Submitted:
11 February 2026
Posted:
12 February 2026
You are already at the latest version
Abstract
Background:
Heart failure (HF) is a major cause of morbidity in adults with congenital heart disease (ACHD), who may also have limited access to transplant. Intermittent levosimendan has shown benefit in advanced HF due to acquired heart disease, but currently there are no data in ACHD.
Methods:
We conducted a retrospective analysis of ACHD patients aged >18 years with advanced HF who received ≥3 intermittent levosimendan infusions between March 2020 and January 2026 at a tertiary ACHD centre. Clinical outcomes during follow-up were compared with those in the year preceding treatment. Primary endpoints included safety and HF-related adverse events, particularly HF hospitalizations. Secondary endpoints included changes in New York Heart Association (NYHA) class, NT-proBNP levels, and ventricular systolic function assessed by echocardiography.
Results:
Twelve patients (median age 44.6 years, 25% female) were included, with heterogeneous congenital diagnoses and advanced HF. Five patients had a systemic right ventricle (sRV) and one had a single ventricle with previous Fontan palliation. During a median follow-up of 1.3 years, intermittent levosimendan was generally well tolerated, with no treatment-limiting adverse events. HF hospitalization incidence significantly decreased from 0.83 events/person-year before treatment to 0.20 events/person-year during follow-up (p=0.03). NYHA functional class improved significantly (p=0.005). While no significant changes were observed in NT-proBNP or left ventricular ejection fraction, patients with an sRV demonstrated a significant improvement in right ventricular fractional area change (27±7.4% to 30.6±7%, p=0.02). Two deaths occurred, consistent with the severity of underlying disease and not directly attributable to levosimendan.
Conclusions:
In this real-world cohort of ACHD patients with advanced HF, intermittent levosimendan administration was safe and associated with improved symptoms, reduced HF hospitalizations, and enhanced systemic right ventricular function. These findings support the potential role of intermittent levosimendan as a therapeutic option in selected ACHD patients and underscore the need for prospective, adequately powered studies to confirm efficacy and define optimal patient selection.
Keywords:
heart failure
; levosimendan
; ACHD
; congenital heart disease
; advance heart failure
* correspondence: flavia.fusco@ospedalideicolli.it; tel.: +390817064206
1. introduction
heart failure (hf) is highly prevalent among adults with congenital heart disease (achd) and its treatment in this complex population presents unique challenges that differ substantially from acquired heart disease. the underlying congenital anatomy, prior surgical repairs, heterogeneous hemodynamics, and frequent comorbidities complicate hf management in this population, and evidence for hf therapies is limited due to exclusion from most randomized trials and the absence of large dedicated studies. timing of referral for advanced therapies such as cardiac transplantation is also difficult, with many patients deemed ineligible due to complex anatomy, prior surgical history, elevated immunologic sensitization, or end-organ dysfunction — contributing to high waitlist mortality in achd candidates [1,2]. mechanical circulatory support, is often underutilized in achd, partly due to the lack of devices tailored to diverse anatomies and the technical challenges posed by complex anatomies [3]. in patients with refractory hf, intermittent administration of levosimendan—a calcium-sensitizing inotrope with vasodilatory properties—has been reported to improve haemodynamic status and quality of life, reduce hf hospitalizations [4], and facilitate optimization of background heart failure therapy [5]. in selected patients with acquired heart disease, intermittent levosimendan has been recommended as a viable option for bridge to cardiac transplantation by the 2024 guidelines for the evaluation and care of cardiac transplant candidates of the international society for heart and lung transplantation [6]. however, in patients with congenital heart disease, evidence remains extremely limited. to date, data are largely confined to reports of potential benefit in the perioperative setting in pediatric populations [7] and to a single case series describing three adults with advanced disease [8].
therefore, the present study aimed to describe the experience of our tertiary adult congenital heart disease centre with intermittent levosimendan administration in achd patients with advanced heart failure.
2. methods
2.1. patients’ selection and data collection
we retrospectively reviewed the digitally stored medical records at our tertiary centre for all patients with a diagnosis of congenital heart disease, aged >18 years with hf who received at least 3 levosimendan infusions between march 2020 and january 2026. exclusion criteria were absence of a congenital heart disease, age ≤18 years, receipt of fewer than three levosimendan infusions, incomplete medical records, peri-operative only or emergency use of levosimendan, non–hf indications (e.g. patients undergoing levosimendan treatment before cardiac catheterization only to verify improvement of baseline data allowing transplant listing). patients’ medical records were reviewed to collect data on the previous medical history, previous surgeries, medical treatment and clinical status at latest follow-up. adverse events recorded during follow-up included any hospitalization for cardiac causes; acute heart failure, defined as the rapid onset or worsening of symptoms and signs of fluid overload requiring urgent medical evaluation and treatment; sustained arrhythmias, defined as abnormal heart rhythms persisting for >30 seconds or requiring immediate medical intervention (electrical cardioversion or pharmacological treatment) due to haemodynamic instability; appropriate implantable cardioverter-defibrillator (icd) therapies (antitachycardia pacing or shocks); acute kidney injury (aki), defined as a clinical syndrome characterized by a rapid decline in renal function occurring within hours or days; death; and the need for heart transplantation.
the study was performed in line with the principles of the declaration of helsinki and approval was granted by institutional ethics committee. as the present study involved the retrospective analysis of data collected during clinical activity, the institutional review board waived the need for written patient informed consent.
2.2. levosimendan administration protocol
at our institution, the decision to initiate periodic levosimendan administration is made following a multidisciplinary case review, with a shared agreement that no alternative therapeutic options are available for the patient.
patients considered for intermittent levosimendan infusion may include those with:
- heart failure with reduced ejection fraction (hfref; ef <35%) refractory to guideline-directed medical therapy
- hfref patients already listed for heart transplantation with ongoing clinical instability
- hfref patients on optimized medical therapy with worsening symptoms with new york heart association (nyha) functional class>2, or recent hf hospitalization, prior to listing for transplantation, as a last attempt to achieve clinical recovery
- heart failure with preserved ejection fraction (hfpef) unresponsive to conventional therapy.
all patients evaluated for levosimendan administration at our institution undergo a comprehensive baseline assessment, including electrocardiography, physical examination, nyha functional class evaluation, transthoracic echocardiography, and laboratory testing. levosimendan was administered according to a standardized protocol based on periodic infusions. the first administration is usually a full dose (12.5 mg) over a 24-48 hours period and was performed in naïve patients during inpatient hospitalization to allow close monitoring for potential adverse events, particularly symptomatic hypotension and ventricular arrhythmias, as well as symptom evolution during infusion. patients with a baseline systolic blood pressure (sbp) <80 mmhg are generally considered ineligible for levosimendan therapy. in patients with baseline sbp between 80 and 90 mmhg, infusion is generally initiated at a reduced rate of 0.05 μg/kg/min. during infusion, patients undergo continuous ecg monitoring and periodic non-invasive blood pressure measurements. if sbp remains stable or within safety limits, the infusion rate might be increased after the first 60 minutes, up to a maximum of 0.2 μg/kg/min. patients who tolerate the initial infusion subsequently receive outpatient treatment, consisting of levosimendan 6.25 mg administered every two weeks over a 6-hour infusion. more fragile patients, or those with significant hypotension who are unable to tolerate an infusion rate of at least 0.1 μg/kg/min, continue treatment with 12.5 mg once monthly during inpatient hospitalization.
2.3. echocardiography
comprehensive echocardiographic exams were periodically performed utilizing a ge vivid-e80 machine (ge healthcare, wauwatosa, wi, usa). standard m-mode, 2-dimensional, color, pulsed and continuous-wave doppler images were acquired according to the european association of cardiovascular imaging guidelines [9]. left ventricular (lv) ef was assessed with biplane simpson’s method and global longitudinal strain (gls). for patients with a systemic right ventricle (srv), systolic function was assessed using a multiparametric approach with a combination of rigjht ventricular (rv) systolic function parameters: tapse, s-wave, fractional area change (fac), rvgls. diastolic function was evaluated with e/a and e/e’measurements. systolic pulmonary artery pressure (spap) was measured from the tricuspid regurgitation jet velocity applying the modified bernoulli equation [9], as recommended. analogously, in patients with a srv ventricular pressure was estimated from the mitral regurgitation jet. valvular regurgitation/stenosis severity was assessed using multiparametric evaluation in agreement with guidelines [9]. right atrial pressure was derived from the inferior vena cava diameter and collapsibility [9].
2.4. endpoints
primary endpoints included safety of levosimendan treatment and efficacy in reducing the number of adverse events in achd patients. events at follow-up were compared to those occurring in the year before treatment initiation. primary efficacy endpoints included:
- (a)
- death for any reason
- (b)
- new transplant listing/necessity of mechanical circulatory support (mcs)
- (c)
- unscheduled hospital admission for hf
- (d)
- occurrence of sustained ventricular tachycardia(vt), defined as vt>30s or non-sustained vt with symptoms, or icd appropriate therapies
- (e)
- a composite of both all the previous
safety was defined as the absence of adverse events. both efficacy and safety events were adjudicated by a consensus of the investigators.
secondary endpoints were quantifiable parameters, including nt-pro b natriuretic peptide (nt-probnp) and lv and srv systolic function assessed by echocardiography. additional endpoint was improvement in new york heart association (nyha) class.
2.5. statistical analysis
statistical analysis was performed using r (version 4.0.5). continuous variables were reported as mean±sd or median [iqr], according to data distribution. comparisons between baseline and follow-up data were assessed with the student t-test or with wilcoxon rank-sum test for paired samples. categorical variables were presented as frequencies (percentage of total). differences in proportions were evaluated with mcnemar’s test. incidence rates were calculated as events per person-year and compared between the pre-treatment period and follow-up using incidence rate differences. p-value< 0.05 was considered statistically significant.
3. results
3.1. study population
twelve patients met the inclusion criteria: 3 (25%) female, median age 44.6[35-61.3] years. demographic data, diagnosis and baseline characteristics of the study population are summarized in Table 1. half of patients had a biventricular physiology with a lv sustaining the systemic circulation (7 patients=58%), while a systemic right ventricle (srv), was present in 5 (41%) patients (4 due to congenitally corrected transposition of the great arteries and 1 due to transposition of the great arteries following atrial switch repair), and 1 one patient had univentricular heart with lv morphology and received fontan palliation with an extracardiac conduit. half of patients had severe disease complexity according to the anatomical classification [11]. before starting levosimendan, all patients had a history of at least 1 hf-related hospitalizations, with 50% with multiple previous acute hf decompensation episodes. six patients had at least 2 surgical and/or percutaneous procedures and 4 (33%) had an implantable defibrillator. the fontan-palliated patient was already in heart and live transplant list at baseline all patients had symptoms, as demonstrated by nyha class≥2. median nt-probnp was 1576[706-3023] pg/ml. baseline ef among patients with a slv (including the single ventricle patients) was 37.6±8%, while among patients with a srv baseline fac was 27±7.4%. however, 4(66%) out of the 6 patients with slv had biventricular failure with 3 showing predominantly rv failure (fac of 25±11%). median systolic pulmonary pressure estimated by echocardiography in patients with slv was 38[29.5-62]mmhg. cardiac catheterization data were available for 5(42%) patients (Table 2): two patients showed pulmonary arterial hypertension, one following atrial switch procedure and one with previous tetralogy of fallot repair.
3.2. levosimendan treatment
the indication for treatment initiation was acute decompensation in four cases (33%). after the first in-hospital administration, only three patients (25%) were selected for outpatient treatment. however, one patient with single-ventricle physiology and a previous fontan operation did not tolerate outpatient administration because of transient severe hypotension occurring two hours after infusion initiation; therefore, subsequent cycles were scheduled as in-hospital treatments at one-month intervals. all other patient underwent monthly in-hospital administration of 12.5 mg.
no severe adverse events requiring treatment interruption occurred during levosimendan infusions, and no episodes of sustained ventricular tachycardia were recorded. two patients temporarily discontinued treatment: one due to patient preference related to difficulty in reaching the hospital, although this patient subsequently experienced clinical deterioration and treatment was reinitiated; the second patient initially showed clinical improvement, leading to a planned treatment interruption, but developed fluid overload two months after suspension, prompting reinitiation of therapy. one patient continued treatment at local hospital after the first 7 dose administrations.
3.3. follow-up and secondary endpoints
median follow-up after initiation was 1.3[0.7-2.3] years. overall, patients received a median of 8.5 [6.2-15] doses over a median of 10.7[5.8-16.7] months. main findings at last evaluation and comparison with baseline data are showed in Table 3. at last evaluation, there was no significant improvement in ntprobnp values. however, patients reported significant symptoms reduction (Figure 1). moreover, blood test did not demonstrate significant renal function changes. patients with slv did not demonstrate significant ef increase. nevertheless, patients with a srv showed significant improvement of fac.
3.4. outcome
during follow-up, two deaths occurred: one patient with pulmonary hypertension died from an intercurrent pulmonary infection, and one patient experienced an arrhythmic death during hospitalization for routine levosimendan administration, occurring the day after treatment. no other ventricular tachycardia occurred. three hf hospitalizations occurred in 2 patients, in one case accompanied by acute kidney injury, which recovered completely. both patients were managed with i.v. diuretics and optimized medical therapy. two patients are currently under evaluation for transplant list inclusion. hf admission incidence significantly decreased from 0.83 (95% ci 0.39–1.50) events/person-year before treatment to 0.20 (95% ci 0.04–0.60) during follow-up (incidence rate difference, p = 0.03).
4. discussion
in this real-world cohort of complex achd patients with advanced hf, intermittent levosimendan administration was safe and associated with significant symptom improvement, increased rv fac in patients with a systemic right ventricle (srv), and a reduction in hf admissions during follow-up compared with the year prior to treatment initiation. deaths in our cohort were consistent with the severity of the underlying conditions, largely anticipated, and unrelated to treatment. the reduction in hf events is clinically meaningful, as recurrent hospitalizations substantially contribute to morbidity, healthcare utilization, and reduced quality of life in achd patients [10,11].
adult survival in complex congenital heart disease has improved substantially, leading to a growing population with late-onset hf that often remains refractory to conventional therapies. standard hf treatments, validated in acquired hf, have limited efficacy in achd, particularly in patients with fontan physiology [12,13] or srv [14], despite recent promising results from novel therapies [15,16,17,18]. in our cohort, a statistically significant improvement was observed only in fac among patients with srv, though the small sample size may have limited the ability to detect additional significant benefits. favorable but non-significant trends were noted for nt-probnp reduction and lv ef improvement.
mechanistically, levosimendan enhances cardiac performance by increasing contractility without raising myocardial oxygen demand and by reducing afterload through vasodilation, mediated by calcium sensitization and ca²⁺-dependent opening of atp-sensitive k⁺ channels in vascular smooth muscle cells [19]. these effects may be particularly beneficial in achd patients with failing srv or longstanding pressure-overload conditions, where traditional inotropes can exacerbate arrhythmogenic risk and adverse remodeling. the prolonged action of levosimendan’s active metabolite allows intermittent outpatient administration, potentially sustaining clinical benefits between treatments. while intermittent levosimendan use is well documented in general advanced hf populations, evidence specific to achd remains limited. a recent case series of three achd patients with advanced hf demonstrated symptomatic improvement and avoidance of hospital admissions with pulsed levosimendan, supporting its potential role in clinical practice [8]. other studies have shown levosimendan’s efficacy in treating postoperative low cardiac output syndrome (lcos) [20] and in reducing lcos incidence when administered prophylactically in children with congenital heart disease [7].
in broader hf populations, levosimendan’s unique pharmacologic properties have justified repeated intermittent use. the lion-heart study, a double-blind, randomized, placebo-controlled trial, demonstrated reductions in nt-probnp values and hf hospitalizations with intermittent levosimendan in outpatients with advanced chronic hf [21], with similar findings in a subsequent trial [22]. these data supported the level 2a recommendation for intermittent levosimendan in patients with organ hypoperfusion awaiting transplant, per the 2024 international society for heart and lung transplantation guidelines [6]. a recent multicenter retrospective study also showed reduced hf admissions with intermittent levosimendan in patients not eligible for transplant, supporting its use as a destination therapy [23]. however, a randomized trial in patients with severe, potentially reversible cardiogenic shock on extracorporeal membrane oxygenation (ecmo) found that early levosimendan did not significantly shorten time to ecmo weaning compared with placebo [24]. in addition, a randomized controlled study in a small cohort of patients with hf with preserved ejection fraction (hfpef) showed that pulsed levosimendan administration was associated with reductions in pulmonary capillary wedge pressure and improvements in exercise tolerance [25]. these preliminary findings have stimulated further investigation into hfpef associated with pulmonary hypertension, including the development of an oral formulation of levosimendan [26]. on this basis, and given the high prevalence of refractory hf with preserved systolic function in achd, at our institution we started to considere levosimendan infusion also in selected achd patients with preserved ventricular systolic function. notably, a meta-analysis of eight randomized studies demonstrated that levosimendan improves right ventricular systolic function and reduces pulmonary artery pressure [27], findings of particular relevance to the achd population, which encompasses a high proportion of rv failure.
unlike large trials in acquired hf, achd studies have largely been small cohorts or case series, limiting conclusions about benefit magnitude and optimal dosing. our study has several limitations. first, its retrospective design and small sample size preclude definitive causal inference and increase selection bias risk. second, the heterogeneity of congenital lesions and physiology complicates generalizability, as responses may differ between subgroups (e.g., srv vs. slv vs. single ventricle physiology). for this reason, we analyzed lv ef and srv fac separately, further reducing sample size and statistical power. third, objective measures such as exercise capacity, biomarker trends, and formal quality-of-life instruments were not systematically collected, emphasizing the need for prospective evaluation. finally, although levosimendan was generally well tolerated, rare adverse events may not be captured in small cohorts.
5. conclusion
in this real-world cohort of achd patients with advanced hf, intermittent levosimendan was associated with significant symptom improvement, reduced hf admissions compared with the preceding year, and improved rv function in patients with srv. these findings align with limited achd case series and broader registry data in acquired hf, suggesting that levosimendan may reduce hospitalization burden and improve clinical stability in selected patients. prospective, adequately powered studies are needed to confirm these results, define optimal dosing, and identify patient subgroups most likely to benefit.
References
- Merás, P; Riesgo-Gil, F; Rybicka, J; Barradas-Pires, A; Smith, J; Kempny, A; Brookes, P; Simon, A; Gatzoulis, MA. Heart transplantation at a single tertiary adult congenital heart disease centre: Too little, too late? Int J Cardiol 2021, 322, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Meshulami, N; Shah, P; Kaushik, S; Murthy, R. Cardiac transplantation in adult congenital heart disease: a narrative review. J Thorac Dis. 2023, 15(9), 5074–5087. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cedars, A; Vanderpluym, C; Koehl, D; Cantor, R; Kutty, S; Kirklin, JK. An Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) analysis of hospitalization, functional status, and mortality after mechanical circulatory support in adults with congenital heart disease. J Heart Lung Transplant. 2018, 37(5), 619–630. [Google Scholar] [CrossRef] [PubMed]
- Masarone, D; Kittleson, MM; Pollesello, P; Marini, M; Iacoviello, M; Oliva, F; Caiazzo, A; Petraio, A; Pacileo, G. Use of Levosimendan in Patients with Advanced Heart Failure: An Update. J Clin Med. 2022, 11(21), 6408. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Masarone, D; Kittleson, MM; Martucci, ML; Valente, F; Gravino, R; Verrengia, M; Ammendola, E; Contaldi, C; Di Palma, V; Caiazzo, A; Petraio, A; Pollesello, P; Pacileo, G. Levosimendan as a "Bridge to Optimization" in Patients with Advanced Heart Failure with Reduced Ejection-A Single-Center Study. J Clin Med. 2022, 11(14), 4227. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Peled, Y; Ducharme, A; Kittleson, M; Bansal, N; Stehlik, J; Amdani, S; Saeed, D; Cheng, R; Clarke, B; Dobbels, F; Farr, M; Lindenfeld, J; Nikolaidis, L; Patel, J; Acharya, D; Albert, D; Aslam, S; Bertolotti, A; Chan, M; Chih, S; Colvin, M; Crespo-Leiro, M; D'Alessandro, D; Daly, K; Diez-Lopez, C; Dipchand, A; Ensminger, S; Everitt, M; Fardman, A; Farrero, M; Feldman, D; Gjelaj, C; Goodwin, M; Harrison, K; Hsich, E; Joyce, E; Kato, T; Kim, D; Luong, ML; Lyster, H; Masetti, M; Matos, LN; Nilsson, J; Noly, PE; Rao, V; Rolid, K; Schlendorf, K; Schweiger, M; Spinner, J; Townsend, M; Tremblay-Gravel, M; Urschel, S; Vachiery, JL; Velleca, A; Waldman, G; Walsh, J.; Hummel, J; Rücker, G; Stiller, B.; International Society for Heart and Lung Transplantation Guidelines for the Evaluation and Care of Cardiac Transplant Candidates-2024. Prophylactic levosimendan for the prevention of low cardiac output syndrome and mortality in paediatric patients undergoing surgery for congenital heart disease. J Heart Lung Transplant.;Cochrane Database Syst Rev 2024, 43(10) 8(8), 1529–1628.e54 CD011312. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wannaz, L; Boillat, L; Perez, MH; Di Bernardo, S. Prophylactic use of levosimendan in preoperative setting for surgical repair of congenital heart disease in children. Front Pediatr. 2023, 11, 1205971. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cranley, J; Hardiman, A; Freeman, LJ. Pulsed Levosimendan in advanced heart failure due to congenital heart disease: a case series. Eur Heart J Case Rep. 2020, 4(3), 1–6. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lang, RM; Badano, LP; Mor-Avi, V; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2015, 28, 1–39. [Google Scholar] [CrossRef]
- Menachem, JN; Schlendorf, KH; Mazurek, JA; Bichell, DP; Brinkley, DM; Frischhertz, BP; Mettler, BA; Shah, AS; Zalawadiya, S; Book, W; Lindenfeld, J. Advanced Heart Failure in Adults With Congenital Heart Disease. JACC Heart Fail 2020, 8(2), 87–99. [Google Scholar] [CrossRef] [PubMed]
- Ly, R; Karsenty, C; Amedro, P; Cohen, S; Domanski, O; Godart, F; Radojevic, J; Vaksmann, G; Naccache, N; Boubrit, A; Bataille, V; Hascoet, S; Ladouceur, M. Health-Related Quality of Life and Its Association With Outcomes in Adults With Congenital Heart Disease and Heart Failure: Insight From FRESH-ACHD Registry. J Am Heart Assoc. 2023, 12(8), e027819. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lubert, AM; Cedars, A; Almond, CS; Amdani, S; Conway, J; Friedland-Little, JM; Gajarski, RJ; Kindel, SJ; Lorts, A; Morales, DLS; O'Connor, MJ; Peng, DM; Rosenthal, DN; Smyth, L; Sutcliffe, DL; Schumacher, KR. Considerations for Advanced Heart Failure Consultation in Individuals With Fontan Circulation: Recommendations From ACTION. Circ Heart Fail 2023, 16(2), e010123. [Google Scholar] [CrossRef] [PubMed]
- Barracano, R; Merola, A; Fusco, F; Scognamiglio, G; Sarubbi, B. Protein-losing enteropathy in Fontan circulation: Pathophysiology, outcome and treatment options of a complex condition. Int J Cardiol Congenit Heart Dis 2022, 7, 100322. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Misra, A; Rodriguez-Monserrate, CP; Gauvreau, K; Dellborg, M; Fusco, F; Gupta, T; Kay, J; Kutty, S; Kauling, RM; Nicolarsen, J; Roos-Hesselink, J; John, AS; Wong, J; Burchill, LJ; Krieger, EV; Lubert, AM; Gallego, P; Kuo, M; Aboulhosn, J; Cramer, J; Antonova, P; Baker, D; Dehghani, P; Opotowsky, AR; van Dissel, A; Grewal, J; Yeung, E; Fernandes, S; Ginde, S; Khairy, P; Han, F; Muhll, IV; Wilson, WM; Kay, WA; Pylypchuk, S; Sarubbi, B; O'Donnell, C; Rodriguez, F, 3rd; Jayadeva, PS; Celermajer, DS; Shah, S; Cotts, T; DeZorzi, C; Magalski, A; Valente, AM; Broberg, CS. Propensity Score Analysis of Possible Medication Effects on Outcomes in Patients With Systemic Right Ventricles. JACC Adv. 2024, 4(1), 101443. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fusco, F; Scognamiglio, G; Merola, A; Iannuzzi, A; Palma, M; Grimaldi, N; Sarubbi, B. Safety and Efficacy of Sacubitril/Valsartan in Patients With a Failing Systemic Right Ventricle: A Prospective Single-Center Study. Circ Heart Fail 2023, 16(2), e009848. [Google Scholar] [CrossRef] [PubMed]
- Nederend, M; Kiès, P; Regeer, MV; Vliegen, HW; Mertens, BJ; Robbers-Visser, D; Bouma, BJ; Tops, LF; Schalij, MJ; Jongbloed, MRM; Egorova, AD. Tolerability and beneficial effects of sacubitril/valsartan on systemic right ventricular failure. Heart 2023, 109(20), 1525–1532. [Google Scholar] [CrossRef] [PubMed]
- Fusco, F; Scognamiglio, G; Abbate, M; Merola, A; Grimaldi, N; Ciriello, GD; Sarubbi, B. Dapagliflozin in Patients With a Failing Systemic Right Ventricle: Results From the DAPA-SERVE Trial. JACC Heart Fail 2024, 12(4), 789–791. [Google Scholar] [CrossRef] [PubMed]
- Albertini, M; Waldmann, V; David, P; Barat, A; Legendre, A; Chaussade, AS; Iserin, L; Ladouceur, M. Safety and Efficacy of Dapagliflozin in Patients With Systemic Right Ventricular Dysfunction: DAPA-SRV Trial. J Am Heart Assoc. Epub. 2025, 14(11), e040302. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pathak, A; Lebrin, M; Vaccaro, A; Senard, JM; Despas, F. Pharmacology of levosimendan: inotropic, vasodilatory and cardioprotective effects. J Clin Pharm Ther. 2013, 38(5), 341–9. [Google Scholar] [CrossRef] [PubMed]
- Wannaz, L; Boillat, L; Perez, MH; Di Bernardo, S. Prophylactic use of levosimendan in preoperative setting for surgical repair of congenital heart disease in children. Front Pediatr. 2023, 11, 1205971. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Comín-Colet, J; Manito, N; Segovia-Cubero, J; Delgado, J; García Pinilla, JM; Almenar, L; Crespo-Leiro, MG; Sionis, A; Blasco, T; Pascual-Figal, D; Gonzalez-Vilchez, F; Lambert-Rodríguez, JL; Grau, M; Bruguera, J. LION-HEART Study Investigators. Efficacy and safety of intermittent intravenous outpatient administration of levosimendan in patients with advanced heart failure: the LION-HEART multicentre randomised trial. Eur J Heart Fail 2018, 20(7), 1128–1136. [Google Scholar] [CrossRef] [PubMed]
- García-González, MJ; Aldea Perona, A; Lara Padron, A; Morales Rull, JL; Martínez-Sellés, M; de Mora Martin, M; López Díaz, J; López Fernandez, S; Ortiz Oficialdegui, P; Jiménez Sosa, A. Efficacy and safety of intermittent repeated levosimendan infusions in advanced heart failure patients: the LAICA study. ESC Heart Fail 2021, 8(6), 4820–4831. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dobarro, D; Donoso-Trenado, V; Solé-González, E; Moliner-Abós, C; Garcia-Pinilla, JM; Lopez-Fernandez, S; Ruiz-Bustillo, S; Diez-Lopez, C; Castrodeza, J; Méndez-Fernández, AB; Vaqueriza-Cubillo, D; Cobo-Marcos, M; Tobar, J; Sagasti-Aboitiz, I; Rodriguez, M; Escolar, V; Abecia, A; Codina, P; Gómez-Otero, I; Pastor, F; Marzoa-Rivas, R; González-Babarro, E; de Juan-Baguda, J; Melendo-Viu, M; de Frutos, F; Gonzalez-Costello, J. Intermittent inotropic support with levosimendan in advanced heart failure as destination therapy: The LEVO-D registry. ESC Heart Fail 2023, 10(2), 1193–1204. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Combes, A; Saura, O; Nesseler, N; Lebbah, S; Rozec, B; Levy, B; Fellahi, JL; Beurton, A; Meslin, S; Gaudard, P; Bouglé, A; Vincentelli, A; Sonneville, R; Lebreton, G; Lévy, D; Ouattara, A; Tubach, F. LEVOECMO Trial Group and the International ECMO Network (ECMONet). Levosimendan to Facilitate Weaning From ECMO in Patients With Severe Cardiogenic Shock: The LEVOECMO Randomized Clinical Trial. JAMA 2026, 335(1), 60–69. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Burkhoff, D; Borlaug, BA; Shah, SJ; Zolty, R; Tedford, RJ; Thenappan, T; Zamanian, RT; Mazurek, JA; Rich, JD; Simon, MA; Chung, ES; Raza, F; Majure, DT; Lewis, GD; Preston, IR; Rich, S. Levosimendan Improves Hemodynamics and Exercise Tolerance in PH-HFpEF: Results of the Randomized Placebo-Controlled HELP Trial. JACC Heart Fail 2021, 9(5), 360–370. [Google Scholar] [CrossRef] [PubMed]
- Yaku, H; Burkhoff, D; Borlaug, BA; Lala, A; Butler, J; Rich, S; Shah, SJ. Oral Levosimendan for the Treatment of Pulmonary Hypertension due to Heart Failure With Preserved Ejection Fraction: Rationale and Design of the LEVEL Trial S1071-9164(25)00293-3. J Card Fail. Epub ahead of print. 2025. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y; Wei, Z; Zhang, C; Lu, C; Zeng, Z. The effect of levosimendan on right ventricular function in patients with heart dysfunction: a systematic review and meta-analysis. Sci Rep. 2021, 11(1), 24097. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Figure 1.
nyha class change during follow-up.
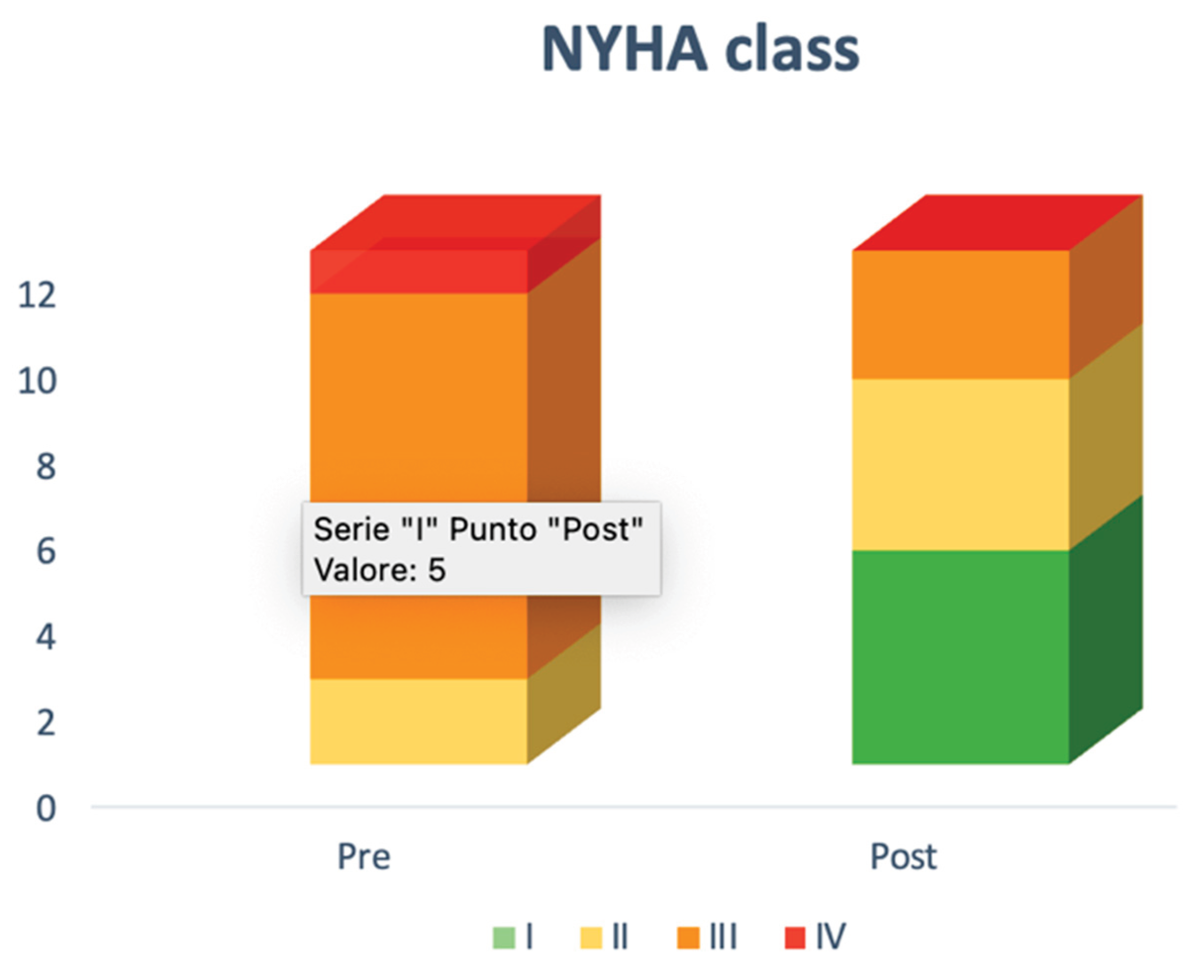

Table 1.
demographic data and baseline characteristic in the study population.
| sex (female) | 3(25%) |
| age (years) | 44.6[35-61.3] |
| weight (kg) | 71±17 |
| height (cm) | 167±9 |
bmi  (kg/m2) (kg/m2) |
25±5 |
| bsa (m2) | 2±0.3 |
| main diagnosis | 2 aortic coarctation 2 atrial septal defect 1 partial anomalous venous return 1 tetralogy of fallot 1 atrioventricular septal defect with straddling valve 1 transposition of the great arteries 4 congenitally corrected transposition of the great arteries |
| associated defects | 1 atrial septal defect 1 bicuspid aortic valve 1 right isomerism 2 ventricular septal defects 1 pulmonary stenosis 1 coarctation repair |
| surgical/percutaneous procedures | 2 coarctation repair (2 end to end anastomosis, 1 subclavian flap) 3 atrial septal defect closure (1 with a fenestrated device, 2 surgically) 1 glenn and fontan procedure 1 tetralogy of fallot repair 1 tricuspid valve annuloplasty and mitral valve edge-to-edge repair 1 correction of anomalous pulmonary veins drainage 1 percutaneous closure of left atrial appendage 1 mustard operation 2 ventricular septal defect closure 1 pulmonary stenosis relief 3 blalock taussing shunt 1 pulmonary artery banding 1 rashkind balloon atrial septostomy 1 fontan conduit stenting 1 fontan conduit replacement |
| total number of procedures01 2 5 |
2(17%) 4(33%) 5(42%) 1(8%) |
| residual defects | 2 pulmonary arterial hypertension 1 severe aortic stenosis 5 severe tricuspid regurgitation 1 severe pulmonary regurgitation 1 mitral regurgitation |
| genetic disorder | 1 turner syndrome |
| comorbidity | 1(8%) hepatocellular carcinoma 2(17%) ckd 4(33%) copd 2(17%) hypothyroidism |
| cardiovascular risk factors | 1(8%) diabetes 2 (17%) hypertension 3(25%) obesity 3 (25%) dyslipidemia 2(17%) stable coronary syndrome and previous ptca |
| pm | 1(8%) |
| icd | 4(33%) |
| nyha class (ii/iii/iv) | 2(17%)/9(75%)/1(8%) |
| previous hospitalization for hf | 12(100%) |
| hf hospitalization >1 | 6(50%) |
| history of supraventricular tachycardia | 4(33%) |
| history of ventricular tachycardia | 5(42%) |
| baseline rhythm | 8(66%) sinus 2(17%) ventricular pacing 2(17%) atrial fibrillation |
| baseline sbp (mmhg) | 108±10 |
| baseline hr (bpm) | 76±12 |
| treatment | 7(58%) arni 8 (66%) gliflozins 3(25%) acei/arb 9 (75%) beta-blockers 7(58%) mra 8(66%) diuretics 2(17%) ivabradine (25%) doac 2(17%) warfarin 2(17%) antiplateletes 2(18%) amiodaron |
abbreviations: acei= angiotensin-converting enzyme inhibitors, arb= angiotensin-receptor blockers, bmi=body mass index, bsa=body surface area, ckd= chronic kidney disease, copd=chronic obstructive pulmonary disease, doac=direct oral anticoagulants, hf=heart failure, hr=heart rate, icd=implantable cardioverter/defibrillator, nyha=new york heart association, pmk=pacemaker, ptca=percutaneous transluminal coronary angioplasty, sbp=systolic blood pressure, tga=transposition of the great arteries. continuous variables are expressed as mean±sd or median[iqr], according to data distribution.
Table 2.
baseline cardiac catheterization data (n=5).
| papm (mmhg) | 26±9 |
| pcwp (mmhg) | 14±5 |
| pvri (wu) | 3±1.9 |
| ci (l/min/m2) | 3±1.8 |
abbreviations: ci=cardiac index, papm=mean pulmonary artery pressure, pcwp=pulmonary capillary wedge pressure, pvri= indexed pulmonary vascular resistance.
Table 3.
comparison between baseline and follow-up data.
| baseline | follow-up | p-value | |
|---|---|---|---|
| ntprobnp (pg/ml) | 1576[705-3023] | 967[241-2263] | 0.3 |
| creatinine (mg/dl) | 0.84±0.25 | 0.88±0.17 | 0.4 |
| nyha class iii-iv | 10(83%) | 3(25%) | 0.005 |
| lv ef* (%) | 37.6±8 | 43.6±5 | 0.1 |
| rv fac** (%) | 27±7.4 | 30.6±7 | 0.02 |
abbreviations: ef=ejection fraction, fac=fractional area change, lv=left ventricle, nyha=new york heart association, rv=right ventricle, *=only patients with systemic left ventricle, **=only patients with systemic right ventricle.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



