Submitted:
11 February 2026
Posted:
15 February 2026
You are already at the latest version
Abstract
Background: Severe traumatic brain injury (TBI) remains associated with high in-hospital mortality. Although classical clinical predictors are widely used, additional biomarkers reflecting systemic dysfunction may improve prognostic assessment. Small intestinal bacterial overgrowth (SIBO) may represent a late marker of critical illness. This study evaluated the prognostic value of SIBO compared with traditional predic-tors in severe TBI. Methods: In this retrospective cohort study, 174 patients with severe TBI (Glasgow Coma Scale ≤ 8) were included. Baseline clinical parameters were rec-orded at admission. Quantitative cultures of small intestinal aspirates were obtained at admission (colony-forming units per milliliter, CFU/mL; CFU1) and on days 12–14 (CFU14). Multivariable logistic regression, receiver operating characteristic (ROC), and landmark analyses were performed. Results: Age (OR 1.06 per year, 95% CI 1.03–1.10, p < 0.001), lower GCS (OR 0.48 per point, 95% CI 0.28–0.83, p = 0.008), and res-piratory dysfunction reflected by lower PaO₂/FiO₂ values independently predicted mortality. Late bacterial load >10⁵ CFU/mL showed a strong association with death (OR 5.15, 95% CI 2.15–12.34, p < 0.001). Baseline CFU1 was not significant. The model demonstrated good discrimination (AUC = 0.84). Landmark analysis confirmed higher post-day-14 mortality and delayed discharge with elevated CFU14. Conclusions: Late intestinal bacterial overgrowth is independently associated with mortality and may complement traditional predictors for risk stratification in severe TBI.
Keywords:
traumatic brain injury
; intensive care
; small intestinal bacterial overgrowth
; gut mi-crobiota
; prognostic biomarkers
; mortality prediction
; critical illness
; survival analysis
; landmark analysis
; microbiological diagnostics
1. Introduction
Traumatic brain injury (TBI) remains one of the leading causes of death and disability worldwide. According to contemporary epidemiological estimates, more than 50–60 million new cases of TBI are registered annually, with severe forms representing the most clinically significant proportion and being characterized by high mortality and pronounced neurological consequences [1].
Despite advances in neurosurgery and intensive care, mortality in severe TBI remains high and in a number of studies reaches 30–40%, especially in patients requiring prolonged mechanical ventilation and treatment in intensive care units [2]. Fatal outcomes in this pathology are determined not only by the primary mechanical brain injury but also by secondary factors — hypoxia, systemic inflammation, metabolic disturbances, and the development of multiple organ dysfunction.
In this regard, the search for factors allowing prediction of disease course and outcomes becomes particularly relevant. Traditionally, age, level of consciousness according to the Glasgow Coma Scale, oxygenation parameters, and systemic metabolic indicators are considered key predictors of mortality. These variables formed the basis of widely used prognostic models such as IMPACT and CRASH [3,4]. Nevertheless, even when these models are used, the accuracy of prediction remains limited, which indicates the need to search for additional biomarkers reflecting systemic pathophysiological changes in critically ill patients.
In recent years, increasing attention has been paid to the role of intestinal dysfunction and microbiota in critical conditions. Impaired gastrointestinal motility, increased intestinal barrier permeability, and bacterial translocation are considered important components of the systemic inflammatory response and multiple organ failure [5]. One of the manifestations of these processes is small intestinal bacterial overgrowth syndrome (small intestinal bacterial overgrowth, SIBO), characterized by a pathological increase in the number of microorganisms in the lumen of the small intestine, usually defined as ≥ 10⁵ colony-forming units per milliliter of aspirate [6].
Although SIBO has been well studied in gastroenterology, its significance in intensive care unit patients and, in particular, in severe TBI remains insufficiently investigated. Theoretically, pronounced bacterial hypercolonization may reflect the severity of intestinal dysfunction, systemic inflammation, and the overall critical condition, which allows it to be considered as a potential marker of an unfavorable prognosis.
Aim of the Study
The aim of the present study was to assess and compare the prognostic significance of traditional clinical predictors of mortality (age, GCS, oxygenation parameters, and metabolic indicators) and a late microbiological marker — the degree of bacterial colonization of the small intestine in patients with severe traumatic brain injury.
2. Materials and Methods
2.1. Study Design and Population
A retrospective observational study was conducted in two tertiary hospitals to identify clinical predictors and late microbiological markers of in-hospital mortality in patients with severe traumatic brain injury (TBI). Patients were treated in the anesthesiology and intensive care departments of Ternopil Emergency Hospital, and Khmelnytsky Regional Hospital between September 1, 2023, and November 30, 2024.
A total of 174 patients were included in the final analysis. Inclusion criteria were: severe traumatic brain injury (Glasgow Coma Scale ≤ 8).
Exclusion criteria: cardiogenic pulmonary edema; decompensated chronic obstructive pulmonary disease; pulmonary embolism; malignant neoplasms; diabetic ketoacidosis; decompensated renal failure; acute myocardial infarction.
All patients were ventilated using Hamilton C6 ventilators. Arterial blood gases were analyzed using ABL800 FLEX analyzers (Radiometer, Denmark). Intracranial pressure (ICP) was monitored using Integra Neurosciences MPM-1 devices. Blood glucose levels were measured by the glucose oxidase method using a SUPER GL analyzer (Dr. Müller, Germany).
Severe TBI was defined based on the clinical presentation, neuroimaging data, and the need for intensive care. For the main analysis, a subgroup of patients with GCS ≤ 8 was used.
2.2. Baseline
At admission, age, body mass index, GCS, PaO₂/FiO₂, PaCO₂, and blood glucose were recorded.
2.3. Enteral Nutrition and Microbiology
For enteral nutrition, a nasointestinal tube was inserted beyond the ligament of Treitz. During tube placement, small intestinal contents were aspirated. On days 12–14, the tube was reinserted and repeated sampling was performed.
Culturing of small intestinal contents was performed with quantitative assessment in CFU/mL on day 1 (CFU1) and day 12–14 (CFU14). Identification was performed using VITEK 2 Compact (bioMérieux). Severe bacterial overgrowth was defined as >10⁵ CFU/mL according to commonly accepted microbiological thresholds.
2.4. Outcomes
The primary outcome was in-hospital mortality (Event day). Discharge was considered censoring (Entry day).
2.5. Statistical Analysis
Statistical analysis was performed using MedCalc® version 20.009 (MedCalc Software Ltd., Ostend, Belgium) and Python-based statistical packages. Continuous data are presented as median and IQR or minimum–QI–median–QIII–maximum. Multivariable logistic regression was used to assess mortality factors. The late marker — bacterial colonization on days 12–14 (CFU14) — was analyzed separately. Collinearity was assessed using VIF. Discrimination was evaluated by ROC/AUC. For events after day 14, a landmark approach was applied; for discharge, death was treated as a competing risk.
Receiver operating characteristic (ROC) analysis was performed to evaluate predictive accuracy, and the area under the curve (AUC) with 95% confidence intervals was calculated. A two-sided p-value < 0.05 was considered statistically significant. No formal sample size calculation was performed due to the retrospective design.
3. Results
3.1. Baseline Characteristics
A total of 174 patients with severe traumatic brain injury were included. The median age was 48 years (IQR 43–62.75; range 22–74). The median body mass index was 31 kg/m² (IQR 29–33). Neurological status at admission corresponded to severe traumatic brain injury, with a median Glasgow Coma Scale (GCS) score of 7 (IQR 7–8; range 5–8). Respiratory function was characterized by a median PaO₂/FiO₂ ratio of 356 (IQR 345–378) and PaCO₂ of 44 mmHg (IQR 38–45). The median blood glucose level was 8 mmol/L (IQR 7–10).
Detailed baseline characteristics are presented in Table 1.
Baseline microbiological assessment (CFU1) demonstrated low bacterial load (<10³ CFU/mL) in 85.1% of patients, moderate growth (10³–10⁵ CFU/mL) in 10.9%, and pronounced bacterial growth (>10⁵ CFU/mL) in 4.0% (Table 2).
3.2. Multivariable Logistic Regression
To assess independent factors associated with in-hospital mortality, a multivariable logistic regression model was constructed including age, neurological status at admission (GCS), oxygenation parameters (PaO₂/FiO₂), blood glucose level, and severe bacterial colonization of the small intestine on day 14 (CFU14 >10⁵).
Age demonstrated a statistically significant association with mortality: each additional year of life increased the risk of death by 6% (OR 1.06; 95% CI 1.03–1.10; p < 0.001).
A higher Glasgow Coma Scale score was an independent protective factor: an increase of 1 point was associated with an approximately 52% reduction in the probability of death (OR 0.48; 95% CI 0.28–0.83; p = 0.008).
Respiratory dysfunction was also associated with an unfavorable outcome: lower PaO₂/FiO₂ values were independently associated with increased mortality.
Blood glucose did not demonstrate independent prognostic significance in the multivariable model (p = 0.245).
The most pronounced effect was observed for the late microbiological marker: patients with severe bacterial overgrowth in the small intestine on day 14 (CFU14 >10⁵) had more than a fivefold increase in the risk of death (OR 5.15; 95% CI 2.15–12.34; p < 0.001).
Baseline bacterial colonization at admission (CFU1) did not demonstrate independent prognostic significance.
The results of the regression analysis are presented in Table 3.
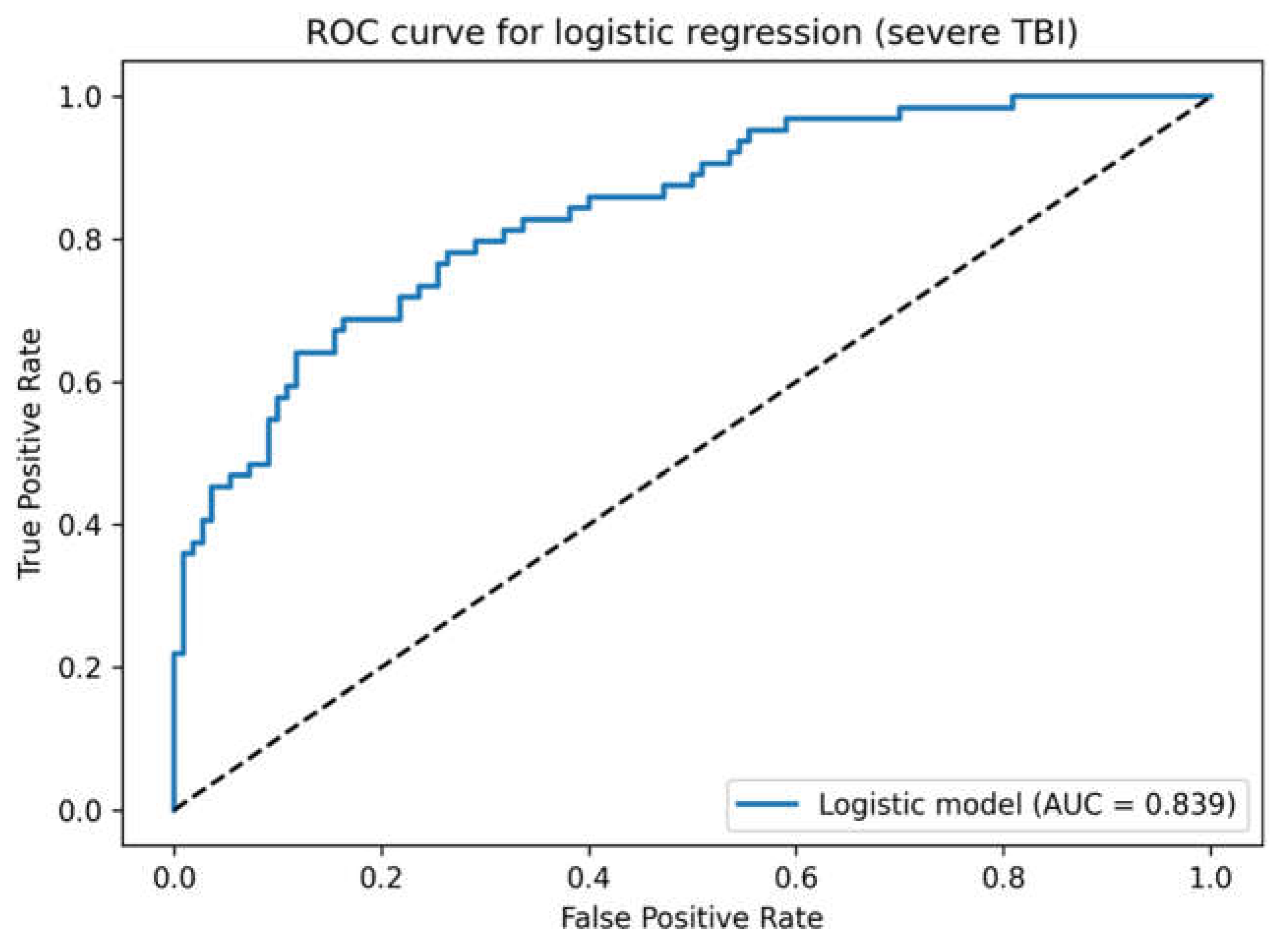
3.3. ROC Analysis
Receiver operating characteristic analysis of the multivariable logistic regression model demonstrated good predictive ability, with an area under the curve (AUC) of 0.84, indicating very good discrimination between survivors and non-survivors.
Figure 1.
ROC curve for the multivariable logistic regression model predicting in-hospital mortality.
Figure 1.
ROC curve for the multivariable logistic regression model predicting in-hospital mortality.
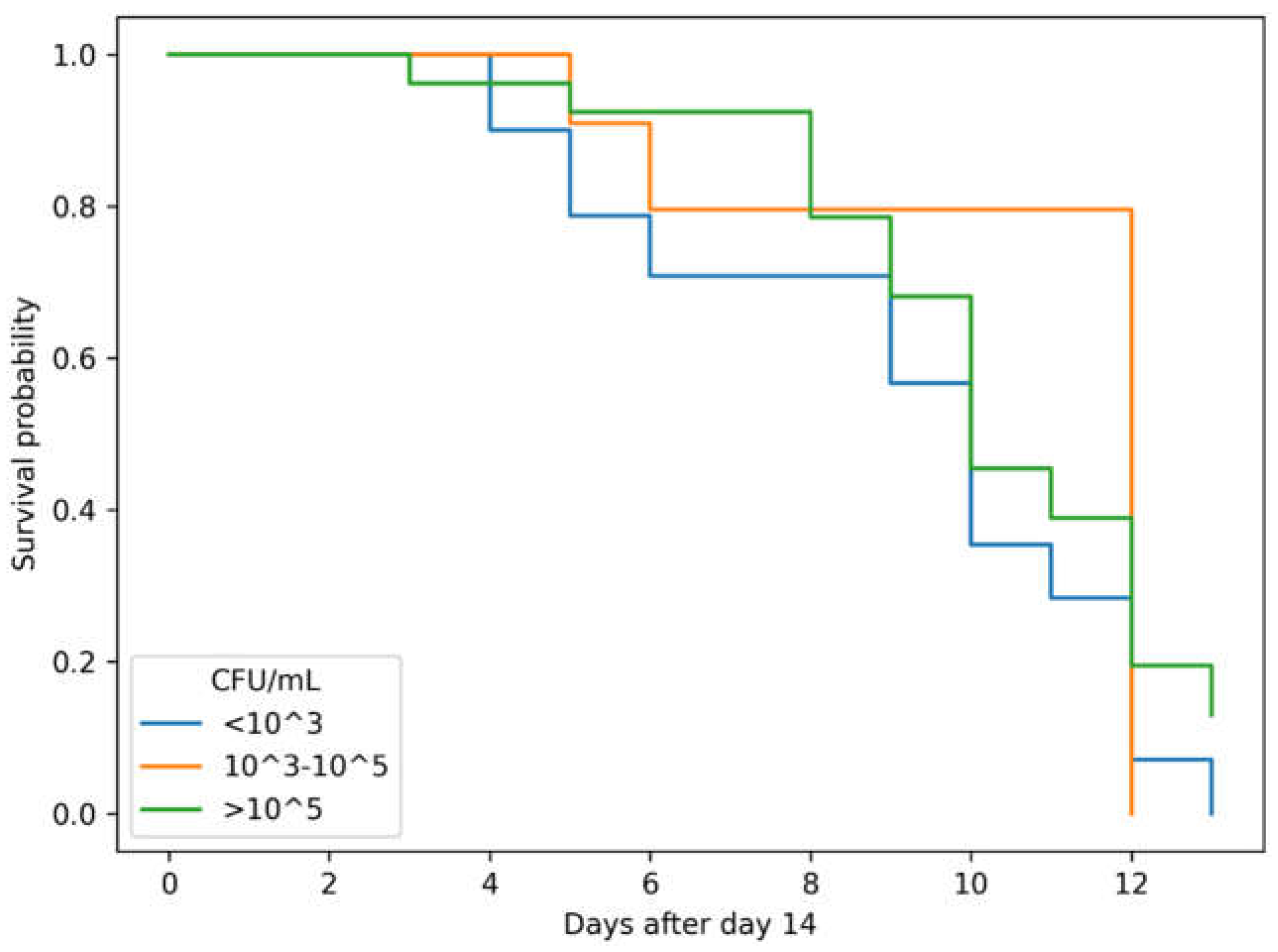
3.4. Landmark Analysis of Mortality (Day 14)
In the landmark analysis including patients alive on day 14, the risk of death increased with increasing degree of bacterial colonization of the small intestine. The data are presented in Table 4.
Figure 2.
Kaplan–Meier survival curves after day 14 according to bacterial load.
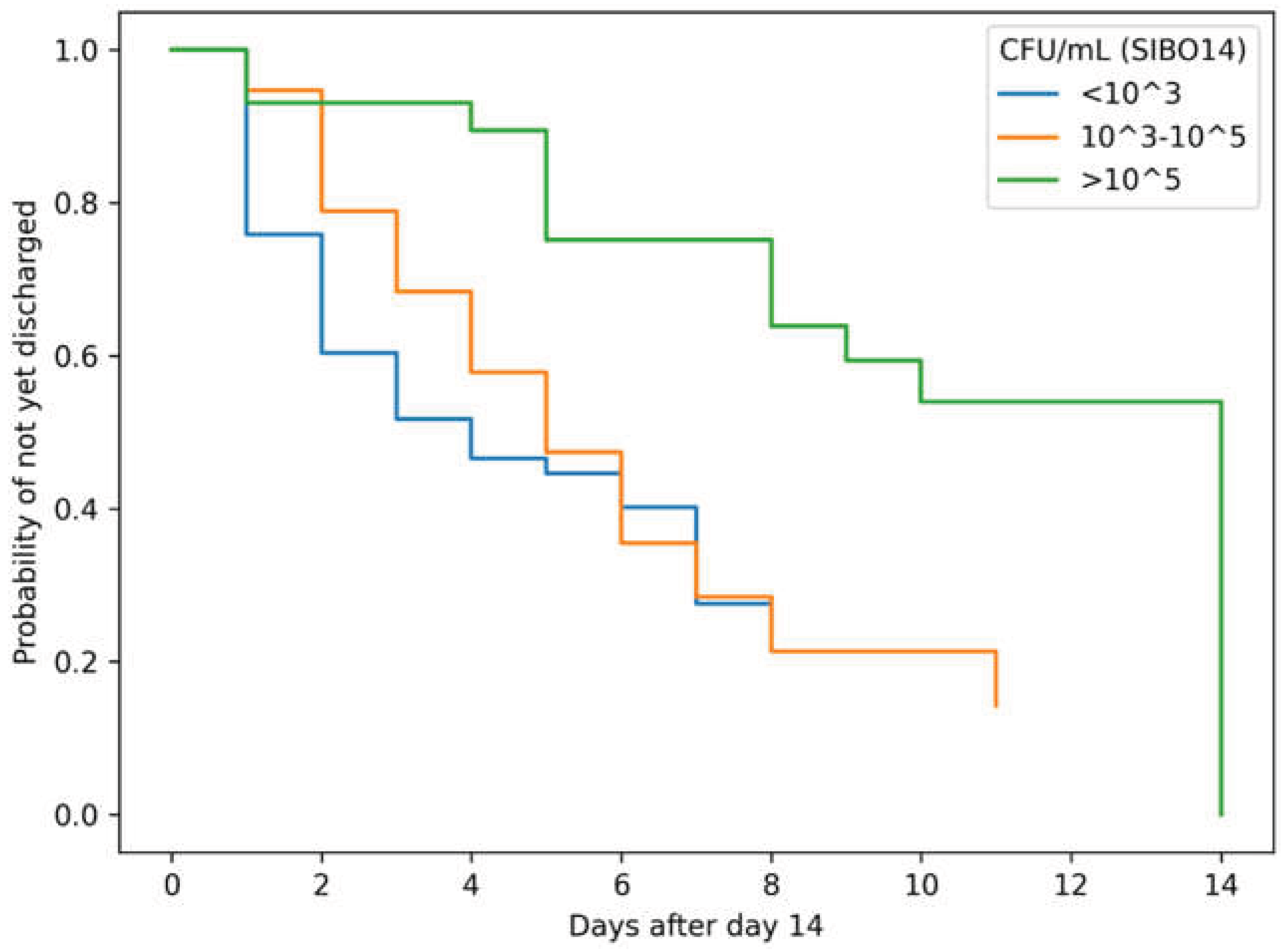
3.5. Landmark Analysis of Discharge
Landmark analysis demonstrated an association between the degree of bacterial colonization and the probability and timing of discharge. Death was treated as a competing event. The results are presented in Table 5.
Figure 3.
Landmark Kaplan–Meier curves for time to discharge after day 14.
4. Discussion
In our study, classical clinical predictors such as age, the degree of neurological impairment at admission, and respiratory dysfunction were independent risk factors for in-hospital mortality in severe TBI. This fully agrees with previous large multicenter studies in which age was recognized as one of the strongest prognostic factors of traumatic brain injury outcome [1,7]. In several cohort and prognostic analyses, age demonstrated an almost linear relationship with the probability of an unfavorable outcome and mortality, with elderly patients having a significantly worse prognosis [8,9].
The level of consciousness measured by the Glasgow Coma Scale (GCS) is a fundamental clinical predictor of outcome and is included in all widely recognized international prognostic models, including IMPACT and CRASH, where decreasing GCS is consistently associated with an exponential increase in mortality [3,8]. Similarly, in our model, GCS retained independent prognostic value.
Gas exchange disturbances are also considered important determinants of an unfavorable outcome. It is known that hypoxemia aggravates secondary ischemic brain injury, increases intracranial pressure, and is associated with increased mortality in neurocritical care patients [9,10]. In several studies, the PaO₂/FiO₂ ratio was used as an objective indicator of respiratory dysfunction and was independently associated with fatal outcomes in critically ill patients [11].
Similar results were obtained in studies of trauma populations in intensive care units, where the combination of severe neurological deficit and respiratory failure significantly increased the risk of in-hospital mortality [12].
Thus, the clinical factors identified in our work fully correspond to previously published data and confirm the validity of the studied cohort.
The degree of bacterial colonization of the small intestine on days 12–14 (CFU14) demonstrated a pronounced and independent association with in-hospital mortality and length of hospitalization. It is important to emphasize that this indicator should be considered not as a baseline predictor, but as a late dynamic marker of the severity of the critical condition, reflecting the development of intestinal dysfunction during treatment.
Small intestinal bacterial overgrowth syndrome (SIBO) has traditionally been studied mainly in gastroenterological practice. According to current clinical guidelines, SIBO is defined as a pathological increase in bacterial load in the small intestine, most often with a threshold of ≥10⁵ CFU/mL in aspirate [6].
In the general population, the prevalence of SIBO remains relatively low and, according to systematic reviews, ranges from 2 to 22% depending on the diagnostic method and criteria [13]. Thus, the low frequency of pronounced bacterial hypercolonization at admission identified in our study (CFU1, CFU/ml >10⁵ about 4%) corresponds to data for a conditionally “healthy” or uncomplicated population and confirms that severe bacterial growth is not the baseline state of most patients.
At the same time, already after 12–14 days of treatment in the intensive care unit, the frequency of pronounced hypercolonization in our cohort increased significantly, and the indicator itself became a strong independent marker of an unfavorable outcome. Similar observations have been described in other studies of critically ill patients. Thus, in a prospective study of ICU patients, SIBO was detected in approximately 36% of patients and was associated with complications and prolonged hospital stay [14].
Pathophysiologically, the results we obtained appear logical. It is known that patients with severe TBI often develop pronounced gastrointestinal dysmotility, slowing of peristalsis, and stasis of intestinal contents, which create conditions for excessive bacterial growth [15]. Additionally, the use of sedatives, opioids, vasopressors, and prolonged mechanical ventilation aggravates impairment of intestinal motility and barrier function.
Disruption of intestinal barrier integrity and the phenomenon of bacterial translocation are considered key mechanisms of systemic inflammation and multiple organ failure in intensive care [5,16]. In this context, SIBO may act not only as a local microbiological phenomenon but also as an indicator of a generalized inflammatory response and the severity of organ dysfunction.
Moreover, acid-suppressive therapy (proton pump inhibitors) and antibiotics used in intensive care units are able to alter the composition of the microbiota and contribute to hypercolonization of the small intestine [17]. These factors could additionally contribute to the increase in bacterial load in our cohort.
Thus, if at admission the small intestinal microbiota in most patients corresponded to conditionally normal values, then the development of pronounced bacterial growth by day 14 probably reflects a combination of intestinal hypomotility, barrier dysfunction, drug effects, and systemic inflammation. This may explain a strong association we identified between CFU14 and increased mortality and longer hospital stay.
Consequently, the obtained data allow small intestinal hypercolonization on days 12–14 to be considered a potential late biomarker of an unfavorable course of critical illness, complementing traditional clinical predictors.
In the present study, pronounced bacterial hypercolonization of the small intestine on days 12–14 (CFU/mL >10⁵) proved to be a strong independent factor associated with mortality, as well as with slower discharge after day 14. It is important to emphasize that hypercolonization of the small intestine on days 12–14 should be considered primarily as a “late marker,” rather than a baseline predictor, since it reflects the dynamics of the critical condition and the development of intestinal dysfunction during treatment [6].
The prevalence of SIBO in the general/healthy population varies substantially depending on the diagnostic method (breath tests vs aspirate), criteria, and thresholds; however, in most studies, SIBO in healthy controls is detected within approximately <2%–22% [18]. Clinical reviews and methodological works also emphasize that the “gold standard” (small intestinal aspirate culture) is limited by invasiveness and the risk of contamination, whereas breath tests have limitations in sensitivity and specificity [6,19].
Against this background, our baseline data appear expected: at admission, pronounced SIBO (>10⁵ CFU/mL) was observed rarely (about 4%), which is comparable with the lower estimates for the “conditionally healthy” prevalence and confirms that in most patients severe hypercolonization is not a baseline condition but develops later. At the same time, already on days 12–14, the proportion of patients with >10⁵ CFU/mL in our cohort increased noticeably (in the landmark sample), which is consistent with the concept that critical illness is accompanied by impaired motility/barrier function and dysbiosis [20,21].
Data on SIBO in the ICU are indeed more limited than in outpatient populations; however, in recent years studies have appeared indicating a high prevalence of SIBO in critically ill patients. In a prospective observational study in mechanically ventilated ICU patients, SIBO was detected in approximately 36.5% of patients and was associated with unfavorable ICU surrogates (for example, VAP and longer length of stay) [14].
This is in good agreement with our conclusion that pronounced hypercolonization on days 12–14 reflects disease severity and is accompanied by worse clinical outcomes.
Pathophysiologically, our results can be explained by the following reasons:
- Gastrointestinal dysmotility in the ICU. Critically ill patients often develop impaired motility of the stomach and small intestine; key factors include mechanical ventilation, vasopressors, opioids/sedation, severe systemic inflammatory response, and metabolic disorders [21,22]. Slowing of intestinal transit and decreased propulsive peristalsis create conditions for bacterial hypercolonization and retrograde migration of flora.
- Barrier dysfunction and translocation. Critical illness is accompanied by increased intestinal permeability and the risk of bacterial/endotoxin translocation, which is discussed within the concepts of “gut-origin sepsis” and gut-induced MODS [5,23]. In this context, SIBO may be not only a local phenomenon but also part of a systemic cascade of inflammation and organ dysfunction.
- Acid suppression and antibiotics. All our patients widely received PPIs/H2-blockers (stress ulcer prophylaxis) and antibiotics, which may alter the microbial profile and facilitate excessive bacterial growth. The association between acid suppression and SIBO/increased bacterial titers has been described in clinical studies and reviews [24].
- Enteral nutrition and postpyloric tube placement. Although enteral nutrition generally supports mucosal trophism, in severe critical illness the combination of nutritional load, dysmotility, and changes in biliary-pancreatic secretion may contribute to dysbiosis. Additionally, the very fact of prolonged postpyloric tube placement (in our case beyond the ligament of Treitz) facilitates access/contamination and may change local conditions [25,26]. Collectively, these mechanisms explain well why baseline CFU1 in most patients is low, but by days 12–14, under conditions of prolonged mechanical ventilation/sedation/acid suppression/antibiotics/vasopressors and pronounced gastrointestinal dysfunction, significant bacterial growth may develop, which in our cohort is associated with worsening prognosis.
It should be noted that data on quantitative assessment of bacterial load by small intestinal aspirate in ICU/neurocritical care patients are substantially fewer than breath test data in other patient categories [6], which contributes to the relevance of the present study.
5. Conclusions
In patients with severe traumatic brain injury, classical clinical variables, including age, neurological status assessed by the Glasgow Coma Scale, and oxygenation parameters, remain independent predictors of in-hospital mortality. These findings are consistent with previously published prognostic models and confirm the validity of the studied cohort.
At the same time, the degree of bacterial colonization of the small intestine assessed on days 12–14 (CFU14) demonstrated a strong and independent association with mortality and length of hospital stay. Unlike baseline clinical characteristics, this parameter should be considered a late dynamic marker reflecting the development of gastrointestinal dysfunction during critical illness rather than an initial predictor.
Baseline bacterial colonization at admission (CFU1) did not demonstrate independent prognostic significance, whereas pronounced hypercolonization during intensive care was associated with worse outcomes, delayed discharge, and increased mortality risk. These findings suggest that intestinal dysbiosis and impaired gut barrier function may play an important role in the systemic pathophysiology of critically ill neurotrauma patients.
Thus, assessment of small intestinal bacterial load during treatment may complement traditional clinical predictors and improve risk stratification in patients with severe traumatic brain injury.
Further prospective multicenter studies are required to confirm the prognostic value of SIBO and to clarify whether modulation of intestinal microbiota could represent a potential therapeutic target in this population.
6. Limitations
The present study has several limitations that should be taken into account when interpreting the obtained results.
First, the study has a retrospective two-center design, which potentially limits the generalizability of the conclusions and does not allow complete exclusion of the influence of hidden confounding factors. However, the consecutive inclusion of all patients with severe TBI and the use of standardized intensive care protocols made it possible to minimize systematic selection bias.
Second, quantitative assessment of bacterial colonization was performed based on culture of small intestinal aspirate. Although this method is considered a reference (“gold standard”) for the diagnosis of SIBO [6], it remains invasive and is theoretically susceptible to the risk of sample contamination. Nevertheless, sampling was performed through a postpyloric tube according to a unified technique, which reduces the probability of diagnostic error.
Third, the composition of the intestinal microbiota in intensive care unit patients may be influenced by numerous factors, including antibiotic therapy, acid-suppressive drugs, sedatives, vasopressors, and features of enteral nutrition. These interventions are part of the standard treatment of critically ill patients and could act as potential confounders; however, at the same time, they reflect real clinical practice and therefore increase the external validity of the results.
Fourth, assessment of SIBO was performed only at two time points (at admission and on days 12–14), which does not allow tracking the exact dynamics of the development of bacterial hypercolonization. Future studies with more frequent microbiota monitoring could clarify the temporal patterns of SIBO formation in neurocritical care patients.
Fifth, breath tests (hydrogen/methane) were not used. However, in intubated critically ill patients, conducting such studies is technically difficult and may be less accurate compared with direct microbiological examination of aspirate.
Finally, despite the use of multivariable analysis, it is impossible to completely exclude the influence of unmeasured factors. Therefore, the identified association between pronounced bacterial hypercolonization and mortality does not prove a causal relationship and requires confirmation in prospective multicenter studies.
Nevertheless, the strengths of the study include a relatively homogeneous cohort of patients with severe TBI, the use of a quantitative microbiological method, the application of the landmark approach, as well as the consistency of results obtained by different statistical methods (logistic regression, Kaplan–Meier analysis, and ROC curves), which increases the reliability of the conclusions obtained.
Antibiotic exposure and proton pump inhibitor use were not quantitatively adjusted in the regression model.
Author Contributions
Conceptualization: O.O.; Methodology: O.O.; Formal analysis: O.Y.; Investigation: O.Y., K.K.; Data curation: O.Y.; Writing – original draft: O.O., M.R., J.K.; Writing – review and editing: O.O. M.R.; Supervision: M.R.; Project administration: M.R.; Funding acquisition: M.R. All authors have read and agreed to the published version of the manuscript.
Funding
Wroclaw University of Science and Technology.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Bioethics Committee of Ternopil National Medical University (No. 239, 18 August 2022).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
The data presented in this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors acknowledge the use of an artificial intelligence–based language tool (ChatGPT, OpenAI, San Francisco, CA, USA) for assistance with English translation. The authors reviewed and approved all content.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Dewan, MC; Rattani, A; Gupta, S; Baticulon, RE; Hung, YC; Punchak, M.; et al. Estimating the global incidence of traumatic brain injury. J Neurosurg. 2018, 130(4), 1080–1097. [Google Scholar] [CrossRef]
- Maas, AIR; Menon, DK; Manley, GT; Abrams, M; Åkerlund, C; Andelic, N; et al. Traumatic brain injury: progress and challenges in prevention, clinical care, and research . Lancet Neurol. 2022, 21(11), 1004–1060. [Google Scholar] [CrossRef]
- Steyerberg, EW; Mushkudiani, N; Perel, P; Butcher, I; Lu, J; McHugh, GS; et al. Predicting outcome after traumatic brain injury: development and international validation of prognostic scores based on admission characteristics. PLoS Med. 2008, 5, e165. [Google Scholar] [CrossRef]
- Schuijt, TJ; Lankelma, JM; Scicluna, BP; et al. The gut microbiota plays a protective role in the host defence against pneumococcal pneumonia. Gut 2016, 65, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Zaborin, A; Smith, D; Garfield, K; et al. Membership and behavior of ultra-low-diversity pathogen communities present in the gut of humans during prolonged critical illness. mBio 2014, 5(5), e01361-14. [Google Scholar] [CrossRef] [PubMed]
- Prognosis in Moderate and Severe Traumatic Brain Injury: A Systematic Review of Contemporary Models and Validation Studies . J Neurotrauma 2020, 37(1), 1–13. [CrossRef]
- Lingsma, HF; Roozenbeek, B; Steyerberg, EW; Murray, GD; Maas, AIR. Early prognosis in traumatic brain injury: from prophecies to predictions. Lancet Neurology 2010, 9, 543–554. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Head injury: assessment and early management (NICE guideline NG232); NICE: London, 2023. [Google Scholar]
- Carney, N; Totten, AM; O’Reilly, C; Ullman, JS; Hawryluk, GWJ; Bell, MJ; et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 2017, 80, 6–15. [Google Scholar] [CrossRef]
- Hawryluk, GWJ; Rubiano, AM; Totten, AM; O’Reilly, C; Ullman, JS; Bratton, SL; et al. Guidelines for the Management of Severe Traumatic Brain Injury: 2020 update of the decompressive craniectomy recommendations. Neurosurgery 2020, 87(3), 427–434. [Google Scholar] [CrossRef] [PubMed]
- Acute respiratory distress syndrome: the Berlin definition. JAMA 2012, 307, 2526–2533. [CrossRef]
- Ulvik, A; Kvåle, R; Wentzel-Larsen, T; Flaatten, H. Multiple organ failure after trauma affects long-term survival and functional status. Critical Care 2007, 11, R95. [Google Scholar] [CrossRef]
- Pimentel, M; Saad, RJ; Long, MD; Rao, SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. Am J Gastroenterol. 2020, 115, 165–178. [Google Scholar] [CrossRef]
- Karakosta, A; Katsanos, K; Tsirigotis, P; Vrettou, C; Chatzimichail, A; Liaskos, C; et al. High prevalence of small intestinal bacterial overgrowth syndrome in ICU patients: an observational study. J Intensive Care Med. 2024, 39, 355–362. [Google Scholar] [CrossRef]
- Deane, AM; Chapman, MJ; Fraser, RJ; Bryant, LK; Burgstad, C; Nguyen, NQ. Mechanisms underlying feed intolerance in the critically ill: implications for treatment. World J Gastroenterol. 2007, 13(29), 3909–3917. [Google Scholar] [CrossRef] [PubMed]
- Assimakopoulos, SF; Triantos, C; Thomopoulos, K; Fligou, F; Maroulis, I; Marangos, M; et al. Gut-origin sepsis in the critically ill patient: pathophysiology and treatment. Infection 2018, 46(6), 751–760. [Google Scholar] [CrossRef] [PubMed]
- Su, T; Lai, S; Lee, A; He, X; Chen, S. Meta-analysis: proton pump inhibitors moderately increase the risk of small intestinal bacterial overgrowth. Journal of Gastroenterology 2018, 53, 27–36. [Google Scholar] [CrossRef]
- Rezaie, A; Buresi, M; Lembo, A; et al. Hydrogen and methane-based breath testing in gastrointestinal disorders: the North American Consensus. Am J Gastroenterol. 2017, 112, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Kashyap, P; Moayyedi, P; Quigley, EMM; Simren, M; Vanner, S; et al. Critical appraisal of the SIBO hypothesis and breath testing. Neurogastroenterol Motil 2024, 36, e14817. [Google Scholar] [CrossRef]
- Wischmeyer, PE. Tailoring nutrition therapy to illness and recovery. Critical Care 2017, 21 (Suppl 3), 316. [Google Scholar] [CrossRef]
- Govil, D; Pal, D. Gastrointestinal motility disorders in critically ill. Indian J Crit Care Med 2020, 24 (Suppl 4), S179–S182. [Google Scholar] [CrossRef]
- Ladopoulos, T; Giannaki, M; Alexopoulou, C; Proklou, A; Pediaditis, E; Kondili, E. Gastrointestinal dysmotility in critically ill patients. Ann Gastroenterol. 2018, 31, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Potruch, A; Schwartz, A; Ilan, Y. The role of bacterial translocation in sepsis. Ther Adv Gastroenterol. 2022, 15, 17562848221094214. [Google Scholar] [CrossRef] [PubMed]
- Dukowicz, AC; Lacy, BE; Levine, GM. Small intestinal bacterial overgrowth: a comprehensive review. Gastroenterol Hepatol (N Y) 2007, 3, 112–122. [Google Scholar] [PubMed]
- Singer, P; Blaser, AR; Berger, MM; Alhazzani, W; Calder, PC; Casaer, MP; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clinical Nutrition 2019, 38, 48–79. [Google Scholar] [CrossRef]
- Jiyong, J; Tiancha, H; Huiqin, W; Jingfen, J. Effect of gastric versus post-pyloric feeding on the incidence of pneumonia in critically ill patients: observations from traditional and Bayesian random-effects meta-analysis. Clin Nutr. 2013, 32, 8–15. [Google Scholar] [CrossRef]

Table 1.
Descriptive statistics of baseline demographic and clinical characteristics (n = 174).
| Parameter | Minimum | QI (25%) | Median | QIII (75%) | Maximum |
| Age, years | 22 | 43 | 48 | 62.75 | 74 |
| Body mass index, kg/m² | 26 | 29 | 31 | 33.0 | 36 |
| GCS at admission, points | 5 | 7 | 7 | 8.0 | 8 |
| PaO₂/FiO₂ | 305 | 345 | 356 | 378 | 411 |
| PaCO₂, mmHg | 33 | 38 | 44 | 45 | 46 |
| Blood glucose, mmol/L | 5 | 7 | 8 | 10 | 11 |
Table 2.
CFU1 — degree of bacterial colonization of the small intestine at admission.
| CFU1 category | n | % |
| <10³ | 148 | 85.1 |
| 10³–10⁵ | 19 | 10.9 |
| >10⁵ | 7 | 4.0 |
| Total | 174 | 100 |
Table 3.
Results of multivariable logistic regression analysis.
| Variable | OR | 95% CI | p-value |
| Age (per 1 year) | 1.06 | 1.03–1.10 | <0.001 |
| GCS (per 1 point) | 0.48 | 0.28–0.83 | 0.008 |
| PaO₂/FiO₂ | 0.74 | 0.68–0.91 | 0.006 |
| Glucose | 1.13 | 0.92–1.40 | 0.245 |
| CFU14 >10⁵ | 5.15 | 2.15–12.34 | <0.001 |
Table 4.
Landmark analysis of mortality after day 14.
| CFU14 | Number of patients (n) | Deaths | Mortality risk (%) |
| <10³ | 58 | 18 | 31.0 |
| 10³–10⁵ | 19 | 4 | 21.1 |
| >10⁵ | 29 | 16 | 55.2 |
| Total | 106 | 38 | 35.8 |
Table 5.
Landmark analysis of discharge after day 14.
| CFU14 | n | Discharged | Discharge rate (%) | Median days to discharge |
| <10³ | 58 | 40 | 69.0 | 4 |
| 10³–10⁵ | 19 | 15 | 78.9 | 5 |
| >10⁵ | 29 | 14 | 48.3 | 8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



