotional functioning (B = 16.2, p < 0.001), experienced less pain (B = −23.2, p < 0.001), and indicated a higher global HRQoL (B = 12.4, p < 0.01).
Age. Younger participants (< 35 years) showed higher burden in nausea/vomiting (B = −6.1, p = 0.01 for 36–55 years; B = −12.6, p < 0.001 for > 55 years) and parenting and fertility (B = −43.2, p < 0.001 for 36–55 years).
Education. No significant associations were observed between educational level and HRQoL in either the EORTC QLQ-C30 or the DTF-QoL domains.
Employment status. Involuntarily unemployed participants, including those receiving a disability pension, reported a substantially higher burden across multiple DTF domains compared to employed individuals. The most prominent differences were found in job and education (B = 44.5, p < 0.001), emotional consequences (B = 26.7, p < 0.001), physical consequences (B = 26.0, p < 0.001), and effect on relationships (B = 25.4, p < 0.001).Consistent with these findings, unemployed participants also demonstrated significantly lower HRQoL in the EORTC QLQ-C30, with reductions across 13 of 15 domains. Marked differences were observed in physical (B = −27.4, p < 0.001), role (B = −33.0, p < 0.001), emotional (B = −23.8, p < 0.001), social functioning (B = −40.3, p < 0.001), and global HRQoL (B = −25.3, p < 0.001). In addition, they reported significantly higher symptom burden, particularly for fatigue (B = 31.8, p < 0.001), insomnia (B = 39.6, p < 0.001), and financial difficulties (B = 48.5, p < 0.001).
3.5. Factors Related to the Course of Disease
In the DTF-QoL, time since treatment showed no significant associations with any of the assessed domains. For time since diagnosis, higher burden in physical consequences was observed 5–10 years after diagnosis compared with patients diagnosed within the past 0–5 years (B = 11.5, p = 0.03).
In the EORTC QLQ-C30, participants with more than 10 years since treatment reported better cognitive functioning (B = 20.0, p = 0.02) and lower fatigue (B = −17.9, p = 0.04). Similarly, insomnia was less pronounced among participants diagnosed more than 10 years prior (B = −12.2, p = 0.03) compared with those diagnosed within the past 0–5 years.
Patients with a tumor recurrence reported lower burden in supportive care (B = −11.4, p = 0.03) compared with those without recurrence.
3.6. Treatment Related Factors
Patients who had received surgery, systemic therapy, and radiotherapy reported significantly higher burden in several DTF-QoL domains compared to those treated with surgery alone and/or systemic therapy. The most affected domains were physical consequences (B = 11.9, p = 0.02), physical limitations (B = 11.8, p = 0.02), and treatment-related concerns (B = 11.5, p = 0.03).
In the EORTC QLQ-C30, this group also demonstrated lower physical functioning (B = −15.3, p < 0.001), lower global HRQoL (B = −9.6, p = 0.02), and higher pain scores (B = 13.9, p = 0.04).
Similarly, participants who had undergone two or more lines of systemic therapy reported greater pain/discomfort (B = 19.0, p < 0.01), higher impact on body image (B = 15.3, p < 0.01), and more pronounced diarrhea (B = 13.4, p = 0.04) than those who had received one or no prior line of systemic therapy.
3.7. Tumor Related Factors
Patients with tumors of the lower extremities reported the highest burden across several HRQoL domains. Compared with this reference group, participants with tumors located in the upper extremities (B = −17.2, p = 0.02), trunk (B = −13.0, p = 0.02), abdominal wall (B = −16.0, p < 0.01), and head and neck region (B = −18.2, p = 0.02) showed significantly lower physical consequences in the DTF-QoL. The domain parenting and fertility was less affected in patients with upper extremity tumors (B = −46.5, p < 0.01). Lower treatment-related concerns were also observed in tumors of the upper extremities (B = −24.3, p < 0.01), abdominal wall (B = −14.1, p = 0.02), and head and neck (B = −26.6, p < 0.01).
In the EORTC QLQ-C30, participants with tumors in the trunk (B = 12.8, p = 0.01) and abdominal wall (B = 11.4, p = 0.03) reported better physical functioning compared to those with tumors in the lower extremities.
4. Discussion
This study provides the first comprehensive assessment of health-related quality of life (HRQoL) in German patients with sporadic desmoid-type fibromatosis using both the disease-specific DTF-QoL and the generic EORTC QLQ-C30. By combining data from the PROSa-DES and PROSa cohorts, it offers a contextualized view of symptom burden, functioning, and psychosocial impact in a national sample of DT patients.
4.1. Quality of Life in Context
Compared with the German general population, DT patients showed substantial and clinically relevant impairments, particularly in role, social, and emotional functioning, as well as higher levels of pain, fatigue, and insomnia. The observed mean differences correspond to moderate to large effect sizes, indicating significant decrements in patient-perceived health status [20].
When compared with sarcoma patients, German DT patients reported higher scores in physical, role, and social functioning with differences exceeding the threshold for clinical relevance on the EORTC QLQ-C30 scales [20]. In contrast, emotional functioning and global health status were comparable between groups, suggesting that emotional well-being remains similarly affected in both DTF and malignant sarcoma populations. Likewise, pain, fatigue, and insomnia scores were largely comparable, indicating that symptom burden can reach malignant-like levels despite the benign histology of DT. Taken together, these findings illustrate that while DT patients experience better role and social participation than sarcoma patients, their emotional as well as aspects of their symptomatic burden remains clinically significant and largely unmitigated by the benign nature of the disease. Consistent with previous reports, chronic pain and fatigue are among the most frequent and distressing symptoms in DT, often persisting long after active treatment and substantially affecting sleep and daily functioning [13,14,21,22,23,24].
Notably, when compared with Dutch/UK DT cohorts, German patients showed large and clinically meaningful differences in several EORTC QLQ-C30 domains—particularly role, emotional, and social functioning—as well as a higher burden of fatigue, pain, and insomnia. Similarly, scores on the DTF-QoL were consistently worse in the German cohort, most prominently in the domains parenting and fertility, concerns about condition, and diagnostic and treatment trajectory. Comparisons with the Indian DT-cohort revealed the same direction of effects, though differences were generally less pronounced.
A comparable pattern can be seen in European normative data reported by Nolte et al. [17], where the German general population scored lower in global health and emotional functioning than respondents from The Netherlands. When comparing the PROSa results with those of the Dutch SURVSARC study [25], German patients showed lower physical, role, and social functioning and higher levels of fatigue and pain. Beyond differences in healthcare organization, these cross-national variations may also reflect cultural differences in health perception and response behavior [26].
Additionally, the treatment history differed substantially between the Dutch/ UK cohort and the German patients. In the Dutch/ UK cohort, over a Third of patients were managed with active surveillance only, compared with less than 10% in the present cohort. The proportion of patients receiving drug therapy was comparable, whereas surgery had been performed far more frequently in the German cohort (67% vs. 27%) [13]. This more intensive treatment history likely reflects longer disease duration and surgical management during periods when active surveillance was not yet established as a reasonable initial strategy. Consequently, patients may have been exposed to more extensive information about potential complications and side effects, which could contribute to heightened concern and distress compared with an approach that begins with observation and reserves treatment for disease progression.
The observed disparities are therefore likely multifactorial, shaped by differences in healthcare structures, treatment strategies, social support systems, and cultural interpretations of quality-of-life constructs, rather than being solely attributable to disease-specific mechanisms.
4.2. Determinants of HRQoL
4.2.1. Gender
Gender consistently emerged as a key determinant of HRQoL in desmoid-type fibromatosis. Across both generic and disease-specific measures, women reported lower functioning and higher symptom burden than men, confirming findings from previous DT- [13,22,27], and broader oncology research [28]. They are probably attributed to a complex interplay of biological, psychological, and sociocultural factors—such as hormonal influences, greater emotional expressiveness, higher body-image sensitivity, and differing coping styles. The patterns suggest that female patients represent a particularly vulnerable group in whom targeted psycho-oncological and social support interventions may be especially beneficial.
4.2.2. Employment Status
Employment status was another strong and consistent predictor of HRQoL. Patients who were unemployed or receiving disability pensions reported substantially poorer functioning and higher symptom burden than those in active employment. This observation aligns with previous evidence from the PROSa study [29]. Similar patterns have been observed elsewhere, where work participation is closely associated to improved HRQoL outcomes [30,31]. Beyond a better financial stability, employment provides structure and a can create sense of purpose all of which contribute to psychological well-being and resilience. Loss of work or occupational disability may intensify fatigue, anxiety, and social withdrawal. These findings highlight the importance of early vocational counseling and workplace reintegration programs as key components of care for DT patients.
4.3. Disease-Related Factors
The duration since diagnosis or treatment showed only limited associations with HRQoL, suggesting that time since treatment nor time since diagnosis are not always reliable predictors of recovery. Improvements were reported in fatigue, cognitive functioning, and insomnia, while HRQoL in most other domains remained stable over time rather than showing continuous improvement. In contrast, the highest burden of physical consequences was reported 5–10 years after diagnosis, indicating a prolonged impact of the disease on daily life. These findings are consistent with previous research in DT [13], which similarly observed persistent functional and psychosocial burden even many years after diagnosis. The observed inconsistent time effects indicate that DT behaves as a chronic condition with enduring physical and emotional consequences, rather than a disease from which patients fully recover once treatment ends. This chronicity may reflect both the hardly predictable clinical course—with repeated recurrences and prolonged surveillance—and sustained psychological processes such as fear of progression or adaptation fatigue. Consequently, long-term care for DT patients should not rely solely on time as a healing factor but include ongoing monitoring, symptom management, and psychosocial support to address persistent challenges in daily life.
4.4. Treatment-Related Factors
Treatment modality and intensity emerged as important determinants of HRQoL. Patients who had received combined local and systemic therapies—particularly multimodal regimens involving surgery, radiotherapy, and systemic treatment—reported lower physical functioning and global QoL, together with higher levels of pain and treatment-related concerns. These results mirror findings from previous DT studies showing that treatment intensity and invasiveness are among the strongest contributors to long-term symptom burden [13]. Repeated or multimodal interventions may amplify pain, fatigue, and fear of recurrence, while also affecting body image and social participation.
Similarly, patients who underwent multiple lines of systemic therapy experienced greater discomfort and poorer body image, consistent with cumulative treatment-related toxicity and the psychological toll of repeated therapeutic failure [32]. Such associations emphasize that even in a disease managed with curative intent, the cost of achieving local control can be substantial in terms of long-term quality of life. Despite worldwide consensus and prospective randomized trials [24,33,34,35] there was no registered drug available until very recently (Nirogacestat, and Sorafenib in Germany since August 2024 by GBA allowance). This might also contribute to the level of anxiety about whether access to therapy will be available once required by disease progression
4.5. Tumor Location
Tumor site was another relevant determinant of HRQoL. Patients with tumors of the lower extremities reported the highest functional limitations and physical consequences, whereas those with lesions of the trunk, abdominal wall, or head and neck experienced comparatively better functioning and less treatment-related concern. Similar patterns have been observed in studies on both DT and sarcoma populations [13,15,18]. These findings underline that HRQoL in DT is not only determined by tumor biology but also by the functional and psychosocial context of the tumor`s anatomical location, suggesting that rehabilitation and psychosocial support should be tailored accordingly.
Overall, HRQoL in DT is influenced by multiple interacting factors rather than by disease activity alone. Female gender and unemployment consistently predicted lower HRQoL, reflecting psychosocial vulnerability and the stabilizing role of work participation. Intensive or multimodal treatment was linked to persistent physical and symptomatic burden, while time since diagnosis or treatment showed little improvement over time, pointing to the chronic nature of the disease. Tumor site, particularly lesions of the lower extremities, added further heterogeneity through mobility restrictions and body image concerns. Together, these findings emphasize that HRQoL in DT patients is shaped by both medical and psychosocial dimensions, requiring integrated long-term care that supports physical recovery and emotional adaptation alike.
4.6. Clinical and Psychosocial Implications
The results underline that desmoid-type fibromatosis requires a chronic-care perspective rather than short-term oncological follow-up. Persistent pain, fatigue, and emotional distress call for structured long-term programs that integrate symptom control, psychological support, and physical rehabilitation. Given the strong influence of gender and employment status, interventions should include gender-sensitive counseling and vocational reintegration support. Routine assessment of HRQoL with instruments such as the DTF-QoL or EORTC QLQ-C30 can help identify patients at risk for long-term distress and guide individualized supportive care. Overall, multidisciplinary coordination between oncology, psycho-oncology, and rehabilitation services is essential to sustain quality of life beyond tumor management.
4.7. Strengths and Limitations
Major strengths of this study include the comparatively large DT cohort, the use of both generic and disease-specific HRQoL instruments, and the integration of reference data from sarcoma and international DT populations. These features provide a broad contextual understanding of quality of life in this rare disease. However, the cross-sectional design limits causal interpretation. Recruitment through patient organizations could have led to selection bias toward more engaged or long-term survivors. Likewise, most hospital-based participants were recruited from a single specialized center, which may limit representativeness. A further potential source of bias concerns educational level, as patients with higher education are typically overrepresented in observational studies of this kind. Moreover, when comparing our DTF cohort with external datasets, standardization for sex and gender was not possible, which may have influenced between-cohort comparisons. Finally, because the majority of participants were long-term patients, recent therapeutic developments—such as the growing use of active surveillance strategies—are not fully reflected in this dataset.
5. Conclusions
Desmoid-type fibromatosis causes a sustained reduction in health-related quality of life, in some aspects comparable in magnitude to that of malignant sarcomas. HRQoL is determined not by disease activity alone, but by psychosocial and treatment-related factors—particularly gender, employment status, treatment intensity, and tumor site. As improvements over time remain limited, DT should be regarded as a chronic condition requiring long-term, multidisciplinary care. Integrating routine HRQoL assessment and individualized support into clinical follow-up can help preserve functioning and well-being in this rare tumor population.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Factors associated with the DTF QoL Scales. Univariate analyses. p= p-value. SD= standard deviation. ST= systemic therapy. RT= radio therapy. *Included in multivariable model. **T-test. ***Anova. Significant differences bold. Table 2: Factors associated with Scales of the EORTC QLQ-C30. Univariate analyses. p= p-value. SD= standard deviation. ST= systemic therapy. RT= radio therapy. PF= physical functioning. RF= role functioning. EF= emotional functioning. CF= cognitive functioning. SF= social functioning. FD= financial difficulties. *Included in multivariable model. **T-test. ***Anova. Significant differences bold.
Author Contributions
ME, RH and PH were jointly involved in the project conceptualization of PROSa-DES. ME wrote the first draft and analyzed the data. RH served as project coordinator during the data acquisition phase of PROSa-DES. CB supervised the project from a patient’s perspective. PH, JJ, BK, SR, DP, RG were responsible for patients’ recruitment at their respective centers. JS and MKS served as PIs of the PROSa study. All authors were involved in the investigation, validation, reviewing, and editing of the manuscript.
Funding
The PROSa-DES study received a grant by the patient advocacy group SOS-desmoid e.V., Mannheim, Germany and support by the Desmoid Tumor Research Foundation (DTRF), Woodcliff Lake, NJ 07677, USA.
Conflicts of Interest
BK has an advisory role for Ayala, Bayer, Boehringer Ingelheim, Deciphera, Parabilis Medicines, PharmaMar, SpringWorks Therapeutics and receives research funding from Cogent, Immunome, PharmaMar, SpringWorks Therapeutics. DP reports grants/research supports (institutional fees) from: Boehringer Ingelheim, BMS, PharmaMar, Recordati, Deciphera, Lilly, Roche, Blueprint Medicines (all outside the submitted work), honoraria or consultation fees (institutional fees) from Boehringer Ingelheim, PharmaMar, Roche, Springworks, AstraZeneca (all outside the submitted work), institutional fees for participation in a company sponsored speaker’s bureau from: Boehringer Ingelheim, PharmaMar, Blueprint Medicines, Springworks (all outside the submitted work). Unrelated to this study, JS reports institutional grants for investigator-initiated research from the German Federal Joint Committee, German Ministry of Health, German Ministry of Research, European Union, German Federal State of Saxony, Novartis, Sanofi, ALK, and Pfizer. He participated in advisory board meetings as a paid consultant for Sanofi, Lilly, and ALK. All other authors have no competing interests associated with this work.
AI Disclosure Statement
Generative artificial intelligence (ChatGPT-5.0, OpenAI, 2025) was used only to improve language clarity and readability. No AI tools were used for data collection, analysis, or interpretation. All AI-assisted edits were reviewed and verified by the authors to ensure accuracy and integrity.
References
- Hohenberger, P.; Menge, F.; Hohenberger, R.; Kasper, B.; Marx, A.; Haller, F.; Baumgarten, C.; Wardelmann, E.; Jakob, J. Trauma and Sporadic Desmoid Tumor Development: An Approach toward Real Incidence and Aspects of Causality. Cancer 2024, 130, 51–59. [Google Scholar] [CrossRef]
- Lazar, A.J.F.; Tuvin, D.; Hajibashi, S.; Habeeb, S.; Bolshakov, S.; Mayordomo-Aranda, E.; Warneke, C.L.; Lopez-Terrada, D.; Pollock, R.E.; Lev, D. Specific Mutations in the Beta-Catenin Gene (CTNNB1) Correlate with Local Recurrence in Sporadic Desmoid Tumors. Am J Pathol 2008, 173, 1518–1527. [Google Scholar] [CrossRef]
- Trautmann, M.; Rehkämper, J.; Gevensleben, H.; Becker, J.; Wardelmann, E.; Hartmann, W.; Grünewald, I.; Huss, S. Novel Pathogenic Alterations in Pediatric and Adult Desmoid-Type Fibromatosis – A Systematic Analysis of 204 Cases. Sci Rep 2020, 10, 3368. [Google Scholar] [CrossRef] [PubMed]
- Schiessling, S.; Kihm, M.; Ganschow, P.; Kadmon, G.; Büchler, M.W.; Kadmon, M. Desmoid Tumour Biology in Patients with Familial Adenomatous Polyposis Coli. Br J Surg 2013, 100, 694–703. [Google Scholar] [CrossRef] [PubMed]
- Rosa, A.A.; Carolina, A.P.; Marta, A.V.; Francisco, A.; Adriana, F.G.; Natalia, G.; Pablo, L.L.; Cristina, M.F.; Lidia, M.S.; Ulrike, N.; et al. Desmoid Tumors—Experience from a Referral Center, Part 1: Multidisciplinary Review and Practical Recommendations. Cancers 2025, 17, 3470. [Google Scholar] [CrossRef] [PubMed]
- Alman, B.; Attia, S.; Baumgarten, C.; Benson, C.; Blay, J.-Y.; Bonvalot, S.; Breuing, J.; Cardona, K.; Casali, P.G.; Van Coevorden, F.; et al. The Management of Desmoid Tumours: A Joint Global Consensus-Based Guideline Approach for Adult and Paediatric Patients. European Journal of Cancer 2020, 127, 96–107. [Google Scholar] [CrossRef]
- Kasper, B.; Raut, C.P.; Gronchi, A. Desmoid Tumors: To Treat or Not to Treat, That Is the Question. Cancer 2020, 126, 5213–5221. [Google Scholar] [CrossRef]
- Schut, A.-R.W.; Lidington, E.; Timbergen, M.J.M.; Younger, E.; van der Graaf, W.T.A.; van Houdt, W.J.; Bonenkamp, J.J.; Jones, R.L.; Grünhagen, D.J.; Sleijfer, S.; et al. Development of a Disease-Specific Health-Related Quality of Life Questionnaire (DTF-QoL) for Patients with Desmoid-Type Fibromatosis. Cancers (Basel) 2022, 14, 709. [Google Scholar] [CrossRef]
- Gounder, M.M.; Maddux, L.; Paty, J.; Atkinson, T.M. Prospective Development of a Patient-reported Outcomes Instrument for Desmoid Tumors or Aggressive Fibromatosis. Cancer 2020, 126, 531–539. [Google Scholar] [CrossRef]
- Gounder, M.M.; Atkinson, T.M.; Bell, T.; Daskalopoulou, C.; Griffiths, P.; Martindale, M.; Smith, L.M.; Lim, A. GOunder/Desmoid Tumor Research Foundation DEsmoid Symptom/Impact Scale (GODDESS©): Psychometric Properties and Clinically Meaningful Thresholds as Assessed in the Phase 3 DeFi Randomized Controlled Clinical Trial. Qual Life Res 2023, 32, 2861–2873. [Google Scholar] [CrossRef]
- Timbergen, M.J.M.; van der Graaf, W.T.A.; Grünhagen, D.J.; Younger, E.; Sleijfer, S.; Dunlop, A.; Dean, L.; Verhoef, C.; van de Poll-Franse, L.V.; Husson, O. Assessing the Desmoid-Type Fibromatosis Patients’ Voice: Comparison of Health-Related Quality of Life Experiences from Patients of Two Countries. Sarcoma 2020, 2020, 2141939. [Google Scholar] [CrossRef] [PubMed]
- Schut, A.-R.W.; de Bruin, L.E.; de Rooij, B.H.; Lidington, E.; Timbergen, M.J.M.; van der Graaf, W.T.A.; van Houdt, W.J.; Bonenkamp, J.J.; Jones, R.L.; Grünhagen, Dirk.J.; et al. Physical Symptom Burden in Patients with Desmoid-Type Fibromatosis and Its Impact on Health-Related Quality of Life and Healthcare Use. Cancer Medicine 2023, 12, 13661–13674. [Google Scholar] [CrossRef] [PubMed]
- Schut, A.-R.W.; Lidington, E.; Timbergen, M.J.M.; Younger, E.; van der Graaf, W.T.A.; van Houdt, W.J.; Bonenkamp, J.J.; Jones, R.L.; Grünhagen, D.J.; Sleijfer, S.; et al. Unraveling Desmoid-Type Fibromatosis-Specific Health-Related Quality of Life: Who Is at Risk for Poor Outcomes. Cancers (Basel) 2022, 14, 2979. [Google Scholar] [CrossRef] [PubMed]
- Garg, V.; Rastogi, S.; Kalra, K.; Bhoriwal, S.; Barwad, A.; Dhamija, E.; Upadhyay, A.; Gamangatti, S. Health-Related Quality of Life (HRQoL), Anxiety, and Depression in Patients with Desmoid Type Fibromatosis. Support Care Cancer 2022, 30, 10089–10098. [Google Scholar] [CrossRef]
- Eichler, M.; Hentschel, L.; Singer, S.; Hornemann, B.; Richter, S.; Hofbauer, C.; Hohenberger, P.; Kasper, B.; Andreou, D.; Pink, D.; et al. Health Related Quality of Life over Time in German Sarcoma Patients. An Analysis of Associated Factors - Results of the PROSa Study. Frontiers in Endocrinology 2023, 14. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Nolte, S.; Liegl, G.; Petersen, M.A.; Aaronson, N.K.; Costantini, A.; Fayers, P.M.; Groenvold, M.; Holzner, B.; Johnson, C.D.; Kemmler, G.; et al. General Population Normative Data for the EORTC QLQ-C30 Health-Related Quality of Life Questionnaire Based on 15,386 Persons across 13 European Countries, Canada and the Unites States. European Journal of Cancer 2019, 107, 153–163. [Google Scholar] [CrossRef]
- Eichler, M.; Hentschel, L.; Richter, S.; Hohenberger, P.; Kasper, B.; Andreou, D.; Pink, D.; Jakob, J.; Singer, S.; Grützmann, R.; et al. The Health-Related Quality of Life of Sarcoma Patients and Survivors in Germany—Cross-Sectional Results of a Nationwide Observational Study (PROSa). Cancers 2020, 12, 3590. [Google Scholar] [CrossRef]
- Eichler, M.; Singer, S.; Hentschel, L.; Richter, S.; Hohenberger, P.; Kasper, B.; Andreou, D.; Pink, D.; Jakob, J.; Grützmann, R.; et al. The Association of Health-Related Quality of Life and 1-Year-Survival in Sarcoma Patients—Results of a Nationwide Observational Study (PROSa). Br J Cancer 2022, 1–9. [Google Scholar] [CrossRef]
- Cocks, K.; King, M.T.; Velikova, G.; Martyn St-James, M.; Fayers, P.M.; Brown, J.M. Evidence-Based Guidelines for Determination of Sample Size and Interpretation of the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. JCO 2011, 29, 89–96. [Google Scholar] [CrossRef]
- Bektas, M.; Bell, T.; Khan, S.; Tumminello, B.; Fernandez, M.M.; Heyes, C.; Oton, A.B. Desmoid Tumors: A Comprehensive Review. Adv Ther 2023, 40, 3697–3722. [Google Scholar] [CrossRef]
- Husson, O.; Younger, E.; Dunlop, A.; Dean, L.; Strauss, D.C.; Benson, C.; Hayes, A.J.; Miah, A.; Van Houdt, W.; Zaidi, S.; et al. Desmoid Fibromatosis through the Patients’ Eyes: Time to Change the Focus and Organisation of Care? Support Care Cancer 2019, 27, 965–980. [Google Scholar] [CrossRef] [PubMed]
- Penel, N.; Bonvalot, S.; Le Deley, M.-C.; Italiano, A.; Tlemsani, C.; Pannier, D.; Leguillette, C.; Kurtz, J.-E.; Toulmonde, M.; Thery, J.; et al. Pain in Desmoid-Type Fibromatosis: Prevalence, Determinants and Prognosis Value. Int J Cancer 2023, 153, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Gounder, M.; Ratan, R.; Alcindor, T.; Schöffski, P.; van der Graaf, W.T.; Wilky, B.A.; Riedel, R.F.; Lim, A.; Smith, L.M.; Moody, S.; et al. Nirogacestat, a γ-Secretase Inhibitor for Desmoid Tumors. N Engl J Med 2023, 388, 898–912. [Google Scholar] [CrossRef] [PubMed]
- van Eck, I.; den Hollander, D.; Desar, I.M.E.; Soomers, V.L.M.N.; van de Sande, M.A.J.; de Haan, J.J.; Verhoef, C.; Vriens, I.J.H.; Bonenkamp, J.J.; van der Graaf, W.T.A.; et al. Unraveling the Heterogeneity of Sarcoma Survivors’ Health-Related Quality of Life Regarding Primary Sarcoma Location: Results from the SURVSARC Study. Cancers 2020, 12, 3083. [Google Scholar] [CrossRef]
- Timbergen, M.J.M.; van der Graaf, W.T.A.; Grünhagen, D.J.; Younger, E.; Sleijfer, S.; Dunlop, A.; Dean, L.; Verhoef, C.; van de Poll-Franse, L.V.; Husson, O. Assessing the Desmoid-Type Fibromatosis Patients’ Voice: Comparison of Health-Related Quality of Life Experiences from Patients of Two Countries. Sarcoma 2020, 2020, 2141939. [Google Scholar] [CrossRef]
- Ingley, K.M.; Klein, R.; Theobalds, N.; Burtenshaw, S.; Abdul Razak, A.R.; Chen, B.; Xu, W.; Gladdy, R.; Li, M.; Gupta, A.A. High Prevalence of Persistent Emotional Distress in Desmoid Tumor. Psychooncology 2020, 29, 311–320. [Google Scholar] [CrossRef]
- Schwarz, R.; Hinz, A. Reference Data for the Quality of Life Questionnaire EORTC QLQ-C30 in the General German Population. European Journal of Cancer 2001, 37, 1345–1351. [Google Scholar] [CrossRef]
- Eichler, M.; Hentschel, L.; Singer, S.; Hornemann, B.; Hohenberger, P.; Kasper, B.; Andreou, D.; Pink, D.; Jakob, J.; Arndt, K.; et al. Distress in Soft-Tissue Sarcoma and Gastrointestinal Stromal Tumours Patients—Results of a German Multicentre Observational Study (PROSa). Psycho-Oncology 2022, 31, 1700–1710. [Google Scholar] [CrossRef]
- Singer, S.; Szalai, C.; Briest, S.; Brown, A.; Dietz, A.; Einenkel, J.; Jonas, S.; Konnopka, A.; Papsdorf, K.; Langanke, D.; et al. Co-Morbid Mental Health Conditions in Cancer Patients at Working Age – Prevalence, Risk Profiles, and Care Uptake. Psycho-Oncology 2013, 22, 2291–2297. [Google Scholar] [CrossRef]
- Gutiérrez-Rojas, L.; Porras-Segovia, A.; Dunne, H.; Andrade-González, N.; Cervilla, J.A. Prevalence and Correlates of Major Depressive Disorder: A Systematic Review. Braz J Psychiatry 2020, 42, 657–672. [Google Scholar] [CrossRef]
- Tansir, G.; Sharma, A.; Biswas, B.; Sah, S.N.; Roy, S.; Deo, S.V.S.; Agarwala, S.; Khan, S.A.; Bakhshi, S.; Pushpam, D. A Real-World Study on the Clinicopathological Profile, Treatment Outcomes and Health-Related Quality of Life, Anxiety and Depression among Patients with Desmoid Tumor at Two Tertiary Care Centers in India. Front Oncol 2024, 14, 1382856. [Google Scholar] [CrossRef]
- Alman, B.; Attia, S.; Baumgarten, C.; Benson, C.; Blay, J.-Y.; Bonvalot, S.; Breuing, J.; Cardona, K.; Casali, P.G.; van Coevorden, F.; et al. The Management of Desmoid Tumours: A Joint Global Consensus-Based Guideline Approach for Adult and Paediatric Patients. European Journal of Cancer 2020, 127, 96–107. [Google Scholar] [CrossRef]
- Gounder, M.M.; Mahoney, M.R.; Van Tine, B.A.; Ravi, V.; Attia, S.; Deshpande, H.A.; Gupta, A.A.; Milhem, M.M.; Conry, R.M.; Movva, S.; et al. Sorafenib for Advanced and Refractory Desmoid Tumors. N Engl J Med 2018, 379, 2417–2428. [Google Scholar] [CrossRef]
- Toulmonde, M.; Pulido, M.; Ray-Coquard, I.; Andre, T.; Isambert, N.; Chevreau, C.; Penel, N.; Bompas, E.; Saada, E.; Bertucci, F.; et al. Pazopanib or Methotrexate-Vinblastine Combination Chemotherapy in Adult Patients with Progressive Desmoid Tumours (DESMOPAZ): A Non-Comparative, Randomised, Open-Label, Multicentre, Phase 2 Study. Lancet Oncol 2019, 20, 1263–1272. [Google Scholar] [CrossRef]
Figure 1.
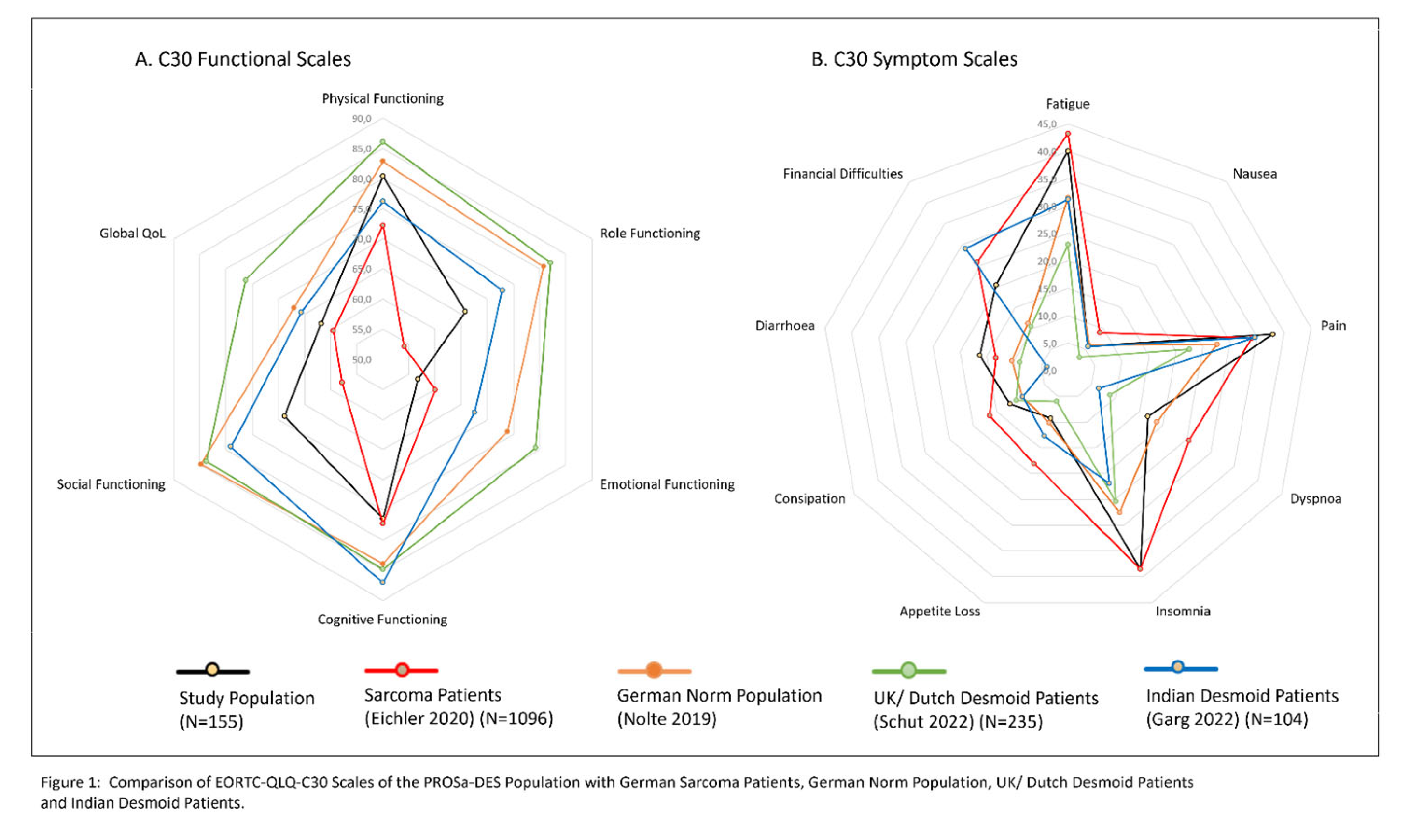
Figure 2.
Comparison of DTF QoL Scales of the PROSa-DES Population with UK/ Dutch Desmoid Patients (Shut 2022). Mean and Standard Deviation. W1= Emotional and psychological consequences. W2= Physical consequences. W3= Pain and discomfort. I1= Concerns about condition. I2= Job and education. I3= Doctor–patient relationship, communication and information. I4= Effect of DT on relationships. I5= Physical limitations and consequences. I6= Diagnostic and treatment trajectory of DT. I7= Parenting and fertility. I8= Body image and sensation. I9= Supportive care. I10= Concerns around treatment and its consequences. I11= Unpredictable course and nature of DT. DT= desmoid tumor.
Figure 2.
Comparison of DTF QoL Scales of the PROSa-DES Population with UK/ Dutch Desmoid Patients (Shut 2022). Mean and Standard Deviation. W1= Emotional and psychological consequences. W2= Physical consequences. W3= Pain and discomfort. I1= Concerns about condition. I2= Job and education. I3= Doctor–patient relationship, communication and information. I4= Effect of DT on relationships. I5= Physical limitations and consequences. I6= Diagnostic and treatment trajectory of DT. I7= Parenting and fertility. I8= Body image and sensation. I9= Supportive care. I10= Concerns around treatment and its consequences. I11= Unpredictable course and nature of DT. DT= desmoid tumor.
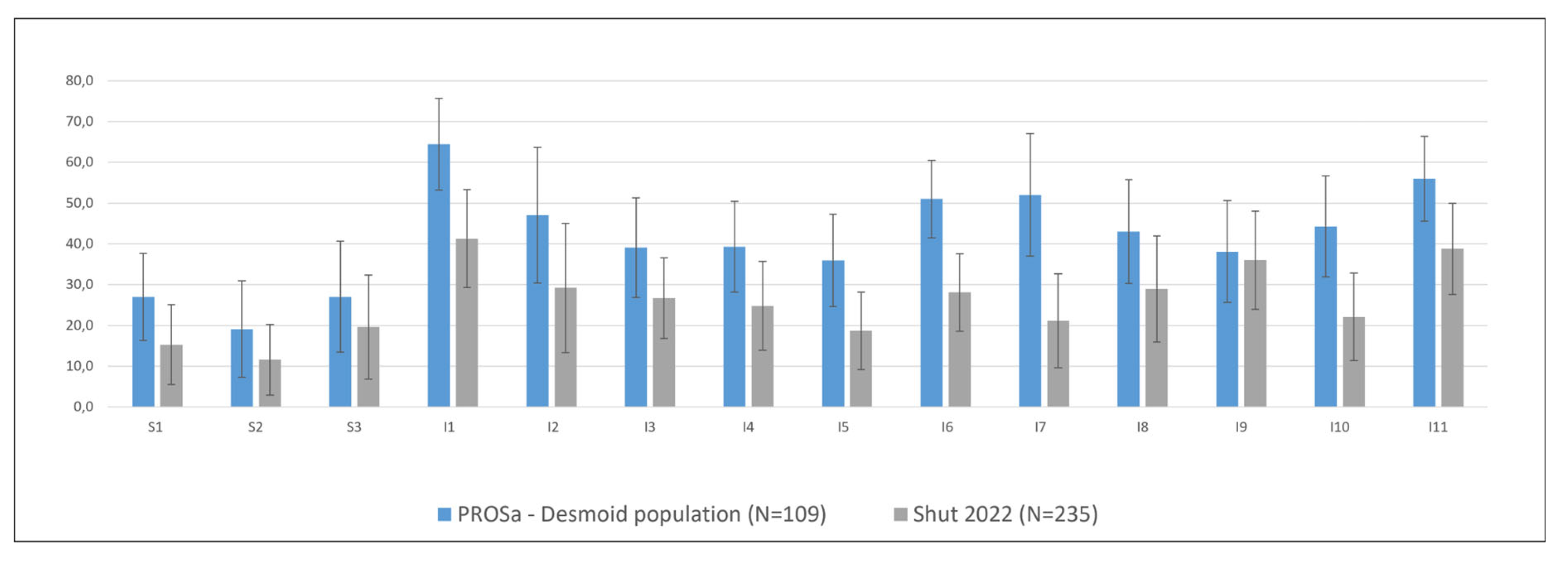

Table 1.
Description study population. Comparison of patients from the PROSa and the PROSa-DES studies.
Table 1.
Description study population. Comparison of patients from the PROSa and the PROSa-DES studies.
| Variable | Complete Dataset | PROSa-Desmoid | PROSa | |||
|---|---|---|---|---|---|---|
| Value | N | % | N | % | N | % |
| All | 155 | 109 | 70.3 | 46 | 29.7 | |
| Age Groups | ||||||
| 18-35 | 45 | 29.6 | 29 | 26.9 | 16 | 36.4 |
| 36-55 | 74 | 48.7 | 57 | 52.8 | 17 | 38.6 |
| > 55 | 33 | 21.7 | 22 | 20.4 | 11 | 25 |
| Age (mean. SD) | 45.0 | 14.3 | 45.7 | 14.1 | 43.4 | 14.8 |
| Gender | ||||||
| female | 108 | 69.7 | 76 | 69.7 | 32 | 69.6 |
| male | 45 | 29 | 31 | 28.4 | 14 | 30.4 |
| diverse | 2 | 1.3 | 2 | 1.8 | 0 | 0 |
| Time since diagnosis | ||||||
| 0-<5 year | 64 | 41.6 | 29 | 26.6 | 35 | 77.8 |
| 5-<10 year | 34 | 22.1 | 31 | 28.4 | 3 | 6.7 |
| > 10 years | 56 | 36.4 | 49 | 45 | 7 | 15.6 |
| Time since diagnosis (mean. SD) | 7.9 | 6.4 | 9.5 | 6.1 | 4.0 | 5.4 |
| Time since treatment | ||||||
| in treatment | 17 | 17.9 | ||||
| 0-<5 years | 28 | 25.7 | ||||
| 5-<10 years | 30 | 31.6 | ||||
| more than 10 years | 20 | 21.1 | ||||
| Time since treatment (mean. SD) | 5.8 | 4.7 | ||||
| Medical lines | ||||||
| 0 to 1 | 83 | 53.5 | ||||
| 2 or more | 23 | 14.8 | ||||
| unknown | 3 | 1.9 | ||||
| Recurrence after Surgery | ||||||
| no | 52 | 33.5 | 33 | 30.3 | 19 | 41.3 |
| yes | 60 | 38.7 | 43 | 39.4 | 17 | 37 |
| unknown or no OP | 43 | 27.7 | 33 | 30.3 | 10 | 21.7 |
| Tumor Location | ||||||
| Lower extremity (incl hip/ pelvis) | 48 | 31 | 32 | 29.4 | 16 | 34.8 |
| Shoulder & upper extremity | 12 | 7.7 | 8 | 7.3 | 4 | 8.7 |
| Trunk (thoracic wall & back) | 27 | 17.4 | 20 | 18.3 | 7 | 15.2 |
| Abdominal wall | 17 | 11 | 17 | 15.6 | 0 | 0 |
| Intra-abdominal | 36 | 23.2 | 24 | 22 | 12 | 26.1 |
| Head & neck | 8 | 5.2 | 7 | 6.4 | 1 | 2.2 |
| not defined/ multifocal | 7 | 4.5 | 1 | 0.9 | 6 | 13 |
| Received treatments | ||||||
| surgery only | 30 | 27.5 | ||||
| ST only | 14 | 12.8 | ||||
| ST + surgery | 19 | 17.4 | ||||
| ST + RT + surgery | 21 | 19.3 | ||||
| none (W&W) | 7 | 6.4 | ||||
| all other | 18 | 16.5 | ||||
| Education | ||||||
| basic/ medium | 58 | 37.7 | 36 | 33 | 22 | 48.9 |
| high | 96 | 62.3 | 73 | 67 | 23 | 51.1 |
| Status Employment | ||||||
| employed | 114 | 73.5 | 78 | 71.6 | 36 | 78.3 |
| unemployed. disability pension | 17 | 11 | 14 | 12.8 | 3 | 6.5 |
| retirement pension | 15 | 9.7 | 12 | 11 | 3 | 6.5 |
| other | 9 | 5.8 | 5 | 4.6 | 4 | 8.7 |
Table 2.
Factors associated with the DTF QoL Scales. Multivariable Regression. B=unstandardized regression coefficient. p= p-value. ST= systemic therapy. RT= radio therapy. *Others not shown. Significant differences bold.
Table 2.
Factors associated with the DTF QoL Scales. Multivariable Regression. B=unstandardized regression coefficient. p= p-value. ST= systemic therapy. RT= radio therapy. *Others not shown. Significant differences bold.
| Desmoid-Type Fibromatosis Quality of Life Questionnaire (DTF QoL) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptom Scales B (p) |
Impact Scales B (p) |
|||||||||||||
| W1 Emotional consequences |
W2 Physical consequences |
W3 Pain and discomfort |
1 Concerns Condition |
2 Job & Education |
3 Doctor–patient relationship |
4 Effect of DTF on relationships |
5 Physical limitations and consequences |
6 Diagnostic and treatment trajectory |
7 Parenting and fertility |
8 Body image and sensation |
9 Supportive care |
10 Concerns around treatment and its consequences |
11 Unpredictable course and nature of DTF |
|
| Age Groups | ||||||||||||||
| 18-35 years (ref) | ||||||||||||||
| 36-55 years | / | / | / | -1,2 (0,81) |
/ | / | / | / | / |
-43,2 (0,00) |
2,5 (0,65) |
/ | / | / |
| > 55 years | / | / | / | -11,3 (0,07) |
/ | / | / | / | / | -6,5 (0,40) |
-8,5 (0,22) |
/ | / | / |
| Gender* | ||||||||||||||
| woman (ref) | ||||||||||||||
| men |
-11,9 (<,01) |
-12,2 (<,01) |
-15,7 (<,01) |
-10,4 (0,03) |
/ |
-17,6 (<,001) |
-19,2 (<,001) |
-13,5 (<,01) |
-13,0 (<,001) |
-26,6 (<,001) |
-14,7 (<,01) |
-16,3 (<,001) |
-15,4 (<,01) |
-14,9 (<,001) |
| Time since treatment | ||||||||||||||
| In treatment (ref) | ||||||||||||||
| 0–<5 years | / | / | / | / | / | / | / | / | / | / | / | / | / | / |
| 5–<10 years | / | / | / | / | / | / | / | / | / | / | / | / | / | / |
| >10 years | / | / | / | / | / | / | / | / | / | / | / | / | / | / |
| Time since diagnosis | ||||||||||||||
| 0–<5 years (ref.) | ||||||||||||||
| 5–<10 years | / |
11,5 (0,03) |
/ | / | / | / | / | / | / | / | / | -6,1 (0,31) |
/ | / |
| >10 years | / | 1,7 (0,73) |
/ | / | / | / | / | / | / | / | / | -8,9 (0,12) |
/ | / |
| No of ST lines | ||||||||||||||
| 0 or 1 line (ref.) | ||||||||||||||
| ≥2 lines | 7,3 (0,11) |
/ |
19,0 (<,01) |
7,7 (0,14) |
12,3 (0,09) |
/ | 5,5 (0,24) |
8,4 (0,09) |
/ | / |
15,3 (<,01) |
/ | 9,7 (0,07) |
13,9 (<,01) |
| Recurrence* | ||||||||||||||
| no (ref.) | ||||||||||||||
| yes | / | / | / | / | / | / | / | / | / | -13,3 (0,10) |
/ |
-11,4 (0,03) |
/ | / |
| Tumor location* | ||||||||||||||
| Lower extremity (incl hip/ pelvis) (ref.) |
||||||||||||||
| Upper extremity | / |
-17,2 (0,02) |
6,3 (0,46) |
/ | / | / | / | / | / |
-46,5 (<,01) |
/ | / |
-24,3 (<,01) |
/ |
| Trunk (thoracic wall & back) |
/ |
-13,0 (0,02) |
-10,1 (0,12) |
/ | / | / | / | / | / | -17,2 (0,09) |
/ | / | -7,0 (0,23) |
/ |
| Abdominal wall | / |
-16,0 (<,01) |
-12,4 (0,07) |
/ | / | / | / | / | / | -10,2 (0,29) |
/ | / |
-14,1 (0,02) |
/ |
| Intra-abdominal | / | -10,6 (0,06) |
-8,2 (0,20) |
/ | / | / | / | / | / | 1,2 (0,90) |
/ | / | -7,7 (0,19) |
/ |
| Head & Neck | / |
-18,2 (0,02) |
-4,3 (0,64) |
/ | / | / | / | / | / | -30,5 (0,06) |
/ | / |
-26,6 (<,01) |
/ |
| Received treatments* | ||||||||||||||
| Surgery and/ or ST (ref.) |
||||||||||||||
| ST + RT + surgery | / |
11,9 (0,02) |
9,9 (0,09) |
7,3 (0,18) |
/ | / | / |
11,8 (0,02) |
7,4 (0,10) |
/ | 9,1 (0,13) |
/ |
11,5 (0,03) |
6,8 (0,16) |
| Education | ||||||||||||||
| basic/ medium (ref.) | ||||||||||||||
| high | / | / | / | / | / | / | / | / | / | / | / | / | / | / |
| Status Employment* | ||||||||||||||
| employed (ref.) | ||||||||||||||
| unemployed, disability pension |
26,0 (<,001) |
26,7 (<,001) |
16,9 (0,01) |
/ |
44,5 (<,001) |
/ |
25,4 (<,001) |
20,9 (<,001) |
/ | / | / | / |
18,8 (<,01) |
/ |
| retirement pension | 5,8 (0,33) |
11,3 (0,05) |
-1,1 (0,87) |
/ | 16,8 (0,20) |
/ | 5,0 (0,40) |
9,4 (0,13) |
/ | / | / | / | -1,5 (0,83) |
/ |
Table 3.
Factors associated with Scales of the EORTC QLQ-C30. B=unstandardized regression coefficient. p= p-value. ST= systemic therapy. RT= radio therapy. * Others not shown. Significant differences bold.
Table 3.
Factors associated with Scales of the EORTC QLQ-C30. B=unstandardized regression coefficient. p= p-value. ST= systemic therapy. RT= radio therapy. * Others not shown. Significant differences bold.
| European Organisation for Research and Treatment of Cancer Quality of Life Core Questionnaire (EORTC QLQ-C30) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Functional Scales B (p) |
Symptom Scales B (p) |
||||||||||||||
| PF (N=109) | RF (N=109) | EF (N=154) | CF (N=109) | SF (N=154) | Global QoL (N=107) | FA (N=109) | NV (N=151) | Pain (N=109) | Dyspnea (N=153) | Insomnia (N=154) | Appetite Loss (N=155) | Constipation (N=154) | Diarrhea (N=109) | Financial Diff (N=152) | |
| Age Groups | |||||||||||||||
| 18-35 years (ref) | |||||||||||||||
| 36-55 years | / | / | / | / | / | / | / | -6.1 (0.01) | / | -7.6 (0.11) | / | / | / | / | / |
| > 55 years | / | / | / | / | / | / | / | -12.6 (<.001) | / | -0.5 (0.94) | / | / | / | / | / |
| Gender* | |||||||||||||||
| woman (ref) | |||||||||||||||
| men | 13.1 (<.001) | / | 16.2 (<.001) | / | / | 12.4 (<.01) | / | / | -23.2 (<.001) | / | / | / | / | / | / |
| Time since treatment | |||||||||||||||
| In treatment (ref) | |||||||||||||||
| 0–<5 years | / | / | / | 2.3 (0.77) |
/ | -3.9 (0.46) | -4.3 (0.60) | / | / | / | / | / | / | / | / |
| 5–<10 years | / | / | / | 6.2 (0.42) |
/ | -0.9 (0.87) | -6.2 (0.45) | / | / | / | / | / | / | / | / |
| >10 years | / | / | / | 20.0 (0.02) | / | 7.7 (0.19) |
-17.9 (0.04) | / | / | / | / | / | / | / | / |
| Time since diagnosis | |||||||||||||||
| 0–<5 years (ref.) | |||||||||||||||
| 5–<10 years | / | / | / | / | / | / | / | 2.2 (0.41) |
/ | / | -3.5 (0.60) | / | / | 3.5 (0.62) |
/ |
| >10 years | / | / | / | / | / | / | / | -3.1 (0.19) | / | / | -12.2 (0.03) | / | / | -10.7 (0.09) | / |
| No. of ST lines | |||||||||||||||
| 0 or 1 line (ref.) | |||||||||||||||
| ≥2 lines | / | / | / | / | / | / | / | / | 12.0 (0.07) | / | / | / | / | 13.4 (0.04) | / |
| Recurrence* | |||||||||||||||
| no (ref.) | |||||||||||||||
| yes | / | / | / | / | / | / | / | / | / | / | / | / | / | / | / |
| Tumor location* | |||||||||||||||
| Lower extremity (incl hip/ pelvis) (ref.) | |||||||||||||||
| Upper extremity | 9.9 (0.13) |
/ | / | / | / | / | / | / | / | / | / | / | / | / | / |
| Trunk (thoracic wall & back) | 12.8 (0.01) | / | / | / | / | / | / | / | / | / | / | / | / | / | / |
| Abdominal wall | 11.4 (0.03) | / | / | / | / | / | / | / | / | / | / | / | / | / | / |
| Intra-abdominal | 1.8 (0.71) |
/ | / | / | / | / | / | / | / | / | / | / | / | / | / |
| Head & Neck | 5.5 (0.42) |
/ | / | / | / | / | / | / | / | / | / | / | / | / | / |
| Received treatments* | |||||||||||||||
| surgery and/ or ST (ref.) | |||||||||||||||
| ST + RT + surgery | -15.3 (<.001) | -12.9 (0.07) | / | / | / | -9.6 (0.02) | 12.1 (0.07) | / | 13.9 (0.04) | / | / | / | / | / | / |
| Education | |||||||||||||||
| basic/ medium (ref.) | |||||||||||||||
| high | / | / | / | / | / | / | / | / | / | / | / | / | 8.4 (0.05) |
-8.8 (0.15) | / |
| Status Employment* | |||||||||||||||
| employed (ref.) | |||||||||||||||
| unemployed, disability pension | -27.4 (<.001) | -33.0 (<.001) | -23.8 (<.001) | -34.9 (<.001) | -40.3 (<.001) | -25.3 (<.001) | 31.8 (<.001) | 15.3 (<.001) | 33.5 (<.001) | 12.7 (0.07) | 39.6 (<.001) | 14.3 (<.01) | / | / | 48.5 (<.001) |
| retirement pension | -4.4 (0.41) | -10.0 (0.25) | 2.9 (0.68) |
-5.2 (0.51) | -6.9 (0.38) | -3.5 (0.52) | 1.7 (0.83) |
6.8 (0.12) |
-0.6 (0.94) | 9.7 (0.26) |
8.7 (0.31) |
3.8 (0.46) |
/ | / | 10.5 (0.18) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



