Submitted:
21 February 2026
Posted:
26 February 2026
You are already at the latest version
Abstract
Objectives: To provide an evidence-based reference for preventing and managing pediatric acute asthma exacerbations by examining epidemiology and long-term trends of hospitalized cases in Beijing over 30 years. Methods: Retrospective analysis of clinical data from children hospitalized for acute asthma exacerbation at Peking University Third Hospital from 1994 to 2023. Data included demographics, onset timing, and hospital stay duration. Participants were categorized into three age groups: toddlerhood (≥1–3 years), preschool age (≥3–7 years), and school age (≥7–15 years) to assess the distribution of pediatric patients across different years, seasons, and months. Results: The study included 1,106 pediatric patients (65.73% male, 34.27% female) with a median age of 4 years. Hospitalizations peaked in 1999 (8.40%) and declined, reaching the lowest point in 2020 (1.45%) during the COVID-19 pandemic. Most admissions occurred in autumn (34.27%), especially in October (13.29%). Preschool and school-age children had higher admissions in autumn, while infants had more admissions in winter and spring. The average hospital stay was 5.35 ± 2.65 days, longest for infants, with no deaths reported. Conclusions: Over 30 years, pediatric hospitalizations for acute asthma exacerbations in Beijing have declined. The majority of patients were male and preschool-age, with peak admissions in autumn. These findings suggest improved asthma management but highlight the need for enhanced prevention and management strategies, especially for male patients, school-age children, and during autumn, to reduce acute exacerbations and hospitalizations. The results suggest that while asthma management for children has improved, further enhancement of prevention and control strategies is still needed. Targeted efforts to reduce acute exacerbations and hospitalizations remain crucial.
Keywords:
children
; allergy
; asthma exacerbation
; epidemiology
1. Introduction
Asthma is the most prevalent chronic respiratory condition that is not caused by infection in childhood. In the last 30 years, rapid industrialization has led to significant changes in lifestyles and living environments, which have been accompanied by a no-table increase in the prevalence of childhood asthma nationwide. However, there has also been a remarkable improvement in the standardization of diagnosis and manage-ment during the same period. Consistent with domestic and international data from recent decades, the global prevalence of childhood asthma continues to rise persis-tently [1,2]. Asthma has substantial negative effects on children, hindering their phys-ical growth and development, affecting their mental health, and imposing considerable psychological distress and economic burden on both families and society [3].
Therefore, examining the causes behind these acute asthma exacerbations and working to reduce the hospitalization rates associated with them is vital for decreasing the incidence and mortality related to childhood asthma.
The pathogenesis of bronchial asthma is a highly complex process. Although the underlying mechanisms are not fully understood, increasing evidence indicates that asthma results from the combined effects of genetic and environmental factors [4]. However, environmental conditions, climate, and demographic characteristics vary significantly by region. As the capital of China, Beijing faces unique geographical chal-lenges, including high air pollution, which makes epidemiological analysis of asthma in this region particularly important. Acute exacerbations of asthma are the leading reason for hospital admissions among children with this condition, with approximate-ly 17% of pediatric patients with asthma requiring inpatient management [5]. In critical cases, it may even pose a risk to children’s lives. Therefore, assessing the etiological factors underlying acute exacerbation of asthma and reducing the hospitalization rate related to such episodes are critical for lowering the morbidity and mortality of child-hood asthma.
Based on this, this study conducted a retrospective analysis of the clinical data of children aged 1–15 years who were hospitalized due to acute asthma exacerbation in Beijing from 1994 to 2023. The primary goal was to investigate the clinical characteris-tics of these patients, to provide evidence-based resources for the prevention, treat-ment, and long-term management of acute asthma exacerbation in childhood in Beijing, and the findings are reported as follows.
2. Materials and Methods
2.1. General Information
This study included 1,106 children aged 1–15 years with acute asthma exacerba-tion admitted from January 1994 to December 2023 to the Department of Pediatrics, Peking University Third Hospital. Based on age, the patients were stratified into the following three groups: toddlerhood (1 ≤ age < 3 years), preschool age (3 ≤ age < 7 years), and school age (7 ≤ age < 15 years).
It was infeasible to conduct informed consent notification and obtain signed informed consent forms, as this study is a retrospective analysis based on clinical medical record data with an extended time span. The need for signing relevant informed consent forms was waived on the premise of maximizing the protection of patients’ rights, interests, and privacy, following submission to and review by the Medical Ethics Committee of Peking University Third Hospital. Ethics Approval Number: M20250542.
2.2. Inclusion and Exclusion Criteria
Inclusion criteria were as follows: (1) Pediatric inpatients who met the diagnostic criteria for childhood asthma issued in China across different eras [6,7,8,9,10]; (2) Those aged 1 to 15 years old (inclusive of 1 and 15 years old); and (3) Those with complete medical records.
Exclusion criteria were as follows: (1) Children with asthma in the clinical remission or chronic persistent phase; (2) Children who have enrolled multiple times during the same acute exacerbation phase; (3) Those with specific respiratory system diseases such as bronchial foreign bodies, respiratory tract malformations, lung tumors, or lung trauma; and (4) Those with severe diseases involving other systems including the heart, brain, liver, gastrointestinal tract, and kidneys.
2.3. Methods
This study analyzed demographic (age, gender, date of birth) and clinical data (visit year, visit season, visit month, length of hospital stay) from 1994 to 2023 of hospitalized children aged 1-15 years with acute asthma exacerbation. The gender distribution of the children was specifically examined, and the distribution characteristics by different years, seasons, months, and lengths of hospital stay were also assessed.
2.4. Statistical Methods
SPSS 24.0 software was used for statistical data analysis. Descriptive analysis was employed to examine the general demographic characteristics of hospitalized children with acute asthma exacerbation. Measurement data conforming to normal distribution were expressed as mean ± standard deviation (x̄ ± SD); for those not conforming to normal distribution, median and interquartile range were used. T-test and one-way analysis of variance (ANOVA) were commonly used for assessing measurement data, while chi-square test (χ2 test) and rank sum test were used for analyzing count data. The statistical significance was set at p < 0.05.
3. Results
3.1. Gender Distribution of Hospitalized Children with Acute Asthma Exacerbation
This study enrolled 1106 hospitalized children with acute asthma exacerbation, consisting of 727 males (65.73%) and 379 females (34.27%).
3.2. Age (Group) Distribution of Hospitalized Children with Acute Asthma Exacerbation
The median age of hospitalized children with acute asthma exacerbation in this study was 4 years (interquartile range, IQR: 2–7). The participants were stratified into the following three age groups: toddlerhood (1 ≤ age < 3 years), preschool age (3 ≤ age < 7 years), and school age (7 ≤ age < 15 years), with 306, 517, and 283 cases, respectively. The preschool age group accounted for approximately half of the total cohort, which is the highest proportion (46.75%), followed by the toddlerhood group, which constituted more than a quarter (27.67%) of the patients.
3.3. Gender Differences in Hospitalized Children with Acute Asthma Exacerbation Across Different Age Groups
The number of male hospitalized children with acute asthma exacerbation was consistently higher than that of females across all age groups. Specifically, the male-to-female ratio was approximately 2.5:1 (218 vs. 88), 1.8:1 (334 vs. 183), and 1.6:1 (175 vs. 108) in the toddlerhood, preschool age, and school age groups, respectively. Figure 1 illustrates these gender disparities across age strata.
Males were predominant than females across all age groups, with gender disparities diminishing with increasing age. A significant difference in gender distribution among the three groups (χ2 = 6.322, P < 0.05; Table 1) was exhibited through statistical analysis. Post-hoc pairwise comparisons showed no significant differences between toddlerhood and preschool age (χ2 = 3.836, P = 0.05) or between preschool and school age (χ2 = 0.605, P = 0.437). However, a remarkable difference was noted between toddlerhood and school age (χ2 = 5.856, P = 0.016).
3.4. Annual Distribution of Hospitalized Children with Acute Asthma Exacerbation
From 1994 to 2023, 1,106 children with acute asthma exacerbation were admitted to Peking University Third Hospital. Between 1994 and 1997, the annual admissions remained relatively stable, followed by a significant increase in 1998 and a peak in 1999. After 2000, the total number of admissions generally showed a gradual decline, with two minor peaks documented in 2013 and 2018–2019. In 2020, admissions dropped to their lowest level and subsequently demonstrated a slow upward trajectory over 2021–2023. The annual admission figures are illustrated in Figure 2.
3.5. Monthly Distribution of Hospitalized Children with Acute Asthma Exacerbation
Figure 3 illustrates the monthly distribution of hospitalized children with acute asthma exacerbation at Peking University Third Hospital between 1994 and 2023. The highest monthly admission volume was in October (147 cases, 13.29%), followed by November (126 cases, 11.39%) and September (106 cases, 9.58%). In contrast, February had the lowest reported number of admissions (45 cases, 4.06%).
3.6. Seasonal Distribution of Hospitalized Children with Acute Asthma Exacerbation
Hospitalized children admitted to Peking University Third Hospital between 1994 and 2023 owing to acute asthma exacerbation were categorized according to season based on meteorological standards as follows: spring (March–May), summer (June–August), autumn (September–November), and winter (December–February of the following year). As illustrated in Figure 4, autumn was consistently the peak season for admissions. The number of hospitalized patients in each season was as follows: spring, 263 cases (23.78%); summer, 247 cases (22.33%); autumn, 379 cases (34.27%); and winter, 217 cases (19.62%).
3.7. Seasonal Distribution of Hospitalized Children with Acute Asthma Exacerbation Across Different Age Groups
The seasonal distribution of hospitalized children with acute asthma exacerbation varied across age groups. Preschool and school-age children consistently demonstrated an autumn peak in admissions, as illustrated in Figure 5, whereas toddlerhood children demonstrated a higher admission volume in spring and winter.
3.8. Seasonal Distribution of Hospitalized Children with Acute Asthma Exacerbation by Gender.
Both genders demonstrated an autumn peak in the seasonal distribution of hospitalized cases, as depicted in Figure 6.
3.9. Length of Hospital Stay in Children with Acute Asthma Exacerbation
The mean length of hospital stay (LOS) for children admitted with acute asthma exacerbation was 5.35 ± 2.65 days over the 30 years from 1994 to 2023. The overall trend showed a downward decline, followed by a stable plateau from 2004 onward, with the lowest LOS documented in 2020 (Figure 7).
3.10. Length of Hospital Stay (LOS) for Acute Asthma Exacerbation Across Different Age Groups
There was a statistically significant difference in LOS among hospitalized children with acute asthma exacerbation across distinct age groups (F=5.19, P=0.006). The toddlers demonstrated the longest duration of hospitalization. Post-hoc pairwise comparisons showed that toddlers had a significantly longer LOS than both preschool and school-age children (F=1.068 and 9.339, respectively; both P<0.05). In contrast, there was no statistically significant difference in LOS between preschool and school-age children (F=19.393, P>0.05). These results are illustrated in Figure 8.
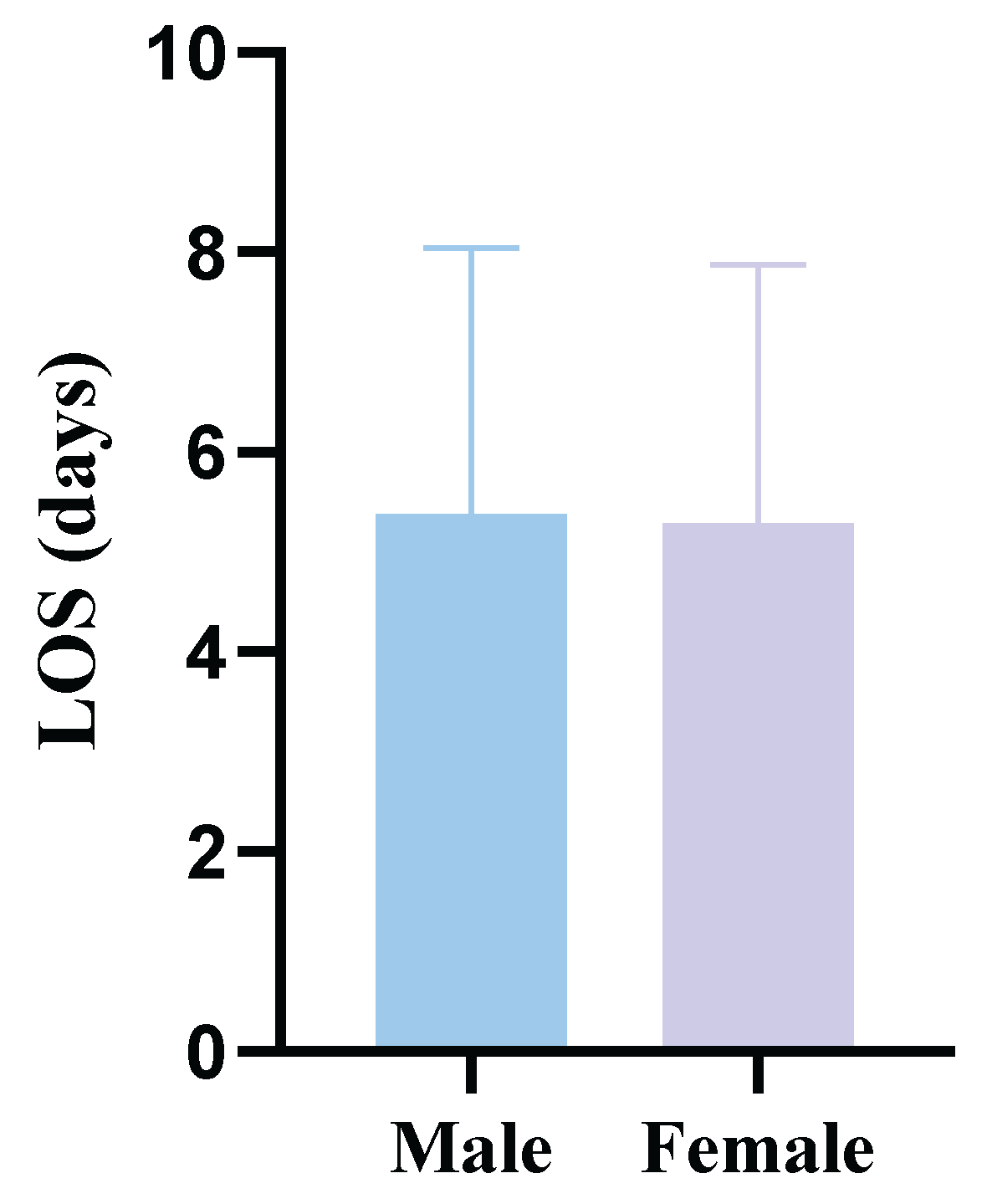
3.12. Length of Hospital Stay (LOS) for Acute Asthma Exacerbation by Gender
There was no statistically significant difference in LOS between males and females among hospitalized children with acute asthma exacerbation (males: 5.38 ± 2.66 days; females: 5.29 ± 2.58 days; F=0.95, P=0.58).
Figure 9.
Differences in Length of Hospital Stay (LOS) among hospitalized children with acute asthma exacerbation by gender.
Figure 9.
Differences in Length of Hospital Stay (LOS) among hospitalized children with acute asthma exacerbation by gender.
4. Discussion
Allergic diseases have emerged as a significant public health challenge that requires prioritization for prevention, control, and research in the 21st century. Acute asthma exacerbations are among the most frequent causes of hospital admissions for children; the costs account for a substantial portion of total asthma-related medical expenses, placing considerable economic and psychological burdens on families [11]. Timely, proactive and effective interventions are essential for alleviating acute exacerbations of bronchial asthma in children and preventing life-threatening developments. This study aims to investigate the epidemiological patterns of hospitalization and the temporal trends of acute asthma exacerbations in Chinese children by conducting a retrospective analysis of clinical data.
This study found that male children represented a higher proportion than female children among those admitted for acute asthma exacerbation, with a male-to-female ratio of approximately 1.9:1—supporting results from earlier studies [12]. This male predominance is in line with the overall incidence pattern of childhood asthma, where boys are more frequently affected than, reflecting the gender distribution seen in hospitalized cases of acute exacerbation. During childhood, the incidence of asthma is persistently higher in males compared to females [13]. Importantly, this gender-related difference in incidence is consistent with the gender distribution of pediatric patients hospitalized for acute asthma exacerbations. In addition, male sex has been recognized as an independent risk factor for unresolved asthma in the pediatric population. Several factors may contribute to this gender disparity. Physiologically, male children tend to possess narrower airways, which makes them more vulnerable to airflow limitation when there are fluctuations in airway tension. Moreover, their IgE levels are typically higher than those of females, enhancing their susceptibility to airway hyperresponsiveness and subsequent increase of respiratory smooth muscle tension. Behaviorally, male children participate in more outdoor activities compared to their female counterparts, leading to more frequent exposure to pathogenic agents [14,15]. Notably, this gender disparity diminishes over the course of asthma. In this study, the ratio of male-to-female hospitalized children with acute asthma exacerbation varied across age groups: approximately 2.5:1, 1.8:1, and 1.6:1 in toddlers, preschoolers, and school-age children, indicating a gradual narrowing trend with increasing age. Epidemiological studies on asthma in both adults and children have observed a reversal of this gender distribution, while asthma is more prevalent in young boys, adult women exhibit a higher prevalence. This implies that the onset of asthma may be associated with an individual’s hormonal secretions [16,17].
Asthma can occur throughout life; however, it is especially common in childhood. Epidemiological studies show that 87.6% of children with asthma experience their first acute exacerbation by the age of 5 years [18]. This study revealed that the average age of children hospitalized for acute asthma exacerbations was 4 years. Preschool children represented the largest proportion (46.75%), followed by toddlers (27.67%), which is in accordance with the evidence reported in existing literature [19]. In China, kindergarten enrollment typically begins at the age of 3 years. Upon entering kindergarten, children may struggle to adjust to the new environment and are at higher risk for cross-infections—respiratory tract infections are widely recognized as a key precipitating factor for asthma exacerbations. Some researchers argue that the clinical manifestations of asthma in young children are not very specific. Additionally, young children cannot participate in pulmonary function tests, making the objective assessment of airflow limitation and airway inflammation challenging. Moreover, many children with wheezing before 3 years discontinue wheezing episodes after 6 years, leading to the consensus that bronchial asthma should not be diagnosed prematurely in this young population [20]. However, this study exhibited a higher rate of hospitalization among younger children compared to older age groups. Therefore, early accurate diagnosis and timely intervention for asthma in young children are critical for preventing asthma exacerbations and optimizing long-term clinical outcomes.
The primary triggers for acute exacerbations are weather fluctuations, upper respiratory tract infections, and inhaled allergens [21,22]. Notably, acute asthma exacerbations demonstrate distinct seasonal variations and regional differences across geographical areas. Seasonal disparities in exacerbation rates are often associated with the seasonal shifts of triggering factors, while regional variations are primarily attributed to differences in local climatic conditions [23,24]. In this study, October was revealed as the month with the highest admission volume on analysis of 30-year data on children hospitalized for acute asthma in Beijing. The top three months for admissions were October (147 cases, 13.29%), November (126 cases, 11.39%), and September (106 cases, 9.58%), whereas February recorded the lowest number of cases (45 cases, 4.1%). A positive correlation between the number of emergency department visits for asthma exacerbations and ambient pollen concentrations was further confirmed by a 26-year longitudinal study [25]. Beijing features remarkable seasonal changes owing to its location in the temperate zone—autumn, in particular, is characterized by dry weather, abrupt climatic shifts, and significant diurnal temperature variations. In addition, the proliferation and prevalence of various pathogens, coupled with increased exposure to flowering plants, collectively enhance the risk of acute asthma exacerbations in children [26]. During this season, indoor dust mite levels also fluctuate seasonally; Sun et al. [27] reported that dust mite density in residential environments reaches its annual peak in autumn. The seasonal distribution of acute exacerbations varied across different age groups: preschool and school-age children demonstrated an autumn peak, while toddlers exhibited a predominance of exacerbations in spring and winter. A plausible explanation for acute asthma exacerbations is that respiratory tract infections play a significant role in triggering these events. The high incidence of occurrence of exacerbations during autumn among preschool and school-age children may be attributed to the increased prevalence of cross-infections following school enrollment. Understanding the marked seasonal variations in acute asthma exacerbations is essential for enhancing asthma prevention and control strategies. This insight highlights the importance of implementing targeted preventive measures against respiratory tract infections in children before the onset of autumn each year.
This study was limited by the sole analysis of hospitalization data for acute asthma exacerbations in children. Future studies should expand the collection of data to include the incidence of childhood asthma in Beijing, specific triggers of acute exacerbation episodes, age at the initial onset, treatment modalities, and clinical outcomes. Such comprehensive analyses will offer more robust data support for the prevention and management of acute asthma exacerbations in children in Beijing.
5. Conclusions
In conclusion, male patients outnumbered female patients among children aged 1–15 years hospitalized for acute asthma exacerbations in Beijing. Preschool children comprised the largest proportion of admissions, with the highest hospitalization rate occurring in autumn and a distinct peak in October. Comprehensive prevention and control strategies should be customized to reduce the incidence and hospitalization rate of childhood acute asthma exacerbations, based on the environmental characteristics of Beijing.
Author Contributions
Conceptualization, X.Z. and Y.X.; methodology, X.Z.; software, M.L.; validation, K.L., Y.X.; formal analysis, M.L.; investigation, Y.X.; resources, Y.X.; data curation, K.L.; writing—original draft preparation, X.Z; writing—review and editing, Y.X.; visualization, Z.G; supervision, Y.X.; project administration, Y.X.; funding acquisition, Y.X. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Innovation and Translation Fund of Peking University Third Hospital (BYSYZHKC126) and National Science and Technology Major Project (2025ZD0548700).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Medical Ethics Committee of Peking University Third Hospital(protocol code M20250542, 31 July 2025). Ethics Approval Number: M20250542.
Informed Consent Statement
Patient consent was waived. Because this article is a retrospective study, the involvement of data from the past 30 years, and it is difficult to obtain the signature of informed consent.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding authors.].
Acknowledgments
Thanks to all the staff and patients and their families who participated in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| LOS | Length of Hospital Stay |
| ANOVA | One-way analysis of variance |
| IQR | Interquartile range |
References
- Stern, J.; Pier, J.; Litonjua, A.A. Asthma epidemiology and risk factors. Semin. Immunopathol. 2020, 42, 5-15.
- Zhou, W.; Tang, J. Prevalence and risk factors for childhood asthma: a systematic review and meta-analysis. BMC Pediatr. 2025, 25, 50. [CrossRef]
- Shin, Y.H.; Hwang, J.; Kwon, R.; Lee, S.W.; Kim, M.S.; Shin, J.I.; Yon, D.K. Global, regional, and national burden of allergic disorders and their risk factors in 204 countries and territories, from 1990 to 2019: A systematic analysis for the Global Burden of Disease Study 2019. Allergy 2023, 78, 2232-2254. [CrossRef]
- Wang, J.; Zhou, Y.; Zhang, H.; Hu, L.; Liu, J.; Wang, L.; Wang, T.; Zhang, H.; Cong, L.; Wang, Q. Pathogenesis of allergic diseases and implications for therapeutic interventions. Signal Transduct. Target. Ther. 2023, 8, 138. [CrossRef]
- Ducharme, F.M.; Zemek, R.; Chauhan, B.F.; Gravel, J.; Chalut, D.; Poonai, N.; Guertin, M.C.; Quach, C.; Blondeau, L.; Laberge, S. Factors associated with failure of emergency department management in children with acute moderate or severe asthma: a prospective, multicentre, cohort study. Lancet Respir. Med. 2016, 4, 990-998. [CrossRef]
- National Cooperative Group on Childhood Asthma Control. Standard procedures for diagnosis and treatment of childhood asthma (trial version). Chin. J. Tuberc. Respir. Dis. 1993, 16, 10-12.
- National Cooperative Group on Childhood Asthma Control. Standardized procedures for childhood asthma prevention and treatment (trial version). Chin. J. Pediatr. 1998, 24-27.
- Subspecialty Group of Respiratory Diseases, Society of Pediatrics, Chinese Medical Association; Editorial Board of Chinese Journal of Pediatrics. Guidelines for childhood bronchial asthma prevention and treatment (trial version). Chin. J. Pediatr. 2004, 42, 100-106.
- Subspecialty Group of Respiratory Diseases, Society of Pediatrics, Chinese Medical Association; Editorial Board of Chinese Journal of Pediatrics. Guidelines for the diagnosis, prevention and treatment of childhood bronchial asthma. Chin. J. Pediatr. 2008, 46, 745-753.
- Subspecialty Group of Respiratory Diseases, Society of Pediatrics, Chinese Medical Association; Editorial Board of Chinese Journal of Pediatrics. Guidelines for the diagnosis, prevention and treatment of childhood bronchial asthma (2016 edition). Chin. J. Pediatr. 2016, 54, 167-181.
- Pijnenburg, M.W.; Fleming, L. Advances in understanding and reducing the burden of severe asthma in children. Lancet Respir. Med. 2020, 8, 1032-1044. [CrossRef]
- Cheng, J.; Tsang, Y.P.; Lam, Y.Y.; Chu, A.K.Y.; Ng, C.S.Y.; Chan, C.H.Y.; Fung, Y.L.; Chau, P.S.Y.; Luk, D.C.K. Prevalence and severity of asthma among school children in Hong Kong. Hong Kong Med. J. 2024, 30, 371-379. [CrossRef]
- Wang, T.; Shi, H.; Wan, G.; Zhao, Z.; Norback, D.; Pu, G.; Ma, S.; Dong, H.; Yao, J.; Lu, J.; et al. Prevalence and influencing factors of wheeze and asthma among preschool children in Urumqi city: a cross-sectional survey. Sci. Rep. 2023, 13, 2263. [CrossRef]
- Namysłowski, A.; Lipiec, A.; Zieliński, W.; Piekarska, B.; Raciborski, F.; Szylling, A.; Samel-Kowalik, P.; Walkiewicz, A.; Borowicz, J.; Samoliński, B. Place of residence, gender, month of birth and age influence on the concentration of specific IgE antibodies in serum. The Epidemiology of Allergic Diseases in Poland (ECAP survey): part three. Postepy Dermatol. Alergol. 2022, 39, 800-805. [CrossRef]
- Zein, J.G.; Denson, J.L.; Wechsler, M.E. Asthma over the adult life course: Gender and hormonal influences. Clin. Chest Med. 2019, 40, 149-161.
- Chowdhury, N.U.; Guntur, V.P.; Newcomb, D.C.; Wechsler, M.E. Sex and gender in asthma. Eur. Respir. Rev. 2021, 30, 210067. [CrossRef]
- Rosas-Salazar, C.; Chirkova, T.; Gebretsadik, T.; Chappell, J.D.; Peebles, R.S., Jr.; Dupont, W.D.; Jadhao, S.J.; Gergen, P.J.; Anderson, L.J.; Hartert, T.V. Respiratory syncytial virus infection during infancy and asthma during childhood in the USA (INSPIRE): a population-based, prospective birth cohort study. Lancet 2023, 401, 1669-1680. [CrossRef]
- Moral, L.; Vizmanos, G.; Torres-Borrego, J.; Praena-Crespo, M.; Tortajada-Girbés, M.; Pellegrini, F.J.; Asensio, Ó. Asthma diagnosis in infants and preschool children: a systematic review of clinical guidelines. Allergol. Immunopathol. 2019, 47, 107-121. [CrossRef]
- Jackson, D.J.; Gern, J.E. Rhinovirus infections and their roles in asthma: Etiology and exacerbations. J. Allergy Clin. Immunol. Pract. 2022, 10, 673-681. [CrossRef]
- Bacharier, L.B.; Guilbert, T.W.; Jartti, T.; Saglani, S. Which wheezing preschoolers should be treated for asthma? J. Allergy Clin. Immunol. Pract. 2021, 9, 2611-2618. [CrossRef]
- Mahesh, S.; Ramamurthy, M.B. Management of acute asthma in children. Indian J. Pediatr. 2022, 89, 366-372.
- Jones, H.; Lawton, A.; Gupta, A. Asthma attacks in children-challenges and opportunities. Indian J. Pediatr. 2022, 89, 373-377. [CrossRef]
- Zheng, J.; Yue, L.; Wang, B.; Li, Y.; Zhang, L.; Xue, B.; Tian, X.; Lei, R.; Luo, B. Seasonal characteristics of ambient temper-ature variation (DTR, TCN, and TV(0-t)) and air pollutants on childhood asthma attack in a dry and cold city in China. En-viron. Res. 2023, 217, 114872. [CrossRef]
- Prapamontol, T.; Norbäck, D.; Thongjan, N.; Suwannarin, N.; Somsunun, K.; Ponsawansong, P.; Radarit, K.; Kawichai, S.; Naksen, W. Asthma and rhinitis in wet and dry season among students in upper Northern Thailand: the role of building dampness and household air pollution. Int. J. Environ. Health Res. 2023, 33, 710-722. [CrossRef]
- Lappe, B.L.; Ebelt, S.; D’Souza, R.R.; Manangan, A.; Brown, C.; Saha, S.; Harris, D.; Chang, H.H.; Sole, A.; Scovronick, N. Pollen and asthma morbidity in Atlanta: A 26-year time-series study. Environ. Int. 2023, 177, 107998. [CrossRef]
- Hu, Y.; Cheng, J.; Jiang, F.; Liu, S.; Li, S.; Tan, J.; Yin, Y.; Tong, S. Season-stratified effects of meteorological factors on childhood asthma in Shanghai, China. Environ. Res. 2020, 191, 110115. [CrossRef]
- Sun, Y.; Cui, L.; Hou, J.; Luo, S.; Norbäck, D.; Sundell, J. Role of ventilation and cleaning for controlling house dust mite allergen infestation: A study on associations of house dust mite allergen concentrations with home environment and life styles in Tianjin area, China. Indoor Air 2022, 32, e13084.Author 1, A.B.; Author 2, C.D. Title of the article. Abbreviated Journal Name Year, Volume, page range. [CrossRef]
Figure 1.
Gender disparities in hospitalized children with acute asthma exacerbation among different age groups.
Figure 1.
Gender disparities in hospitalized children with acute asthma exacerbation among different age groups.
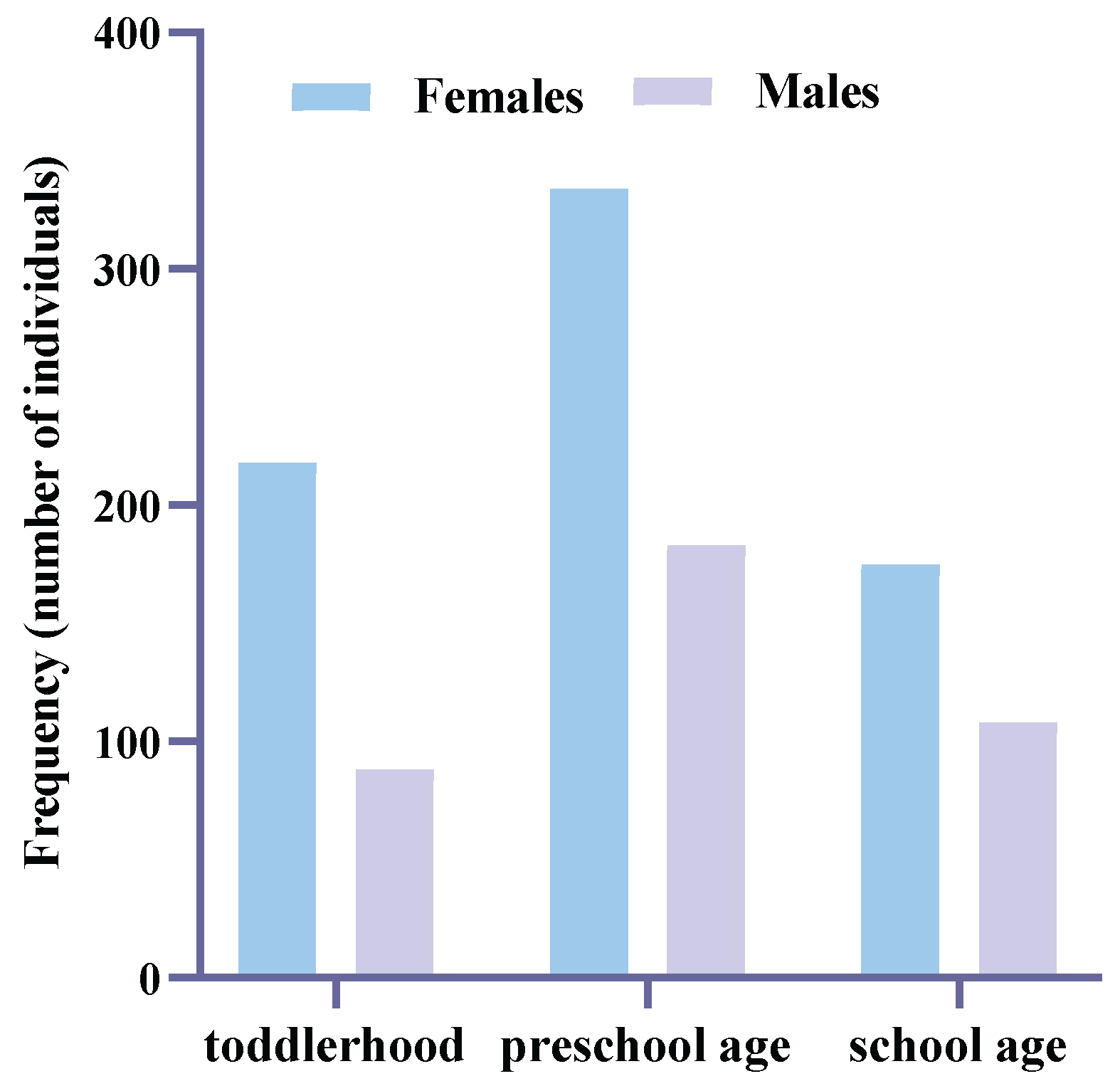
Figure 2.
Annual distribution of hospitalized children with acute asthma exacerbation.
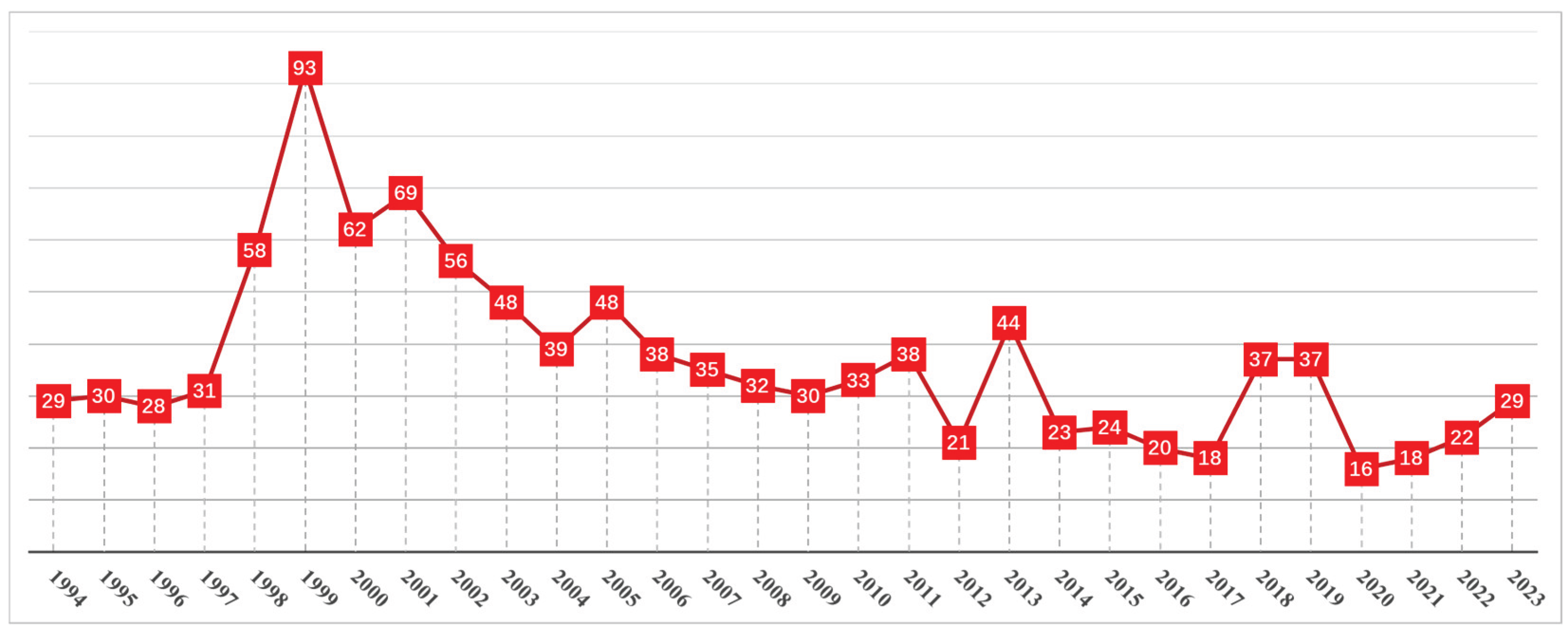
Figure 3.
Monthly distribution of hospitalized children with acute asthma exacerbation.
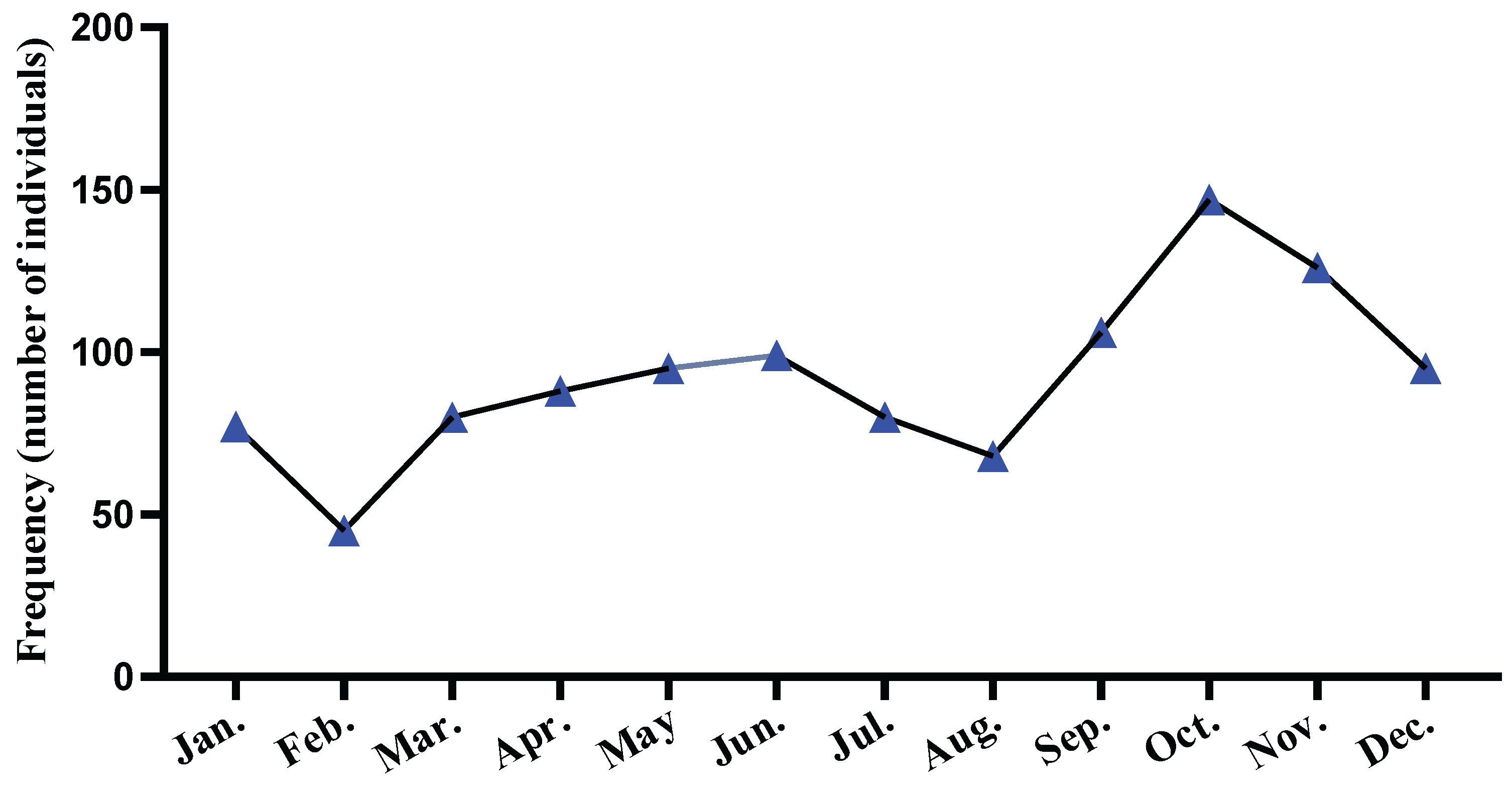
Figure 4.
Seasonal distribution of hospitalized children with acute asthma exacerbation.
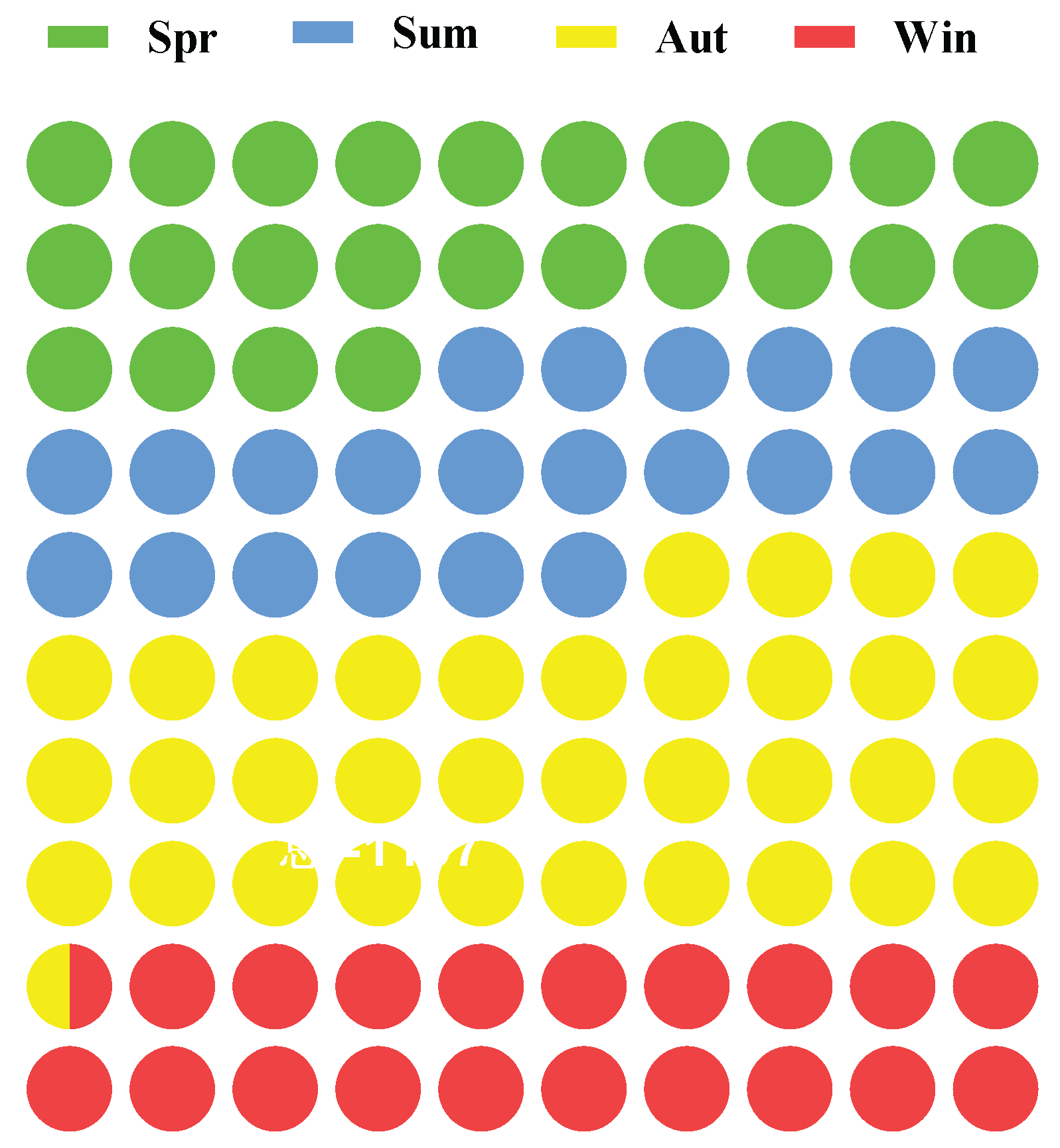
Figure 5.
Seasonal distribution of hospitalized children with acute asthma exacerbation across different age groups.
Figure 5.
Seasonal distribution of hospitalized children with acute asthma exacerbation across different age groups.
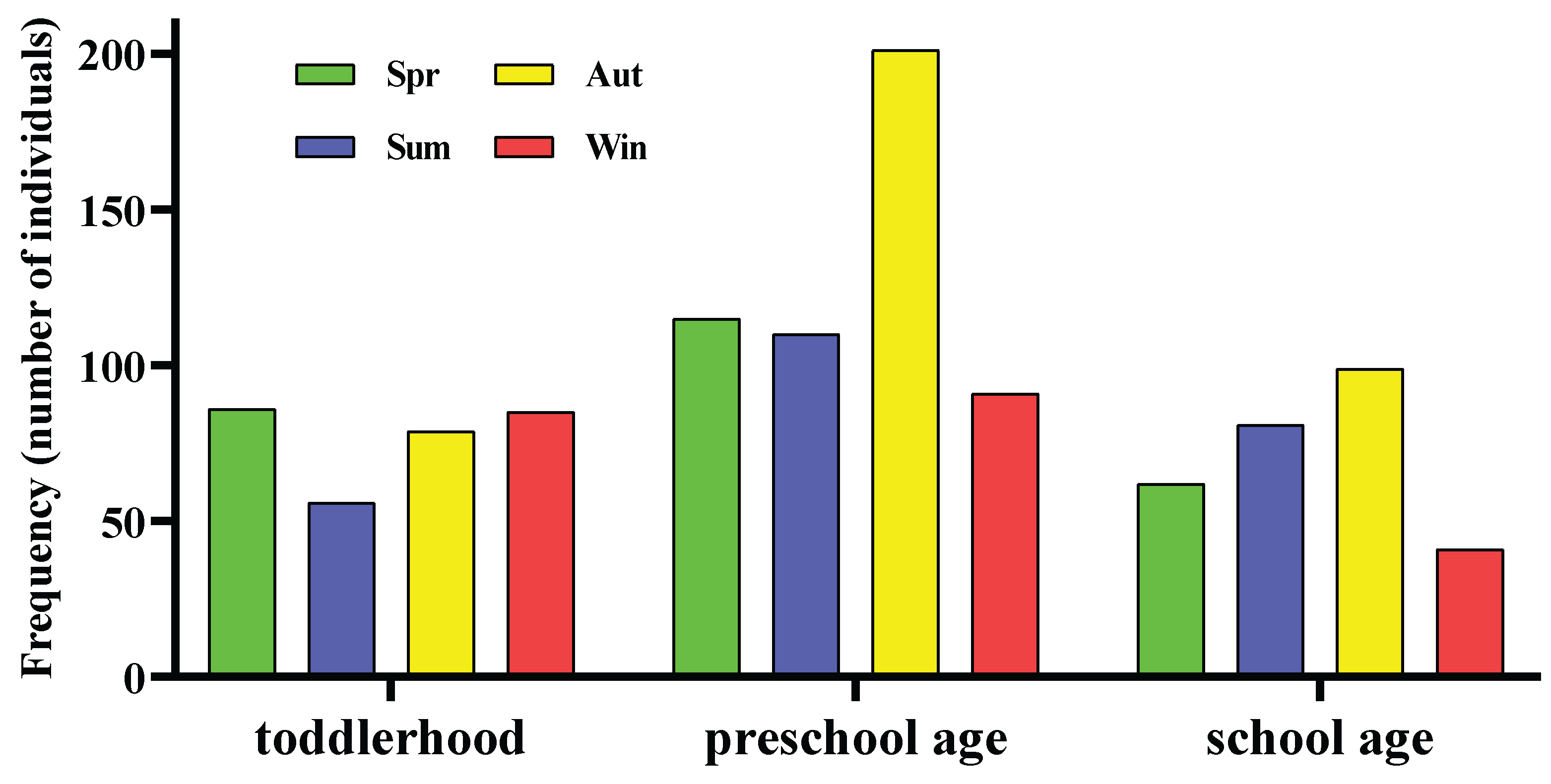
Figure 6.
Seasonal distribution of hospitalized children with acute asthma exacerbation by gender.
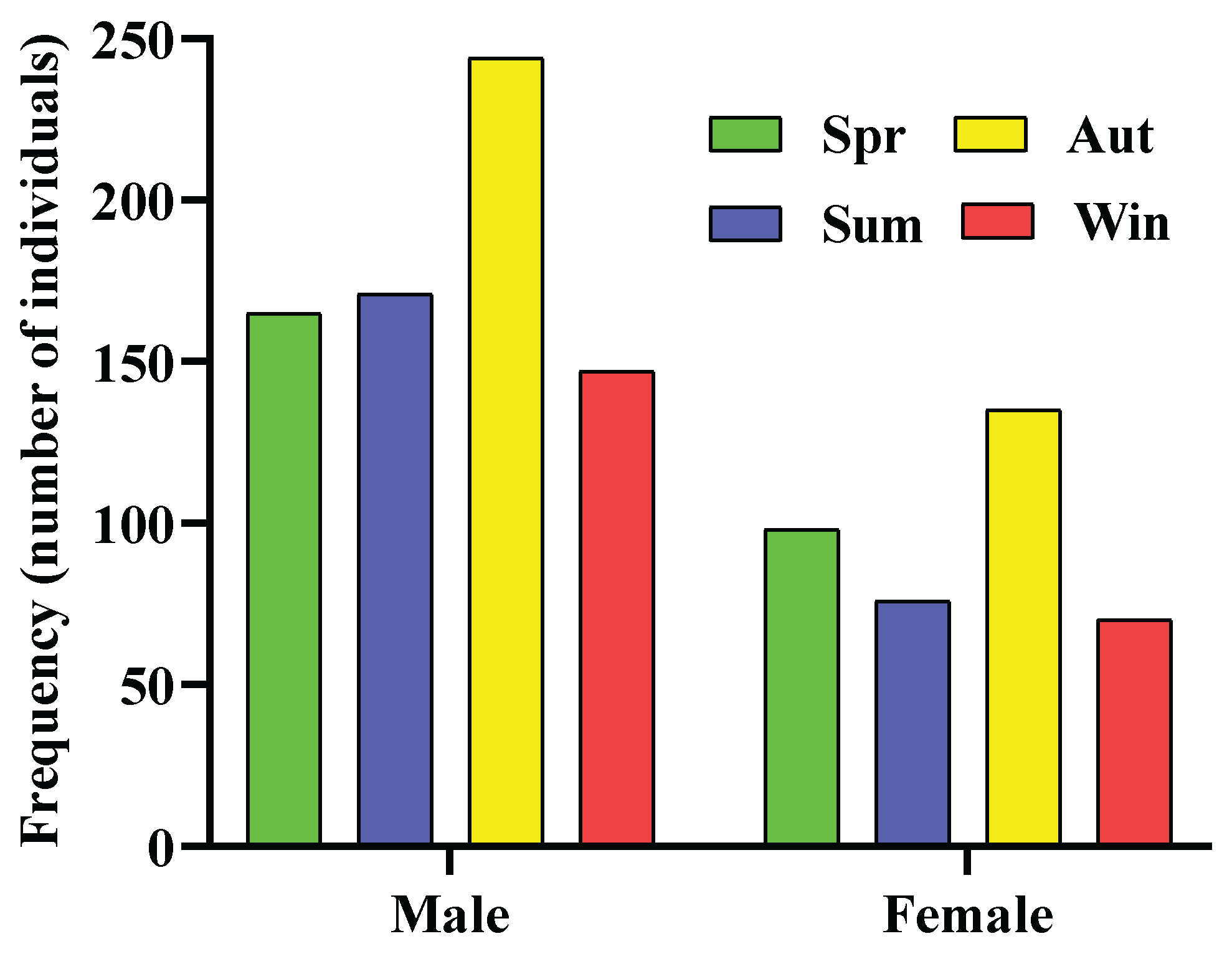
Figure 7.
Annual distribution of mean Length of Hospital Stay (LOS) for acute asthma exacerbation.
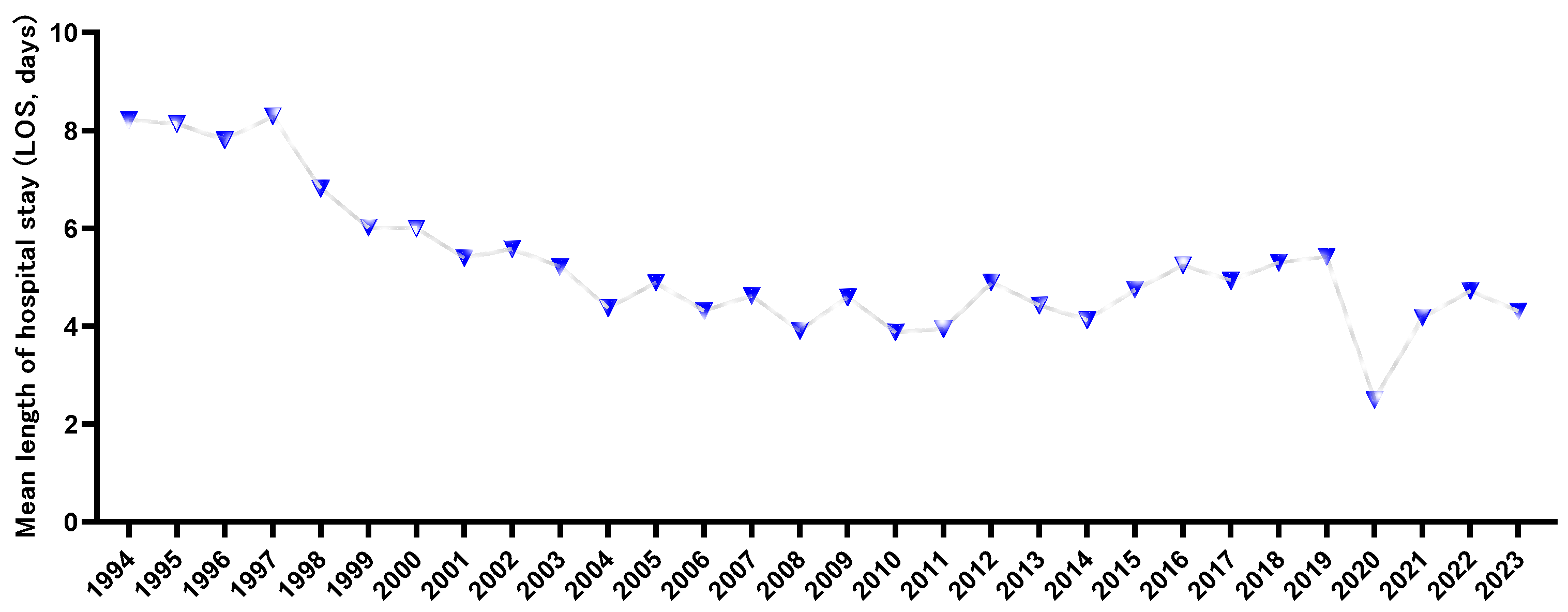
Figure 8.
Differences in the Length of Hospital Stay (LOS) among hospitalized children with acute asthma exacerbation across age groups.
Figure 8.
Differences in the Length of Hospital Stay (LOS) among hospitalized children with acute asthma exacerbation across age groups.
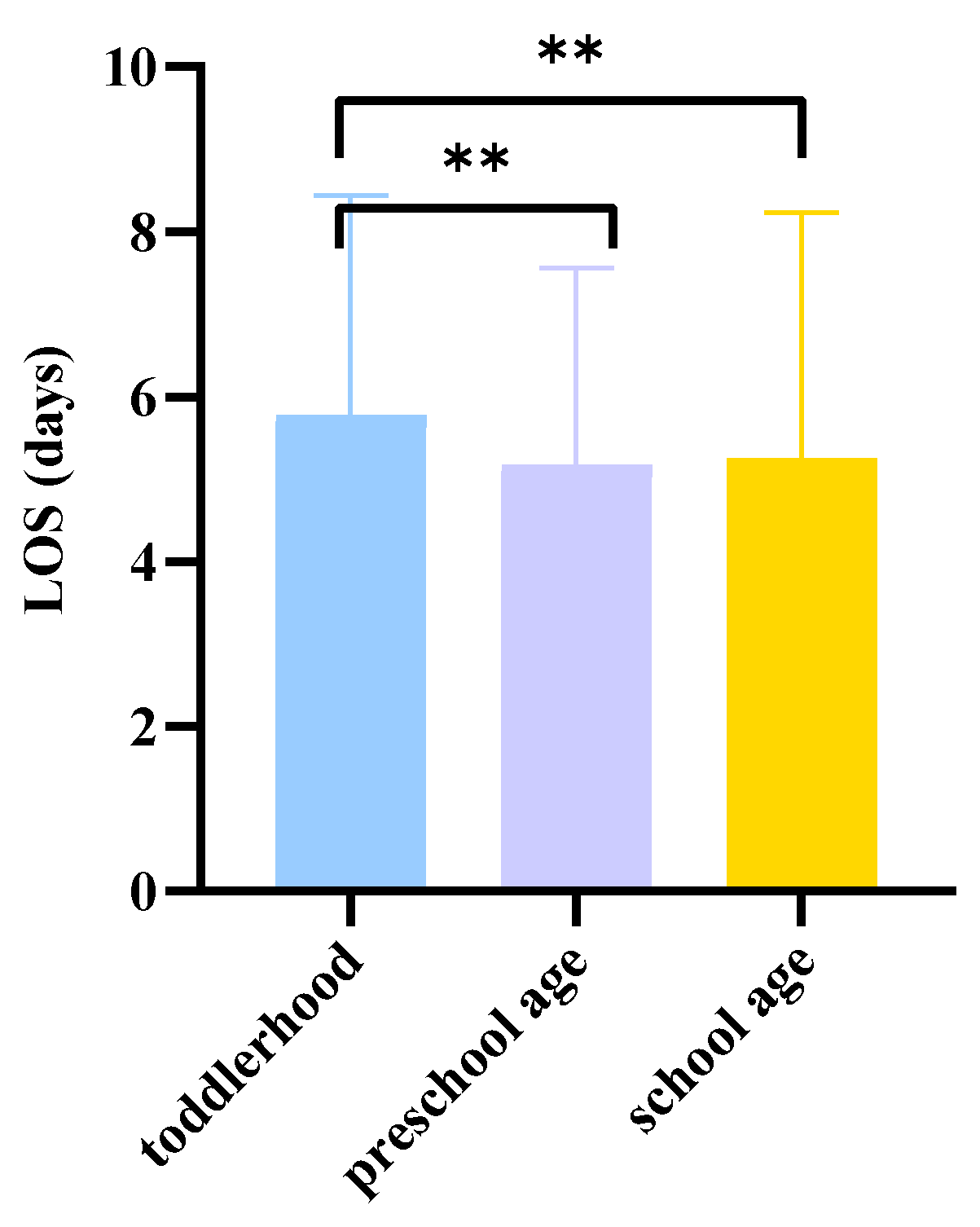

Table 1.
Comparison of gender disparities in hospitalized children with acute asthma exacerbation across different age groups.
Table 1.
Comparison of gender disparities in hospitalized children with acute asthma exacerbation across different age groups.
| Group | Total (n) | Males | Females | χ2 Test | |
|---|---|---|---|---|---|
| χ2 Value | P Value | ||||
| toddlerhood | 306 | 218 (71.24%) | 88 (28.76%) | 6.32 | 0.04 |
| preschool age | 517 | 334 (64.60%) | 183 (35.40%) | ||
| school age | 283 | 175 (61.84%) | 108 (38.16%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



