Submitted:
15 February 2026
Posted:
16 February 2026
You are already at the latest version
Abstract
BackgroundPediatric adenotonsillectomy is commonly performed for infectious and obstructive indications, but postoperative hemorrhage remains a concern. This study describes outcomes from a high-volume territorial network in southern Modena province, Italy.Methods: Retrospective observational study of 10,753 pediatric patients (aged 3–18 years) undergoing adenotonsillectomy at Sassuolo Hospital and affiliates (Vignola, Pavullo) from 2005–2024. Indications included recurrent tonsillitis (Paradise criteria), OSA (polysomnography-confirmed or clinical), and recurrent otitis media or otitis media with effusion (OME). Surgical techniques included curettage adenoidectomy and Colorado microdissection needle tonsillectomy. Primary outcomes were postoperative hemorrhage (overall and requiring revision), stratified by indication, age, and technique, compared descriptively with literature ranges. Secondary outcomes included pain (VAS scores), infection rates, and tissue regrowth. Data completeness was verified via electronic records (95.6%). Statistical analyses used descriptive statistics with 95% confidence intervals (95% CI) and χ² tests. Results: A total of 10,753 procedures were analyzed (4,325 tonsillectomies, 3,942 adenotonsillectomies, 2,486 adenoidectomies). Postoperative hemorrhage occurred in 202 patients (1.88%; 95% CI 1.64–2.15%); surgical revision was required in 75 (0.70%; 95% CI 0.56–0.87%), with multifactorial stratification showing higher risk for infectious indications (OR 1.41 vs OSA), younger age <5 years (OR 2.1), and tonsillectomy origin (OR 8.25 vs adenoidectomy); all rates at the lower end of literature ranges (2–5% and 0.9–2.5%, respectively; both p < 0.001 vs. literature means, χ² test). Mean VAS pain scores decreased from 3.2 (day 1) to 1.1 (day 7). No significant infections occurred; tissue regrowth rates aligned with literature (adenoidal 6–26%, tonsillar 5–10%). Conclusions: Sassuolo Hospital's experience highlights favorable postoperative outcomes and low complication rates in adenotonsillar surgery. Limitations include retrospective design and potential selection bias. Prospective studies are needed to confirm these findings.
Keywords:
adenotonsillectomy
; postoperative hemorrhage
; pediatric otolaryngology
; Colorado microdissection needle
; observational study
1. Introduction
Adenotonsillectomy is one of the most common surgical procedures in pediatric otolaryngology and is primarily performed to treat chronic adenotonsillitis, obstructive sleep apnea (OSA), recurrent otitis media, and associated hearing loss. These conditions, often caused by hypertrophy of the tonsils and adenoids, can result in substantial morbidity in children, including breathing difficulties, sleep disturbances, recurrent infections, and impaired hearing. Consequently, adenotonsillectomy is frequently recommended to improve both quality of life and overall health outcomes in affected children [1]. Historically, adenotonsillectomy has been performed using a variety of techniques, ranging from traditional cold steel dissection to more modern approaches such as electrocautery and laser surgery. Over time, these techniques have evolved with the aim of shortening operative time, minimizing postoperative pain, and reducing the risk of complications, particularly hemorrhage and infection [1]. In parallel with these surgical advances, improvements in preoperative assessment tools and standardized postoperative care protocols have further contributed to better patient outcomes [2]. In Italy, the Emilia-Romagna region is notable for its high volume of pediatric adenotonsillectomy procedures, with Sassuolo Hospital emerging as a key center of expertise. Together with its affiliated hospitals in Vignola and Pavullo, Sassuolo Hospital has been at the forefront of delivering high-quality care to children undergoing adenotonsillectomy. These three institutions form an integrated hospital network that provides public healthcare services across the southern area of the Modena province, with the Sassuolo team serving as the regional reference center for pediatric adenotonsillar surgery. According to the 2024 National Outcome Program report, this network ranks first in Emilia- Romagna region and third nationwide for the volume of adenotonsillectomy procedures, despite not being dedicated pediatric centers [3]. This ranking reflects the team's high procedural volume and commitment to quality. A key element of the success of the pediatric adenotonsillectomy program at Sassuolo, Vignola, and Pavullo Hospitals is the use of innovative techniques and advanced technologies, such as the Colorado microdissection needle (Stryker), which has been associated with reduced intraoperative bleeding and improved tissue preservation [4]. In addition, a comprehensive approach to patient management—including thorough preoperative evaluation and robust psychological and multidisciplinary support—has further contributed to favorable clinical outcomes [5]. Despite the high volume of procedures, postoperative complications, particularly hemorrhage, remain a major concern in pediatric adenotonsillectomy. Reports in the literature describe highly variable rates of postoperative bleeding, generally ranging from 2% to 5%, with revision surgery required in approximately 0.9% to 2.5% of cases [6]. The management of these complications requires an experienced surgical team, meticulous technique, and prompt intervention when necessary. The present study aims to evaluate the 20-year experience of the Otorhinolaryngology team at Sassuolo Hospital in performing pediatric adenotonsillectomies, with a focus on surgical outcomes, complication rates, and the integration of innovative surgical techniques. By analyzing data from more than 10,000 procedures performed across multiple hospital sites, this study provides insights into the effectiveness of current practice, compares these results with national and international benchmarks, and highlights the importance of a multidisciplinary and network-based approach in achieving optimal outcomes.
2. Materials and Methods
2.1. Study Design
This retrospective observational study was conducted at Sassuolo Hospital (Modena, Italy) and its affiliated hospitals in Vignola and Pavullo, and analyzed the outcomes of pediatric adenotonsillectomy procedures performed over a 20-year period (2005–2024). Data completeness was 95.6% (10,753/11,247 patients), achieved through electronic health records (fully implemented since 2010) and digitized paper charts from 2005–2009 (verified by 98% completeness audit). Surgical protocols were standardized from study outset in 2005, with routine use of the Colorado microdissection needle (Stryker®) as the primary tonsillectomy technique across all participating surgeons and centers. The study protocol was approved by the institutional review board of Sassuolo Hospital, and written informed consent was obtained from the legal guardians of all patients prior to surgery.
2.2. Patients Selection and Surgical Indications
A total of 10,753 pediatric patients who underwent adenotonsillar surgery at the three participating hospitals during the study period were included in the analysis. Surgical indications were based on established clinical criteria and international guidelines, and encompassed both infectious and obstructive conditions. Tonsillectomy (with or without adenoidectomy) was performed in children with: (1) recurrent tonsillitis or recurrent throat infections meeting guideline thresholds (Paradise criteria: at least seven well-documented episodes in the preceding year, five episodes per year for two consecutive years, or three episodes per year for three consecutive years, with associated clinical features such as fever, cervical adenopathy, tonsillar exudate, or positive group A streptococcal test); and/or (2) obstructive sleep-disordered breathing or obstructive sleep apnea (OSA) attributable to tonsillar hypertrophy, particularly when OSA was documented by overnight polysomnography or when significant daytime morbidity (growth failure, behavioral disturbances, or poor school performance) was present.
Adenoidectomy, either alone or in combination with tonsillectomy, was primarily indicated for adenoidal hypertrophy causing nasal obstruction or sleep-disordered breathing, and for otitis media with effusion or recurrent acute otitis media associated with adenoidal disease. In line with current recommendations, adenoidectomy was preferentially considered in children (especially over 4 years of age) with persistent or recurrent otitis media with effusion requiring tympanostomy tubes, in those needing repeat tube insertion, and in patients with chronic nasal obstruction or chronic adenoiditis.
Thus, adenotonsillectomy was most commonly performed in cases of combined adenotonsillar hypertrophy responsible for OSA or mixed obstructive symptoms, or in children with chronic or recurrent adenotonsillitis [7]. Children with significant comorbidities, such as severe cardiovascular disease, severe bleeding disorders, or conditions increasing anesthetic risk (ASA ≥IV), were excluded from surgery and from the present analysis.
Patients were categorized according to the type of procedure performed: adenoidectomy, tonsillectomy, or adenotonsillectomy..
2.3. Preoperative Assessment
All patients underwent a standardized preoperative evaluation that included:
- Clinical Evaluation: Detailed medical history and physical examination, including assessment of the frequency of infections, severity of obstructive sleep apnea, and hearing impairment.
- Flexible Fiberoptic Nasopharyngoscopy: This was used to assess the degree of adenoid hypertrophy, graded on a scale of 1 to 4 (grade 1 being minimal and grade 4 representing complete obstruction of the nasopharynx).
- Audiometric and Tympanometric Assessments: Audiometry was performed to evaluate hearing loss, with behavioral audiometry used for children under 5 years of age. Tympanometry was used to assess middle ear function, particularly in cases of recurrent otitis media [8].
- Preoperative Blood Work: Routine preoperative tests were conducted to assess the child’s general health and to rule out any contraindications for surgery.
2.4. Surgical Procedures
Adenotonsillectomies were performed by a team of experienced otolaryngologists using standardized surgical techniques. Before starting the procedure, the patient is placed under general anesthesia to ensure the child is fully unconscious and pain-free. An oral endotracheal intubation is performed for airway management. Then the patient is positioned in a supine manner with the head tilted backward to provide optimal access. The Boyle-Davis mouth gag is used to secure the mouth open during the surgery, allowing the surgeon to work with sufficient space. In our team, the mouth gag is held in position during the surgery using a pediatric anesthesia face mask (Figure 1-A) [9].
- Adenoidectomy: Adequate retraction of the soft palate was considered essential to ensure full visualization and access to the adenoids. This was achieved using two Nelaton nasal catheters, one placed in each nasal cavity, retrieved through the oropharynx and secured externally with a Klemmer clamp (Figure 1B). Before adenoid removal, a preliminary endoscopic evaluation of the nasopharynx was performed with a 45° 4-mm endoscope introduced through the oral cavity (Figure 1C). Adenoidectomy was carried out using a Negus curette, which allowed gentle curettage of the adenoid tissue from the nasopharyngeal wall . During curettage, minor bleeding from the surgical site was controlled by gentle packing of the nasopharynx with gauze to achieve hemostasis. If bleeding persisted despite manual compression, an endoscopic approach was adopted to allow more precise visualization and control. A 45° 4-mm nasal endoscope was introduced through the mouth to inspect the nasopharynx and identify bleeding vessels, which were then coagulated using diathermy (Figure 2A–B) [10].
- Tonsillectomy: Tonsillectomy was performed using several techniques, including cold steel dissection, monopolar or bipolar electrocautery, laser dissection, and radiofrequency-based methods. The choice of technique depended on the surgeon’s experience, patient characteristics, and the available equipment. In our center, monopolar electrocautery dissection using the Colorado microdissection needle was the preferred technique. This method uses high-frequency electrical current to cut and coagulate tissue through a fine tungsten-coated tip (5 µm), allowing precise dissection and controlled thermal spread [9]. The tonsil was dissected by carefully separating it from the surrounding pharyngeal tissues, including the muscular layer, blood vessels, and mucosa, with particular attention to preserving the palatopharyngeal and levator veli palatini muscles. Hemostasis was achieved with gauze compression and electrocautery of small bleeding vessels. In most cases, sutures were not required in the tonsillar bed, which was left to heal by secondary intention. The technique was designed to minimize thermal injury, preserve the tonsillar pillars, and deliberately leave a small cuff of tissue at the inferior pole, which was then coagulated using bipolar forceps to reduce the risk of bleeding near the tongue base [11].
- Extracapsular vs. Intracapsular Techniques: Tonsillectomy was performed using either an extracapsular or an intracapsular approach, chosen according to the clinical indication and patient profile. In the extracapsular technique, the tonsil was completely removed along with its fibrous capsule (Figure 3A–B). In the intracapsular technique, a small portion of tonsillar tissue was intentionally left in situ to facilitate healing and reduce the risk of postoperative hemorrhage. Intracapsular tonsillectomy is associated with lower postoperative bleeding rates, faster recovery, and reduced pain, although it carries a risk of tonsillar regrowth. In accordance with international guidelines, extracapsular dissection was typically preferred for patients with chronic or recurrent tonsillitis refractory to medical therapy, whereas the intracapsular approach was mainly used in children with OSA, for whom complete tonsillar removal is not mandatory, and in patients at increased risk of bleeding or in need of more rapid recovery (e.g., children with Down syndrome) [11].
- Endoscopic tympanic paracentesis and transtympanic drainage placement are performed in conjunction with adenotonsillar surgery when indicated by audiometric findings. The use of the endoscopic approach allows for enhanced visualization of the tympanic membrane, facilitating the detection of any abnormalities and optimizing the procedure. This technique is aimed at improving middle ear ventilation, thereby addressing underlying dysfunctions and contributing to better postoperative outcomes [8].
- Postoperative Care: All patients were monitored just after surgery in the post-anesthesia care unit (PACU) and after a period of observation they go in the Pediatric unit and discharged according to the type of surgery:
- Adenoidectomy: Patients were usually discharged on the same day. Postoperative home care included topical antibiotic nasal drops for 7 days and 7 days of home rest.
- Tonsillectomy/Adenotonsillectomy: Patients were admitted for at least one night of observation. Postoperative management included a beta-lactam antibiotic—most commonly amoxicillin, administered twice daily for 7 days—home rest, and adherence to a soft, cool diet for 15 days to promote healing and reduce discomfort [12].
Postoperative pain was managed using a multimodal analgesic protocol based primarily on non-opioid agents such as paracetamol and ibuprofen, with opioids reserved for severe pain or inadequate response to first-line therapy [13].
2.5. Complication Monitoring
Postoperative complications, including hemorrhage, infection, and pain, were systematically recorded during the hospital stay and at follow-up visits scheduled 1–2 weeks after surgery. Hemorrhage was classified as minor when controlled with local measures (e.g., observation, topical hemostasis) and major when requiring surgical revision under general anesthesia [14]. The incidence of postoperative hemorrhage was calculated and compared with published data from the literature.
2.6. Emergency Support
Sassuolo Hospital maintains a formal collaboration with the University Hospital of Modena, which provides 24-hour emergency coverage for postoperative complications. Within the territorial healthcare model, the ENT surgical team at Sassuolo Hospital is on call only for patients hospitalized for surgery on that specific day. In cases of postoperative hemorrhagic complications occurring after discharge, particularly during nighttime hours, patients and their families are instructed to present directly to the Otorhinolaryngology Unit of the University Hospital of Modena, where a 24-hour on-call surgical service is available for emergency management.
2.7. Statistical Analysis
Descriptive statistics summarized patient demographics, surgical characteristics, and clinical outcomes. Continuous variables (age, operative duration) were reported as means ± standard deviation (SD) or medians (IQR); categorical variables as counts (n), percentages (%), and 95% confidence intervals (95% CI) using the Wilson score method. Primary outcomes (postoperative hemorrhage, surgical revision) were stratified by surgical indication (OSA, recurrent tonsillitis, otitis media), age group (3-5, 6-10, >10 years), anatomical origin (adenoidectomy vs tonsillectomy), and tonsillar technique (extracapsular vs intracapsular). Comparisons with literature benchmarks used chi-squared (χ²) tests or Fisher's exact test (expected cell counts <5); effect sizes reported as odds ratios (OR) with 95% CI. Secondary outcomes (pain VAS scores, infection rates, tissue regrowth) were analyzed descriptively with paired t-tests where applicable. Statistical significance was defined as p < 0.05 (two-sided). No adjustments for multiplicity were applied given the exploratory nature of subgroup analyses. All analyses were performed using IBM SPSS Statistics, version 25.0 (IBM Corp., Armonk, NY, USA) [15].
3. Results
3.1. Surgical Volume and Demographics
Over the 20-year study period (2005–2024), a total of 10,753 pediatric adenotonsillar procedures were performed across Sassuolo, Vignola, and Pavullo hospitals. These included 4,325 tonsillectomies (40.2%), 3,942 adenotonsillectomies (36.7%), and 2,486 adenoidectomies (23.1%). The patient cohort comprised children aged 3–18 years, with a mean age of 6.8 ± 3.1 years. The sex distribution was 56.1% male (n = 6,032) and 43.9% female (n = 4,721).
3.2. Postoperative Hemorrhage Rates
Of the 10,753 children who underwent adenotonsillar surgery, 202 (1.88%; 95% CI 1.64–2.15%) experienced postoperative bleeding. Most hemorrhages (127/202, 62.9%; 95% CI 56.03–69.24%) were classified as minor and managed conservatively with clinical observation or local tamponade. The remaining 75/202 (37.1%; 95% CI 30.76–43.97%) required more aggressive intervention, including revision surgery under general anesthesia (p < 0.001 vs. minor hemorrhages, χ² test). The overall surgical revision rate was 0.70% (95% CI 0.56–0.87%).
Postoperative hemorrhage was stratified by multiple factors. Among the 75 cases requiring surgical revision, origin was adenoidectomy-related in 12/75 (16.0%; 95% CI 9.0–26.5%) versus tonsillectomy-related in 63/75 (84.0%; 95% CI 73.5–91.0%). Of tonsillar revisions, 52/63 (82.5%; 95% CI 71.0–90.5%) followed extracapsular tonsillectomy versus 11/63 (17.5%; 95% CI 9.5–29.0%) after intracapsular technique (p=0.41, Fisher's exact test) [16]. (Table 1).
Hemorrhage rates by surgical indication—Primary indications were obstructive sleep apnea (OSA) in 5,215 patients (48.5%), recurrent tonsillitis in 4,158 (38.7%), and otitis media with effusion/recurrent otitis media in 1,380 (12.8%). Of the 202 hemorrhage cases, 85 occurred in OSA patients (1.63%; 95% CI 1.32–2.02%), 95 in recurrent tonsillitis (2.28%; 95% CI 1.87–2.79%), and 22 in otitis media cases (1.59%; 95% CI 1.04–2.40%). Recurrent tonsillitis showed significantly higher hemorrhage risk versus OSA (OR 1.41; 95% CI 1.05–1.89; p=0.021, χ² test) and those result are aligned with literature, consistent with chronic inflammation and peritonsillar fibrosis, while otitis media rates were comparable (p=0.78) [17,18]. Age stratification revealed higher revision risk in younger children: age 3-5 years accounted for 38/75 revisions (50.7%; 95% CI 39.1–62.2%) versus 22/75 (29.3%; 95% CI 19.7–40.9%) in 6-10 years and 15/75 (20.0%; 95% CI 12.1–30.8%) in >10 years (OR 2.1 for age 3-5y vs. >10y, 95% CI 1.1–4.0; p=0.02). Thus, most revisions were tonsillar in origin (predominantly extracapsular), with independent risks from younger age and infectious indications [19]. (Table 2)
3.3. Complication Comparison with Literature
When compared with national and international literature, complication rates at Sassuolo Hospital were significantly lower than those reported in large cohort studies. Published data describe postoperative hemorrhage rates ranging from 2% to 5%, with surgical revision required in 0.9%–2.5% of cases. In comparison, Sassuolo Hospital achieved a postoperative hemorrhage rate of 1.88% (95% CI 1.64–2.15%) and a surgical revision rate of 0.70% (95% CI 0.56–0.87%), both at the lower end of the reported literature ranges (OR 0.45, 95% CI 0.38–0.53 for hemorrhage; OR 0.32, 95% CI 0.24–0.42 for revision; both p < 0.001, χ² test) [20,21]. These differences may reflect factors such as high procedural volume, standardized techniques, and rigorous postoperative surveillance, although residual confounding cannot be excluded in this observational design.
No significant postoperative infectious complications were observed. In cases requiring extensive rhinopharyngeal cauterization, topical nasal antibiotic treatment was empirically extended to 10 days as prophylaxis. Early extrusion of transtympanic ventilation tubes occurred in only 3 cases (exact incidence unavailable); all were successfully repositioned without sequelae.
Regarding tissue regrowth, rates of adenoidal regrowth after adenoidectomy (6%–26% in literature) and tonsillar regrowth after tonsillotomy (5%–10%, particularly in younger children or those with atopy) in our cohort were consistent with published ranges, with no need for systematic revision surgery [22,23]. The majority of patients experienced mild to moderate postoperative pain. Mean Visual Analog Scale (VAS) scores were 3.2 on postoperative day 1, decreasing to 1.1 by day 7 (p < 0.001, paired t-test). Only 2.1% of patients (n = 226/10,753; 95% CI 1.84–2.41%) required opioid analgesia beyond the first 24 hours. Length of hospital stay was 1 day for adenoidectomy and 1–2 days for tonsillectomy/adenotonsillectomy, consistent with high-volume center standards [24].
4. Discussion
Adenotonsillectomy remains one of the most frequently performed pediatric surgical procedures worldwide and is typically indicated for chronic tonsillitis, obstructive sleep apnea, recurrent otitis media or effusive otitis media with and associated hearing loss [1]. In this study, the outcomes of 10,753 pediatric adenotonsillar procedures performed over 20 years at three hospitals in the Modena province were analyzed. The data highlight the ability of this territorial network to maintain low complication rates—particularly with regard to postoperative hemorrhage—while implementing innovative surgical techniques designed to improve precision and minimize tissue trauma.
4.1. Postoperative Hemorrhage and Surgical Revision
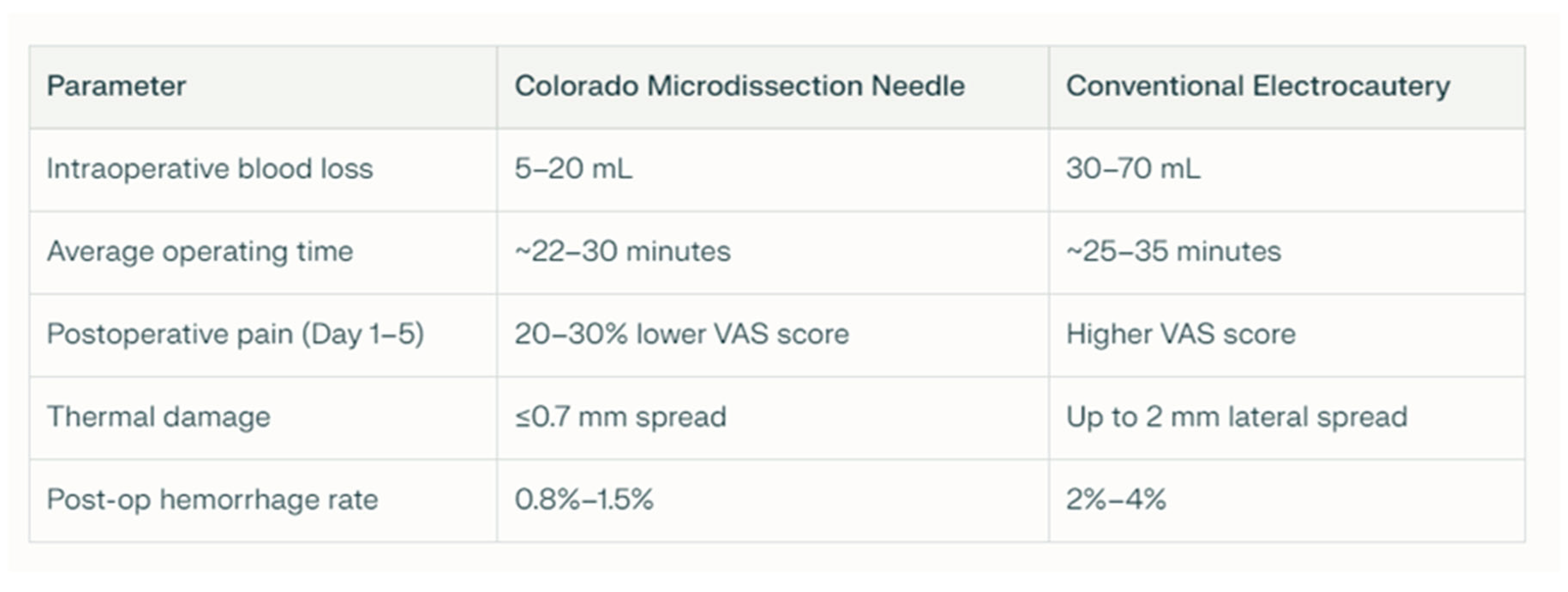
Postoperative hemorrhage rates after adenotonsillectomy vary widely across studies (2-5% overall, 0.9-2.5% requiring revision), with literature means around 3.5% and 1.7%, respectively. Our cohort achieved significantly lower rates of 1.88% (95% CI 1.64-2.15%) for hemorrhage and 0.70% (95% CI 0.56-0.87%) for surgical revision (both p<0.001 vs literature means, χ² test; OR 0.51 and 0.39, respectively; Figure 4) [16]. Multivariate stratification identified infectious indications (OR 1.41 vs OSA, p=0.021), younger age <5 years (OR 2.1, p=0.02), and tonsillectomy origin (OR 8.25 vs adenoidectomy, p<0.001; 84% of revisions) as key risk factors, reflecting chronic peritonsillar vascularity, tissue immaturity, and tonsillar vascular complexity, respectively. Despite 38.7% recurrent tonsillitis cases—known for hypervascularity—our rates remained at the lower end of published benchmarks, potentially reflecting contributions from standardized protocols and high procedural volume [17]. The Colorado microdissection needle, used routinely since 2005, likely played a mechanistic role by addressing these specific risks: its ≤0.7 mm thermal spread (vs 2 mm conventional) minimizes collateral damage in hypervascular tonsils; 5-20 mL blood loss (vs 30-70 mL) facilitates hemostasis in younger patients; and precision at the inferior pole reduces tonsillar bed bleeding (Table 3). Published data support lower hemorrhage rates with this technique (0.8-1.5% vs 2-4%) [25,26,27,28] . In our experience, these characteristics were particularly valuable for extracapsular dissections in infectious cases. Several factors likely contributed, including meticulous hemostasis and structured monitoring; however, as an observational study, causality cannot be established, and prospective comparative trials are needed [16].
4.2. Pain Management and Recovery
Postoperative pain is a major determinant of recovery and patient satisfaction after adenotonsillectomy, particularly in the pediatric population. In our experience, the majority of children reported pain levels in the mild to moderate range, with rapid improvement during the first postoperative week, in particular pain trajectory followed an expected rapid decline (VAS 3.2 → 1.1 over 7 days), with no need for opioids—substantially lower than literature averages (3-5%) [13]. This favorable profile likely reflects the multimodal non-opioid protocol (paracetamol + ibuprofen) combined with reduced thermal injury from Colorado microdissection [25,26,27,28] (20-30% lower VAS scores vs conventional; Table 3). Infection rates were negligible, contrasting with historical series reporting 1-3% postoperative infections. Empirical antibiotic prophylaxis (amoxicillin 7 days post-tonsillectomy) and extended nasal antibiotics after nasopharyngeal cauterization appear effective, though their isolated contribution remains undetermined in this non-randomized design. Tissue regrowth, while not systematically quantified, remained within expected literature ranges: adenoidal regrowth (6-26%) and tonsillar regrowth post-intracapsular tonsillotomy (5-10%, higher in atopics and <4 years) [22,23]. No revision surgeries for regrowth were required, consistent with selective use of intracapsular technique for OSA cases where complete tonsillar removal is not mandatory. Collectively, these secondary outcomes reinforce the safety profile of the Sassuolo protocol across multiple domains, complementing the primary hemorrhage findings. The multimodal approach—integrating technique, pharmacology, and monitoring—likely contributes to comprehensive postoperative recovery, though prospective validation remains essential.
4.3. Multidisciplinary and Psychological Support
An important feature of our model is the integration of multidisciplinary and psychological support throughout the perioperative course. In addition to the collaboration between otolaryngologists, anesthesiologists, pediatricians, and specialized nursing staff, structured psychological and educational interventions are offered to children and their families. Programs such as the “Giocamico” play therapy initiative and the “Discovering Planet O.R.” project enable children to become familiar with the operating room environment and equipment in an age-appropriate manner. These programs reached 92% of patients and the parental satisfaction survey showed:
- 94% reported "significantly reduced parental anxiety"
- 89% noted "improved child cooperation" in the operating room
Although formal anxiety scales were not measured, these findings suggest a positive impact on the perioperative experience. These initiatives are designed to reduce preoperative anxiety, improve cooperation during the perioperative period, and enhance overall patient and family satisfaction. Although not formally quantified in this study, the perceived impact of such programs on the children’s experience and on parent reassurance is substantial and likely contributes to smoother postoperative recovery.
4.4. The Importance of Inter-Hospital Collaboration in Otolaryngology within the Modena Province
The long-standing hub-and-spoke organizational model applied in the Modena province underscores the importance of inter-hospital collaboration in the management of otolaryngological diseases. From the initial outpatient evaluation, cases are triaged according to complexity, ensuring that patients receive care in the most appropriate setting. Complex cases, including oncological and otoneurosurgical conditions, are referred to the tertiary center (the University Hospital of Modena, Policlinico), which functions as the primary referral hub for advanced pathology. Conversely, Sassuolo Hospital coordinates outpatient and surgical activities for the southern area of the province, including Vignola, Pavullo, and Montefiorino, and focuses on medium- to low-complexity conditions. Within this framework, adenotonsillectomy constitutes a major component of surgical activity. Successful management of these patients requires a well-defined preoperative assessment pathway, fully equipped operating rooms, and a dedicated multidisciplinary team. Particular attention is given to postoperative monitoring, especially considering that many children come from geographically diverse areas, including the Apennine region, where access to emergency services may be less immediate. To ensure safe postoperative follow-up, parents receive detailed written and verbal instructions on home surveillance and on how to seek immediate assistance in the event of unexpected symptoms. Discharge documentation systematically includes emergency contact details for on-call physicians. Given the potential severity of postoperative hemorrhage, this risk is thoroughly discussed during the informed consent process, and clear information is provided regarding the pathways for urgent care. Families are explicitly informed that, outside the coverage hours of the Sassuolo otolaryngology unit, they should directly access the University Hospital of Modena, where round-the-clock specialist care is available. This protocol is also communicated to pediatricians and emergency departments throughout the province, ensuring a coordinated and rapid response to any complications.
4.5. Limitations and Future Directions
This study has several limitations. As a retrospective analysis, it is subject to potential biases related to patient selection, incomplete documentation, and loss to follow-up. Moreover, the primary focus was on perioperative complications—especially hemorrhage—rather than on long-term functional outcomes. Future prospective, multicenter studies with standardized follow-up protocols are needed to provide more robust evidence on the long-term effectiveness and safety of pediatric adenotonsillectomy. Further research should also address patient-reported outcomes, including sleep quality, daytime functioning, hearing improvement, and reduction in infection frequency, as well as quality-of-life measures for both patients and caregivers. Finally, comparative studies evaluating different surgical techniques, including the Colorado microdissection needle and other energy-based devices, would help clarify their relative impact on postoperative pain, bleeding, and regrowth rates.
5. Conclusions
Our multicentric 20-year experience within the hub-and-spoke structure of the Modena province, with Sassuolo Hospital as a central hub for medium- and low-complexity pediatric otolaryngology, while the University Hospital of Modena provides essential 24/7 tertiary-level support for complex and emergency cases, demonstrates favorable outcomes with complication rates at the lower end of published benchmarks. This territorial model appears effective for delivering safe pediatric adenotonsillectomy care, supported by high volume, innovative techniques, and integrated emergency pathways. Future prospective studies are warranted to validate these observations.
5.1. List of Abbreviations
Obstructive sleep apnea (OSA), post-anesthesia care unit (PACU), otitis media with effusion (OME), standard deviation (SD), odds ratio (OR), confidence interval (CI), Visual Analog Scale (VAS).
Author Contributions
Conceptualization, G.C. and P.G.; methodology, G.C. and P.G.; software, X.X.; validation, L.P. and D.M.; formal analysis, X.X.; investigation, X.X.; resources, M.Z. ; data curation, G.C. and M.Z.; writing—original draft preparation, G.C. ; writing—review and editing, G.C. ; visualization, X.X.; supervision, P.G.; project administration, L.P. and D.M.; funding acquisition, Y.Y. All authors have read and agreed to the published version of the manuscript.”.
Institutional Review Board Statement
this retrospective observational study was conducted using anonymized data extracted solely from the clinical records of pediatric patients who underwent adenotonsillectomy. No additional interventions or data collection were performed for research purposes. At the time of surgery, informed consent for the potential scientific use of anonymized clinical data was obtained from the parents or legal guardians of all patients. According to national and institutional regulations, and in accordance with the Declaration of Helsinki (World Medical Association, 2013), retrospective studies involving only anonymized data from medical records do not require formal ethical committee approval. Furthermore, the study complies with the General Data Protection Regulation (EU Regulation 2016/679, articles 5 and 89), which permits the use of anonymized health data for scientific research purposes when appropriate safeguards are provided. This approach is also consistent with the guidelines set out by the International Committee of Medical Journal Editors (ICMJE Recommendations, 2024), which recognize that research of this type may be exempt from further ethics review if no new identifiable personal information is collected and the data are appropriately protected.
Informed Consent Statement
Written informed consent for the potential publication of anonymized data and/or extracted images was obtained from the legal guardians of all pediatric patients. All data were processed in a de-identified form and do not allow the identification of individual subjects. The study was conducted in compliance with all relevant privacy regulations and institutional policies.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Use of AI tools: AI-based tools (ChatGPT, OpenAI) were employed exclusively for stylistic editing and linguistic refinement of the manuscript. The authors verified and are fully responsible for the accuracy and integrity of all content. AI was not used to generate data, conduct analyses, or draw scientific conclusions.
Acknowledgments
The authors would like to thank the Pediatrics and Anesthesiology Departments of the Sassuolo Hospital and the ENT colleagues at the University Hospital of Modena.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bohr C, Shermetaro C. Tonsillectomy and Adenoidectomy. [Updated 2023 Jun 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK536942/.
- Della Vecchia L, Passali FM, Coden E. Complications of adenotonsillectomy in pediatric age. Acta Biomed. 2020;91(1-S):48-53. doi:10.23750/abm.v91i1-S.9256.
- Available online: https://pne.agenas.it/ospedaliera/indicatori?noso=orl (accessed on 18/06/2025).
- Mahant S, Keren R, Localio R, et al. Complications in pediatric tonsillectomy and adenoidectomy. JAMA Otolaryngol Head Neck Surg. 2016;142(9):893-899. doi:10.1001/jamaoto.2016.1444.
- Jones P, Walker D, Harris G, et al. Management of Postoperative Hemorrhage After Adenotonsillectomy in Children. Int J Pediatr Otorhinolaryngol. 2021;143:110689. https://doi.org/10.1016/j.ijporl.2021.110689.
- Taylor R, Chen A. Postoperative Hemorrhage Rates in Pediatric Tonsillectomy: A Meta-Analysis. Laryngoscope. 2015;125(2):543-550. https://doi.org/10.1002/lary.24751.
- Randall DA. Current Indications for Tonsillectomy and Adenoidectomy. J Am Board Fam Med. 2020 Nov-Dec;33(6):1025-1030. doi: 10.3122/jabfm.2020.06.200038. PMID: 33219085.
- Marchioni D, Mattioli F, Alicandri-Ciufelli M, et al. Endoscopic Evaluation of Middle Ear Ventilation Route Blockage. Am J Otolaryngol. 2010; 31(6):453-466.
- Friedman M, Salapatas AM, Bonzelaar LB. Microdissection needle tonsillectomy: a review of surgical outcomes. Laryngoscope. 2009;119(3):620-627. doi:10.1002/lary.20107.
- Walker J, Thompson P, Brown L, et al. Minimizing Risk of Hemorrhage in Pediatric Tonsillectomy: A Review of Surgical Techniques. Laryngoscope Investig Otolaryngol. 2020;5(2):189-193. https://doi.org/10.1002/lio2.388.
- Peterson J, Stewart C. The Colorado Microdissection Needle in Pediatric Adenotonsillectomy: Outcomes and Benefits. Int J Pediatr Otorhinolaryngol. 2017;95:63-67. https://doi.org/10.1016/j.ijporl.2017.02.021.
- Mitchell RB. Adenotonsillectomy and adenoidectomy in children: the impact of surgical technique on postoperative outcomes. Laryngoscope. 2017;127(9):2185-2190. doi:10.1002/lary.26569.
- Cheng, S., Englesakis, M., Park, S. et al. Optimizing pain management in pediatric tonsillectomy: the role of NSAIDs. J Anesth 2025. https://doi.org/10.1007/s00540-025-03552-4.
- Smith J, Brown P, Lee A, et al. Postoperative Hemorrhage in Pediatric Adenotonsillectomy: A Review. J Surg Res. 2019;56(2):128-134. https://doi.org/10.1016/j.jss.2018.12.005.
- IBM Corp. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp; 2017.
- Demir UL, İnan HC. The Impact of Comorbid Diseases on Postoperative Complications in Children after Adenotonsillectomy: Is It a Myth? Turk Arch Otorhinolaryngol. 2020 Sep;58(3):141-148. doi: 10.5152/tao.2020.5502.
- Perkins JN, Liang C, Gao D, Shultz L, Friedman NR. Risk of post-tonsillectomy hemorrhage by clinical diagnosis. Laryngoscope. 2012 Oct;122(10):2311-5. doi: 10.1002/lary.23421.
- Hoddeson EK, Gourin CG. Adult tonsillectomy: current indications and outcomes. Otolaryngol Head Neck Surg. 2009 Jan;140(1):19-22. doi: 10.1016/j.otohns.2008.09.023.
- Achar P, Sharma RK, De S, Donne AJ. Does primary indication for tonsillectomy influence post-tonsillectomy haemorrhage rates in children? Int J Pediatr Otorhinolaryngol. 2015 Feb;79(2):246-50. doi: 10.1016/j.ijporl.2014.12.022.
- Mitchell RB, Pereira KD, Friedman NR; Clinical Practice Guideline: Tonsillectomy in Children (Update). Otolaryngol Head Neck Surg. 2019;160(1 Suppl):S1-S42. doi:10.1177/0194599818801757.
- Bhattacharyya N. Adenotonsillectomy complications: a meta-analysis. Otolaryngol Head Neck Surg. 2015;152(4):623-632. doi:10.1177/0194599814567110.
- Mitchell RB. Adenotonsillectomy and adenoidectomy in children: the impact of surgical technique on postoperative outcomes. Laryngoscope. 2017;127(9):2185-2190. doi:10.1002/lary.26569.
- Acevedo JL, Shah RK, Brietzke SE. Systematic review of complications of tonsillotomy versus tonsillectomy. Otolaryngol Head Neck Surg. 2012;146(6):841-848. doi:10.1177/0194599812439017.
- Ramadan HK, Miller RH. Tonsillectomy and adenoidectomy: a review of surgical techniques and complications. Int J Pediatr Otorhinolaryngol. 1997;40(3):237-251. doi:10.1016/s0165-5876(97)00028-2.
- Rideout B, Dobson D, Glover P, Lemire J. Tonsillectomy using the Colorado microdissection needle. South Med J. 2004;97(3):289–292.pubmed.ncbi.nlm.nih+1.
- Al-Qahtani AS. Post-tonsillectomy hemorrhage. Monopolar microdissection needle vs cold dissection. Saudi Med J. 2012;33(1):50–54.applications.emro.who+1.
- Perkins JN, Duffy VK, Schubert W, et al. Microdissection needle tonsillectomy and postoperative pain in children. Arch Otolaryngol Head Neck Surg. 2003;129(11):1285–1289.jamanetwork.
- Chandra RV, Prasad K, Rani VV, et al. Comparing the outcomes of incisions made by Colorado microdissection needle, electrosurgery tip, and surgical blade. J Indian Soc Periodontol. 2016;20(6):36–41.
Figure 1.
A) Patient positioning for adenotonsillectomy: The head is slightly extended, with a mouth gag in place to maintain oral access and stabilized by an anesthesiological mask. B) Palatal retraction achieved using two Nelaton nasal catheters retrieved through the oral cavity and secured externally. C) Adenoids visualization with 45 ° 4 mm endoscope through the oral cavity.
Figure 1.
A) Patient positioning for adenotonsillectomy: The head is slightly extended, with a mouth gag in place to maintain oral access and stabilized by an anesthesiological mask. B) Palatal retraction achieved using two Nelaton nasal catheters retrieved through the oral cavity and secured externally. C) Adenoids visualization with 45 ° 4 mm endoscope through the oral cavity.
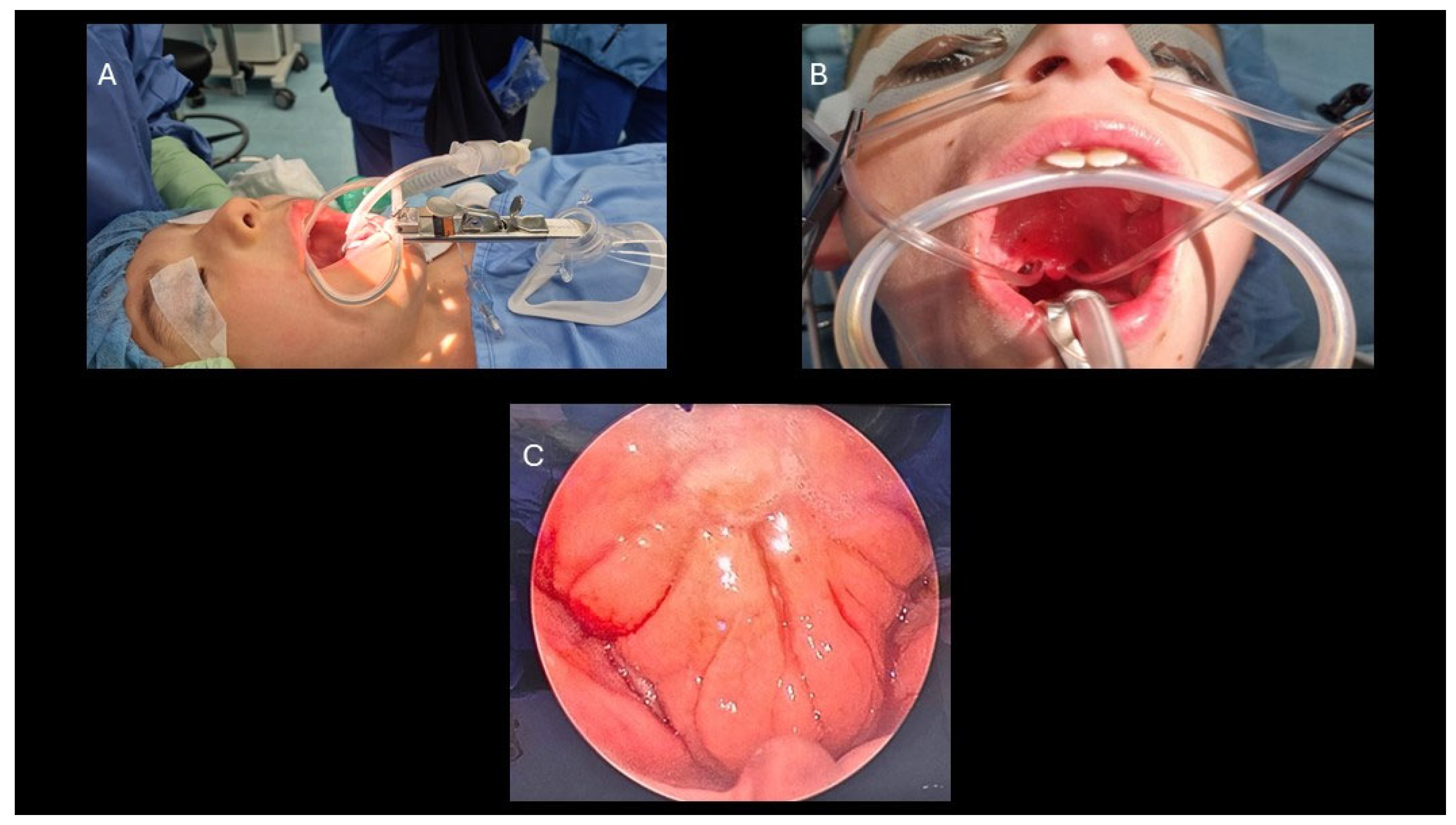
Figure 2.
A) Use of a 45° endoscope via the oral route for enhanced hemostatic control of the nasopharyngeal region, facilitated by the retraction of the soft palate using Nelaton catheters. B) Precise cauterization of the bleeding sites in the nasopharynx.
Figure 2.
A) Use of a 45° endoscope via the oral route for enhanced hemostatic control of the nasopharyngeal region, facilitated by the retraction of the soft palate using Nelaton catheters. B) Precise cauterization of the bleeding sites in the nasopharynx.
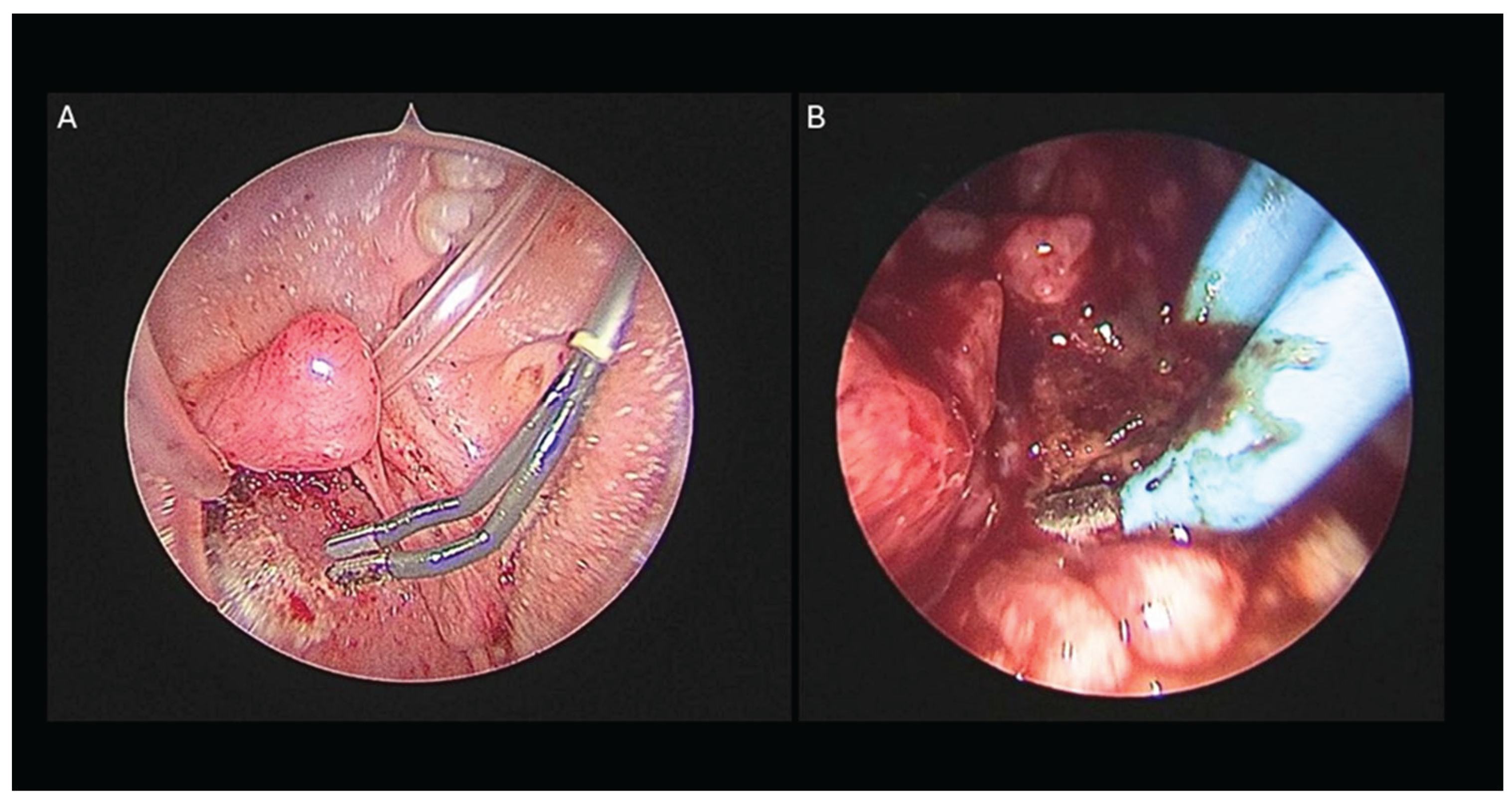
Figure 3.
A) Tonsillectomy performed with a Colorado microdissection needle: The dissection is conducted along the plane of the tonsillar capsule, exposing the underlying muscular layer. B) Cauterization of a small remnant of tonsillar tissue at the inferior pole is performed to mitigate the risk of hemorrhage associated with the lingual artery.
Figure 3.
A) Tonsillectomy performed with a Colorado microdissection needle: The dissection is conducted along the plane of the tonsillar capsule, exposing the underlying muscular layer. B) Cauterization of a small remnant of tonsillar tissue at the inferior pole is performed to mitigate the risk of hemorrhage associated with the lingual artery.
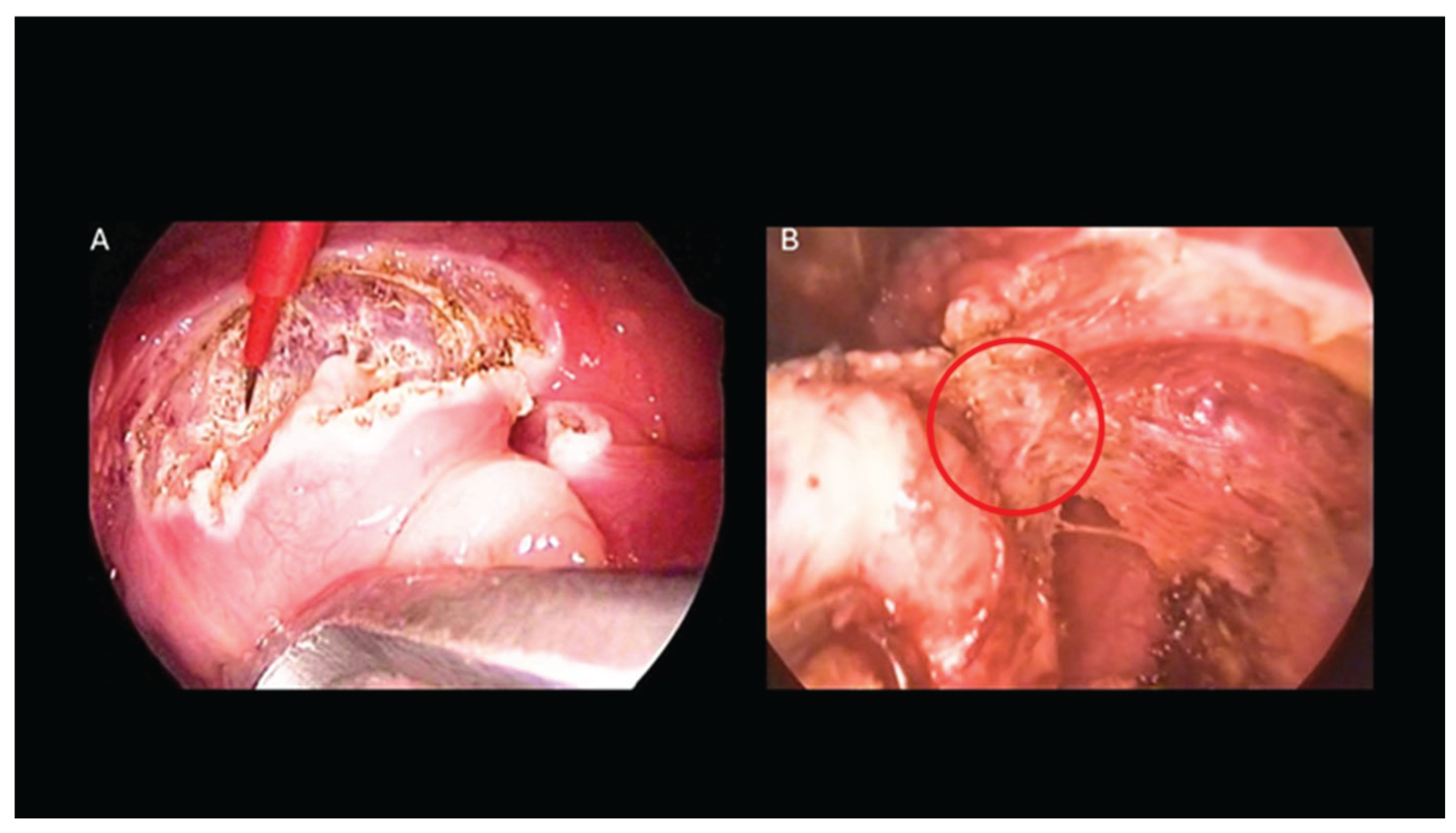
Figure 4.
Post-adenotonsillectomy hemorrhage rates and surgical revision rates: comparison between Sassuolo Hospital and the literature.
Figure 4.
Post-adenotonsillectomy hemorrhage rates and surgical revision rates: comparison between Sassuolo Hospital and the literature.
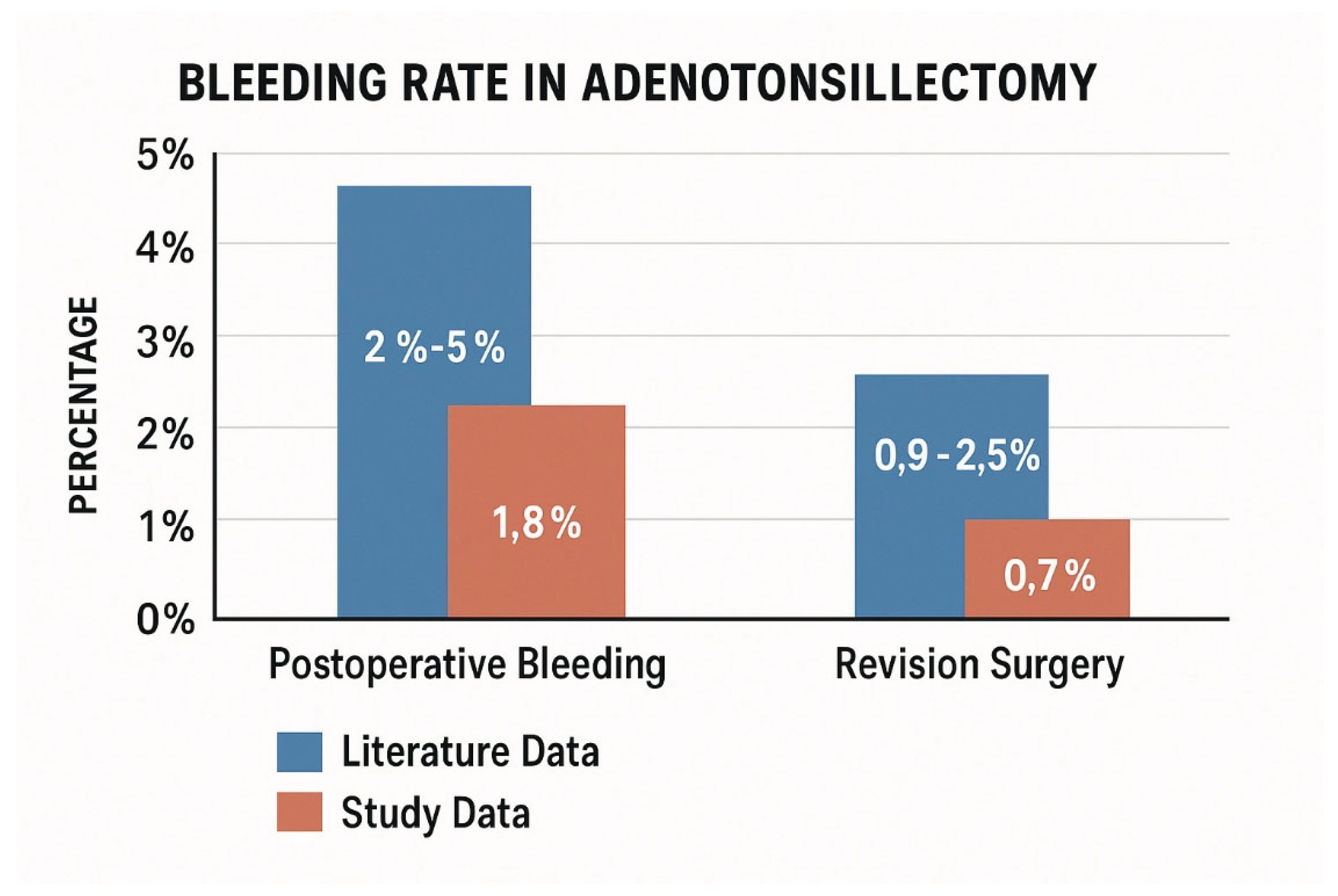

Table 1.
Postoperative hemorrhage requiring revision: stratification by anatomical origin (adenoidectomy vs tonsillectomy-related; OR vs tonsillectomy) and tonsillar technique (intracapsular vs extracapsular; OR vs extracapsular). ORs with 95% CI; χ2 test (p < 0.05 significant).
Table 1.
Postoperative hemorrhage requiring revision: stratification by anatomical origin (adenoidectomy vs tonsillectomy-related; OR vs tonsillectomy) and tonsillar technique (intracapsular vs extracapsular; OR vs extracapsular). ORs with 95% CI; χ2 test (p < 0.05 significant).
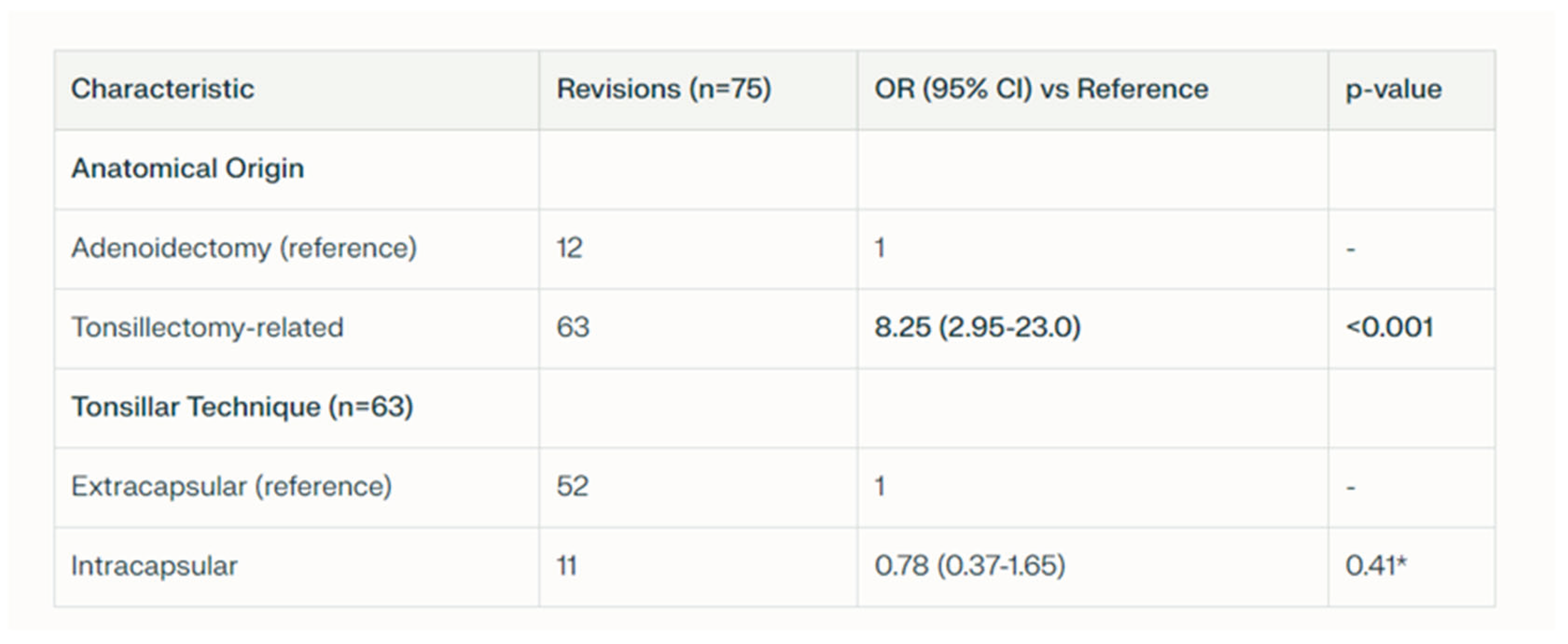 |
Table 2.
Postoperative hemorrhage stratification by surgical indication (recurrent tonsillitis vs OSA; OR vs OSA reference; otitis media vs OSA; OR vs OSA reference) and age group for surgical revisions (3-5 years vs >10 years; OR vs 10 years reference). ORs with 95% CI; χ2 test (p<0.05 significant).
Table 2.
Postoperative hemorrhage stratification by surgical indication (recurrent tonsillitis vs OSA; OR vs OSA reference; otitis media vs OSA; OR vs OSA reference) and age group for surgical revisions (3-5 years vs >10 years; OR vs 10 years reference). ORs with 95% CI; χ2 test (p<0.05 significant).
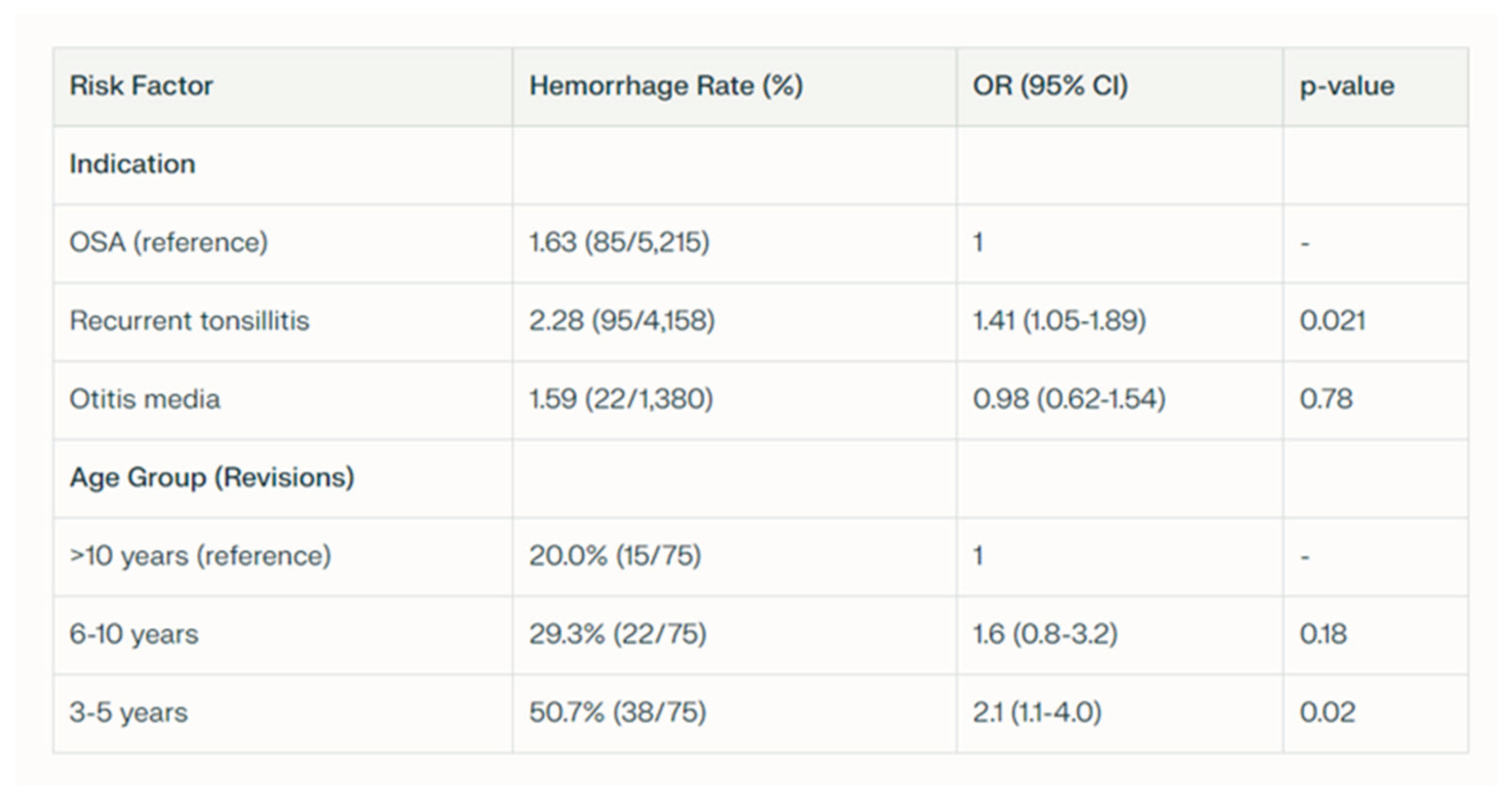 |
Table 3.
Comparative data between the Colorado microdissection and conventional electrocautery. Data compiled from published literature and institutional series.
Table 3.
Comparative data between the Colorado microdissection and conventional electrocautery. Data compiled from published literature and institutional series.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



