Submitted:
11 February 2026
Posted:
12 February 2026
You are already at the latest version
Abstract
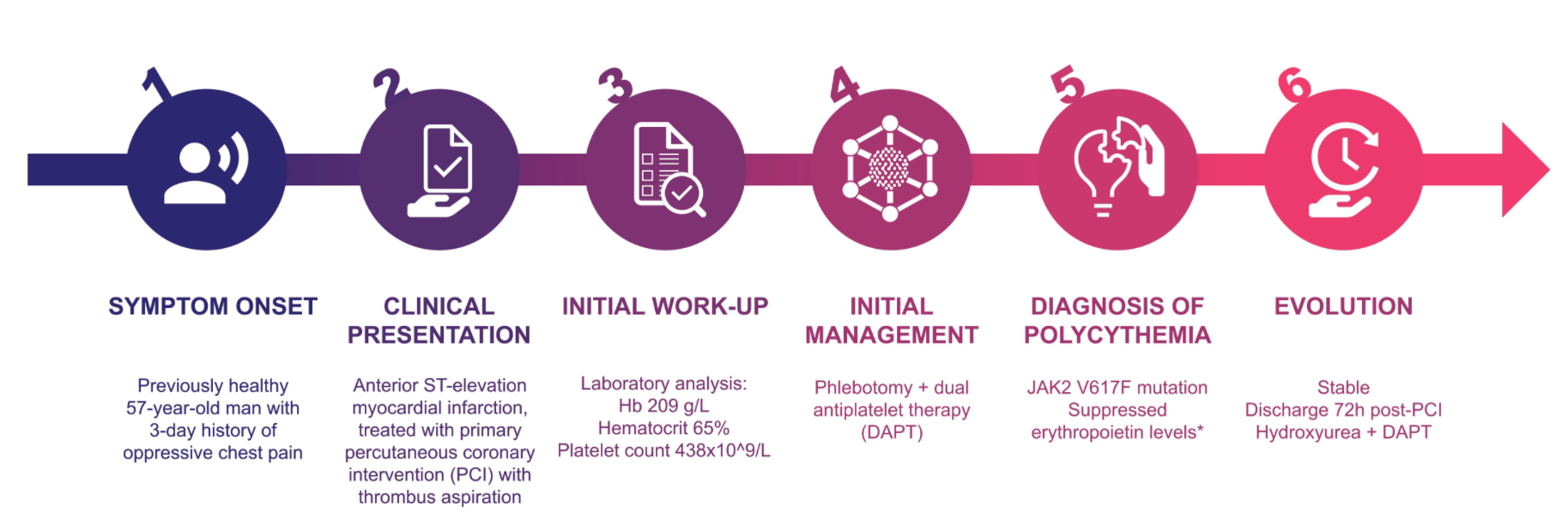
Background: Polycythemia vera is a myeloproliferative neoplasm associated with a high risk of thrombosis. While well-documented, acute coronary syndromes as the initial manifestation of polycythemia vera are rare. Case Summary: We report the case of a previously healthy 57-year-old male with no cardiovascular risk factors who presented with an anterior ST-elevation myocardial infarction. Coronary angiography revealed a subocclusive lesion in the left anterior descending artery, which was successfully treated with primary percutaneous coronary intervention. Initial laboratory tests revealed elevated hemoglobin (209 g/L) and haematocrit (65%), along with thrombocytosis (438 x 109/L). The combination of a single-vessel coronary lesion in a patient without conventional risk factors and the presence of hematologic abnormalities raised suspicion for polycythemia vera. Subsequent investigation confirmed the diagnosis based on a positive JAK2 V617F mutation and suppressed erythropoietin levels. The patient was treated with therapeutic phlebotomy shortly after the angioplasty and later initiated hydroxyurea to maintain haematocrit < 45% in association with dual antiplatelet therapy. Conclusions: This case highlights a rare but critical presentation of acute myocardial infarction as the first clinical manifestation of polycythemia vera. It underscores the importance of considering polycythemia vera in the differential diagnosis for patients presenting with an acute coronary syndrome, especially in the absence of traditional cardiovascular risk factors. Early recognition and prompt therapeutic intervention are crucial to prevent future thrombotic events and improve patient prognosis.
Keywords:
polycythemia vera
; acute myocardial infarction
; coronary thrombosis
; myeloproliferative neoplasms
; JAK2 V617F mutation
; case report
1. Introduction
Polycythemia vera (PV) is a chronic myeloproliferative neoplasm characterised by clonal proliferation of pluripotent hematopoietic stem cells, predominantly leading to an absolute increase in red blood cell mass [1,2,3,4]. It is often accompanied by leukocytosis, thrombocytosis, and splenomegaly [3,4]. Morbidity and mortality result mainly from thrombotic/hemorrhagic complications and by transformation to overt myelofibrosis or acute leukemia [3,4,5]. Thrombosis stem from a multifactorial prothrombotic state, largely driven by JAK2 gene mutations present in most patients [1,2,3,6,7,8,9,10,11].
While cardiovascular events may occur, acute coronary syndrome (ACS) as the first manifestation is rare [8,10,11,12]. Prompt recognition of PV in patients with ACS is crucial, as early disease-directed therapy plays a pivotal role in preventing future thrombotic events. We report a 57-year-old man presenting with an anterior ST-elevation myocardial infarction (STEMI), in whom erythrocytosis and thrombocytosis led to PV diagnosis (low erythropoietin levels and a JAK2 V617F mutation), illustrating this rare presentation.
2. Case Description
A previously healthy 57-year-old man presented to the emergency department with oppressive chest pain after a 10-km walk, progressively worsening over three days. He had no cardiovascular risk factors or family history of coronary artery disease or sudden cardiac death.
On arrival, he was hypertensive (blood pressure 169/120 mmHg) with a normal heart rate and peripheral oxygen saturation on room air 91–95%. Physical examination was unremarkable. Electrocardiography showed anterior-lateral ST-segment elevation (Figure 1), consistent with an anterior STEMI. He received loading doses of aspirin and unfractionated heparin before expedited transfer for coronary angiography.
Angiography revealed a sub-occlusive proximal left anterior descending (LAD) artery lesion, and primary percutaneous coronary intervention (PCI) with thrombus aspiration and angioplasty restored flow (Figure 2). A transthoracic echocardiogram performed shortly thereafter demonstrated apical akinesia with preserved left ventricular ejection fraction, and no significant valvular disease.
Initial laboratory testing showed marked erythrocytosis and thrombocytosis: hemoglobin 209 g/L, haematocrit 65%, and platelets 438 × 109/L (Table 1). The lipid profile revealed triglycerides 0.97 mmol/L, HDL-cholesterol 1.06 mmol/L, and LDL-cholesterol 3.47 mmol/L. High-sensitivity troponin peaked at 17,837.8 pg/mL (ULN 28.9–39.2 pg/mL). In a patient with an acute arterial thrombotic event and no conventional cardiovascular risk factors, the single-vessel culprit pattern together with the hematologic abnormalities prompted evaluation for an underlying myeloproliferative neoplasm, particularly PV.
Despite hydration, erythrocytosis and an elevated haematocrit persisted; therapeutic phlebotomy was performed 8 hours post-angiography. Subsequent etiologic evaluation for polycythemia identified a JAK2 V617F mutation and a suppressed serum erythropoietin level (<0.6 mU/mL; reference interval 2.6–19 mU/mL), fulfilling the 2016 WHO diagnostic criteria for PV.
Throughout hospitalisation, the patient remained hemodynamically stable (Killip class I) without aquagenic pruritus, headache, visual disturbances, or other features of additional arterial or venous thrombosis. No further hypertensive episodes were recorded during hospitalisation. Hospital course was uneventful, and he was discharged after 72 hours. During the 1-year follow-up, the patient remained asymptomatic and experienced no cardiovascular events.
4. Discussion
Acute myocardial infarction as the sentinel manifestation of PV is very uncommon, with fewer than 15 reported cases [6,10,11,12,13]. This case illustrates the importance of carefully integrating clinical, angiographic, and hematologic data to reveal occult PV.
Non-modifiable risk factors for PV include advanced age, male sex, and European descent, while modifiable risk factors comprise smoking, obesity, hypertension, diabetes mellitus, and hyperlipidemia [2]. Beyond its etiology, PV is associated with a substantial symptom burden, with dizziness, headaches, visual disturbances, erythromelalgia, distal paresthesia, and acrocyanosis having a marked impact on quality of life [2,3,4]. The disease also carries a high risk of morbidity and mortality, characterized by hemorrhagic complication rates of approximately 4% [2,6] and thrombotic complication rates ranging from 20% to 40% during follow-up, of which approximately 50% are arterial events [1,4,6]. While long-term reports show that myocardial infarction occurs in 11.4% of PV cases over 10 years [10], STEMI as the presenting event of PV is exceptionally rare.
The combination of single-vessel STEMI, marked erythrocytosis and thrombocytosis, and JAK2 V617F positivity strongly supports PV as the culprit mechanism. The mildly elevated LDL and absence of diffuse atherosclerosis, together with thrombus aspiration findings and exclusion of other prothrombotic conditions —including atrial fibrillation, malignancy, and autoimmune disease, argue against typical atherosclerotic infarction.
Multiple mechanisms plausibly converged to precipitate coronary thrombosis in this setting. Elevated haematocrit increases whole-blood viscosity, reduces microvascular perfusion, and amplifies shear stress; conditions that favor platelet activation and thrombin generation [5]. PV further entails qualitative platelet and leukocyte abnormalities that promote adhesion and intravascular thrombosis, even when angiographic atherosclerosis is limited. In addition, JAK2-driven signaling enhances endothelial activation and procoagulant pathways [7]. Red-cell adhesiveness, mediated in part by Lu/BCAM activation downstream of JAK2 V617F, provides an additional prothrombotic substrate [7]. Neutrophil extracellular traps (NETs) have also been implicated in myeloproliferative neoplasms and may contribute to arterial and venous events [8]. The resulting milieu can trigger an acute LAD event with relatively modest underlying plaque burden.
Diagnosis followed WHO 2016 diagnostic criteria for PV (Table 2): absolute erythrocytosis, JAK2 V617F positivity, and subnormal erythropoietin. Bone marrow biopsy was not required, as sustained absolute erythrocytosis plus clonal marker and low EPO suffice for diagnosis [14]. Importantly, the biochemical profile and oxygen saturation trajectory argue against secondary causes of erythrocytosis; a low EPO is particularly helpful in distinguishing PV from hypoxia-driven or exogenous etiologies (including common causes such as smoking, obstructive sleep apnea, obesity-hypoventilation syndrome, chronic hypoxia) [2].
Following prompt reperfusion of the proximal LAD, management centered on PV risk reduction. Persistent erythrocytosis after hydration prompted therapeutic phlebotomy, targeting a haematocrit <45% per CYTO-PV5. Low-dose aspirin is recommended in PV and can be continued alongside the post-PCI antiplatelet regimen when not contraindicated [3,4,5]. For long-term prevention, contemporary frameworks classify patients as high risk if ≥60 years or with a history of thrombosis; although <60 years, the index myocardial infarction fulfills the latter criterion, supporting initiation of cytoreductive therapy to reduce recurrent events and the need for phlebotomy [3,4,5]. Hydroxyurea is the preferred first-line agent, with pegylated interferon-α as an alternative—particularly in younger patients or when fertility and cytopenia considerations favor its use [2,4]. Accordingly, given high-risk PV, dual antiplatelet therapy was maintained and hydroxyurea was initiated to maintain Htc < 45%, with coordinated follow-up in Cardiology and Hematology.
Regarding prognosis, risk factors for survival include advanced age, leukocytosis, and a history of thrombosis [2,4]. Furthermore, prior arterial events, hyperlipidemia, and hypertension have been identified as predictors of subsequent arterial events in a multivariate analysis by Cerquozzi et al. [9] These facts make the current case particularly noteworthy.
This case emphasizes that MI without conventional risk factors — especially single-vessel disease plus erythrocytosis/thrombocytosis — screening for PV (CBC trends, serum EPO, and JAK2) is inexpensive and may prevent recurrent arterial or venous events through timely cytoreduction and haematocrit control.
5. Conclusions
In conclusion, this case report highlights the exceptional presentation of an AMI as the first clinical manifestation of previously unrecognized PV. In patients with ACS and unexplained erythrocytosis/thrombocytosis, clinicians should suspect PV. Early diagnosis is crucial, as timely cytoreductive therapy and haematocrit control can significantly reduce future cardiovascular risk.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/doi/s1, Figure S1: title; Table S1: title; Video S1: title.
Funding
This research received no external funding.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACS MDPI |
Acute Coronary Syndrome Multidisciplinary Digital Publishing Institute |
| DOAJ LAD PCI PV STEMI |
Directory of open access journals Left Anterior Descending Artery Percutaneous Coronary Intervention Polycythemia vera ST-Elevation Myocardial Infarction |
References
- Waggoner, M. Polycythemia vera: thinking beyond the hematocrit. J Adv Pract Oncol. 2023, 14(5), 405. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.; Griffin, L.; Harris, D.R. Polycythemia vera: rapid evidence review. Am Fam Physician 2021, 103(11), 680–687. [Google Scholar] [CrossRef] [PubMed]
- Mesa, R.A. New guidelines from the NCCN for polycythemia vera. Clin Adv Hematol Oncol. 2017, 15(11), 848. [Google Scholar] [PubMed]
- Tefferi, A.; Barbui, T. Polycythemia vera: 2024 update on diagnosis, risk-stratification, and management. Am J Hematol. 2023, 98(9), 1465–1487. [Google Scholar] [CrossRef] [PubMed]
- Marchioli, R.; Finazzi, G.; Specchia, G.; Cacciola, R.; Cavazzina, R.; Cilloni, D.; De Stefano, V.; Elli, E.; Iurlo, A.; Latagliata, R.; Lunghi, F. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013, 368(1), 22–33. [Google Scholar] [CrossRef] [PubMed]
- Cerquozzi, S.; Barraco, D.; Lasho, T.; Finke, C.; Hanson, C.A.; Ketterling, R.P.; Pardanani, A.; Gangat, N.; Tefferi, A. Risk factors for arterial versus venous thrombosis in polycythemia vera: a single center experience in 587 patients. Blood Cancer J. 2017, 7(12), 662. [Google Scholar] [CrossRef] [PubMed]
- Kroll, M.H.; Michaelis, L.C; Verstovsek, S. Mechanisms of thrombogenesis in polycythemia vera. Blood Rev. 2015, 29(4), 215–221. [Google Scholar] [CrossRef] [PubMed]
- Wolach, O.; Sellar, R.S.; Martinod, K.; Cherpokova, D.; McConkey, M.; Chappell, R.J.; Silver, A.J.; Adams, D.; Castellano, C.A.; Schneider, R.K.; Padera, R..F. Increased neutrophil extracellular trap formation promotes thrombosis in myeloproliferative neoplasms. Sci Transl Med. 2018, 10(436), eaan8292. [Google Scholar] [CrossRef] [PubMed]
- Landolfi, R.; Di Gennaro, L.; Barbui, T.; De Stefano, V.; Finazzi, G.; Marfisi, R.; Tognoni, G.; Marchioli, R. Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera. Blood 2007, 109(6), 2446–2452. [Google Scholar] [CrossRef] [PubMed]
- Manan, M.R.; Kipkorir, V.; Nawaz, I.; Waithaka, M.W.; Srichawla, B.S.; Gãman, A.M.; Diaconu, C.C.; Gãman, M.A. Acute myocardial infarction in myeloproliferative neoplasms. World J Cardiol. 2023, 15(11), 571. [Google Scholar] [CrossRef] [PubMed]
- Silveira, C.F.D.S.M.P.D.; Vitali, L.B.S.L.; Faustino, F.G.; Maurício, A.D.C.V.; Teixeira, R.; Bazan, S.G.Z. Acute myocardial infarction as first onset of polycythemia vera. Arq Bras Cardiol. 2020, 114, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Cengiz, B.; Aytekin, V.; Bildirici, U.; Sahin, S.T.; Yurdakul, S.; Aytekin, S.; Kucukkaya, R. A rare cause of acute coronary syndromes in young adults - myeloproliferative neoplasms: A case series. Rev Port Cardiol. 2019, 38(9), 613–617. [Google Scholar] [CrossRef] [PubMed]
- Okabe, H.; Sonoda, S.; Abe, K.; Doi, H.; Matsumura, T.; Otsuji, Y. Acute myocardial infarction following sequential multi-vessel occlusion in a case of polycythemia vera. J Cardiol Cases 2019, 20(4), 111–114. [Google Scholar] [CrossRef] [PubMed]
- Barbui, T.; Thiele, J.; Gisslinger, H.; Kvasnicka, H.M.; Vannucchi, A.M.; Guglielmelli, P.; Orazi, A.; Tefferi, A. The 2016 WHO classification and diagnostic criteria for myeloproliferative neoplasms: document summary and in-depth discussion. Blood Cancer J. 2018, 8(2), 15. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Electrocardiogram at admission with sinus rhythm and ST segment elevation in V3-V6.
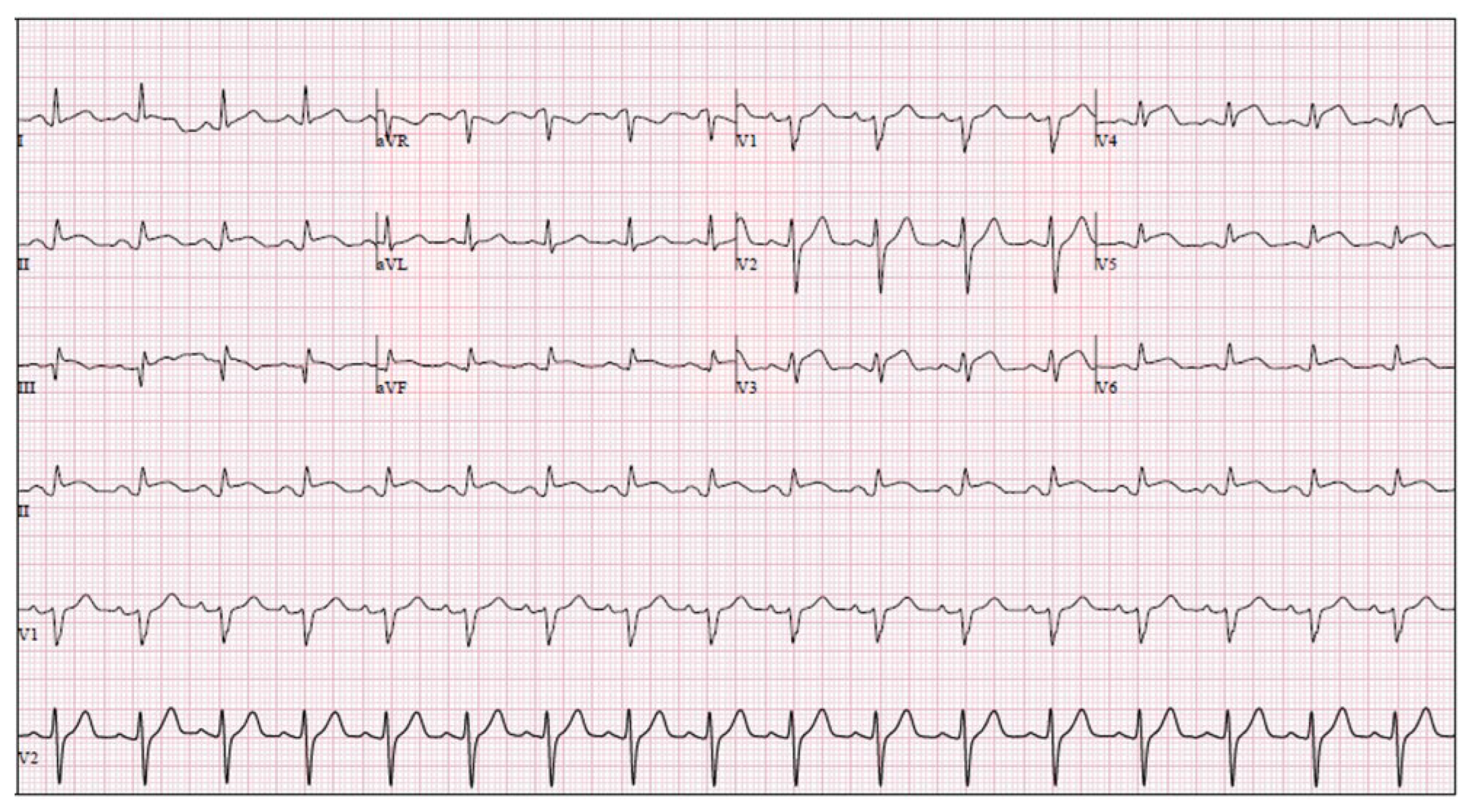
Figure 2.
Coronary angiography: (a and b) Pre-intervention views demonstrating a sub-occlusive culprit lesion in the proximal left anterior descending (LAD) artery with ostial involvement of the first diagonal branch; (c) final angiogram after primary percutaneous coronary intervention, showing resolution of the culprit stenosis and restored anterograde flow in the LAD.
Figure 2.
Coronary angiography: (a and b) Pre-intervention views demonstrating a sub-occlusive culprit lesion in the proximal left anterior descending (LAD) artery with ostial involvement of the first diagonal branch; (c) final angiogram after primary percutaneous coronary intervention, showing resolution of the culprit stenosis and restored anterograde flow in the LAD.
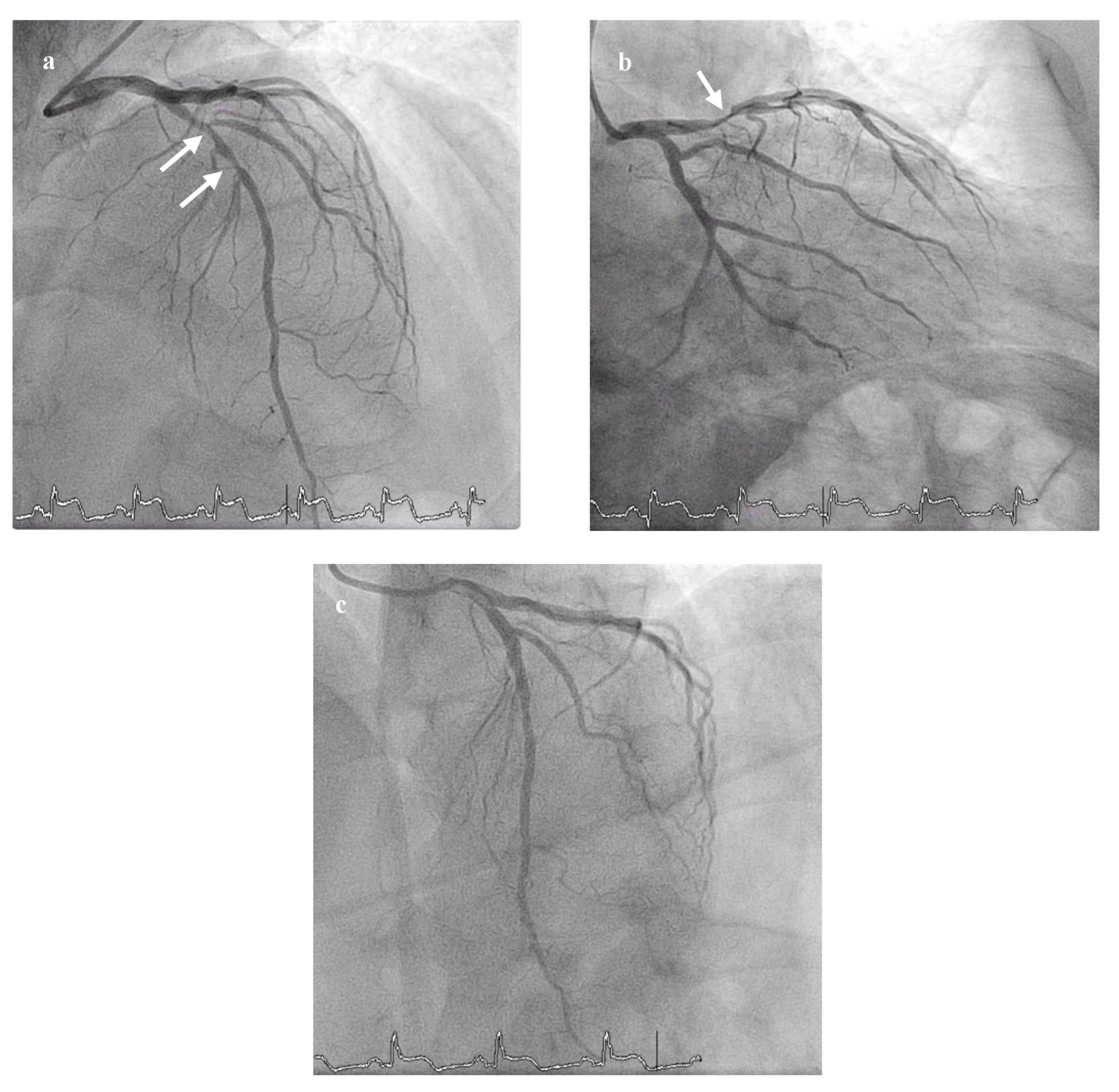

Table 1.
The patient’s clinical laboratory data.
| Blood test | Admission | Discharge | 1st Cardiology Appointment |
|---|---|---|---|
| Hemoglobin | 209 g/L | 179 g/L | |
| Haematocrit | 64.9% | 55.2% | |
| Erythrocytes | 7.91 x 109/L | 6.77 x 109/L | |
| Leucocytes | 9.0 x 109/L | 6.5 x 109/L | |
| Platelets | 438 x 109/L | 448 x 109/L | |
| LDL cholesterol | 3.47 mmol/L | ||
| HDL cholesterol | 1.06 mmol/L | ||
| Triglycerides | 0.97 mmol/L | ||
| hs-Troponin I | 6796 pg/mL | 2752 pg/mL | |
| Erythropoietin | < 0,6 mU/mL | ||
| JAK2 kinase mutation | JAK-2 V617F mutation: positive |
1 hs – high sensitivity.
Table 2.
2016 World Health Organization diagnostic criteria for polycythemia vera1.
| Major criteria |
|---|
| Hemoglobin > 16.5 g/dL (men) / > 16.0 g/dL (women) or Haematocrit > 49% (men) / > 48% (women) or increased red cell mass (RCM) |
| Bone Marrow biopsy showing hypercellularity for age with trilineage growth (panmyelosis) including prominent erythroid, granulocytic and megakaryocytic proliferation with pleomorphic, mature megakaryocytes (differences in size) |
| Presence of JAK2 or JAK2 exon 12 mutation |
| Minor criteria |
| Subnormal serum erythropoietin level |
| A diagnosis of PV can be established by satisfying the complete triad of major criteria, or by meeting the first two major criteria plus any one minor criteria |
1 Table adapted from Barbui et al. Blood Cancer J 2018; 8:15 [14].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



