
Submitted:
11 February 2026
Posted:
12 February 2026
You are already at the latest version
Abstract
Background: Continuity of care is a core component of high-quality, patient-centered health systems and a central domain of nursing practice, particularly for older adults and people living with chronic and complex conditions. Yet discontinuities remain common during transitions between hospital and community care, contributing to fragmented communication, delayed follow-up, negative patient experiences, and avoidable harm. Methods: This narrative review synthesizes key conceptual and empirical literature on continuity of care and care transitions, with a focus on how continuity is defined, conceptualized, and strengthened across settings. Results: Continuity is presented as a multidimensional construct encompassing informational, management, and relational continuity, and its relationship to overlapping constructs such as discharge planning, care coordination, and transitional care is clarified. Evidence summarized in this review indicates that persistent gaps in information transfer and unclear professional accountability con-tinue to undermine safe and effective transitions, underscoring the importance of structured transitional processes and strong interprofessional collaboration. The review also highlights patient-reported approaches to assessing continuity and transitional care qual-ity, including validated instruments that capture the patient perspective, alongside ad-ministrative indicators. Finally, nursing-relevant approaches that may strengthen continuity including nurse-led transitional care, navigation and care-coordination roles, inte-grated care approaches, and patient-centered models in primary and community care- are discussed. Conclusions: Overall, continuity of care should be understood as both a structural and relational process that requires multi-level strategies to reduce fragmentation, improve coordination, and enhance patient experience across care transitions.
Keywords:
continuity of care
; care transitions
; transitional care
; care coordination
; discharge planning
; patient experience
; integrated care
1. Introduction
Continuity of care is widely recognized as a fundamental component of high-quality, patient-centered healthcare and a core attribute of strong primary and community-based health systems. In nursing practice across settings, continuity is not only a structural characteristic of care delivery but also a relational and professional commitment that supports safety, trust, and therapeutic effectiveness over time. This review also summarizes key evidence identified through iterative, non-systematic database and targeted citation searches to support health service and nursing practice implications.
As populations age and the prevalence of chronic and multimorbid conditions increases, more patients require care from multiple providers, disciplines, and organizations. This makes continuity both increasingly complex and increasingly important.
Transitions between hospital and community care represent a particularly vulnerable point in the patient journey. These transitions involve changes in care teams, treatment plans, and responsibility for follow-up, and they are often accompanied by gaps in communication, unclear accountability, and fragmented information. Research has linked such discontinuities to medication discrepancies, delayed follow-up, duplicated investigations, preventable complications, and negative patient experiences [1,2,3,4].
In routine nursing work, continuity is closely tied to core professional responsibilities in discharge planning, care coordination, patient education, and ongoing monitoring in the community. When continuity is weak, the burden of fragmentation is frequently shifted to patients and informal caregivers, who may need to navigate complex systems with limited guidance.
Continuity challenges are also shaped by health system context. In settings characterized by geographic, organizational, or workforce disparities (for example, rural or peripheral regions), access to services and timely follow-up may be limited, further complicating efforts to sustain coherent care over time [5]. In such contexts, strengthening continuity is both a quality and an equity priority.
Against this background, this narrative review synthesizes key conceptual and empirical literature on continuity of care across care transitions, with particular attention to nursing practice and patient experience. The review (1) describes how continuity is defined and conceptualized, (2) clarifies its relationship to related constructs such as discharge planning and transitional care, (3) summarizes why continuity matters for patients and health systems, and (4) discusses selected approaches to strengthening continuity across settings. Although previous reviews have examined specific interventions or aspects of care transitions, fewer have synthesized continuity of care as a multidimensional construct integrating conceptual frameworks, patient experience, and nursing-relevant perspectives across health system contexts.
2. Materials and Methods
This narrative review draws on influential conceptual and empirical literature addressing continuity of care, care transitions, and related constructs in hospital and community settings. The purpose was to integrate and interpret central themes and perspectives to clarify concepts, highlight mechanisms, and discuss implications for nursing practice and patient experience across hospital-to-community transitions.
Literature identification and scope. Literature was identified through iterative, non-systematic searches of major health and nursing databases (PubMed and CINAHL), complemented by targeted searches for seminal and highly cited papers and reference-list screening of key articles. We performed iterative searches in PubMed and CINAHL (covering 2002–2024) using combinations of keywords related to continuity of care and transitions (e.g., “continuity of care”, “care transitions”, “discharge planning”, “transitional care”, “care coordination”, and “patient experience/patient-reported measures”). Reference lists of key articles were screened and citation tracking was used to identify seminal and highly cited frameworks and additional relevant studies. Search terms were refined iteratively and included combinations of: continuity of care, care transitions, discharge planning, transitional care, care coordination, patient experience, and patient-reported measures.
Searches were scoped to reflect the publication years represented in the evidence base included in this review (2002–2024).
Eligibility and prioritization. Priority was given to: (a) widely cited conceptual frameworks defining continuity and its dimensions; (b) empirical studies, trials, and reviews focusing on transitions of care-particularly among older adults and people living with chronic or complex conditions; and (c) articles addressing patient perspectives and measurement approaches, including patient-reported instruments relevant to the hospital-to-community transition.
Data charting and synthesis approach. For included sources, we charted key characteristics (e.g., setting/population, focal construct or intervention, continuity dimension(s) addressed, and practice-relevant implications) and synthesized findings narratively. Because this is a narrative (rather than systematic) review, the synthesis does not aim to be exhaustive; instead, it emphasizes conceptual integration and practice-relevant interpretation. Where evidence was heterogeneous in terms of populations, settings, definitions, and outcomes, findings were presented as thematic patterns rather than pooled quantitative estimates.
Quality appraisal. A formal risk-of-bias appraisal was not undertaken because the review aim was conceptual and integrative and the included evidence was methodologically heterogeneous (spanning conceptual frameworks, trials, cross-sectional studies, and systematic/scoping reviews), which also precluded quantitative synthesis.
3. Results
3.1. Conceptualizing Continuity of Care
Continuity of care is a complex, multidimensional concept discussed across medicine, nursing, health services research, and policy. A highly influential multidisciplinary review by Haggerty and colleagues (2003) [6] defined continuity as the degree to which a series of discrete healthcare events is experienced by patients as coherent, connected, and consistent with their medical needs and personal context. This definition highlights continuity as both a system property and a patient experience constructed over time. More recent conceptual syntheses have further refined this framework, emphasizing the dynamic interaction between informational, management, and relational continuity across complex care transitions [7].
Haggerty et al. (2003) [6] proposed three interrelated dimensions of continuity that remain widely used in research and practice:
Informational continuity: The availability and use of relevant information on past events, personal circumstances, and patient preferences to make current care appropriate. In transitions, this includes complete and timely transfer of discharge summaries, medication lists, pending test results, and follow-up plans.
Management continuity: A consistent and coherent approach to managing a health condition that is responsive to a patient’s changing needs. This is particularly important for chronic and complex conditions requiring coordinated input from multiple professionals over time.
Relational continuity: An ongoing therapeutic relationship between a patient and one or more providers. In nursing and primary care, this is often expressed through trust, mutual knowledge, and a sense of responsibility and accountability that extends beyond single encounters.
These dimensions operate dynamically during transitions, where failures in one domain may disrupt the others. They underscore that continuity is not synonymous with any single intervention or organizational arrangement. Rather, it emerges from the interaction between information systems, organizational processes, professional roles, and interpersonal relationships. For nurses, continuity is enacted through formal mechanisms (such as care plans, discharge procedures, and follow-up protocols) and through sustained relationships with patients and families.
3.2. Why Continuity Matters: Mechanisms and Outcomes
Continuity of care influences patient outcomes and experiences through interrelated mechanisms that are particularly salient during transitions between hospital and community settings.
Communication and information transfer: Breakdowns in communication between hospital-based teams and community providers are among the most consistently documented problems in transitional care. Kripalani et al. (2007) [1] described substantial deficits in the timeliness, completeness, and accuracy of information transferred at discharge, including missing test results, unclear follow-up plans, and discrepancies in medication lists. Such failures undermine informational continuity and increase the risk of duplication, delays, and avoidable harm.
Patient safety and clinical outcomes: Discontinuity has been associated with missed warning signs, delayed interventions, and reduced capacity for early detection of deterioration after discharge, while higher continuity has been linked to improved outcomes and reduced mortality in several studies [8]. Transitional care interventions designed to strengthen continuity have demonstrated improved outcomes for high-risk older adults, including reductions in rehospitalization and better post-discharge management [3,9].
Patient experience, trust, and therapeutic relationships: Continuity is a central determinant of patient experience. Patient experience reflects whether care is perceived as coordinated, respectful, understandable, and responsive to individual needs and has been associated with improved clinical safety and effectiveness outcomes [10,11]. Relational continuity supports trust and engagement in self-management and can reduce anxiety during vulnerable transition periods.
System-level implications: At the system level, poor continuity contributes to inefficiency, duplication of services, and potentially avoidable acute-care utilization. In contrast, systems that prioritize continuity and coordination, especially for people with complex needs, are better positioned to deliver effective and person-centered care [12].
3.3. Measuring Continuity and Patient Experience
Continuity can be measured from the perspectives of professionals, health systems, and patients. Administrative and provider-based indicators (for example, continuity indices derived from visit patterns) provide information about service utilization but capture only limited aspects of how continuity is experienced.
Because continuity is fundamentally longitudinal and relational, patient-reported measures are particularly important. Patient-reported instruments can assess whether care was perceived as coherent, coordinated, and supportive, complementing outcomes such as readmissions or emergency department use.
One instrument specifically developed to assess patients’ perceptions of continuity across the hospital-to-community transition is the Patient Continuity of Care Questionnaire (PCCQ). Hadjistavropoulos et al. (2008) [13] reported acceptable reliability and validity, capturing key elements of discharge and post-discharge processes including information transfer, coordination, and preparedness for self-management.
Broader patient experience surveys (for example, CAHPS-based tools) often include domains that overlap with continuity, such as care coordination and communication [10,14]. For quality improvement, combining patient-reported measures with clinical and administrative indicators provides a more complete understanding of whether care processes occurred and whether they were experienced as meaningful and supportive.
3.4. Vulnerable Populations and High-Risk Transitions
Continuity challenges are especially pronounced among older adults and individuals living with multiple chronic conditions. These patients often receive care from numerous professionals across settings over extended periods, increasing the likelihood of fragmented information, inconsistent management plans, and unclear responsibility for follow-up.
Older adults with complex needs may experience polypharmacy, functional limitations, cognitive impairment, and social vulnerability, all of which can complicate discharge planning and post-discharge management. System constraints can further exacerbate these risks. For example, delayed transfers of care have been associated with prolonged hospital stays and adverse outcomes among older patients [[1[5].
From a nursing perspective, high-risk transitions often require intensive coordination, education, and monitoring in the community. When continuity is weak, patients and families may be left to navigate complex systems with insufficient guidance, increasing the likelihood of unmet needs and avoidable complications.
Health system characteristics, including resource constraints, workforce shortages, and geographic disparities, shape the risk of discontinuity. In rural or peripheral settings, limited access to specialized services and timely follow-up can intensify continuity challenges, making proactive coordination and strong community-based nursing services particularly important [5].
3.5. Interventions to Strengthen Continuity Across Transitions
A wide range of interventions has been developed to improve continuity of care and reduce adverse outcomes during transitions between hospital and community settings. Although interventions differ in scope and intensity, most aim to strengthen informational, management, and relational continuity.
3.6. Transitional Care Programs
Transitional care models are among the most extensively studied approaches to improving continuity across care settings. Programs commonly include structured discharge planning, patient and caregiver education, medication reconciliation, and proactive follow-up after discharge.
Nurse-led transitional care interventions for high-risk older adults have been associated with improved post-discharge outcomes and reduced rehospitalization [3]. Coleman’s Care Transitions Intervention emphasizes patient empowerment, improved self-management, and continuity of information across settings [2][9].
These models highlight the role of nurses in maintaining continuity beyond the hospital stay by providing sustained contact, monitoring, and coordination so that care plans are communicated, implemented, and adapted to evolving needs.
3.7. Navigation and Care Coordination Roles
Navigation and care coordination can support patients, particularly older adults and those with chronic illness, in moving through complex systems. Manderson et al. (2012) [[1[6] found that navigation roles may facilitate access to services, improve coordination between providers, and support patients during transitions.
These roles are often undertaken by nurses or other health professionals who act as consistent points of contact, strengthening management continuity and, when sustained over time, relational continuity.
3.8. Integrated Care Approaches
Integrated care frameworks aim to reduce fragmentation by improving coordination and collaboration across organizational and professional boundaries and have been conceptualized as multilevel integration across clinical, professional, organizational, and system dimensions [17]. Gröne and Garcia-Barbero (2002) [12] described integrated care as a response to increasing system complexity and the needs of patients who require services from multiple providers over time.
While integrated care is a broad policy and organizational concept, its objectives align closely with continuity: ensuring that care is experienced as coherent, connected, and person-centered.
3.9. Patient-Centered Models in Primary and Community Care
Primary care-based models, including the Patient-Centered Medical Home (PCMH), have been promoted as mechanisms to improve continuity, coordination, and quality of care. The PCMH emphasizes team-based care, proactive population management, enhanced access, and sustained relationships between patients and care teams [[1[8].
For nurses working in primary and community settings, such models can provide structures that support ongoing follow-up, coordination with other services, and long-term therapeutic relationships.
Figure 1 presents a conceptual model summarizing how the three continuity dimensions influence mechanisms during care transitions and, in turn, patient and system outcomes.
4. Discussion
This review highlights continuity of care as a foundational component of high-quality, patient-centered healthcare, particularly during transitions between hospital and community settings. The framework proposed by Haggerty et al. (2003) [6] remains useful for clinical and organizational improvement because informational, management, and relational continuity are interdependent; strengthening only one dimension in isolation is unlikely to substantially reduce fragmentation.
From a nursing perspective, a consistent pattern is the central role of nurses in operationalizing continuity through discharge planning, education, medication reconciliation, follow-up, and coordination across settings. Nurse-led and nurse-involved transitional care models illustrate that continuity is enacted not only through protocols but also through sustained professional relationships and clear clinical accountability [3,9,19]. Systematic reviews indicate that structured transitional care interventions may improve patient outcomes and reduce adverse events following discharge, particularly among older adults and patients with complex care needs [20].
A recurring issue across studies is vulnerability of information transfer at discharge. Despite longstanding awareness, deficits in completeness and timeliness of communication between hospital-based and community providers remain common [1]. Technical solutions such as electronic records and standardized forms are necessary but may be insufficient without explicit role clarity, ownership of follow-up, and shared expectations across settings.
The close relationship between continuity and patient experience also emerges clearly. Measures of patient experience capture coordination, respect, clarity, and responsiveness, which closely mirror elements of continuity [10,13]. Relational continuity can support trust and engagement in self-management and help identify emerging problems early, especially among older adults and people living with chronic or complex conditions.
Practical implications for nursing and service delivery include: (1) assigning clear responsibility for post-discharge follow-up, (2) ensuring discharge information is complete, timely, and usable by community providers, (3) providing patients and caregivers with a clear, plain-language plan for medications, red flags, and appointments, and (4) using structured follow-up contacts (for example, phone calls or home visits) to confirm understanding and address barriers to implementation.
Finally, continuity challenges may be amplified in health systems facing geographic and resource constraints, such as rural or peripheral regions [5]. Strengthening community-based nursing services and interprofessional collaboration is likely to be critical for both quality and equity.
Together, these findings suggest that continuity of care should be understood not only as an organizational goal but as a dynamic relational process co-created by patients, professionals, and healthcare systems. Strengthening informational, management, and relational continuity may represent a key pathway toward safer and more patient-centered care transitions.
4.1. Limitations
As a narrative review, this paper does not follow a formal systematic search protocol and therefore cannot claim to have identified all relevant publications on continuity of care and care transitions. Literature is heterogeneous in terms of populations, settings, definitions, and outcome measures, limiting direct comparability between studies and precluding quantitative synthesis. Selection and interpretation in narrative reviews may be influenced by the prominence of seminal work and the reviewers’ judgments regarding relevance. In addition, much of the evidence emphasizes older adult populations and specific health system contexts, which may limit generalizability to other groups and settings.
4.2. Future directions
Future research should further examine how continuity is experienced across diverse health system contexts, including community and peripheral settings. Greater emphasis is needed on patient-reported measures that capture continuity longitudinally rather than at isolated transition points.
Additional research is also needed on sustained nursing roles beyond the immediate post-discharge period, including chronic care management and interprofessional coordination over time. Implementation-focused studies could clarify how organizational models such as integrated care and patient-centered primary care can be translated into routine practice in ways that meaningfully strengthen continuity.
5. Conclusions
Continuity of care is a central element of high-quality, patient-centered healthcare and a critical determinant of safe and effective transitions between hospital and community settings. It is not a single intervention, but a multidimensional construct encompassing informational, management, and relational components that together shape how care is experienced over time.
Discontinuities remain common during transitions, particularly for older adults and individuals with chronic or complex conditions and are associated with risks to patient safety and patient experience. Nurses play a pivotal role in addressing these challenges through discharge planning, coordination, education, and follow-up in the community.
Strengthening continuity requires coordinated action at multiple levels: robust communication processes and information infrastructure, clear professional responsibility and accountability, and organizational structures that support sustained therapeutic relationships. Evaluation should combine utilization and clinical outcomes with patient-reported measures that capture whether care is experienced as coherent, supportive, and responsive.
Author Contributions
LM conceived the review; YS and KG drafted the manuscript; LM, YS and KG critically revised the manuscript. All authors read and approved of the final manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement:. Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
During manuscript preparation, ChatGPT (version 5.2) was used to support the development of the illustrative figure. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CAHPS | Consumer Assessment of Healthcare Providers and Systems |
| CG-CAHPS | Clinician & Group Consumer Assessment of Healthcare Providers and Systems |
| CINAHL | Cumulative Index to Nursing and Allied Health Literature |
| NHS | National Health Service |
| PCCQ | Patient Continuity of Care Questionnaire |
| PCMH | Patient-Centered Medical Home |
References
- Kripalani, S.; LeFevre, F.; Phillips, C.O.; Williams, M.V.; Basaviah, P.; Baker, D.W. Deficits in communication and information transfer between hospital-based and primary care physicians. JAMA 2007, 297, 831–841. [Google Scholar] [CrossRef] [PubMed]
- Coleman, E.A.; Boult, C. Improving the quality of transitional care for persons with complex care needs. J. Am. Geriatr. Soc. 2003, 51, 556–557. [Google Scholar] [CrossRef] [PubMed]
- Naylor, M.D.; Brooten, D.A.; Campbell, R.L.; Maislin, G.; McCauley, K.M.; Schwartz, J.S. Transitional care of older adults hospitalized with heart failure: A randomized, controlled trial. J. Am. Geriatr. Soc. 2004, 52, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Cohen, E.; Lindman, I. Importance of continuity of care from a patient perspective—A cross-sectional study in Swedish health care. Scand. J. Prim. Health Care 2024, 42, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Iglehart, J.K. The challenging quest to improve rural health care. N. Engl. J. Med. 2018, 378, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Haggerty, J.L.; Reid, R.J.; Freeman, G.K.; Starfield, B.H.; Adair, C.E.; McKendry, R. Continuity of care: A multidisciplinary review. BMJ 2003, 327, 1219–1221. [Google Scholar] [CrossRef] [PubMed]
- Holland, D.E.; Harris, M.R. Discharge planning, transitional care, coordination of care, and continuity of care: Clarifying concepts and terms from the hospital perspective. Home Health Care Serv. Q. 2007, 26, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Pereira Gray, D.J.; Sidaway-Lee, K.; White, E.; Thorne, A.; Evans, P.H. Continuity of care with doctors—A matter of life and death? A systematic review. BMJ Open 2018, 8, e021161. [Google Scholar] [CrossRef] [PubMed]
- Coleman, E.A. Falling through the cracks: Challenges and opportunities for improving transitional care for persons with continuous complex care needs. J. Am. Geriatr. Soc. 2003, 51, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Holt, J.M. Patient experience in primary care: A systematic review of CG-CAHPS surveys. J. Patient Exp. 2019, 6, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Doyle, C.; Lennox, L.; Bell, D. A systematic review of evidence on the links between patient experience and clinical safety and effectiveness. BMJ Open 2013, 3, e001570. [Google Scholar] [CrossRef] [PubMed]
- Gröne, O.; Garcia-Barbero, M. Trends in Integrated Care—Reflections on Conceptual Issues; World Health Organization: Copenhagen, Denmark, 2002; Available online: https://scholar.google.com/citations?view_op=view_citation&hl=en&user=tg6oDCIAAAAJ&citation_for_view=tg6oDCIAAAAJ:IjCSPb-OGe4C.
- Hadjistavropoulos, H.; Biem, H.; Sharpe, D.; Bourgault-Fagnou, M.; Janzen, J. Patient perceptions of hospital discharge: Reliability and validity of a Patient Continuity of Care Questionnaire. Int. J. Qual. Health Care 2008, 20, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Khatri, R.; Endalamaw, A.; Erku, D.; Wolka, E.; Nigatu, F.; Zewdie, A.; Assefa, Y. Continuity and care coordination of primary health care: A scoping review. BMC Health Serv. Res. 2023, 23, 750. [Google Scholar] [CrossRef] [PubMed]
- Jasinarachchi, K.H.; Ibrahim, I.R.; Keegan, B.C.; Mathialagan, A.; McGourty, K.; Phillips, J.; Gill, G.V.; Myint, P.K. Delayed transfer of care from NHS secondary care to primary care in England: its determinants, effect on hospital bed days, prevalence of acute medical conditions and deaths during delay, in older adults aged 65 years and over. BMC Geriatr. 2009, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Manderson, B.; McMurray, J.; Piraino, E.; Stolee, P. Navigation roles support chronically ill older adults through healthcare transitions: A systematic review of the literature. Health Soc. Care Community 2012, 20, 113–127. [Google Scholar] [CrossRef] [PubMed]
- Valentijn, P.P.; Schepman, S.M.; Opheij, W.; Bruijnzeels, M.A. Understanding integrated care: A comprehensive conceptual framework based on the integrative functions of primary care. Int. J. Integr. Care 2013, 13, e010. [Google Scholar] [CrossRef] [PubMed]
- Jackson, G.L.; Powers, B.J.; Chatterjee, R.; Bettger, J.P.; Kemper, A.R.; Hasselblad, V.; Dolor, R.J.; Irvine, R.J.; Heidenfelder, B.L.; Kendrick, A.S.; Gray, R.; Williams, J.W. The Patient-Centered Medical Home: A systematic review. Ann. Intern. Med. 2012, 158, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Facchinetti, G.; D’Angelo, D.; Piredda, M.; et al. Continuity of care interventions for preventing hospital readmission of older people with chronic diseases: A meta-analysis. Int. J. Nurs. Stud. 2020, 101, 103396. [Google Scholar] [CrossRef] [PubMed]
- Le Berre, M.; Maimon, G.; Sourial, N.; et al. Impact of transitional care services for chronically ill older adults: A systematic review. J. Am. Geriatr. Soc. 2017, 65, 1597–1608. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Continuity of Care Across Hospital-to-Community Transitions.
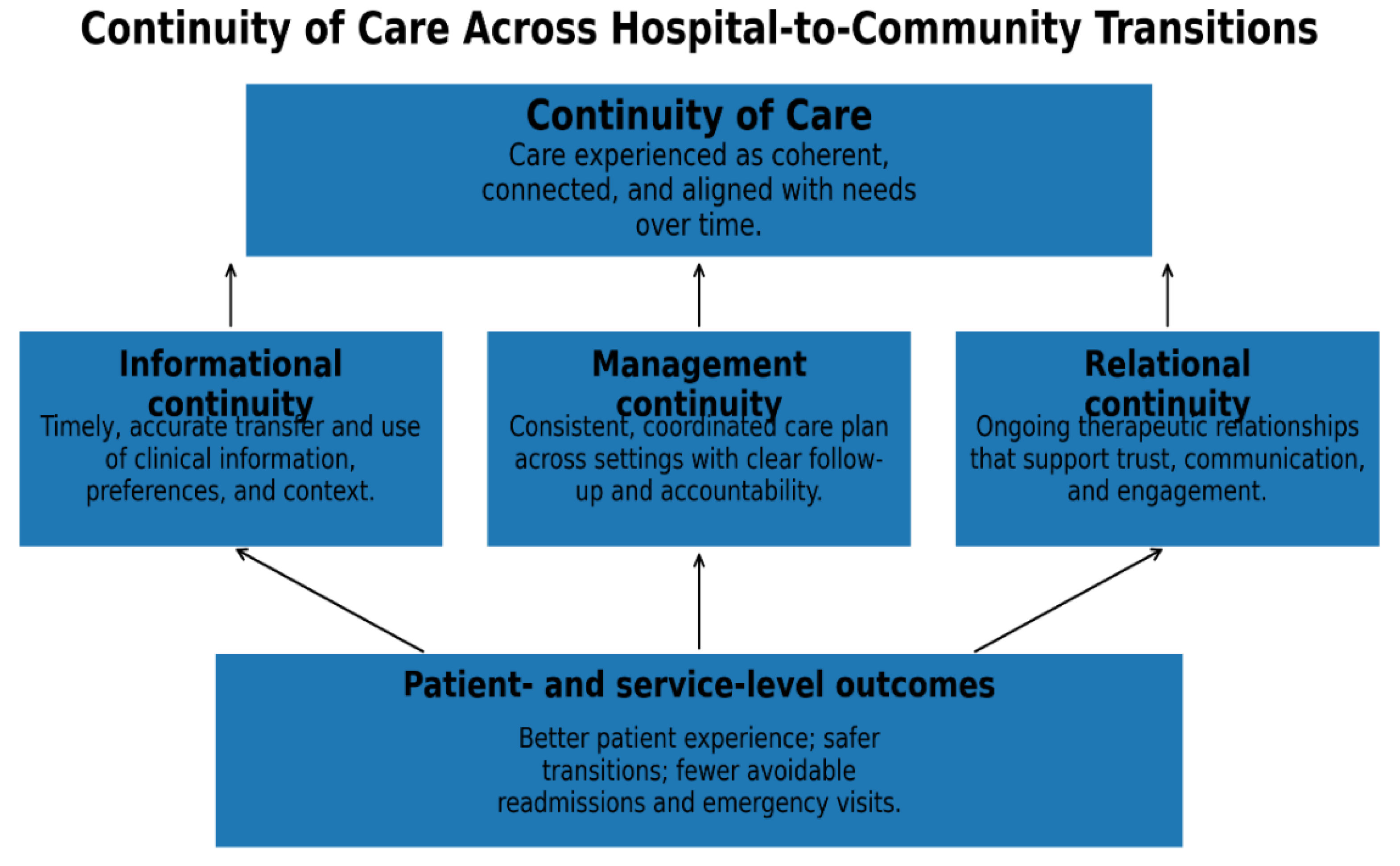

Table 1.
Overlapping constructs and how they contribute to continuity of care during hospital-to-community transitions.
Table 1.
Overlapping constructs and how they contribute to continuity of care during hospital-to-community transitions.
| Primary continuity dimension | How it contributes to continuity? | Brief definition | Term |
| Informational; Management | Improves completeness and timeliness of transition information and clarifies immediate next steps after discharge | Structured preparation for leaving hospital (information transfer, medications, follow-up arrangements, education, readiness) | Discharge planning |
| Management; Informational | Reduces fragmentation by aligning roles, responsibilities, and follow-up across settings | Organizing care activities across providers/services to ensure a coherent plan and clear accountability | Care coordination |
| Management; Informational; (often) Relational | Supports implementation and adaptation of the care plan after discharge; reduces early post-discharge gaps | Time-limited set of practices bridging hospital-to-community (e.g., structured discharge, medication reconciliation, proactive follow-up) | Transitional care (programs/models) |
| Management; Relational | Strengthens continuity by improving follow-through, reducing barriers, and maintaining a consistent “anchor” during transitions | A consistent point-of-contact (often nurse-led) who supports patients in moving through complex systems and accessing services | Navigation and care coordination roles |
| Management (system-level); Informational | Creates system-level structures that enable coherent care journeys for patients receiving services from multiple providers over time | Multi-level coordination across organizational/professional boundaries to reduce fragmentation (clinical–organizational–system integration) | Integrated care approaches |
| Relational; Management | Supports ongoing follow-up and coordination in the community, reinforcing longitudinal therapeutic relationships | Primary care models emphasizing team-based care, proactive management, enhanced access, and sustained relationships | Patient-centered models in primary/community care (e.g., Patient-Centered Medical Home—PCMH) |
| All three (cross-cutting assessment) | Complements administrative outcomes by measuring continuity as lived experience (including coordination/communication domains) | Tools capturing whether care was experienced as coherent, coordinated, respectful, and responsive | Patient experience and patient-reported measures (e.g., PCCQ; CAHPS/CG-CAHPS domains) |
*Continuity dimensions: informational, management, relational continuity.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



