Submitted:
24 February 2026
Posted:
26 February 2026
You are already at the latest version
Abstract
Objective: Neurological complications following allogeneic hematopoietic stem cell transplantation (allo-HSCT) are rare but serious events that significantly impact morbidity and mortality. This study aims to evaluate the incidence, clinical spectrum, and associated risk factors of neurological complications in patients who underwent allo-HSCT at a single center. Methods: We retrospective analyzed 108 patients who underwent allo-HSCT between January 2022 and December 2024. Patients were categorized by transplant type: myeloablative related donor (n=48), myeloablative unrelated donor (n=36), and haploidentical transplant (n=24). Neurological complications were observed in 18 patients (16.7%) and analyzed in terms of demographics, transplant type, hematologic diagnosis, conditioning regimen, infections, GVHD status, and outcomes. Results: The mean age of affected patients was 52.56 years (range 20–71), with equal gender distribution. Neurological complications developed between day 15 and day 395 post-transplant (mean: day 200). CMV positivity was detected in 14 of 17 patients with neurological complications. Acute GVHD was present in 11 patients and chronic GVHD in 5 patients. Statistical analysis revealed a significant association between neurological complications and CMV positivity (p=0.000), acute GVHD (p=0.014), and chronic GVHD (p=0.009). Ten patients died, with causes including disease progression, severe GVHD, CMV encephalitis, and hemophagocytic syndrome. Conclusion: Neurological complications post-allo-HSCT are diverse and often fatal. CMV infection, acute and chronic GVHD are significant risk factors. Early diagnosis and multidisciplinary management are essential to improve outcomes.
Keywords:
allogeneic bone marrow transplantation
; neurological complications
; plasmapheresis
Introduction
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is a curative treatment for various hematologic malignancies. Despite its therapeutic potential, allo-HSCT is associated with a range of complications, including neurological events that can severely affect patient outcomes.
Neurological complications (NC) are frequently seen after allo-HSCT and are associated with significant morbidity and mortality [1,2].
These complications are heterogeneous and not easy to classify; they may include different entities such as infections, disease relapse, drug-related toxicity, cerebrovascular events, and metabolic and immune-mediated disorders.
NCs following are allo-HSCT classified according to the time of onset; early complications are generally associated with conditioning regimen, bone marrow aplasia, and drug toxicity, while later neurological complications may arise due to infections, graft-versus-host disease (GVHD), and/or immunosuppressive therapy. The reported incidence of NCs following allo-HSCT varies widely from 8% to 55% in different retrospective studies, depending on the definition of NCs, study population, follow-up, and type of allogeneic stem cell transplantation procedure [3,4,5].
The most common mechanisms for the development of NC’s following allo-HSCT are:
- Drug toxicity (calcineuron inhibitors, methotrexate, busulfan, other cytotoxic agents, radiation, azoles),
- Opportunistic infections,
- Disruption of metabolic homeostasis due to sepsis or organ failure,
- Recurrence of underlying malignancy in the central nervous system.
There is a wide overlap between the clinical features of different central nervous system syndromes. Therefore, differential diagnosis is difficult in clinical practice. The resulting delay in clinical management can lead to a significant increase in mortality. (6-12)
This study provides a retrospective analysis of all major central nervous system complications observed in patients who underwent transplantation at a single institution over a two-year period. The aim of this analysis was to assess the incidence of various central nervous system disorders, identify risk factors, and analyze their impact on the outcome of allogeneic stem cell transplantation.
Methods
Eligibility Criteria
All adult patients with hematological diseases who underwent allogeneic stem cell transplantation (alloHSCT) at Medicana Izmir Hospital between January 2022 and December 2024 were included in this study. The hospital's Institutional Ethics Committee approved the protocol, and written informed consent was obtained from all patients in accordance with the Declaration of Helsinki.
Data Collection
Patients who developed neurological complications were retrospectively examined in detail by a hematologist and a neurologist, focusing on neurological symptoms, diagnostic methods, time and cause of symptom onset, type of transplant, immunosuppressive treatments received, GVHD status, and infections.
Systemic immune and inflammation markers such as the systemic immune-inflammatory index (SII), neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), HALP (hemoglobin, albumin, lymphocyte, and platelet) score, are parameters readily obtainable using routine complete blood counts and albumin values, and their prognostic value has been studied recently [13,14,15,16,17,18,19]..SII (platelet count × neutrophil count/lymphocyte count) reflects the balance between host inflammatory and immune status and has been associated with survival outcomes in various solid tumors [20,21,22,23,24,25,26]. Similarly, high NLR and PLR values have been associated with poor prognosis in both oncological and hematological cancers [27,28,29,30].
In our study, SII, NLR, PLR, and HALP scores were examined in patients with hematological malignancies who underwent allogeneic transplantation, and the aim was also to compare patients who developed neurological complications with those who did not.
This retrospective study included 108 patients who underwent allo-HSCT at Medicana Izmir Hospital between January 2022 and December 2024. Patients were classified by transplant type: myeloablative related donor (n=48), myeloablative unrelated donor (n=36), and haploidentical transplant (n=24).
Neurological complications were identified in 18 patients (16.7%) and analyzed for demographic data, hematologic diagnosis, conditioning regimen, GVHD status, infections, NLR, PLR, SII, Halp score and outcomes.
Transplantation Procedures
Conditioning Regimens
The conditioning regimens were administered according to institutional protocols, based on the hematopoietic stem cell source, donor type, patient age, comorbidities, and underlying disease. Conditioning regimens according to donor type—matched sibling donor (MSD), HLA-matched unrelated donor (MUD) considering high-resolution typing of HLA-A, -B, -C, -DRB1, and -DQB1 or haploidentical family donor
GVHD Prophylaxis and Therapy
GVHD prophylaxis differed according to the type of hematopoietic stem cells source.
Allo-HSCT from MSD received cyclosporine combined with mycophenolate mofetil (MMF),
Patients undergoing allo-HSCT from an MUD received a combination of cyclosporine with MMF and antithymocyte globulin (ATG) and post-transplantation cyclophosphamide (on days +3 and +5)
Haploidentical allo-HSCT received post-transplantation cyclophosphamide (on days +3 and +5) combined with cyclosporine and MMF.
Definitions
NC’s was defined as any neurological event occurring between the start of the conditioning regimen and the last follow-up. The onset of a neurological event was defined as the first day of neurological symptoms leading to diagnosis. NC’s were divided into CNS and peripheral nervous system (PNS) events. They were classified into different categories according to diagnosis made by a combination of clinical, radiological, laboratory, and microbiological findings. Pre-existing neurological complications were not included in the study.
Calculation of Immune-Inflammatory Indices
Systemic immune-inflammation index (SII): platelet count × neutrophil count/lymphocyte count.
Neutrophil-to-lymphocyte ratio (NLR): neutrophil count/lymphocyte count.
Platelet-to-lymphocyte ratio (PLR): platelet count/lymphocyte count.
Monocyte-lymphocyte ratio (MLR): monocyte count/ lymphocyte count
The HALP (hemoglobin, albumin, lymphocyte, and platelet) score:
hemoglobin(g/L) x albumin (g/L) x absolute lymphocyte count (k/μL) divided by platelets (k/μL)
Statistical Analyses
Statistical analyses were conducted using “IBM SPSS Statistics for Windows, Version 25.0 (Statistical Package for the Social Sciences, IBM Corp., Armonk, NY, USA)”. Descriptive statistics are presented as n and % for categorical variables, and as mean ± SD and median (min–max) for continuous variables. An ROC curve analysis was used in the prediction of morbidity via various indices. The Kaplan–Meier method was used to compare survival and EFS durations among clinical groups, with p < 0.05 considered statistically significant
Results
Patient, Transplantation, and Graft Characteristics
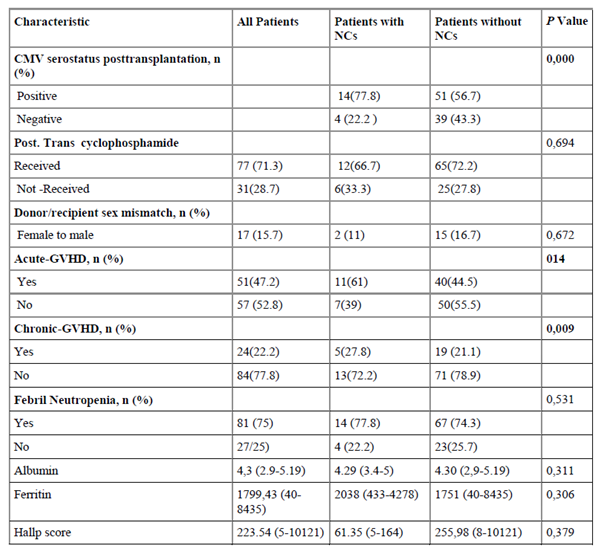
One hundred eight consecutive allo-HSCT recipients who allografted at our institution were included in this study. Patient, disease, and transplantation characteristics according to the development of NCs are summarized in Table 1. In our series, allo-HSCT was performed using an MSD in 48 patients (44.4%), 36 (33.3%) from an MUD, and 24 (22.2%) from a haploidentical donor. The median patient age was 47 years, and most patients had acute leukemia (77.8%). The median follow-up of surviving patients was 71 months (range, 11 to 213 months).
Of the patients, 57 (52.8%) were male. 36 patients (33.3%) received ATG, and 77 patients (71.3%) received post-transplant cyclophosphamide. In 17 patients (15.7%), the transplant was performed from a female donor to a male patient. Acute GVHD developed in 51 patients (47.2%), and chronic GVHD in 24 patients (22.2%). Febrile neutropenia was observed in 81 patients (75%). NC’s developed in 18 (16.7%) of the 108 patients included in the study.
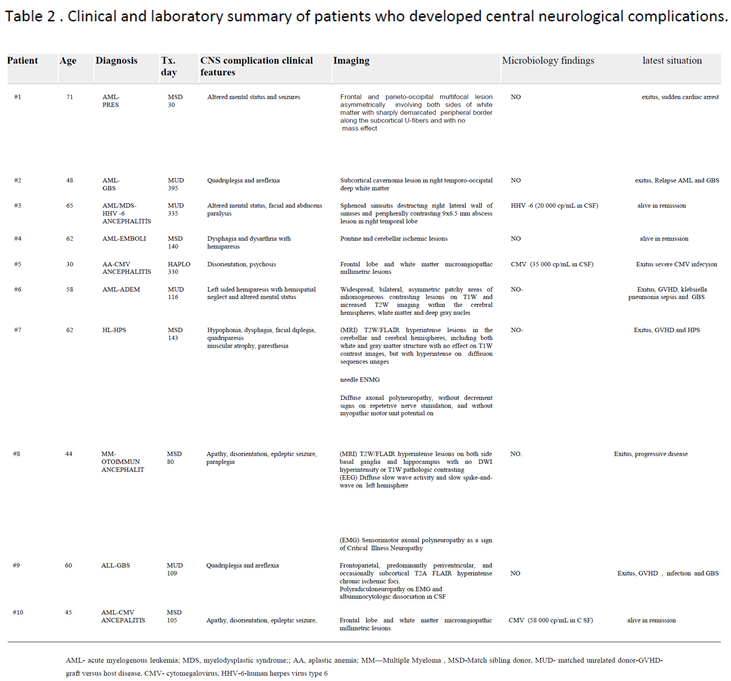
The age range of 18 patients who developed complications (20-71 years) had a mean of 52.56 years, 50% were female, and 50% were male. Regarding the type of transplant, 9 patients received myeloablative related, 6 patients myeloablative unrelated, and 3 patients haploidentical allogeneic stem cell transplants. NC’s developed between 15-395 days, with a mean of 200 days post-transplant. As for the conditioning regimen, 14 patients received fludarabine-melphalan, 4 patients received fludarabine-treosulfan, and 12 patients received post-transplant cyclophosphamide treatment. ATG was added to the conditioning regimen for the 6 patients with unrelated transplants. Regarding the neurological complications that developed; 2 patients had Guillain-Barré syndrome, 2 patients had CMV encephalitis, 1 patient had HHV-6 encephalitis 1 patient had Posterior reversible encephalopathy syndrome (PRES), 1 patient had Acute Disseminated Encephalomyelitis (ADEM) , 1 patient had autoimmune encephalitis, 1 patient had widespread emboli in the pons and cerebellum, 1 patient had central nervous system involvement due to hemophagocytic syndrome (HPS) (These 10 patients are described in detail in Table 2) , 2 patients had neuropathic pain due to varicella-zoster infection and 3 patients had central nervous system involvement (2 patients with AML, 1 patient with multiple myeloma), polyneuropathy developed in 3 patients. Neurological complications most frequently occurred in patients diagnosed with AML (44.4%); acute GVHD was observed in 11 of the 18 patients who developed complications (3 patients IBMT grade A, 4 patients grade B, 4 patients grade C). Acute GVHD developed in the skin in 10 patients, in the liver in 3 patients, and in the gastrointestinal system in 7 patients, while chronic GVHD developed in 5 patients.
When patients who developed neurological complications were examined, it was observed that CMV positivity was significantly higher in these patients (p=0.000), with Acute GVHD in 11 patients (p=0.014) and Chronic GVHD in 5 patients (p=0.009).
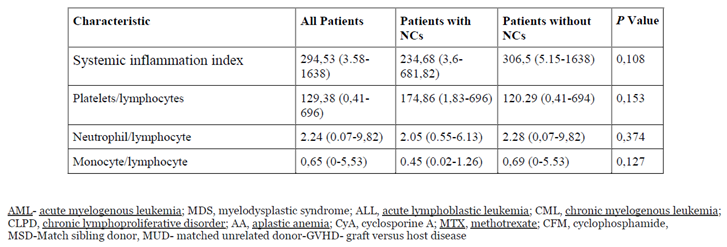
When comparing patients who developed neurological complications with those who did not, no statistically significant differences were found in terms of age, gender, disease diagnosis, transplant type, post-transplant cyclophosphamide use, ATG use, transplant from a female donor to a male patient, febrile neutropenia, albumin level, ferritin level, HALP score, SII, PLR, NLR, MLR .(Table 1)

During the complications, 11 patients were receiving immunosuppressive therapy, and 6 patients had fever. Cerebrospinal fluid (CSF) analysis revealed HHV-6 positivity in 1 patient and CMV positivity in 2 patients. Central nervous system involvement was present in three patients (1 patient with multiple myeloma, 2 patients with AML). NC’s developed in four patients during disease relapse. Plasma exchange was applied to 4 patients who developed Guillain-Barre syndrome and to 1 patient with HPS with CNS involvement and 1 patient with ADEM . During follow-up, 10 of the 18 patients who developed neurological complications were lost.
Only one patient died within the first 100 days after transplantation, eight patients died within the first year, and one patient died after the first year of the transplant. Examining the causes of death, one patient died of sudden cardiac arrest while in remission, one patient from HPS with CNS involvement, one patient from resistant CMV infection, one patient from ADEM syndrome and severe GIS GVHD, three patients from disease progression, one patient from resistant Klebsiella pneumonia infection- Guillain-Barre syndrome and disease progression, one patient from pneumonia, and one patient from severe GIS-skin GVHD, Guillain-Barre syndrome, and pneumonia. Four of the deceased patients had relapsed disease. Summaries of all patients who developed central neurological complications are presented in Table 2.
Discussion
NC’s post-allo-HSCT are diverse and associated with high mortality. CMV infection, acute GVHD, and chronic GVHD are significant risk factors. Early diagnosis, infection control, and multidisciplinary management are essential to improve patient outcomes.
This study was conducted to identify NC’s that develop in patients undergoing allo-HSCT at our center. Despite the limitations imposed by the retrospective nature of the study, this single-center study included a relatively homogeneous conditioning regimen and GVHD prophylaxis. One of the aims of this study was to evaluate NCs according to donor source. There is little published data on the effect of transplantation from an alternative donor (MUD or haploidentical) on the incidence of NC’s [33]. and neurological complications have developed more frequently after allo-HSCT from an alternative donor [34,35].
Previous studies [31,32,36,37,38] have reported that approximately 8.3–24% of patients develop NC’s after HSCT. Inter-study comparisons are difficult due to the heterogeneity of patient and transplantation characteristics, definitions of neurological events, and follow-up time. NC’s , particularly those related to the central nervous system, including encephalopathy, have been associated with a poor prognosis leading to a high mortality rate after allo-HSCT [39,40], and accurate and timely diagnosis and intervention are crucial to improve outcomes in these cases.
In our study, NC’s developed in 18 of the 108 patients (16.7%) who participated in the study.
Systemic inflammatory processes are thought to be closely related to endothelial dysfunction, a damaged blood-brain barrier, and decreased cerebral blood flow.(41) Leukocytes are important components of systemic inflammation and play a significant role in immune regulation. Platelets have a primary role in the thrombo-inflammation of stroke and predict poor functional outcomes. The inflammatory response damages brain tissue by causing damage both inside and outside blood vessels, and also damage to neurons.(42) In contrast, lymphocytes are known to control the inflammatory response by regulating and repairing inflammation during cerebral ischemia.
When comparing patients who developed NC’s with those who did not, no statistically significant differences were found in albumin levels, ferritin levels, systemic immune and inflammation markers such as HALP score, SII, PLR, NLR, MLR (table 1)
Leukoencephalopathy can develop due to chemotherapy and subsequent calcineurin inhibitors used by patients, but in many cases it may be mild and reversible [43]. PRES resulting from acute blood pressure increase associated with calcineurin inhibitors and corticosteroids is a clinical syndrome typically characterized by visual changes, changes in mental status, and seizures [44].
In our patient group, only one patient developed PRESS syndrome. We believe the reason for this low number is due to the fact that cyclosporine blood levels were monitored very closely in the patients and their blood pressure was followed very carefully.
In our current analysis, infection was found to be a more frequent cause of neurological complications. Individuals undergoing HSCT are particularly susceptible to viruses, bacteria, or invasive molds, and CNS infection has been shown to be an indicator of a poor prognosis [2,37,38,45].
The incidence of CNS infection after allo-HSCT can be as high as 15% [24]. Aspergillus and toxoplasmosis are among the most common causes, and other fungi and viruses can also be a source of CNS infection. Previous studies have shown that high-risk disease status is a risk factor for CNS infection, which significantly reduces overall survival [2].
However, in practice there are several limitations in identifying the causative microorganisms because brain biopsy can be problematic for patients with poor underlying conditions and PCR detection, despite the high sensitivity and specificity of this test, is only possible for a few cerebrospinal fluid viruses such as HSV and CMV [46].
CMV reactivation and GVHD emerged as significant contributors. CMV’s neuroinvasive potential and immunosuppressive effects are well documented.
CMV positivity was detected in the CSF of two of our patients.
Furthermore, patients with high blood CMV-PCR levels showed statistically significant neurological complications. (p-value 0.000)
In one patient, although HHV type 6 could not be detected in the cerebrospinal fluid (CSF), it was detected in a PCR test taken from a dural biopsy. This patient received long-term intravenous ganciclovir treatment and is currently in remission and free of infection, 18 months after the initial infection.
Therefore, to improve patient outcomes, prophylactic antibacterial, antifungal, and antiviral treatments should be administered depending on the time elapsed after stem cell transplantation and the patient's immune status.
Three of our patients had central nervous system involvement during follow-up (2 patients with AML, 1 patient with multiple myeloma). Since all ALL patients had received CNS prophylaxis, no recurrence was observed.
In many previous studies, GVHD has been identified as a risk factor for neurological sequelae [7,31,32,46,47] and the prognosis of CNS- GVHD is claimed to be very poor [48].
GVHD may disrupt the blood-brain barrier and promote neuroinflammation.
In addition to CNS- GVHD, neurological events associated with CNS infections and thrombotic microangiopathy (TMA) may be frequently observed in patients with GVHD following increased use of calcineuron inhibitors and corticosteroids [49]. In our current study, no patient was diagnosed with CNS- GVHD, but NC’s were observed to develop statistically significantly more frequently in patients who developed acute and chronic GVHD (p values 0.014 and 0.009, respectively).
Immune-mediated neurological complications can frequently develop. (50) In our patient group, GBS was suspected in 2 patients, ADEM in one patient, and HPS-CNS involvement in one patient. All four patients were initially treated with plasmapheresis, and after no response, IVIG treatment was given. However, all patients died due to various neurological and infectious complications.
Conclusions
NC’s after allo-HSCT can present with various clinical manifestations and require early diagnosis and a multidisciplinary approach. Immunosuppressive therapy, presence of infection, and disease relapse may be significant risk factors for the development of complications. These findings indicate that clinical awareness needs to be increased in terms of preventing and managing neurological complications.
Author Contributions
S.K. designed and planned the study, and E.Ö. enrolled patients in the outpatient clinic, took blood samples, evaluated the results, designed and wrote the manuscript, and calculated the statistics. CH and VN enabled neurological evaluation of patients, planning of their treatment, and follow-up. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Izmir Katip Celebi University Non-Interventional Ethics Committee (approval date: 25 December 2021 protocol number 99 GOA; decision no. 144).
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Acknowledgments
The authors would like to thank all the patients and the lab team for their contributions.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Pruitt, AA; Graus, F; Rosenfeld, MR. Neurological complications of transplantation: Part 1: Hematopoietic cell transplantation. Neurohospitalist 2013, 3, 24–38. [Google Scholar] [CrossRef] [PubMed]
- Maffini, E; Festuccia, M; Brunello, L; Boccadoro, M; Giaccone, L; Bruno, B. Neurologic complications after allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2017, 23, 388–397. [Google Scholar] [CrossRef]
- Antonini, G; Ceschin, V; Morino, S; et al. Early neurologic complications following allogeneic bone marrow transplant for leukemia: a prospective study. Neurology 1998, 50, 1441–1445. [Google Scholar] [CrossRef] [PubMed]
- Sostak, P; Padovan, CS; Yousry, TA; Ledderose, G; Kolb, HJ; Straube, A. Prospective evaluation of neurological complications after allogeneic bone marrow transplantation. Neurology 2003, 60, 842–848. [Google Scholar] [CrossRef]
- Kang, JM; Kim, YJ; Kim, JY; et al. Neurologic complications after allogeneic hematopoietic stem cell transplantation in children: analysis of prognostic factors. Biol Blood Marrow Transplant. 2015, 21, 1091–1098. [Google Scholar] [CrossRef]
- Straathof, K; Anoop, P; Allwood, Z; et al. Long-term outcome following cyclosporine-related neurotoxicity in paediatric allogeneic haematopoietic stem cell transplantation. Bone Marrow Transplant. 2017, 52(1), 159–162. [Google Scholar] [CrossRef]
- Schmidt-Hieber, M; Silling, G; Schalk, E; et al. CNS infections in patients with hematological disorders (including allogeneic stem-cell transplantation)-Guidelines of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Medical Oncology (DGHO). Ann Oncol 2016, 27(7), 1207–1225. [Google Scholar] [CrossRef]
- Hanajiri, R; Kobayashi, T; Yoshioka, K; et al. Central nervous system infection following allogeneic hematopoietic stem cell transplantation. Hematol Oncol Stem Cell Ther. 2017, 10(1), 22–28. [Google Scholar] [CrossRef]
- Schmidt-Hieber, M; Engelhard, D; Ullmann, A; et al. Central nervous system disorders after hematopoietic stem cell transplantation: a prospective study of the Infectious Diseases Working Party of EBMT. J Neurol. 2020, 267(2), 430–439. [Google Scholar] [CrossRef]
- Behre, G; Becker, M; Christopeit, M. BK virus encephalitis in an allogeneic hematopoietic stem cell recipient. Bone Marrow Transplant. 2008, 42(7), 499. [Google Scholar] [CrossRef] [PubMed]
- Behre, G; Christopeit, M; Weber, T. Successful treatment of Candida spp. encephalitis occurring under Caspofungin treatment after allogeneic stem cell transplantation. Ann Hematol. 2009, 88(1), 93–94. [Google Scholar] [CrossRef]
- Christopeit, M; Grundhoff, A; Rohde, H; et al. Suspected encephalitis with Candida tropicalis and Fusarium detected by unbiased RNA sequencing. Ann Hematol. 2016, 95(11), 1919–1921. [Google Scholar] [CrossRef]
- Chu, B.; Chen, Y.; Pan, J. Prognostic significance of systemic immune inflammation index for ovarian cancer: An updated systematic review and meta-analysis. J. Ovarian Res. 2025, 18, 41. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, Y.; Guo, C.; Li, S.; Huang, C. Systemic immune-inflammation index as a predictor of survival in non-small cell lung cancer patients undergoing immune checkpoint inhibition: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2025, 210, 104669. [Google Scholar] [CrossRef]
- Tan, Y.; Hu, B.; Li, Q.; Cao, W. Prognostic value and clinicopathological significance of pre-and post-treatment systemic immune-inflammation index in colorectal cancer patients: A meta-analysis. World J. Surg. Oncol. 2025, 23, 11. [Google Scholar] [CrossRef]
- Hai-Jing, Y.; Shan, R.; Jie-Qiong, X. Prognostic significance of the pretreatment pan-immune-inflammation value in cancer patients: An updated meta-analysis of 30 studies. Front. Nutr. 2023, 10, 1259929. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.C.; Liu, H.; Liu, D.C.; Tong, C.; Liang, X.W.; Chen, R.H. Prognostic value of pan-immune-inflammation value in colorectal cancer patients: A systematic review and meta-analysis. Front. Oncol. 2022, 12, 1036890. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Chen, H.; Chen, Z.; Tan, J.; Wu, F.; Li, X. Prognostic value of neutrophil-to-lymphocyte ratio in patients with hepatocellular carcinoma receiving curative therapies: A systematic review and meta-analysis. BMC Cancer 2025, 25, 571. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Wang, Y.; Jiang, Y.; Yang, J.; Zhang, Y. The prognostic impact of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio on patients with small cell lung cancer receiving first-line platinum-based chemotherapy: A systematic review and meta-analysis. BMC Pulm. Med. 2024, 24, 630. [Google Scholar] [CrossRef]
- Zhang, J.H.; Huang, D.H.; Chen, Z.Y. Prognostic role of systemic immune-inflammation index in solid tumors: A systematic review and meta-analysis. Oncotarget 2017, 8, 75381–75388. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhao, Y.; Wen, J.; Wang, Y.; Li, J. Impact of systemic immune-inflammation index and its evaluation of optimal threshold in patients with limited-stage small cell lung cancer: A retrospective study based on 572 cases. Transl. Cancer Res. 2025, 14, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Yin, P.; Jiao, B.; Shi, Z.; Qiao, F.; Xu, J. Detecting the preoperative peripheral blood systemic immune-inflammation index (SII) as a tool for early diagnosis and prognosis of gallbladder cancer. BMC Immunol. 2025, 26, 7. [Google Scholar] [CrossRef]
- Bal, O.; Acikgoz, Y.; Yildiz, B.; Kos, F.T.; Algin, E.; Dogan, M. Simple and easily accessible prognostic markers in ewing sarcoma; neutrophil-lymphocyte ratio, neutrophil-platelet score and systemic-inflammation index. J. Cancer Res. Ther. 2023, 19, 1241–1247. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.; Xue, J.; Yang, L.; Xia, L.; He, W. Predictive value of prognostic nutritional and systemic immune-inflammation indices for patients with microsatellite instability-high metastatic colorectal cancer receiving immunotherapy. Front. Nutr. 2023, 10, 1094189. [Google Scholar] [CrossRef]
- Chen, X.; Hong, X.; Chen, G.; Xue, J.; Huang, J.; Wang, F.; Ali, W.; Li, J.; Zhang, L. The Pan-Immune-Inflammation Value predicts the survival of patients with anaplastic lymphoma kinase-positive non-small cell lung cancer treated with first-line ALK inhibitor. Transl. Oncol. 2022, 17, 101338. [Google Scholar] [CrossRef]
- Fu, F.; Deng, C.; Wen, Z.; Gao, Z.; Zhao, Y.; Han, H.; Zheng, S.; Wang, S.; Li, Y.; Hu, H.; et al. Systemic immune-inflammation index is a stage-dependent prognostic factor in patients with operable non-small cell lung cancer. Transl. Lung Cancer Res. 2021, 10, 3144–3154. [Google Scholar] [CrossRef]
- Howard, R.; Kanetsky, P.A.; Egan, K.M. Exploring the prognostic value of the neutrophil-to-lymphocyte ratio in cancer. Sci. Rep. 2019, 9, 19673. [Google Scholar] [CrossRef]
- Yang, R.; Chang, Q.; Meng, X.; Gao, N.; Wang, W. Prognostic value of Systemic immune-inflammation index in cancer: A meta-analysis. J. Cancer 2018, 9, 3295–3302. [Google Scholar] [CrossRef]
- Hou, Y.; Li, X.; Yang, Y.; Shi, H.; Wang, S.; Gao, M. Serum cytokines and neutrophil-to-lymphocyte ratio as predictive biomarkers of benefit from PD-1 inhibitors in gastric cancer. Front. Immunol. 2023, 14, 1274431. [Google Scholar] [CrossRef]
- Guan, Y.; Xiong, H.; Feng, Y.; Liao, G.; Tong, T.; Pang, J. Revealing the prognostic landscape of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in metastatic castration-resistant prostate cancer patients treated with abiraterone or enzalutamide: A meta-analysis. Prostate Cancer Prostatic Dis. 2020, 23, 220–231. [Google Scholar] [CrossRef] [PubMed]
- Sanz, J.; Boluda, J.C.; Martín, C.; et al. Single-unit umbilical cord blood transplantation from unrelated donors in patients with hematological malignancy using busulfan, thiotepa, fludarabine and ATG as myeloablative conditioning regimen. Bone Marrow Transplant. 2012, 47, 1287–1293. [Google Scholar] [CrossRef]
- Sanz, G.F.; Saavedra, S.; Planelles, D.; et al. Standardized, unrelated donor cord blood transplantation in adults with hematologic malignancies Blood. 2001, 98, 2332–2338. [Google Scholar] [CrossRef]
- Seigers, R.; Fardell, J.E. Neurobiological basis of chemotherapy-induced cognitive impairment: A review of rodent research. Neurosci. Biobehav. Rev. 2011, 35, 729–741. [Google Scholar] [CrossRef]
- Uckan, D.; Çetinkaya, D.U.; Yigitkanli, I.; Tezcan, I.; Tuncer, M.; Karasimav, D.; Oguz, K.K.; Topcu, M. Life-threatening neurological complications after bone marrow transplantation in children. Bone Marrow Transplant. 2004, 35, 71–7. [Google Scholar] [CrossRef]
- Koh, K.N.; Park, M.; Kim, B.E.; Im, H.J.; Seo, J.J. Early central nervous system complications after allogeneic hematopoietic stem cell transplantation in children. Korean J. Hematol. 2010, 45, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Sanz, J.; Picardi, A.; Hernández Boluda, J.C.; et al. Impact of graft-versus-host disease prophylaxis on outcomes after myeloablative single-unit umbilical cord blood transplantation. Biol Blood Marrow Transplant. 2013, 19, 1387–1392. [Google Scholar] [CrossRef]
- Hinchey, J.; Chaves, C.; Appignani, B.; et al. A reversible posterior leukoencephalopathy syndrome N. Engl J Med. 1996, 334, 494–500. [Google Scholar] [CrossRef]
- Feske, S.K. Posterior reversible encephalopathy syndrome: a review. Semin Neurol 2011, 31, 202–215. [Google Scholar] [CrossRef]
- Balaguer-Rosello, A.; Bataller, L.; Lorenzo, I.; et al. Infections of the central nervous system after unrelated donor umbilical cord blood transplantation or human leukocyte antigen-matched sibling transplantation. Biol Blood Marrow Transplant. 2017, 23, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Gray, R.J. A class of K-sample tests for comparing the cumulative incidence of a competing risk. Ann Stat. 1988, 16, 1141–1154. [Google Scholar] [CrossRef]
- Evans, LE; Taylor, JL; Smith, CJ; et al. Cardiovascular comorbidities, inflammation, and cerebral small vessel disease. Cardiovasc Res. 2021, 117(13), 2575–2588. [Google Scholar] [CrossRef]
- Rawish, E; Nording, H; Münte, T; et al. Platelets as mediators of neuroinflammation and thrombosis. Front Immunol. 2020, 11, 548631. [Google Scholar] [CrossRef]
- Cox, D.R. Regression models and life-tables. J R Stat Soc Ser B Methodol. 1972, 34, 187–202. [Google Scholar] [CrossRef]
- Mantel, N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother Rep. 1966, 50, 163–170. [Google Scholar]
- Siegal, D.; Keller, A.; Xu, W.; et al. Central nervous system complications after allogeneic hematopoietic stem cell transplantation: incidence, manifestations, and clinical significance. Biol Blood Marrow Transplant. 2007, 13, 1369–1379. [Google Scholar] [CrossRef] [PubMed]
- Narimatsu, H.; Miyamura, K.; Iida, H.; et al. Early central nervous complications after umbilical cord blood transplantation for adults. Biol Blood Marrow Transplant. 2009, 15, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Husain, S. Infections of the central nervous system in transplant recipients. Transpl Infect Dis. 2000, 2, 101–111. [Google Scholar] [CrossRef]
- Beitinjaneh, A.; McKinney, A.M.; Cao, Q.; et al. Toxic leukoencephalopathy following fludarabine-associated hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2011, 17, 300–308. [Google Scholar] [CrossRef]
- Rambaldi, A.; Grassi, A.; Masciulli, A. Busulfan plus cyclophosphamide versus busulfan plus fludarabine as a preparative regimen for allogeneic haemopoietic stem-cell transplantation in patients with acute myeloid leukaemia: an open-label, multicentre, randomised, phase 3 trial. Lancet Oncol. 2015, 16, 1525–1536. [Google Scholar] [CrossRef]
- Hernández-Boluda, J.C.; Lis, M.J.; Goterris, R.; et al. Guillain-Barré syndrome associated with cytomegalovirus infection after allogeneic hematopoietic stem cell transplantation. Transpl Infect Dis. 2005, 7, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Antonini, G.; Ceschin, V.; Morino, S.; et al. Early neurologic complications following allogeneic bone marrow transplant for leukemia: a prospective study. Neurology 1998, 50, 1441–1445. [Google Scholar] [CrossRef] [PubMed]
- Barba, P.; Piñana, J.L.; Valcárcel, D.; et al. Early and late neurological complications after reduced-intensity conditioning allogeneic stem cell transplantation. Biol Blood Marrow Transplant. 2009, 15, 1439–1446. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



