
Submitted:
11 February 2026
Posted:
12 February 2026
You are already at the latest version
Abstract
Background and Clinical Significance: Myolipoma is a rare benign tumor, typically found in the retroperitoneum and characterized by a combination of mature adipo-cytes and well-differentiated smooth muscle cells. Myoplipomas usually present a de-lay in diagnosis due to the painless and slow growing clinical behaviour; therefore, the lesion can reach a large dimension with a challenging treatment. Case Presentation: We present the case of a retroperitoneal myolipoma infiltrating the left hip of an 11-year-old male. It was suspected based on magnetic resonance imaging; The patient has been successfully treated with surgical excision without complications. Histologi-cal examination revealed mature adipose tissue infiltrating skeletal striated muscle. The muscle fibers appeared normal, while the dense connective tissue was infiltrated by clusters of mature lymphocytes. Conclusions: Although myolipoma is extremely rare in male children and has never been reported to infiltrate the hip, it should be considered in the differential diagnosis of fat-containing retroperitoneal masses.
Keywords:
myolipoma
; neoplasm
; soft tissue tumors
; pelvis
; retroperitoneal
; hip
; excision
1. Introduction
Soft-tissue lipoma is a rare benign mesenchymal neoplasm that typically presents as a painless, slow-growing mass. It most commonly affects adult males between the fifth and seventh decades of life. According to its anatomical location, lipomas are classified as superficial (subcutaneous) or deep (muscular). Deep lipomas are further subdivided into intermuscular and periosteal types; however, they may also infiltrate skeletal muscle (intramuscular) or bone (intraosseous) [1,2]. Lipomas may occur in association with other mesenchymal components, resulting in histological variants such as myolipoma. Myolipomas, infiltrating smooth muscle, were first described by Meis and Enzinger in 1991. They are mainly composed of mature adipocytes and well-differentiated smooth muscle cells. Myolipomas have been most frequently reported in the retroperitoneum. Additional reported sites include the subcutaneous tissue, orbital region, pericardium, rectus sheath of the anterior abdominal wall, and the abdominal cavity, where they may be attached to the abdominal wall. [2,3,4]. We report the clinical, radiological, and histological features of a rare case of an abdominal myolipoma infiltrating the left hip, in which a delayed diagnosis resulted in a challenging therapeutic management.
2. Case Presentation
2.1. History
We present the case of an 11-year-old male patient who was admitted to our hospital with a 3 months’ history of left hip pain radiating to the left thigh, particularly when asleep. The patient was born through vaginal delivery with no complications and is healthy with no previous medical history. Upon physical examination, there was tenderness over the left hip with a decreased range of motion, particularly adduction. No swelling was detected.
2.2. Diagnostic Approach
Laboratory examinations revealed elevated sedimentation rate (29 mm/1hr. Normal value below 10 mm/1hr), insufficient 25-OH vitamin D3 (22.8 ng/ml. Value of Moderate deficiency 12,5-29 ng/ml), and normal phosphatase alkaline (190 U/L). The laboratory results also came negative for Anti-CCP (Anti-Cyclic Citrullinated Peptide).
An X-Ray of the hip and left femur was taken and showed no visible bone or joint lesion. The patient was treated by a general orthopedic surgeon and was given NSAIDs (Ibuprofen) and Paracetamol for symptom relief.
Due to the persistence of symptoms, MRI of both hips was performed, and it showed a moderate amount of left joint effusion associated with significant synovitis and adjacent soft tissue edema involving the obturator muscle with resultant mild decentralization of the femur remaining partially covered by acetabular edge. The patient was treated conservatively with rest, physiotherapy, and use of crutches and NSAIDs for symptom relief.
Thirteen months later, the patient underwent a new pelvis MRI examination due to the worsening of symptoms and a significant decrease in range of motion of the left hip. MRI revealed a large heterogeneous soft-tissue mass in the abdominal cavity, with extension to the hip joint, presenting both fat and muscle signal intensity with heterogeneous enhancement post gadolinium, and associated with extensive peri-osseous fatty infiltration, a reactive soft-tissue component, and advanced severe atrophy of the left obturator muscles (Figure 1). Those findings were not observed in the previous MRI.
At this stage, an incisional biopsy was performed, which revealed no pathological tissue.
Due to the persistence of symptoms, the patient underwent a follow-up MRI six months later, which showed no significant changes compared with the previous images. Therefore, the orthopedic surgeon decided together with the urology consultant to operate on the hip as well as the abdominal area.
2.3. Surgical Treatment
The surgical approach employed was an extended Smith–Petersen approach, continued medially to the midline through a horizontal incision. Intraoperatively, guided by preoperative MRI findings, the surgeon traced the diseased tissue and identified its attachment to the lateral internal pelvic wall, with extension through the ischium toward the acetabulum
The mass presented smooth capsula. Once the neoplasm was dissected, it was completely released from the acetabulum, resulting in restoration of hip mobility.
2.4. Pathological Finding
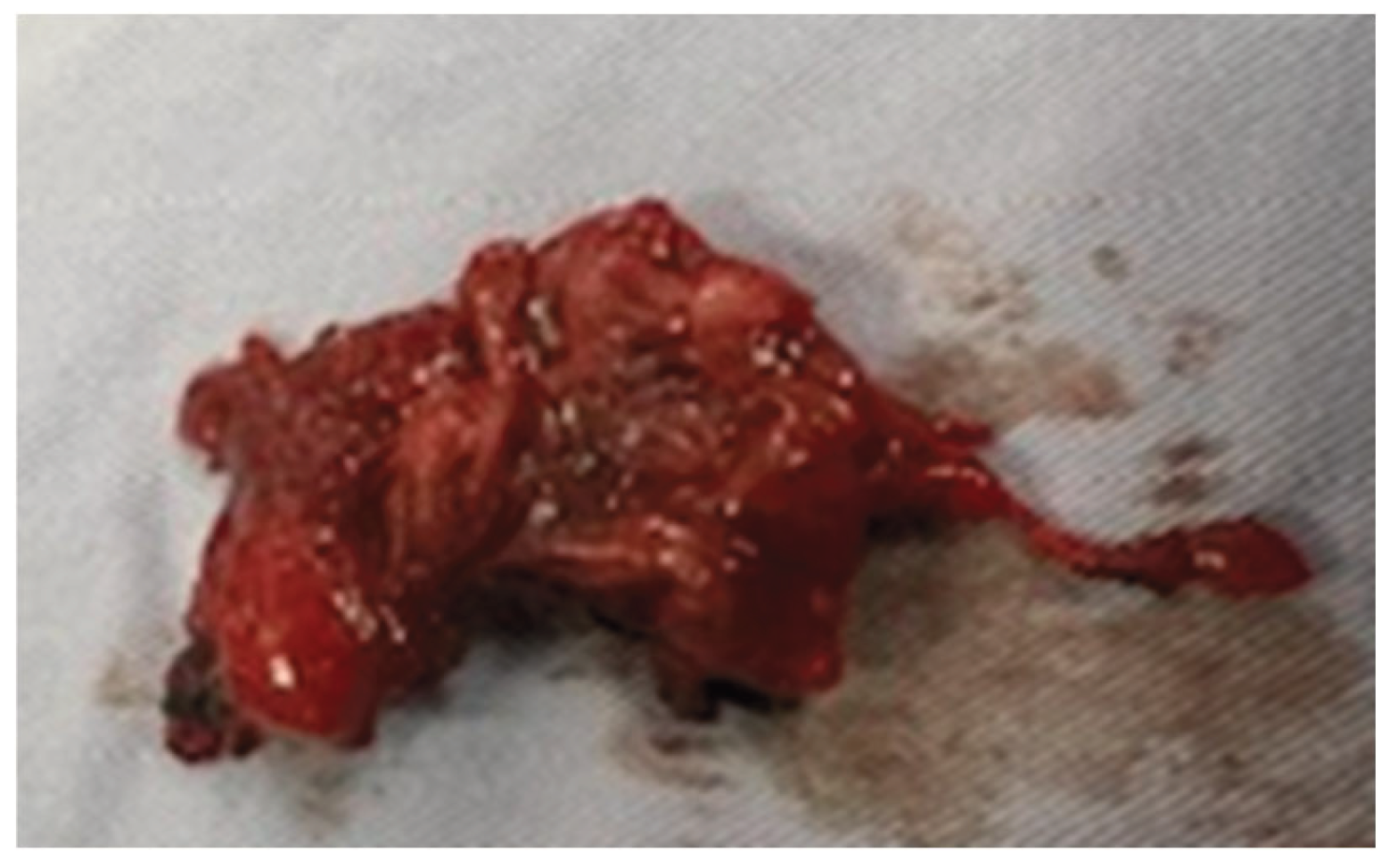
On gross examination, the mass had a solid, rubbery consistency, was well circumscribed, and measured 23 cm in greatest dimension. (Figure 2).
Histological examination of multiple specimens obtained from four different sites (soft tissue, bone, tumor, and hip) revealed mature adipose tissue infiltrating skeletal striated muscle. The muscle fibers appeared normal, while the dense connective tissue showed infiltration by clusters of mature lymphocytes. No features of malignancy were identified. These findings supported the diagnosis of a myolipoma infiltrating the hip.
2.5. Follow-Up
At 1, 6, 12 and 24 months follow-up, the patient was free of symptoms. Physical and Ultrasound examinations showed favorable outcome without evidence of disease.
4. Discussion
Lipomas are the most common benign mesenchymal neoplasm in humans. They usually grow in male adults ages between 50 and 70. Lipomas can occur in combination with other mesenchymal elements, giving rise to variants including myolipoma that infiltrate smooth muscle. [6,7]
Unlike typical lipomas, myolipomas have a slightly higher tendency to occur in women during their fifth and sixth decades of life. As for their localization, the retroperitoneum is the most common location for their growth, then comes less common localizations like sub-cutaneous tissue, orbital region, the pericardium, the rectus sheath of the anterior abdominal wall and erector spinae [7].
In contrast, our patient is a young male with a retroperitoneal myolipoma infiltrating the left hip, a location that, to the best of our knowledge, was never reported in literature.
The histological aspect of these tumors consists of variable amounts of benign smooth muscle fibers and mature adipose tissue with no lipoblasts, floret-like giant cells or zones of atypia. Cellular areas composed of bundles of spindle shaped eosinophilic cells and reminiscent of smooth muscle are dispersed within the mature adipose tissue cells. Myolipoma may be misdiagnosed as other adipocytic or mesenchymal tumors, including well-differentiated liposarcoma, spindle cell lipoma, angiomyolipoma, leiomyoma with fatty degeneration, lipoleiomyosarcoma, and leiomyosarcoma. [3,7]. Myolipomas are most confused as well-differentiated liposarcoma due to their similar fat content. Histologically, liposarcomas contain lipoblasts or floret-like giant cells, are encapsulated and show a fatty mass with poorly defined internal areas of non-adipose tissue [2]. Pathogenesis of myolipoma remains unclear. There are two main theories, namely adipose metaplasia and multipotential Mullerian cell origin [6,7,8,9].
Imaging is considered the gold standard for the diagnosis of myolipoma. Ultrasound may suggest the presence of a myolipoma, as the lipomatous regions of the tumor appear hyperechogenic; however, it cannot provide a definitive diagnosis. On CT and MRI, the lipomatous areas demonstrate typical fat characteristics. In contrast, the non-lipomatous regions display nonspecific solid features, with soft-tissue attenuation on CT, intermediate signal intensity on T1-weighted MRI, and intermediate to high signal intensity on T2-weighted MRI. [5]. The MRI we’ve done to our patient showed extensive peri-osseus fatty infiltration by soft tissue reaction which correlates with the fact that MRI shows the features of fat tissue in lipomatous components of myolipoma.
A preoperative biopsy is necessary to confirm the diagnosis, particularly in lesions larger than 5 cm. In our case, the histological findings from the preoperative biopsy revealed no pathological tissue. Therefore, a follow-up MRI was performed after 6 months, which showed no change in the fatty lesion, and surgical excision was subsequently undertaken due to the persistence of symptoms.
Surgical excision is the optimal treatment of myolipoma [2,10]. No cases of local recurrence, metastatic disease or malignant transformation have been reported in literature.
This case is reported due to its extreme rarity. To the best of our knowledge, this is the first case of a retroperitoneal myolipoma infiltrating the hip in a child.
5. Conclusions
Myolipoma is a rare tumor that should be considered in the differential diagnosis of retroperitoneal masses. MRI is highly useful in the evaluation of these tumors and can raise suspicion for a myolipoma, guiding further diagnostic assessment. Histological examination is mandatory to confirm the histopathologic aspect. showing a common adipose tissue infiltrating a skeletal striated muscle.
In the rare event of retroperitoneal myolipoma infiltrating the hip joint, surgical excision is the treatment of choice that can lead to complete recovery.
Author Contributions
Conceptualization, B.E. and H.Z.; methodology, A.V.; software, H.Z.; validation, L.D. and L.C..; formal analysis, L.C.; investigation, B.E..; resources, B.E..; data curation, H.Z..; writing—original draft preparation, B.E.; writing—review and editing, V.E. and L.D.; visualization, L-C.; supervision, L.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest
Abbreviations
The following abbreviations are used in this manuscript:
| NSAIDs | Nonsteroidal anti-inflammatory drugs |
| MRI | Magnetic Resonance Imaging |
References
- Debras, R.; Sciot, R.; Hompes, D.; Sinnaeve, F.; Wafa, H. An egg in the leg: Case report of an osteochondrolipoma. SICOT-J 2021, 7, 59. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Park, S.E.; Lee, J.U.; Choi, E.S. MRI of a subcutaneous myolipoma in the ankle: a case report. Korean J Radiol 2011, 12(5), 641–645. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Behranwala, K.A.; Chettiar, K.; El-Bahrawy, M.; Stamp, G.; Kakkar, A.K. Retroperitoneal myolipoma. World J Surg Oncol 2005, 3, 72. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dellachà, A.; Di Marco, A.; Foglia, G.; Fulcheri, E. Il lipoleiomioma dell'utero [Lipoleiomyoma of the uterus]. Pathologica 1997, 89(6), 737–741. [Google Scholar] [PubMed]
- Murphey, M.D.; Carroll, J.F.; Flemming, D.J.; Pope, T.L.; Gannon, F.H.; Kransdorf, M.J. From the archives of the AFIP: benign musculoskeletal lipomatous lesions. Radiographics 2004, 24(5), 1433–1466. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Imamura, T.; Irie, H.; Tanaka, F.; Fukushima, J.; Fukusato, T.; Harasawa, A.; Shiga, J. Myolipoma of the retroperitoneum. Pathol Int. 2004, 54(6), 460–463. [Google Scholar] [CrossRef] [PubMed]
- Michal, M. Retroperitoneal myolipoma. A tumour mimicking retroperitoneal angiomyolipoma and liposarcoma with myosarcomatous differentiation. Histopathology 1994, 25(1), 86–88. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Igarashi, T.; Noguchi, A.; Ito, M.; Nagaoka, Y.; Takeshita, C.; Takeda, N.; Watanabe, T.; Yoshioka, I.; Hirabayashi, K.; Fujii, T. Giant retroperitoneal myolipoma mimicking liposarcoma: report of a resected case and review of the literature. Int Cancer Conf J 2024, 13(2), 144–152. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fukushima, M.; Schaefer, I.M.; Fletcher, C.D. Myolipoma of Soft Tissue: Clinicopathologic Analysis of 34 Cases. Am J Surg Pathol 2017, 41(2), 153–160. [Google Scholar] [CrossRef] [PubMed]
- Oh, M.H.; Cho, I.C.; Kang, Y.I.; Kim, C.Y.; Kim, D.S.; Cho, H.D.; Kim, H.K. A case of retroperitoneal lipoleiomyoma. J Korean Med Sci. 2001, 16(2), 250–252. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Figure 1.
MRI showing large heterogeneous soft-tissue mass in the abdominal cavity, with extension to the hip joint.
Figure 1.
MRI showing large heterogeneous soft-tissue mass in the abdominal cavity, with extension to the hip joint.

Figure 2.
Macroscopic aspect of the excised mass.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



