Submitted:
23 February 2026
Posted:
25 February 2026
You are already at the latest version
Abstract
Central retinal artery occlusion (CRAO) is an acute ophthalmic emergency causing irreversible vision loss due to retinal ischemia. Inflammation is increasingly recognized as a contributor to vascular occlusions, but the relationship between systemic inflammatory biomarkers and structural retinal damage in CRAO remains unclear. This retrospective study included 37 patients with non-arteritic CRAO presenting within 168 hours of symptom onset. Optical coherence tomography (OCT) classified ischemic severity as mild, moderate, or severe based on inner retinal morphology. Systemic inflammatory indices, including neutrophil-to-lymphocyte ratio (NLR), systemic immune-inflammation index (SII), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), and systemic inflammation response index (SIRI), were calculated from admission blood tests, and associations were analyzed using ordinal logistic regression. Increasing severity correlated with higher NLR and SII levels (p < 0.05). Univariable analysis showed significant associations for NLR, SII, neutrophil count, white blood cell count, and central macular thickness (CMT). Multivariable regression identified NLR (OR = 8.398, p = 0.007) and CMT (OR = 1.052, p = 0.001) as independent predictors of greater ischemic damage. Other indices were not significant. These findings indicate that NLR is the primary systemic inflammatory predictor of OCT-defined severity in acute CRAO, with CMT providing complementary structural information.
Keywords:
central retinal artery occlusion
; optical coherence tomography
; systemic inflammation
; inflammatory indices
; retinal ischemia
; neutrophil-to-lymphocyte ratio
1. Introduction
Central retinal artery occlusion (CRAO) is an ophthalmic emergency and a rare but severe cause of sudden monocular vision loss, characterized by abrupt interruption of central retinal arterial perfusion with subsequent inner retinal ischemia [1]. Its annual incidence is estimated at about 1–2 per 100,000, increasing markedly with age [2].
Most cases are non-arteritic and are primarily attributed to thromboembolic mechanisms, with emboli arising from atherosclerotic disease of the ipsilateral carotid circulation or from cardiac sources [2,3]. CRAO is associated with multiple vascular risk factors such as smoking, hypertension, dyslipidemia, diabetes, elevated body mass index, coagulopathy, cardiac disease (notably atrial fibrillation) and a family history of vascular disease [2,3,4,5].
Systemic inflammation has been increasingly linked to retinal microvascular dysfunction, with inflammatory markers consistently associated with adverse changes in retinal vessel caliber, particularly venular dilation, reflecting impaired microcirculation [6]. Accordingly, indices derived from the complete blood count (CBC), such as the neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), monocyte to lymphocyte ratio (MLR), systemic immune inflammation index (SII), and systemic inflammation response index (SIRI), have been proposed as accessible markers of inflammatory burden in retinal artery occlusion [7,8]. While several studies report elevated indices in central retinal artery occlusion, it is less clear how these markers relate to the extent of acute structural retinal damage. Recent evidence indicates that systemic inflammatory processes may also manifest in ocular fluids, with measurable changes observed in tear and serum crystallization patterns [9].
Optical coherence tomography (OCT) is a rapid, noninvasive imaging modality that provides high resolution assessment of retinal architecture, allowing objective characterization of acute ischemic injury and severity stratification based on inner retinal changes [1,4,10]. Acute CRAO is characterized on OCT by inner retinal hyperreflectivity, thickening, and progressive loss of layer stratification [11,12,13]. Retinal thickening has been shown to evolve in a time-dependent manner after symptom onset, whereas later stages are typically marked by resolution of edema and subsequent inner retinal atrophy [14,15].
Therefore, the aim of this study was to evaluate the association between systemic inflammatory indices and optical coherence tomography-based severity in patients presenting with acute non-arteritic central retinal artery occlusion (NA-CRAO). We hypothesized that higher inflammatory indices are associated with more severe structural retinal involvement.
2. Materials and Methods
2.1. Study Design and Setting
We conducted a retrospective observational study at the “Sf. Spiridon” Clinical Emergency County Hospital, Iași, Romania. Medical records of patients diagnosed with non-arteritic central retinal artery occlusion between 1 January 2016 and 31 December 2025 were reviewed.
The study was approved by the Research Ethics Committee of “Grigore T. Popa” University of Medicine and Pharmacy, Iași (approval no. 482/27.10.2024) and was conducted in accordance with the Declaration of Helsinki. Given the retrospective design, the requirement for informed consent was waived
Consecutive patients were identified from the hospital electronic medical records database using the ICD-10 code group H34.x (retinal vascular occlusions). All retrieved records underwent individual chart review, and only cases with a confirmed diagnosis of NA-CRAO were included based on clinical documentation and available imaging. Figure 1 illustrates the flow diagram of patient selection and exclusion.
Patients were eligible for inclusion if they fulfilled all of the following criteria:
- Confirmed NA-CRAO based on clinical documentation and available imaging;
- Acute presentation, defined as ≤168 hours from symptom onset;
- Swept-source OCT at presentation (DRI OCT Triton, Topcon) suitable for OCT severity grading and CMT (Center Thickness) extraction
- Complete blood count at presentation allowing calculation of inflammatory indices
Patients were excluded if any of the following were present:
- Other types of retinal arterial occlusion (branch, isolated cilioretinal, mixed or atypical forms) or arteritic CRAO;
- Retinal disease, uveitis, glaucoma, ocular trauma, previous ocular surgery, or media opacities precluding reliable OCT acquisition;
- Conditions or treatments with potential to confound inflammatory indices, including acute infection, malignancy, recent major surgery or trauma (<3 months), major cardiovascular or cerebrovascular disease, advanced renal or hepatic failure, diabetes mellitus, hematologic disorders, autoimmune disorders, current systemic corticosteroid or immunosuppressive therapy or current regular NSAID use;
- Missing essential clinical, imaging, or laboratory data.
A total of 37 patients met the inclusion criteria and were included in the final analysis.
2.2. Data Collection
Demographic variables (age and sex), cardiovascular risk factors (hypertension, dyslipidemia, and smoking status), ophthalmic evaluation at presentation (affected eye, visual acuity, and intraocular pressure), OCT parameters, and laboratory results were retrospectively extracted from electronic and paper medical records using a standardized data collection form. All data were anonymized prior to analysis.
Best-corrected visual acuity (BCVA) was recorded in Snellen and subsequently converted to logMAR for analysis and reporting, assigning predefined values for low vision (CF 2.10, HM 2.40, LP 2.7) [16].
2.3. Optical Coherence Tomography Assessment
Macular OCT performed at presentation using a swept-source device (DRI OCT Triton, Topcon, Tokyo, Japan) was retrospectively analyzed in all included cases. A standardized 3D macular scan (7 × 7 mm, 512 × 256) was used for morphological assessment and OCT severity grading. All scans were reviewed for image quality, centration, and segmentation reliability prior to grading and thickness extraction.
Based on morphological features observed on OCT images at presentation, patients were classified into three severity grades (mild, moderate, and severe) according to the OCT-based classification proposed by Mangla et al [12]. Mild NA-CRAO was defined by inner retinal hyperreflectivity without inner retinal thickening and with preserved inner retinal layer stratification. Moderate NA-CRAO was defined by inner retinal hyperreflectivity with inner retinal thickening while maintaining preserved stratification. Severe NA-CRAO was defined by inner retinal hyperreflectivity with inner retinal thickening accompanied by loss of inner retinal layer stratification. These grading criteria are summarized in Table 1, and representative OCT B-scans illustrating each severity category are presented in Figure 2.
OCT severity was graded independently by two investigators, with disagreements resolved by consensus. Interobserver reliability for OCT severity classification was evaluated using weighted Cohen’s kappa, indicating excellent reproducibility (κ = 0.808).
2.4. Inflammatory Indices
Complete blood count parameters obtained at presentation, including total leukocyte, neutrophil, lymphocyte, monocyte, and platelet counts, were extracted from laboratory records. The neutrophil-to-lymphocyte ratio was calculated by dividing the neutrophil count by the lymphocyte count, the platelet-to-lymphocyte ratio by dividing the platelet count by the lymphocyte count, and the monocyte-to-lymphocyte ratio by dividing the monocyte count by the lymphocyte count. The systemic immune-inflammation index was calculated as the product of platelet and neutrophil counts divided by the lymphocyte count, while the systemic inflammation response index was calculated as the product of neutrophil and monocyte counts divided by the lymphocyte count.
2.5. Statistical Analysis
Statistical analysis was performed using SPSS version 29.0. Descriptive statistics were reported as mean ± standard deviation (SD) or median and interquartile range (IQR), depending on data distribution. Categorical variables were expressed as counts and percentages. Normality of continuous variables was assessed using the Kolmogorov–Smirnov test. For group comparisons, one-way analysis of variance (ANOVA) was used for normally distributed variables, with Levene’s test applied to assess homogeneity of variances. In case of variance homogeneity, post hoc analysis was performed using the Tukey test; when variances were unequal, the Games–Howell test was applied. For non-normally distributed variables, the Kruskal–Wallis test was used, followed by pairwise post hoc comparisons with appropriate adjustment for multiple testing.
Ordinal logistic regression models were constructed to evaluate associations between inflammatory indices and OCT-based ischemic severity grades. Variables with p < 0.10 in univariable analysis were considered for multivariable modeling. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Model fit was assessed using the Nagelkerke R² and the test of parallel lines to verify the proportional odds assumption.
A two-tailed p-value < 0.05 was considered statistically significant, while p-values between 0.05 and 0.10 were interpreted as indicating a statistical trend.
3. Results
3.1. Baseline Characteristics
A total of 37 patients with acute NA-CRAO were included. Based on OCT findings, ischemic severity was classified as mild in 7 patients (18.9%), moderate in 16 (43.2%), and severe in 14 (37.8%). Baseline demographic and clinical characteristics are summarized in Table 2.
The mean age was 65.9 ± 10.5 years and most patients were male (64.9%). Baseline presentation parameters including laterality, intraocular pressure, best-corrected visual acuity (logMAR), and time from symptom onset were comparable across OCT severity groups (all p > 0.05).
Cardiovascular risk factors did not differ significantly according to ischemic severity, although dyslipidemia showed a borderline association with OCT severity (p = 0.055). The presence of a cilioretinal artery was observed in mild and moderate cases but not in severe ischemia; however, this did not reach statistical significance (p = 0.068).
3.2. OCT Severity and Inflammatory Indices
CMT differed significantly across ischemic severity groups (p < 0.001), with progressively higher values observed with increasing severity (Table 3).
Post-hoc analyses showed higher CMT in severe ischemia compared with mild (p < 0.001) and moderate ischemia (p = 0.001).
Among the inflammatory markers analyzed, significant differences across severity groups were observed for neutrophil count (p = 0.013), NLR (p = 0.029), and SII (p = 0.018) (Table 4).
Post hoc comparisons indicated that both NLR and SII were significantly higher in the severe group compared to the mild group. WBC, monocytes, lymphocytes, platelets, MLR, PLR, and SIRI did not differ significantly across groups (all p > 0.05).
3.3. Univariable Regression Analysis
Ordinal logistic regression was used to evaluate the association between systemic inflammatory markers and OCT-based ischemic severity. In univariable analysis, CMT, NLR, SII, neutrophil count, and WBC were significantly associated with greater ischemic severity (p < 0.05). Among these, NLR exhibited the strongest effect size (OR = 2.659; 95% CI: 1.240–5.703; p = 0.012). This indicates that each one-unit increase in NLR was associated with a 2.659-fold higher odds of belonging to a more severe OCT ischemia category. In contrast, dyslipidemia and the presence of a cilioretinal artery were not significantly associated with severity (p > 0.05)(Table 5).
3.4. Multivariable Regression Analysis
Prior to multivariable modeling, correlations between candidate predictors were assessed using Spearman coefficients to minimize multicollinearity. Strong correlations were observed between NLR and neutrophil count (rho = 0.574, p < 0.001) as well as between NLR and SII (rho = 0.842, p < 0.001), whereas no significant correlation was found between NLR and CMT (rho = 0.153, p = 0.366). CMT showed a moderate correlation with WBC (rho = 0.355, p = 0.031). Based on these findings, the multivariable ordinal logistic regression model included NLR and CMT as independent predictors.
In this model, both variables remained independently associated with ischemic severity (Table 6).
4. Discussion
This study explored the association between systemic inflammatory markers and OCT-based structural severity in patients with acute NA-CRAO. To our knowledge, it is among the first studies to relate these indices to the extent of retinal tissue injury captured by OCT. We found that a higher systemic inflammatory burden, reflected by elevated NLR and SII, was associated with more extensive ischemic damage. These findings suggest that certain inflammatory markers may reflect underlying pathophysiological processes contributing to retinal tissue injury, and thus hold potential value for early risk stratification. By integrating systemic inflammation markers with structural OCT findings, our results support the concept that systemic inflammation is not merely a consequence but potentially a contributor to ischemic burden in CRAO.
Our findings are consistent with a recent meta-analysis demonstrating significantly elevated NLR and PLR levels in patients with retinal artery occlusion compared with controls. The pooled analysis of eight retrospective studies including 1,444 participants reported a moderate to large effect size for NLR and a smaller but significant effect for PLR, despite substantial between-study heterogeneity [7].
Systemic inflammatory markers derived from the complete blood count have been widely investigated in CRAO, although their clinical utility varies substantially by marker and context. Among them, NLR has been most consistently reported to be significantly higher in CRAO patients versus controls [17,18,19,20]. As a composite marker reflecting neutrophilia and relative lymphopenia, NLR is considered a surrogate of innate immune activation and systemic stress, processes that are mechanistically relevant to acute arterial occlusion.
In our cohort, higher NLR values were observed with increasing ischemic severity, supporting a graded link between systemic inflammation and the extent of retinal damage assessed on structural imaging. This pattern suggests that NLR captures more than disease presence alone, instead reflecting an inflammatory response that scales with ischemic burden. This inflammatory milieu is thought to promote endothelial dysfunction, embolic propensity, and microvascular vulnerability, thereby predisposing to more extensive ischemic injury. Taken together, these findings point to a more prominent role of the neutrophil-related inflammatory response in the most severe CRAO presentations.
Central macular thickness represents a direct structural manifestation of retinal ischemic injury following abrupt perfusion failure [21,22,23,24]. The absence of correlation between NLR and CMT in our cohort, together with their additive effects in multivariable analysis, supports a complementary mechanistic framework in which systemic inflammatory burden and local retinal tissue response operate through distinct but convergent pathways. Notably, NLR emerged as the dominant systemic predictor, with each one-unit increase associated with an 8.398-fold higher odds of belonging to a more severe OCT-defined ischemia category, whereas CMT showed a smaller but stable independent association reflecting local tissue injury. Thus, while NLR may influence vascular vulnerability and microvascular injury, CMT provides tissue-level quantification of ischemic damage, and their combined assessment offers a more comprehensive stratification of disease severity in acute NA-CRAO.
Notably, Elbeyli et al. reported that red cell distribution width (RDW) showed greater discriminatory performance than NLR and PLR and was the only independent predictor of CRAO in multivariable analysis, underscoring that different inflammatory markers may capture distinct aspects of the systemic response to retinal ischemia [18].
Platelet-to-lymphocyte ratio has been proposed as an index reflecting platelet activation alongside relative lymphopenia, linking inflammatory and prothrombotic pathways. However, evidence regarding PLR in RAO remains heterogeneous. While some studies reported higher PLR in affected patients than in controls, others found no meaningful differences [17,19]. Consistent with this variability, PLR was not associated with ischemic severity in our cohort, suggesting it may lack sensitivity in capturing the extent of retinal tissue damage.
Systemic immune-inflammation index has emerged as a versatile and accessible biomarker that reflects the interplay between systemic inflammation and immune status. Its clinical relevance has been demonstrated across multiple domains, including oncology, cardiovascular and cerebrovascular diseases, infectious conditions, and autoimmune disorders, where it correlates with disease severity, mortality risk, and prognosis [25,26,27,28]. In our cohort, higher SII values were associated with greater ischemic severity, reflecting the possible contribution of systemic inflammatory and thrombotic activity to the extent of retinal ischemic involvement. SII may thus serve as a useful tool for risk stratification and clinical monitoring in acute NA-CRAO.
In contrast, MLR and SIRI showed no significant association with ischemic severity, reinforcing the need to prioritize markers more closely linked to the underlying pathophysiology.
The present study provides novel insight into the clinical interpretation of systemic inflammatory indices in CRAO. While previous studies have primarily focused on the presence and elevation of inflammatory markers in CRAO, our study advances this perspective by demonstrating that these indices are not only elevated, but also proportionally associated with the degree of ischemic retinal injury, as assessed by OCT. This distinction is clinically meaningful, as it reframes inflammatory markers from simple indicators of disease presence to potential tools for quantifying tissue damage and stratifying acute ischemic severity.
Optical coherence tomography enables high-resolution, layer-specific visualization of ischemic injury in CRAO which directly reflects the extent of retinal damage [24,29,30,31,32]. Furthermore, recent studies recognize OCT as the primary modality for assessing ischemic injury severity, due to its capacity to detect early retinal edema, hyperreflectivity, and disorganization of inner retinal layers [33,34,35].
Mangla et al. [12] introduced a purely OCT based morphological classification system for CRAO, addressing the heterogeneity and subjectivity of previous models, which relied on mixed clinical, angiographic, and imaging criteria and commonly categorized CRAO severity as incomplete, subtotal, or total. Their grading reflects a continuous progression of structural and pathological changes, closely aligned with capillary plexus involvement and the extent of ischemic retinal injury. Furthermore, the described changes follow a consistent temporal evolution, allowing for early detection and providing a practical framework for longitudinal assessment of disease severity and potential treatment response. For our study, we adopted this grading because it uses objective, routinely available features in acute care, providing a reproducible and quantifiable measure of severity.
In a recent retrospective study, Hu et al. [8] examined peripheral blood inflammatory indices in CRAO and related them to disease severity using a composite grading system that integrated fluorescein fundus angiography, funduscopic cherry-red spot, and OCT characteristics to classify cases as incomplete, subtotal, or total CRAO. NLR, SII, and MHR were higher in CRAO than in controls, but across severity grades only MHR (driven by lower HDL-C) was associated with total CRAO, whereas NLR and SII did not significantly differ between subtypes.
While Hu et al. primarily characterize disease severity at the vascular and clinical level our study focuses on the severity of tissue level ischemic damage, quantified on OCT. By defining severity exclusively through OCT-based morphological criteria we sought to capture the downstream retinal consequences of ischemia, rather than upstream perfusion abnormalities. In this context, systemic inflammatory indices are interpreted in relation to structural retinal damage, providing a complementary perspective that does not depend on perfusion imaging. Thus, the two frameworks capture different dimensions of CRAO severity and are best viewed as complementary.
From a clinical perspective, integrating structural retinal injury on OCT with inflammatory indices adds contextual information that supports severity assessment and may inform subsequent systemic evaluation.This is feasible in routine acute care, since both OCT and complete blood count parameters are typically available without delaying workflows.
Our findings should be interpreted in light of several limitations. The retrospective design and modest sample size may limit statistical power and generalizability. Blood samples were obtained upon presentation but not standardized by time of day or fasting state, which may influence inflammatory indices. OCT grading was focused on structural findings without correlating with long-term visual outcomes. Furthermore, strict exclusion criteria may reduce applicability to broader populations. Future prospective studies are needed to validate these associations and assess their prognostic utility.
5. Conclusions
Systemic inflammatory burden, particularly reflected by NLR and SII, is significantly associated with OCT-defined ischemic severity in acute non-arteritic CRAO. NLR emerged as the dominant systemic predictor, while acute CMT provided complementary structural information on tissue-level injury. These findings highlight the combined role of systemic inflammation and local retinal response in shaping ischemic severity and support the potential utility of integrating inflammatory indices with OCT for early severity stratification.
Author Contributions
Conceptualization, A.M.N., C.M.B. and M.F.; methodology, A.M.N. and R.E.C.; validation, R.E.C., P.C.M., M.M.G., A.F.O. and C.M.B.; formal analysis, C.G.D.; investigation, A.M.N., C.V.G. and R.E.C.; resources, C.M.B.; data curation, A.M.N., S.A.N., M.C.A. and D.T.M., P.C.M., M.M.G. and A.F.O.; writing—original draft preparation, A.M.N.; writing—review and editing, M.F., C.M.B., and R.E.C.; visualization, A.M.N., M.F., D.T.M., P.C.M., A.F.O, M.M.G. and S.A.N.; supervision, M.F. and C.M.B.; project administration, A.M.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research is a study from a PhD thesis of Aurelia Mihaela Nica, and it received research funding from the University of Medicine and Pharmacy “Gr. T. Popa” (No. 482/27 October 2024).
Institutional Review Board Statement
The study design and protocol were performed according to the tenets of the Declaration of Helsinki for research involving human subjects and approved by the Ethics Committee of “Grigore T. Popa” University of Medicine and Pharmacy Iasi, Romania (No. 482/approval date on 27 October 2024).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ANOVA | Analysis of Variance |
| BCVA | Best-Corrected Visual Acuity |
| CBC | Complete Blood Count |
| CF | Counting Fingers |
| CI | Confidence Interval |
| CMT | Central Macular Thickness |
| CRAO | Central Retinal Artery Occlusion |
| HDL-C | High-Density Lipoprotein Cholesterol |
| HM | Hand Motion |
| ICD-10 | International Classification of Diseases, 10th Revision |
| IOP | Intraocular Pressure |
| IQR | Interquartile Range |
| logMAR | logarithm of the Minimum Angle of Resolution |
| LP | Light Perception |
| MLR | Monocyte-to-Lymphocyte Ratio |
| NA-CRAO | Non-Arteritic Central Retinal Artery Occlusion |
| NLR | Neutrophil-to-Lymphocyte Ratio |
| OCT | Optical Coherence Tomography |
| OR | Odds Ratio |
| PLR | Platelet-to-Lymphocyte Ratio |
| RAO | Retinal Artery Occlusion |
| SD | Standard Deviation |
| SII | Systemic Immune-Inflammation Index |
| SIRI | Systemic Inflammation Response Index |
| WBC | White Blood Cell count |
References
- Kovach, J.L.; Bailey, S.T.; Kim, S.J.; Lim, J.I.; Vemulakonda, G.A.; Ying, G. shuang; Flaxel, C.J. Retinal and Ophthalmic Artery Occlusions Preferred Practice Pattern®. Ophthalmology 2025, 132, P270–P302. [CrossRef]
- Scott, I.U.; Campochiaro, P.A.; Newman, N.J.; Biousse, V. Retinal Vascular Occlusions. The Lancet 2020, 396, 1927–1940. [CrossRef]
- MacGrory, B.; Schrag, M.; Biousse, V.; Furie, K.L.; Gerhard-Herman, M.; Lavin, P.J.; Sobrin, L.; Tjoumakaris, S.I.; Weyand, C.M.; Yaghi, S. Management of Central Retinal Artery Occlusion: A Scientific Statement from the American Heart Association. Stroke 2021, 52, E282–E294.
- Chen, C.; Singh, G.; Madike, R.; Cugati, S. Central Retinal Artery Occlusion: A Stroke of the Eye. Eye Basingstoke 2024, 38, 2319–2326.
- Diel, N.J.; Gerner, S.T.; Doeppner, T.R.; Juenemann, M.; Maxhuni, T.; Frühwald, T.; Worm, A.; Alhaj Omar, O.; Lytvynchuk, L.; Struffert, T.; et al. Comparison of Vascular Risk Profile and Clinical Outcomes among Patients with Central (Branch) Retinal Artery Occlusion versus Amaurosis Fugax. Neurol. Res. Pract. 2024, 6, 27. [CrossRef]
- Liu, M.; Lovern, C.; Lycett, K.; He, M.; Wake, M.; Wong, T.Y.; Burgner, D.P. The Association between Markers of Inflammation and Retinal Microvascular Parameters: A Systematic Review and Meta-Analysis. Atherosclerosis 2021, 336, 12–22. [CrossRef]
- Chuang, S.H.; Chang, C.H. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio in Retinal Artery Occlusion: A Meta-Analysis. Graefes Arch. Clin. Exp. Ophthalmol. 2024 2631 2024, 263, 47–57. [CrossRef]
- Hu, W.; Huang, Y.; Zhou, Q.; Huang, X. Relation between Peripheral Blood Inflammatory Indices and Severity of Central Retinal Artery Occlusion. PeerJ 2024, 12. [CrossRef]
- Ganea, C.V.; Alexa, A.I.; Anton, N.; Sandu, C.A.; Bilha, M.I.; Donica, V.C.; Pavel, I.A.; Ciuntu, R.E.; Bogdanici, C.M. A Multimodal Analysis of Serum and Tear Crystallization Patterns in Patients with Obesity. J. Clin. Med. 2026, 15, 773. [CrossRef]
- Zeppieri, M.; Marsili, S.; Enaholo, E.S.; Shuaibu, A.O.; Uwagboe, N.; Salati, C.; Spadea, L.; Musa, M. Optical Coherence Tomography (OCT): A Brief Look at the Uses and Technological Evolution of Ophthalmology. Med. 2023 Vol 59 Page 2114 2023, 59, 2114. [CrossRef]
- Furashova, O.; Matthé, E. Retinal Changes in Different Grades of Retinal Artery Occlusion: An Optical Coherence Tomography Study. Invest. Ophthalmol. Vis. Sci. 2017, 58, 5209–5216. [CrossRef]
- Mangla, R.; Venkatesh, R.; Sangoram, R.; Acharya, I.; Parmar, Y.; Prabhu, V.; Yadav, N.K.; Chhablani, J. Retinal OCT Findings in Acute Central Retinal Artery Occlusion of Varying Severity at Different Disease Stages – a Retrospective, Observational Study. Int. J. Retina Vitr. 2023, 9. [CrossRef]
- Wang, W.; Lei, T.; Wang, R.; Zhang, B.; Wang, X.; Ma, T. Correlation of Visual Acuity Changes and Optical Coherence Tomography Imaging in Patients with Central Retinal Artery Occlusion Post-Arterial Thrombolysis. Sci. Rep. 2025, 15. [CrossRef]
- Ochakovski, G.A.; Wenzel, D.A.; Spitzer, M.S.; Poli, S.; Härtig, F.; Fischer, M.D.; Dimopoulos, S.; Schultheiss, M. Retinal Oedema in Central Retinal Artery Occlusion Develops as a Function of Time. Acta Ophthalmol. (Copenh.) 2020, 98, e680–e684. [CrossRef]
- Cornut, P.-L.; Bieber, J.; Beccat, S.; Fortoul, V.; Poli, M.; Feldman, A.; Denis, P.; Burillon, C. [Spectral domain OCT in eyes with retinal artery occlusion]. J. Fr. Ophtalmol. 2012, 35, 606–613. [CrossRef]
- Moussa, G.; Bassilious, K.; Mathews, N. A Novel Excel Sheet Conversion Tool from Snellen Fraction to LogMAR Including ‘Counting Fingers’, ‘Hand Movement’, ‘Light Perception’ and ‘No Light Perception’ and Focused Review of Literature of Low Visual Acuity Reference Values. Acta Ophthalmol. (Copenh.) 2021, 99, e963–e965. [CrossRef]
- Dursun, M.E.; Hazar, L.; Karahan, M.; Ava, S.; Erdem, S.; Vural, E.; Keklikçi, U. Evaluation of Plasma Inflammatory Markers in Patients with Nonarteritic Retinal Artery Occlusion. Retina-Vitr. 2023, 32, 91–96. [CrossRef]
- Elbeyli, A.; Kurtul, B.E.; Ozcan, D.O.; Ozcan, S.C.; Dogan, E. Assessment of Red Cell Distribution Width, Platelet/Lymphocyte Ratio, Systemic Immune-Inflammation Index, and Neutrophil/Lymphocyte Ratio Values in Patients with Central Retinal Artery Occlusion. Ocul. Immunol. Inflamm. 2022, 30, 1940–1944. [CrossRef]
- Guven, S.; Kilic, D. Neutrophil to Lymphocyte Ratio (NLR) Is a Better Tool Rather than Monocyte to High-Density Lipoprotein Ratio (MHR) and Platelet to Lymphocyte Ratio (PLR) in Central Retinal Artery Occlusions. Ocul. Immunol. Inflamm. 2021, 29, 997–1001. [CrossRef]
- Zhang, Y.; Xing, Z.; Deng, A. Unveiling the Predictive Capacity of Inflammatory and Platelet Markers for Central Retinal Artery Occlusion. Thromb. Res. 2023, 232, 108–112. [CrossRef]
- Chen, S.N.; Hwang, J.F.; Chen, Y.T. Macular Thickness Measurements in Central Retinal Artery Occlusion by Optical Coherence Tomography. Retina 2011, 31, 730–737. [CrossRef]
- Abdellah, M.M. Multimodal Imaging of Acute Central Retinal Artery Occlusion. Med. Hypothesis Discov. Innov. Ophthalmol. 2019, 8, 283–290.
- Kim, H.; Kim, H.K.; Yang, J.Y.; Kim, S.S. Optical Coherence Tomography Measurement and Visual Outcome in Acute Central Retinal Artery Occlusion. Korean J. Ophthalmol. KJO 2018, 32, 303–311. [CrossRef]
- Matthé, E.; Eulitz, P.; Furashova, O. ACUTE RETINAL ISCHEMIA IN CENTRAL VERSUS BRANCH RETINAL ARTERY OCCLUSION. Retina 2020, 40, 1118–1123. [CrossRef]
- Han, J.; Du, G.; Guo, S.; Hao, J.; Wang, Y.; Li, R.; Lang, X.; Zhang, Y.; Zhu, X.; Cui, H. Association Between Atopic Dermatitis and Systemic Immune-Inflammation Index: Evidence From NHANES 1999–2006. Mediators Inflamm. 2026, 2026, 5512492. [CrossRef]
- Ma, X.; Zhou, Y.; Li, Z.; Mao, G.; Wei, H.; Zhao, T. Comparison of the Predictive Performance of Systemic Immune-Inflammation Index and Neutrophil-to-Lymphocyte Ratio for Three-Month Poor Functional Outcome in Ischemic Stroke: A Systematic Review and Meta-Analysis. Ann. Med. 2026, 58. [CrossRef]
- Paçacı, B.; Kocaaslan, E.; Demirel, A.; Akagündüz, F.; Tunç, M.A.; Ağyol, Y.; Güren, A.K.; Çelebi, A.; Işık, S.; Çoban, E.; et al. Prognostic Value of Systemic Immune-Inflammation Index in Mucosal Malignant Melanoma. J. Clin. Med. 2026, 15, 890. [CrossRef]
- Yan, W.; Zhang, B.; Zhang, X.; Li, X.; Yu, Y.; Liu, Y.; Guo, L.; Lv, H. Association of Systemic Inflammation Indices With Mortality in Coronary Atherosclerosis Patients With and Without Standard Modifiable Risk Factors. Mediators Inflamm. 2026, 2026, 8830121. [CrossRef]
- Matthé, E.; Wittig, D.; Kuhn, M.; Eulitz, P.; Schoen, K.; Sandner, D.; Furashova, O. Manual Measurement of SD-OCT Images of Hyperreflective Retinal Layers in Acute Retinal Vessel Occlusion Is Reliable, Repeatable and Reproducible. Sci. Rep. 2025, 15, 34471. [CrossRef]
- Wenzel, D.A.; Kromer, R.; Poli, S.; Steinhorst, N.A.; Casagrande, M.K.; Spitzer, M.S.; Schultheiss, M. Optical Coherence Tomography-Based Determination of Ischaemia Onset - the Temporal Dynamics of Retinal Thickness Increase in Acute Central Retinal Artery Occlusion. Acta Ophthalmol. (Copenh.) 2021, 99, e247–e252. [CrossRef]
- Wenzel, D.A.; Poli, S.; Casagrande, M.; Druchkiv, V.; Spitzer, M.S.; Bartz-Schmidt, K.U.; Grohmann, C.; Schultheiss, M. Inner Retinal Layer Hyperreflectivity Is an Early Biomarker for Acute Central Retinal Artery Occlusion. Front. Med. 2022, 9. [CrossRef]
- Mac Grory, B.; Schrag, M.; Poli, S.; Boisvert, C.J.; Et., A. Structural and Functional Imaging of the Retina in Central Retinal Artery Occlusion – Current Approaches and Future Directions. J. Stroke Cerebrovasc. Dis. 2021. [CrossRef]
- Bénard-Séguin, É.; Nahab, F.; Pendley, A.M.; Duran, M.R.; Soto, M.T.; Keadey, M.; Wright, D.W.; Newman, N.J.; Biousse, V. Eye Stroke Protocol in in the Emergency Department. J. Stroke Cerebrovasc. Dis. 2024, 33. [CrossRef]
- Casagrande, M.; Kromer, R.; Wenzel, D.A.; Poli, S.; Spitzer, M.S.; Druchkiv, V.; Schultheiss, M.; Dimopoulos, S. Determination of Ischemia Onset Based on Automatically Generated Spectralis SD-OCT Values in Acute Central Retinal Artery Occlusion. J. Ophthalmol. 2021, 2021. [CrossRef]
- Ahn, S.J.; Woo, S.J.; Park, K.H.; Jung, C.; Et., A. Retinal and Choroidal Changes and Visual Outcome in Central Retinal Artery Occlusion: An Optical Coherence Tomography Study. Am. J. Ophthalmol. 2015. [CrossRef]
Figure 1.
Flow diagram of patient selection.
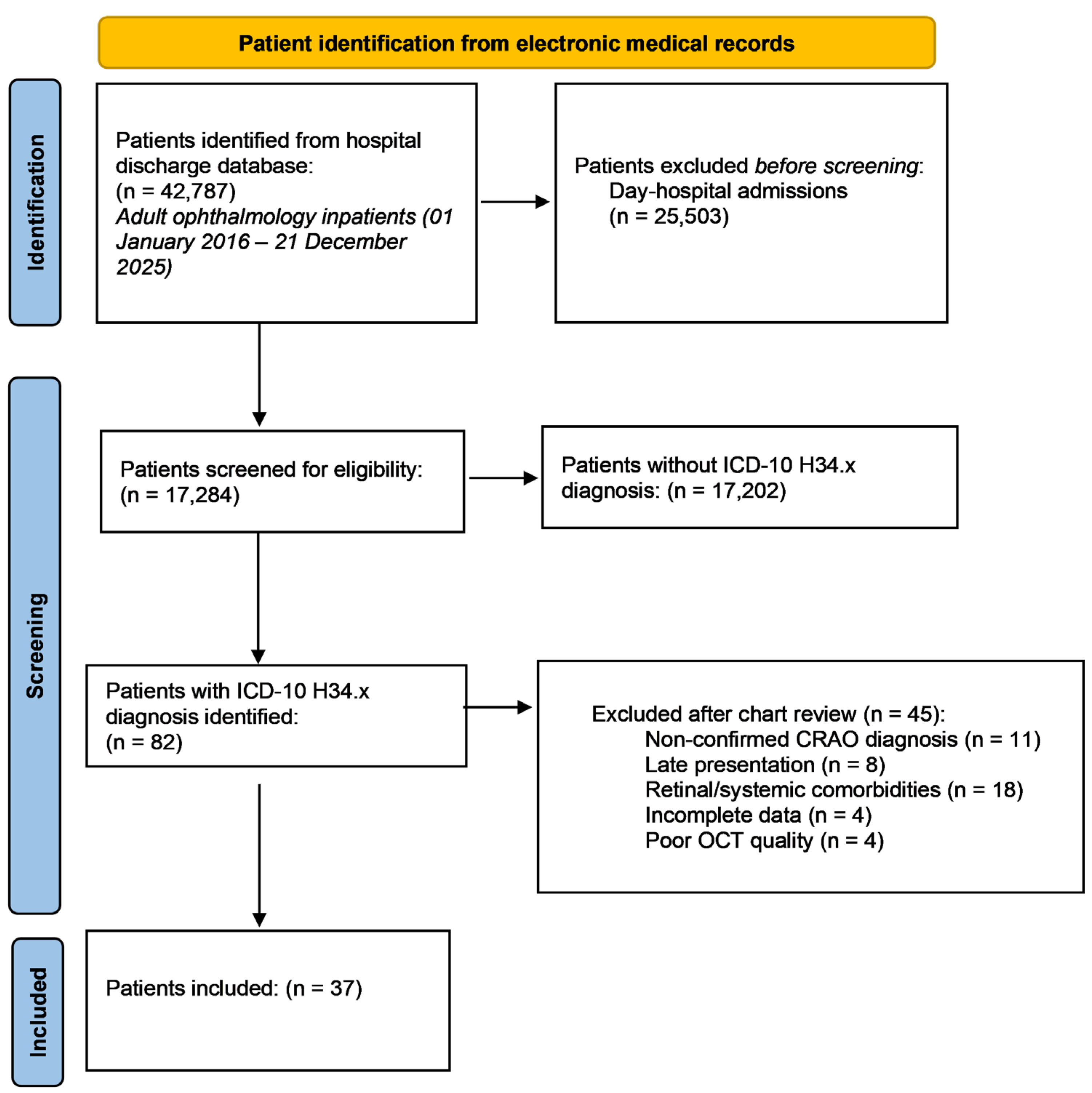
Figure 2.
Representative OCT images showing normal macular morphology and OCT-defined ischemic severity in acute NA-CRAO. (a) Normal retinal architecture; (b) Mild: inner retinal hyperreflectivity without inner retinal thickening, with preserved stratification. (c) Moderate: inner retinal hyperreflectivity with inner retinal thickening, with preserved stratification. (d) Severe: inner retinal hyperreflectivity with inner retinal thickening and loss of inner retinal layer stratification.
Figure 2.
Representative OCT images showing normal macular morphology and OCT-defined ischemic severity in acute NA-CRAO. (a) Normal retinal architecture; (b) Mild: inner retinal hyperreflectivity without inner retinal thickening, with preserved stratification. (c) Moderate: inner retinal hyperreflectivity with inner retinal thickening, with preserved stratification. (d) Severe: inner retinal hyperreflectivity with inner retinal thickening and loss of inner retinal layer stratification.
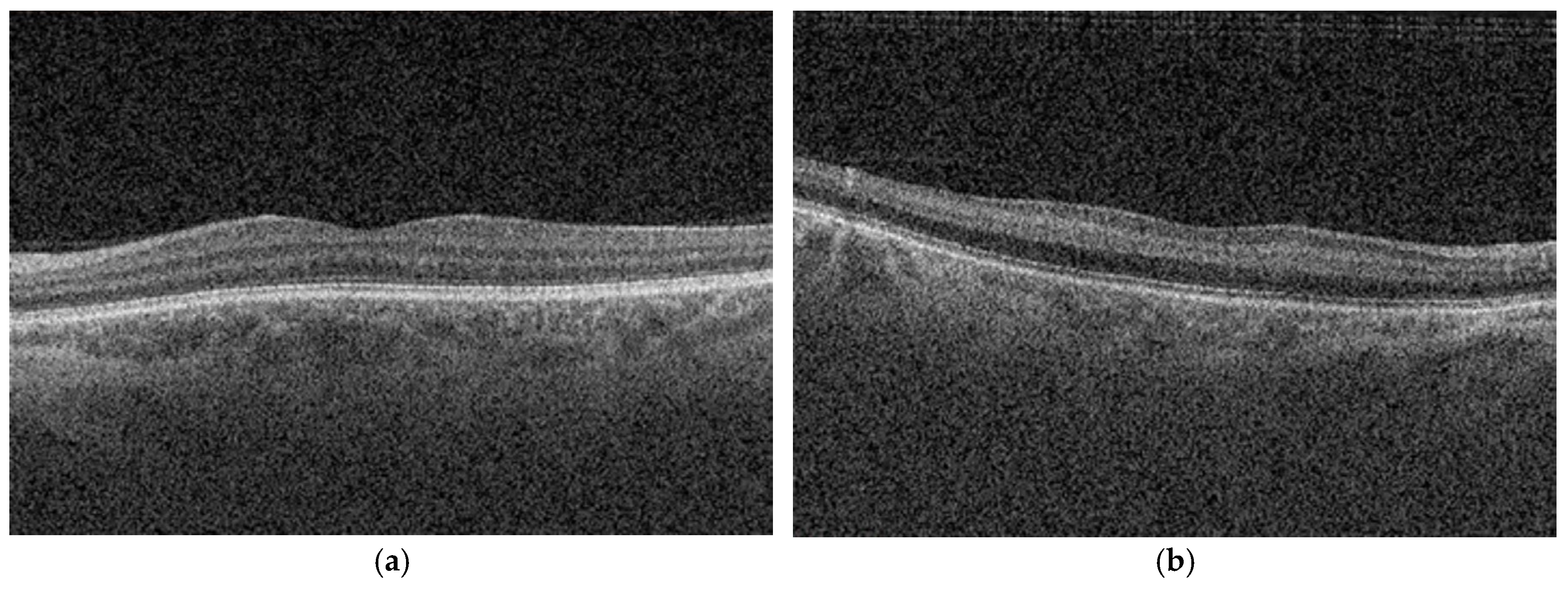
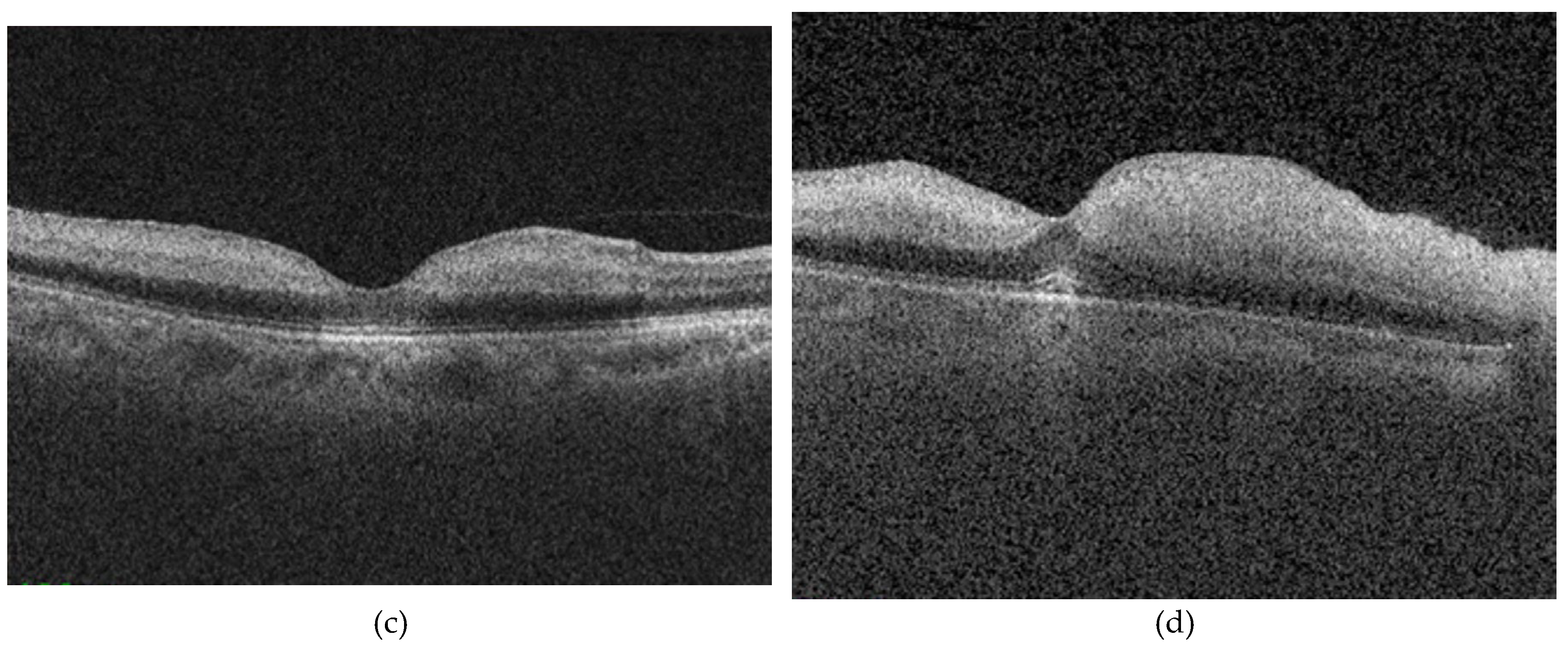

Table 1.
OCT-based severity classification of acute NA-CRAO.
| OCT characteristic | Mild CRAO | Moderate CRAO | Severe CRAO |
|---|---|---|---|
| Inner retinal hyperreflectivity | Present | Present | Present |
| Inner retinal thickening | Absent | Present | Present |
| Inner retinal layer stratification | Preserved | Preserved | Lost |
OCT= optical coherence tomography; NA-CRAO= non-arteritic central retinal artery occlusion.
Table 2.
Baseline demographic and clinical characteristics according to OCT-based ischemic severity.
Table 2.
Baseline demographic and clinical characteristics according to OCT-based ischemic severity.
| Variable | Total (n = 37) | Mild (n = 7) | Moderate (n = 16) | Severe (n = 14) | p-value |
|---|---|---|---|---|---|
| Age (years, mean ± SD) | 65.9 ± 10.5 | 62.9 ± 13.8 | 67.8 ± 8.4 | 65.4 ± 11.2 | 0.573a |
| Male sex, n (%) | 24 (64.9) | 4 (57.1) | 12 (75.0) | 8 (57.1) | 0.530b |
| Right eye, n (%) | 24 (64.9) | 5 (71.4) | 12 (75.0) | 7 (50.0) | 0.331b |
| IOP (mmHg), median (IQR) | 14.0 (12.0–16.5) | 13.0 (12.0–17.0) | 13.5 (10.0–15.5) | 14.0 (12.0–17.3) | 0.666c |
| BCVA, logMAR, median (IQR) | 2.30 (2.00–2.30) | 2.30 (0.70–2.70) | 2.30 (2.00–2.30) | 2.30 (2.00–2.70) | 0.564c |
| Time from onset (h), median (IQR) | 12 (8–33) | 10 (8–48) | 24 (10–28) | 18 (8–39) | 0.903c |
| Hypertension, n (%) | 31 (83.8) | 6 (85.7) | 14 (87.5) | 11 (78.6) | 0.794b |
| Dyslipidemia, n (%) | 19 (51.4) | 1 (14.3) | 11 (68.8) | 7 (50.0) | 0.055b |
| Smoking, n (%) | 8 (21.6) | 0 (0.0) | 3 (18.8) | 5 (35.7) | 0.161b |
| Cilioretinal artery present, n (%) | 6 (16.2) | 1 (14.3) | 5 (31.3) | 0 (0.0) | 0.068ᶜ |
p-values were calculated using the ᵃone-way ANOVA, bPearson’s chi-square test, cKruskal-Wallis test. A p-value < 0.05 was considered statistically significant. IOP=intraocular pressure; IQR=interquartile range; BCVA=best-corrected visual acuity;.
Table 3.
CMT across OCT-based ischemic severity.
| Parameter | Mild (n=7) | Moderate (n=16) | Severe (n=14) | p-value |
|---|---|---|---|---|
| CMT (µm), median (IQR) | 254 (247–263) | 283 (256–301) | 404 (341–481) | <0.001c |
p-values were calculated using the cKruskal-Wallis test; CMT= central macular thickness; OCT= optical coherence tomography; IQR=interquartile range;.
Table 4.
Systemic inflammatory markers across OCT-based ischemic severity.
| Variable | Mild (n = 7) | Moderate (n = 16) | Severe (n = 14) | p-value |
|---|---|---|---|---|
| WBC (cells × 10⁹/L, mean ± SD) | 7.09 ± 2.04 | 7.78 ± 1.90 | 8.97 ± 1.60 | 0.067ᵃ |
| Neutrophils (cells × 10⁹/L, mean ± SD) | 4.10 ± 1.28 | 4.93 ± 1.39 | 6.04 ± 1.47 | 0.013a |
| Monocytes (cells × 10⁹/L, mean ± SD) | 0.60 ± 0.24 | 0.68 ± 0.09 | 0.64 ± 0.22 | 0.576a |
| Lymphocytes (cells × 10⁹/L, mean ± SD) | 2.19 ± 0.70 | 1.94 ± 0.61 | 2.14 ± 0.56 | 0.550a |
| Platelets (cells × 10⁹/L, mean ± SD) | 252 ± 64 | 231 ± 32 | 264 ± 70 | 0.258a |
| NLR (mean ± SD) | 1.89 ± 0.42 | 2.69 ± 0.80 | 3.02 ± 1.08 | 0.029a |
| MLR (mean ± SD) | 0.29 ± 0.11 | 0.39 ± 0.14 | 0.31 ± 0.11 | 0.122a |
| PLR (mean ± SD) | 125.9 ± 45.3 | 132.6 ± 52.2 | 127.8 ± 31.6 | 0.929a |
| SII (mean ± SD) | 480.6 ± 169.0 | 621.2 ± 204.5 | 773.8 ± 248.9 | 0.018a |
| SIRI (median, IQR) | 857.6 (610.6–1150.4) | 655.8 (397.3–912.7) | 705.0 (610.6–1167.4) | 0.101c |
p-values were calculated using the ᵃone-way ANOVA, bPearson’s chi-square test, cKruskal-Wallis test. NLR= neutrophil-to-lymphocyte ratio; MLR= monocyte-to-lymphocyte ratio; PLR= platelet-to-lymphocyte ratio; SII= systemic immune-inflammation index; SIRI= systemic inflammation response index; IQR=interquartile range.
Table 5.
Univariable ordinal logistic regression analyses for OCT-based ischemic severity.
| Variable | OR | 95% CI | p-value |
|---|---|---|---|
| CMT | 1.040 | 1.018–1.063 | <0.001 |
| WBC (×10⁹/L) | 1.493 | 1.051–2.119 | 0.025 |
| Neutrophil count (×10⁹/L) | 1.948 | 1.224–3.099 | 0.005 |
| NLR | 2.659 | 1.240–5.703 | 0.012 |
| SII | 1.004 | 1.001–1.008 | 0.005 |
| Dyslipidemia | 0.567 | 0.167–1.916 | 0.361 |
| Presence of cilioretinal artery | 2.852 | 0.537–15.120 | 0.218 |
OR=odds ratio; CI=confidence interval; CMT=central macular thickness; NLR=neutrophil-to-lymphocyte ratio; WBC=white blood cell count; SII=systemic immune-inflammation index.
Table 6.
Multivariable ordinal logistic regression. CMT= central macular thickness; NLR= neutrophil-to-lymphocyte ratio.
Table 6.
Multivariable ordinal logistic regression. CMT= central macular thickness; NLR= neutrophil-to-lymphocyte ratio.
| Variable | OR | 95% CI | p-value |
|---|---|---|---|
| CMT | 1.052 | 1.022–1.083 | 0.001 |
| NLR | 8.398 | 1.799–39.213 | 0.007 |
Higher NLR was associated with increased odds of more severe ischemia (OR 8.398, 95% CI 1.799–39.213; p = 0.007), while CMT also showed a significant association (OR 1.052, 95% CI 1.022–1.083; p = 0.001). The model demonstrated good explanatory power (Nagelkerke R² = 0.804) and satisfied the proportional odds assumption (test of parallel lines, p > 0.05).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



