Submitted:
10 February 2026
Posted:
12 February 2026
You are already at the latest version
Abstract
Environmental accumulation and human exposure to micro- and nanoplastics (MNPs) are increasing as plastic production rises, yet whether this has been paralleled by greater bioaccumulation in human lungs remains unclear. We conducted a comparative study of paraffin-embedded lung tissues collected post mortem from two series of autopsy cases from the same tertiary care medical center, including individuals who died in 1991 (n = 42) and in 2024 (n = 57). Microplastic abundance, size, and polymer type were assessed using laser-direct infrared (LDIR) imaging. Confirmatory analyses were performed in representative subsets using pyrolysis–gas chromatography/mass spectrometry and scanning electron microscopy. Collagen I staining and CD68 infiltration were evaluated to assess fibrosis and inflammation. MNPs were identified by LDIR in lung samples from 8 of 42 individuals (19%) who died in 1991 and 44 of 57 (77%) who died in 2024. The median MNP burden per gram of tissue (interquartile range) increased from 12.9 particles (11.3–13.7) to 19.9 (15.5–28.2), while mean particle diameter decreased. Polymer composition shifted from polyethylene predominance (51.7%) in 1991 to a more heterogeneous profile in 2024, including polyethylene terephthalate (28.4%), polyvinyl chloride (14.3%), and polystyrene (14.2%), findings corroborated by pyrolysis–gas chromatography/mass spectrometry and scanning electron microscopy. Lung samples containing MNPs showed greater CD68 and collagen I abundance than samples without detectable MNPs. Over the past three decades, MNP contamination of human lung tissue has become markedly more prevalent, compositionally diverse, and characterized by smaller particles, with accompanying histological features consistent with inflammation and fibrosis.
Keywords:
microplastics
; nanoplastics
; lung
; accumulation
; trend
; inflammation
; fibrosis
Introduction
Plastics are pervasive in modern life. However, plastics’ wide and increasing use has resulted in extensive plastic pollution [1]. Waste plastic released into the environment degrades to produce micro- and nanoplastics (MNPs), fragments smaller than 5 mm and 1 µm, respectively. MNPs are identified today in ecosystems worldwide [2]. Recently, MNPs have been detected in many human organs. In selected cases, they are associated with adverse clinical outcomes [3,4,5,6].
Plastic production has increased almost six-fold since the early 1990s, reaching an annual rate of nearly 600 million metric tons at present [1,7]. This increasing output is associated with progressively rising levels of MNPs in multiple ecosystems [1,8,9]. Preliminary evidence suggests that such environmental trends might be mirrored in human tissues [5]. The lung, continuously exposed to inhaled particles, is a critical site for assessing temporal trends in human exposure to pollution, representing a potential reservoir for airborne contaminants including MNPs [10]. However, no study to date has evaluated whether pulmonary bioaccumulation of MNPs has changed over time nor how the composition or morphology of MNPs have evolved.
To address this question, we conducted a comparative analysis of post-mortem lung specimens from two autopsy cases collected in 1991 and in 2024, respectively. Using laser-direct infrared (LDIR) imaging, we assessed MNP number, size distribution, and polymer composition in the two case series. To corroborate findings obtained from LDIR imaging, we analyzed a subset of 20 random samples, i.e. 10 from each case series, with pyrolysis–gas chromatography/mass spectrometry (Py-GC/MS) and scanning electron microscopy (SEM). This orthogonal, multi-technique strategy provides converging evidence by combining mass-based polymer identification with particle-based chemical imaging and morphological characterization, consistent with recent recommendations to communicate analytical confidence in the identification of human MNPs [11]. In addition, we compared collagen I deposition and CD68 abundance in positive vs negative samples for MNPs to evaluate fibrosis and inflammation associated with the presence of MNPs.
Methods
Study Design
We performed a comparative autopsy-based study using lung tissue samples collected post-mortem from two independent case series of deceased individuals. The first comprised autopsies performed between January and December 1991 at the Institute of Legal/Forensic Medicine of University Hospital of Campania “Luigi Vanvitelli” and the second consisted of autopsies performed between January and September 2024 at the same institution using identical procedures. In both cases, corpses were kept at 5 °C and autopsies were performed with a standardized protocol based on a sequential examination of all organs. For both case series, only paraffin sections obtained from the posterior basal segment of the lower lobes were considered, in order to minimize variability related to regional exposure within the lung. Inclusion criteria for samples were: 1- being derived from autopsies with a minimum dataset of information relative to age and sex of the individual, and availability of data; 2- being derived from an autopsy performed within 48 hours from the declaration of death, from corpses with no signs of decomposition, and not dead for pulmonary causes; 3- availability of the appropriate segment of the lung and preserved histological structure. Data were retrieved from archived records for the 1991 series and from electronic databases for the 2024 cases and were used in an anonymized manner for data analysis. The study design in summarized in Supplementary Figure S1.
Lung tissues were fixed in 10% buffered formalin and embedded in paraffin through standard histopathologic procedures. The subsequent laboratory procedures were conducted under strict anti-contamination conditions, using non-plastic equipment. Blank paraffin sections and procedural blanks performed with the same methodology were also prepared in a subsequent moment and tested as a quality-control measure. The Institutional Ethics Committee of the University of Campania “Luigi Vanvitelli” approved the study.
End Points and Sample Size Estimation
The primary endpoint was the total abundance of microplastic particles in lung tissue in the 2024 vs the 1991 case series, as measured by LDIR. Secondary endpoints included MNP presence (yes/no) in the two series, mean particle diameter, and polymer composition. Py-GC/MS and SEM were used as confirmatory technologies for these endpoints in a randomly selected subset of samples. Ancillary endpoints were the abundance of CD68 and Collagen I in MNP-positive vs MNP-negative samples.
To estimate the sample size, a previous study suggested that brain samples collected post-mortem from individuals deceased either in 2016 or 2024 and analyzed with Py-GC/MS showed a mean difference of 1572 µg g−1 with a standard deviation (estimated from quartiles through the formula Q3-Q1/1.35) of 2222 µg g−1 [5]. Considering an alpha of 0.05, a beta of 0.2, and an expected proportion of 70% vs 30% of samples in the 2024 vs 1991 case series, we calculated a sample size of 80 sections using the T statistic and non-centrality parameter, with the intention of comparing two means of a continuous measure. We increased such estimate by 20% and set a target of 96 samples.
Quantitation and Characterization of MNPs, and Immunohistochemistry
Quantitation and characterization of MNPs through LDIR, Py-GC/MS, and SEM, as well as the immunochemistry analyses relative to CD68 and Collagen I are detailed in the Supplementary Methods.
Statistical Analysis
Continuous variables were assessed for normality through the Shapiro-Wilk test and expressed as median (IQR) or mean ±SD, while categorical variables as n (%). MNPs prevalence, abundance, and size were compared between the two case series using the Mann–Whitney U test for continuous data and the Fisher exact test for categorical variables. A comparison between MNP positive and MNP negative samples, independently of case series, was also performed. A two-tailed P value of <.05 was considered statistically significant. Statistical analyses were performed using GraphPad Prism, version 9.1.2.
Results
The final number of samples included in the study derived from 99 autopsy cases: 42 collected in 1991 and 57 in 2024 (Figure 1A). The demographic and clinical characteristics of the two series are summarized in Table 1. The mean (SD) age was 61±11 years in 1991 and 64.9±9.4 years in 2024; 69.1% and 59.6% of participants were men, respectively. There were no differences in terms age, sex, causes and season of death between the two case series.
Representative LDIR micrographs for the two case series are shown in Figure 1B while an example of particles detected for each polymer with the associated spectra is reported in Supplementary Figure S2. Microplastics were identified in 8 of 42 lungs (19%) from 1991 and in 44 of 57 lungs (77%) from 2024 (Figure 1C). Among those with evidence of microplastics, the median (Q1-Q3) particle count increased from 12.9 (11.3-13.7) in 1991 to 19.9 (15.5-28.2) microplastics/g of tissue in 2024 (Figure 1D). Polymer composition shifted from polyethylene (PE) (51.7%) and polypropylene (PP) (27.8%) predominance in 1991 to a more heterogeneous pattern in 2024, i.e. polyethylene terephthalate (PET) (28.4%), polyvinyl chloride (PVC) (14.3%), polystyrene (PS) (14.2%), PE (27.5%), and PP (13.5%) (Figure 1E). Relative to morphology, particles detected in samples from 1991 had a larger diameter compared with those in 2024 samples (Figure 1F).
To corroborate findings obtained from LDIR imaging, we analyzed a subset of 20 random samples, i.e. 10 from each case series, also with Py-GC/MS and SEM (11). The baseline characteristics of these cases were comparable with the rest of the population (Supplementary Table S1). Py-GC/MS corroborated the findings relative to the higher prevalence (Figure 2A) and the more variegated repertoire (Figure 2B) of MNPs in samples derived from the 2024 and compared with the 1991 series. Evaluation of these cases using the back-scattered electrons with SEM and derived spectral x-ray maps evidenced some particles showing a reduction in the presence of carbon and a greater abundance of sulfur (Figure 2C and Supplementary Figure S3). Given the probable non-biologic nature of this amount of localized sulfur deposits, these results suggest the presence of MNPs derived from vulcanized plastics. The presence of such particles was more pervasive in the 2024 case series.
We then compared the characteristics between samples positive (n = 52) vs those negative (n= 47) for microplastics, independently of the case series, and found no differences (Supplementary Table S2). However, samples with evidence of MNPs, compared with those without, showed a higher abundance of both Collagen I and CD68 (Supplementary Figure S4), suggesting a more consistent fibrotic and inflammatory burden.
Discussion
This comparative autopsy study provides the first direct evidence of a marked temporal increase in plastic contamination of the human lung. Over a 33-year interval, the prevalence of lungs containing detectable microplastics and their mean particle abundance increased substantially. These observations parallel the global surge in plastic-related pollution [1,7] and possibly align to the trend of MNPs abundance, heterogeneity, and size in the environment [8].
Only one previous study has explored trends in MNPs accumulation in humans, comparing individuals deceased either in 2016 or in 2024 [5]. In that study, Py-GC/MS data suggested an increasing MNPs concentration over time in liver and brain samples but not in kidney [5]. MNP abundance was not influenced by age, sex, ethnicity, or cause of death, similar to the results provided here. Our data, spanning a larger time range and focusing on a tissue directly exposed to air levels of pollutants, corroborates and extends those findings, thus sustaining the hypothesis that MNP accumulation is increasing over time in humans.
Previous studies have reported of MNPs in human lungs, in samples derived from both living and deceased individuals [12,13,14]. One study performed with lung samples from autopsy cases collected in 2021 and using a different methodology provided results similar to those presented here for the 2024 series in terms of both prevalence of MNPs positivity and types of polymer detected [12]. More broadly, studies with lung samples suggest PE, PET, and PP as the most common MNPs detected, possibly reflecting their widespread use [15].
Occupational exposure studies report a range of pulmonary diseases in workers exposed to different plastics [15]. However, whether exposure to ambient levels of MNPs in the general population and the related accumulation in the lungs are pathogenic phenomena is unknown. To this regard, the use of autopsy samples impedes the exploration of associations between MNPs and diseases, given the lack of this latter information. On the other hand, the higher degree of inflammation and fibrosis in samples positive for MNPs is consistent with preclinical data suggesting a pro-inflammatory and pro-fibrotic role for MNPs in the lung [15]. Further studies are needed to explore this issue.
Use of an autopsy case series entails risk of residual confounding, because detailed clinical and demographic information on individual patients was not available. In addition, given that we did not test autopsy samples derived from other centers our findings might not be geographically generalizable. Given the limit of detection with LDIR, we did not collect detailed data relative to the specific accumulation of nanosized particles, i.e. those more likely reaching the alveoli and the blood.
In summary, results of our study suggest that MNP contamination of the human lung is increasing over time and reflects increases in environmental plastic pollution in recent decades. These observations suggest the need for systematic biomonitoring of MNPs also in living individuals to explore the long-term health consequences of exposure to plastic-related pollution.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
RM, FP, RLG, VP, AM, CS, AC, PL, PP, MB, GP, and PI conceived the idea, designed and supervised the study, analyzed data, and wrote the manuscript. LG, GF, TS, LVM, MM, EM, DG, AF, FF, IP, GF, AF, SH, AF, SG, GF, CL, GM, Ach, FO, BA, ND, and MLB collected samples, recovered data, performed the experiments, provided background expertise, and/or reviewed the manuscript for intellectual content.
Funding
This work has been supported by Italian Ministry of Health through Ricerca Corrente to IRCCS MultiMedica, and by Ricerca Ateneofund for Outcomes Research in Cardiovascular Diseases. Role of the Funder/Sponsor: The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Conflict of Interest
The authors have no conflict of interests to declare relatively to this manuscript.
References
- Landrigan, P. J.; et al. The Lancet Countdown on health and plastics. Lancet 2025, 406, 1044–1062. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; et al. Potential Health Impact of Microplastics: A Review of Environmental Distribution, Human Exposure, and Toxic Effects. Environment & health 2023, 1, 249–257. [Google Scholar] [CrossRef]
- Marfella, R.; et al. Microplastics and Nanoplastics in Atheromas and Cardiovascular Events. The New England journal of medicine 2024, 390, 900–910. [Google Scholar] [CrossRef] [PubMed]
- Roslan, N. S.; et al. Detection of microplastics in human tissues and organs: A scoping review. Journal of global health 2024, 14, 04179. [Google Scholar] [CrossRef] [PubMed]
- Nihart, A. J.; et al. Bioaccumulation of microplastics in decedent human brains. Nature medicine 2025, 31, 1114–1119. [Google Scholar] [CrossRef] [PubMed]
- Prattichizzo, F.; et al. Micro-nanoplastics and cardiovascular diseases: evidence and perspectives. European heart journal 2024, 45, 4099–4110. [Google Scholar] [CrossRef] [PubMed]
- Geyer, R.; Jambeck, J. R.; Law, K. L. Production, use, and fate of all plastics ever made. Science advances 2017, 3, e1700782. [Google Scholar] [CrossRef] [PubMed]
- Miyazono, K.; et al. Long-Term Changes in the Abundance, Size, and Morphotype of Marine Plastics in the North Pacific. Environmental science & technology 2025, 59, 4608–4617. [Google Scholar] [CrossRef]
- Eberhard, T.; Casillas, G.; Zarus, G. M.; Barr, D. B. Systematic review of microplastics and nanoplastics in indoor and outdoor air: identifying a framework and data needs for quantifying human inhalation exposures. Journal of exposure science & environmental epidemiology 2024, 34, 185–196. [Google Scholar] [CrossRef]
- Laumbach, R. J.; Kipen, H. M. Respiratory health effects of air pollution: update on biomass smoke and traffic pollution. The Journal of allergy and clinical immunology 2012, 129, 3-11; quiz 12-13. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.V.; et al. Communicating Confidence in the Reliability of Micro- and Nanoplastic Identification in Human Health Studies. Environment & Health Article ASAP. [CrossRef]
- Amato-Lourenco, L. F.; et al. Presence of airborne microplastics in human lung tissue. Journal of hazardous materials 2021, 416, 126124. [Google Scholar] [CrossRef] [PubMed]
- Jenner, L. C.; et al. Detection of microplastics in human lung tissue using muFTIR spectroscopy. The Science of the total environment 2022, 831, 154907. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; et al. Microplastics in the Lung Tissues Associated with Blood Test Index. Toxics 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Vasse, G. F.; Melgert, B. N. Microplastic and plastic pollution: impact on respiratory disease and health. European respiratory review: an official journal of the European Respiratory Society 2024, 33. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Microplastics prevalence, abundance, size, and type in 1991 and 2024 case series according to LDIR. (A) Flowchart of samples inclusion for the 1991 and 2024 case series. (B) Representative LDIR images for the 1991 and 2024 case series. (C) Prevalence of microplastics (MNPs) in the two case series; *p < 0.001, Fisher’s exact test. (D) Number of microplastics per gram of tissue in positive samples from cases of 1991 vs 2024; *p < 0.001, Mann-Whitney test. (E) Relative distribution (%) of the different polymers identified in positive samples from the 1991 and 2024 case series. (F) Particle diameter of microplastics detected in positive samples from the 1991 and the 2024 case series; *p < 0.001, Mann-Whitney test. PE: Polyethylene, PP: Polypropylene, PET: Polyethylene terephthalate, PS: Polystyrene, PVC: Polyvinyl chloride, PA: Polyamide.
Figure 1.
Microplastics prevalence, abundance, size, and type in 1991 and 2024 case series according to LDIR. (A) Flowchart of samples inclusion for the 1991 and 2024 case series. (B) Representative LDIR images for the 1991 and 2024 case series. (C) Prevalence of microplastics (MNPs) in the two case series; *p < 0.001, Fisher’s exact test. (D) Number of microplastics per gram of tissue in positive samples from cases of 1991 vs 2024; *p < 0.001, Mann-Whitney test. (E) Relative distribution (%) of the different polymers identified in positive samples from the 1991 and 2024 case series. (F) Particle diameter of microplastics detected in positive samples from the 1991 and the 2024 case series; *p < 0.001, Mann-Whitney test. PE: Polyethylene, PP: Polypropylene, PET: Polyethylene terephthalate, PS: Polystyrene, PVC: Polyvinyl chloride, PA: Polyamide.
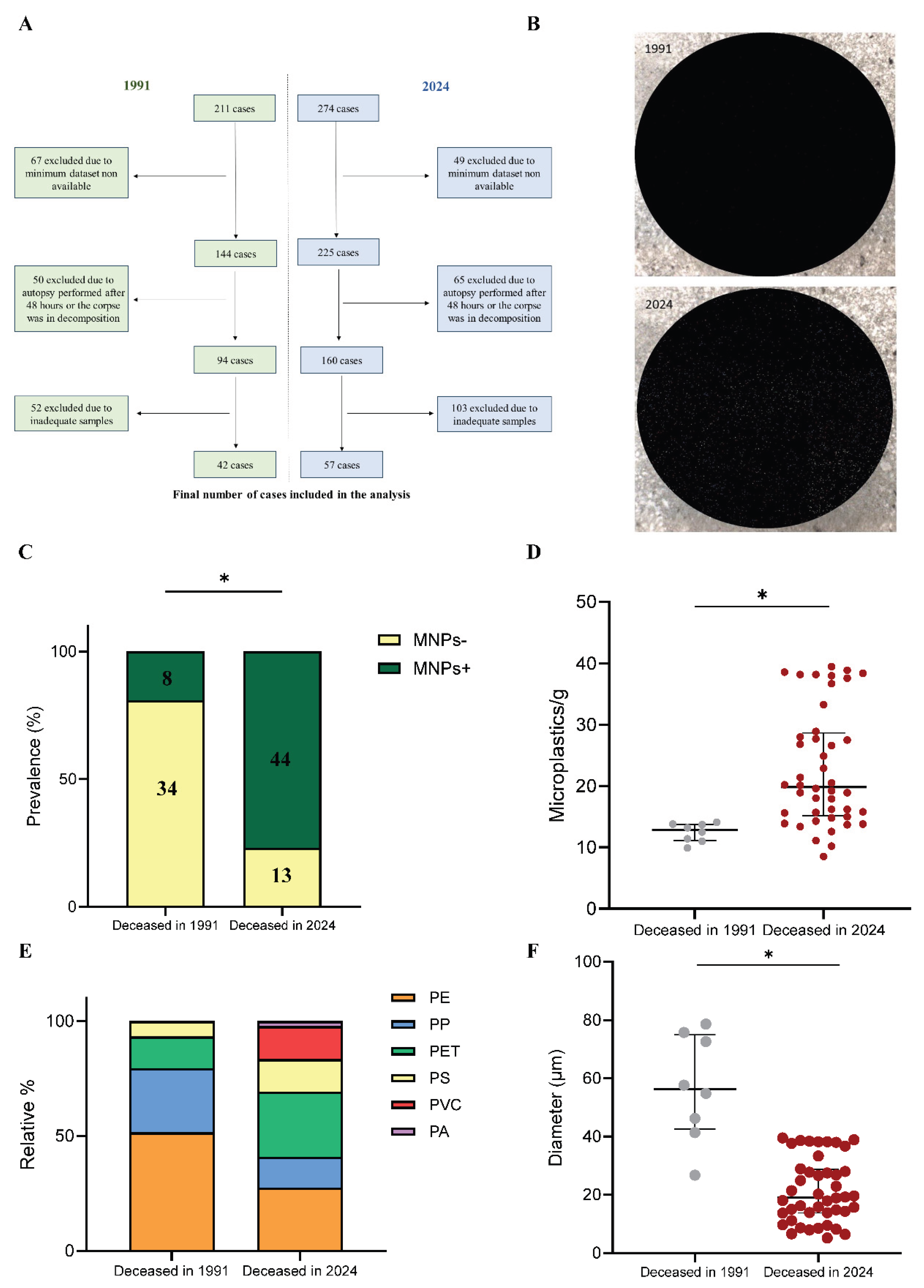
Figure 2.
Analysis with pyrolysis–gas chromatography/mass spectrometry and scanning electron microscopy in a subset of 20 samples. (A) Prevalence of micro- and nanoplastics (MNPs) in the 1991 and 2024 case series according to Py-GC/MS data; *p < 0.05, Fisher’s exact test. (B) Relative distribution (%) of the different polymers identified in positive samples from the 1991 and 2024 case series using the same technology. (C) Example of a particle identified with SEM in a sample from the 2024 case series, with the relative EDX spectrum suggesting a high abundance of sulphur.
Figure 2.
Analysis with pyrolysis–gas chromatography/mass spectrometry and scanning electron microscopy in a subset of 20 samples. (A) Prevalence of micro- and nanoplastics (MNPs) in the 1991 and 2024 case series according to Py-GC/MS data; *p < 0.05, Fisher’s exact test. (B) Relative distribution (%) of the different polymers identified in positive samples from the 1991 and 2024 case series using the same technology. (C) Example of a particle identified with SEM in a sample from the 2024 case series, with the relative EDX spectrum suggesting a high abundance of sulphur.
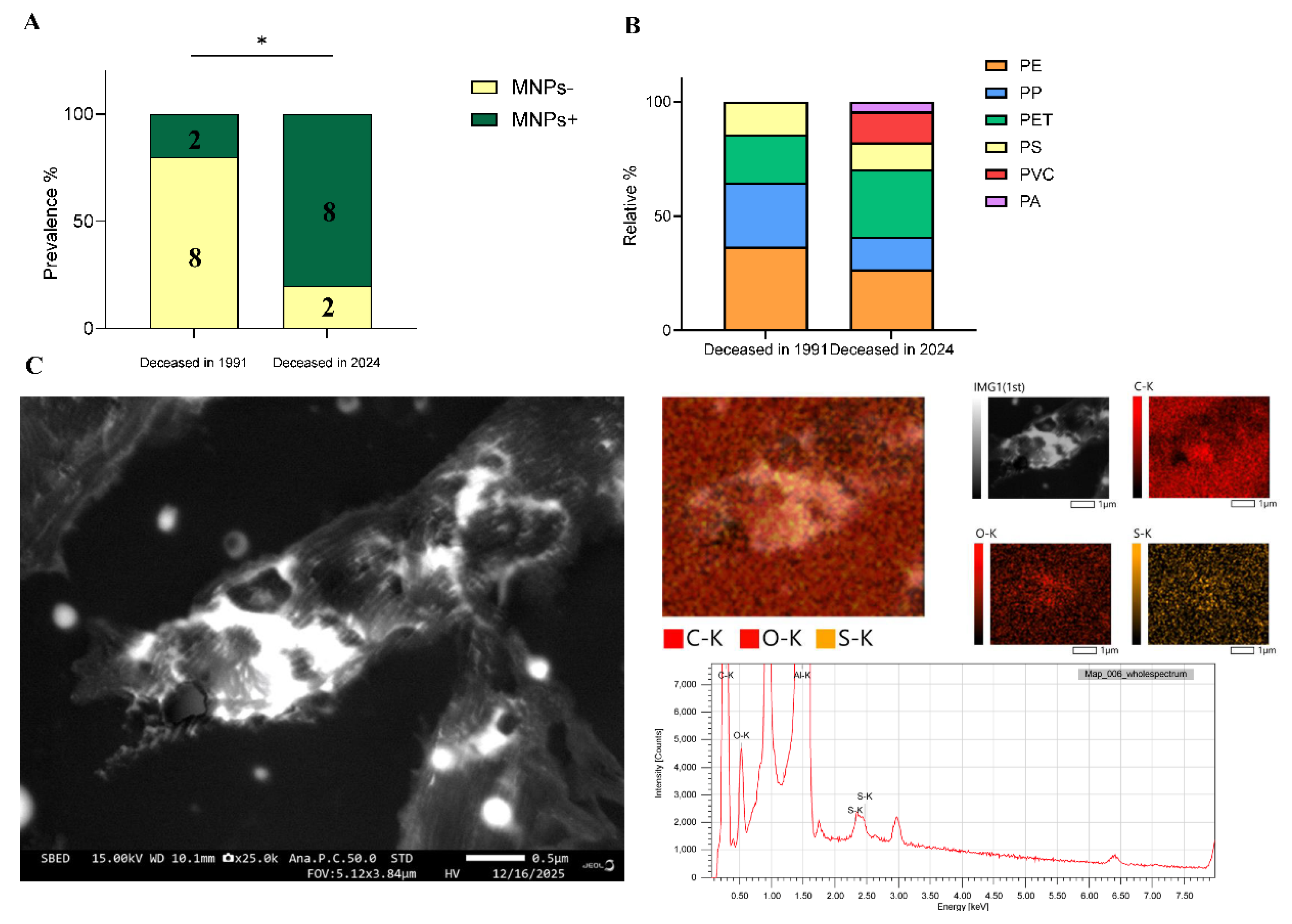

Table 1.
Demographic and clinical characteristics of the two case series.
| Variable | Deceased in 1991 (n=42) |
Deceased in 2024 (n=57) |
p-value |
|---|---|---|---|
| Age (years) | 63,5 (54.3-67.8) | 65 (59-71) | 0.111 |
| Males, n (%) | 29 (69.1) | 34 (59.6) | 0.401 |
| Nationality | |||
| Italian, n (%) | 39 (92.9) | 50 (87.7) | 0.518 |
| Other, n (%) | 3 (7.1) | 7 (12.3) | 0.518 |
| Manner of death | |||
| Natural cause, n (%) | 29 (69.1) | 37 (64.9) | 0.830 |
| Non-natural cause, n (%) | 13 (30.9) | 20 (35.1) | 0.830 |
| Mechanism of death | |||
| Cardiac cause, n (%) | 15 (51.7) | 19 (51.4) | >0.999 |
| Cerebral cause, n (%) | 6 (20.7) | 7 (18.9) | >0.999 |
| Others, n (%) | 8 (27.6) | 11 (29.7) | >0.999 |
| Place of death | |||
| Home, n (%) | 29 (69) | 38 (66.7) | 0.831 |
| Hospital, n (%) | 2 (4.8) | 5 (8.8) | 0.695 |
| Others, n (%) | 11 (26.2) | 14 (24.5) | >0.999 |
| Season of death | |||
| Spring, n (%) | 9 (21.4) | 14 (24.6) | 0.812 |
| Summer, n (%) | 10 (23.8) | 15 (26.3) | 0.819 |
| Autumn, n (%) | 12 (28.6) | 13 (22.8) | 0.641 |
| Winter, n (%) | 11 (26.2) | 15 (26.3) | >0.999 |
Continuous variables are presented as mean (SD), while categorical variables are presented as number (n) and the relative percentage (%).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



