Submitted:
14 February 2026
Posted:
26 February 2026
You are already at the latest version
Abstract
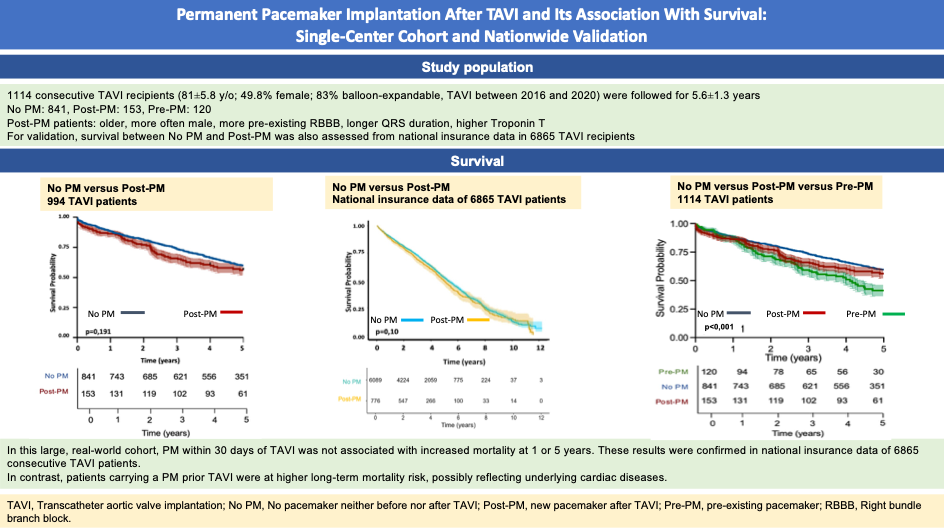
Background: Permanent pacemaker (PM) implantation is a well-recognized complication of transcatheter aortic valve implantation (TAVI), but its long-term prognostic impact remains uncertain. Objective: To evaluate the association between PM implantation and all-cause mortality in TAVI recipients.Methods: We performed a post-hoc analysis of a prospective single-center TAVI registry (2016–2020). The primary endpoint was all-cause mortality at 1 and 5 years. Cox regression and Kaplan–Meier analyses were applied. Validation using the nationwide AUTHEARTVISIT claims database was performed.Results: Among 1114 consecutive TAVI patients (mean age 81 ± 5.8 years; 49.8% female), 120 (10.8%) had a pre-existing PM (Pre-PM), and 153 (13.7%) received a new PM within 30 days post-TAVI (Post-PM). Post-PM patients were older (p=0.006), more often male (p<0.001), had higher Troponin T levels (p=0.002), more pre-existing right bundle branch block (p<0.001) and longer QRS duration (p<0.001) compared to patients without PM. On multivariate analysis, one-year mortality was associated with Troponin T (p=0.002) and NT-proBNP (p=0.002) serum levels. Pre-and Post-PM status was not associated with 1-year mortality (p=0.455, p=975). However, Pre-PM was independently associated with 5-year mortality (HR 1.4, 95% CI: 1.0–1.9, p=0.03), whereas Post-PM was not (HR 1.2, 95% CI: 0.8–1.6, p=0.22). Findings were confirmed in the nationwide AUTHEARTVISIT cohort. Conclusion: In this large, real-world TAVI cohort with national validation, Post-PM status was not associated with mortality at 1 or 5 years. In contrast, Pre-PM identified patients at higher long-term risk, possibly reflecting underlying cardiac disease.
Keywords:
aortic stenosis
; transcatheter aortic valve implantation
; pacemaker
; mortality
Introduction
Transcatheter aortic valve implantation (TAVI) has become an established treatment for patients with severe aortic stenosis across the entire risk spectrum. Initially reserved for inoperable or high-risk patients, TAVI is now frequently performed in intermediate- and low-risk individuals, with a continuously rising number of procedures worldwide [1]. As procedural safety has improved, focus has shifted to long-term outcomes and complications that may impact prognosis.
One of the most common adverse events following TAVI is the development of conduction disturbances, often necessitating permanent pacemaker (PM) implantation. While newer-generation devices and improved implantation techniques have reduced the incidence of paravalvular leaks, they have not consistently decreased the need for PM implantation [2,3]. Notably, PM rates vary significantly between different valve platforms, with self-expanding valves showing higher rates than balloon-expandable systems [4,5]. In light of the expanding TAVI population, the potential long-term consequences of pacing—such as electrical dyssynchrony, heart failure, and device-related complications—are gaining clinical and ethical importance [6,7,8].
However, the prognostic significance of post-TAVI PM implantation remains controversial. Some studies and meta-analyses have suggested associations with increased long-term mortality and heart failure hospitalizations [4,9,10,11], while others—including large national registries—have found no negative impact [12,13]. Methodological differences, heterogeneous patient populations, and limited adjustment for confounders complicate interpretation.
In this study, we aimed to evaluate the impact of permanent PM implantation on short- and long-term all-cause mortality after TAVI in a large, unselected single-center cohort, complemented by external validation using a nationwide Austrian dataset [14]. Particular attention was paid to the distinction between pre-existing and procedure-related PMs and to known predictors of pacing, in order to contribute clinically relevant evidence to this ongoing debate. To ground our analysis in current evidence, we additionally conducted a structured literature search to synthesize contemporary knowledge on PM implantation after TAVI.
Methods
- Study Design and Population
This is a post-hoc analysis of a prospective, single-center observational cohort including all consecutive patients who underwent TAVI at the Department of Cardiology, University Hospital St. Pölten (Austria), between January 1, 2016, and December 31, 2020. The primary objective was to compare 1-year and 5-year all-cause mortality between patients requiring permanent PM implantation within 30 days after TAVI (Post-PM) and those not requiring a PM (No PM). Additionally, we assessed mortality in patients with a pre-existing PM at the time of TAVI (Pre-PM). The study was conducted in accordance with the Declaration of Helsinki (2013 revision) and approved by the local ethics committee of Karl Landsteiner University (EK1066/2022).
- Procedural Management and Follow-Up
Patient eligibility for TAVI was determined by a multidisciplinary heart team. Procedures were performed primarily via transfemoral access (99.6%) under conscious sedation. In four cases, subclavian access with general anesthesia was used. Device selection was left to the operator’s discretion. Temporary PMs were placed via femoral venous access in all patients without a prior PM or ICD. These were removed post-procedurally in the absence of an indication for permanent pacing. ECGs were obtained at baseline, immediately post-procedure, and daily for the first three days. All patients underwent continuous cardiac monitoring for ≥72 hours and received transthoracic echocardiography prior to discharge.Permanent PM implantation was performed in accordance with European Society of Cardiology (ESC) guidelines applicable at the time [15,16].
Follow-up visits were conducted at 1 year either on-site or via the referring physician. Thereafter, annual telephone interviews were performed to assess vital status and late PM implantations, with follow-up continuing up to 8 years post-procedure. Vital status was cross-verified using data from Statistics Austria.
- Data Collection
The institutional TAVI registry collected comprehensive data including demographics (age, sex, height, weight), medical history, TAVI indication, and 1- and 5-year mortality. Laboratory, ECG, and echocardiographic parameters were recorded pre-procedurally and on postoperative day 1. Survival data were censored at December 31, 2023.
- External Validation – AUTHEARTVISIT Study
To validate our findings and strengthen their generalizability, we analysed data from the AUTHEARTVISIT study [14]. This dataset includes anonymized national health insurance data of all patients who underwent TAVI in Austria between January 1, 2010, and December 31, 2020. Patients were stratified based on whether they received a permanent PM within 30 days post-TAVI.
- Structured Literature search
We conducted a structured literature search including both original studies and meta-analyses. Studies were classified by outcome, distinguishing those reporting no significant effect of Post-PM on mortality from those demonstrating a significant effect.
- Endpoints
The primary endpoint was all-cause mortality at 1 and 5 years following TAVI.
- Statistical Analysis
Continuous variables are expressed as mean ± standard deviation (SD) and were compared using two-tailed t-tests. Univariate and multivariate logistic regression analyses were performed to determine factors associated with PM implantation. Cox proportional hazards models were used to assess associations between variables and 1- and 5-year mortality.Only variables with p<0.05 in the univariate analysis were included in the multivariate models, except for creatinine and Troponin-T, which were excluded due to collinearity with renal function and serum NT-proBNP. Continuous variables were dichotomized at the median for regression analyses.
Survival analyses were performed using the Kaplan–Meier method. Curves were generated for each group, and the number at risk, events, and censored observations were reported annually. Median survival times and yearly survival probabilities with 95% confidence intervals (CIs) were calculated. Group comparisons were made using the log-rank test.
All statistical analyses were conducted using SPSS version 30 (IBM Corp., Armonk, NY, USA), GraphPad Prism 9 (GraphPad Software, La Jolla, CA, USA), and R version 4.4.1.
Results
Between January 1, 2016 and December 31, 2020 1114 consecutive patients (mean age 81 ± 5.8 years; 555 (49.8%) female) underwent TAVI (927 (83.2%) balloon-expandable transcatheter heart valves (THV)) and were followed for a mean of 5.6±1.3 years. Among them, 120 patients (10.8%) already carried a permanent PM at the time of TAVI, including 3 with cardiac resynchronization therapy. Among the remaining 994 patients, 153 (15.4%) underwent new PM implantation within 30 days following TAVI (Figure 1).
From the AUTHEARTVISIT national dataset, 6865 patients (mean age 81±5.8 years), 3803 (55.4%) female) were analyzed. Of these, 776 (11.3%) were Post-PM cases.
- Baseline Clinical and Demographic Characteristics
Baseline clinical and procedural characteristics of Pre-PM, Post-PM and No PM patients are summarized in Table 1. In brief, Post-PM compared to No PM patients were older (81.9± 5.5 vs. 80± 5.7 years, p= 0.006), less likely to be female (71 (46.4%) vs. 445 (52.9%), p<0.001), and had higher rates of peripheral artery disease (16 (10.5%) vs. 53 (6.3%), p=0.019). They presented with higher Troponin T levels (28.3µg/l (IQR 18-32.1) vs. 23 µg/l (IQR 16-37), p= 0.002), higher rates of pre-existing right bundle branch block (RBBB, 43 (28.1%) vs. 27 (3.2%), p<0.001), and a longer QRS duration (110ms (IQR 90-140) vs. 100ms (80-110), p<0.001), respectively.
Compared with Pre-PM, Post-PM patients were more likely to be female (71 (46.4%) vs. 39 (32.5%), p<0.001), had less atrial fibrillation (AF, 55 (35.9%) vs. 64 (53.3%), p=0.002), lower N-terminal pro-brain natriuretic peptide (NT-proBNP) levels (1273 (IQR 468-2779) vs. 2593 (IQR 1081-5055), p<0.001) and presented with higher left ventricular ejection fraction (LVEF, 60% (IQR 60-60) vs. 55% (IQR 35-60), p< 0.001). Furthermore, they had more RBBB (43 (28.1%) vs. 3 (2.5%), p<0.001), left bundle branch block (LBBB, 11 (7.2%) vs. 2 (1.7%), p=0.007), and left anterior hemiblock (LAH, 52 (36.1%) vs. 23 (20%), p<0.001) and shorter QRS duration (110ms (IQR 90-140) vs. 130ms (IQR 110-150), p<0.001).
Demographic characteristics of the AUTHEARTVISIT cohort are presented in Table 2. In brief No PM patients were more likely to be female (3400 (55.8%) vs. 403 (51.9%,), p= 0.043) and had less hyperlipidemia (1494 (24.5%) vs. 218 (28.0%), p= 0.035).
- Procedural data
Table 1 shows procedural characteristics. The majority of patients (83.2%) received balloon-expandable THVs. As compared to Pre-PM patients Post-PM recipients were implanted with smaller aortic bioprostheses (26.9mm± 2.2 vs. 27.2mm ± 2.0, p<0.001). In 99.6% a femoral access was used.
- Pacemaker implantation after TAVI
All patients in need of a permanent PM who were in sinus rhythm received dual-chamber pacing, and all patients in AF recieved single-chamber PMs. Neither CRT devices or conduction system-pacing nor devices with ICD function were implanted.
- Predictors of PM implantation within 30 days of TAVI
Predictors of Post-PM are demonstrated in Table 3. On univariate logistic regression, the following variables were significantly associated with PM implantation within 30 days: age (p=0.040), RBBB (p<0.001), LAH (p<0.001), LVEF (p = 0.020), and prosthesis size (p = 0.002). In multivariate analysis, only RBBB (p < 0.001), LAH (p = 0.020), LVEF (p = 0.007), and prosthesis size > 26mm (p = 0.002) remained independently associated with the need for PM implantation after 30 days while valve type (83.2% balloon-expandable) was not.
- Outcome at one and five years
Kaplan–Meier survival estimates (Figure 2A) demonstrated no significant difference in 1-year all-cause mortality between patients with and without PM (log-rank p = 0.41). Likewise, stratification by pacemaker status (No PM, Pre-PM, Post-PM) showed comparable 1-year survival rates (Figure 2B; p = 0.71). At 5 years, mortality was comparable between Post-PM and No PM groups (Figure 2C; p = 0.191), whereas patients with any PM exhibited higher mortality than those without, largely attributable to excess deaths in the Pre-PM subgroup (Figure 2D, graphical abstract; p < 0.001).
In univariate Cox regression for 1-year mortality , neither Post-PM (HR 1.10, 95% CI 0.70–1.90, p = 0.455) nor Pre-PM (HR 0.90, 95% CI 0.50–1.70, p = 0.975) was associated with early mortality. In contrast, several baseline parameters demonstrated significant associations: troponin T > 24 pg/mL (HR 3.3, 95% CI 2.1–5.3, p < 0.001), NT-proBNP > 1532 ng/L (HR 2.8, 95% CI 1.8–4.4, p < 0.001), LVEF < 60% (HR 1.7, 95% CI 1.2–2.4, p < 0.001), EuroSCORE II ≥5 points (HR 1.7, 95% CI 1.2–2.4, p = 0.002), and chronic kidney disease (CKD, HR 2.6, 95% CI 1.4–4.9, p = 0.002). After multivariate adjustment, only troponin T (HR 2.2, 95% CI 1.3–3.8, p = 0.002) and NT-proBNP (HR 2.2, 95% CI 1.3–3.8, p = 0.002) remained independently associated with 1-year mortality as detailed in Table 4.
At 5-year follow-up, Pre-PM was significantly associated with increased all-cause mortality (HR 1.6, 95% CI 1.2–2.1, p < 0.001), whereas Post-PM did not reach statistical significance (HR 1.2, 95% CI 0.9–1.5, p = 0.181). Other univariate predictors of adverse long-term outcome included age > 82 years (HR 1.3, 95% CI 1.1–1.6, p < 0.001), AF (HR 1.5, 95% CI 1.3–1.9, p < 0.001), CKD (HR 2.2, 95% CI 1.4–3.2, p < 0.001), troponin T (HR 2.0, 95% CI 1.6–2.4, p < 0.001), and NT-proBNP (HR 1.8, 95% CI 1.5–2.3, p < 0.001). In the multivariate model, Pre-PM remained an independent predictor of long-term mortality (HR 1.4, 95% CI 1.0–1.9, p = 0.030), while Post-PM remained non-significant (HR 1.2, 95% CI 0.8–1.6, p = 0.220). Independent covariates associated with late mortality comprised age > 82 years (HR 1.3, 95% CI 1.1–1.7, p = 0.004), AF (HR 1.3, 95% CI 1.0–1.7, p = 0.006), CKD (HR 2.0, 95% CI 1.1–3.8, p = 0.020), troponin T (HR 1.6, 95% CI 1.2–2.0, p < 0.001), and NT-proBNP (HR 1.4, 95% CI 1.1–1.8, p = 0.006) as depicted in Table 5.
- AUTHEARTVISIT National Dataset
Kaplan–Meier survival curves from the AUTHEARTVISIT cohort are shown in Figure 3, comparing Post-PM and No PM patients. The median follow-up time was 4.25 years (graphical abstract). There was no statistically significant difference in all-cause mortality between the two groups (log-rank p = 0.100). Estimated median survival was 4.95 years (95% CI: 4.60–5.35) for Post-PM patients and 5.26 years (95% CI: 5.11–5.46) for No PM patients (HR 1.06; 95% CI: 0.98-1.11, p=0.1).
- Overview of key studies on post-TAVI permanent PM and clinical outcomes
A literature overwiew is depicted in Table 6. Across the included studies, rates of Post-PM ranged between 12% and 31%. Follow-up durations extended up to 10 years. Several registries and cohort studies, including SWEDEHEART [12], UK-TAVI [17], PARTNER 2 S3 [18], TAVI-NOR [19], Hochstadt et al. [13] and the present study, reported no significant association between Post- PM implantation and long-term all-cause mortality. On the other hand, the SwissTAVI [9], FRANCE-TAVI [20], and the Danish cohort [10] identified an increased risk of mortality in Post-PM patients.
Discussion
In this large, single-center, all-comer TAVI cohort, PM implantation within 30 days was not associated with an increased risk of mortality at 1 or 5 years, whereas pre-existing PM identified patients at greater long-term risk. We validated the finding of a neutral impact of Post-PM using the nationwide AUTHEARTVISIT dataset of over 6,800 TAVI recipients [14].
Although the need for post-TAVI PM is an established procedural complication, its impact on short- and long-term outcomes remains debated. Evidence is limited, with only a handful of dedicated studies [9,10,13,15] and two recent meta-analyses [4,11], and results remain inconsistent. A summary of these data is provided in Table 6.

Table 6.
Overview of key studies on post-TAVI permanent pacemaker implantation (PM) and clinical outcomes.
Table 6.
Overview of key studies on post-TAVI permanent pacemaker implantation (PM) and clinical outcomes.
| Study | Design & Population | Study Period | Valve Types | Post-PM Rate | Follow-up | Mean Age | Main Findings | Limitations |
|---|---|---|---|---|---|---|---|---|
| Studies reporting no significant effect of post-TAVI PM on mortality | ||||||||
| Present Study (Lamm et al., 2025) | Single-center prospective cohort, n = 1,114+ validation in AUTHEARTVISIT (n ≈ 8,000) |
2011–2022 | 84% balloon-expandable, 12% self-expanding, 4% | 14% | Median 4.2 y | 81 ± 6 | Post-PM not associated with increased 1- or 5-year mortality; confirmed in national dataset; Pre-PM significantly associated with worse outcomes | No pacing-burden or CT-based depth data; no cause-specific mortality or HF hospitalization analysis |
| SWEDEHEART [12] | Nationwide registry, n = 3,420 | 2008–2018 | 38% ballon expandable, Self-expandable (not reported) |
14% | Median 2.7 y Up to 10 y |
82 ± 7 | No significant differences in mortality, HF hospitalization, or endocarditis between Post-PM and No-PM groups | No pacing-burden data; older-generation devices |
| Hochstadt et al. [13] | Single-center study, n = 1,489 | 2009–2019 | Ballon expandable (not reported) 62% self-expandable |
19% | Up to 6 y | 80 ± 7 | No significant association between Post-PM and long-term mortality, even at high pacing burden; Pre-PM significantly associated with higher mortality | Retrospective design, no CT-based implantation-depth assessment |
| Chen (2024) PARTNER 2 S3 [18] |
Multicenter registry, USA, n = 857 | 2014–2017 | Balloon-expandable (SAPIEN 3 only) | 12.5% | 60 Months | PM 83 ± 5 No PM 81 ± 7 |
No increased long-term mortality with post-TAVI PM; outcomes mainly driven by comorbidities | Limited sample size, device-specific, retrospective design |
| Wasim (2025) TAVI-NOR [19] |
Single-center n = 548 |
2012–2019 | ≈70% self-expanding, 18% mechanically expandable |
31.5% | 84 Months | 80 ± 7 | No significant difference in 7-year mortality between post-PM and no-PM groups | Small cohort, high SEV share, retrospective |
| Myat (2021) UK-TAVI [17] |
Nationwide registry, n = 6,815 |
2007-2015 | ≈60% balloon-expandable, ≈40% self-expanding | 19.2% | 84 Months | PM 82 ±7 No PM 81 ±7 |
No independent association of post-PM with long-term mortality after adjustment | Retrospective design, limited granularity of procedural data |
| Studies reporting increased risk associated with post-TAVI PM | ||||||||
| Swiss TAVI [9] | Nationwide registry, n = 13,360 | 2011–2022 | 49% balloon-expandable, 47% self-expanding, 2,5% mechanically expandable | 20% | Median 4.9 y 120 Months |
81 ± 6 | Post-PM associated with higher all-cause mortality; absolute survival differences small; Kaplan–Meier curves cross multiple times | No valve-specific subgroup analyses, no pacing-burden data, potential non-proportional hazards |
| Danish Study [10] | Single-center study, n =816 | 2007–2017 | 9% balloon-expandable, 83% self-expanding, 8% mechanically expandable | 16% | Median 3.5 y | 81 ± 7 | Post-PM associated with increased long-term mortality, HF hospitalization, and reduced LVEF | High SEV share, limited generalizability, retrospective Design |
| Auffret (2024) FRANCE-TAVI [20] |
Nationwide retrospective registry, n = 34,717 | 2013–2019 | ≈60% balloon-expandable, ≈40% self-expanding | 20.1% | 60 Months |
PM 83± 6 No PM 82 ± 7 |
Post-PM associated with higher long-term mortality; absolute effect size modest | Retrospective design, no pacing-burden or CT-depth data |
CI, Confidence interval; CT, Computed tomography; HR, Hazard Ratio; HF, Heart failure; MI, myocardial infarction; PM, Pacemaker; Post-PM, New pacemaker after TAVI; Pre-PM, Pre-existing pacemaker; RR, Relative risk; SEV, Self-expanding valve.
The findings of the present study align with the population-based SWEDEHEART registry [12], which included 3,420 transfemoral TAVI patients and reported no significant differences in mortality, heart failure hospitalization, or endocarditis between patients with and without Post-PM. Similarly, Hochstadt et al. [13] found no association between Post-PM and long-term mortality—even in patients with high pacing burden—whereas Pre-PM was linked to significantly worse outcomes (HR≈1.53; p=0.002). Moreover, declines in LVEF occurred more frequently among Post-PM patients.
In contrast, the SwissTAVI registry [9] recently reported a significant increase in long-term mortality among Post-PM patients (n=13,360, TAVI 2011–2022). Several differences between this registry and the aforementioned studies warrant attention. Balloon-expandable valves were used in <50% of SwissTAVI patients compared to ~80% in SWEDEHEART and our cohort, and Post-PM rates differed substantially (SwissTAVI 20%, SWEDEHEART 14%, present study 18%). Furthermore, the Kaplan–Meier curves in SwissTAVI crossed repeatedly, suggesting possible non-proportional hazards, yet no time-stratified or landmark analyses were performed. Although p-values reached statistical significance, absolute survival differences remained small. Similarly, a Danish single-center study [10] of >800 patients (79% self-expanding valves) reported increased late mortality, heart failure hospitalizations and reduced LVEF among Post-PM patients.
When contextualizing our findings within prior evidence, results across individual studies have been heterogeneous., [10,12,13] Cohorts with a high proportion of balloon-expandable valves- such as ours, SWEDEHEART [12], Hochstadt et al. [13], and PARTNER 2 S3 [18] consistently found no significant association between Post-PM and long-term mortality. By contrast, studies with greater use of self-expanding valves, including SwissTAVI [9] and the Danish study [10], reported an increased mortality risk. These discrepancies may reflect differences in valve technology, implantation techniques, and unmeasured confounders. Notably, in the smaller TAVI-NOR [19] cohort, which reported the highest Post-PM rate and frequent use of self-expanding and mechanically expandable valves, no difference in long-term mortality was observed - paradox potentially attributable to liberal implantation practices and limited statistical power. In our study, the proportion of self-expanding valves was very low which precludes clinically meaningful subgroup analyses.
Two recent meta-analyses further illustrate this complexity. Faroux et al. [4] pooled data from >50,000 patients across 30 studies and reported increased risks of all-cause mortality (RR=1.17, 95% CI 1.11–1.25) and heart failure hospitalization (RR=1.18, 95% CI 1.03–1.36) in Post-PM patients, though cardiac death was not significantly increased. In line with this, Zito et al. [11] performed a systematic review of 31 studies (n=51,069) and found similar results: increased all-cause mortality (RR=1.18, 95% CI 1.10–1.25) and higher heart failure rehospitalizations (RR=1.32), but no difference in stroke or myocardial infarction. Both meta-analyses are limited by retrospective designs, heterogeneous methodologies, and incomplete adjustment for valve type or pacing burden, highlighting the need for more granular, contemporary data.
Mechanistically, chronic right ventricular pacing can cause dyssynchrony and adverse remodeling, especially at high pacing burdens [21,22], but these effects usually require years to manifest. This likely explains why Pre-PM was associated with worse outcomes in our cohort. Post-TAVI conduction disturbances, on the other hand, are often transient and may resolve spontaneously, especially with modern high-implantation techniques [23]. Leadless pacemakers [24] may further reduce pacing-related complications, but long-term data remain limited. Finally, given the advanced age of our study population, pacing may contribute only marginally to overall mortality, where competing comorbidities dominate.
- Strengths and limitations
To enhance statistical power and generalizability, we combined our prospective single-center cohort with the large nationwide AUTHEARTVISIT dataset [14], which strengthens external validity. Furthermore, strengths of our study include a large sample size, standardized procedural protocols, guideline-based PM indications, long follow-up, and independent validation across two datasets.
However, several limitations should be acknowledged. First, claims-based data are inherently limited by potential miscoding, lack of device-level details, and reduced clinical granularity. Second, pacing-specific parameters—such as pacing burden, PM dependency, and use of conduction-system pacing or leadless devices—were unavailable, which restricts mechanistic interpretation. Third, procedural factors such as CT-based implantation depth and valve positioning were not analyzed. Fourth, outcomes beyond all-cause mortality—including cause-specific mortality, heart failure hospitalizations, and endocarditis rates—were not captured. Finally, no subgroup analyses by TAVI platform could be performed, which limits direct comparison with studies reporting divergent outcomes.
Conclusions
Taken together, our findings indicate that in contemporary, balloon-expandable–dominated elderly populations, post-TAVI PM implantation does not impose a clinically relevant survival disadvantage. In contrast, PM implantation before TAVI was associated with significantly worse long-term outcomes, likely reflecting underlying conduction disease and comorbid burden.
However, recent registry data and meta-analyses suggest that increased mortality risk may exist in subgroups treated predominantly with self-expanding valves. As TAVI expands to younger, lower-risk populations, careful evaluation of the long-term impact of pacing-related remodeling and conduction disturbances becomes increasingly important. Future research should focus on subgroup analyses by valve type, pacing burden quantification, and the role of novel technologies, such as conduction-system pacing and leadless pacemakers, to optimize device selection and patient outcomes. In younger patients with decades of pacing exposure ahead, the potential for long-term harm must be carefully balanced against procedural safety, device costs, and healthcare resource allocation.
- Clinical perspective
What is known: The impact of pacemaker (PM) implantation on outcomes after transcatheter aortic valve implantation (TAVI) remains controversial.
What is new: This large, real-world TAVI cohort with national validation demonstrated no increased mortality at 1 or 5 years after implantation of a new PM within 30 days after TAVI. However, a pre-existing PM prior TAVI identified patients at increased risk of long-term mortality, possibly reflecting underlying cardiac disease.
What is next: This cohort mainly comprised patients in their eighties at increased risk, therefore, the findings may not be generalizable to younger or low-risk populations. Further studies in younger patients are needed to clarify the long-term impact of TAVI-associated PM implantation.
Author Contributions
GL and JM are responsible for conceptualization. GL, PH, MG, MW, KS, CN, RM, JA, MH, JHA, conceived the study and curated data. GL, CV, JA and JM wrote the paper and visualized the data. GL, CV, HJA, UH, and CN cleaned, analyzed, and verified the underlying data. All authors commented on the paper, oversaw the analysis, and edited the final manuscript. All authors contributed to the study design. All authors contributed to drafting the paper and revised the manuscript for important intellectual content. All authors had full access to all of the data in the study and had final responsibility for the decision to submit for publication.
Funding
This research received no specific funding.
Clinical Trial Registration
This post-hoc analysis of our registry was not registered, as registration is not required for observational studies by the declaration of Helsinki. The study was approved by the local ethics committee (EK1066/2022).
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki (as revised in 2013) and was approved by the Institutional Ethics Committee of the Karl Landsteiner University of Health Sciences (EK1066/2022).
Data Availability Statement
Data are available from the corresponding author on reasonable request.
Permission to Reproduce Material from Other Sources
We did not reproduce material from other sources.
Acknowledgments
We acknowledge support by Open Access Publishing Fund of Karl Landsteiner University, Krems, Austria.
Conflicts of Interest
The authors declare no conflicts of interest.
Disclosures
Nothing to disclose.
Abbreviations
| CI | confidence interval |
| HR | hazard ratio |
| LBBB | left bundle branch block |
| LVEF | left ventricular ejection fraction |
| PM | pacemaker |
| Pre-PM | pre-existing pacemaker |
| Post-PM | new pacemaker within 30 days of TAVI |
| No PM | no pacemaker neither before nor after TAVI |
| RBBB | right bundle branch block |
| TAVI | transcatheter aortic valve implantation |
References
- Sharma T, Krishnan AM, Lahoud R, Polomsky M, Dauerman HL. National Trends in TAVR and SAVR for Patients With Severe Isolated Aortic Stenosis. J Am Coll Cardiol. 2022;80(21):2054-2056. [CrossRef]
- Cilingiroglu M, Marmagkiolis K. Paravalvular leak versus need for permanent pacemaker after TAVR: Sailing between Scylla and Charybdis. Catheter Cardiovasc Interv. 2017:155-156. [CrossRef]
- Van Rosendael PJ,Delgado V, Bax JJ. Conduction disturbances after transcatheter aortic valve implantation. Eur Heart J 2018; 39(21):2003-2013.
- Faroux L, Chen S, Muntane-Carol G, et al. Clinical impact of conduction disturbances in transcatheter aortic valve replacement recipients: A systematic review and meta-analysis. Eur Heart J. 2020;41:2771–2781. [CrossRef]
- Ravaux JM, Di Mauro M, Vernooy K et al. Permanent pacemaker implantation following transcatheter aortic valve implantation using self-expandable, balloon- expandable or mechanically expandalbe devices: a network meta-analysis. Europace. 2021;23(12):1998-2009. [CrossRef]
- Steinberg JS, Fischer A, Wang P et al. The clinical implications of cumulative right ventricular pacing in the Multicenter Automatic Defibrillator Trial II. J Cardiovasc Electrophysiol. 2005;16: 359 –365. [CrossRef]
- Gupta R, Mahajan S, Behnoush AH et al.Short- and Long-Term Clinical Outcomes Following Permanent Pacemaker Insertion Post-TAVR: A Systematic Review and Meta-Analysis. JACC Cardiovascular Interventions 2022;15:1683-92.
- Shen L, Jhund PS, Docherty KF et al. Prior Pacemaker Implantation and Clinical Outcomes in Patients With Heart Failure and Preserved Ejection Fraction. J Am Coll Cardiol HF 2019;7:418–27. [CrossRef]
- Badertscher P, Stortecky S, Serban T et al. SwissTAVI Investigators. Long-term outcomes of patients requiring pacemaker implantation after transcatheter aortiv valve replacement: The SwissTAVI registry. JACC Cardiovasc Interv. 2025 May 12;18(9):1163-1171.
- Jorgensen TH, De Backer O, Gerds TA, Bieliauskas G, Svendsen JH, Sondergaard L. Mortality and heart failure hospitalization in patients with conduction abnormalities after transcatheter aortic valve replacement. J Am Coll Cardiol Intv. 2019;12:52–61. [CrossRef]
- Zito A, Princi G, Lombardi M et al. Long-term clinical impact of permanent pacemaker implantation in patients undergoing transcatheter aortic valve implantation: a systematic review and meta-analysis. Europace. 2022 Jul 21;24(7):1127-1136. [CrossRef]
- Rück A, Saleh N, Glaser N. Outcomes Following Permanent Pacemaker Implantation After Transcatheter Aortic Valve Replacement: SWEDEHEART Observational Study. JACC Cardiovasc Interv. 2021;14(19):2173-2181.
- Hochstadt A, Merdler I, Meridor Y, et al. Effect of pacemaker implantation after transcatheter aortic valve replacement on long- and mid-term mortality. Heart Rhythm. 2021;18:199–206. [CrossRef]
- Auer J, Krotka P, Reichardt B, et al. Selection for transcatheter versus surgical aortic valve replacement and mitdterm survival: results of the AUTHEARTVISIT study. Eur J Cardiothorac Surg. 2024;66(1):ezae214. [CrossRef]
- The Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Brignole M, Auricchio A, Baron-Esquivias G, et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. European Heart Journal (2013) 34, 2281–2329.
- Kusumoto FM, Schoenfeld MH, Barrett C et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2019;74(7): 932-987.
- Myat A, Mouy F, Buchner L et al. Survival relative to pacemaker status after transcatheter aortic valve implantation. Cath Cardiovasc Intv 2021;98(3): E444-452. [CrossRef]
- Chen S, Dizon J, Hahn R et al. Predictors and 5-year clinical outcomes of pacemaker after TAVR. J Am Coll Cardiol Intv 2024;17:1325–1336. [CrossRef]
- Wasim D, Ali AM, Bleie O et al. Prevalence and predictors of permanent pacemaker implantation in patients with aortic stenosis undergoing transcatheter aortic valve implantation: a prospective cohort study. BMJ Open 2025;15:e093073. [CrossRef]
- Auffret V, Boulmier D, Didier R et al. Clinical effects of permanent pacemaker implantation after transcatheter aortic valve implantation: Insights from the nationwideFRANCE-TAVI registry. Arch Cardiovasc Dis. 2024;117(3):213-223. [CrossRef]
- Sweeney MO, Hellkamp AS, Ellenbogen KA et al. Adverse effect of ventricular pacing on heart failure and atrial fibrillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation2003;107:2932–2937.
- Yu CM, Chan JY, Zhang Q, et al. Biventricular pacing in patients with bradycardia and normal ejection fraction. N Engl J Med. 2009;361: 2123–2134. [CrossRef]
- Costa G, Zappulla P, Barbanti M, et al. Pacemaker dependency after transcatheter aortic valve implantation: incidence, predictors and long-term outcomes. EuroIntervention. 2019;15:875–883. [CrossRef]
- Ueyama HA, Miyamoto Y, Hashimoto K, et al. Comparison of Patient Outcomes Between Leadless vs Transvenous Pacemakers Following Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv 2024;17:1779–1791. [CrossRef]
Figure 1.
CONSORT Statement of patient inclusion. 1114 patients were analyzed. Of whom 120 (10.8%) received a PM prior to TAVI and accordingly were excluded from the primary analysis. 841 (75.5%) patients did not require a PM implantation and 153 (13.7%) underwent PM implantation within 30 days post TAVI.
Figure 1.
CONSORT Statement of patient inclusion. 1114 patients were analyzed. Of whom 120 (10.8%) received a PM prior to TAVI and accordingly were excluded from the primary analysis. 841 (75.5%) patients did not require a PM implantation and 153 (13.7%) underwent PM implantation within 30 days post TAVI.
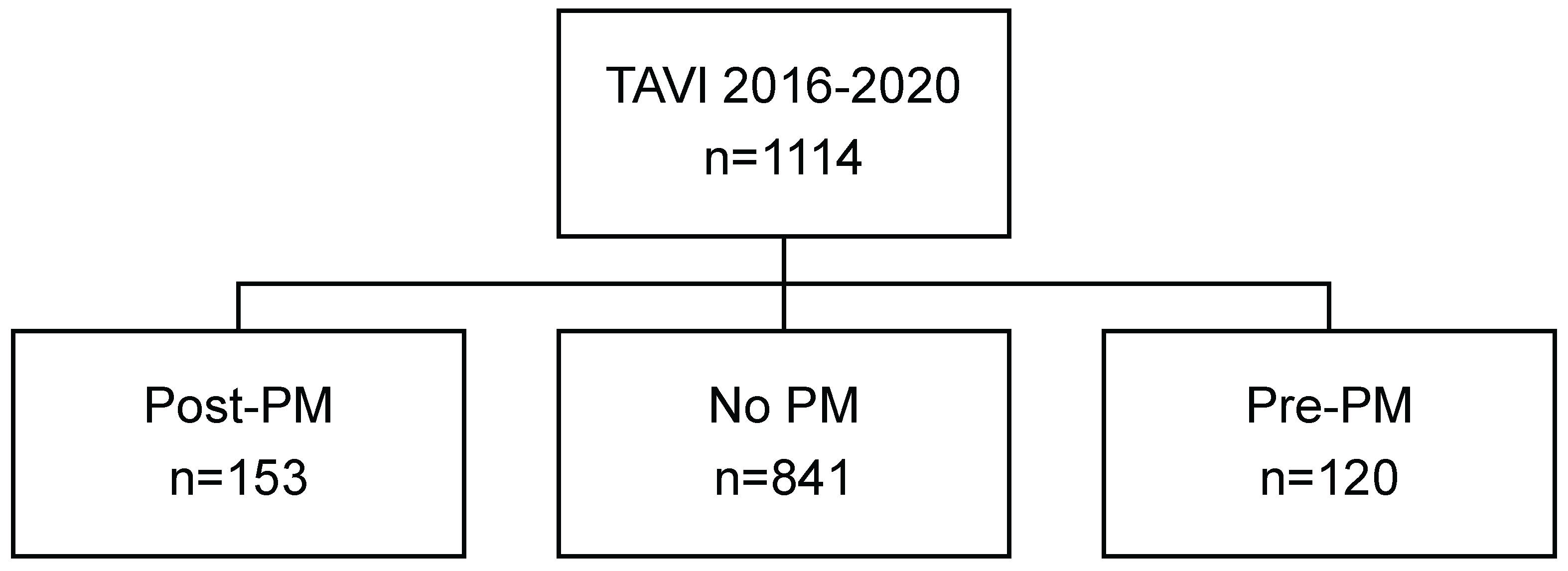
Figure 2.
1 and 5-year mortality in patients requiring PM insertion. There was no difference in 1- year survival probability in Post-PM compared to No PM patients as depicted in (A). In addition, there was no difference in 1- year survival probability in Pre-PM, Post-PM or No PM patients (B). Further, there was no difference in 5-year mortality in No compared to Post-PM patients as shown in C. In contrast, there was a significant difference in 5-year survival probability in Pre-PM compared to Post- or No PM patients (D).
Figure 2.
1 and 5-year mortality in patients requiring PM insertion. There was no difference in 1- year survival probability in Post-PM compared to No PM patients as depicted in (A). In addition, there was no difference in 1- year survival probability in Pre-PM, Post-PM or No PM patients (B). Further, there was no difference in 5-year mortality in No compared to Post-PM patients as shown in C. In contrast, there was a significant difference in 5-year survival probability in Pre-PM compared to Post- or No PM patients (D).
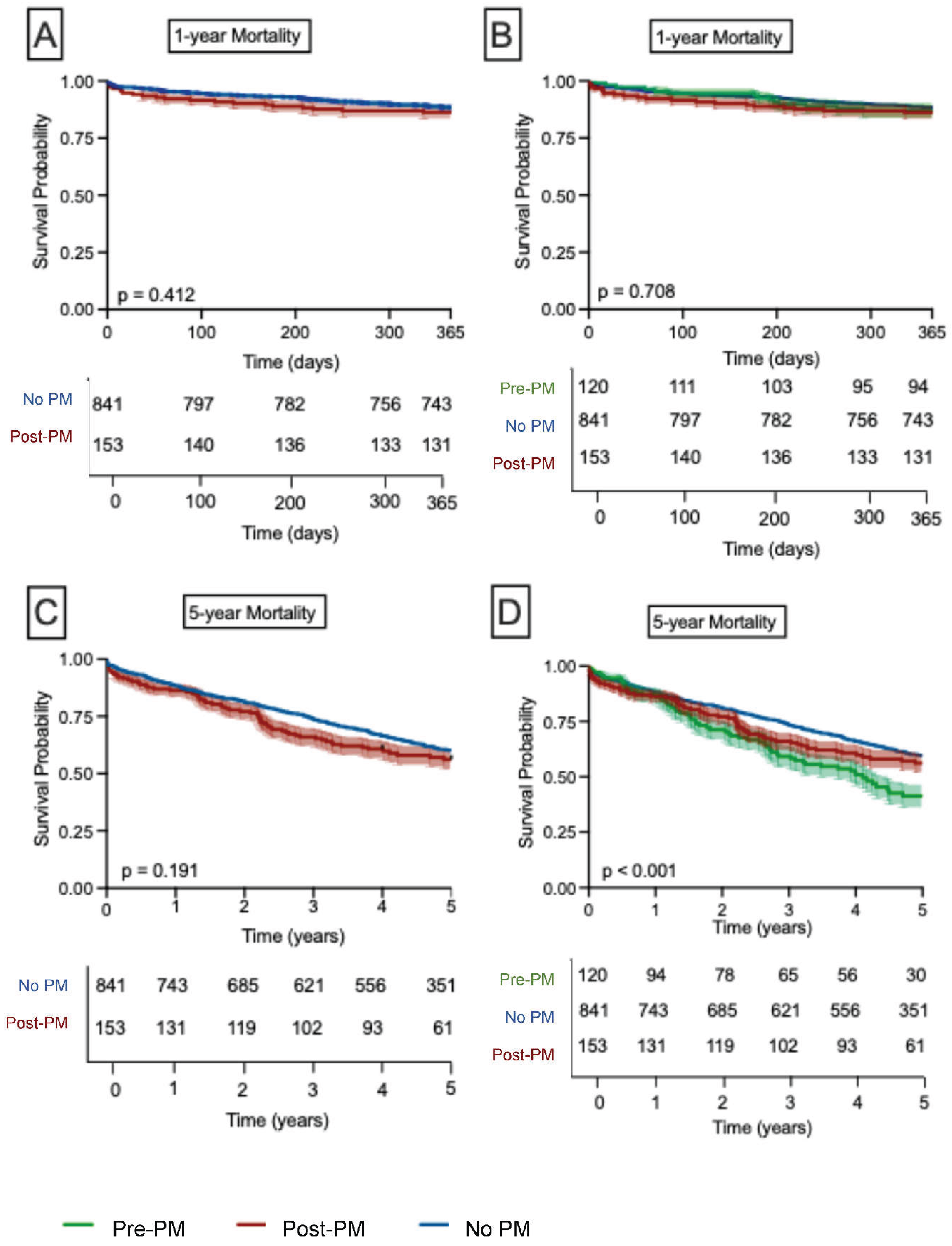
Figure 3.
Long-term mortality of 6865 Post- and No PM patients. Data of the AUTHEARTVISIT study. There was no difference in 12-year survival probability in Post-PM compared to No PM patients.
Figure 3.
Long-term mortality of 6865 Post- and No PM patients. Data of the AUTHEARTVISIT study. There was no difference in 12-year survival probability in Post-PM compared to No PM patients.
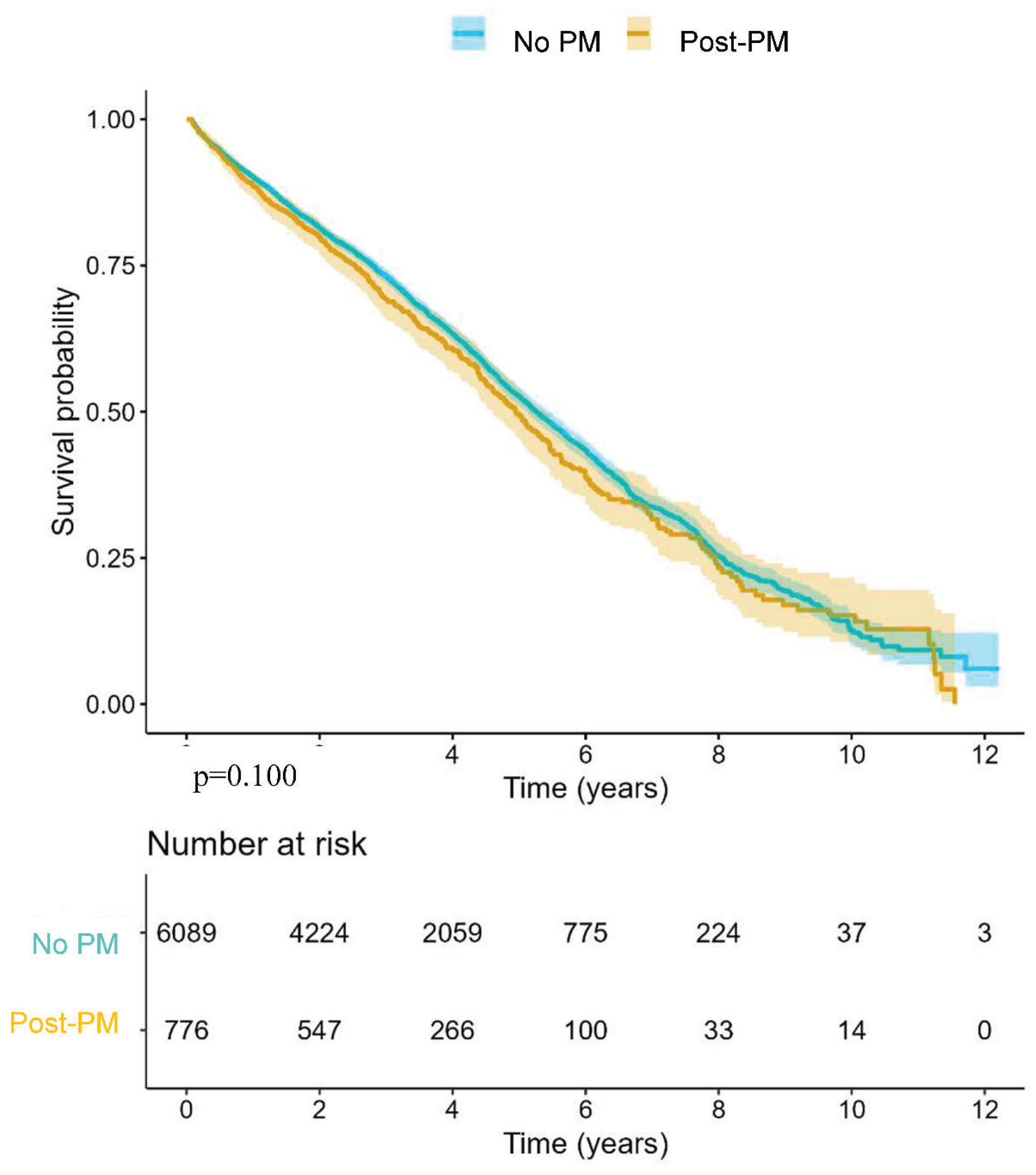
Table 1.
Baseline clinical and demographic data.
| No PM n=841 |
Post-PM n=153 |
Pre-PM N=120 |
p-value | |
|---|---|---|---|---|
| Demographic data | ||||
| Age (years) ## | 805.7 | 81.95.5 | 82.55.8 | 0.006 |
| Gender (female) # | 445 (52.9) | 71 (46.4) | 39 (32.5) | <0.001 |
| BMI (kg/m2) ## | 28.07.5 | 28.512.7 | 28.5 10.7 | 0.246 |
| Comorbidities and biomarkers: | ||||
| DM # | 282 (33.5) | 40 (33.3) | 43 (28.1) | 0.417 |
| CAD # | 420 (49.9) | 71 (46.4) | 67 (55.8) | 0.298 |
| PAD # | 53 (6.3) | 16 (10.5) | 15 (12.5) | 0.019 |
| AF # | 311 (37.0) | 55 (35.9) | 64 (53.3) | 0.002 |
| Euroscore II ## | 4.5.5 | 5.45.9 | 5.5.3 | 0.246 |
| Troponin T (µg/l) * | 23 (16.0; 37.0) | 28.3 (18.0; 32.1) | 30.4 (20.1; 41.0) | 0.002 |
| NT-proBNP (ng/l)* | 1508 (553; 3755) | 1273 (468; 2779) | 2593 (1081; 5055) | <0.001 |
| CRP (mg/dl) * | 0.3 (0.1; 0.7) | 0.2 (0.1; 0.4) | 0.3 (0.1; 0.8) | 0.208 |
| Creatinine (mg/dl) * | 1.0 (0.9; 1.3) | 1.1 (0.9; 1.4) | 1.1 (0.9; 1.4) | 0.003 |
| ECG-parameters (prior to intervention): | ||||
| RBBB # | 27 (3.2) | 43(28.1) | 3 (2.5) | <0.001 |
| LBBB # | 85 (10.1) | 11 (7.2) | 2 (1.7) | 0.007 |
| LAH # | 166 (21.3) | 52 (36.1) | 23 (20) | <0.001 |
| QRS duration * | 100 (80; 110) | 110 (90; 140) | 130 (100; 150) | <0.001 |
| PQ interval * | 170 (150; 200) | 180 (150; 220) | 190 (162; 217) | 0.116 |
| Resting heart rate (bpm) * | 71 (63; 81) | 70 (61; 78) | 60 (60, 70) | 0.047 |
| Echo-parameters (prior to intervention): | ||||
| LVEF (%)* | 60 (50, 60) | 60 (60, 60) | 55 (35, 60) | <0.001 |
| AVmean Gradient (mmHg) * | 44 (36; 55) | 44 (37; 52) | 40 (30; 51) | 0.064 |
| AVA (cm2) * | 0.7 (0.6; 0.8) | 0.7 (0.6; 0.8) | 0.7 (0.6; 0.9) | 0.017 |
| AV Vmax (m/s)* | 4.2 (3.8; 4.6) | 4.2 (3.8; 4.5) | 4.0 (3.5; 4.5) | 0.060 |
| Procedural parameters | ||||
| Valve type | ||||
| Edwards SAPIEN 3 THV- Model 9600 TFX # | 440(52.4) | 83 (54.2) | 73 (60.8) | |
| Edwards Sapien 3 Ultra THV- Model 9750 TFX # | 259 (30.8) | 36 (23.5) | 27 (22.5) | |
| Edwards SAPIEN XT THV-Model 9300 TFX # | 4 (0.5) | 2 (1.7) | 2 (1.3) | |
| Portico™ Transcatheter Aortic Valve # | 76 (9.0) | 17 (11.1) | 13 (10.8) | |
| Evolut™ R system # | 23 (2.7) | 5 (3.3) | 2 (1.7) | |
| Evolut™ PRO+ system # | 5 (0.6) | 1 (0.7) | 0 (0.0) | |
| LOTUS Edge™ Aortic Valve System # | 31 (3.7) | 9 (5.9) | 3 (2.5) | |
| ALLEGRA™ TAVI System TF # | 2 (0.2) | 0 (0.0) | 0 (0.0) | 0.467 |
| Aortic valve size (mm) # | 26.2 2.2 | 26.92.2 | 27.22.0 | <0.001 |
| Type of expansion | ||||
| Balloon-expandable # | 704 (83.7) | 121 (79.1) | 102 (85.0) | |
| Self-expanding # | 106 (12.6) | 23 (15.0) | 15 (12.5) | |
| Mechanically expandable # | 31 (3.7) | 9 (5.9) | 3 (2.5) | 0.516 |
| Balloon pre-dilatation # | 20 (2.4) | 2 (1.3) | 3 (2.5) | 0.699 |
| Balloon post-dilatation # | 86 (10.2) | 15 (9.8) | 10 (8.3) | 0.809 |
| Complications | ||||
| Annular rupture # | 2 (0.2) | 1 (0.7) | 0 (0.0) | 0.550 |
| Cardiac arrest # | 2 (0.2) | 1 (0.7) | 0 (0.0) | 0.550 |
| Aortic dissection # | 1 (0.1) | 0 (0.0) | 0 (0.0) | 0.850 |
| Conversion to open surgery # | 2 (0.2) | 0 (0.0) | 1 (0.8) | 0.393 |
AF, Atrial fibrillation; AV, Aortic valve; AVA, Aortic valve area; BMI, Body mass index; CAD, Coronary artery disease; CRP, C-reactive protein; DM, Diabetes mellitus; LAH, Left anterior hemiblock; LBBB, Left bundle branch block; LVEF, Left ventricular ejection fraction; No PM, No pacemaker neither before nor after TAVI; NT-proBNP, N-terminal pro-brain natriuretic peptide; Post-PM, New pacemaker after TAVI; Pre-PM, Pre-existing pacemaker; PAD, Peripheral artery disease; RBBB, Right bundle branch block; THV, Transcatheter heart valve; TF, Transfemoral; Vmax, Maximum velocity; # n (%),## mean ± SD, * median (IQR).
Table 2.
Clinical and demographic data of the AUTHEARTVISIT Study.
| No PM n = 6089 |
Post-PM n = 776 |
p-value |
|
|---|---|---|---|
| Demographic data | |||
| Age (years)* | 81 (78 - 85) | 82 (78 - 85) | 0.107 |
| Gender (female)# | 3400 (55.8) | 403 (51.9) | 0.043 |
| Comorbidities | |||
| Heart failure # | 1422 (23.3) | 190 (24.4) | 0.512 |
| ACS# | 122 (2.0) | 15 (1.9) | 1 |
| Stroke# | 113 (1.8) | 14 (1.8) | 1 |
| Diabetes mellitus# | 1206 (19.8) | 154 (19.8) | 1 |
| Obesity# | 347 (5.7) | 53 (6.8) | 0.236 |
| Hyperlipidemia# | 1494 (24.5) | 218 (28.0) | 0.035 |
| Hyperuricemia# | 224 (3.6) | 38 (4.9) | 0.117 |
| Valvular CMP# | 5571 (91.4) | 718 (92.5) | 0.364 |
| Ischemic CMP# | 3213 (52.7) | 408 (52.5) | 0.951 |
| Artherosclerosis# | 506 (8.3) | 64 (8.2) | 1 |
| Pulmonary diseases# | 382 (6.2) | 52 (6.7) | 0.702 |
| Kidney diseases Yes# | 1235 (20.2) | 176 (22.6) | 0.131 |
| Malignant diseases# | 385 (6.32%) | 49 (6.31%) | 1 |
ACS, Acute coronary syndrome; CMP, cardiomyopathy; No PM, No pacemaker neither before nor after TAVI; Post-PM, New pacemaker after TAVI; # n; * median (IQR).
Table 3.
Logistic regression analysis of PM implantation within 30 days after TAVI.
| Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|
| OR | CI 95% | p-value | OR | CI 95% | p-value | ||
| Age | ≥ 82 years | 1.4 | 1.0-2.0 | 0.040 | 1.1 | 0.7-1.7 | 0.441 |
| Sex | Male | 1.2 | 0.9-1.7 | 0.172 | |||
| DM | 0.7 | 0.5-1.1 | 0.171 | ||||
| CAD | 0.8 | 0.6-1.2 | 0.362 | ||||
| PAD | 1.6 | 0.9-3.0 | 0.077 | ||||
| AF | 0.9 | 0.6-1.3 | 0.817 | ||||
| Euroscore II | ≥5 points | 1.1 | 0.7-1.6 | 0.465 | |||
| Troponin T (µg/l) | ≥24 pg/ml | 1.2 | 0.8-1.8 | 0.201 | |||
| NT-proBNP (ng/l) | ≥1532 ng/L | 0.8 | 0.5-1.1 | 0.273 | |||
| Creatinine (mg/dl) | ≥1.3mg/dl | 1.2 | 0.9-1.8 | 0.148 | |||
| RBBB | 11.9 | 7.1-20.1 | <0.001 | 12.1 | 6.8-21.4 | <0.001 | |
| LBBB | 0.6 | 0.3-1.3 | 0.267 | ||||
| LAH | 2.0 | 1.4-3.0 | <0.001 | 1.6 | 1.0-2.5 | 0.020 | |
| LVEF | <60% | 1.6 | 1.0.-2.4 | 0.020 | 1.9 | 1.1-3.0 | 0.007 |
| Prosthesis size | >26 mm | 1.7 | 1.2-2.4 | 0.002 | 1.8 | 1.2-2.7 | 0.002 |
| Balloon pre-dilatation | 0.5 | 0.1-2.3 | 0.426 | ||||
| Balloon post-dilatation | 0.9 | 0.5-1.7 | 0.916 | ||||
AF, Atrial fibrillation; CAD, Coronary artery disease; CI, Confidence interval; DM, Diabetes mellitus; LVEF, Left Ventricular Ejection fraction; LAH, Left anterior hemiblock; LBBB, Left bundle branch Block; NT-proBNP, N-terminal pro-brain natriuretic peptide; OR, Odds ratio; PAD, Peripheral artery disease; RBBB, Right bundle branch block.
Table 4.
Cox regression analysis for 1-year mortality.
| Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|
| HR | CI 95% | p-value | HR | CI 95% | p-value | ||
| 1-year all-cause mortality | |||||||
| PM | No PM | 1.0 | |||||
| Post-PM | 1.1 | 0.7-1.9 | 0.455 | ||||
| Pre-PM | 0.9 | 0.5-1.7 | 0.975 | ||||
| Age | ≥ 82 years | 1.1 | 0.8.1.6 | 0.319 | |||
| Gender | Male | 0.9 | 0.6-1.3 | 0.775 | |||
| DM | 1.0 | 0.7-1.4 | 0.976 | ||||
| CAD | 1.1 | 0.8-1.6 | 0.375 | ||||
| PAD | 0.9 | 0.7-1.3 | 0.956 | ||||
| AF | 0.7 | 0.2-2.0 | 0.590 | ||||
| CKD | 2.6 | 1.4-4.9 | 0.002 | 1.4 | 0.5-3.8 | 0.511 | |
| Euroscore II | ≥5 points | 1.7 | 1.2-2.4 | 0.002 | 1.1 | 0.7-1.8 | 0.515 |
| Troponin T | ≥24 pg/ml | 3.3 | 2.1-5.3 | <0.001 | 2.2 | 1.3-3.8 | 0.002 |
| NT-proBNP | ≥1532 ng/L | 2.8 | 1.8-4.4 | <0.001 | 2.2 | 1.3-3.8 | 0.002 |
| Creatinine | ≥1.3mg/dl | 1.6 | 1.2-2.3 | 0.003 | |||
| RBBB | 1.3 | 07-2.4 | 0.372 | ||||
| LBBB | 0.8 | 0.4.1.5 | 0.546 | ||||
| LAH | 1.1 | 0.7-1.7 | 0.403 | ||||
| LVEF | <60% | 1.7 | 1.2-2-4 | <0.001 | 1.1 | 0.7-1.7 | 0.629 |
Significant variables of the univariate analysis were included in the multivariate analysis. AF, Atrial fibrillation; CAD, Coronary artery disease; CI, Confidence interval; CKD, Chronic kidney disease; DM, Diabetes mellitus; LVEF, Left ventricular ejection fraction; LAH, Left anterior hemiblock; LBBB, Left bundle branch block; HR, Hazard ratio; NT-proBNP, N-terminal pro-brain natriuretic peptide; PAD, Peripheral artery disease; RBBB, Right bundle branch block.
Table 5.
Cox regression analysis for 5-year mortality.
| Univariate | Multivariate | |||||||
|---|---|---|---|---|---|---|---|---|
| HR | CI 95% | p-value | HR | CI 95% | p-value | |||
| 5 year all-cause mortality | ||||||||
| PM | No PM | 1.0 | ||||||
| Post-PM | 1.2 | 0.9-1.5 | 0.181 | 1.2 | 0.8-1.6 | 0.220 | ||
| Pre-PM | 1.6 | 1.2-2.1 | <0.001 | 1.4 | 1.0-1.9 | 0.030 | ||
| Age | ≥ 82 years | 1.3 | 1.1.-1.6 | <0.001 | 1.3 | 1.1-1.7 | 0.004 | |
| Sex | Female | 1.0 | 0.8-1.2 | 0.556 | ||||
| DM | 1.1 | 0.9-1.3 | 0.170 | |||||
| CAD | 1.1 | 0.9-1.3 | 0.286 | |||||
| PM | 1.1 | 0.9-1.3 | 0.083 | |||||
| AF | 1.5 | 1.3-1.9 | <0.001 | 1.3 | 1.0-1.7 | 0.006 | ||
| CKD | 2.2 | 1.4-3.2 | <0.001 | 2.0 | 1.1-3.8 | 0.020 | ||
| Euroscore II | ≥5 points | 1.5 | 1.2-1.8 | <0.001 | 1.2 | 0.9-1.5 | 0.159 | |
| Troponin T | ≥24 pg/ml | 2.0 | 1.6-2.4 | <0.001 | 1.6 | 1.2-2.0 | <0.001 | |
| NTproBNP | ≥1532 ng/L | 1.8 | 1.5-2.3 | <0.001 | 1.4 | 1.1-1.8 | 0.006 | |
| Creatinine | ≥1.3mg/dl | 1.5 | 1.3-1.9 | <0.001 | ||||
| RBBB | Yes | 1.3 | 0.9-1.9 | 0.071 | ||||
| LBBB | Yes | 1.3 | 0.9-1.5 | 0.072 | ||||
| LAH | Yes | 1.2 | 0.7-1.7 | 0.096 | ||||
| LVEF | <60% | 1.5 | 1.2-2.8 | <0.001 | 1.0 | 0.8-1.3 | 0.656 | |
Significant variables of the univariate analysis were included in the multivariate analysis. AF, Atrial fibrillation; CAD, Coronary artery disease; CI, Confidence interval; CKD, Chronic kidney disease; DM, Diabetes mellitus; LVEF, Left ventricular ejection fraction; LAH, Left anterior hemiblock; LBBB, Left bundle branch block; HR, Hazard ratio; NT-proBNP, N-terminal pro-brain natriuretic peptide; PAD, Peripheral artery disease; PM, pacemaker; RBBB, Right bundle branch block.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



