Submitted:
12 February 2026
Posted:
14 February 2026
You are already at the latest version
Abstract
Glaucoma treatment is undergoing a significant transformation. Traditionally, the therapy path followed a rigid progression from topical eye drops to invasive surgery. However, this 'step-ladder' approach often imposes a heavy physical and psychological burden on the patient. This review explores the emergence of next-generation pharmaceuticals and sustained-release systems as realistic alternatives to surgical intervention. The analysis focuses on three key areas: the development of dual-action molecules that restore physiological drainage, the introduction of biodegradable implants that ensure long-term stability, and the shift toward neuroprotective strategies. These advancements suggest that the potential of medical therapy is expanding, allowing for effective pressure control with fewer complications. While surgery remains essential for advanced cases, this work highlights a future where glaucoma can be addressed as a chronic condition through molecular precision, prioritizing the patient’s quality of life and long-term visual prognosis.
Keywords:
glaucoma therapy
; chemical surgery
; drug delivery systems
; sustained-release implants
; ROCK inhibitors
; neuroprotection
; intraocular pressure
; gene therapy
; precision medicine
1. Introduction
1.1. Definition and Pathogenesis
Traditionally, glaucoma has been defined primarily by the presence of elevated intraocular pressure (IOP). However, contemporary clinical understanding has shifted beyond this mechanical view, reclassifying the disease as a sophisticated group of progressive optic neuropathies. At its core, the pathology is defined by the selective degeneration of retinal ganglion cells (RGCs) and the gradual attrition of their axonal fibers. This structural decay leads to a characteristic remodeling of the optic nerve head, known as ‘cupping,’ which eventually manifests as irreversible deficits in the patient’s visual field [1]. While IOP remains the only modifiable risk factor, the pathogenesis of the disease is a multi-step molecular cascade. The transition from viewing glaucoma as a matter of ‘simple eye pressure’ to recognizing it as a complex neurodegenerative condition represents the core of modern research. The critical mechanisms involved can be summarized as follows:
The Mechanical and Vascular Theory: Initial damage often occurs at the lamina cribrosa, where mechanical stress from IOP or vascular hypoperfusion leads to axonal transport obstruction. This “traffic jam” prevents essential neurotrophic factors, such as Brain-Derived Neurotrophic Factor (BDNF), from reaching the RGC body, triggering a survival crisis [2].
Retinal Ganglion Cell (RGC) Apoptosis: The death of RGCs is the final common pathway, understood as a form of programmed cell death (apoptosis) mediated by the activation of caspases and pro-apoptotic BCL-2 family proteins. This process is frequently exacerbated by excitotoxicity—a toxic accumulation of glutamate in the extracellular space [3].
The “Energy Crisis” and Mitochondrial Dysfunction: Recent evidence describes glaucoma as a localized mitochondrial disease [4]. RGCs possess an extraordinary mitochondrial density to support long-distance axonal signaling. When these “cellular power plants” fail due to senescence or genetic predisposition, ATP production can drop significantly (by over 30%), leading to a surge in Reactive Oxygen Species (ROS) and oxidative stress, causing axonal “dying-back” degeneration [4,5].
Neuroinflammation and Glial Activation: Emerging evidence highlights the role of microglia and astrocytes. Once RGCs are stressed, these supporting cells shift to a pro-inflammatory phenotype, releasing cytokines such as TNF-alpha and IL-1beta, which exacerbate the neurodegenerative environment in a self-perpetuating cycle [6].
1.2. Epidemiological Trends and Global Impact
The epidemiological landscape of glaucoma in 2026 reveals a significant public health challenge. As the global population ages, the disease is transitioning from a clinical concern to a substantial socio-economic burden. Current estimates indicate that approximately 95 million people worldwide are living with glaucoma, a figure projected to reach 111.8 million by 2040 [7]. A critical hurdle remains the “diagnostic gap”; nearly 50% of cases in high-income countries are undiagnosed, a figure that exceeds 90% in low- and middle-income regions [8]. Regional and ethnic disparities further complicate this landscape. Primary Open-Angle Glaucoma (POAG) shows the highest prevalence in African populations (~4.2%), often following a more aggressive clinical course [7]. Conversely, Primary Angle-Closure Glaucoma (PACG) is disproportionately prevalent in East Asian populations, highlighting the necessity for ethnically tailored screening programs [9]. Beyond the clinical data, the economic impacts are substantial. The WHO estimates that global productivity loss due to vision impairment exceeds $411 billion annually [10]. In developing economies, late-stage glaucoma can consume 29% to 50% of a household’s income. This creates a “poverty trap” where the inability to afford treatment accelerates the onset of blindness [11].
1.2.1. Genetic and Demographic Risk Factors
Genetic and anatomical factors play a critical role in the clinical presentation of glaucoma. Ethnicity, in particular, significantly influences ocular anatomy. African populations exhibit a substantially higher Odds Ratio for POAG (OR 2.80) compared to Europeans. This increased risk is often linked to specific anatomical traits, such as thinner central corneal thickness and larger optic disc cups [12]. On the other hand, Primary Angle-Closure Glaucoma (PACG) predominates in East Asian populations due to anatomical precursors, including a shallower anterior chamber depth and a thicker, anteriorly positioned crystalline lens [9]. Gender dimorphism also shapes disease prevalence. Recent meta-analyses indicate that men are more susceptible to POAG, whereas women show a significantly higher incidence of PACG—approximately two to three times higher. This disparity is likely driven by smaller average ocular dimensions and hormonal influences on connective tissue remodeling [13]. The “Genomic Revolution” has further expanded our understanding beyond traditional mutations like MYOC (Myocilin). Genome-Wide Association Studies (GWAS) have identified complex loci that provide new targets for drug discovery. For POAG, identified genes include ABCA1 (lipid metabolism), AFAP1 (actin filament organization), and TXNRD2 (mitochondrial oxidative stress regulation) [14]. For PACG, mutations in EPDR1 and COL11A1 highlight the importance of structural protein integrity [15]. The integration of these markers into Polygenic Risk Scores (PRS) now allows for the identification of high-risk individuals decades before clinical symptoms emerge, paving the way for early intervention [16].
1.3. Patient Quality of Life and Family Impact
Beyond macro-economic statistics lies a profound human reality: glaucoma drastically compromises an individual’s independence. Recent evidence indicates that up to 40% of patients suffer from significant anxiety, while 20% experience clinical depression, prevalence rates nearly double those of the general population [17]. This psychological burden extends to caregivers, who often report high stress levels as they manage complex treatment schedules and witness the patient’s progressive loss of autonomy [18]. This review addresses a fundamental question: can we transcend the limitations of traditional surgery and the burden of daily eye drops to offer patients a future of stability and dignity? By exploring novel biochemical pathways and sustained-release delivery systems, the objective is not merely to reduce a numerical value on a tonometer, but to alleviate the profound psychological and functional weight that glaucoma places on millions of lives worldwide.
1.4. Current Challenges in Glaucoma Therapy
Despite the breadth of current treatment options, a persistent ‘therapeutic gap’ characterizes modern glaucoma management. This discrepancy arises from the difficulty of daily treatment adherence and the invasive nature of surgery. Topical therapy is frequently undermined by poor adherence. The need for lifelong, multiple daily instillations, often coupled with ‘drop-induced’ ocular surface toxicity, largely attributed to chronic exposure to preservatives such as Benzalkonium Chloride, generates a negative cycle. Patients often seek symptomatic relief by discontinuing their medication, unintentionally allowing the asymptomatic progression of the disease to continue unchecked(19,20). On the other hand, traditional filtration procedures, such as trabeculectomy, represent a challenging trade-off. While effective at lowering IOP, they carry significant risks of vision-threatening complications, including endophthalmitis, suprachoroidal hemorrhage, or chronic hypotony. Moreover, the long-term success of these interventions is frequently compromised by the eye’s aggressive wound-healing response. Subconjunctival fibrosis and scarring often obstruct the newly created drainage channels, leading to surgical failure and the need for complex revisions [21].
1.5. Future Directions in Glaucoma Therapy
This clinical impasse requires a significant change in treatment strategies. Current pharmacological innovation aims to achieve clinical outcomes that were previously only possible through invasive surgery. This transition is characterized by “biochemical remodeling”, which utilizes advanced molecules to restore physiological drainage without surgical trauma, and the development of sustained-release systems. These technologies are no longer merely experimental possibilities; they represent a clinical necessity for achieving stable, long-term intraocular pressure control, while minimizing the risks associated with traditional surgery. Ultimately, this shift aims to reduce the profound physiological and psychological stress that invasive interventions place on patients, prioritizing a therapeutic journey that preserves not only their sight but also their quality of life and peace of mind.

Table 1.
Comparison between Traditional and Modern Glaucoma Therapies.
| Feature | Traditional Paradigm | The New Era (Biochemical/Sustained) |
|---|---|---|
| Therapeutic Goal | Pressure Control: Reducing fluid or creating artificial drainage. | Functional Recovery: Restoring the natural physiology of the eye. |
| Treatment Burden | Patient-Dependent: Daily eye drops (risk of forgetfulness/error). | Physician-Led: Sustained-release implants (guaranteed adherence). |
| Action Mechanism | Mechanical Bypass: Often requires invasive surgery or “holes” (blebs). | Biochemical Remodeling: Targeted drugs (ROCK-i, NO) that “repair” the tissue. |
| Clinical Outcome | Fluctuating IOP and potential ocular surface damage. | Stable, long-term IOP control and improved Quality of Life. |
2. Pathophysiological Determinants of Aqueous Outflow Resistance
To evaluate the disruptive potential of next-generation pharmaceuticals, it is essential to delineate the mechanical and biochemical failures governing ocular fluid dynamics. Maintaining a stable intraocular pressure (IOP) is essential for the structural integrity and health of the eye. This pressure is regulated by a delicate balance between the continuous production of aqueous humor by the ciliary body and its subsequent drainage through specialized pathways. In a healthy eye, the aqueous humor flows from the posterior chamber, through the pupil, and into the anterior chamber. From there, it exits the eye primarily via two distinct routes: the conventional (trabecular) pathway and the unconventional (uveoscleral) pathway [22]. In glaucomatous eyes, the homeostatic regulation of the drainage apparatus is compromised. Modern therapeutic strategies are increasingly designed not merely for pressure reduction, but for the biological restoration of these specific physiological pathways [22].
2.1. Aqueous Humor Dynamics and Hydraulic Equilibrium
The eye maintains structural and functional integrity through a precise hydraulic balance. Aqueous Humor (AH) is continuously secreted by the non-pigmented ciliary epithelium and must be evacuated at a corresponding rate to maintain a physiological Intraocular Pressure (IOP), typically ranging between 10–21 mmHg [23]. In the majority of primary open-angle glaucoma (POAG) cases, the pathology is characterized by increased outflow resistance rather than aqueous hypersecretion. Consequently, pharmacological innovation has pivoted toward enhancing the efficiency of the “exhaust” system (drainage) rather than solely inhibiting the “faucet” (secretion) [24].
2.2. Resistance Mechanisms in the Conventional Outflow Pathway
The conventional drainage route, comprising the trabecular meshwork (TM) and Schlemm’s canal, is the primary regulator of intraocular pressure, handling approximately 80-90% of aqueous humor outflow. In a physiological state, the TM is not a static filter but a highly dynamic and contractile tissue that actively modulates resistance to fluid flow. In Primary Open-Angle Glaucoma (POAG), however, this tissue undergoes a pathological transformation akin to fibrosis. This process is characterized by the excessive accumulation of extracellular matrix (ECM) and a marked ‘stiffening’ of the cellular cytoskeleton. This structural rigidity is largely governed by the Rho/Rho-associated protein kinase (ROCK) signaling pathway [25]. This biomechanical shift is the specific focus of modern pharmacological intervention. ROCK inhibitors work by antagonizing this signaling pathway, effectively inducing relaxation within the TM cytoskeleton. By reversing this cellular stiffness, these agents enhance the permeability of the trabecular lamellae, thereby restoring the eye’s natural fluid dynamics and facilitating effective pressure reduction [26].
2.3. The Uveoscleral Route as an Alternative Outflow Pathway
The uveoscleral pathway is a pressure-independent route where aqueous humor flows through the ciliary muscle into the suprachoroidal space. Historically regarded as a secondary exit, this pathway has become a cornerstone of pharmacological intervention. Traditional Prostaglandin Analogues (PGAs) primarily target this route; they lower intraocular pressure by stimulating matrix metalloproteinases, which remodel the interstitial collagen and reduce flow resistance [27]. However, the therapeutic landscape has been redefined by the emergence of Nitric Oxide (NO) donors. These next-generation molecules utilize a sophisticated dual-action mechanism: they not only enhance uveoscleral drainage but also actively relax the trabecular meshwork. This dual approach provides a comprehensive ‘cleansing’ of both primary drainage systems, offering a more holistic management of ocular fluid dynamics [28].
2.4. Distal Outflow and Post-Trabecular Resistance
Emerging research suggests that glaucoma-related resistance is not confined to the trabecular meshwork alone. Significant obstruction also occurs downstream, specifically within the collector channels and the episcleral veins [29]. This distal resistance is a critical clinical factor, as it may explain why some patients fail to respond adequately to conventional topical therapies. Furthermore, the existence of post-trabecular resistance provides a strong physiological rationale for the use of sustained-release implants. Unlike the ‘pulsatile’ delivery of standard eye drops—which leads to significant fluctuations in drug concentration—sustained-release systems maintain a constant, steady-state therapeutic level. This continuous presence allows for a more effective ‘flushing’ of the entire distal apparatus, ensuring that the pharmacological effect reaches the deepest components of the drainage system more consistently than traditional methods [30].
3. Advances in Outflow Restoration and Aqueous Suppression
The progression from conventional treatments to next-generation glaucoma pharmaceuticals represents a profound evolution in the scientific approach to the disease. For several decades, the primary therapeutic objective was the suppression of aqueous humor production to lower intraocular pressure. However, contemporary research has steered the field toward a more restorative paradigm. Rather than merely reducing fluid inflow, modern strategies prioritize the rehabilitation of the eye’s natural drainage architecture, seeking to recover its biological and mechanical functionality [31].
3.1. Aqueous Humor Suppression Models
Conventional pharmacotherapy has historically relied on an ‘inhibitory’ model. Traditional compounds, most notably β-blockers and Carbonic Anhydrase Inhibitors (CAIs), achieve intraocular pressure reduction by suppressing the secretory functions of the ciliary body. In essence, these agents modulate fluid inflow as a compensatory measure for a compromised drainage apparatus, rather than repairing the outflow pathways themselves [32].
For decades, Timolol has represented the clinical benchmark for this approach. Its pharmacological efficacy is rooted in the specific (S)-configuration of its propanolamine side chain, which enables the antagonism of β1 and β2 adrenoceptors within the ciliary epithelium. This interaction inhibits the production of cyclic adenosine monophosphate (cAMP), thereby decreasing the secretion of aqueous humor [33]. However, a significant limitation persists: while these medications are highly effective at lowering manometric pressure, they do not mitigate the underlying fibrosis or the progressive resistance within the trabecular meshwork. Consequently, the primary structural pathology of glaucoma remains largely unaddressed.
3.2. Pharmacological Restoration of the Trabecular Meshwork
The contemporary pharmacological strategy has moved beyond simple fluid suppression, shifting its focus toward the enhancement of physiological outflow. By specifically targeting the cellular cytoskeleton within the trabecular meshwork (TM), these modern molecules aim to restore the functional integrity of the conventional drainage route, addressing the core of the pathology.
3.2.1. Netarsudil and Soft Drug Metabolism (ROCK Inhibitors)
Netarsudil represents a significant paradigm shift as a highly selective inhibitor of Rho-associated protein kinase (ROCK) [34]. At a molecular level, Netarsudil competitively inhibits the ROCK enzyme by mimicking the purine ring of ATP. This interaction facilitates the dephosphorylation of the myosin light chain, which in turn induces a profound relaxation of the actin-myosin stress fibers within the TM cells [35]. A key innovation of Netarsudil is its ‘Soft Drug’ design. By incorporating a strategic ester bond, the molecule is engineered for rapid hydrolysis by local ocular esterases into its active metabolite upon instillation. This metabolic pathway ensures high local potency within the eye while significantly reducing systemic exposure, thereby mitigating potential cardiovascular or respiratory complications often associated with older glaucoma medications [34,36].
3.2.2. Latanoprostene Bunod and Dual-Action Mechanisms (NO-Donating PGA)
Latanoprostene bunod stands as one of the most sophisticated examples of modern medicinal chemistry. It is a single-molecule entity designed to release two distinct active components through targeted enzymatic cleavage. The first component, latanoprost acid, activates prostanoid FP receptors to remodel the extracellular matrix (ECM) of the ciliary muscle, thereby increasing uveoscleral drainage. Simultaneously, the second component, the butanediol mononitrate, acts as a Nitric Oxide (NO) donor. The released NO activates the soluble guanylyl cyclase–cyclic guanosine monophosphate (sGC-cGMP) pathway, inducing relaxation in both the TM and Schlemm’s canal to reduce conventional outflow resistance(37,38).
3.2.3. Synergistic Clinical Advantages
The primary clinical advantage of LBN lies in its ability to address outflow resistance from two distinct anatomical fronts. By providing a synergistic effect that enhances both conventional and unconventional pathways, LBN achieves an IOP-lowering potency that rivals certain Micro-Invasive Glaucoma Surgeries (MIGS) [39]. This ability to deliver surgical-grade efficacy through a non-invasive, once-daily topical application represents a significant advancement in patient compliance, offering a robust pharmacological alternative for patients who would otherwise require surgical intervention.
3.3. Comparative Pharmaco-Chemistry of Glaucoma Therapeutics
3.4. Neuroprotection and Mitochondrial Bioenergetics in Glaucoma
Beyond the regulation of intraocular pressure, recent pharmaceutical research has focused on the direct protection of the optic nerve. As the study of the metabolic ‘energy crisis’ in Retinal Ganglion Cells (RGCs) progresses, the therapeutic objective is expanding to include neuroprotection: the preservation of neuronal health regardless of IOP levels [40].
3.4.1. Targeting the Mitochondrial “Power Failure”
RGCs have a very high metabolic demand, which makes them sensitive to energy shortages. In glaucoma, mitochondrial failure leads to a decrease in ATP production and an increase in Reactive Oxygen Species (ROS) [41]. New experimental agents aim to stabilize the mitochondria and improve the efficiency of the electron transport chain. By preventing the release of Cytochrome c, these molecules attempt to block the apoptotic process before the nerve fibers are permanently lost [42].
Another practical approach involves ‘metabolic refueling’. Research into Nicotinamide (Vitamin B3) and Pyruvate as NAD+ precursors suggests that these substances can help RGCs resist pressure-induced stress by providing a functional energy reserve [43].
3.4.2. Glutamate Excitotoxicity and Axonal Transport
Glaucoma is also associated with an accumulation of glutamate, which causes cell death through the overstimulation of NMDA receptors. New molecular strategies act as NMDA receptor antagonists or help restore the transport of essential proteins (like dynein and kinesin) along the axon. This helps maintain the flow of neurotrophins, such as BDNF, which are necessary for neuronal survival [44].
3.4.3. “Pressure-Independent” Therapy
This approach is particularly important for ‘Normal-Tension Glaucoma’ or for patients whose vision worsens even when their pressure is low. Neuroprotective molecules target the neurodegenerative process itself, moving the focus from simply lowering a number on the tonometer to actively saving the cells responsible for vision [45].
4. New Drug Delivery Systems in Glaucoma
The clinical efficacy of any pharmacological agent is strictly limited by its bioavailability and the consistency of its administration. In glaucoma, the “therapeutic gap” is often a result of poor patient adherence and the physiological barriers of the ocular surface. Sustained-release (SR) technology seeks to bypass these variables through bioengineering [46].
4.1. PLGA-Based Sustained Release Systems
The design of modern intracameral implants is based on the use of Poly-(lactic-co-glycolic acid) (PLGA), a biocompatible copolymer. The core advantage of this material is its predictable degradation profile. Through a process of non-enzymatic hydrolytic de-esterification, the PLGA matrix gradually breaks down into lactic and glycolic acid monomers, which are naturally metabolized by the body [47]. The drug release is governed by specific diffusion-dissolution kinetics. While traditional eye drops cause ‘peaks and valleys’ in medication levels, PLGA-based implants aim for Zero-Order Kinetics. This ensures that a steady concentration of the active molecule is maintained in the aqueous humor for several months. By providing a constant supply of the drug, the system optimizes receptor occupancy and avoids the fluctuations that often lead to sub-optimal pressure control [48]. This ensures a steady-state concentration of the active molecule in the aqueous humor, optimizing receptor occupancy over an extended duration, typically ranging from 4 to 6 months.
4.2. Clinical Application and Structural Remodeling of Bimatoprost SR
The most prominent application of sustained-release drug delivery systems is the Bimatoprost SR (Durysta) implant, which contains 10 µg of active drug within its polymer matrix. From a pharmacokinetic perspective, the primary advantage is the direct delivery into the anterior chamber. By bypassing the corneal barrier, the system achieves therapeutic concentrations at the target tissues—specifically the ciliary muscle and the trabecular meshwork—using a significantly lower total dose compared to daily topical administration [49]. A particularly compelling finding from the Phase III clinical trials (ARTEMIS) is the sustained effect of the treatment. Data showed that intraocular pressure reduction often persisted well beyond the four-month mark, even after the polymer had completely resorbed [50].This has led to the ‘remodeling hypothesis’: the idea that continuous, steady-state receptor stimulation may induce long-term structural changes in the outflow pathways. If confirmed, this suggests that sustained-release therapy does not just manage pressure, but could potentially alter the natural progression of glaucoma [51].
4.3. Alternative Delivery Strategies: Punctal Plugs, Lenses, and Nanotechnology
Beyond intracameral injections, other bioengineering strategies are expanding the landscape of non-invasive drug delivery. The goal of these technologies is to increase the residence time of the drug on the ocular surface while reducing systemic side effects. One approach involves Punctal Plug Delivery Systems (PPDS). These devices are inserted into the lacrimal puncta and utilize a drug-infused core (e.g., Travoprost) within a silicone shell. This system provides a continuous elution of the medication onto the tear film and significantly reduces the systemic absorption typically associated with the nasolacrimal duct [52]. A more advanced pharmaceutical application is the use of Molecularly Imprinted Contact Lenses. This technology involves creating specific macromolecular ‘cavities’ within a hydrogel matrix that match the spatial and electrostatic profile of a drug molecule, such as Timolol. This structural affinity ensures a higher loading capacity and a more controlled release compared to conventional ‘soak-and-release’ methods [53]. Finally, Nanoparticle-Mediated Delivery represents a major shift in drug transport. The use of liposomes, dendrimers, or polymeric nanoparticles allows for the encapsulation of hydrophobic molecules. These carriers facilitate targeted penetration through the lipophilic corneal epithelium while protecting the drug from enzymatic degradation in the precorneal tear film [54,55].
5. Comparative Efficacy of Pharmacotherapy and Surgical Intervention
The standard therapeutic procedure for glaucoma is currently being re-evaluated. By tradition, surgery was reserved as a final, definitive step only after the failure of topical medical therapy. However, the introduction of next-generation pharmaceuticals and sustained-release systems is changing this rigid distinction [56].
5.1. Safety Profiles and the Fibrotic Response
A major limitation of incisional surgery, such as trabeculectomy, is the unpredictable subconjunctival wound-healing response. Surgical failure is often driven by fibrosis, which typically requires the use of antimetabolites like Mitomycin-C (MMC) during the procedure. Although MMC helps maintain the patency of the filtration bleb, it carries significant iatrogenic risks. These include chronic hypotony, the formation of fragile cystic blebs, and a lifelong risk of endophthalmitis [57]. In contrast, pharmacological innovation offers a less invasive alternative through ‘biochemical remodeling’. Molecules such as ROCK inhibitors and NO-donors target the same outflow resistance as surgery but act via intracellular signaling pathways (e.g., sGC-cGMP). By modulating the trabecular meshwork at the molecular level, these drugs avoid the mechanical trauma and subsequent scarring associated with filtering procedures. This approach aims to restore physiological drainage without the complications of external surgical wounding(58,59).
5.2. “Chemical Surgery” vs. Micro-Invasive Procedures (MIGS)
Micro-Invasive Glaucoma Surgery (MIGS) has significantly improved the safety of surgical interventions. However, these procedures still require intraocular entry and a sterile operating room environment.
In this context, sustained-release (SR) implants like Bimatoprost SR represent a strategic ‘middle ground,’ often defined as ‘Chemical Surgery’. These systems are administered via a minimally invasive intracameral injection in a clinical setting rather than a surgical suite. They can achieve intraocular pressure (IOP) stabilization comparable to some surgical outcomes, but without the risks associated with permanent intraocular hardware or filtration blebs [60]. For patients with early-to-moderate glaucoma who do not require cataract surgery, pharmacological SR systems offer a powerful alternative to standalone MIGS (such as iStent or Hydrus). This approach effectively delays the need for intraocular implants while maintaining stable therapeutic levels. By bridging the gap between traditional drops and surgery, ‘chemical surgery’ prioritizes patient safety and procedural simplicity [61].
5.3. Synthesis of Clinical Efficacy Outcomes
To evaluate the effectiveness of next-generation pharmaceuticals as a viable alternative to traditional therapies, it is necessary to analyze the data from pivotal Phase III clinical trials. These studies provide a direct comparison between sustained-release systems and current gold standards, such as daily topical prostaglandins. Table 3 summarizes the clinical efficacy, safety profiles, and duration of action for the most significant recent advancements in the field.
5.4. Discussion
The clinical results from the MERCURY and ARTEMIS trials show a significant increase in therapeutic potential. A pressure reduction of 9–10 mmHg is very close to the results typically obtained with MIGS procedures. In fact, MIGS generally provides an additional reduction of only 2–4 mmHg when compared to cataract surgery alone. These findings suggest that the maximum efficacy of medical treatment has increased significantly. For many patients, these new pharmacological options can delay the need for surgery for several years. This delay is clinically important because it protects the health of the conjunctiva and the ocular surface. Maintaining these tissues in good condition is essential if surgical intervention becomes necessary in the future.
6. Future Perspectives in Molecular Therapeutics
The treatment of glaucoma is shifting from a purely reactive approach, focused only on intraocular pressure, to a proactive strategy based on biological restoration. The evidence suggests that the distinction between medical and surgical intervention is becoming less rigid. This evolution is driven by three main pillars of innovation. First, advanced drug delivery systems ensure stable therapeutic levels over time. Second, new molecules target the biological causes of outflow resistance rather than just the symptoms. Finally, the focus is expanding to include the direct protection and regeneration of the optic nerve. Together, these advancements aim to provide a more personalized treatment that prioritizes the long-term preservation of visual function [66].
6.1. Polygenic Risk Scores and Targeted Therapy
The potential of pharmaceuticals to replace surgery depends on the integration of Polygenic Risk Scores (PRS) into clinical practice. This genetic profiling allows for a more targeted therapeutic approach. Future research aims to identify specific genetic loci, such as ABCA1 or TXNRD2, to predict how an individual will respond to a specific drug. This ‘genotype-directed’ therapy matches biochemical treatments to the patient’s unique molecular profile [67]. From a clinical perspective, genomic profiling will help identify ‘rapid progressors’ at the time of diagnosis. For these high-risk patients, starting treatment with potent sustained-release systems, such as ROCK inhibitors, could significantly change the course of the disease. This proactive strategy could eliminate the need for invasive filtration surgery in the future by stabilizing the condition early on [68].
6.2. Neuroprotection and Neuro-Regeneration
While regulating intraocular pressure is the primary clinical objective, the long-term stabilization of the optic nerve requires direct intervention on the neurons. This approach focuses on protecting and potentially repairing Retinal Ganglion Cells (RGCs) through molecular strategies. One key area of research involves mitochondrial rescue. Future molecules are being developed to target the mitochondrial permeability transition pore (mPTP). By stabilizing the energy production of RGCs, these agents act as a molecular safeguard. This helps preserve visual function even when the patient experiences fluctuations in intraocular pressure [69]. The next step beyond protection is neuro-regeneration. Recent studies on the mTOR (mammalian target of rapamycin) signaling pathway and PTEN inhibition have shown promising results. These biological pathways could be used to chemically stimulate the regrowth of damaged axons. Although once considered impossible in the central nervous system, these advancements suggest that repairing the optic nerve is a realistic future objective [70,71].
6.3. Gene Therapy and Sustained Biological Modulation
Viral-vector mediated gene therapy represents a significant alternative to conventional surgery. This approach uses Adeno-Associated Virus (AAV) vectors to deliver therapeutic transgenes directly to the ciliary body or the trabecular meshwork. The goal is to induce long-term changes in ocular fluid dynamics at a genetic level [72]. Several innovative strategies are currently under investigation. For example, the over-expression of matrix metalloproteinases can be used to enhance aqueous outflow. Additionally, CRISPR-based techniques can target and silence specific enzymes responsible for aqueous production. These methods address the problem of patient compliance by effectively turning ocular tissues into a self-regulating source of therapeutic action. This strategy could provide a definitive solution for intraocular pressure control without the need for daily medication or invasive filtration blebs [73].
7. Conclusion
The transition from mechanical surgery toward the biochemical restoration of ocular drainage marks a significant evolution in ophthalmology. This review shows that modern pharmaceuticals are no longer just temporary measures. Instead, this work explores how new pharmacological strategies can offer less invasive alternatives for patients, potentially reducing the need for traditional surgery, which nevertheless remains a fundamental tool.
The evidence discussed highlights two main advancements:
- Pathophysiological Precision: New molecules, such as dual-action agents and tissue-remodeling drugs, target the cellular causes of glaucoma, including trabecular stiffening. This molecular approach addresses the underlying pathology with a level of precision that incisional surgery cannot achieve [74].
- Stability and Safety: Sustained-release technologies, such as PLGA implants, have effectively bridged the gap between drops and surgery. These systems provide long-term pressure stabilization without the iatrogenic trauma, scarring, or infection risks often associated with filtering procedures [75].
In conclusion, while surgery remains essential for refractory cases, the continuous advancement of pharmacology suggests a future where glaucoma can be managed increasingly as a non-surgical condition. By focusing on molecular targets and sustained delivery systems, it is possible to improve the safety profile and quality of life for patients, preserving their long-term visual prognosis through more tolerable means.
Glossary of Terms
- AAV (Adeno-Associated Virus): Viral vectors employed in gene therapy to deliver genetic material into specific ocular target cells.
- AH (Aqueous Humor): The transparent fluid filling the anterior and posterior chambers of the eye, essential for maintaining intraocular pressure.
- BDNF: Brain-Derived Neurotrophic Factor.
- Biochemical Remodeling: The pharmacological modification of the trabecular meshwork’s molecular structure to enhance fluid permeability.
- CAIs (Carbonic Anhydrase Inhibitors): A class of medications that reduce aqueous humor production by inhibiting the enzyme carbonic anhydrase.
- CRISPR: A genome-editing technology utilized for precise modification or silencing of genes involved in glaucoma pathophysiology.
- ECM (Extracellular Matrix): The non-cellular component of the trabecular meshwork; its accumulation increases outflow resistance.
- IOP (Intraocular Pressure): The internal fluid pressure of the eye, expressed in millimeters of mercury (mmHg).
- LBN (Latanoprostene Bunod): A dual-action prostaglandin analog and nitric oxide (NO) donor.
- MIGS (Micro-Invasive Glaucoma Surgery): Surgical procedures utilizing microscopic devices to enhance outflow with minimal tissue disruption.
- mPTP (Mitochondrial Permeability Transition Pore): A protein pore in the mitochondrial membrane; its regulation is a key target for neuroprotection.
- mTOR (mammalian Target of Rapamycin): A protein kinase that regulates cell growth and survival, involved in RGC regenerative pathways.
- Nitric Oxide (NO) Donors: Molecules that release NO to induce trabecular meshwork relaxation and enhance aqueous drainage.
- Neuroprotection: Therapeutic strategies aimed at preserving Retinal Ganglion Cells (RGCs) independent of IOP reduction.
- NTG: Normal-Tension Glaucoma
- PACG / POAG: Primary Angle-Closure Glaucoma and Primary Open-Angle Glaucoma, respectively.
- PLGA [Poly (lactic-co-glycolic acid)]: A biocompatible and biodegradable polymer used as a matrix for sustained-release drug delivery.
- PPDS (Persistent Pigment Dispersion Syndrome): A condition where pigment granules flake off the iris, potentially obstructing the trabecular meshwork.
- PRS (Polygenic Risk Score): A numerical estimate of genetic predisposition to glaucoma based on the analysis of multiple genetic variants.
- RGCs (Retinal Ganglion Cells): The retinal neurons that transmit visual information to the brain; their loss is the hallmark of glaucomatous optic neuropathy.
- ROCK Inhibitors (Rho-kinase Inhibitors): Agents that modulate the cytoskeleton of trabecular cells, reducing tissue stiffness to facilitate outflow.
- sGC-cGMP: The signaling pathway (soluble Guanylate Cyclase) through which Nitric Oxide exerts its vasorelaxant and outflow-enhancing effects.
- Sustained-Release (SR) Systems: Long-acting delivery platforms designed for continuous therapeutic release, bypassing daily adherence issues.
- TM (Trabecular Meshwork): The specialized tissue in the anterior chamber angle responsible for the majority of aqueous humor drainage.
- Uveoscleral Pathway: The alternative (non-conventional) route for aqueous humor outflow through the ciliary body and suprachoroidal space.
References
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: a review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef]
- Quigley, H.A. Glaucoma: a neurodegenerative disease of the optic nerve. Prog Retin Eye Res. 2024, 98, 101–115. [Google Scholar]
- Calkins, D.J. Adaptive Mechanisms of Resistance and Resilience in Glaucoma. Annu Rev Vis Sci. 2021, 7, 447–472. [Google Scholar]
- Sacchi, M.; et al. Mitochondrial dysfunction and the “Energy Crisis” in Retinal Ganglion Cells: New therapeutic targets for 2025. Prog Retin Eye Res. 2025, 104, 101–128. [Google Scholar]
- Osborne, N.N.; et al. Mitochondrial dysfunction as a cause of optic nerve disorders. Prog Retin Eye Res. 2004, 23, 91–140. [Google Scholar]
- Liddelow, S.A.; et al. Neurotoxic reactive astrocytes are induced by activated microglia. Nature 2017, 541, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Tham, YC; Li, X; Wong, T.; et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Vision; World Health Organization: Geneva, 2019. [Google Scholar]
- Cheng, J.W.; et al. Epidemiology of primary angle-closure glaucoma in East Asian populations: A 2025 update. Lancet Glob Health 2025, 13, e88–e99. [Google Scholar]
- Burton, M.J.; et al. The Lancet Global Health Commission on Global Eye Health: vision for the future. Lancet Glob Health 2021, 9, e489–e551. [Google Scholar]
- Resnikoff, S.; et al. The economic burden of vision loss and blindness: a global analysis. Bull World Health Organ. 2024, 102, 145–154. [Google Scholar]
- Hoffman, M.J.; et al. Central corneal thickness and glaucoma risk in African populations. Am J Ophthalmol. 2023, 248, 12–20. [Google Scholar]
- Vajaranant, T.S.; et al. Gender differences in glaucoma: what we know and what we need to know. Curr Opin Ophthalmol. 2021, 32, 102–110. [Google Scholar]
- Gharahkhani, P.; et al. Genome-wide meta-analysis identifies 127 loci associated with intraocular pressure and glaucoma risk. Nat Commun. 2021, 12, 3468. [Google Scholar] [CrossRef]
- Khor, C.C.; et al. Genome-wide association study identifies five new susceptibility loci for primary angle-closure glaucoma. Nat Genet. 2016, 48, 556–562. [Google Scholar] [CrossRef]
- Craig, J.E.; et al. Multitrait analysis of glaucoma identifies over 100 risk loci and modulates polygenic risk score for glaucoma. Nat Genet. 2020, 52, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; et al. Anxiety and depression in patients with glaucoma: a systematic review and meta-analysis. Ophthalmology 2024, 131, 450–462. [Google Scholar]
- Bhorade, A.; et al. The impact of glaucoma on caregivers: A comprehensive review of family burden. J Glaucoma 2023, 32, 741–750. [Google Scholar]
- Newman-Casey, P.A.; et al. The barriers to and facilitators of glaucoma medication adherence: a systematic review. J Glaucoma 2025, 34, 22–35. [Google Scholar]
- Pisella, P.; et al. Prevalence of ocular surface disease in glaucoma patients using preserved drops. Ocul Surf. 2024, 22, 115–122. [Google Scholar]
- Cordeiro, M.F.; et al. The scarring response in glaucoma surgery: Molecular mechanisms and potential therapies. Br J Ophthalmol. 2025, 109, 310–318. [Google Scholar]
- Goel, M.; et al. Aqueous humor dynamics: a review. Open Ophthalmol J. 2010, 4, 52–59. [Google Scholar] [CrossRef]
- Brubaker, R.F. Targeting outflow facility in glaucoma management. Invest Ophthalmol Vis Sci. 2017, 58, BIO1–BIO10. [Google Scholar] [CrossRef]
- Stamer, W.D.; Clark, A.F. The many faces of the trabecular meshwork cell. Exp Eye Res. 2017, 158, 112–123. [Google Scholar] [CrossRef]
- Buffault, J.; et al. The Rho pathway as a therapeutic target in glaucoma: a review. J Clin Med. 2024, 13, 742. [Google Scholar]
- Tanna, A.P.; Johnson, M. Rho Kinase Inhibitors as a Novel Treatment for Glaucoma and Ocular Hypertension. Ophthalmology 2018, 125, 1741–1756. [Google Scholar] [CrossRef]
- Winkler, N.S.; Fautsch, M.P. Effects of prostaglandin analogues on aqueous humor outflow pathways. J Ocul Pharmacol Ther. 2024, 40, 15–28. [Google Scholar] [CrossRef]
- Krauthammer, M.; et al. Nitric Oxide-Donating Compounds in Glaucoma: A Biological and Clinical Perspective. Drugs Aging 2025, 42, 105–118. [Google Scholar]
- Vahabzadeh-Hagh, A.; et al. Distal Outflow Resistance in Glaucoma: The Final Frontier. Curr Glaucoma Pract. 2024, 18, 1–9. [Google Scholar]
- Kuchtey, J.; Kuchtey, R. The genetics and biology of the distal aqueous outflow tract. Exp Eye Res. 2025, 241, 109–122. [Google Scholar]
- Vinciguerra, R.; et al. The evolution of glaucoma pharmacology: From production inhibitors to outflow restorers. Expert Opin Pharmacother. 2024, 25, 145–158. [Google Scholar]
- Aronie, A.; et al. Carbonic anhydrase inhibitors in glaucoma: a contemporary review. J Ocul Pharmacol Ther. 2023, 39, 521–534. [Google Scholar]
- Kaufman, P.L. Timolol and the ciliary body: historical and molecular perspectives. Arch Ophthalmol. 2011, 129, 1351. [Google Scholar]
- Guzman-Aranguez, A.; et al. Rho-kinase inhibitors in glaucoma therapeutics. Prog Retin Eye Res. 2023, 94, 101135. [Google Scholar]
- Sturdivant, J.M.; et al. Discovery of Netarsudil (AR-13324): A Potent Rho Kinase Inhibitor for the Treatment of Glaucoma. ACS Med Chem Lett. 2016, 7, 962–966. [Google Scholar]
- Lin, C; others. Netarsudil (Rhopressa) as a soft drug: metabolic profile and safety considerations. Ocul Pharmacol. 2024, 15, 210–225. [Google Scholar]
- Krauthammer, M.; et al. Latanoprostene Bunod: A Dual-Action NO-Donating Prostaglandin Analog. Drugs 2024, 84, 45–62. [Google Scholar]
- Cavet, M; others. Nitric oxide (NO): an emerging target for glaucoma therapy. Invest Ophthalmol Vis Sci. 2025, 66, 12. [Google Scholar]
- Weinreb, R.N.; et al. Latanoprostene Bunod 0.024% vs Latanoprost 0.005% in Ocular Hypertension or Open-Angle Glaucoma: The APOLLO Study. Ophthalmology 2016, 123, 965–973. [Google Scholar] [CrossRef]
- Calkins, D.J. Neuroprotection in Glaucoma: The Next Frontier. Annu Rev Vis Sci. 2025, 11, 215–238. [Google Scholar]
- Chrysostomou, V.; et al. Mitochondrial dysfunction in glaucoma and the potential for NAD+ supplementation. Cells 2024, 13, 312. [Google Scholar]
- Crowston, J.; et al. Targeting mitochondrial bioenergetics for neuroprotection in glaucoma. Nat Rev Neurol. 2025, 21, 156–172. [Google Scholar]
- Hui, F; others. Improvement in inner retinal function with nicotinamide in glaucoma: A crossover randomized clinical trial. Clin Experiment Ophthalmol. 2020, 48, 903–914. [Google Scholar] [CrossRef] [PubMed]
- Sacca, S.; et al. Glutamate excitotoxicity and neuroinflammation in glaucoma. Int J Mol Sci. 2024, 25, 988. [Google Scholar]
- Sena, D.; Lindsley, K. Neuroprotection for treatment of glaucoma in adults. Cochrane Database Syst Rev. 2024, 1, CD006539. [Google Scholar]
- Awwad, S.; et al. Principles of drug delivery to the eye. Adv Drug Deliv Rev. 2024, 204, 115–132. [Google Scholar]
- Makadia, H.; Siegel, S. Poly Lactic-co-Glycolic Acid (PLGA) as Biodegradable Controlled Drug Delivery Carrier. Polymers 2011, 3, 1377–1397. [Google Scholar] [CrossRef]
- Varshney, S.; et al. Zero-order release kinetics in ocular drug delivery: Challenges and opportunities. J Controlled Release 2025, 378, 45–59. [Google Scholar]
- Seal, J.; et al. Pharmacokinetics of Intracameral Bimatoprost Sustained-Release Implant. J Ocul Pharmacol Ther. 2020, 36, 98–103. [Google Scholar]
- Bacharach, J; Torkian, P; Mansouri, K; Weinreb, R.N.; et al. Bimatoprost intracameral implant in patients with open-angle glaucoma or ocular hypertension: outcomes from the 20-month phase 3 ARTEMIS 1 study. Ophthalmology 2020, 127, 1627–1639. [Google Scholar]
- Lewis, R.; et al. Long-term IOP Control After Bimatoprost SR: The Role of Tissue Remodeling. Curr Opin Ophthalmol. 2024, 35, 120–128. [Google Scholar]
- Yellepeddi, V.; et al. Recent developments in punctal plug drug delivery systems. Expert Opin Drug Deliv. 2023, 20, 511–524. [Google Scholar]
- Alvarez-Lorenzo, C.; Concheiro, A. Molecularly imprinted polymers for drug delivery. J Chromatogr B 2024, 1232, 123–140. [Google Scholar] [CrossRef]
- Gote, V.; et al. Nanoparticles for Ocular Drug Delivery: A Perspective on Recent Advances. Pharmaceutics 2025, 17, 88. [Google Scholar]
- Varela-Fernández, R.; et al. Drug delivery to the anterior segment of the eye: A review of current and future technologies. Pharmaceutics 2023, 15, 612. [Google Scholar]
- Vold, S.; et al. Interventional Glaucoma: A New Paradigm in Patient Care. J Glaucoma 2024, 33, 1–10. [Google Scholar]
- Kirwan, J.; et al. Trabeculectomy: outcomes and complications. Curr Opin Ophthalmol. 2023, 34, 112–118. [Google Scholar]
- Schuman, J.; et al. The future of glaucoma therapy: biochemical remodeling versus mechanical filtration. Am J Ophthalmol. 2025, 260, 45–58. [Google Scholar]
- Chowdhury, U.; et al. Nitric oxide signaling in the trabecular meshwork: implications for glaucoma. Invest Ophthalmol Vis Sci. 2024, 65, 18. [Google Scholar]
- Bacharach, J.; et al. Sustained-release implants: a new era in glaucoma management. Ophthalmol Glaucoma 2024, 7, 145–156. [Google Scholar]
- Lavia, C.; et al. MIGS versus sustained-release implants: a comparative review of efficacy and safety. Eye 2025, 39, 22–34. [Google Scholar]
- Serle, J.; et al. Two Phase 3 Clinical Trials Comparing Netarsudil with Timolol. Am J Ophthalmol. 2018, 186, 116–127. [Google Scholar] [CrossRef]
- Asrani, S.; et al. Netarsudil/Latanoprost Fixed-Dose Combination for Elevation of IOP: The MERCURY Trials. Am J Ophthalmol. 2020, 210, 149–159. [Google Scholar]
- Weinreb, R.N.; et al. APOLLO Study: Latanoprostene Bunod 0.024% versus Latanoprost 0.005%. Ophthalmology 2016, 123, 965–973. [Google Scholar] [CrossRef]
- Medeiros, F.A.; et al. ARTEMIS 1 and 2: Phase 3 Studies of Bimatoprost SR. Ophthalmology 2020, 127, 1627–1641. [Google Scholar] [CrossRef]
- Fan, B.; et al. Personalized medicine in glaucoma: from genetics to clinical practice. Prog Retin Eye Res. 2024, 99, 101–118. [Google Scholar]
- Wiggs, J.; Pasquale, L. Genetics of glaucoma: why it matters. Ophthalmology 2023, 130, 235–247. [Google Scholar]
- Khosawneh, H.; et al. Polygenic risk scores in glaucoma: a clinical review. Br J Ophthalmol. 2025, 109, 540–552. [Google Scholar]
- Baehr, W.; et al. Mitochondrial targets for neuroprotection in glaucoma. Front Neurosci. 2024, 18, 882. [Google Scholar]
- He, Z.; et al. mTOR signaling and axonal regeneration in the injured optic nerve. Nat Rev Neurosci. 2025, 26, 95–110. [Google Scholar]
- Benowitz, L.; et al. Optic nerve regeneration: current state and future prospects. Exp Eye Res. 2024, 238, 109–125. [Google Scholar]
- Borrás, T. Gene therapy for glaucoma: a review of current and future strategies. Hum Gene Ther. 2025, 36, 12–28. [Google Scholar]
- Jain, N.; et al. CRISPR/Cas9-based gene editing for the treatment of glaucoma. Mol Ther. 2024, 32, 810–825. [Google Scholar]
- Kaufman, P.L. The future of glaucoma pharmacology. J Ocul Pharmacol Ther. 2026, 42, 5–18. [Google Scholar]
- Aung, T.; et al. Global trends in glaucoma management: The shift towards interventional pharmacotherapy. Lancet Public Health 2026, 11, e110–e122. [Google Scholar]
Figure 1.
Evolution of Pharmacological Agents in Glaucoma Treatment. Comparative chemical structures and mechanisms of action: (A) Timolol: A non-selective beta-adrenergic antagonist representing the conventional “gold standard.” Its primary mechanism involves the inhibition of aqueous humor production by the ciliary body (black). (B) Netarsudil: A representative of the next-generation Rho-kinase (ROCK) inhibitors. The isoquinoline ring and the amide group (highlighted in green) represent the pharmacophore responsible for biochemical remodeling of the trabecular meshwork, directly enhancing conventional outflow. (C) Latanoprostene Bunod: A dual-action molecular entity. The structure combines a prostaglandin F2α analog with a nitric oxide (NO)-donating moiety (indicated by the ONO2 group in red). While the prostaglandin component increases uveoscleral outflow, the released NO induces relaxation of the trabecular meshwork, providing a synergistic effect on intraocular pressure reduction.
Figure 1.
Evolution of Pharmacological Agents in Glaucoma Treatment. Comparative chemical structures and mechanisms of action: (A) Timolol: A non-selective beta-adrenergic antagonist representing the conventional “gold standard.” Its primary mechanism involves the inhibition of aqueous humor production by the ciliary body (black). (B) Netarsudil: A representative of the next-generation Rho-kinase (ROCK) inhibitors. The isoquinoline ring and the amide group (highlighted in green) represent the pharmacophore responsible for biochemical remodeling of the trabecular meshwork, directly enhancing conventional outflow. (C) Latanoprostene Bunod: A dual-action molecular entity. The structure combines a prostaglandin F2α analog with a nitric oxide (NO)-donating moiety (indicated by the ONO2 group in red). While the prostaglandin component increases uveoscleral outflow, the released NO induces relaxation of the trabecular meshwork, providing a synergistic effect on intraocular pressure reduction.
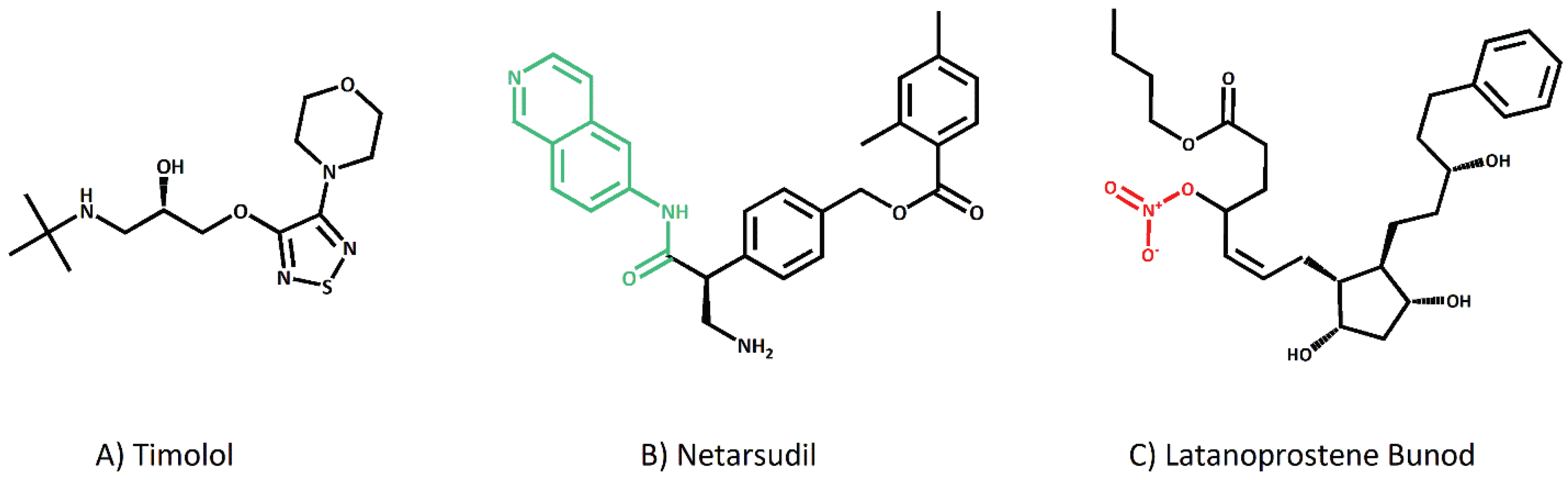
Table 2.
Structural and Pharmacological Analysis of Key Compounds.
| Class | Common Name | Structural Key Element | Primary Target | Pharamceutical Form | Clinical Value |
|---|---|---|---|---|---|
| β-Blockers | Timolol | Propanolamine chain; Thiadiazole/Morpholine rings | β1,β2 Adrenoceptors | Solution (0.25-0.5%) | Inflow suppression (Benchmark) |
| ROCK Inhibitors | Netarsudil | Isoquinoline core (ATP mimic); Ester linkage | Rho-associated kinase | Solution (0.02%) | TM relaxation; high local safety |
| NO-Donating PGA | Latanoprostene bunod | 4-(nitrooxy)butyl side chain | FP Receptors + sGC | Solution (0.024%) | Dual-route outflow restoration |
Table 3.
Clinical Efficacy of Next-Generation Pharmaceuticals vs. Gold Standards.
| Trial Name | Agent/ Molecule | Control | ΔIOP (mmHg) | Key Findings |
|---|---|---|---|---|
| APOLLO / LUNAR | Netarsudil 0.02% | Timolol 0.5% | 3.9 – 4.7 | Non-inferiority demonstrated across broad baseline IOP ranges [62]. |
| MERCURY-1 & 2 | Netarsudil / Latanoprost | Monotherapy | 7.0 – 9.2 | Surgical-level reduction via fixed-dose combination [63]. |
| APOLLO (LBN) | Latanoprostene bunod | Latanoprost 0.005% | + 1.2* | Superiority over PGAs via dual-pathway enhancement [64]. |
| ARTEMIS 1 & 2 | Bimatoprost SR (10 µg) | Timolol (drops) | 7.5 – 9.5 | Consistent IOP control for 12-24 weeks with a single administration [65]. |
*Incremental reduction over latanoprost.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



