Submitted:
24 February 2026
Posted:
25 February 2026
You are already at the latest version
Abstract
Objective: To screen the independent risk factors for 30-day postoperative complications in patients with arteriosclerosis obliterans of the lower extremities (ASO), construct and validate a visualized nomogram prediction model, and provide a quantitative tool for perioperative risk assessment and individualized intervention. Methods: A single-center retrospective cohort study was performed to collect clinical data from ASO patients who underwent surgical treatment. Univariate and multivariate Logistic regression analyses were used to screen independent risk factors and establish the nomogram. The discrimination, calibration and clinical utility of the model were evaluated by Bootstrap internal validation, receiver operating characteristic (ROC) curve, calibration curve and optimal cutoff value analysis. Results: Advanced age, smoking history, diabetes mellitus, and preoperative ankle-brachial index (ABI) < 0.4 were independent risk factors for 30-day postoperative complications in ASO patients (P < 0.05). The C-index and area under the curve (AUC) of the model were both 0.806 (95%CI: 0.762–0.851), and the Bootstrap-corrected C-index was 0.799, indicating good discrimination. The calibration curve showed favorable overall agreement, and the Hosmer–Lemeshow test yielded χ² = 7.234 (P = 0.512), suggesting satisfactory calibration. The optimal diagnostic performance was obtained at the cutoff value of 0.29, with a sensitivity of 69.91%, specificity of 82.24%, and Youden index of 0.522. Conclusion: The nomogram model constructed in this study exhibits favorable predictive performance, is intuitive and easy to apply, and can accurately assess the risk of postoperative complications. It provides a reliable basis for perioperative risk stratification and optimized intervention strategies in clinical practice, with high value for clinical application and popularization.
Keywords:
arteriosclerosis obliterans of the lower extremities
; ankle-brachial index
; postoperative complications
; nomogram
; prediction model
; risk factors
1. Introduction
Arteriosclerosis obliterans (ASO) of the lower extremities represents a local manifestation of systemic atherosclerosis involving the lower extremity vasculature. Its incidence has been rising annually alongside the accelerating global population aging and high prevalence of metabolic diseases[1]. Despite the remarkable improvement in limb salvage rates achieved by advances in endovascular intervention and open surgical techniques, postoperative complications—including puncture-site hematoma, incision infection, lymphatic leakage, and thrombosis—still occur frequently, with a reported incidence ranging from 10% to 25% in clinical studies[2].
Previous relevant studies have mostly focused on the optimization of surgical approaches and evaluation of postoperative vascular patency, whereas targeted quantitative predictive tools for short-term postoperative complications remain scarce. The ankle-brachial index (ABI), a classic non-invasive indicator that assesses the severity of lower extremity ischemia by measuring the ratio of ankle to brachial systolic blood pressure, serves as the gold standard for the diagnosis of ASO. In recent years, multiple studies have confirmed that ABI not only reflects the severity of macrovascular lesions in the lower extremities but also acts as a biomarker of systemic vascular function, and is closely associated with adverse cardiovascular events and postoperative prognosis[3]. However, the clinical application of ABI is currently mostly limited to the diagnosis and severity grading of ASO; its value in predicting non-vascular postoperative complications has not been fully quantified. Moreover, visualized risk prediction models integrating ABI with patients’ baseline clinical characteristics are still lacking in clinical practice.
Based on the large-sample retrospective clinical data from Drum Tower Hospital Affiliated to Nanjing University School of Medicine, this study screened independent risk factors for short-term postoperative complications in patients with ASO and constructed a nomogram model for predicting postoperative complications by integrating preoperative ABI and clinical characteristics. This model aims to provide a simple and accurate assessment tool for perioperative risk stratification and management in ASO patients, thereby reducing the incidence of postoperative complications and improving surgical outcomes.
2. Materials and Methods
2.1. Study Subjects
A total of 512 patients with arteriosclerosis obliterans (ASO) admitted to the Department of Vascular Surgery of our hospital from January 2023 to January 2025 were retrospectively enrolled. Among them, 33 patients received only conservative treatment due to advanced age, poor physical condition, or refusal of surgery, and the remaining 479 patients who underwent surgical treatment were included in the model development cohort.
Inclusion criteria: ① Met the diagnostic criteria specified in the Guidelines for the Diagnosis and Treatment of Arteriosclerosis Obliterans of the Lower Extremities (2017 Edition); ② Confirmed by computed tomography angiography (CTA) or digital subtraction angiography (DSA); ③ With complete clinical baseline data and preoperative ankle-brachial index (ABI) measurements; ④ Underwent endovascular intervention or open surgical treatment.
Exclusion criteria: ① Complicated with severe psychiatric disorders or cognitive impairment, unable to cooperate with diagnosis, treatment and follow-up; ② History of ipsilateral lower extremity amputation; ③ Complicated with severe coagulopathy (international normalized ratio > 2.0) or bleeding diathesis; ④ Complicated with malignant tumors, severe hepatic or renal failure, or other end-stage systemic diseases.
The study protocol was approved by the Medical Ethics Committee of Drum Tower Hospital Affiliated to Nanjing University School of Medicine in November 2022 (approval number: 2022-256-01). All study procedures were performed in accordance with medical ethical standards. All included patients had complete clinical data with no missing values.
2.2. Sample Size Calculation
According to the principles of sample size estimation for Logistic regression models, each predictive variable requires at least 10–15 outcome events (Events Per Variable, EPV)[4]。This study planned to include 5 candidate predictive variables (age, smoking history, diabetes mellitus history, preoperative ABI, and surgical method), assuming a complication incidence of approximately 23.6%. The minimum required sample size was calculated as follows: (5 variables × 15 EPV) / 0.236 ≈ 318 cases. A total of 479 patients were finally enrolled, and the sample size was sufficient to meet statistical requirements.
2.3. Data Collection
Baseline clinical data of patients were extracted from the hospital electronic medical record system, including gender, age, body mass index (BMI), smoking history (defined as smoking ≥ 10 cigarettes per day for ≥ 1 year), and comorbidities (hypertension, diabetes mellitus, and coronary heart disease). All patients had complete clinical data with no missing values.
The ankle-brachial index (ABI) of all patients was measured using a standardized method within 1 week before surgery: after the patients rested in a supine position for 10 minutes, a Doppler ultrasound device was used to measure the systolic blood pressure of the bilateral brachial arteries, dorsalis pedis arteries, and posterior tibial arteries. The ratio of the highest ankle arterial systolic blood pressure to the highest brachial arterial systolic blood pressure was taken as the ABI value of the patient.
According to previous literature and clinical practice experience[5]-[6], ABI < 0.4 corresponds to Rutherford classification grades 4–6, indicating critical limb ischemia, which is a clinically recognized important cutoff point. In this study, ABI was first included as a continuous variable in the preliminary analysis, and a restricted cubic spline was used to fit its relationship with complication risk. The results showed an obvious risk inflection point around ABI = 0.4. Further comparison of model fit among different cutoff values (0.3, 0.4, 0.5) revealed that the Akaike Information Criterion (AIC) value of the dichotomous model with 0.4 as the cutoff (447.6) was significantly better than that of the continuous variable model (452.3) and models with other cutoff values. Therefore, considering clinical guideline recommendations, spline curve analysis results, and model goodness of fit, ABI was finally dichotomized with 0.4 as the cutoff: ABI ≥ 0.4 was defined as the relatively mild to moderate ischemia group, and ABI < 0.4 as the critical ischemia group[7]。
Meanwhile, surgical methods were extracted from surgical records, including endovascular intervention, open surgery, and hybrid surgery.
2.4. Outcome Measures
The primary outcome measure of this study was the occurrence of complications within 30 days after surgery, specifically including bleeding/hematoma at the puncture or incision site, surgical site infection, lymphatic leakage, acute arterial thrombosis, deep vein thrombosis, and cardiovascular and cerebrovascular accidents. All complications were diagnosed in accordance with the diagnostic criteria specified in the 9th Edition of Surgery and relevant clinical practice guidelines. The diagnosis was independently completed by two senior vascular surgeons. In case of divergent opinions, a unified conclusion was reached through collective departmental consultation. For patients with multiple complications, only one event was counted per patient to avoid duplicate calculation[8]。
2.5. Statistical Methods
Data analysis was performed using SPSS 26.0 statistical software and R software (version 4.5.2, with the rms, pROC, ggplot2, and dplyr packages loaded). After passing the normality test, measurement data conforming to a normal distribution were expressed as the mean ± standard deviation (x̄±s), and between-group comparisons were conducted using the independent-sample t-test. Enumeration data were presented as case number (percentage) [n (%)], and between-group comparisons were performed using the Chi-square (χ²) test.
Potential risk factors for postoperative complications were screened via univariate analysis. Variables with P<0.05 in the univariate analysis were included in the multivariate Logistic regression model, and the forward stepwise regression method was used to identify independent risk factors for postoperative complications[9]. Based on the screened independent risk factors, a nomogram prediction model was constructed using the rms package in R.
Internal validation of the model was performed using the Bootstrap method with 1000 resamplings to correct for model overfitting, and the adjusted C-index and optimism were calculated. The concordance index (C-index, equivalent to the area under the receiver operating characteristic curve, AUC) was used to evaluate the model’s discrimination: a value closer to 1 indicated better discrimination. Generally, a C-index of 0.5–0.7 was considered low discrimination, 0.7–0.8 moderate to good discrimination, and >0.8 excellent discrimination.
Calibration curves were plotted to assess the consistency between the predicted probability of complication occurrence and the actual incidence. The Hosmer–Lemeshow goodness-of-fit test was used for quantitative evaluation of calibration, with P>0.05 indicating satisfactory model calibration. The optimal risk cutoff value of the model was determined using the Youden index (sensitivity + specificity − 1). All statistical tests were two-sided, and P<0.05 was considered statistically significant[10]。
3. Results
3.1. Baseline Characteristics of Patients
A total of 512 patients with arteriosclerosis obliterans (ASO) were enrolled in this study, with a mean age of 69.4±8.2 years, including 474 males (92.6%). Among them, 479 patients were in the surgical treatment group and 33 patients in the conservative treatment group. The comparison of baseline characteristics between the two groups showed that the mean age and preoperative average ABI value in the conservative treatment group were significantly higher than those in the surgical treatment group (with P values of 0.001 and 0.003, respectively). However, no statistically significant differences were observed in gender, body mass index (BMI), smoking history, or the comorbidity rates of hypertension, diabetes mellitus, and coronary heart disease between the two groups (all P > 0.05)[11], indicating that the baseline characteristics of the two groups were comparable. Details are shown in Table 1.
3.2. Univariate Analysis of Postoperative Complications
Among the 479 ASO patients who underwent surgical treatment, 113 (23.6%) developed complications within 30 days after surgery. The distribution of main complication types in these 113 patients was as follows: 41 cases (36.28%) of puncture site/incision hematoma, 23 cases (20.35%) of surgical site infection, 19 cases (16.81%) of deep vein thrombosis, 13 cases (11.50%) of acute arterial thrombosis, 10 cases (8.85%) of lymphatic leakage, and 7 cases (6.19%) of cardiovascular and cerebrovascular accidents.
The results of univariate analysis showed that the age (70.6±7.9 years vs. 67.3±8.2 years), proportion of smoking history (72.6% vs. 60.1%), and proportion of diabetes mellitus history (51.3% vs. 40.2%) in the complication group were significantly higher than those in the non-complication group, while the mean preoperative ABI value (0.31±0.12 vs. 0.43±0.10) was significantly lower than that in the non-complication group (all P < 0.05). Surgical method was associated with the incidence of postoperative complications: the complication rate in patients who underwent open/hybrid surgery (18.6%) was higher than that in patients who underwent endovascular intervention (8.4%) (P = 0.002). No statistically significant differences were found in gender, BMI, hypertension history, or coronary heart disease history between the two groups (all P > 0.05). Details are shown in Table 2.
3.3. Multivariate Logistic Regression Analysis and Nomogram Model Construction
Variables with P<0.05 in the univariate analysis (age, smoking history, diabetes mellitus history, preoperative ABI, and surgical method) were included in the multivariate Logistic regression model.
The results of multivariate Logistic regression analysis showed that advanced age (OR=1.08, 95%CI: 1.03-1.14, P=0.003), smoking history (OR=1.88, 95%CI: 1.02-3.36, P=0.043), diabetes mellitus history (OR=2.40, 95%CI: 1.36-3.47, P=0.005), and preoperative ABI < 0.4 (OR=3.04, 95%CI: 1.39-6.64, P=0.005) were independent risk factors for 30-day postoperative complications in ASO patients (all P < 0.05). Surgical method did not reach statistical significance in the multivariate analysis (OR=1.05, 95%CI: 0.55-2.00, P=0.886), which may be related to the small sample size of open/hybrid surgery (49 cases, 10.2%) and insufficient statistical power. Details are shown in Table 3.
Based on the independent risk factors (age, smoking history, diabetes mellitus history, and preoperative ABI < 0.4) screened by multivariate Logistic regression, a nomogram model was constructed using the rms package in R software. This model integrates the risk contribution of the above factors and visually maps the occurrence probability of 30-day postoperative complications in ASO patients [12]. The nomogram scoring system is shown in Figure 1.
3.4. Model Performance Validation
3.4.1. Discrimination Evaluation
The concordance index (C-index) of the internal nomogram prediction model was 0.806 (95%CI: 0.762-0.851), and the area under the receiver operating characteristic (ROC) curve (AUC) was 0.806, indicating that the model had good discrimination.
Internal validation was performed via 1000 Bootstrap resamplings. The adjusted C-index was 0.799 with an optimism of 0.008, suggesting a low overfitting risk and good stability of the model. The ROC curve is shown in Figure 2.
3.4.2. Calibration Evaluation
The calibration curve showed (Figure 3) that the model had good agreement with the actual complication incidence in the low and medium predicted probability intervals, with mild deviation in the high predicted probability interval, and overall exhibited good predictive consistency and calibration ability. The Hosmer–Lemeshow goodness-of-fit test yielded χ² = 7.234 (P = 0.512), indicating good calibration of the model, with no significant difference between the predicted probabilities and actual observed values.
3.4.3. Optimal Cutoff Value Analysis
Analysis of diagnostic efficacy at different risk cutoff values showed (Table 4) that the optimal risk cutoff value of the model was 0.29. At this cutoff value, the Youden index reached its maximum value of 0.522, with a model sensitivity of 69.91%, specificity of 82.24%, positive predictive value of 54.86%, negative predictive value of 89.85%, and accuracy of 79.33%. This indicated the optimal diagnostic efficacy and the highest clinical application value. This cutoff value can be used for clinical risk stratification: patients with a predicted risk > 0.29 are classified as high-risk groups, requiring enhanced perioperative monitoring and preventive intervention (Figure 4).
4. Discussion
This study adopted a single-center large-sample retrospective cohort design, screened and identified advanced age, smoking history, diabetes mellitus history, and preoperative ABI < 0.4 as independent risk factors for 30-day postoperative complications in ASO patients, and constructed a visualized nomogram prediction model based on these factors. Among them, preoperative ABI < 0.4 was the risk factor with the highest weight (OR=3.04, 95%CI: 1.39-6.64), confirming that severe lower extremity ischemia is the core driving factor for postoperative complications.
4.1. Correlation Mechanism Between Preoperative ABI and Postoperative Complications
As a classic indicator for evaluating the severity of lower extremity ischemia, the correlation mechanism between preoperative ABI and postoperative complications may be as follows: when ABI < 0.4, lower extremity tissues are in a state of severe ischemia and hypoxia. Insufficient microcirculatory perfusion leads to decreased healing ability of skin and subcutaneous tissues and weakened anti-infection ability, thereby increasing the risk of incision infection, hematoma, and lymphatic leakage. Meanwhile, severe lower extremity ischemia often indicates extensive systemic atherosclerotic lesions; patients are often complicated with cardiovascular and cerebrovascular diseases and other multi-system vascular lesions, resulting in a significantly increased risk of thrombosis and cardiovascular and cerebrovascular accidents after surgery[13].
4.2. Clinical Significance of Other Independent Risk Factors
Diabetes mellitus history and smoking history are important risk factors for postoperative complications in ASO patients, which is consistent with the conclusions of previous studies. Patients with diabetes mellitus have glucose metabolism disorders and microangiopathy, which will further aggravate lower extremity tissue ischemia; at the same time, low immune function is prone to induce infection. Smoking can damage vascular endothelial cells, promote platelet aggregation and thrombosis, and increase the risk of postoperative arterial thrombosis and deep vein thrombosis. In addition, elderly patients have decreased body compensatory capacity and numerous underlying comorbidities, leading to a significantly increased risk of postoperative complications. Therefore, enhanced perioperative monitoring and management are required in clinical practice[14].
4.3. Clinical Application Value of the Nomogram Model
The nomogram model constructed in this study has the following advantages:
First, all included indicators are routine parameters easily accessible in clinical practice. No complex laboratory examinations or imaging evaluations are required, resulting in strong clinical accessibility and simple operation, which is suitable for clinical promotion.
Second, the model intuitively presents the individual risk of postoperative complications in a visualized form. Clinicians and nurses can complete risk stratification within a few minutes, providing a basis for formulating individualized intervention strategies.
Third, the model has stable and reliable predictive efficacy. After Bootstrap internal validation, the original C-index was 0.806, the adjusted C-index was 0.799, and the optimism was only 0.008, indicating a low risk of model overfitting. The calibration curve showed good overall agreement, and the Hosmer–Lemeshow test yielded P=0.512, indicating excellent calibration. When the risk cutoff value was set at 0.29, the model had both excellent sensitivity (69.91%) and specificity (82.24%), with a high negative predictive value of 89.85%, which can effectively screen low-risk patients and avoid overmedicalization.
Fourth, it guides individualized intervention. According to the model score, patients can be divided into three groups: low-risk (<0.20), medium-risk (0.20-0.40), and high-risk (>0.40). For high-risk patients, the following clinical intervention measures can be taken:
Preoperative optimization: Strictly control blood glucose (<7.0 mmol/L), enforce smoking cessation for at least 2 weeks, and improve lower extremity perfusion (staged surgery if necessary);
Intraoperative refined operation: Shorten operation time, reduce tissue damage, and strengthen hemostasis;
Postoperative intensive management: Enhance incision care, prophylactic use of antibiotics, early anticoagulation to prevent thrombosis, and close monitoring of cardiovascular and cerebrovascular events.
4.4. Clinical Explanation for Higher ABI in the Conservative Treatment Group
This study found that the preoperative ABI in the conservative treatment group (0.45±0.10) was significantly higher than that in the surgical treatment group (0.38±0.12, P=0.003). Although this phenomenon seems contradictory, it is consistent with clinical practice. Patients in the conservative treatment group were older (73.5±7.9 vs 69.1±8.1, P=0.001). Despite the relatively higher ABI, surgical treatment was not chosen because comprehensive evaluation showed that the surgical risk outweighed the benefits due to advanced age, poor physical condition, numerous comorbidities (such as severe cardiac insufficiency and poor pulmonary function), and poor surgical tolerance[15]. This suggests that clinical decision-making cannot rely solely on the single indicator of ABI, but needs to comprehensively consider various factors such as the patient’s overall condition, severity of comorbidities, and surgical tolerance.
4.5. Limitations of the Study
This study has several limitations:
First, it was a single-center retrospective study. The study samples were geographically concentrated in Jiangsu Province, with potential selection bias. The external applicability of the model needs to be verified by multi-center prospective studies.
Second, sample size limitation. Although the total sample size reached 479 cases, only 49 cases (10.2%) underwent open/hybrid surgery, which may lead to insufficient statistical power of this variable. Future studies need to expand the sample size for further verification.
Third, failure to include some potential factors. This study did not include factors such as postoperative medication (e.g., type and dose of anticoagulant drugs), rehabilitation intervention, nutritional status, and inflammatory indicators (e.g., C-reactive protein, white blood cell count), which may affect the completeness of the model. Future studies can further improve this.
Fourth, lack of external validation. The model only underwent Bootstrap internal validation and no external cohort validation. The universality of the model needs to be further confirmed through multi-center studies to verify its clinical promotion value.
Fifth, short follow-up time. This study only observed short-term complications within 30 days after surgery and did not evaluate long-term prognosis (such as vascular patency rate, amputation rate, and survival rate). Future studies need to extend the follow-up time and construct a long-term prognosis prediction model.
5. Conclusion
In summary, advanced age, smoking history, diabetes mellitus history, and preoperative ABI < 0.4 are independent risk factors for 30-day postoperative complications in patients with arteriosclerosis obliterans of the lower extremities, among which preoperative ABI < 0.4 has the highest predictive weight. The nomogram model constructed in this study has good predictive efficacy (C-index=0.806, Bootstrap-adjusted C-index=0.799) and excellent calibration (H-L test P=0.512). It can intuitively and individually assess the risk of postoperative complications, provide a quantitative tool for perioperative risk stratification and clinical decision-making, and has high clinical practical value. Future studies need to conduct external validation through multi-center prospective studies and explore the inclusion of more biomarkers to further improve prediction accuracy.
6. Declarations
Written informed consent has been obtained from the patient(s) to publish this paper.
All date supporting the findings of this study are available within the paper.
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
This manuscript has not been published or presented elsewhere in part or in entirety, and is not under consideration by another journal. All the authors have approved the manuscript and agree with submission to your esteemed journal.
This study was supported by the following grants: National Natural Science Foundation for Young Scientists of China (Grant No. 82100517); Natural Science Foundation of Jiangsu Province (Grant No. SBK2020042213).
All authors made substantial contributions to the conception, data collection, statistical analysis, drafting and revision of the study, and have read and approved the final manuscript.
References
- Victor, A; Jean-Baptiste, R. The ‘Ten Commandments’ of 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases. European heart journal 2018, 39(9), 722. [Google Scholar]
- Jie, Z; Guojun, Z; Lin, Z. Implementation of holistic nursing interventions based on fast track surgery concept in patients with lower extremity arterial occlusive disease[J]. Medicine 2023, 102(49), e36485. [Google Scholar]
- R G F F ,D G M ,I B , et al. Ankle Brachial Index Combined With Framingham Risk Score to Predict Cardiovascular Events and Mortality: A Meta-analysis[J]. JAMA: The Journal of the American Medical Association 2008, 300(2), 197–208.
- L N ,R W H ,A J D , et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II).[J]. Journal of vascular surgery 2007, 45, Suppl SS5-67.
- Conte, S.M.; Bradbury, W.A.; Kolh, P. Global vascular guidelines on the management of chronic limb-threatening ischemia[J]. Journal of Vascular Surgery 2019, 69(6), 3S-125S.e40. [Google Scholar] [CrossRef] [PubMed]
- Moshkele, H.M.; Mirmoosavi, S.; Najafi, T.M. Low Ankle-Brachial Index Is Associated With Albuminuria and Diabetic Kidney Disease in Type 2 Diabetes; A Cross Sectional Study.[J]. Endocrinology, diabetes & metabolism 2025, 8(6), e70115. [Google Scholar]
- Bhasin, N; Scott, A J D. Ankle Brachial Pressure Index: identifying cardiovascular risk and improving diagnostic accuracy[J]. Journal of the Royal Society of Medicine 2007, 100(1), 4–5. [Google Scholar] [CrossRef] [PubMed]
- Che, D; Jiang, Z; Xiang, X. Predictors of amputation in patients with diabetic foot ulcers: a multi-centre retrospective cohort study. Endocrine 2024, 85(1), 181–189. [Google Scholar] [CrossRef] [PubMed]
- Tang, T; Shen, Y; Bai, X. Predicting surgical site infections using a novel nomogram in patients undergoing hepatectomy[J]. HPB 2019, 21(S2), S361–S361. [Google Scholar] [CrossRef]
- Lai, J; Lin, P; Zhuang, J. Development and internal validation of a nomogram based on peripheral blood inflammatory markers for predicting prognosis in nasopharyngeal carcinoma.[J]. Cancer medicine 2024, 13(7), e7135–e7135. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G; Yi, Q; Tong, Y. Effect of Different Antithrombotic Regimens to Prevent Postoperative Restenosis in Patients With Lower Extremity Arteriosclerosis[J]. American Journal of Therapeutics 2021, 28(4), e517–e520. [Google Scholar]
- ZN, C; K, W; GX, Z. A nomogram to predict major adverse cardiovascular events of patients with acute chest pain, Non-ST-segment deviation, and normal troponin concentrations.[J]. European review for medical and pharmacological sciences 2020, 24(19), 10096–10106. [Google Scholar]
- Sorensen, M C; Abramowitz, D S; Malik, K R. Inter-Society Consensus for the Management of Peripheral Arterial Disease Correlates Better Than the Society for Vascular Surgery Lower Extremity Threatened Limb Classification Based on Wound, Ischemia, and foot Infection (WIfI) in Predicting Major Amputation[J]. Journal of Vascular Surgery 2016, 64(3), 837–838. [Google Scholar]
- Manabe, D; Arizumi, T; Aoyagi, H. Risk factors for post-endoscopic retrograde cholangiopancreatography complications in very elderly patients aged 90 years or older-No additional risk.[J]. Geriatrics & gerontology international 2024, 25(1), 54–60. [Google Scholar]
- G, S H; B, D S; MuhammadSaad, H. Trends In Mortality And Post-Operative Complications Among Octogenarian Patients Undergoing Carotid Endarterectomy.[J]. Journal of vascular surgery 2023, 78(1), 132–140.e2. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Nomogram for Predicting the Risk of 30-Day Postoperative Complications in ASO Patients.
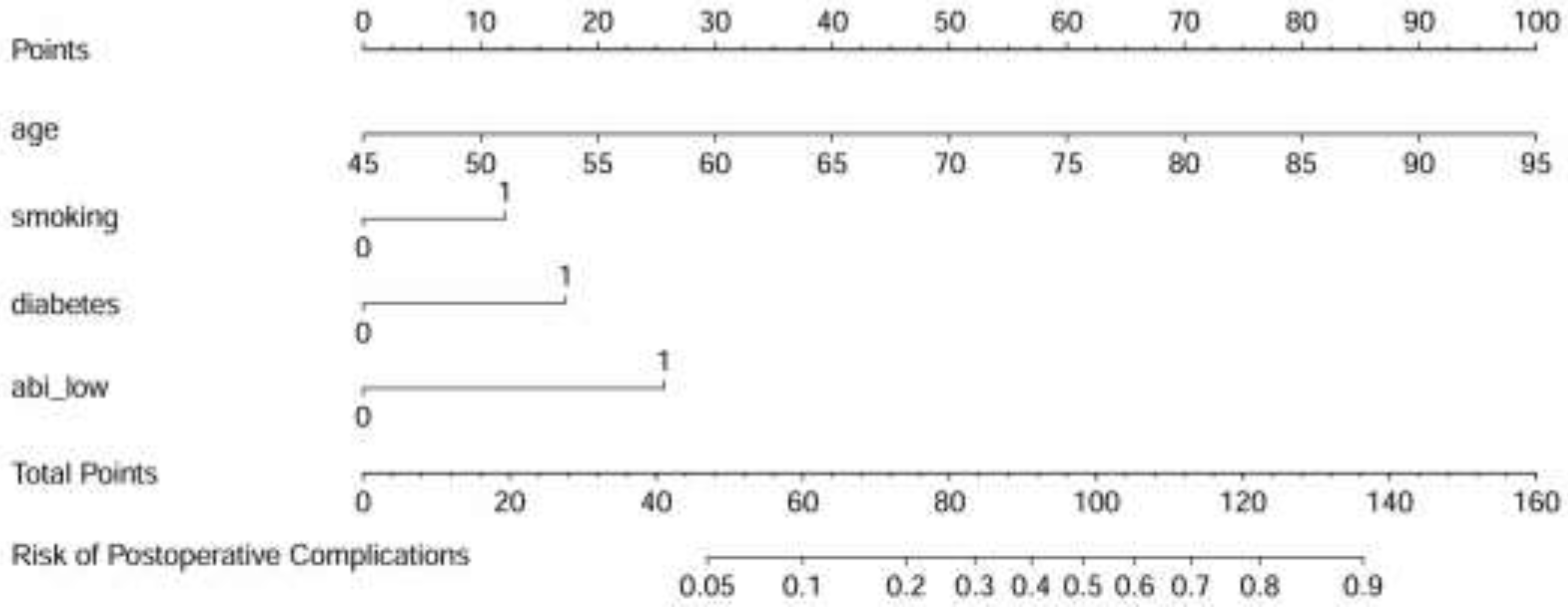
Figure 2.
Receiver Operating Characteristic (ROC) Curve of the Prediction Model for Postoperative Complications in Patients with Arteriosclerosis Obliterans of the Lower Extremities.
Figure 2.
Receiver Operating Characteristic (ROC) Curve of the Prediction Model for Postoperative Complications in Patients with Arteriosclerosis Obliterans of the Lower Extremities.
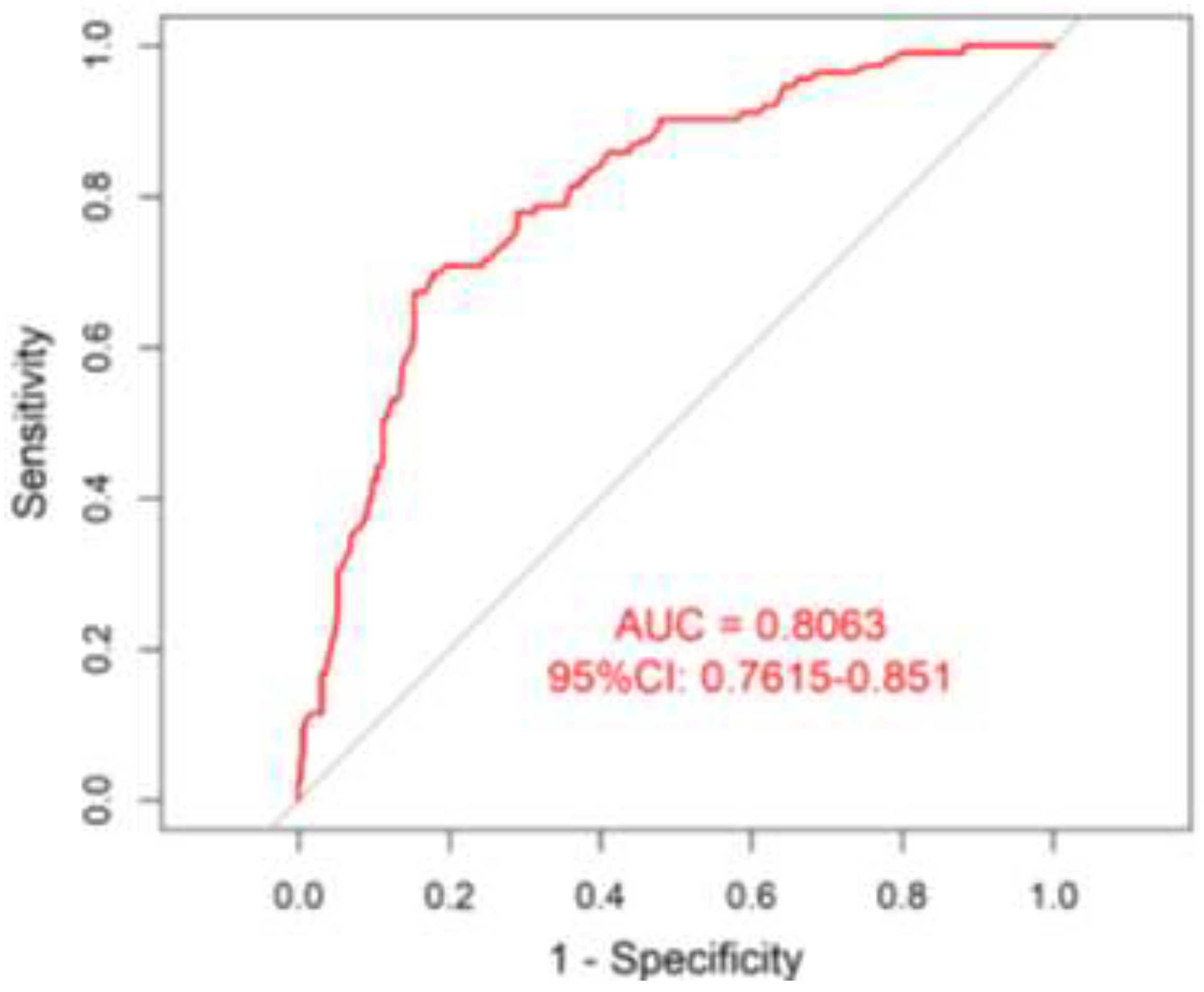
Figure 3.
Calibration Curve of the Postoperative Complication Risk Prediction Model Validated by the Bootstrap Method.
Figure 3.
Calibration Curve of the Postoperative Complication Risk Prediction Model Validated by the Bootstrap Method.
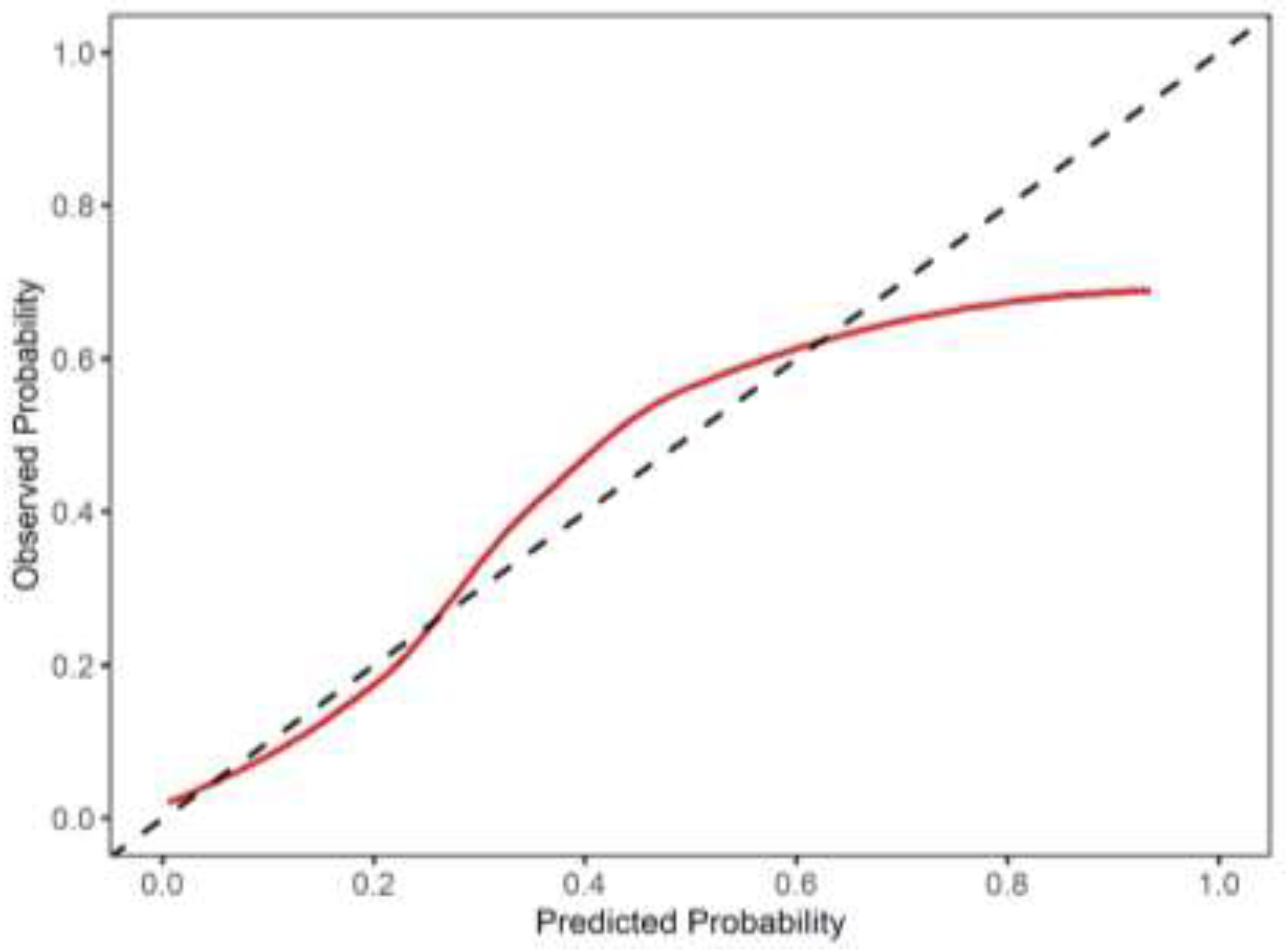
Figure 4.
Youden Index Curve and Optimal Cutoff Value of the Postoperative Complication Risk Prediction Model.
Figure 4.
Youden Index Curve and Optimal Cutoff Value of the Postoperative Complication Risk Prediction Model.
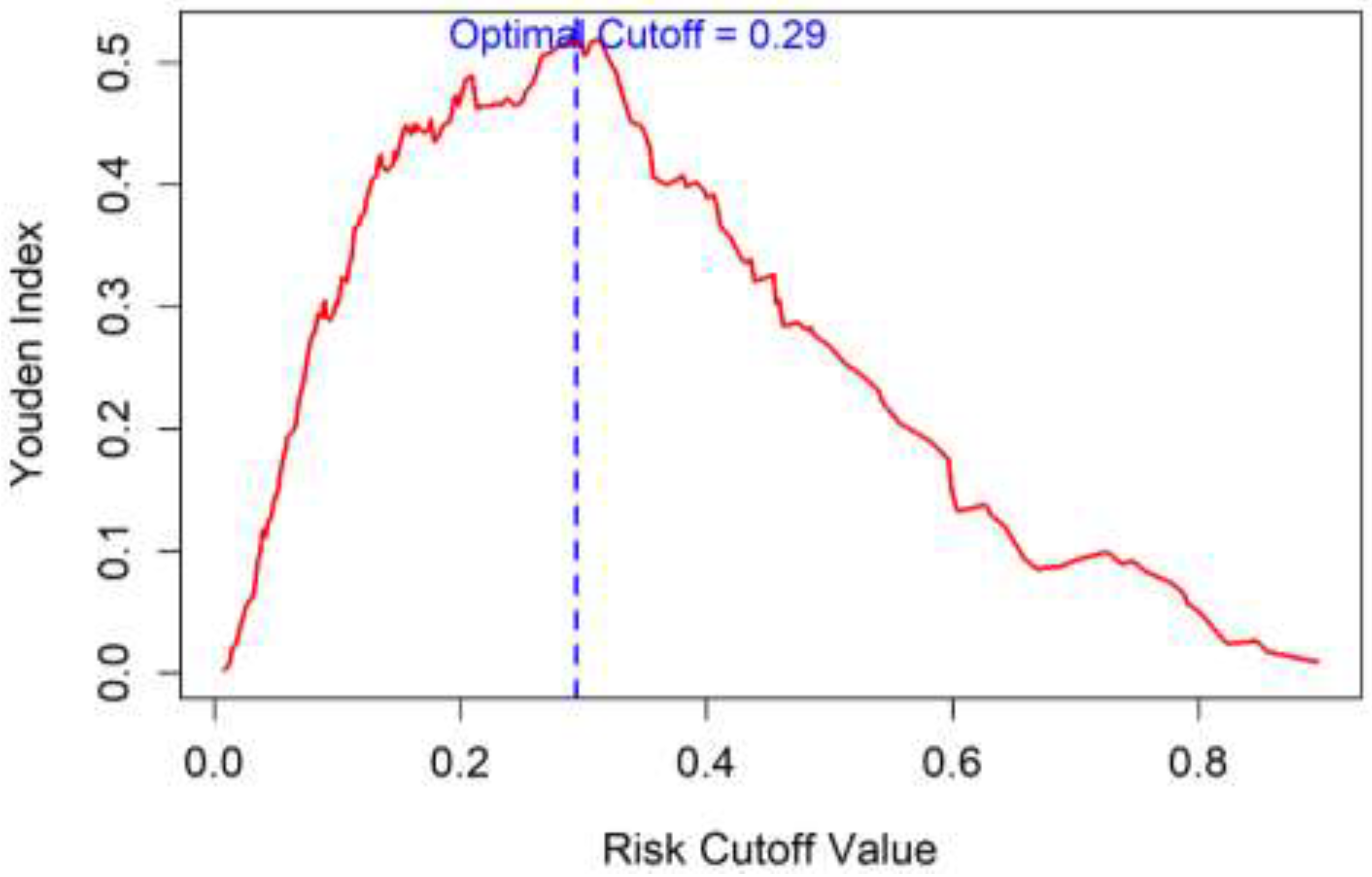

Table 1.
Baseline Demographic and Clinical Characteristics of 512 Patients with ASO.
| Variables | Total population(n=512) | Surgical treatment group(n=479) | Conservative treatment group(n=33) | t/χ² value | P value |
|---|---|---|---|---|---|
| Age (years, x̄±s) | 69.4±8.2 | 69.1±8.1 | 73.5±7.9 | 3.254 | 0.001 |
| Male [n (%)] | 474(92.6) | 443(92.5) | 31(93.9) | 0.102 | 0.749 |
| BMI(kg/m²,x̄±s) | 24.1±3.2 | 24.2±3.1 | 23.8±3.5 | 0.587 | 0.557 |
| Smoking history [n (%)] | 292(57.0) | 275(57.4) | 17(51.5) | 0.481 | 0.488 |
| Comorbidities [n (%)] |
— | — | — | — | — |
| Hypertension | 293(57.2) | 272(56.8) | 21(63.6) | 0.526 | 0.468 |
| Diabetes mellitus | 238(46.5) | 221(46.1) | 17(51.5) | 0.351 | 0.553 |
| Coronary heart disease | 148(28.9) | 135(28.2) | 13(39.4) | 1.762 | 0.185 |
| Preoperative ABI (x̄±s) | 0.38±0.12 | 0.38±0.12 | 0.45±0.10 | 2.987 | 0.003 |
Table 2.
Univariate Analysis of Factors Related to Postoperative Complications (n=479).
| Variables | Non-complication group (n=366) | Complication group (n=113) | t/χ² value | P value |
|---|---|---|---|---|
| Age (years, x̄±s) | 67.3±8.2 | 70.6±7.9 | 3.450 | 0.001 |
| Male [n (%)] | 338(92.3) | 105(92.9) | 0.040 | 0.840 |
| BMI (kg/m², x̄±s) | 24.2±3.3 | 24.5±3.5 | 0.720 | 0.471 |
| Smoking history [n (%)] | 220(60.1) | 82(72.6) | 6.180 | 0.013 |
| Hypertension history [n (%)] |
203(55.5) | 62(54.9) | 0.010 | 0.920 |
| Diabetes mellitus history [n (%)] | 147(40.2) | 58(51.3) | 4.820 | 0.028 |
| Coronary heart disease history [n (%)] | 128(35.0) | 32(28.3) | 1.880 | 0.170 |
| Preoperative ABI (x̄±s) | 0.43±0.10 | 0.31±0.12 | 9.910 | <0.001 |
| Surgical method [n (%)] | — | — | 9.530 | 0.002 |
| Endovascular intervention | 338(92.4) | 92(81.4) | — | — |
| Open/hybrid surgery | 28(7.7) | 21(18.6) | — | — |
Table 3.
Multivariate Logistic Regression Analysis of Postoperative Complications.
| Variables | β Value |
Standard Error | Wald χ² Value | P Value |
OR Value | 95% Confidence Interval |
|---|---|---|---|---|---|---|
| Age | 0.080 | 0.027 | 8.73 | 0.003 | 1.08 | 1.03-1.14 |
| Smoking history (Yes) | 0.632 | 0.312 | 4.10 | 0.043 | 1.88 | 1.02-3.36 |
| Diabetes mellitus history (Yes) | 0.875 | 0.315 | 7.74 | 0.005 | 2.40 | 1.36-3.47 |
| Preoperative ABI < 0.4 (Yes) | 1.112 | 0.399 | 7.78 | 0.005 | 3.04 | 1.39-6.64 |
| Surgical method (open/hybrid) | 0.049 | 0.310 | 0.02 | 0.886 | 1.05 | 0.55-2.00 |
Table 4.
Diagnostic Efficacy of the Prediction Model at Different Cutoff Values.
| Risk cutoff value | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Accuracy (%) | Youden index |
|---|---|---|---|---|---|---|
| >0.10 | 91.15 | 39.07 | 31.60 | 93.46 | 51.36 | 0.302 |
| >0.20 | 77.88 | 69.13 | 43.78 | 91.01 | 71.19 | 0.470 |
| >0.29 | 69.91 | 82.24 | 54.86 | 89.85 | 79.33 | 0.522 |
| >0.40 | 50.44 | 88.52 | 57.58 | 85.26 | 79.54 | 0.390 |
| >0.50 | 33.63 | 93.17 | 60.32 | 81.97 | 79.12 | 0.268 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



