Submitted:
11 February 2026
Posted:
12 February 2026
You are already at the latest version
Abstract
Chemotherapy- and/or radiotherapy-induced oral mucositis (CRIOM) is a common and debilitating complication in patients with head and neck cancer, driven largely by excessive proinflammatory cytokine signalling and treatment-associated bacterial dysbiosis. This review synthesizes current mechanistic evidence on cytokine toxicity and microbial imbalance in pathogenesis of CRIOM and to summarize emerging therapeutic strategies targeting these pathways. A structured PubMed search identified preclinical and clinical studies evaluating cytokine-mediated inflammation, microbiome alterations, and interventions with anti-inflammatory or microbiota-modulating effects. The reviewed evidence demonstrates that elevated IL-1β, IL-6, TNF-α, iNOS, and nitric oxide amplify tissue injury and ulceration, while disruption of oral and gut microbial communities, characterized by loss of beneficial commensals and enrichment of pathogenic taxa, further exacerbates mucosal inflammation. Anti-inflammatory agents, including pentoxifylline, atorvastatin, trans-caryophyllene, azilsartan, recombinant human IL-11, and low-level laser therapy reduced cytokine levels and improved mucosal healing. Additionally, microbiome-targeted approaches such as oral microbiota transplantation and a multi-strain probiotic cocktail restored microbial balance and attenuated CRIOM severity. Overall, current findings highlight cytokine toxicity and dysbiosis as synergistic drivers of CRIOM and support anti-inflammatory and microbiome-modulating therapies as promising adjunctive strategies; however, further studies incorporating patient-specific factors is needed to guide optimized clinical application.
Keywords:
head and neck cancer
; oral mucositis
; chemotherapy
; radiotherapy
; cytokine
; cytokine toxicity
; anti-inflammatory
; microbiome
; bacterial dysbiosis
; oral microbiota manipulation
1. Introduction
Recent global cancer estimates indicate that head and neck malignancies represent the third most common cancer type worldwide, with about 1.46 million newly diagnosed cases and nearly 488,000 deaths recorded in 2020 [1]. These cancers account for roughly 7.6% of all cancer incidences and 4.8% of cancer-related mortality [1]. The majority of head and neck cancers are squamous cell carcinomas, originating from the epithelial lining of the oral cavity, pharynx, and larynx [2]. Oral radiotherapy, often combined with chemotherapy, is one of the most prevalent and effective strategies used for the treatment of head and neck cancer [3]. However, this treatment is harmful to the normal tissue of the oral cavity and upper gastrointestinal tract, frequently resulting in oral mucositis: a common side effect and potentially severe complication. [3]. As shown in Figure 1, the pathophysiology of mucositis has been described as a five-phase process [4]. Initially, radiation triggers the production of reactive oxygen species (ROS) in phase 1, leading to the recruitment of innate immunity and the release of proinflammatory cytokines in phase 2. Subsequently, a signal amplification loop occurs in phase 3, leading to further tissue injury, erythema, inflammation, and apoptosis. Phase 4 is characterized by mucosal ulceration and bacterial colonization, often resulting in xerostomia. Finally, phase 5 involves epithelialization and healing.
Oral mucositis clinically manifests as extremely painful lesions in the oral mucosa that are refractory to pain management, due to its multifactorial etiology of both nociceptive and neuropathic mechanisms of injury [5]. These lesions often develop within the first few weeks of radiotherapy or shortly after initiation of cytotoxic chemotherapy and frequently worsen in severity with increasing cumulative treatment dose. In severe cases, patients may develop oral ulcers that cause intractable pain, impede oral intake, delay oncologic therapy, and increase the risk of both local and systemic infections. As oral mucositis progresses, patients experience dysphagia and odynophagia (difficulty and pain with swallowing), dysarthria (slurred speech), and the inability to receive adequate oral nutrition. These symptoms are often exacerbated in head and neck cancer patients by concurrent xerostomia, dysgeusia (taste disturbances), and baseline or treatment-related dysphagia resulting from tumor size and anatomic location. When severe, mucositis can become dose-limiting, leading to treatment interruptions or dose reductions and, in some cases, early cessation of oncologic therapy, which may compromise locoregional control and survival. Thus, oral mucositis contributes significantly to healthcare resource utilization and costs, as it is linked to higher rates of hospital admissions, prolonged inpatient stays, more frequent emergency and outpatient visits, increased nutritional support requirements, and greater reliance on opioid analgesics and antibiotic therapy [6]. Numerous studies have identified cytokine toxicity and bacterial dysbiosis as pivotal factors in the development of chemotherapy- and/or radiotherapy-induced oral mucositis (CRIOM) in head and neck cancer patients, suggesting that therapeutic modulation of these two factors may ameliorate severe oral mucositis [7,8].
This review highlights the potential synergistic roles of cytokine toxicity and bacterial dysbiosis and explores emerging therapeutic approaches targeting both the inflammatory and microbial pathways.
2. Materials and Methods
A literature search was conducted to address cytokine toxicity and bacterial dysbiosis as key contributors to the pathogenesis of oral mucositis and to identify studies investigating the anti-inflammatory and microbiome-modulating mechanisms involved in CRIOM, aimed at alleviating the condition. The search was performed using PubMed, employing the following keywords: “head and neck cancer,” “oral mucositis,” “chemotherapy,” “radiotherapy,” “cytokines,” “cytokine toxicity,” “microbiome,” “bacterial dysbiosis,” “anti-inflammatory,” and “oral microbiota manipulation”. Studies were included if they were original research articles published in English, investigated CRIOM, and evaluated anti-inflammatory agents or microbiome-targeted interventions. Both preclinical studies (in vivo animal models and in vitro cellular experiments) and clinical studies involving patients were included. Exclusion criteria comprised studies unrelated to oral mucositis, those not addressing inflammatory or microbiome-related mechanisms, and articles without full-text access.
3. Cytokine Toxicity: The Overproduction of Proinflammatory Cytokines During CRIOM
The increase in the production of proinflammatory cytokines during chemotherapy and/or radiotherapy in head and neck cancer patients, has been known as a central factor for oral mucositis development [9]. While chemotherapy and radiotherapy remain among the most effective therapeutic strategies for eradicating malignant cells and improving patient survival, their cytotoxic mechanisms also affect normal rapidly dividing tissues, such as the oral epithelium [10]. Upon chemotherapy and/or radiotherapy, a massive generation of reactive oxygen species (ROS) occurs, causing the damage of the genetic contents of oral epithelial cells, their death by apoptosis and upregulation of several transcriptional factors such as nuclear factor-kB (NF-kB), contributing to the production of a variety of proinflammatory cytokines [11,12]. This upregulation of inflammatory cytokines during the second phase of chemotherapy or radiotherapy is a key player in causing oral tissue damage seen in phases 3 and 4 [4].
3.1. The Major Proinflammatory Cytokines in CRIOM
Saliva is a clinically meaningful fluid that reflects the local mucosal environment, allowing non-invasive monitoring of cytokine modulation during treatment [13]. In a study involving 55 patients with advanced head and neck cancer undergoing chemoradiation therapy, there was a significant rise in proinflammatory cytokines, particularly IL-1β, IL-6, and TNF during chemoradiation therapy with higher levels correlating with more severe mucositis, as compared to the control group. Interestingly, early increase in IL-1β and IL-6 by week 3 was an even stronger predictor of high-grade mucositis, indicating that salivary cytokine profiles can reflect and even anticipate local tissue inflammation and damage. Therefore, the authors confirmed the role of proinflammatory cytokines in the CRIOM severity, in particular that IL-1β and IL-6 exert a stronger devastating effect.
3.2. The Upregulation of Proinflammatory Cytokines Triggers the Production of Other Proinflammatory Elements, Deteriorating Oral Mucositis
In another study, the authors evaluated the role of proinflammatory cytokines and other mediators, including inducible nitric oxide synthase (iNOS) and nitric oxide (NO) in CRIOM [14]. The enzyme iNOS plays an essential role in the macrophage inflammatory response by producing NO, which is strongly induced by proinflammatory stimuli [15]. NO functions as a signalling molecule central to inflammation: exerting anti-inflammatory effects under normal conditions but acting as a pro-inflammatory mediator when overproduced [16]. In this study, Cobalt-60 (Co-60) radiation was applied to the hamster cheek pouches to induce oral mucositis [14]. On day 13 of treatment, when myeloperoxidase, an inflammatory marker, peaked, there was also a marked increase in IL-1β, TNF, NO and iNOS, along with a reduction in IL-10 levels, all contributing to mucositis development. On the other hand, treatment with pentoxiphylline (PTX), a methylxanthine derivative known to suppress proinflammatory cytokines and inhibit TNF gene transcription, led to a significant decrease in TNF, IL-1 β and iNOS expression, thus preventing Co-60 induced oral mucositis as reflected by lower myeloperoxidase levels. Since PTX partially reduced iNOS, the authors hypothesized that direct iNOS inhibition might further prevent mucositis. Treatment with aminoguanidine (AMG), an iNOS inhibitor, reduced myeloperoxidase expression and lowered TNF and IL-1 β levels, alongside decreases in citrulline and nitrite concentrations, though iNOS expression was unchanged. These findings suggest that TNF and IL-1 β play a key role in CRIOM pathogenesis, possibly by inducing iNOS and nitric oxide production as a terminal mediator.
3.3. The Upregulation of Proinflammatory Cytokines Leads to Dysphagia, Necessitating Installation of a PEG
Oral mucositis can substantially impair patients’ ability to maintain adequate oral intake, and in more severe cases, nutrition must be supported through enteral methods such as nasogastric (NG) or orogastric (OG) tubes, or through percutaneous endoscopic gastrostomy (PEG) placement when feeding difficulties and dysphagia persist [17,18]. Meirovitz et al. (2010) investigated the relationship between serum cytokine levels and severity of mucositis necessitating installation of a PEG tube in head and neck cancer patients undergoing combined chemo-radiation therapy [17]. IL-6 level rose significantly after the second week of the therapy and correlated with PEG tube need: patients requiring PEG tube had a median IL-6 of 5.6 pg/ml, versus 3.2 pg/ml in others. IL-1, TNF and IL-10 did not show any association. Interestingly, IL-8 levels decreased during treatment: a paradox given its proinflammatory role, echoing previous reports [17,19,20]. However, as these studies focused on healthy tissue responses to irradiation, Meirovitz et al. (2010) suggested that IL-8 may help protect against irradiation damage. Overall, elevated IL-6 level was positively correlated with mucositis severity and dysphagia, leading to the installation of a PEG.
3.4. The Strengths, Gaps in the Knowledge and Suggested Improvements
Although the current studies highlight the key role of proinflammatory cytokine overproduction in oral mucositis, important knowledge gaps persist regarding its pathogenesis in head and neck cancer patients receiving chemo- or radiotherapy. Two important factors missing among these articles are the effects of sex and age on proinflammatory cytokine production contributing to oral mucositis. The effects of sex and age have been confirmed for other oral inflammatory diseases, such as periodontal disease [21]. Similarly, sex appears to influence susceptibility to oral mucosal injury, with evidence showing that women have a higher likelihood of developing severe oral mucositis during intensive treatments such as autologous stem cell transplantation. This difference has been linked to sex-related variations in immune responses, hormonal influences on mucosal integrity and inflammatory regulation, and differences in epithelial turnover, all of which may increase vulnerability to mucosal damage. [22]. Another limitation of the included studies is that they do not identify which oral cell populations are responsible for the cytokine elevations they report. In reality, multiple cell types, including oral epithelial cells, resident immune cells such as macrophages and dendritic cells, and stromal cells such as fibroblasts, can all produce pro-inflammatory cytokines during mucosal injury [23]. The other considerable issue by the authors is not investigating the mechanisms of action involved in the upregulation of proinflammatory cytokines. Knowing the mechanisms of action is also important for prevention and treatment purposes. The proteins involved in the pathways of proinflammatory cytokine production can be feasible targets for the inhibition of proinflammatory cytokines.
4. The Alleviation of Oral Mucositis Using Anti-inflammatory Approaches
The study of inflammatory processes in CRIOM enables the development of targeted, biology-based strategies for the modulation of oral mucositis [24]. Anti-inflammatory interventions remain a promising strategy for their prevention and treatment [25], as inhibiting proinflammatory cytokines such as TNF and IL-1β has been shown to alleviate CRIOM [26,27,28]. However, since inflammatory signalling also contributes to the therapeutic effects of chemo- and radio-therapy, excessive suppression can impair cancer cell killing. Recent studies suggest that mechanism-based therapies, illustrated in Figure 2, can alleviate mucositis without compromising anticancer efficacy, as some anti-inflammatory or antioxidant agents selectively protect normal mucosa while preserving tumor sensitivity to treatment-induced apoptosis. This selectivity supports the development of safe adjunctive therapies for mucositis management that do not interfere with chemotherapy or radiation outcomes [29].
4.1. The Anti-Inflammatory Effects of the Drugs Pentoxifylline, Atorvastatin, and Trans-Caryophyllene Contribute to the Alleviation of Oral Mucositis
Oral mucositis, characterized by epithelial breakdown, ulceration, and inflammatory cell infiltration, is driven by cytokines such as TNF, IFN-γ, and TGF-β [30]. Pentoxifylline, atorvastatin, and trans-caryophyllene have been investigated for their preventive potential by suppressing TNF and IFN-γ expression, regulating nitric oxide production, and promoting epithelial recovery [30]. In a 5-fluorouracil-induced oral mucositis model in male Wistar rats, these agents reduced cytokine (TNF, IFN-γ, and TGF-β) expression, decreased ulceration, and enhanced re-epithelial [30]. Preventative atorvastatin therapy significantly lowered TNF serum levels as compared to control and other experimental groups, while trans-caryophyllene treatment reduced in-situ TNF expression and inflammation, supporting healing. Systemically, trans-caryophyllene modulated IFN-γ levels during the onset and healing stages of oral mucositis (Days 8 and 15 of the experiment, respectively), indicating that this cytokine does not directly influence the worsening (Day 11) of the ulcers. Pentoxifylline also showed significant effects during ulcer remission (Day 15). Atorvastatin reduced systemic levels of TNF and INF-γ across all stages. Histologically, trans-caryophyllene prevented oral wounds and atorvastatin improved surface healing, suggesting that both agents mitigate oral mucositis by lowering proinflammatory mediators.
4.2. The Drug Azilsartan (AZT) Helps Alleviate Oral Mucositis Through Its Anti-Inflammatory Effects
Azilsartan (AZT), an angiotensin II receptor blocker with anti-inflammatory and tissue-protective properties, was investigated for its potential to mitigate CRIOM [31]. The drug modulates cytokines by reducing TNF-α and IL-1β, increasing IL-10, and enhancing growth factors such as VEGF and FGF, thereby promoting epithelial repair and limiting mucosal inflammation. Using a 5-fluorouracil-induced oral mucositis model in Syrian hamsters, the study evaluated the effects of AZT on mucosal injury and healing [31]. They used macroscopic analysis, and cheek pouch samples were removed for histopathologic analysis. In this study, TNF, IL-1β, IL-10, VEGF, FGF, KGF and TGF-α levels were measured using ELISA and immunohistochemical analysis. The results revealed a significant decrease in TNF and IL-1β upon oral treatment with 1 mg/kg AZT. Furthermore, the AZT1/5-FU group showed dramatically increased levels of IL-10 and TGF-α compared to the 5-FU/saline group. The most effective dose for the AZT efficacy was 1 mg/kg, in which AZT generally demonstrated effectiveness regardless of dose, with a lower dose being preferred for achieving the optimal clinical outcomes by speeding up the healing process. In addition, the findings illustrated that AZT sped up the healing process in an experimental model of 5-FU–induced oral mucositis by promoting granulation tissue formation, the migration of fibroblasts and keratinocytes, and collagen deposition. These results were supported by the elevated levels of TGF-α, FGF, and KGF, along with the upregulation of VEGF, which has been linked to angiogenesis in scar tissue. Together, administration of AZT at a dose of 1 mg/kg sped up the healing process by stimulating growth factors that are critical for angiogenesis and re-epithelialization, along with increasing IL-10 levels.
4.3. The Mechanisms by which Recombinant Human Interleukin-11 Modulates the Progression of Radiation-Induced Oral Mucositis
Interleukin-11 (IL-11), a cytokine with cytoprotective and anti-inflammatory properties, was investigated for its ability to mitigate radiation-induced oral mucositis [32]. IL-11 downregulates pro-inflammatory cytokines such as IL-1β and TNF-α, protects connective tissue, and promotes epithelial proliferation and differentiation, thereby reducing inflammation and preserving mucosal integrity. Using a model of acute radiation injury in male golden Syrian hamsters, recombinant human IL-11 (rhIL-11) was evaluated for its effects on mucosal cytokine expression, apoptosis, and histological alterations [32]. According to the mucositis scores, there was an increased mucositis severity at day 15; however, animals treated with rhIL-11 showed less mucositis compared to placebo controls, suggesting the first evidence that rhIL-11 can modulate radiation-induced mucositis. This study observed that local tissue levels of IL-1β and TNF significantly increased after radiation, and this rise in both cytokines paralleled the progression of mucositis. However, a significant decrease in IL-1β levels, as detected by immunohistochemical and PCR techniques, was observed in rhIL-11-treated animals. This reduction was associated with a lower severity of mucositis. Immunohistochemical analysis indicated that the decrease in IL-1β levels was not caused by a reduction in the intensity of the inflammatory infiltrate, but rather due to lower expression of the cytokine by submucosal inflammatory cells. Moreover, RNA levels of TNF and IL-1β were lower in rhIL-11-treated hamsters. Unlike IL-1β and TNF, there were no differences in IL-2 or TGF-β levels between the control and rhIL-11-treated hamsters. This observation implies a significant connection between elevated IL-1β and TNF levels and the development of mucositis, supporting the concept that rhIL-11 activity might partially stem from its ability to suppress the expression of these proinflammatory cytokines.
4.4. Biomodulation of Inflammatory Cytokines Associated with Oral Mucositis by Low-Level Laser Therapy
Low-level laser therapy (LLLT) was investigated for its potential to modulate inflammatory cytokine expression associated with oral mucositis [33]. LLLT has been shown to promote wound healing by enhancing cell proliferation, migration, and growth factor expression, while also reducing inflammatory mediator release [33]. Because inflammatory cytokines such as TNF, IL-6, and IL-8 play a central role in the onset and severity of mucositis, this study evaluated the biomodulatory effects of LLLT on their gene and protein expression in lipopolysaccharide-stimulated human gingival fibroblasts [33]. In this study, primary gingival fibroblasts were treated with LPS and exposed to LLLT irradiation at 0, 0.5, 1.5 or 3 J cm-². The gene expression levels of TNF, IL-1β, IL-6, and IL-8 were assessed using Real-Time PCR, and the protein synthesis of these cytokines was measured using ELISA. According to the results, non-irradiated gingival fibroblasts exposed to LPS exhibited an increased expression of all cytokines studied, except for IL-1β, compared to cells not exposed to LPS. Irradiation following LPS treatment at energy densities of 1.5 J/cm² and 3 J/cm² reduced the expression of TNF, IL-6, and IL-8. Although 0.5 J/cm² was not effective in modulating the gene expression of these inflammatory cytokines. Regarding the results obtained by ELISA, low-level laser therapy reduced TNF synthesis at all energy densities, while IL-6 synthesis was decreased at 1.5 J/cm² and 3 J/cm². However, the therapy did not affect the synthesis of IL-1β and IL-8. These results showed that LLLT had a beneficial biomodulatory impact on the expression of inflammatory cytokines related to oral mucositis in human gingival fibroblasts.
4.5. The Strengths, Gaps in the Knowledge, and Suggested Improvements
The primary strength of the presented articles is the strong data showing that modulating the production of proinflammatory cytokines can attenuate CRIOM, as summarized in Table 1. Therefore, their findings may be promising adjunctive treatments for oral mucositis. However, some weaknesses are evident in the articles, particularly their lack of consideration for the side effects of the drugs used, which is essential for determining whether these agents can be safely applied for anti-inflammatory management of oral mucositis. They could have compared cytokine levels after anti-inflammatory treatment with a normal range that an individual’s body needs to function properly. They could also monitor for the occurrence of immunosuppressive diseases upon drug treatment. The other considerable issue is that the authors did not consider the effects of sex and age in their results. Finally, the articles presented in sections 3.1, 3.2 and 3.3 were animal in vivo, and the article presented in section 3.4 was an in vitro human model, so there is a need to investigate how the treatment would work for an in vivo human model.
5. The Role of Oral Microbiota in CRIOM
The commensal microbiota can enormously impact the colonization and resistance of pathogenic microorganisms and stimulate primary immunity [34]. Upon oral microbiota dysbiosis, the oral mucosal epithelial defense can be compromised, thus accelerating the pathological processes [34]. Exposure to cytotoxic cancer treatments such as chemotherapy and/or radiotherapy is linked to significant alterations in the oral microbiome. However, distinguishing between cause and effect has been extremely challenging [35]. Several studies have documented that the alterations in the oral microbiome after exposure to chemotherapy- and/or radiotherapy contribute to the development of oral mucositis [35]. Recent research indicates that improved outcomes for oral mucositis are linked to a more resilient oral microbiome that remains stable upon chemotherapy- and/or radiotherapy treatments [36,37]. Furthermore, during the fourth stage of the mucositis, the ulceration phase, the breaks in the submucosa permit some microorganisms, typically symbiotic inhabitants of healthy mucosa, to invade this tissue, leading to an inflammation response mediated by mononuclear infiltrating cells, hence promoting new pro-inflammatory cytokines release that can amplify expression of pro-apoptotic mediators and increase tissue damage [38].
5.1. Oral Dysbiosis Has a Significant Detrimental Impact on the Severity of Oral Mucositis
In a study, the authors determined whether the commensal microbiota can influence the severity of CRIOM [39]. In this study, specific-pathogen-free (SPF) and germ-free Swiss Webster mice in the experimental groups were administered 5-Fluorouracil (5-FU) to induce oral mucositis. Then, differences in epithelial thickness, cell proliferation/turnover rates, and expression levels of metalloproteinases and pro-inflammatory mediators were analyzed using histopathological and immunohistochemical tests. The oral cavities of germ-free mice are devoid of any microorganisms. In contrast, SPF mice harbour bacteria from the genera Streptococcus, Lactobacillus, Staphylococcus, Enterococcus and Propionibacterium. The results revealed that 5-FU-treated SPF mice exhibited characteristic histopathological features of oral mucositis, with a significant reduction in the proliferation of oral mucosal cells compared to the other groups. The qualitative analysis revealed that the oral epithelium was dramatically thinner in 5-FU-treated SPF mice compared to 5-FU-treated germ-free mice. Histological grading showed that the severity of oral mucositis was grade 3 in SPF mice and grade 1 in germ-free mice. The levels of proinflammatory cytokines, such as IL-1β, TNF, and MPO, were significantly higher in the oral mucosa of SPF mice compared to germ-free mice. They also discovered that the proinflammatory cytokines IL-1β, TNF and MPO are expressed by cells in the oral epithelium, endothelium, and mucosal connective tissues in 5-FU-treated SPF mice. They detected increased levels of MPO in the connective tissues of the oral mucosa in 5-FU-treated SPF mice. MPO, released from neutrophil’s azurophilic granules, facilitates the production of hypochlorous acid, leading to oxidative damage to host tissue. In addition, they observed elevated levels of expression of MMP-3 and -9 in the basal epithelium, lamina propria and submucosa of 5-FU-treated SPF mice. MMP-3 may contribute to mucosal damage by disrupting cell-to-cell and cell-to-extracellular matrix (ECM) connections through the degradation of collagens, fibronectin, laminin, aggrecan, insulin-like growth factor binding protein-3, and serpins [39]. As tissue injury advances during the development of oral mucositis, the tight junction proteins such as E-cadherin, occludin and claudin-1 are downregulated, which can further weaken the barrier function of oral mucosa [39]. This increased permeability allows bacterial products to pass through, resulting in further tissue damage [39]. Hence, upon tissue damage, both pathogen-associated molecular patterns (PAMPs) generated by bacterial products and damage-associated molecular patterns (DAMPs) resulting from cellular stress and tissue injury are recognized by the oral epithelium, fibroblasts, and endothelial cells via their pattern recognition receptors (PRRs) including toll-like receptor (TLR)-2, -4, -9, and nucleotide-binding oligomerization domain-containing protein-1 (NOD-1) and -2, resulting in intensified inflammatory responses [39]. Together, comparing the 5-FU-treated SPF and germ-free mice, the germ-free mice showed less severe oral mucositis.
5.2. Chemotherapy-Induced Oral Mucositis Is Associated with Bacterial Dysbiosis
In the study performed by Hong et al. (2019), the authors demonstrated that chemotherapy-induced oral mucositis is associated with bacterial dysbiosis and suggested that these dysbiotic changes can worsen chemotherapy-induced epithelial injury. In this study, they used 49 subjects receiving 5-fluorouracil (5-FU) or doxorubicin-based chemotherapy, and 30 non-cancer subjects, as a control for microbiome stability, then evaluated them longitudinally during one cycle [40]. They also conducted in vitro assays to assess the antibacterial potential of 5-FU on oral microorganisms and its interaction with commensal bacteria in oral epithelial tissues. The results revealed that during chemotherapy, the oral bacteriome experienced significant disruptions. They included that while antibiotic and acid inhibitor intake played a role in these changes, disruptions were also linked to antineoplastics and were independently and significantly associated with the severity of oral mucositis. They found that the changes in the bacteria associated with the mucositis involved a reduction in common health-associated commensals from genera like Streptococcus, Actinomyces, Gemella, Granulicatella, and Veillonella. However, there was an increase in some gram-negative bacteria, such as Fusobacterium nucleatum and Prevotella oris. Also, during chemotherapy, transcriptional responses showed an increase in the expression of genes involved in innate immunity and apoptosis. Finally, using a multilayer epithelial construct, they demonstrated that dysbiotic shifts associated with mucositis may worsen mucosal damage. This is because the mucositis-depleted Streptococcus salivarius was tolerated as a commensal, whereas the mucositis-enriched F. nucleatum exhibited pro-inflammatory and pro-apoptotic properties [40]. All in all, this study illustrated that chemotherapy-induced oral mucositis is linked to bacterial dysbiosis and shows that dysbiotic shifts can potentially worsen epithelial injury caused by antineoplastic treatments.
5.3. Bacterial Colonization and Gene Expression Vary During Different Stages of Mucositis.
In one study, the authors assessed the bacterial colonization and evaluated the genes’ expression of MCR-1 (mobilized colistin resistance), VIM2 (β-lactam resistance), TET(K) (tetracycline resistance) and blaKPC (carbapenem resistance) at 3 time points (onset, during, and at the end), among 24 oral mucositis patients with oral cancers undergoing radiotherapy and concomitant radiochemotherapy [41]. The results revealed that the facultative anaerobes isolated from saliva included Staphylococcus aureus (22%, N=16), Staphylococcus epidermidis (29%, N=21), Pseudomonas aeruginosa (28%, N=20), Escherichia coli (25%, N=18), and Klebsiella pneumoniae (26%, N=19). In the study groups, subjects treated with chemoradiation exhibited higher prevalence rates of S. aureus (50%, N=6), P. aeruginosa (41.7%, N=5), and S. epidermidis (33.3%, N=4), whereas E. coli (16.7%, N=2) was the least prevalent by the end of the 6th week of therapy. The Mann-Whitney U test indicated no statistically significant difference in the presence of organisms between the study groups at the 1st, 3rd week, and at the end of therapy. The bacterial isolates collected during and at the end of therapy exhibited higher levels of antibiotic-resistance genes (VIM2, MCR-1, TET(K), blaKPC) compared to those collected at the start of the therapy. Together, Bacterial colonization and gene expression varied throughout the different stages of oral mucositis.
5.4. The Strengths, Gaps in the Knowledge, and Suggested Improvements
The primary merit among the presented articles is identifying some of the bacteria that experience a change in their population due to CRIOM. So, by knowing how a change in the population of bacteria would affect the severity of the oral mucositis, it is possible to manage the severity of the oral mucositis accordingly. However, the articles have several flaws. One is that the authors did not examine whether there is a sex and age difference in the microbiome and microbiota dysbiosis. It could be an important clue whether male and female patients should be treated differently. Also, in the experiment by Subramaniam & Muthukrishnan (2019), the authors should have examined precisely how the development of antibiotic resistance impacts the severity of the CRIOM. They could have compared the severity of the oral mucositis according to each individual’s antibiotic resistance. Therefore, it could aid in identifying a drug targeting antibiotic resistance genes that would provide the most protective results for the amelioration of oral mucositis.
6. The Manipulation of Oral Microbiota for the Management of Oral Mucositis
Understanding the role of evolving polymicrobial oral communities in causing or worsening cancer therapy-induced oral mucositis is essential to preventing the severe negative effects associated with CRIOM [42]. On the other hand, the composition of gut microbiota may change during the treatment, which could also influence the severity of the CRIOM in head and neck cancer patients [43]. Proinflammatory gut microbes, whether presented at the baseline or increased after chemotherapy and/or radiotherapy, can worsen inflammatory processes in the oral cavity, leading to severe oral mucositis. This could be due to the changes in the intestinal environment, like inflammation and disruption of the intestinal barrier, or the systemic effects of the gut microbiota on the immune system [44]. Although gut microbes with anti-inflammatory properties can beneficially impact oral mucositis by maintaining intestinal balance and reducing systemic inflammatory signals [44]. Consequently, the modification of gut microbiota has attracted considerable interest among clinicians and scientists as a viable method for alleviating CRIOM in head and neck cancer patients [45], [46]. These therapeutic concepts are further summarized in Figure 3, which outlines microbiome-modulating approaches and their mechanisms of action in alleviating chemotherapy- and/or radiotherapy-induced oral mucositis.
6.1. Oral Microbiota Transplantation Is A Feasible Approach to Fighting Against Radiotherapy-Induced Oral Mucositis
In a study by Xiao et al. (2021), the authors found that by performing oral microbiota transplantation (OMT), it is possible to fight against head and neck radiotherapy-induced oral mucositis in mice. Fractionated radiation was administered to simulate radiotherapy for nasal, oral and laryngeal cancers (NOALCs) in mouse models [47]. They also recruited 44 nasal, oral and laryngeal cancer patients and compared Lactobacillaceae levels during radiotherapy. They analyzed the oral bacterial composition of healthy mouse donors, finding Streptococcus and Rodentibacter to be the most abundant. They transplanted oral microbiomes from healthy mouse donors to mice that were exposed to local head and neck irradiation. The results revealed that OMT ameliorated irradiation-induced oral mucositis. Hematoxylin and eosin staining showed thinning epithelium and flattened tongue papillae after radiation exposure. However, OMT ameliorated the injuries. The proinflammatory cytokines, IL-1, IL-6, TNF and TGFβ in tongue tissues and plasma could be reduced by OMT. To understand how OMT reduces radiation-induced oral mucositis, they analyzed the oral bacteria in mice after head and neck irradiation, with and without OMT treatment. The results revealed that irradiation did not change the ɑ-diversity of the oral bacteria, but 10 days of OMT increased the ɑ-diversity. Also, OMT reversed the cumulative increase in β-diversity caused by irradiation. Based on 16S rRNA gene sequencing among clinical samples, they observed that radiotherapy to NOALC patients or total head irradiation in mice raised Lactobacillaceae levels; however, OMT reversed this change. Suggesting that Lactobacillaceae might play a key role in the development of radiation-induced oral mucositis, however, it can be counteracted by OMT. Collectively, their findings indicated that OMT alters the oral bacterial composition to combat radiation-induced dysbiosis and mucositis in the oral cavity. Finally, to further investigate the underlying mechanism by which OMT protects against radiation-induced oral mucositis, they used high-throughput sequencing to assess gene expression in tongue tissues from irradiated mice with and without OMT. The most significant response was from S100a9, which was downregulated after irradiation and upregulated by OMT. Silencing S100a9 negated OMT’s protective effects, worsening symptoms and increasing inflammatory factors, suggesting S100a9’s role in OMT-mediated recovery.
6.2. The Use of Modified Probiotic Cocktail Can Significantly Diminish the Severity of Oral Mucositis
In a study, the authors determined the protective effects of probiotic cocktail treatment on chemoradiotherapy (CCRT)-induced oral mucositis in nasopharyngeal cancer (NPC) patients and rat model [48]. The results revealed that providing patients with a probiotic cocktail of Lactobacillus plantarum, Bifidobacterium animalis, Lactobacillus rhamnosus, and Lactobacillus acidophilus had a protective effect against chemoradiotherapy (CCRT)-induced oral mucositis. It was via improving their immunity as they experienced a decreased reduction rate of CD3+, CD4+, and CD8+ T cells compared to the placebo group [48]. Importantly, they figured out that the probiotic cocktail altered the composition of the intestinal microbiome in patients with NPC, in which it increased the abundance of Firmicutes and decreased the abundance of Bacteroidetes and Actinobacteria to normal levels. As a result, the probiotic cocktail restored the gut dysbiosis in patients with NPC who underwent CCRT, resulting in the attenuation of CCRT-induced oral mucositis severity. For the rat mucositis model, both radiation and chemotherapy were used for the induction of oral mucositis with busulfan. There was a significant decrease in the mRNA expression of proinflammatory cytokines IL-6, IL-1β, and TNF in the tongue tissue, indicating that the probiotic cocktail reduced tongue tissue inflammation and pathological damage in the rats with oral mucositis caused by radiotherapy and chemotherapy. Also, the probiotic cocktail downregulated the expressions of TLR4 and P-NF-κB/NF-κB, and significantly inhibited cell apoptosis. In addition, the probiotic cocktail significantly restored the intestinal tight junction proteins ZO-1 and Claudin-1expression to normal levels. Thus, immune activation and inflammation are prevented, reducing TNF, IL-1β, and IL-6 in the oral cavity, which eventually could ameliorate oral mucositis [48]. Finally, the results revealed that the probiotic cocktail could reverse the gut dysbiosis induced by radiotherapy and chemotherapy in rats as well as by increased beneficial bacteria like Firmicutes, Lachnospiraceae, and Ruminococcus, while reducing harmful bacteria like Bacteroidetes and Bacteroides, suggesting that it helps prevent inflammation in the treated rats. Together, the probiotic cocktail significantly reduced the severity of oral mucositis in patients with NPC, possibly by regulating gut microbiota and boosting immunity. Experiments on rats further confirmed that the probiotic cocktail alleviates CCRT-induced oral mucositis severity by modulating gut dysbiosis related to inflammatory responses.
6.3. The Strengths, Gaps in the Knowledge, and Suggested Improvements
It was very insightful of the authors to discuss the modulation of the oral and intestinal microbiota in terms of ameliorating oral mucositis, summarized in Table 2, as it is a relatively easy and uncomplicated approach for the patients. However, in the study conducted by Xiao et al., 2021, the authors should have provided some information on how the oral microbiota transplantation approach is performed for patients in practice.
7. Conclusions
To date, numerous strategies have been explored to prevent or mitigate oral mucositis, and the presented therapeutic approaches highlight selected studies that exemplify different biological mechanisms, including anti-inflammatory and microbiome-modulating interventions. Cytokine toxicity and microbiota dysbiosis represent two key contributors to CRIOM in head and neck cancer patients. The implemented strategies demonstrated significant efficacy in managing severe oral mucositis conditions, showcasing their potential as viable treatments for mitigating the intensity and discomfort associated with this condition. This comprehensive review of the currently known approaches identified a range of viable strategies to alleviate the painful and debilitating effects of oral mucositis for patients. Further examination of numerous parameters, including sex and age, is still required to ascertain the feasibility of these approaches. The meticulous evaluation will ensure that the proposed methods are effective and applicable across diverse patient populations.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zhou, T.; Huang, W.; Wang, X.; Zhang, J.; Zhou, E.; Tu, Y.; Zou, J.; Su, K.; Yi, H.; Yin, S. Global Burden of Head and Neck Cancers from 1990 to 2019. iScience 2024, 27, 109282. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and Neck Squamous Cell Carcinoma. Nat Rev Dis Primers 2020, 6, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Toshkov, I.A.; Gleiberman, A.S.; Mett, V.L.; Hutson, A.D.; Singh, A.K.; Gudkov, A.V.; Burdelya, L.G. Mitigation of Radiation-Induced Epithelial Damage by the TLR5 Agonist Entolimod in a Mouse Model of Fractionated Head and Neck Irradiation. Radiation Research 2017, 187, 570–580. [Google Scholar] [CrossRef] [PubMed]
- Sonis, S.T. Oral Mucositis. Anticancer Drugs 2011, 22, 607–612. [Google Scholar] [CrossRef]
- Villa, J.F.; Strang, A.; Owolabi, A.; Ramirez, M.F. Addressing Pain in Oral Mucositis: Narrative Review of Current Practices and Emerging Treatments. JPR 2025, 18, 3723–3741. [Google Scholar] [CrossRef]
- Elad, S.; Yarom, N.; Zadik, Y.; Kuten-Shorrer, M.; Sonis, S.T. The Broadening Scope of Oral Mucositis and Oral Ulcerative Mucosal Toxicities of Anticancer Therapies. CA: A Cancer Journal for Clinicians 2022, 72, 57–77. [Google Scholar] [CrossRef]
- Feng, J.; Gao, M.; Zhao, C.; Yang, J.; Gao, H.; Lu, X.; Ju, R.; Zhang, X.; Zhang, Y. Oral Administration of Probiotics Reduces Chemotherapy-Induced Diarrhea and Oral Mucositis: A Systematic Review and Meta-Analysis. Front. Nutr. 2022, 9. [Google Scholar] [CrossRef]
- Ferreira, A.S.; Macedo, C.; Silva, A.M.; Delerue-Matos, C.; Costa, P.; Rodrigues, F. Natural Products for the Prevention and Treatment of Oral Mucositis—A Review. Int J Mol Sci 2022, 23, 4385. [Google Scholar] [CrossRef]
- Sonis, S.T. The Pathobiology of Mucositis. Nature Reviews Cancer 2004, 4, 277–284. [Google Scholar] [CrossRef]
- Wu, H.G.; Song, S.Y.; Kim, Y.S.; Oh, Y.T.; Lee, C.G.; Keum, K.C.; Ahn, Y.C.; Lee, S. Therapeutic Effect of Recombinant Human Epidermal Growth Factor (rhEGF) on Mucositis in Patients Undergoing Radiotherapy, with or without Chemotherapy, for Head and Neck Cancer. Cancer 2009, 115, 3699–3708. [Google Scholar] [CrossRef]
- Maria, O.M.; Eliopoulos, N.; Muanza, T. Radiation-Induced Oral Mucositis. Front. Oncol. 2017, 7. [Google Scholar] [CrossRef]
- Nguyen, H.; Sangha, S.; Pan, M.; Shin, D.H.; Park, H.; Mohammed, A.I.; Cirillo, N. Oxidative Stress and Chemoradiation-Induced Oral Mucositis: A Scoping Review of In Vitro, In Vivo and Clinical Studies. Int J Mol Sci 2022, 23, 4863. [Google Scholar] [CrossRef]
- Bossi, P.; Bergamini, C.; Miceli, R.; Cova, A.; Orlandi, E.; Resteghini, C.; Locati, L.; Alfieri, S.; Imbimbo, M.; Granata, R.; et al. Salivary Cytokine Levels and Oral Mucositis in Head and Neck Cancer Patients Treated With Chemotherapy and Radiation Therapy. International Journal of Radiation Oncology*Biology*Physics 2016, 96, 959–966. [Google Scholar] [CrossRef]
- Bastos Moura, J.F.; Mota, J.M.S.C.; Leite, C.A.V.; Wong, D.V.T.; Bezerra, N.P.; Brito, G.A.D.C.; Lima, V.; Cunha, F.Q.; Ribeiro, R.A. A Novel Model of Megavoltage Radiation-Induced Oral Mucositis in Hamsters: Role of Inflammatory Cytokines and Nitric Oxide. International Journal of Radiation Biology 2015, 91, 500–509. [Google Scholar] [CrossRef]
- McNeill, E.; Crabtree, M.J.; Sahgal, N.; Patel, J.; Chuaiphichai, S.; Iqbal, A.J.; Hale, A.B.; Greaves, D.R.; Channon, K.M. Regulation of iNOS Function and Cellular Redox State by Macrophage Gch1 Reveals Specific Requirements for Tetrahydrobiopterin in NRF2 Activation. Free Radic Biol Med 2015, 79, 206–216. [Google Scholar] [CrossRef]
- Sharma, J.N.; Al-Omran, A.; Parvathy, S.S. Role of Nitric Oxide in Inflammatory Diseases. Inflammopharmacology 2007, 15, 252–259. [Google Scholar] [CrossRef]
- Meirovitz, A.; Kuten, M.; Billan, S.; Abdah-Bortnyak, R.; Sharon, A.; Peretz, T.; Sela, M.; Schaffer, M.; Barak, V. Cytokines Levels, Severity of Acute Mucositis and the Need of PEG Tube Installation during Chemo-Radiation for Head and Neck Cancer--a Prospective Pilot Study. Radiat Oncol 2010, 5, 16. [Google Scholar] [CrossRef]
- Wei, M.; Ho, E.; Hegde, P. An Overview of Percutaneous Endoscopic Gastrostomy Tube Placement in the Intensive Care Unit. J Thorac Dis 2021, 13, 5277–5296. [Google Scholar] [CrossRef]
- Reers, S.; Pfannerstill, A.-C.; Rades, D.; Maushagen, R.; Andratschke, M.; Pries, R.; Wollenberg, B. Cytokine Changes in Response to Radio-/Chemotherapeutic Treatment in Head and Neck Cancer. Anticancer Research 2013, 33, 2481–2489. [Google Scholar] [PubMed]
- Principe, S.; Dikova, V.; Bagán, J. Salivary Cytokines in Patients with Head and Neck Cancer (HNC) Treated with Radiotherapy. J Clin Exp Dent 2019, 11, e1072–e1077. [Google Scholar] [CrossRef]
- Tubero Euzebio Alves, V.; Bruno, M.E.C.; Mukherjee, S.; Wang, L.; Danaher, R.J.; Su, L.; Starr, M.E.; Gonzalez, O.A. Sex-Related Effect of Aging in Gingival Gamma-Delta T Cells. J Dent Res 2024, 103, 62–70. [Google Scholar] [CrossRef]
- Gebri, E.; Kiss, A.; Tóth, F.; Hortobágyi, T. Female Sex as an Independent Prognostic Factor in the Development of Oral Mucositis during Autologous Peripheral Stem Cell Transplantation. Sci Rep 2020, 10, 15898. [Google Scholar] [CrossRef]
- Chen, C.; Zhang, Q.; Yu, W.; Chang, B.; Le, A. d. Oral Mucositis: An Update on Innate Immunity and New Interventional Targets. Journal of Dental Research 2020, 99, 1122–1130. [Google Scholar] [CrossRef]
- Haagen, J.; Krohn, H.; Röllig, S.; Schmidt, M.; Wolfram, K.; Dörr, W. Effect of Selective Inhibitors of Inflammation on Oral Mucositis: Preclinical Studies. Radiotherapy and Oncology 2009, 92, 472–476. [Google Scholar] [CrossRef]
- Nicolatou-Galitis, O.; Sarri, T.; Bowen, J.; Di Palma, M.; Kouloulias, V.E.; Niscola, P.; Riesenbeck, D.; Stokman, M.; Tissing, W.; Yeoh, E.; et al. Systematic Review of Anti-Inflammatory Agents for the Management of Oral Mucositis in Cancer Patients. Support Care Cancer 2013, 21, 3179–3189. [Google Scholar] [CrossRef]
- Ariyawardana, A.; Cheng, K.K.F.; Kandwal, A.; Tilly, V.; Al-Azri, A.R.; Galiti, D.; Chiang, K.; Vaddi, A.; Ranna, V.; Nicolatou-Galitis, O.; et al. Systematic Review of Anti-Inflammatory Agents for the Management of Oral Mucositis in Cancer Patients and Clinical Practice Guidelines. Support Care Cancer 2019, 27, 3985–3995. [Google Scholar] [CrossRef]
- Sironi, M.; Pozzi, P.; Polentarutti, N.; Benigni, F.; Coletta, I.; Guglielmotti, A.; Milanese, C.; Ghezzi, P.; Vecchi, A.; Pinza, M.; et al. INHIBITION OF INFLAMMATORY CYTOKINE PRODUCTION AND PROTECTION AGAINST ENDOTOXIN TOXICITY BY BENZIDAMINE. Cytokine 1996, 8, 710–716. [Google Scholar] [CrossRef]
- Sironi, M.; Milanese, C.; Vecchi, A.; Polenzani, L.; Guglielmotti, A.; Coletta, I.; Landolfi, C.; Soldo, L.; Mantovani, A.; Pinza, M. Benzydamine Inhibits the Release of Tumor Necrosis Factor-α and Monocyte Chemotactic Protein-1 byCandida Albicans-Stimulated Human Peripheral Blood Cells. Int J Clin Lab Res 1997, 27, 118–122. [Google Scholar] [CrossRef]
- Kwon, Y. Mechanism-Based Management for Mucositis: Option for Treating Side Effects without Compromising the Efficacy of Cancer Therapy. Onco Targets Ther 2016, 9, 2007–2016. [Google Scholar] [CrossRef]
- Da Cruz Campos, M.I.; Campos, C.N.; Corrêa, J.O.A.; Aarestrup, F.M.; Aarestrup, B.J.V. Induced Oral Mucositis in Wistar Rats Treated with Different Drugs: Preventive Potential in Cytokine Production. Mol Clin Oncol 2021, 14, 127. [Google Scholar] [CrossRef]
- de Araújo, A.A.; Varela, H.; de Medeiros, C.A.C.X.; de Castro Brito, G.A.; de Lima, K.C.; de Moura, L.M.; de Araújo, R.F. Azilsartan Reduced TNF-α and IL-1β Levels, Increased IL-10 Levels and Upregulated VEGF, FGF, KGF, and TGF-α in an Oral Mucositis Model. PLoS One 2015, 10, e0116799. [Google Scholar] [CrossRef]
- Sonis, S.T.; Peterson, R.L.; Edwards, L.J.; Lucey, C.A.; Wang, L.; Mason, L.; Login, G.; Ymamkawa, M.; Moses, G.; Bouchard, P.; et al. Defining Mechanisms of Action of Interleukin-11 on the Progression of Radiation-Induced Oral Mucositis in Hamsters. Oral Oncology 2000, 36, 373–381. [Google Scholar] [CrossRef]
- Basso, F.G.; Pansani, T.N.; Soares, D.G.; Scheffel, D.L.; Bagnato, V.S.; de Souza Costa, C.A.; Hebling, J. Biomodulation of Inflammatory Cytokines Related to Oral Mucositis by Low-Level Laser Therapy. Photochemistry and Photobiology 2015, 91, 952–956. [Google Scholar] [CrossRef]
- Min, Z.; Yang, L.; Hu, Y.; Huang, R. Oral Microbiota Dysbiosis Accelerates the Development and Onset of Mucositis and Oral Ulcers. Front. Microbiol. 2023, 14. [Google Scholar] [CrossRef]
- Bruno, J.S.; Al-Qadami, G.H.; Laheij, A.M.G.A.; Bossi, P.; Fregnani, E.R.; Wardill, H.R. From Pathogenesis to Intervention: The Importance of the Microbiome in Oral Mucositis. Int J Mol Sci 2023, 24, 8274. [Google Scholar] [CrossRef]
- Laheij, A.M.G.A.; Raber-Durlacher, J.E.; Koppelmans, R.G.A.; Huysmans, M.-C.D.N.J.M.; Potting, C.; van Leeuwen, S.J.M.; Hazenberg, M.D.; Brennan, M.T.; von Bültzingslöwen, I.; Johansson, J.-E.; et al. Microbial Changes in Relation to Oral Mucositis in Autologous Hematopoietic Stem Cell Transplantation Recipients. Sci Rep 2019, 9, 16929. [Google Scholar] [CrossRef]
- Takahashi, M.; Toyosaki, M.; Matsui, K.; Machida, S.; Kikkawa, E.; Ota, Y.; Kaneko, A.; Ogawa, Y.; Ando, K.; Onizuka, M. An Analysis of Oral Microbial Flora by T-RFLP in Patients Undergoing Hematopoietic Stem Cell Transplantation. Int J Hematol 2020, 112, 690–696. [Google Scholar] [CrossRef]
- Pulito, C.; Cristaudo, A.; Porta, C.L.; Zapperi, S.; Blandino, G.; Morrone, A.; Strano, S. Oral Mucositis: The Hidden Side of Cancer Therapy. J Exp Clin Cancer Res 2020, 39, 210. [Google Scholar] [CrossRef]
- Gupta, N.; Quah, S.Y.; Yeo, J.F.; Ferreira, J.; Tan, K.S.; Hong, C.H.L. Role of Oral Flora in Chemotherapy-Induced Oral Mucositis in Vivo. Archives of Oral Biology 2019, 101, 51–56. [Google Scholar] [CrossRef]
- Hong, B.-Y.; Sobue, T.; Choquette, L.; Dupuy, A.K.; Thompson, A.; Burleson, J.A.; Salner, A.L.; Schauer, P.K.; Joshi, P.; Fox, E.; et al. Chemotherapy-Induced Oral Mucositis Is Associated with Detrimental Bacterial Dysbiosis. Microbiome 2019, 7, 66. [Google Scholar] [CrossRef]
- Subramaniam, N.; Muthukrishnan, A. Oral Mucositis and Microbial Colonization in Oral Cancer Patients Undergoing Radiotherapy and Chemotherapy: A Prospective Analysis in a Tertiary Care Dental Hospital. Journal of Investigative and Clinical Dentistry 2019, 10, e12454. [Google Scholar] [CrossRef]
- Motoori, M.; Yano, M.; Miyata, H.; Sugimura, K.; Saito, T.; Omori, T.; Fujiwara, Y.; Miyoshi, N.; Akita, H.; Gotoh, K.; et al. Randomized Study of the Effect of Synbiotics during Neoadjuvant Chemotherapy on Adverse Events in Esophageal Cancer Patients. Clinical Nutrition 2017, 36, 93–99. [Google Scholar] [CrossRef]
- Al-Qadami, G.; Bowen, J.; Van Sebille, Y.; Secombe, K.; Dorraki, M.; Verjans, J.; Wardill, H.; Le, H. Baseline Gut Microbiota Composition Is Associated with Oral Mucositis and Tumour Recurrence in Patients with Head and Neck Cancer: A Pilot Study. Support Care Cancer 2023, 31, 98. [Google Scholar] [CrossRef]
- Al-Qadami, G.; Van Sebille, Y.; Bowen, J.; Wardill, H. Oral-Gut Microbiome Axis in the Pathogenesis of Cancer Treatment-Induced Oral Mucositis. Front. Oral. Health 2022, 3. [Google Scholar] [CrossRef]
- Jiang, C.; Wang, H.; Xia, C.; Dong, Q.; Chen, E.; Qiu, Y.; Su, Y.; Xie, H.; Zeng, L.; Kuang, J.; et al. A Randomized, Double-Blind, Placebo-Controlled Trial of Probiotics to Reduce the Severity of Oral Mucositis Induced by Chemoradiotherapy for Patients with Nasopharyngeal Carcinoma. Cancer 2019, 125, 1081–1090. [Google Scholar] [CrossRef]
- Sharma, A.; Rath, G.K.; Chaudhary, S.P.; Thakar, A.; Mohanti, B.K.; Bahadur, S. Lactobacillus Brevis CD2 Lozenges Reduce Radiation- and Chemotherapy-Induced Mucositis in Patients with Head and Neck Cancer: A Randomized Double-Blind Placebo-Controlled Study. European Journal of Cancer 2012, 48, 875–881. [Google Scholar] [CrossRef]
- Xiao, H.; Fan, Y.; Li, Y.; Dong, J.; Zhang, S.; Wang, B.; Liu, J.; Liu, X.; Fan, S.; Guan, J.; et al. Oral Microbiota Transplantation Fights against Head and Neck Radiotherapy-Induced Oral Mucositis in Mice. Computational and Structural Biotechnology Journal 2021, 19, 5898–5910. [Google Scholar] [CrossRef]
- Xia, C.; Jiang, C.; Li, W.; Wei, J.; Hong, H.; Li, J.; Feng, L.; Wei, H.; Xin, H.; Chen, T. A Phase II Randomized Clinical Trial and Mechanistic Studies Using Improved Probiotics to Prevent Oral Mucositis Induced by Concurrent Radiotherapy and Chemotherapy in Nasopharyngeal Carcinoma. Front. Immunol. 2021, 12. [Google Scholar] [CrossRef]
Figure 1.
Schematic representation of the five-phase biological progression of chemotherapy- and/or radiotherapy-induced oral mucositis. In Phase I (Initiation), radiotherapy and chemotherapy generate reactive oxygen species (ROS), causing DNA damage and activating innate immune cells. Phase II (Primary Damage Response) involves NF-κB activation and the release of proinflammatory cytokines such as TNF-α, IL-1β, and IL-6. In Phase III (Signal Amplification), cytokine toxicity intensifies inflammation and tissue injury through positive feedback mechanisms. Phase IV (Ulceration) is characterized by epithelial breakdown and bacterial invasion, further exacerbating mucosal damage. Finally, in Phase V (Healing), anti-inflammatory cytokines and growth factors promote epithelial regeneration and mucosal restoration. Created in BioRender. Zhou, J. (2026) https://BioRender.com/ltvdniq.
Figure 1.
Schematic representation of the five-phase biological progression of chemotherapy- and/or radiotherapy-induced oral mucositis. In Phase I (Initiation), radiotherapy and chemotherapy generate reactive oxygen species (ROS), causing DNA damage and activating innate immune cells. Phase II (Primary Damage Response) involves NF-κB activation and the release of proinflammatory cytokines such as TNF-α, IL-1β, and IL-6. In Phase III (Signal Amplification), cytokine toxicity intensifies inflammation and tissue injury through positive feedback mechanisms. Phase IV (Ulceration) is characterized by epithelial breakdown and bacterial invasion, further exacerbating mucosal damage. Finally, in Phase V (Healing), anti-inflammatory cytokines and growth factors promote epithelial regeneration and mucosal restoration. Created in BioRender. Zhou, J. (2026) https://BioRender.com/ltvdniq.
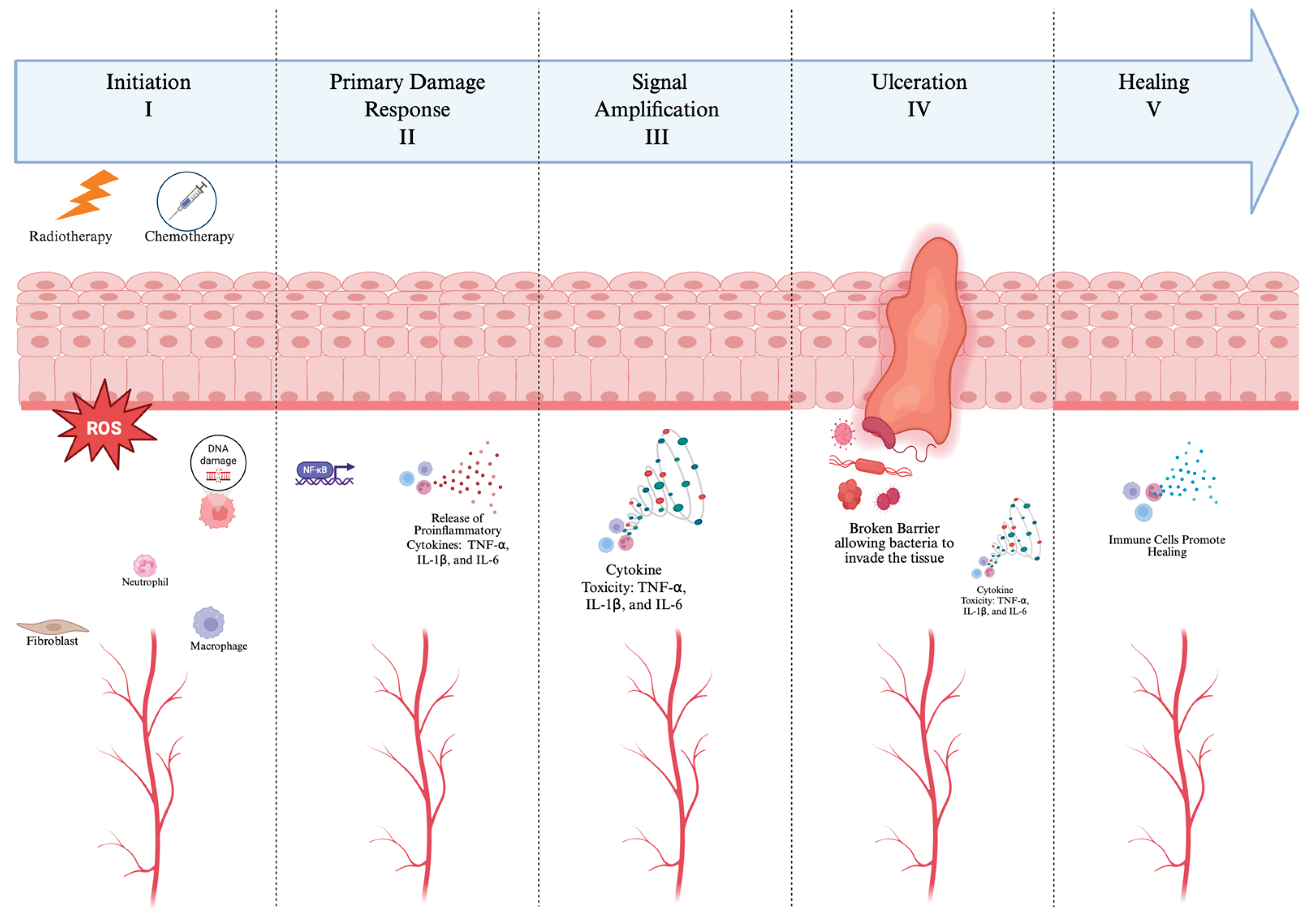
Figure 2.
Overview of anti-inflammatory therapeutic strategies and their mechanisms of action in alleviating chemotherapy- and/or radiotherapy-induced oral mucositis. Pentoxifylline, atorvastatin, and trans-caryophyllene suppress TNF, IFN-γ, and TGF-β to reduce inflammation and enhance re-epithelialization. Azilsartan (AZT) blocks angiotensin II signalling, decreases TNF and IL-1β, increases IL-10, and upregulates growth factors such as VEGF, FGF, KGF, and TGF-α to accelerate tissue repair. Recombinant human IL-11 (rhIL-11) downregulates IL-1β and TNF to lower mucosal cytokine load and preserve epithelial integrity. Low-level laser therapy (LLLT) further decreases TNF, IL-6, and IL-8 expression, exerting biomodulatory effects that reduce inflammation and promote mucosal healing. Created in BioRender. Zhou, J. (2026) https://BioRender.com/suvb78i.
Figure 2.
Overview of anti-inflammatory therapeutic strategies and their mechanisms of action in alleviating chemotherapy- and/or radiotherapy-induced oral mucositis. Pentoxifylline, atorvastatin, and trans-caryophyllene suppress TNF, IFN-γ, and TGF-β to reduce inflammation and enhance re-epithelialization. Azilsartan (AZT) blocks angiotensin II signalling, decreases TNF and IL-1β, increases IL-10, and upregulates growth factors such as VEGF, FGF, KGF, and TGF-α to accelerate tissue repair. Recombinant human IL-11 (rhIL-11) downregulates IL-1β and TNF to lower mucosal cytokine load and preserve epithelial integrity. Low-level laser therapy (LLLT) further decreases TNF, IL-6, and IL-8 expression, exerting biomodulatory effects that reduce inflammation and promote mucosal healing. Created in BioRender. Zhou, J. (2026) https://BioRender.com/suvb78i.
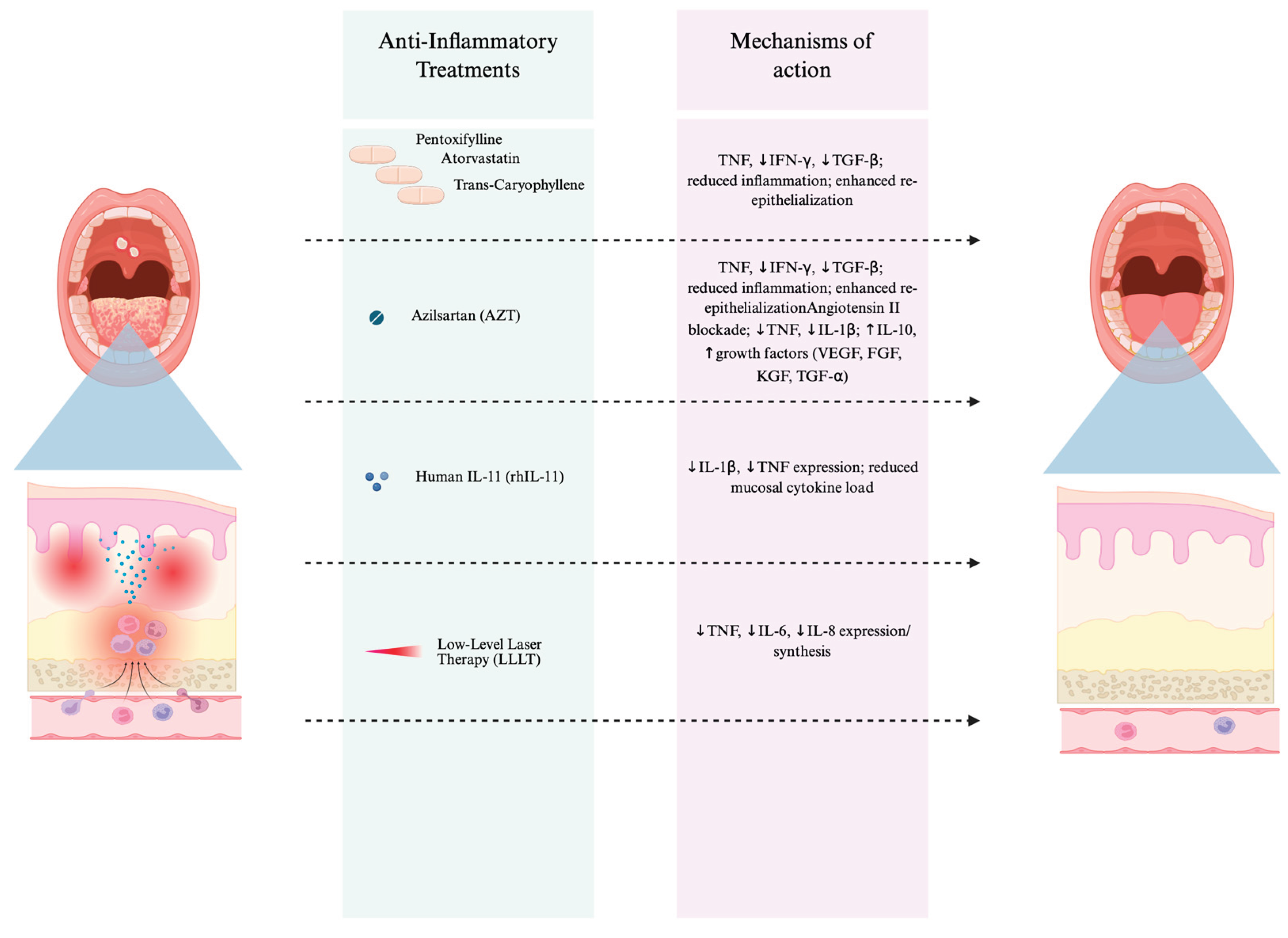
Figure 3.
Overview of microbiome-modulating therapeutic approaches and their mechanisms of action in alleviating chemotherapy- and/or radiotherapy-induced oral mucositis. The figure illustrates two interventions: oral microbiota transplantation (OMT), which restores microbial diversity, decreases IL-1, IL-6, TNF, and TGF-β levels, and upregulates S100a9 expression to promote mucosal repair; and a modified probiotic cocktail containing Lactobacillus plantarum, Bifidobacterium animalis, Lactobacillus rhamnosus, and Lactobacillus acidophilus, which restores the gut–oral microbiome balance, suppresses NF-κB, TLR4, IL-1β, IL-6, and TNF expression, enhances epithelial barrier proteins (ZO-1, Claudin-1), and increases T-cell levels. Together, these microbiome-targeted therapies mitigate inflammation, improve epithelial integrity, and promote recovery from oral mucositis. Created in BioRender. Zhou, J. (2026) https://BioRender.com/5oggw05.
Figure 3.
Overview of microbiome-modulating therapeutic approaches and their mechanisms of action in alleviating chemotherapy- and/or radiotherapy-induced oral mucositis. The figure illustrates two interventions: oral microbiota transplantation (OMT), which restores microbial diversity, decreases IL-1, IL-6, TNF, and TGF-β levels, and upregulates S100a9 expression to promote mucosal repair; and a modified probiotic cocktail containing Lactobacillus plantarum, Bifidobacterium animalis, Lactobacillus rhamnosus, and Lactobacillus acidophilus, which restores the gut–oral microbiome balance, suppresses NF-κB, TLR4, IL-1β, IL-6, and TNF expression, enhances epithelial barrier proteins (ZO-1, Claudin-1), and increases T-cell levels. Together, these microbiome-targeted therapies mitigate inflammation, improve epithelial integrity, and promote recovery from oral mucositis. Created in BioRender. Zhou, J. (2026) https://BioRender.com/5oggw05.
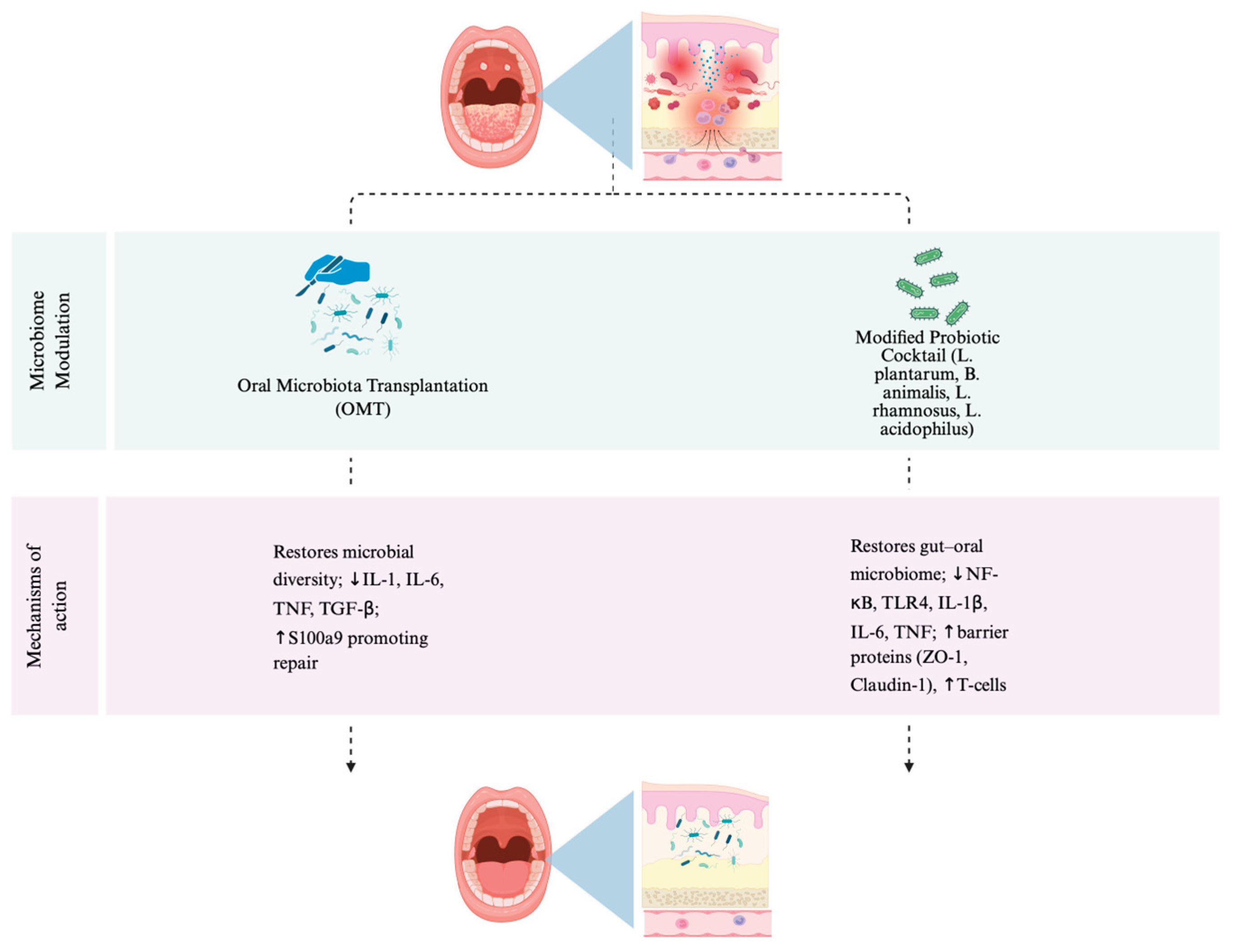

Table 1.
Summary of anti-inflammatory approaches alleviating chemotherapy- and/or radiotherapy-induced oral mucositis.
Table 1.
Summary of anti-inflammatory approaches alleviating chemotherapy- and/or radiotherapy-induced oral mucositis.
| Treatment | Mechanism | Type of Experiment | Model | Outcome | Reference |
|---|---|---|---|---|---|
| Pentoxifylline, Atorvastatin, Trans-Caryophyllene | ↓TNF, ↓IFN-γ, ↓TGF-β; reduced inflammation; enhanced re-epithelialization | In vivo | Wistar rats, 5-FU-induced OM | Attenuation of Oral Mucositis | [30] |
| Azilsartan (AZT) | Angiotensin II blockade; ↓TNF, ↓IL-1β; ↑IL-10, ↑growth factors (VEGF, FGF, KGF, TGF-α) | In vivo | Syrian hamsters, 5-FU-induced OM | Attenuation of Oral Mucositis | [31] |
| Recombinant Human IL-11 (rhIL-11) | ↓IL-1β, ↓TNF expression; reduced mucosal cytokine load | In vivo | Golden Syrian hamsters, radiation-induced OM | Attenuation of Oral Mucositis | [32] |
| Low-Level Laser Therapy (LLLT) | ↓TNF, ↓IL-6, ↓IL-8 expression/synthesis | In vitro | Human gingival fibroblasts (LPS-stimulated) | Attenuation of Oral Mucositis | [33] |
Table 2.
Summary of microbiome-modulating approaches alleviating chemotherapy- and/or radiotherapy-induced oral mucositis.
Table 2.
Summary of microbiome-modulating approaches alleviating chemotherapy- and/or radiotherapy-induced oral mucositis.
| Treatment | Mechanism | Type of Experiment | Model | Outcome | Reference |
|---|---|---|---|---|---|
| Oral Microbiota Transplantation (OMT) | Restores microbial diversity; ↓IL-1, IL-6, TNF, TGF-β; ↑S100a9 promoting repair | In vivo + clinical comparison | Mouse model + patients with head and neck cancer | Attenuation of Oral Mucositis | [47] |
| Modified Probiotic Cocktail (L. plantarum, B. animalis, L. rhamnosus, L. acidophilus) | Restores gut–oral microbiome; ↓NF-κB, TLR4, IL-1β, IL-6, TNF; ↑barrier proteins (ZO-1, Claudin-1), ↑T-cells | Clinical trial + in vivo rat model | NPC patients (CCRT) and the busulfan rat model | Attenuation of Oral Mucositis | [48] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



