Submitted:
16 February 2026
Posted:
26 February 2026
You are already at the latest version
Abstract
Background: The aim of the study was to verify the effectiveness of a 5-week intensive protocol of multilayer bandaging alone or in combination with diet, applied to the clinical practice of lipedema.
Methods: 114 women with lipedema were studied, divided into three groups: 35 women were treated with multilayer bandaging in biweekly sessions for 5 weeks, 48 were treated with the same bandaging protocol combined with an anti-inflammatory diet, and 31 women received no treatment. The effect on anthropometry, lower limb volume, pain caused by the tissue fold, and subjective symptoms were evaluated.
Results: Women who completed the 5-week intensive protocol of multilayer bandaging showed a statistically significant reduction in all observed parameters: body weight, waist and hip circumference, lower limb volume, pain, and subjective symptoms. The group of women treated with multilayer bandaging and diet showed a significantly greater reduction in lower limb volume and body weight. The treatments were effec-tive regardless of age, BMI, clinical stage, and the presence of fovea in both groups. The wearing time with the multilayer bandage had a positive correlation in the group treated with bandage in combination with diet.
Conclusion: A 5-week intensive protocol of multilayer bandaging of the lower limbs is an effective treatment for reducing the symptoms and clinical signs of lipedema at all stages of the disease, even in the absence of edema. Adding nutritional therapy during the bandaging cycle increases the effectiveness of the treatment on the volume of the affected extremities and body weight.
Keywords:
lipedema
; pain
; lipoalgia
; inflammation
; compression therapy
; complex decongestive therapy
; multilayer bandage
; anti-inflammatory diet
; subcutaneous fat tissue
; multidisciplinary care team
1. Introduction
Lipedema is a chronic condition with a significant impact on both physical health and psychosocial well-being. Despite the growing interest in the last years due to increased awareness among both patients and health care professionals, lipedema remains underdiagnosed and misunderstood. The disease almost exclusively affects females; female physiological hormonal changes (puberty, pregnancy, menopause), estrogen-progestin use, and weight gain are all factors related to the onset and worsening of the disease. [1]. As such, a multidisciplinary approach is essential for its proper management. Currently, international guidelines and literature describe two ways of treatment: conservative treatment and surgical treatment [2,3,4,5,6,7,8]. This work focuses on conservative treatment: the primary goals of conservative treatment are the reduction or elimination of symptoms (pain, reduced mobility, edema, fibrosis), the improvement of patients’ quality of life, and the prevention of disease progression and related complications [4]. Cardinal points of conservative management include compression therapy, nutrition, weight management, specific physical activity and physiotherapy, patient education and self-management strategies [2,3,4,5,6,7,8].
Complex decongestive therapy (CDT), commonly recommended in the treatment of lymphedema, consistes of manual lymphatic drainage (MLD), physical therapy, multilayer bandaging (MLB), compression garments, and skin care or each individually [9]. Compression therapy is generally considered useful in all consensus documents and guidelines for reducing discomfort, symptoms, and edema, if present. However, there is no unanimous agreement on how to use it, how often, the type of texture, or the indications, which may vary based on patient characteristics and the stage of the disease. Disagreement regarding the indication for using MLB is even more pronounced. If edema or lipolymphedema is present, especially in the initial stages of treatment, MLB is indicated [4,5,6,7,8], emphasizing that the treatment cannot reduce adipose tissue, but only the edematous component. More recent guidelines [7,8] recognize greater importance for this treatment, which recommend its use not only to reduce the edematous component, but also to treat pain and sensitivity in areas affected by lipedema [7,8]. Treatment is also suggested to reduce disease progression and even for early-stage lipedema [8].
Recent evidence from studies on lymphedema, chronic venous insufficiency, and obesity-related adipose disorders suggests that external compression is beneficial not only for its mechanical decongestant action and tissue fluid shift, but also for modulating the biochemical environment and exerting important biological actions on the subcutaneous tissue, including pain modulation, lymphatic stimulation, and inflammation control [7,10,11,12,13,14,15]. Studies have shown that compression reduces interstitial fluid accumulation, improves lymphatic clearance, and increases tissue oxygenation, thereby reducing the burden of pro-inflammatory cytokines such as interleukin 6 (IL-6), tumor necrosis factor-alpha (TNF-α), and monocyte chemoattractant protein 1 (MCP-1). These mechanisms may help interrupt the inflammatory cycle that drives pain, tissue remodeling, and fibrotic progression in lipedema [16,17,18]. Compression appears to influence macrophage behavior within the adipose matrix, promoting a shift from pro-inflammatory M1 macrophages to M2 anti-inflammatory phenotypes, potentially limiting chronic low-grade inflammation [14,18]. Compression may also exert effects on adipose tissue metabolism itself. Preclinical and translational studies have proposed that mechanical compression can inhibit adipogenesis and reduce adiponeogenesis—the formation of new adipocytes from mesenchymal precursors—by suppressing expression of peroxisome proliferator-activated receptor gamma (PPARγ) and CCAAT/enhancer-binding protein alpha (C/EBPα) [10,18]. This phenomenon could be particularly relevant in lipedema, where adipocyte proliferation contributes to the disease progression. Although these findings have been described primarily in animal models and in vitro systems in humans, these phenomena support a particularly important role for compression therapy on the tissues and limb volumes of patients with lipedema. Despite these indications, to date, efficacy studies remain scarce, they are applied differently in each study, on different patient populations, and use different methods to verify efficacy [8,11,20,21,22,23,24].
Among all the non-surgical treatments available, MLB is uniquely positioned for its ability to provide continuous, targeted compression in a customizable format, allowing it to adapt to different limb shapes and provide low pressure at rest: this feature allows the bandage to remain in place even during nights and periods of rest, allowing the patient to wear it for longer periods and therefore improving its effectiveness. Furthermore, the pressure can be modulated in real time, thus representing an optimal strategy in the intensive decongestant phase, during which the shape, tolerability and characteristics of the limbs can be modified [25]. Clinically, the efficacy of MLB in reducing pain and limb volume in lipedema has been supported by multiple observational studies. Szolnoky et al. demonstrated that a short course of complex decongestive therapy including bandaging led to significant improvements in pain scores and functional symptoms [21]. Additional pilot studies have reported decreases in limb circumference and subjective discomfort following compression protocols, even in the absence of dietary intervention or weight loss [24].
One aspect on which all guidelines agree is that the treatment of lipedema must be based on a multidisciplinary approach, whether conservative or surgical. A multidisciplinary approach is essential to address different aspects of the disease, and it is recognized that different approaches enhance the benefits of others. In this regard, nutritional therapy plays a key role: nutritional measures should be an integral part of lipedema treatment. First, all consensus documents agree that weight gain should be prevented and contained as it can contribute to a worsening of general clinical conditions: although nutritional measures are considered mandatory in cases of associated obesity, they must also be considered in the early stages of the disease, even in the absence of obesity [2,3,4,5,6,7,8]. Furthermore, evidence suggests that a nutritional approach is not only important for weight control, but can also modulate inflammation, edema, and improve body composition [26,27,28,29,30,31,32]. There is still no unanimous consensus on the best diet to treat the disease, but there are some key characteristics that diets should adhere to, including: personalized plans for the patient [3,8], plans that reduce glycemic and insulin spikes [2,6,7], and low intake of inflammatory foods or foods that negatively alter the intestinal flora [2,6,7,8]. It is also recommended to avoid short-term diets [4,7], by preferring long-term modifications.
Although scientific evidence is still limited, efficacy data is growing. In recent years, positive effects of the ketogenic diet (standard or mediterranean type) have been demonstrated not only on body weight reduction but also on pain [31,32,33,34,35] and quality of life [34,35], on the improvement of body composition [33,34,35,36,37], and on the reduction of limb circumferences affected by lipedema [33,36,37]. Only two studies are available on the effects of the low-carbohydrate diet, which demonstrated positive effect on pain reduction, quality of life, body composition, and adipose tissue reduction measured by magnetic resonance imaging (MRI) [38,39]. Only one study is available on the modified Mediterranean diet, which was also found to be effective on body composition and quality of life [40,41], but not directly on pain and limb circumference.
Data on the effectiveness of different types of diets on lipedema are scarce. However, the effects of some specific diets, such as the Mediterranean diet and the ketogenic diet, on inflammatory status, pain modulation, glucose and lipid metabolism, and modulation of the gastrointestinal microbiota have been demonstrated in patients with obesity, metabolic syndrome, and other chronic inflammatory diseases [42,43,44,45].
The aim of this study is to support the positive effect of a multilayer bandaging protocol applied to patients with lipedema, alone or in combination with diet, on anthropometric parameters, lower limb volume, pain, and lipedema symptoms.
2. Materials and Methods
2.1. Study Design
This is a retrospective observational study. All patients were recruited from a large population of woman with lipedema, diagnosed between 2023 and 2025. Inclusion criteria were clinical diagnosis of lipedema (stage 1, 2 and 3), age ≥ 18 years, no previous treatments for lipedema (including bandages and compression stockings) or previous surgical treatment. The exclusion criteria included: pregnancy, breastfeeding, major chronic diseases (such as diabetes mellitus, cardiovascular disease, or renal disease), hormonally unbalanced thyroid disease and lymphedema.
The diagnosis, staging and phenotyping of lipedema was based on clinical findings of characteristic symptoms and signs of the disease, as described in our previous studies [1,23,46]. The population was divided into three groups based on the treatment received:
- patients treated with a 5-week multilayer bandage protocol (BEND)
- patients treated with a 5-week multilayer bandage protocol combined with diet (BEND+DIET)
- patients reevaluated after 5 weeks without receiving any treatment and without dietary modification (CONTR)
All participants completed a 5-week treatment or observation period and provided written informed consent. Patients in the treatment groups (BEND, BEND+DIET) were evaluated at baseline (T0) and after 5 weeks of treatment (T1) with an assessment of anthropometric parameters, limb volume, clinical assessment of pain with the Progressive Pain Check (PPC) method, and subjective symptoms with a dedicated questionnaire, as described below. The control group (CONTR) was evaluated at T0 and after 5 weeks with clinical assessment using the PPC method and a repeat of the symptom questionnaire; data on limb volume, weight changes, and waist and hip circumferences for the control group are not available.
2.2. Clinical Assessment
The clinical examination focused on the evaluation of anthropometric parameters (height, weight, and waist circumference) and the presence and extent of pain provoked by pinching subcutaneous tissue. To assess pain provoked we used the PPC method, as described in our previous work [23,46]: gentle but firm pressure was applied to 11 predefined anatomical sites, and pain at each site was rated on a verbal scale from 0 (no pain) to 4 (severe pain). From these data, three indices were calculated: a total score or Ricolfi-Patton Score (RPS) (sum of all 11 sites evaluated, range 0–44), a score for the lower body or the Lower Body Pain Score (LBPS) (sum of scores from 8 lower body sites, range 0–36) and a score for the upper body or the Upper Body Pain Score (UBPS) (sum of scores from 3 upper body sites, range 0–12).
The volume of the lower limbs was calculated using the trunk formula derived from circumferential measurements taken every 4 cm from the ankle to the groin. The volume calculation used the Kuhnke disk method [47].
2.3. Symptom Assessment
Each item quantifies the severity of the symptom using a 6-point Likert-type scale with the following verbal descriptors for each individual question (0 = none, 1 = very mild, 2 = mild, 3 = moderate, 4 = severe, 5 = very severe). The total score ranges from 0 to 85 points. Symptoms can be assessed individually, and a final score can be calculated from the sum of the individual scores, ranging from 0 to 85 [23,46].
2.4. Treatments
2.4.1. Multilayer Bandage Treatment Protocol
Both the BEND and BEND+DIET groups underwent an intensive cycle of multilayer bandaging according to a protocol that our group has standardized and used for several years for the treatment of lipedema. The protocol involves 10 sessions of multilayer, multicomponent bandaging applied twice a week for 5 consecutive weeks. The bandages are applied by experienced physiotherapists, following the recommendation and supervision of a lymphologist (Figure 1).
The bandage consists of three layers (Figure 2). The first layer (sub-bandage layer) includes a dressing and a padding layer, a non-compressive material (foam, 0.4 mm thick) used to protect the vulnerable area and increase pressure at specific points. The second layer is a medium-stretch bandages (70–140 per cent) performed using the herringbone wrapping technique from the ankle to the groin and, if necessary, extended to the abdomen for anchoring. A third layer (over-bandaging) consists of non-woven adhesive tape and tubular material used to stabilize the bandage. These bandages have low resting pressures and working pressures as they work with muscle contraction, this characteristic allows the bandage to be maintained even during night-time and periods of rest, enabling the patient to wear it for longer periods and thereby enhancing its effectiveness. Proper application requires advanced manual skills to ensure effective tissue containment without restricting functional movement, allowing immediate ambulation and active exercise as part of the integrated conservative management (Figure 3). Patients were instructed to wear the bandages for as many hours per day as tolerable, aiming for continuous daytime use. Each patient kept a clinical diary to record the daily duration of bandage wear and any symptoms or adverse events. At the treatment’s conclusion, diaries were collected and the mean wear time per day was computed.
2.4.2. Dietary Intervention
Patients followed a diet based on our protocol, which we have standardized over time based on scientific evidence and on our specific experience with patients with lipedema. For this study, we excluded patients who had been treated with a ketogenic diet, an approach we also use but reserve just for selected cases.
The nutritional plan applied is primarily based on the Mediterranean diet, but modified in some aspects, relating to macronutrient composition and food selection. The macronutrient composition is 40-50% carbohydrates, 20-30% protein, and 30% fat. It is not a carbohydrate-restricted diet; however, the carbohydrate composition generally varies on alternate days, from days with 40% carbohydrates to days with up to 50%. Furthermore, it is recommended to favor medium- and low-glycemic load carbohydrates and to reduce gluten consumption, preferring the use of naturally gluten-free carbohydrates (such as potatoes, corn, peas, rice, etc.). It is also recommended to choose proteins with lower acidifying properties (preferring fish, legumes, and eggs over meat and dairy products) and to consume at least one serving of raw vegetables per day. Generally, no food is eliminated, but it is essential to pay attention to portions, cooking methods, and combinations, as well as choosing foods that are easily digestible, that activate lipid metabolism, improve carbohydrate metabolism, and reduce inflammation. All subjects followed a calorie-restricted diet of approximately 20% of their daily energy needs and their personal nutritional habits. No specific questionnaires were used to evaluate diet and physical activity, which were assessed by nutritionists and doctors during the visits.
2.5. Statistical Analysis
Anthropometric and clinical data were summarized using descriptive statistics and appropriate measures of precision for each variable (continuous or categorical). Continuous variables were reported as mean and standard deviation (SD) when normally distributed, and as median and interquartile range (IQR) when non-normally distributed. The normality of continuous variables was assessed using the Shapiro–Wilk test. Comparisons among the three study groups were performed using one-way analysis of variance (ANOVA) when all groups showed a normal distribution. When at least one group violated the assumption of normality, the non-parametric Kruskal–Wallis test was applied.
Homogeneity of variances across groups was evaluated using Levene’s test. Paired Student’s t-tests or Wilcoxon signed-rank tests were used to compare values before (T0) and after treatment (T1) within each group. For independent samples, unpaired t-tests or Mann-Whitney U tests (Wilcoxon rank-sum) were applied. Differences in categorical variables were evaluated using the Chi-square test or Fisher’s exact test, as appropriate.
To investigate the associations between clinical outcomes and potential predictors, eight separate multivariate linear regression models were performed, stratified by treatment group: compression bandaging alone (BEND) and compression bandaging plus diet (BEND+DIET).
The dependent variables for these models included the average volume of the lower limbs at follow-up (T1), the volume change (percentage), the total symptom questionnaire score at T1, and the lower body pain score at T1. All models were adjusted for a set of predictors, which included age, BMI, average daily duration of bandaging (mean wear time), stage of disease (Stage 2 or Stage 3), the presence of fovea, and the respective dependent variable measured at baseline (T0). All candidate predictors were selected a priori based on clinical relevance. Multicollinearity was assessed using variance inflation factors, while model assumptions were verified through residual diagnostics, which showed no evidence of heteroscedasticity; residual normality was further evaluated using the Shapiro–Wilk test.
For all statistical tests, a p-value < 0.05 was considered statistically significant. All statistical analyses were performed using R software version 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria).
3. Results
3.1. General Description, Phenotypic, and Staging
A total of 114 women with stage 1, 2, or 3 columnar lipedema (Stage 1 34.2%, Stage 2 42.1%, Stage 3 23.7%) were included. Their mean age was 43.2 years (range 19–79 years) and their Body Mass Index was 30.0 (range 19.7–48.9 kg/m2).
The population was divided into 3 groups as follows:
- Bandage-only treatment group (BEND): 35 patients
- Bandage-plus-diet treatment group (BEND+DIET): 48 patients
- Untreated control group (CONTR): 31 patients
Table 1 shows the characteristics of the entire population and of the population divided into 3 groups. Before starting therapy (T0), the groups did not differ in the main clinical characteristics, including body mass index (BMI), clinical stage distribution, lower limb volume, symptom assessment questionnaire score, and tissue fold pain score.
The mean bandage wear time was 24.7 hours (range 8–52 hours); there was no significant difference between the two treatment groups.
3.2. Anthropometric Measurements and Volumes
3.2.1. Anthropometric Measurements
In both treatment groups (BEND and BEND-DIET), we observed a significant reduction in body weight and waist and hip circumferences from T0 to T1. The BEND-DIET group showed a significantly greater reduction in body weight compared to the no-diet group (0.6% vs. 4.4%, respectively) and a greater reduction in waist and hip circumference (P < 0.001 for all) (Table 2). These parameters were not evaluated in the CONTR group.
3.2.2. Lower Limbs Volume
Lower limb volume (right, left, and mean lower limb volumes) was significantly reduced in both treatment groups (p<0.001). The BEND-DIET group showed significantly greater reductions in right, left, and mean lower limb volumes (p<0.001), demonstrating a percentage reduction in mean volume almost double that of the BEND group (from a 5% reduction to a 9% reduction) (Table 2). This parameter was not assessed in the CONTR group.
3.3. Pain
Pain evoked by the subcutaneous fat fold, assessed with the PPC method, was reduced in a statistically significant way in both treatment groups, BEND and BEND+DIET. The reduction was verified for all three indicators RPS, LBPS and the UBPS in both treatment groups (P< 0.001 for all). There were no significant differences in pain reduction between the BEND group and the BEND+DIET group (Table 2 and Table 3).
Evaluating the change in pain scores at individual PPC assessment points, a significant reduction was observed for all assessed points (p<0.001) except for the forearm in both groups. We found no difference in the results obtained in the BEND and BEND-DIET groups at any score point (Table 3).
The control group, which received no treatment and was reevaluated after 5 weeks, showed no significant differences in the 3 pain scores (RPS, LBPS, and UBPS), nor at any individual body site (Table 3). The change observed in the control group compared to the two treatment groups was significant for all 3 scores of the score and for all individual points except for the forearm (Table 3).
3.4. Symptoms
The subjective symptom assessment using the questionnaire showed a significant reduction in the total score and in each individual item for both the BEND and BEND-DIET groups; no difference in the reduction of the total score or in the scores for each item was detected between the two treatment groups (Table 2 and Table 4).
3.5. Multivariate Analysis
Table 5 and Table 6 show the results of the multivariate regression analysis that was carried out to evaluate the impact of the treatment on pain (Lower Body Pain Score, Models 1 and 5), symptoms (Total Symptom Score, Models 2 and 6), mean lower limb volume (Models 3 and 7), and percentage change in lower limb volume (Models 4 and 8) adjusted for potential confounders (baseline variables, age, BMI, stage of the disease, bandage wearing time and pretibial fovea). The analysis was performed for both treatment groups, BEND (Table 5) and BEND+DIET (Table 6).
The final effect on pain, symptoms, and volume is independent of possible confounding factors such as age, BMI, clinical stage, the presence of a pretibial fovea, and length of time the bandage has been worn (model 1, 2, 3 e 5, 6 e 7).
We also performed the same analysis on the percentage variation of the volume of the lower limbs in both groups (Model 4 and 8): with respect to the factors considered, we did not find any interference except for the time of wearing the bandage in the BEND+DIET group (Model 8, p 0.036)
4. Discussion
Currently, there is no widely shared consensus on the optimal therapeutic strategies for the management of lipedema, resulting in a substantial heterogeneity in the clinical approaches adopted across different healthcare settings. This variability contributes to a high degree of decision-making uncertainty among healthcare professionals and to a significant psychological burden in patients, who frequently report previous therapeutic experiences characterized by limited or absent efficacy. The lack of standardized therapeutic guidelines can be attributed to multiple factors, including the scarcity of high-quality clinical evidence, the fragmentation of available data in the literature, the variability of protocols adopted across specialized centers, and the marked phenotypic and clinic-functional heterogeneity of the population affected by lipedema.
This study was designed to evaluate the clinical efficacy of multilayer bandaging applied according to our intensive protocol, with materials, application methods, bandaging wear times, frequency, and duration of treatment chosen based on our years of clinical experience. The methods we have described to evaluate clinical and subjective outcomes are applied daily to assess the efficacy of the protocols and the various treatments that can be prescribed and applied to individual patients. The protocol we used in this study allowed us to achieve maximum results in the shortest possible time. Our primary goal is to reduce subjective symptoms, which are typically achieved after just a few bandaging sessions, but also, and above all, to reduce the pain caused by the tissue fold. This second aspect is more difficult to achieve; it requires more time and multiple application sessions and represents an aspect we believe to be more significant to evaluate the effectiveness of a treatment or the progression of the disease over time. We recommend evaluating this pain provoked sign together with the others subjective symptoms. Finally, the frequency and duration of the protocol were also calibrated to stabilize results in the medium to long term, reducing the number of patients who need, or depend, on cyclical treatments, which are often required but impact the disease management and the patients’ daily lives.
To this date, no studies have investigated the effectiveness of multilayer bandaging as a standalone therapeutic intervention in the treatment of lipedema. The available evidence comprises only four studies that evaluated bandaging within multimodal protocols, in combination with manual lymphatic drainage, skin care, and therapeutic exercise, or in association with intermittent compression therapy [21,22,48,49]. Furthermore, no studies have explored the effectiveness of bandaging combined with structured dietary interventions. Considering the growing relevance of a multidisciplinary approach in the management of lipedema, a second aim of the present study was to demonstrate that the use of bandaging combined with an anti-inflammatory diet was effective in reducing lower limb volume, subjective symptoms, and pressure-evoked pain.
Our study demonstrates the effectiveness of multilayer medium-stretch bandaging in reducing subjective symptoms, pressure-evoked pain, and lower limb volume, even when used as monotherapy; the outcome was observed in all three stages of lipedema, independently of BMI, age and the presence of fovea sign. As mentioned, the timing and frequency of bandaging are crucial: our protocol requires that the bandage be kept in place as long as possible between sessions and must allow movement, which is encouraged because it improves the effectiveness of the treatment on the tissue and must allow normal daily activities, particularly work, to be performed. In our experience, the longer it is kept in place, the greater the positive effects. This study was not aimed at evaluating the time required to keep the bandage on and in fact no relationship emerged between the duration and the effect on the parameters evaluated in the monotherapy group, while there would appear to be a positive relationship between the time the bandage was kept on and the % reduction in volume in the group also treated with the diet. But it should be emphasized that in this study, the average bandaging time applied to both lower limbs was over 24 hours, with a range, depending on patient tolerance, between 8 and 52 hours, for 5 weeks. Bandage retention tolerance is closely linked to the therapist’s ability to make the bandage as light and functional as possible, without excessive discomfort during movement and, above all, without causing pain.
Although the technique derives from the treatment of lymphedema, there are methodological differences primarily related to the different treatment objectives. Goals also include reducing tissue congestion, improving microvascular and lymphatic perfusion, and edema (if present), as in lymphedema [2,50,51,52], and indeed, treatment is indicated in these cases by the guidelines [2,3,4,5,6,7,8]. In this study, we demonstrated that clinical and subjective improvement is also achieved, and that the results are independent of the presence of signs of edema (pitting): this is a crucial aspect that suggests modifying the treatment indications.
In the case of lipedema, the application must be calibrated and sufficiently long-lasting to have an effect on the inflammatory and fibrotic degenerative phenomena present in the tissue, which are not rapidly reversible, and to have an effect on adipogenesis. Fascinating preclinical and clinical studies supporting this effect on tissue with compression are available and are increasing knowledge in this field. These studies also show that the method of applying the compressive force, which includes mechanical force, direction of the force, duration, and cyclicity of application, has an impact on the effect and must therefore be calibrated [10,11,12,13,14,15,16,17,18,52,53,54]. With these assumptions, we aimed to evaluate the effect of adding an anti-inflammatory diet. This study shows that the addition of the diet did not enhance the reduction of pain and subjective symptoms achieved by bandaging alone, as was also achieved with monotherapy. However, the diet resulted in a greater reduction in lower limb volume (from a 5% to a 9% reduction), body weight (0.6% vs. 4.4%, respectively), and waist and hip circumference (P < 0.001 for all) compared to bandaging alone. From a pathophysiological perspective, an anti-inflammatory diet, in addition to promoting weight reduction, can modulate the chronic low-grade inflammation characteristic of lipedema by reducing the activation of proinflammatory cytokines and improving adipose tissue function, for example by improving insulin sensitivity [28,29,30,31,32,55,56]. Regarding this last concept, in a precedent study, we demonstrated that using insulin sensitizing drugs, as exenatide, represents an efficient way to treat lipedema [46]. It is hypothesized that, in part, the reduction in both systemic and local inflammation may have also facilitated the mobilization of interstitial fluid and pathological fat deposits, amplifying the bandaging effect on limb volume. Volume reduction, coupled with pain relief, may significantly impact not only functional outcomes but also psychological well-being and quality of life. Furthermore, nutritional therapy, which is typically continued long-term in these patients, even after intensive treatment, could promote the maintenance and consolidation of the results achieved over time, also improving adherence to therapy. In addition, improvements in carbohydrate metabolism and insulin sensitivity may contribute to better metabolic control. In this context, dietary management should not be considered merely supportive, but rather a structural component of conservative lipedema treatment.
The results of the present study further support evidence for a multidisciplinary approach in the conservative management of lipedema, confirming the complementary role of both physical and nutritional interventions. In line with major consensus documents and international literature, our data suggest that the combination of targeted therapeutic strategies may produce superior clinical benefits compared to isolated interventions. Overall, these results contribute to addressing a gap in literature by providing preliminary evidence on the interaction between nutritional intervention and our intensive bandaging protocol in lipedema. Nevertheless, several methodological limitations should be acknowledged, including the relatively small sample size, lack of randomization, and limited follow-up duration.
Author Contributions
Conceptualization, methodology, supervision, visualization and writing—review and editing L.P. and L.R.; data curation, investigation, resources and visualization L.P., L.R., V.R., A.M. and G.O.; writing—original draft preparation L.P., L.R., V.R., A.M., G.O., N.C., A.B., L.C., D.R.B and G.P.P.; formal analysis, L.P., L.R. and N.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by Territorial Ethics Committee of the Autonomous Province of Trento for Clinical Trials (approval number: A909 of 06/07/2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CTD | Complex decongestive therapy |
| MLD | manual lymphatic drainage |
| MLB | multilayer bandaging |
| IL-6 | interleukin 6 |
| TNF-α | tumor necrosis factor-alpha |
| MCP-1 | monocyte chemoattractant protein 1 |
| PPARγ | peroxisome proliferator-activated receptor gamma |
| C/EBPα | CCAAT/enhancer-binding protein alpha |
| MRI | magnetic resonance imaging |
| BEND | Bandage-only treatment group |
| BEND+DIET | Bandage-plus-diet treatment group |
| CONTR | Untreated control group |
| BMI | Body mass index |
| PPC | Progressive Pain Check |
| RPS | Ricolfi-Patton Score |
| LBPS | Lower Body Pain Score |
| UBPS | Upper Body Pain Score |
References
- Patton, L; Ricolfi, L; Bortolon, M; et al. Observational Study on a Large Italian Population with Lipedema: Biochemical and Hormonal Profile, Anatomical and Clinical Evaluation, Self-Reported History. Int J Mol Sci. 2024, 25(3), 1599. [Google Scholar] [CrossRef]
- Herbst, KL; Kahn, LA; Iker, E; et al. Standard of care for lipedema in the United States. Phlebology 2021, 36(10), 779–796. [Google Scholar] [CrossRef] [PubMed]
- Halk, AB; Damstra, RJ. First Dutch guidelines on lipedema using the international classification of functioning, disability and health. Phlebology 2017, 32(3), 152–159. [Google Scholar] [CrossRef] [PubMed]
- Wounds, UK; Best. Practice Guidelines: The Management of Lipoedema. 2017. Available online: https://wounds-uk.com/bestpractice-statements/management-lipoedema/ (accessed on 28 August 2017).
- Alcolea, J.M.; Alonso, A.B.; Arroyo, B.A.; Domingo, P.; Garcia, G.A.; Graells, G.M.; Urraca, I.C.; Nipoti, I.E.; Castillo, M.E.; Alvarez, M., Jr.; et al. Consensus Document on Lipedema 2018. In cludes Current Status of Lipedema 2019; LITOGAMA SL: Barcelona, Spain, 2018. [Google Scholar]
- Bertsch, T; Erbacher, G; Elwell, R. Lipoedema: a paradigm shift and consensus. J Wound Care 2020, 29(Sup11b), 1–51. [Google Scholar] [CrossRef]
- Faerber, G; Cornely, M; Daubert, C; et al. S2k guideline lipedema. J Dtsch Dermatol Ges. 2024, 22(9), 1303–1315. [Google Scholar] [CrossRef] [PubMed]
- Amato, ACM; Peclat, APRM; Kikuchi, R; et al. Brazilian Consensus Statement on Lipedema using the Delphi methodology. J Vasc Bras. 2025, 24, e20230183. [Google Scholar] [CrossRef]
- O’Donnell, TF, Jr.; Allison, GM; Iafrati, MD. A systematic review of guidelines for lymphedema and the need for contemporary intersocietal guidelines for the management of lymphedema. J Vasc Surg Venous Lymphat Disord. 2020, 8(4), 676–684. [Google Scholar] [CrossRef]
- Li, G; Fu, N; Yang, X; et al. Mechanical compressive force inhibits adipogenesis of adipose stem cells. Cell Prolif. 2013, 46(5), 586–594. [Google Scholar] [CrossRef]
- Szolnoky, G; Nagy, N; Kovács, RK; et al. Complex decongestive physiotherapy decreases capillary fragility in lipedema. Lymphology 2008, 41(4), 161–166. [Google Scholar]
- Saitou, K; Tokunaga, M; Yoshino, D; et al. Local cyclical compression modulates macrophage function in situ and alleviates immobilization-induced muscle atrophy. Clin Sci (Lond) 2018, 132(19), 2147–2161. [Google Scholar] [CrossRef]
- Rabe, E; Partsch, H; Morrison, N; et al. Risks and contraindications of medical compression treatment - A critical reappraisal. An international consensus statement. Phlebology 2020, 35(7), 447–460. [Google Scholar] [CrossRef] [PubMed]
- Ligi, D; Croce, L; Mannello, F. Inflammation and compression: the state of art. Veins & Lymphatics 2016, 5(1). [Google Scholar] [CrossRef]
- Partsch, H. Assessing the effectiveness of multilayer inelastic bandaging. Journal of Lymphoedema 2007, 2(2), 55. [Google Scholar]
- Beidler, SK; Douillet, CD; Berndt, DF; Keagy, BA; Rich, PB; Marston, WA. Inflammatory cytokine levels in chronic venous insufficiency ulcer tissue before and after compression therapy. J Vasc Surg. 2009, 49(4), 1013–1020. [Google Scholar] [CrossRef]
- Murphy, MA; Joyce, WP; Condron, C; Bouchier-Hayes, D. A reduction in serum cytokine levels parallels healing of venous ulcers in patients undergoing compression therapy. Eur J Vasc Endovasc Surg. 2002, 23(4), 349–352. [Google Scholar] [CrossRef]
- Partsch, H. Compression therapy: clinical and experimental evidence. Ann Vasc Dis. 2012, 5(4), 416–422. [Google Scholar] [CrossRef]
- Hossain, G; Iwata, T; Mizusawa, N; Shima, SWN; Okutsu, T; Ishimoto, K; et al. Compressive force inhibits adipogenesis through COX-2-mediated down-regulation of PPAR-γ2 and C/EBP α. J. Biosci. Bioeng. 2010, 109, 297–303. [Google Scholar] [CrossRef]
- Wright, T; Scarfino, CD; O’Malley, EM. Effect of pneumatic compression device and stocking use on symptoms and quality of life in women with lipedema: A proof-in-principle randomized trial. Phlebology 2023, 38(1), 51–61. [Google Scholar] [CrossRef]
- Szolnoky, G; Varga, E; Varga, M; Tuczai, M; Dósa-Rácz, E; Kemény, L. Lymphedema treatment decreases pain intensity in lipedema. Lymphology 2011, 44(4), 178–182. [Google Scholar]
- Szolnoky, G; Borsos, B; Bársony, K; Balogh, M; Kemény, L. Complete decongestive physiotherapy with and without pneumatic compression for treatment of lipedema: a pilot study. Lymphology 2008, 41(1), 40–44. [Google Scholar]
- Ricolfi, L; Reverdito, V; Gabriele, G; et al. Micromassage Compression Leggings Associated with Physical Exercise: Pilot Study and Example of Evaluation of the Clinical and Instrumental Effectiveness of Conservative Treatment in Lipedema. Life (Basel) 2024, 14(7), 854. [Google Scholar] [CrossRef] [PubMed]
- Czerwińska, M; Gruszecki, M; Rumiński, J; Hansdorfer-Korzon, R. Evaluation of the Effectiveness of Compression Therapy Combined with Exercises Versus Exercises Only Among Lipedema Patients Using Various Outcome Measures. Life (Basel) 2024, 14(11), 1346. [Google Scholar] [CrossRef] [PubMed]
- Collier, M; Barbul, A; Campbell, RF; Filori, P; Haughey, L; Hazledine, M; Hellgren, M; Hopkins, A; Isoherranen, K; Lagus, H; Ryan, H; Moffatt, C. Chronic Oedema of the Lower Limb. Practical guidance on diagnosis, effective treatment and ongoing management. J Wound Management 2025, 26(3 Sup1), S1–S88. [Google Scholar] [CrossRef]
- Chakraborty, A; Crescenzi, R; Usman, TA; et al. Indications of Peripheral Pain, Dermal Hypersensitivity, and Neurogenic Inflammation in Patients with Lipedema. Int J Mol Sci. 2022, 23(18), 10313. [Google Scholar] [CrossRef]
- Kruppa, P; Georgiou, I; Biermann, N; Prantl, L; Klein-Weigel, P; Ghods, M. Lipedema-Pathogenesis, Diagnosis, and Treatment Options. Dtsch Arztebl Int. 2020, 117(22-23), 396–403. [Google Scholar] [CrossRef]
- de Oliveira, J; de Paula, ACP; Guimarães, VHD. Clinical or cultural? Dietary interventions for lipedema: a systematic review. Maturitas 2025, 202, 108716. [Google Scholar] [CrossRef]
- Atabilen Pınar, B; Çelik, MN; Altıntaş Başar, HB; Ağagündüz, D; Karaca, OB. Current Evidence-Based Clinical Nutritional Approaches in Lipedema: A Scoping Review. Nutr Rev 2025. [Google Scholar] [CrossRef]
- Aydin, A; Bilgic, P. Nutritional Approaches and Supplementation in Lipedema Management: A Narrative Review of Current Evidence. Curr Nutr Rep. Published. 2025, 14(1), 113. [Google Scholar] [CrossRef]
- Amato, ACM; Amato, JLS; Benitti, DA. The Efficacy of Ketogenic Diets (Low Carbohydrate; High Fat) as a Potential Nutritional Intervention for Lipedema: A Systematic Review and Meta-Analysis. Nutrients 2024, 16(19), 3276. [Google Scholar] [CrossRef]
- Tel Adıgüzel, K; Yaman, A; Kürklü, NS; Adıgüzel, E. Dietary Inflammatory Index and Mediterranean Diet Score are associated with systemic inflammation in women with lipedema. Int J Obes (Lond). 27 November 2025. [CrossRef]
- Jeziorek, M; Chachaj, A; Sowicz, M; et al. The Benefits of Low-Carbohydrate, High-Fat (LCHF) Diet on Body Composition, Leg Volume, and Pain in Women with Lipedema. J Obes. 2023, 2023, 5826630. [Google Scholar] [CrossRef]
- Di Renzo, L; Gualtieri, P; Zomparelli, S; et al. Modified Mediterranean-Ketogenic Diet and Carboxytherapy as Personalized Therapeutic Strategies in Lipedema: A Pilot Study. Nutrients 2023, 15(16), 3654. [Google Scholar] [CrossRef] [PubMed]
- Sørlie, V; De Soysa, AK; Hyldmo, ÅA; Retterstøl, K; Martins, C; Nymo, S. Effect of a ketogenic diet on pain and quality of life in patients with lipedema: The LIPODIET pilot study. Obes Sci Pract. 2022, 8(4), 483–493. [Google Scholar] [CrossRef] [PubMed]
- Jeziorek, M; Szuba, A; Kujawa, K; Regulska-Ilow, B. The Effect of a Low-Carbohydrate, High-Fat Diet versus Moderate-Carbohydrate and Fat Diet on Body Composition in Patients with Lipedema. Diabetes Metab Syndr Obes. 2022, 15, 2545–2561. [Google Scholar] [CrossRef]
- Jeziorek, M; Chachaj, A; Szuba, A; Różańska, D; Prescha, A. Exploring the Anti-Inflammatory Potential of a Mediterranean-Style Ketogenic Diet in Women with Lipedema. Nutrients 2025, 17(18), 3014. [Google Scholar] [CrossRef] [PubMed]
- Lundanes, J; Sandnes, F; Gjeilo, KH; et al. Effect of a low-carbohydrate diet on pain and quality of life in female patients with lipedema: a randomized controlled trial. Obesity (Silver Spring) 2024, 32(6), 1071–1082. [Google Scholar] [CrossRef]
- Lundanes, J; Gårseth, M; Taylor, S; et al. The effect of a low-carbohydrate diet on subcutaneous adipose tissue in females with lipedema. Front Nutr. 2024, 11, 1484612. [Google Scholar] [CrossRef]
- Di Renzo, L; Cinelli, G; Romano, L; et al. Potential Effects of a Modified Mediterranean Diet on Body Composition in Lipoedema. Nutrients Published. 2021, 13(2), 358. [Google Scholar] [CrossRef]
- Fedre, B; Dessalvi, S; Boccardo, F. A Case Series on Combining Modified Mediterranean Diet and Ketogenic Diet in a “Sandwich” Approach for Patients with Lipedema and Comorbidities. Lymphology 2025, 58(3), 108–118. [Google Scholar] [CrossRef]
- Tsigalou, C; Konstantinidis, T; Paraschaki, A; Stavropoulou, E; Voidarou, C; Bezirtzoglou, E. Mediterranean Diet as a Tool to Combat Inflammation and Chronic Diseases. An Overview. Biomedicines 2020, 8(7), 201. [Google Scholar] [CrossRef]
- Bruna-Mejias, A; San Martin, J; Arciniegas-Diaz, D; et al. Comparison of the Mediterranean Diet and Other Therapeutic Strategies in Metabolic Syndrome: A Systematic Review and Meta-Analysis. Int J Mol Sci. 2025, 26(12), 5887. [Google Scholar] [CrossRef]
- Ferraris, C; Guglielmetti, M; Neri, LCL; et al. A Review of Ketogenic Dietary Therapies for Epilepsy and Neurological Diseases: A Proposal to Implement an Adapted Model to Include Healthy Mediterranean Products. Foods 2023, 12(9), 1743. [Google Scholar] [CrossRef] [PubMed]
- Bailey, MA; Holscher, HD. Microbiome-Mediated Effects of the Mediterranean Diet on Inflammation. Adv Nutr. 2018, 9(3), 193–206. [Google Scholar] [CrossRef] [PubMed]
- Patton, L; Reverdito, V; Bellucci, A; Bortolon, M; Macrelli, A; Ricolfi, L. A Case Series on the Efficacy of the Pharmacological Treatment of Lipedema: The Italian Experience with Exenatide. Clin Pract. 2025, 15(7), 128. [Google Scholar] [CrossRef] [PubMed]
- Kuhnke, E. Volumbestimmung aus Umfangmessungen. Folia Angiologica 1976, 24, 228–232. [Google Scholar]
- Atan, T; Bahar-Özdemir, Y. The Effects of Complete Decongestive Therapy or Intermittent Pneumatic Compression Therapy or Exercise Only in the Treatment of Severe Lipedema: A Randomized Controlled Trial. Lymphat Res Biol. 2021, 19(1), 86–95. [Google Scholar] [CrossRef]
- Esmer, M; Schingale, FJ. Effect of Physical Therapy on Circumference Measurement and Extremity Volume in Patients Suffering from Lipedema with Secondary Lymphedema. Lymphat Res Biol. 2024, 22(1), 8–11. [Google Scholar] [CrossRef]
- Földi, E. Therapie des Lymphödems [Therapy of lymphedema]. Hautarzt 2012, 63(8), 627–633. [Google Scholar] [CrossRef]
- Partsch, H; Mortimer, P. Compression for leg wounds. Br J Dermatol 2015, 173(2), 359–369. [Google Scholar] [CrossRef]
- Al-Ghadban, S; Cromer, W; Allen, M; et al. Dilated Blood and Lymphatic Microvessels, Angiogenesis, Increased Macrophages, and Adipocyte Hypertrophy in Lipedema Thigh Skin and Fat Tissue. J Obes. 2019, 2019, 8747461. [Google Scholar] [CrossRef]
- Trayhurn, P; Wood, IS. Adipokines: inflammation and the pleiotropic role of white adipose tissue. Br J Nutr. 2004, 92(3), 347–355. [Google Scholar] [CrossRef]
- Eidler, SK; Douillet, CD; Berndt, DF; et al. Compression Therapy in the Management of Cellulitis: A Comparative Study. The Journal of Surgery 2018, 6, 68. Available online: https://api.semanticscholar.org/CorpusID:55884619.
- Pasquali, R; Vicennati, V; Gambineri, A; Pagotto, U. Hormones and pathophysiology of obesity. Eat Weight Disord. 2001, 6((3) Suppl 3, 9–20. [Google Scholar]
- Repaci, A; Gambineri, A; Pasquali, R. The role of low-grade inflammation in the polycystic ovary syndrome. Mol Cell Endocrinol. 2011, 335(1), 30–41. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The figure shows 3 types of multilayer bandages used for the treatment of lipedema: with inclusion of foot and abdomen (a), with free foot and inclusion of abdomen (b), bandage that includes the lower limb from ankle to thigh (c).
Figure 1.
The figure shows 3 types of multilayer bandages used for the treatment of lipedema: with inclusion of foot and abdomen (a), with free foot and inclusion of abdomen (b), bandage that includes the lower limb from ankle to thigh (c).
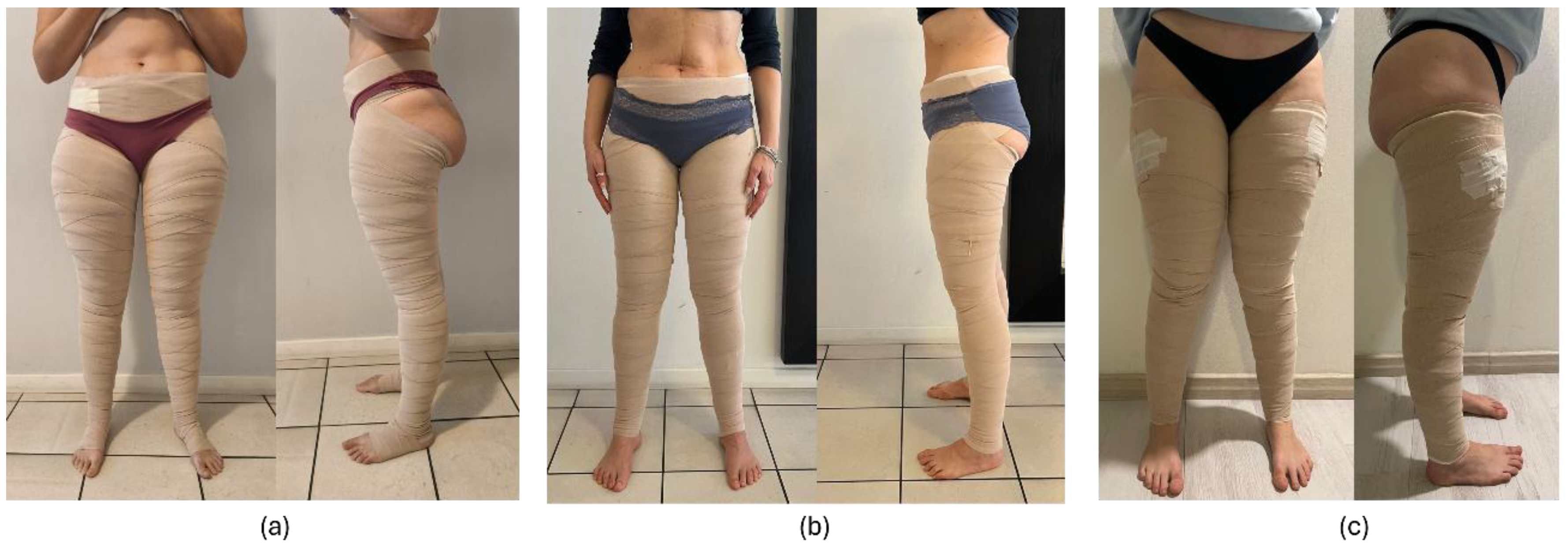
Figure 2.
Multilayer short-stretch compression bandaging of the lower limbs in lipedema, performed by an experienced therapist according to our previously published protocol. The technique includes selective foot sparing, calibrated padding, graduated pressure distribution, and anatomical shaping of thigh and hip regions, while deliberately preserving knee and ankle mobility. Proper application requires advanced manual skills to ensure effective tissue containment without restricting functional movement, allowing immediate ambulation and active exercise as part of integrated conservative management.
Figure 2.
Multilayer short-stretch compression bandaging of the lower limbs in lipedema, performed by an experienced therapist according to our previously published protocol. The technique includes selective foot sparing, calibrated padding, graduated pressure distribution, and anatomical shaping of thigh and hip regions, while deliberately preserving knee and ankle mobility. Proper application requires advanced manual skills to ensure effective tissue containment without restricting functional movement, allowing immediate ambulation and active exercise as part of integrated conservative management.

Figure 3.
Functional multilayer short-stretch compression bandaging allowing active squat and lunge movements, demonstrating preserved hip and knee mobility. The images highlight how effective tissue containment is maintained during dynamic tasks, supporting immediate ambulation and exercise. Preserved movement is an essential component to enhance bandaging efficacy by promoting muscle pump activation and optimizing compression–motion interaction.
Figure 3.
Functional multilayer short-stretch compression bandaging allowing active squat and lunge movements, demonstrating preserved hip and knee mobility. The images highlight how effective tissue containment is maintained during dynamic tasks, supporting immediate ambulation and exercise. Preserved movement is an essential component to enhance bandaging efficacy by promoting muscle pump activation and optimizing compression–motion interaction.


Table 1.
The table shows the anthropometric and clinical data before starting the treatment in the entire population (ALL) and in the population divided into the three groups: patients treated with bandages (BEND), patients treated with bandages and diet (BEND+DIET) and the control group (CONTR). P values refer to the comparison between BEND and BEND+DIET (P value TREAT) and the comparison of all three groups (P value ALL). All tests were two-sided, with a significance level set at p < 0.05.
Table 1.
The table shows the anthropometric and clinical data before starting the treatment in the entire population (ALL) and in the population divided into the three groups: patients treated with bandages (BEND), patients treated with bandages and diet (BEND+DIET) and the control group (CONTR). P values refer to the comparison between BEND and BEND+DIET (P value TREAT) and the comparison of all three groups (P value ALL). All tests were two-sided, with a significance level set at p < 0.05.
| Variable | ALL (114) |
BEND (35) |
BEND+DIET (48) |
CONTR (31) |
P value ALL |
P value TREAT |
|---|---|---|---|---|---|---|
| Age (yrs) - mean (sd) | 43.2 (11.1) | 41.2 (10.3) | 45.2 (12.9) | 42.6 (8.65) | 0.261 | 0.125 |
| Body weight (kg) - mean (sd) | 79.6 (18.5) | 79.6 (19.7) | 81.5 (17.8) | 76.5 (18.3) | 0.376‡ | 0.546† |
| Body mass index (kg/m2) - mean (sd) | 30.0 (6.43) | 30.2 (6.62) | 30.5 (6.54) | 29.0 (6.2) | 0.573 | 0.830 |
| Waist circumference (cm) - mean (sd) | 91.7 (14.6) | 89.7 (13.2) | 92.7 (16.5) | 92.5 (13.1) | 0.617 | 0.358 |
| Hip circumference (cm) - mean (sd) | 116 (12.9) | 116 (13.0) | 116 (13.4) | 114 (12.2) | 0.796 | 0.978 |
| Waist-to-hip ratio - mean (sd) | 0.79 (0.84) | 0.07 (0.01) | 0.79 (0.09) | 0.81 (0.08) | 0.214 | 0.341 |
| Pretibial fovea – n (%) | 34 (33.0) | 11 (36.7) | 16 (35.6) | 7 (25.0) | 0.992 | |
| Telangiectasias – n (%) | 81 (81.8) | 21 (77.8) | 35 (79.5) | 25 (89.3) | 0.438 | 0.859 |
| Distribution of clinical stages | 0.233 | 0.532 | ||||
| Stage 1 – n (%) | 39 (34.2) | 11 (31.4) | 13 (27.1) | 15 (48.8) | ||
| Stage 2 – n (%) | 48 (42.1) | 14 (40.0) | 25 (52.1) | 9 (29.0) | ||
| Stage 3 – n (%) | 27 (23.7 | 10 (28.6) | 10 (20.8) | 7 (22.6) | ||
| Upper limbs involvement - n (%) | 97 (85.1) | 30 (85.7) | 38 (79.2) | 29 (93.0) | 0.234* | 0.634 |
| Lower limb volume – average (mL) - mean (sd) | - | 15538 (4429) | 15841 (3982) | 0.750 | ||
| Lower limb volume - right (mL) - mean (sd) | - | 15532 (4361) | 15945 (4120) | 0.664 | ||
| Lower limb volume – left (mL) - mean (sd) | - | 15545 (4517) | 15736 (3923) | 0.723† | ||
| Total Body Pain Score - mean (sd) | 31.6 (6.30) | 31.2 (6.85) | 30.8 (6.75) | 33.3 (4.59) | 0.320‡ | 0.705† |
| Lower Body Pain Score - mean (sd) | 26.7 (4.56) | 26.1 (4.55) | 26.3 (5.35) | 28.0 (2.77 | 0.195‡ | 0.584† |
| Upper Body Pain Score - mean (sd) | 4.87 (2.81) | 5.11 (3.17) | 4.44 (2.81) | 5.26 (2.37) | 0.445‡ | 0.352† |
| Total Symptoms score – mean (sd) | 43.7 (13.7) | 45.2 (12.8) | 40.6 (13.7) | 46.6 (14.2) | 0.115 | 0.117 |
| Time of use of garments (hours) - mean (sd) | 24.7 (11.5) | 22.3 (9.02) | 26.5 (12.8) | - | 0.177† |
† Wilcoxon rank-sum test used for comparisons between treatment groups. ‡ Kruskal–Wallis test used for overall comparisons among groups. * Fisher test used for overall comparisons among groups.
Table 2.
The table shows data before (T0), after treatment (T1) and the variation obtained with the treatment (Delta) in patients treated with bandages (BEND) and patients treated with bandages and diet (BEND+DIET). The data are expressed with mean (standard deviation). P values refer to the comparison of T0-T1 in each group (P T0-T1) and to the comparison of the variation between the two groups (p DELTA). All tests were two-sided, with a significance level set at p < 0.05.
Table 2.
The table shows data before (T0), after treatment (T1) and the variation obtained with the treatment (Delta) in patients treated with bandages (BEND) and patients treated with bandages and diet (BEND+DIET). The data are expressed with mean (standard deviation). P values refer to the comparison of T0-T1 in each group (P T0-T1) and to the comparison of the variation between the two groups (p DELTA). All tests were two-sided, with a significance level set at p < 0.05.
| BEND | BEND+DIET | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | T0 | T1 | delta | P T0-T1 |
T0 | T1 | delta | P T0-T1 |
P DELTA |
| Body weight (kg) | 79,63 (19.65) | 79.1 (19.4) | -0.50 (1.09) | 0.011 | 81,48 (17.81) | 78.0 (17.7) | -3.45 (1.84) | <0.001 | <0.001 |
| Body weight loss (%) | 0.590 (1.34) | 4.38 (2.56) | <0.001 | ||||||
| Waist circumference (cm) | 88.8 (13.3) | 87.4 (13.0) | 1.37 (2.51) | <0.001† | 90.1 (14.3) | 87.7 (13.9) | 3.86 (3.27) | <0.001† | <0.001† |
| Hip circumference (cm) | 116 (14.1) | 114 (14.4) | 2.04 (2.30) | <0.001† | 115 (12.9) | 112 (12.3) | 3.78 (2.49) | <0.001† | <0.001† |
| Lower limbs volume – average (mL) | 15538 (4429) | 14807 (4360) | 732 (242) | <0.001 | 15841 (3982) | 14418 (3644) | 1423 (662) | <0.001† | <0.001† |
| Volume reduction in the lower limbs – average (%) | 4.96 (1.84) | 9.02 (3.21) | <0.001 | ||||||
| Lower limb volume - right (mL) | 15532 (4361) | 14847 (4316) | 685 (321) | <0.001 | 15945 (4120) | 14498 (3789) | 1447 (650) | <0.001† | <0.001† |
| Lower limb volume – left (mL) | 15545 (4517) | 14847 (4316) | 698 (701) | <0.001 | 15736 (3223) | 14498 (3789) | 1239 (1322) | <0.001† | <0.001 |
| Total Body Pain Score or RPS | 31.2 (6.85) | 14.1 (8.63) | 17.1 (6.88) | <0.001 | 30.8 (6.75) | 13.3 (7.98) | 14.4 (7.99) | <0.001 | NS |
| Lower Body Pain Score | 26.1 (4.56) | 10.3 (6.91) | 15.8 (6.61) | <0.001 | 26.3 (5.35) | 10.1 (6.24) | 16.2 (678) | <0.001 | NS |
| Upper Body Pain Score | 5.11 (3.17) | 3.83 (3.01) | 1.29 (2.02) | <0.001† | 4.44 (2.81) | 3.21 (2.98) | 1.23 (2.40) | <0.001† | NS |
| Total Symptoms score | 44.3 (12.8) | 16.7 (11.7) | 28.5 (10.9) | <0.001 | 40.6 (13.7) | 17.8 (11.7) | 25.9 (10.2) | <0.001 | NS |
NS: Non-Significant; RPS: Ricolfi-Patton Score; † Wilcoxon rank-sum test used for comparisons between treatment groups.
Table 3.
The table shows the initial (T0) and post-treatment (T1) values of pain scores detected by fat folds at various body sites in patients treated with bandages (BEND), patients treated with bandages and diet (BEND+DIET), and the control group (CONTR), as well as the P value for the comparison between T0 and T1 (P T0-T1). The p-value to compare the variation between the two treatment groups (P DELTA TREAT) and between the control group and the bandage-treated group (P DELTA CB), and between the control group and the bandage-treated group plus diet (P DELTA CBD) is also reported. The data are expressed as median and interquartile range (IQR). All tests were two-sided, with a significance level set at p < 0.05.
Table 3.
The table shows the initial (T0) and post-treatment (T1) values of pain scores detected by fat folds at various body sites in patients treated with bandages (BEND), patients treated with bandages and diet (BEND+DIET), and the control group (CONTR), as well as the P value for the comparison between T0 and T1 (P T0-T1). The p-value to compare the variation between the two treatment groups (P DELTA TREAT) and between the control group and the bandage-treated group (P DELTA CB), and between the control group and the bandage-treated group plus diet (P DELTA CBD) is also reported. The data are expressed as median and interquartile range (IQR). All tests were two-sided, with a significance level set at p < 0.05.
| BEND | BEND+DIET | CONTR | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| pain assessment site | T0 | T1 | P t0-t1 | T0 | T1 | P t0-t1 | T0 | T1 | P t0-t1 | P DELTA TREAT | P DELTA CB | P DELTA CBD |
| Medial lower third of the leg Mediana(IQR) |
4(1) | 1(2) | <0.001† | 4(0) | 1(1) | <0.001† | 4(0) | 4(0) | NS† | NS† | <0.001† | <0.001† |
| Middle third of the back of the leg Mediana(IQR) |
4(1) | 1(1.5) | <0.001† | 4(0) | 1(1) | <0.001† | 4(0) | 4(0) | NS† | NS† | <0.001† | <0.001† |
| Medial upper third of the leg Mediana(IQR) |
4(0) | 1(1) | <0.001† | 4(0) | 2(1) | <0.001† | 4(0) | 4(0) | NS† | NS† | <0.001† | <0.001† |
| Lateral upper third of the thigh Mediana(IQR) |
3(2) | 1(1) | <0.001† | 4(2) | 1(2) | <0.001† | 4(1) | 4(1) | NS† | NS† | <0.001† | <0.001† |
| later lower third of the thigh Mediana(IQR) |
4(1) | 1(2) | <0.001† | 4(1) | 1(2) | <0.001† | 4(1) | 4(1) | NS† | NS† | <0.001† | <0.001† |
| Medial upper third of the thigh Mediana(IQR) |
4(1) | 1(2) | <0.001† | 4(1) | 1(1) | <0.001† | 4(0) | 4(0) | NS† | NS† | <0.001† | <0.001† |
| Medial lower third of the thigh Mediana(IQR) |
4(1) | 2(1.5) | <0.001† | 4(1) | 1(1) | <0.001† | 4(0) | 4(0) | NS† | NS† | <0.001† | <0.001† |
| Lower abdomen Mediana(IQR) |
2(3) | 1(2) | <0.001† | 2(1.25) | 0(1) | <0.001† | 2(3) | 2(3) | NS† | NS† | <0.001† | <0.001† |
| Lateral edge of the tissue covering the teres major muscle Mediana(IQR) |
2(2.5) | 1(2) | <0.001† | 2(2) | 1(2) | <0.001† | 2(2) | 2(2) | NS† | NS† | <0.001† | 0.005† |
| Arm Mediana(IQR) |
3(2) | 2(2) | <0.001† | 3(2) | 2(2) | <0.001† | 3(2) | 3(2) | NS† | NS† | <0.001† | <0.001† |
| Forearm Mediana(IQR) |
0(0.5) | 0(1) | NS† | 0(0) | 0(0) | NS † | 0(0) | 0(0) | NS† | NS† | NS† | NS† |
| Total Body Pain Score or RPS | 32(10) | 13(14) | <0.001 | 31(8) | 12.5(10.75) | 12.5(10.75) | 34(7) | 34(7) | NS† | NS | <0.001† | <0.001† |
| Lower Body Pain Score | 27(7) | 9(12) | <0.001 | 28(3) | 10(9.5) | 10(9.25) | 28(6) | 28(6) | NS† | NS | <0.001† | <0.001† |
| Upper Body Pain Score | 6(4) | 4(5) | <0.001† | 4.5(4.75) | 2(3.75) | 2(3.75) | 5(3) | 5(3) | NS† | NS† | <0.001† | 0.001† |
NS: Non-Significant; RPS: RPS: Ricolfi-Patton Pain Lipedema Score; † Wilcoxon rank-sum test used.
Table 4.
The table shows the initial (T0) and post-treatment (T1) values of the scores of the items of the lipedema symptom questionnaire in the 3 groups: patients treated with bandages (BEND), patients treated with bandages and diet (BEND+DIET) and control group (CONTR). The data are expressed as median and interquartile range (IQR). P values refer to the comparison of values recorded before (T0) and after treatment (PT0-T1) in each group. The p-value to compare the change between the two treatment groups (P DELTA TREAT) and between the control group and the bandage-treated group (P DELTA CB), and between the control group and the bandage-treated group plus diet (P DELTA CBD) is also reported. All tests were two-sided, with a significance level set at p < 0.05.
Table 4.
The table shows the initial (T0) and post-treatment (T1) values of the scores of the items of the lipedema symptom questionnaire in the 3 groups: patients treated with bandages (BEND), patients treated with bandages and diet (BEND+DIET) and control group (CONTR). The data are expressed as median and interquartile range (IQR). P values refer to the comparison of values recorded before (T0) and after treatment (PT0-T1) in each group. The p-value to compare the change between the two treatment groups (P DELTA TREAT) and between the control group and the bandage-treated group (P DELTA CB), and between the control group and the bandage-treated group plus diet (P DELTA CBD) is also reported. All tests were two-sided, with a significance level set at p < 0.05.
| BEND | BEND+DIET | CONTR | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Item | T0 | T1 | P T0-T1 |
T0 | T1 | P T0-T1 |
T0 | T1 | P T0-T1 |
P DELTA TREAT |
P DELTA CB | P DELTA CBD |
| Spontaneous pain in the lower limbs | 4(1) | 1(2) | <0.001† | 3(2) | 1(2) | <0.001† | 3(2) | 3(2) | NS† | NS† | 0.001† | <0.001† |
| Feeling of swelling in the lower limbs | 3(1) | 1(1) | <0.001† | 3(1) | 1(1) | <0.001† | 3(1) | 3(1) | NS† | NS† | <0.001† | <0.001† |
| feeling of heaviness in the lower limbs | 4(1) | 1(1) | <0.001† | 4(1) | 1(1) | <0.001† | 4(1) | 4(1) | NS† | NS† | <0.001† | <0.001† |
| Sensation of swelling in the ankles | 2(3) | 0(1) | <0.001† | 3(3) | 0(1) | <0.001† | 3(2) | 3(2) | NS† | NS† | <0.001† | <0.001† |
| Sensation of swelling in the foot (back and toes) | 0(0) | 0(0) | 0.013† | 0(2) | 0(0) | <0.001† | 1(3) | 1(3) | NS† | NS† | 0.005† | 0.003† |
| Sensation of swelling elsewhere (on the hands, around the eyes) | 0(1) | 0(0) | 0.040† | 0(1) | 0(0) | 0.006† | 2(3) | 2(3) | NS† | NS† | 0.036† | 0.013† |
| Skin cold to the touch on the lower limbs | 3(2) | 1(1.5) | <0.001† | 2(4) | 0.5(1.25) | <0.001† | 3(2) | 3(2) | NS† | NS† | <0.001† | <0.001† |
| Hypersensitivity to touch in the lower limbs | 3(2.5) | 1(1.5) | <0.001† | 2(4) | 0(1.25) | <0.001† | 3(2) | 3(2) | NS† | NS† | <0.001† | <0.001† |
| Pressure pain in the lower limbs | 4(1) | 2(1) | <0.001† | 4(1) | 1(2) | <0.001† | 4(1) | 4(1) | NS† | NS† | <0.001† | <0.001† |
| Paresthesia and tingling in the lower limbs | 1(2) | 0(0.5) | 0.003† | 0.5(2) | 0(0) | <0.001† | 1(3) | 1(3) | NS† | NS† | <0.001† | 0.002† |
| Burning sensation in the lower limbs | 1(2) | 0(1) | 0.008† | 0(1) | 0(0) | 0.003† | 1(2) | 1(2) | NS† | NS† | 0.015† | 0.005† |
| Easy bruising | 3(2.5) | 1(2) | <0.001† | 3(2.25) | 1(2) | <0.001† | 3(2) | 3(2) | NS† | NS† | <0.001† | <0.001† |
| Fatigue in the lower limbs when doing movement or physical activity | 3.63(1.5) | 1.54(1.27) | <0.001 | 3.19(1.57) | 1.38(1.2) | <0.001 | 4(1) | 3(1) | NS† | NS | <0.001† | <0.001† |
| Pain in the lower limbs during or after movement/physical activity | 4(1) | 1(2) | <0.001† | 3(2) | 1(1.25) | <0.001† | 3(2) | 3(1) | NS† | NS† | <0.001† | <0.001† |
| Swelling or discomfort in the lower limbs following physical activity | 3(2) | 1(2) | <0.001† | 2(3) | 0(1) | <0.001† | 3(2) | 3(2) | NS† | NS† | <0.001† | <0.001† |
| Pain in the lower limbs when standing for a long time | 4(1) | 1(2) | <0.001† | 3(2.25) | 1(2.25) | <0.001† | 3(1) | 3(1) | NS† | NS† | <0.001† | <0.001† |
| Swelling/discomfort in the lower limbs when standing for a long time | 4(1) | 1(2) | <0.001† | 3(2) | 1(2) | <0.001† | 4(1) | 3(1) | NS† | NS† | <0.001† | <0.001† |
| Total Symptom Score | 44(18) | 16(17) | <0.001 | 40.5(16) | 10.5(16) | <0.001 | 44(22) | 45(20) | NS† | NS | <0.001† | <0.001† |
† Wilcoxon rank-sum test used for comparisons between treatment groups.
Table 5.
Multivariate regression analysis in the BEND group. The table shows the results of 4 distinct multivariate linear regression models in which the dependent variable measured after 4 weeks of treatment (T1) in model 1 is the Lower Body Pain Score, in model 2 Total Symptom Score, in model 3 the average volume of the lower limbs, and in the model 4 the percentage change in the mean volume of the lower limbs. For each model the set of independent variables is the same (age, BMI, clinical stage, bandage wearing time, and presence of pretibial fovea) and furthermore for each model the same dependent variable measured at time 0, before treatment, was added. The analysis was performed in the group of patients treated with bandaging (BEND).
Table 5.
Multivariate regression analysis in the BEND group. The table shows the results of 4 distinct multivariate linear regression models in which the dependent variable measured after 4 weeks of treatment (T1) in model 1 is the Lower Body Pain Score, in model 2 Total Symptom Score, in model 3 the average volume of the lower limbs, and in the model 4 the percentage change in the mean volume of the lower limbs. For each model the set of independent variables is the same (age, BMI, clinical stage, bandage wearing time, and presence of pretibial fovea) and furthermore for each model the same dependent variable measured at time 0, before treatment, was added. The analysis was performed in the group of patients treated with bandaging (BEND).
| DEPENDENT VARIABLE: | Lower Body Pain Score T1 Model 1 |
Total Symptom Score T1 Model 2 |
volume of the lower limbs T1 Model 3 |
% change in lower limb volume. Model 4 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coefficient | [95% conf. interval] | P VALUE | Coefficient | [95% conf. interval] | P VALUE | Coefficient | [95% conf. interval] | P VALUE | Coefficient | [95% conf. interval] | P VALUE | |
| Dependent variable T0 | 0.3422 | [ -0.311, 0.996] | 0.289 | 0.5348 | [0.224, 0.845] |
0.0017 | 0.97850 | [0.914 , 1.043] |
<0.001 | -0.0001 | [-0.001, 0.000] | 0.583 |
| Age | 0.1387 | [ -0.131, 0.408] |
0.297 | 0.1952 | [-0.205, 0.595] |
0.3222 | -3.36479 | [-14.333 , 7.603] |
0.531 | 0.0223 |
[-0.054, 0.0999] |
0.553 |
| BMI | -0.2420 | [-0.876 , 0.392] | 0.437 | 0.2990 | [-0.666, 1.264] | 0.5272 | -7.69172 | [ -49.612, 34.229] |
0.707 | 0.0006 |
[-0.293, 0.294] |
0.997 |
| Stage 2 | 2.6319 | [-4.367, 9.631] |
0.444 | 4.4791 | [-5.266, 14.225] | 0.3509 | -17.09741 | [-275.288, 241.093] | 0.892 | -0.1452 |
[-1.951, 1.660] |
0.869 |
| Stage 3 | 7.2967 | [-3.426, 18.019] | 0.172 | -1.9058 | [-18.475, 14.663] |
0.8137 | 121.33824 | [-344.057, 586.733] | 0.594 | -0.6534 |
[-3.908, 2.601] |
0.681 |
| Bandage wearing time | -0.1650 | [-0.480, 0.150] |
0.290 | 0.1809 | [-0.271, 0.632] | 0.4152 | 0.97684 | [ -11.705 , 13.659] |
0.875 | 0.0007 | [-0.088, 0.089] | 0.987 |
| Pretibial fovea | -1.6227 | [-8.220, 4.975] |
0.615 | -0.6552 | [-10.49, 9.187] | 0.8914 | 118.74814 | [-155.659 , 393.155] | 0.379 | -0.8380 | [-2.757, 1.081] |
0.375 |
BMI: Body Mass Index.
Table 6.
Multivariate regression analysis in the BEND+DIET group. The table shows the results of 4 distinct multivariate linear regression models in which the dependent variable measured after 4 weeks of treatment (T1) in model 1 is the Lower Body Pain Score, in model 2 Total Symptom Score, in model 3 the average volume of the lower limbs, and in the model 4 the percentage change in the mean volume of the lower limbs. For each model the set of independent variables is the same (age, BMI, clinical stage, bandage wearing time, and presence of pretibial fovea) and furthermore for each model the same dependent variable measured at time 0, before treatment, was added. The analysis was performed in the group of patients treated with bandaging and diet (BEND+DIET).
Table 6.
Multivariate regression analysis in the BEND+DIET group. The table shows the results of 4 distinct multivariate linear regression models in which the dependent variable measured after 4 weeks of treatment (T1) in model 1 is the Lower Body Pain Score, in model 2 Total Symptom Score, in model 3 the average volume of the lower limbs, and in the model 4 the percentage change in the mean volume of the lower limbs. For each model the set of independent variables is the same (age, BMI, clinical stage, bandage wearing time, and presence of pretibial fovea) and furthermore for each model the same dependent variable measured at time 0, before treatment, was added. The analysis was performed in the group of patients treated with bandaging and diet (BEND+DIET).
| DEPENDENT VARIABLE: | Lower Body Pain Score T1 Model 5 |
Total Symptom Score T1 Model 6 |
volume of the lower limbs T1 Model 7 |
% change in lower limb volume. Model 8 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coefficient | [95% conf. interval] | P VALUE | Coefficient | [95% conf. interval] | P VALUE | Coefficient | [95% conf. interval] | P VALUE | Coefficient | [95% conf. interval] | P VALUE | |
| Dependent variable T0 | 0.25593 | [-0.170, 0.682] |
0.231 | 0.62701 | [0.411, 0.843] |
<0.001 | 0.89824 | [ 0.793, 1.004] |
<0.001 | 0.0000 | [-0.001, 0.001] | 0.945 |
| Age | 0.04621 | [-0.108, 0.201] |
0.548 | -0.15138 | [-0.367, 0.065] |
0.164 | -0.90579 | [ -16.069, 14.257] |
0.904 | -0.0019 |
[-0.090, 0.086 |
0.966 |
| BMI | 0.31379 | [ -0.064,. 691] |
0.101 | 0.17045 | [-0.366, 0.707] | 0.524 | -5.65610 | [-60.934, 49.622] |
0.837 | 0.0334 | [-0.288, 0.355] | 0.835 |
| Stage 2 | -1.69530 | [-6.650, 3.260] |
0.492 | -2.07086 | [-9.374, 5.232] | 0.569 | -42.96491 | [-526.747, 440.817] | 0.858 | 0.9193 | [-1.897, 3.735] | 0.512 |
| Stage 3 | -0.54301 | [-7.065, 5.979] |
0.867 | 1.73793 | [-8.082, 11.557] | 0.722 | -200.14047 | [-894.567, 494.286] | 0.563 | 1.5080 | [-2.534, 5.550] | 0.454 |
| Time of use of garments | -0.02747 | [ -0.190, 0.135] |
0.734 | 0.01468 | [-0.210 , 0.240] | 0.895 | -11.55433 | [-26.515, 3.406] |
0.126 | 0.0919 |
[0.005, 0.179] |
0.036 |
| Pretibial fovea | -0.30457 | [ -4.731, 4.122] |
0.890 | -0.45878 | [-6.583, 5.665] | 0.880 | 174.29107 | [-245.813, 594.395] |
0.406 | -0.4766 | [-2.299, 1.969] | 0.700 |
BMI: Body Mass Index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



