Submitted:
09 February 2026
Posted:
10 February 2026
You are already at the latest version
Abstract
Objectives: This narrative review aimed to synthesize available evidence on procedures used for bedside ultrasonography-guided verification of nasogastric tube (NGT) placement. Methods: A comprehensive search was conducted in five databases, supplemented by gray literature and clinical guidelines, without restrictions on language or publication year. Eligible studies focused on ultrasound-guided NGT insertion or verification in adults. Data were extracted and synthesized descriptively using the I-AIM framework (Indication, Acquisition, Interpretation, and decision-Making). Results: 29 studies were included, most of them observational and conducted in intensive care or emergency settings. Ultrasound was primarily indicated for enteral nutrition, with gastric decompression less frequently reported. Acquisition protocols varied, though supine positioning, convex abdominal probes, and linear cervical probes were most common. The gastric antrum and esophagus were the main landmarks, with interpretation based on direct tube visualization and dynamic fogging; color Doppler was occasionally employed. Radiography remained the reference standard in over 90% of studies, though a few initiated feeding based on ultrasound alone. Facilitators included bedside feasibility, absence of radiation, and timeliness, whereas barriers encompassed operator dependency, limited visualization in patients with obesity or gas interposition, and heterogeneity of protocols. Conclusions: Ultrasonography is a promising, safe, and innovative method for NGT verification that can reduce delays, avoid radiation exposure, and improve patient safety. With structured training, nurses can achieve accuracy comparable to physicians, supporting greater autonomy in clinical decision-making. Standardized protocols and integration into nursing education are essential to ensure reliable and widespread adoption.
Keywords:
evidence-based practice
; intubation
; gatrointestinal
; nursing
; ultrasonography
1. Introduction
Patient safety remains a global concern, with millions of adverse events each year leading to preventable harm and deaths [1]. Among these, the blind insertion of a nasogastric tube (NGT) is a common nursing procedure associated with potentially life-threatening complications, including aspiration and pneumothorax [2,3]. Misplacement rates vary from 0.3% to 8% [4], and in the United Kingdom, undetected malposition is classified as a “never event” because of its serious consequences [5].
Traditional bedside verification methods, such as auscultation, have long been used but are now recognized as unreliable. Guidelines caution against this practice [6], yet studies show that many nurses continue to rely on it, often unaware of its limitations [7]. Radiography remains the gold standard, providing accurate confirmation of tube position [8]. However, routine use is not without challenges: repeated exposure to ionizing radiation, delays in feeding or medication administration, and additional costs to health systems [9,10].
Ultrasonography has emerged as a promising alternative. It allows real-time visualization of the tube during or after insertion, avoids radiation, and can reduce delays in care [11,12]. For nurses, point-of-care ultrasonography offers the possibility of immediate bedside confirmation, supporting safer and more timely clinical decisions [13,14]. Its main limitation is the need for specific training and standardized protocols, but growing evidence supports its feasibility in clinical practice.
Ongoing education and competency in NGT insertion and verification are essential to prevent adverse events and to ensure evidence-based nursing care [15,16]. In this context, ultrasonography represents an important opportunity to enhance safety and autonomy in nursing practice.
Despite growing interest in point-of-care ultrasonography, there is currently no comprehensive review mapping the procedures employed to guide NGT insertion in clinical practice. By synthesizing available evidence, this study addresses a critical gap in the literature. Its findings can inform nursing education, support the development of standardized protocols, and guide the safe integration of ultrasonography into routine care. In doing so, it contributes to advancing nursing knowledge, strengthening patient safety, and enhancing the quality of enteral care delivery.
The aim of this review was to explore the procedures used for bedside ultrasonography-guided nasogastric tube insertion in adult patients.
2. Materials and Methods
This narrative review was guided by Jones’s review process [17], which involves several key steps: (1) defining the research question or topic to be explored; (2) consulting a biomedical librarian for assistance with database navigation; (3) identifying relevant databases; (4) conducting searches using keywords and synonyms, combined with Boolean operators; (5) narrowing the topic to establish a framework for the review; (6) setting criteria for study selection; (7) organizing publications into thematic categories; (8) noting the research methods employed (quantitative, qualitative, or mixed); (9) synthesizing findings by comparing results, identifying patterns, and analyzing consistencies or contradictions; and (10) drawing conclusions by summarizing current knowledge, highlighting inconsistencies and gaps, and suggesting directions for future research.
This narrative review was reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA) [18].
The research question guiding this review was: What procedures are used to insert and confirm a nasogastric tube with the guidance of bedside ultrasonography in adult patients?
The search was conducted across major health science databases, including CINAHL (via EBSCOhost), Embase (via Elsevier), LILACS (via BVS), PubMed via National Institutes of Medicine), and Scopus (via Elsevier). Additional sources consulted included gray literature (Google Scholar and ProQuest Dissertation & Thesis Global), and both national and international guidelines. No restrictions were applied regarding publication date or language.
Eligible sources included primary studies and clinical guidelines that focused on the procedures used for bedside ultrasonography-guided nasogastric tube insertion in adult patients (≥18 years). Exclusion criteria included: studies that did not address the research question; studies that investigated the use of PoCUS solely for gastric residual volume (GRV) assessment; studies involving children or animals; reviews, abstracts, letters, expert opinion; study protocols, trial registrations; studies involving nasoenteric tubes or long-term feeding tubes; studies published in languages that do not use the Latin-Roman alphabet—modern Latin alphabet.
The controlled vocabulary terms available in the Health Sciences Descriptors (DeCS) and Medical Subject Headings (MeSH) were implemented and keywords were used with the Boolean operators AND and OR. Therefore, the search strategy carried out in June 2024 and updated on August 2025 was: (Ultrasonography OR “Point of Care” OR “Point-of-Care” OR POCUS OR “Point-of-care ultrasonography” OR “Point of care ultrasonography” OR “Point-Of-Care Ultrasound” OR “Point Of Care Ultrasound” OR Ultrasso*) AND (“Intubation, Gastrointestinal” OR “Nasogastric Intubation” OR “Nasogastric Tube” OR “Nasogastric Feeding Tube” OR “Nasogastric Tube Placement” OR “Nasogastric Tube insertion”) AND (Adult) (Table S1).
For the purposes of this narrative review, PoCUS was defined as the use of portable ultrasound performed directly by a healthcare provider at the point of care, for real-time diagnostic or clinical monitoring purposes [19]. Nasogastric tube was defined as a short-term feeding device, intended for use up to 4–6 weeks, inserted through the nose and positioned in the stomach [20].
Following the search strategy, all retrieved articles were exported to EndNote® for duplicate removal. The remaining articles were then uploaded to the Rayyan® platform, where two reviewers independently applied the inclusion and exclusion criteria in two stages: initial screening by title and abstract, followed by full-text review. Discrepancies were resolved through consensus, with a third reviewer consulted when necessary.
A descriptive synthesis was undertaken, with results organized thematically using the I-AIM framework (Indication, Acquisition, Interpretation, and decision-Making) [21]. To enhance interpretation, narrative and tabular presentations were complemented with visual tools (infographics and schematic figures) that highlighted procedural variations, recurring patterns, and gaps in practice.
Generative artificial intelligence (ChatGPT, OpenAI, San Francisco, CA, USA) was used in this study to support English language revision for clarity and proficiency and to assist in the conceptual organization and graphical design of Figure 6. The AI tool was not used to generate original data, perform data analysis, interpret results, or draw scientific conclusions. All content was critically reviewed, edited, and validated by the authors, who take full responsibility for the integrity and accuracy of the manuscript.
3. Results
The database search identified 3,815 records, with two additional sources retrieved through other means. After removing duplicates and applying eligibility criteria, 29 studies were included (Figure 1).
Studies were geographically diverse, most conducted in China [22,23,24,25], Brazil [12,26,27], and France [28,29,30,31], with one binational investigation from Italy and Switzerland [32] (Figure 2).
Sample sizes ranged from single-case reports to multicenter cohorts involving over 500 patients, reflecting the heterogeneity of the available evidence (Table 1).
Legend: BUS: Bedside Ultrasound; EC: Enteral Catheter; ED: Emergency Department; ICU: Intensive Care Unit; LMAs: Laryngeal Mask Airways; NGT: Nasogastric Tube; US: Ultrasound.
3.1. Clinical Settings
Most investigations were conducted in intensive care units (ICUs), followed by emergency departments and, less frequently, other clinical environments such as isolation wards or prehospital contexts (Figure 3).
This distribution reflects the procedure’s relevance in critically ill or unstable patients, but also highlights the need for validation in general wards where nurses perform the majority of NGT insertions.
3.2. Indication (I)
Across studies, ultrasound was primarily employed for confirmation of NGT placement in the context of enteral nutrition [12,23,24,25,31,32,34,36,37,38,39,40,41,44,45,46] and gastric decompression [23,24,28,29,30,32,33,38,39,40,42,43,45,46,47,48]. Drug administration [4,32,40,42,43,46], lavage [32,42,43], and diagnostic monitoring [32,38,43] were less frequently cited. This suggests that nutritional safety is the dominant clinical driver for using ultrasound in this domain.
3.3. Acquisition (A)
Protocols varied considerably across studies, underscoring a lack of standardization. Most examinations were performed in the supine position [4,12,22,23,24,25,26,27,29,30,31,32,33,34,35,36,37,38,39,40,43,45,46,47,48], employing convex probes [23,24,26,27,28,29,31,32,33,34,35,36,37,38,39,42,43,44,45,46,47] for abdominal windows and linear probes for cervical windows [4,22,23,36,38,40,43,46,47,49] (Figure 3). The epigastric/subxiphoid region and cervical esophagus were the most frequent acoustic windows [22,24,25,28,33,36,38,42,43,46,47,48] (Figure 4A and 4B), with the gastric antrum often described as the key sonoanatomical landmark (Figure 4B).
Details regarding windows and imaging planes were inconsistently reported. These variations are summarized in Figure 4, which consolidates technical specifications reported across studies.
3.4. Interpretation (I)
Correct NGT placement was most commonly interpreted through direct visualization of the tube as a hyperechoic structure within the stomach [12,23,24,25,32,33,36,39,42,43,44,45] (Figure 3B). Indirect techniques, such as dynamic “fogging” after air injection [22,23,28,33,36,37,39,46,47], were widely reported, while saline injection and color Doppler were less common [23,34,45]. Comparator tests included chest radiography, gastric aspirate pH, and auscultation, with radiography remaining the reference standard in over 90% of studies.
3.5. Decision-Making
Despite its feasibility as an immediate bedside tool, ultrasound rarely replaced radiography in clinical decision-making. In most reports, feeding or medication administration was withheld until radiographic confirmation. Exceptions included selected studies where ultrasound was used as the sole confirmation method when other techniques were impractical, such as in COVID-19 isolation wards [24]. Overall, ultrasound contributed to timelier assessments but did not supplant radiography as the gold standard for clinical decisions.
Figure 5 summarizes key recommendations, emphasizing standardized protocols, structured nurse training, and the need for multicenter trials to strengthen the evidence base
4. Discussion
This narrative review synthesizes evidence on ultrasonography-guided NGT placement using the I-AIM framework [21], highlighting both opportunities and challenges for nursing practice. The findings confirm that ultrasonography is a safe, non-invasive, and rapid bedside method [23], but its use remains inconsistent [50], with radiography still the gold standard [12,38].
For nurses, who are often responsible for NGT insertion, the ability to perform ultrasound verification has transformative potential. Studies show that, after structured training, nurses achieve diagnostic accuracy comparable to physicians, even in intensive care and emergency settings [22,27,37]. This supports international calls to expand nursing autonomy in PoCUS [51,52] and integrate it into clinical education [53,54]. By reducing reliance on chest X-rays, ultrasound can shorten delays in initiating feeding [55], avoid unnecessary transfers [12], and address the limitations of auscultation, a method still used despite guideline warnings of poor reliability [56].
The evidence base is dominated by observational, single-center studies with small samples (Figure 3). Although randomized trials and multicenter cohorts provide encouraging results, heterogeneity in protocols—ranging from probe choice to imaging windows and interpretation criteria—prevents definition of a standardized best practice and explains why radiography remains prioritized for clinical decisions. Feasibility also varies by patient group: visualization is often poorer in individuals with obesity, excessive gastric gas, or altered anatomy [57], and some protocols require two operators [32,49], limiting scalability.
Additional study-specific limitations further constrain applicability. Several investigations underreported key technical details including the type of probe used [12,25,30], probe frequency [12,24,25,30,42], and patient position [42,44]. Moreover, only three studies specified the depth used for ultrasound confirmation of nasogastric tube placement [26,31,45], reducing reproducibility. Populations with obesity [26,35], tracheostomies [26,33], or recent abdominal surgery [26,33]—common in clinical practice—were frequently excluded. Nurse-led research remains underrepresented [12,22,23,25,27,32,39,43,46,49], with most studies conducted by physicians, and outcomes were largely restricted to diagnostic accuracy [23,34,36,40,43,45,46] rather than patient safety, timeliness, or cost-effectiveness.
These gaps indicate clear priorities for future research. Large multicenter trials should validate accuracy and safety across diverse settings, while standardized protocols must be established for patient positioning, probe selection, and adjunctive techniques such as dynamic fogging or Doppler. Studies should evaluate nurse-performed ultrasonography more explicitly, testing training programs, competency frameworks, and simulation-based education. Inclusion of complex patient groups will improve generalizability, and research should extend to clinical and economic outcomes, such as reduced delays, decreased radiation exposure, adverse event prevention, and cost savings. Emerging technologies, including artificial intelligence–assisted interpretation and digital decision support, also warrant investigation.
The implications for nursing practice are substantial. By adopting ultrasonography, nurses can move away from unsafe methods and reduce dependence on radiography, promoting faster, safer, and more patient-centered care. Integrating this technique into nursing workflows enhances professional autonomy and positions nurses as key actors in advancing bedside diagnostics. To achieve this safely, standardized training, competency models, and evidence-based guidelines must be developed and rigorously evaluated.
5. Conclusions
This narrative review demonstrates that ultrasonography is a safe, rapid, and radiation-free method for verifying NGT placement, with clear potential to complement or, in selected contexts, replace radiography. Evidence synthesized through the I-AIM framework shows that ultrasound enables real-time confirmation at the bedside, reduces reliance on unreliable methods such as auscultation, and minimizes delays that compromise timely initiation of enteral nutrition. Although the current evidence base is dominated by small observational studies with methodological heterogeneity, findings consistently highlight the feasibility of nurse-performed ultrasonography, with diagnostic accuracy comparable to physicians when structured training is provided.
For nursing practice, these results underscore the opportunity to integrate ultrasonography into everyday workflows, strengthening professional autonomy and enhancing the safety of one of the most frequent and high-risk procedures in hospital care. To achieve this, standardized protocols, competency frameworks, and inclusion of ultrasound training in nursing curricula are essential.
Future research should focus on robust multicenter trials, standardization of acquisition and interpretation techniques, evaluation of nurse-led implementation, and assessment of clinical and economic outcomes beyond diagnostic accuracy. By addressing these gaps, ultrasonography can be fully established as a reliable, evidence-based tool that empowers nurses, improves patient safety, and advances the quality of enteral care delivery.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Search strategy.
Author Contributions
Conceptualization, M.F.S.A. and F.R.E.G.; methodology, M.F.S.A., V.B.S., P.R.S.R. and F.R.E.G.; software, M.F.S.A., M.G.M. and R.A.P.; validation, P.R.S.R. and F.R.E.G; formal analysis M.F.S.A., M.G.M. and R.A.P.; resources, M.F.S.A. and F.R.E.G.; data curation, M.F.S.A. and F.R.E.G.; writing—original draft preparation, M.F.S.A. and F.R.E.G.; writing—review and editing, M.F.S.A., V.B.S., M.G.M.; R.A.P.; P.R.S.R. and F.R.E.G.; visualization, M.F.S.A., V.B.S., M.G.M.; R.A.P.; P.R.S.R. and F.R.E.G.; supervision, F.R.E.G.; project administration, F.R.E.G.; funding acquisition, F.R.E.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Coordination for the Improvement of Higher Education Personnel – Brazil (CAPES) – Finance Code 001.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BVS | Biblioteca Virtual de Saúde |
| CINAHL | Cumulative Index to Nursing and Allied Health Literature |
| DeCS | Descritores em Saúde (Health Sciences Descriptors) |
| GRV | Gastric Residual Volume |
| I-AIM | Indication, Acquisition, Interpretation, and decision-Making |
| ICU | Intensive Care Unit |
| LILACS | Literatura Latino-Americana e do Caribe em Ciências da Saúde |
| MeSH | Medical Subject Headings |
| NGT | Nasogastric Tube |
| PoCUS | Point-of-Care Ultrasonography |
| PRISMA | Preferred Reporting Items for Systematic reviews and Meta-Analyses |
References
- World Health Organization. Global Patient Safety Action Plan 2021–2030: Towards Eliminating Avoidable Harm in Health Care; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- NHS England. Patient Safety Alert: Nasogastric Tube Misplacement—Continuing Risk of Death and Severe Harm; NHS England: London, UK, 2016. [Google Scholar]
- Zafran, M.; Crook, R.; Tuck, A.; Banerjee, A. Nasogastric tube placement perforating the nasopharynx causing mediastinal passage and feeding into the pleural space. BMJ Case Rep. 2024, 17, e254771. [Google Scholar] [CrossRef]
- Gok, F.; Kilicaslan, A.; Yosunkaya, A. Ultrasound-guided nasogastric feeding tube placement in critical care patients. Nutr. Clin. Pract. 2015, 30, 257–260. [Google Scholar] [CrossRef]
- NHS England. Never Events List 2018; NHS England: London, UK, 2021. [Google Scholar]
- Metheny, N.A.; Krieger, M.M.; Healey, F.; Meert, K.L. A review of guidelines to distinguish between gastric and pulmonary placement of nasogastric tubes. Heart Lung 2019, 48, 226–235. [Google Scholar] [CrossRef]
- Bourgault, A.M.; Heath, J.; Hooper, V.; Sole, M.L.; Nesmith, E.G. Methods used by critical care nurses to verify feeding tube placement in clinical practice. Crit. Care Nurse 2015, 35, e1–e7. [Google Scholar] [CrossRef]
- Fan, X.-N.; et al. Application of nurse-led enteral nutritional feeding strategies in neurological intensive care unit patients. Chin. J. Gen. Pract. 2022, 20, 2151–2155. [Google Scholar] [CrossRef]
- Taylor, S.; Manara, A.R. X-ray checks of NG tube position: A case for guided tube placement. Br. J. Radiol. 2021, 94, 20210432. [Google Scholar] [CrossRef]
- Boeykens, K.; Holvoet, T.; Duysburgh, I. Nasogastric tube insertion length measurement and tip verification in adults: A narrative review. Crit. Care 2023, 27, 317. [Google Scholar] [CrossRef]
- Powers, J.; et al. Development of a competency model for placement and verification of nasogastric and nasoenteric feeding tubes for adult hospitalized patients. Nutr. Clin. Pract. 2021, 36, 517–533. [Google Scholar] [CrossRef] [PubMed]
- Rigobello, M.C.G.; et al. Accuracy and costs of bedside methods for confirming nasoenteral feeding tube position: A diagnostic accuracy study. J. Ultrasound 2024. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Li, Q.; Wu, X.; Wang, X.; Liu, D. Nurse-performed ultrasound: A new weapon against COVID-19. Crit. Care 2020, 24, 430. [Google Scholar] [CrossRef]
- Wang, L.; et al. Association of gastric antrum echodensity and acute gastrointestinal injury in critically ill patients. Nutrients 2022, 14, 566. [Google Scholar] [CrossRef] [PubMed]
- Bloom, L.; Seckel, M.A. Placement of nasogastric feeding tube and postinsertion care review. AACN Adv. Crit. Care 2022, 33, 68–84. [Google Scholar] [CrossRef] [PubMed]
- Melender, H.-L.; Maijala, V. Tactics for teaching evidence-based practice: Video as a support for learning international database searching in nursing education. Worldviews Evid. Based Nurs. 2018, 15, 326–328. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.P. How to conduct a review of the literature. J. Dermatol. Physician Assist. 2023, 17. Available online: https://journals.lww.com/jdpa/fulltext/2023/17020/how_to_conduct_a_review_of_the_literature.9.aspx (accessed on 30 Jan 2026). [CrossRef]
- Page, M.J.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Blaivas, M. A new point of care ultrasound journal. Crit. Ultrasound J. 2009, 1, 1–2. [Google Scholar] [CrossRef]
- Boullata, J.I.; et al. ASPEN safe practices for enteral nutrition therapy. JPEN J. Parenter. Enteral Nutr. 2017, 41, 15–103. [Google Scholar] [CrossRef]
- Bahner, D.P.; Hughes, D.; Royall, N.A. I-AIM: A novel model for teaching and performing point-of-care ultrasound. J. Ultrasound Med. 2012, 31, 295–300. [Google Scholar] [CrossRef]
- Mak, M.Y.; Tam, G. Ultrasonography for nasogastric tube placement verification: An additional reference. Br. J. Community Nurs. 2020, 25, 328–334. [Google Scholar] [CrossRef]
- Tai, P.; et al. Nurse-performed ultrasonography in confirming the position of nasogastric tube in the emergency department. Hong Kong J. Emerg. Med. 2016, 23, 340–349. [Google Scholar] [CrossRef]
- Wenhong, G.M.; Shunji, G.M.; Qun-An, H.M.; Huijuan, X.M. Bedside ultrasonography-guided nasogastric tube placement in COVID-19 patients. Adv. Ultrasound Diagn. Ther. 2020, 4, 131. [Google Scholar] [CrossRef]
- Zhu, X.-J.; Liu, S.-X.; Li, Q.-T.; Jiang, Y.-J. Bedside ultrasonic localization of the nasogastric tube in a patient with severe COVID-19: A case report. World J. Clin. Cases 2022, 10, 4911–4916. [Google Scholar] [CrossRef]
- De Souza, R.; et al. Ultrasound as a method for confirming the positioning of enteral catheters in critically ill patients. Med. Ultrason. 2024, 26, 242. [Google Scholar] [CrossRef]
- Ferraboli, S.F.; Beghetto, M.G. Bedside ultrasonography for the confirmation of nasogastric tube placement: Agreement between nurse and physician. Rev. Gaucha Enferm. 2022, 43, e20220211. [Google Scholar] [CrossRef]
- Brun, P.-M.; et al. Two-point ultrasonography to confirm correct position of the gastric tube in prehospital setting. Mil. Med. 2014, 179, 959–963. [Google Scholar] [CrossRef]
- Chenaitia, H.; et al. Ultrasound to confirm gastric tube placement in prehospital management. Resuscitation 2012, 83, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Piton, G.; Parel, R.; Delabrousse, E.; Capellier, G. Echography for nasogastric tube placement verification. Eur. J. Clin. Nutr. 2017, 71, 669–670. [Google Scholar] [CrossRef]
- Vigneau, C.; Baudel, J.-L.; Guidet, B.; Offenstadt, G.; Maury, E. Sonography as an alternative to radiography for nasogastric feeding tube location. Intensive Care Med. 2005, 31, 1570–1572. [Google Scholar] [CrossRef] [PubMed]
- Mumoli, N.; et al. Bedside abdominal ultrasound in evaluating nasogastric tube placement. Chest 2021, 159, 2366–2372. [Google Scholar] [CrossRef] [PubMed]
- Chiesa, A.F.; et al. Accuracy of ultrasonography in confirming correct positioning of nasogastric tube in the intensive care setting. Chest Crit. Care 2025, 3, 100181. [Google Scholar] [CrossRef]
- Ong, M.Y.; et al. Accuracy of colour Doppler ultrasound for nasogastric tube placement in the emergency department. Emerg. Med. Australas. 2025, 37. [Google Scholar] [CrossRef] [PubMed]
- Hell, J.; Schelker, G.; Schumann, S.; Schmutz, A. Gastric insufflation with and without an inserted gastric tube in second-generation laryngeal mask airways. J. Clin. Anesth. 2024, 99, 111653. [Google Scholar] [CrossRef]
- Ragunathan, T.; et al. Performance of point-of-care ultrasonography in confirming feeding tube placement in mechanically ventilated patients. Diagnostics 2023, 13, 2679. [Google Scholar] [CrossRef]
- Güllüpınar, B.; et al. Nasogastric tube placement verification with ultrasound by emergency nurses. Ann. Clin. Anal. Med. 2022, 13. [Google Scholar] [CrossRef]
- McMullen, C.D.; Anstey, C.; Garrett, P.; Moore, J. Nasogastric tube placement under sonographic observation. Aust. Crit. Care 2022, 35, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Tsolaki, V.; et al. Ultrasonographic confirmation of nasogastric tube placement in the COVID-19 era. J. Pers. Med. 2022, 12, 337. [Google Scholar] [CrossRef] [PubMed]
- Yaseen, M.; et al. Point-of-care ultrasonography-assisted nasogastric tube placement in the emergency department. Eur. J. Emerg. Med. 2022, 29, 431–436. [Google Scholar] [CrossRef]
- Brotfain, E.; et al. Ultrasound assessment of gastric content and nasogastric tube placement in general ICU patients. Crit. Care 2019, 23, 235. [Google Scholar] [CrossRef]
- Ebert, E. Ultrasound for the confirmation of nasogastric tube placement in the emergency department. Brown Emergency Medicine Blog. Available online: https://brownemblog.com (accessed on 25 May 2025).
- Yıldırım, Ç.; et al. Verifying the placement of nasogastric tubes at an emergency center. Emerg. Med. Int. 2018, 2018, 2370426. [Google Scholar] [CrossRef]
- Nedel, W.L.; Jost, M.N.F.; Filho, J.W.F. A simple and fast ultrasonographic method of detecting enteral feeding tube placement. J. Intensive Care 2017, 5, 55. [Google Scholar] [CrossRef]
- Wong, K.W.; et al. Using color flow detection of air insufflation to improve accuracy in verifying nasogastric tube position. Am. J. Emerg. Med. 2017, 35, 333–336. [Google Scholar] [CrossRef]
- Zatelli, M.; Vezzali, N. Four-point ultrasonography to confirm correct position of nasogastric tube. J. Ultrasound 2017, 20, 53–58. [Google Scholar] [CrossRef]
- Kim, H.M.; et al. Effectiveness of ultrasonography in verifying nasogastric tube placement. Scand. J. Trauma Resusc. Emerg. Med. 2012, 20, 38. [Google Scholar] [CrossRef]
- Nguyen, L.; Lewiss, R.E.; Drew, J.; Saul, T. A novel approach to confirming nasogastric tube placement in the ED. Am. J. Emerg. Med. 2012, 30, 1662.e5–1662.e7. [Google Scholar] [CrossRef] [PubMed]
- Brotfain, E.; et al. Nurse-performed ultrasound assessment of gastric residual volume and nasogastric tube placement. Intensive Crit. Care Nurs. 2022, 69, 103183. [Google Scholar] [CrossRef]
- Metheny, N.A. Insufficient evidence to support ultrasonography as a method to rule out improperly positioned nasogastric tubes. Evid. Based Nurs. 2018, 21, 79. [Google Scholar] [CrossRef] [PubMed]
- Boling, B. Expanding the horizon: The case for point-of-care ultrasound in nurse practitioner practice. J. Am. Assoc. Nurse Pract. 2025, 37, 430–432. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; et al. Experiences of critical care nurses implementing point-of-care ultrasound. Nurs. Crit. Care 2025, 30, e70104. [Google Scholar] [CrossRef]
- Alfoti, B.O.O.; et al. Utilization of point-of-care ultrasound in emergency and critical care. Egypt. J. Chem. 2024, 67, 705–716. [Google Scholar] [CrossRef]
- Ventura, S.; et al. Implementation of point-of-care ultrasound training into nurse practitioner education. J. Nurse Pract. 2023, 19. [Google Scholar] [CrossRef]
- Pérez-Calatayud, Á.A.; Carillo-Esper, R. Role of gastric ultrasound to guide enteral nutrition in the critically ill. Curr. Opin. Crit. Care 2023, 29, 123–129. [Google Scholar] [CrossRef] [PubMed]
- askiran, N.; Sari, D. Effectiveness of auscultatory, capnometry, and pH methods to confirm nasogastric tube placement. Int. J. Nurs. Pract. 2022, 28, e13049. [Google Scholar] [CrossRef] [PubMed]
- Tsujimoto, H.; et al. Ultrasonography for confirmation of gastric tube placement. Cochrane Database Syst. Rev. 2017, 4, CD012083. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA flow diagram.
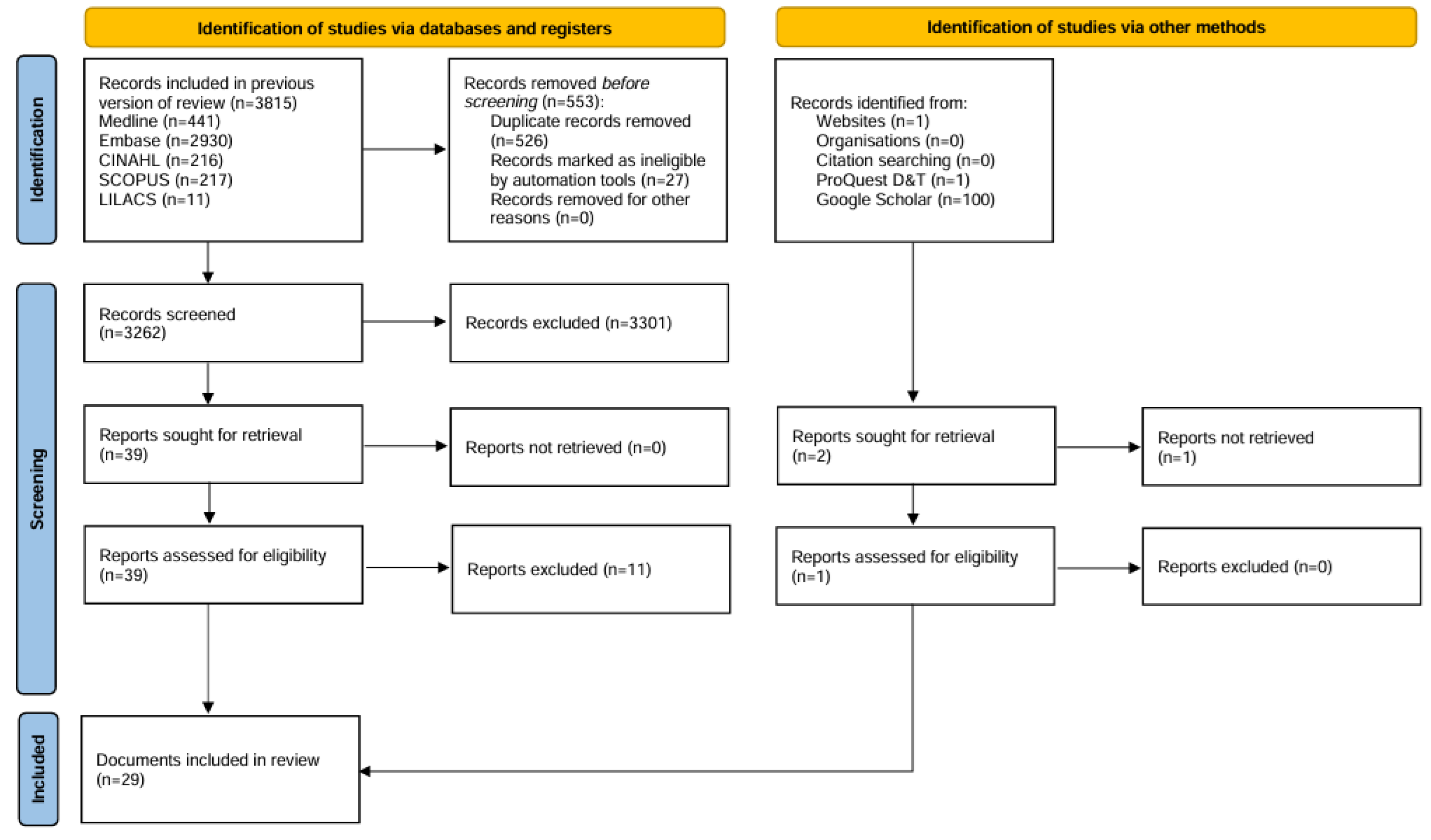
Figure 2.
World map of study locations included in the review. Note: 29 studies were included in this review; however, the world map displays 30 entries because one article reported data from both Italy and Switzerland.
Figure 2.
World map of study locations included in the review. Note: 29 studies were included in this review; however, the world map displays 30 entries because one article reported data from both Italy and Switzerland.
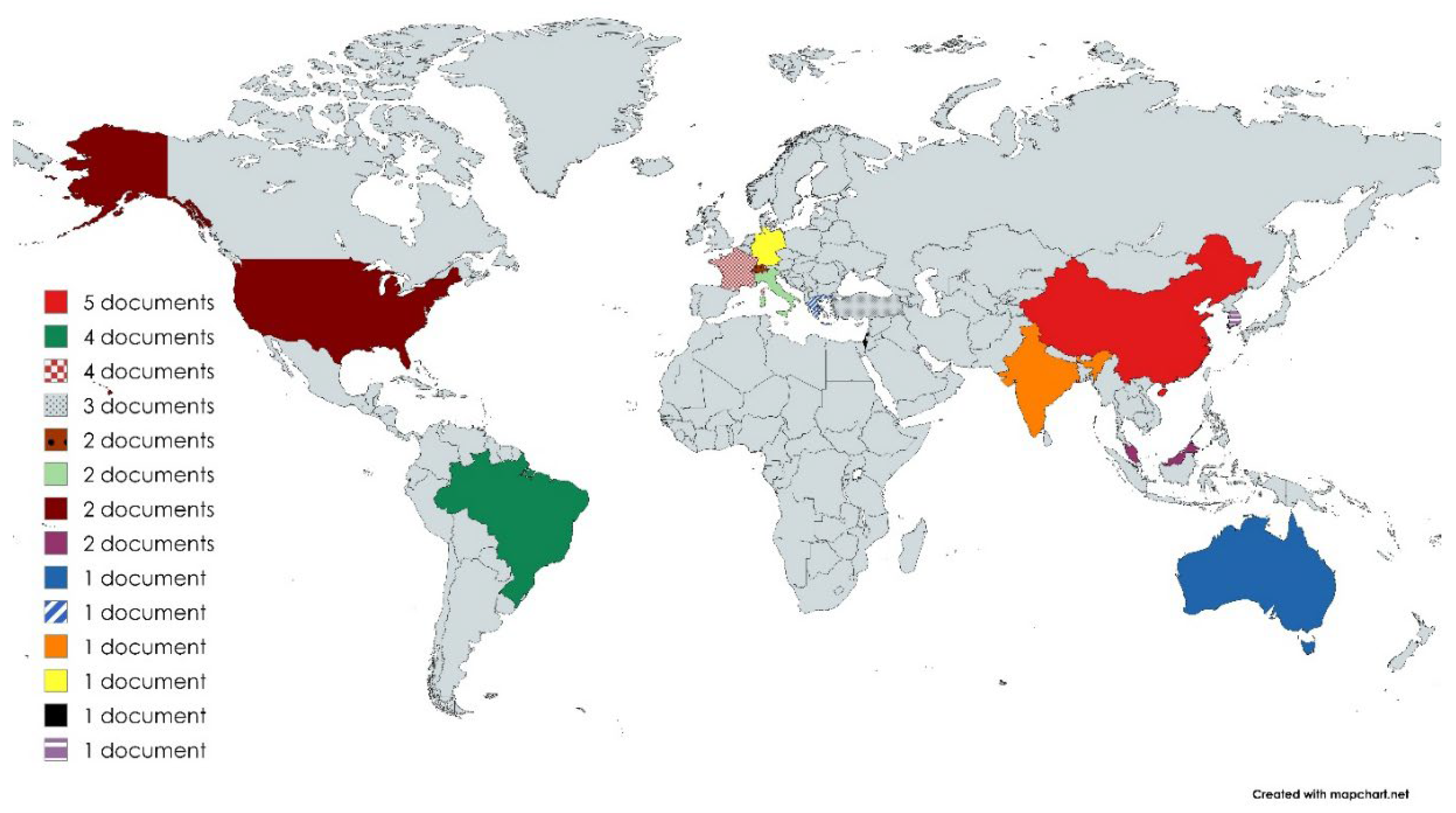
Figure 3.
Representative sonoanatomy for NGT placement verification. (a) Transverse ultrasound view of the esophagus (E) adjacent to the trachea (T) and tracheal rings (TR). (b) Longitudinal abdominal ultrasound demonstrating the gastric antrum (A) in relation to the liver (L). (c) Transversal cervical ultrasound showing the nasogastric tube (NGT) in proximity to the endotracheal tube (ETT). (d) Longitudinal abdominal ultrasound demonstrating the gastric antrum (A) adjacent to the liver (L), with an arrow indicating the nasogastric tube within the antrum.
Figure 3.
Representative sonoanatomy for NGT placement verification. (a) Transverse ultrasound view of the esophagus (E) adjacent to the trachea (T) and tracheal rings (TR). (b) Longitudinal abdominal ultrasound demonstrating the gastric antrum (A) in relation to the liver (L). (c) Transversal cervical ultrasound showing the nasogastric tube (NGT) in proximity to the endotracheal tube (ETT). (d) Longitudinal abdominal ultrasound demonstrating the gastric antrum (A) adjacent to the liver (L), with an arrow indicating the nasogastric tube within the antrum.
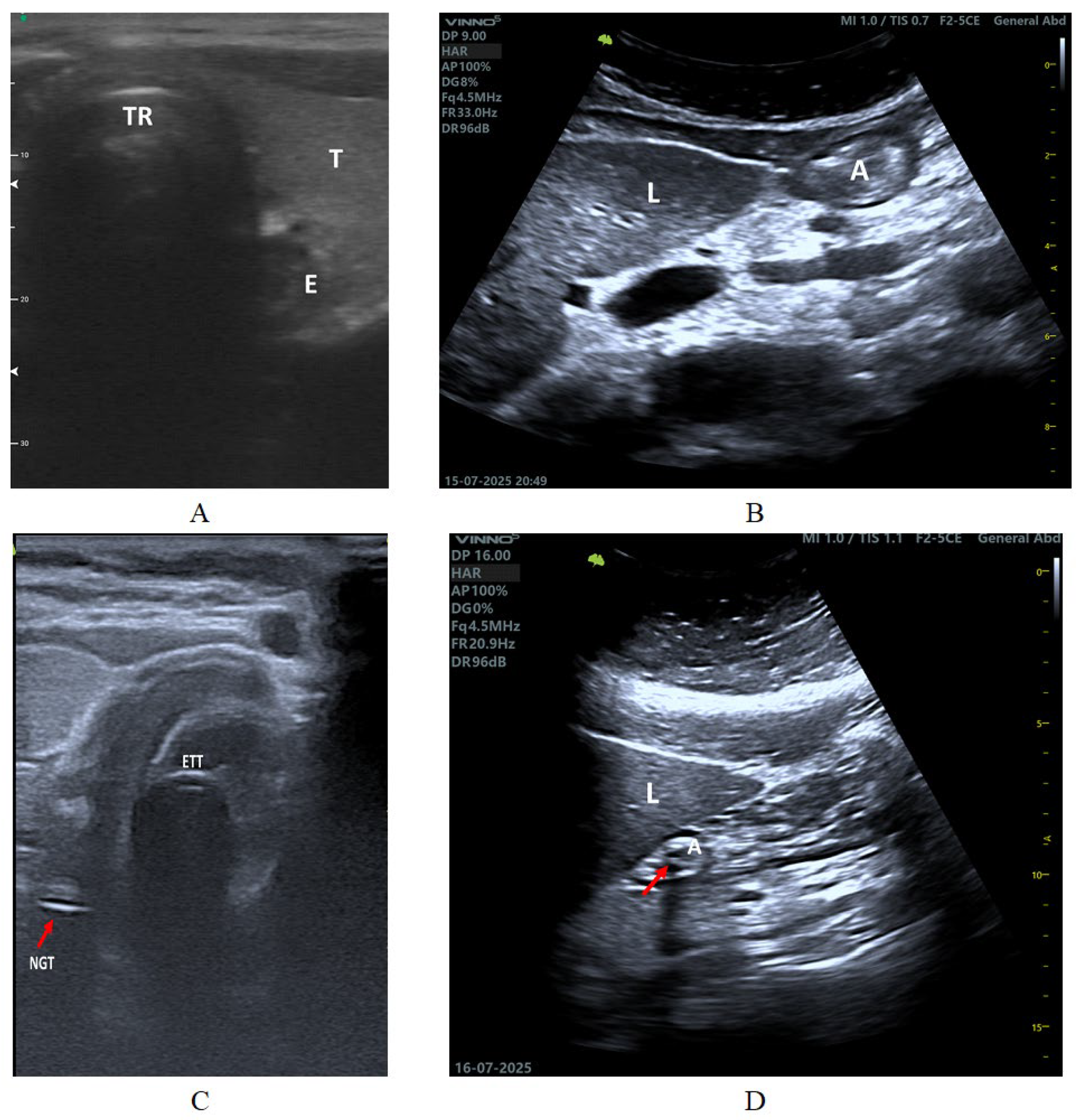
Figure 4.
Ultrasound Windows and Planes for NGT Verification.
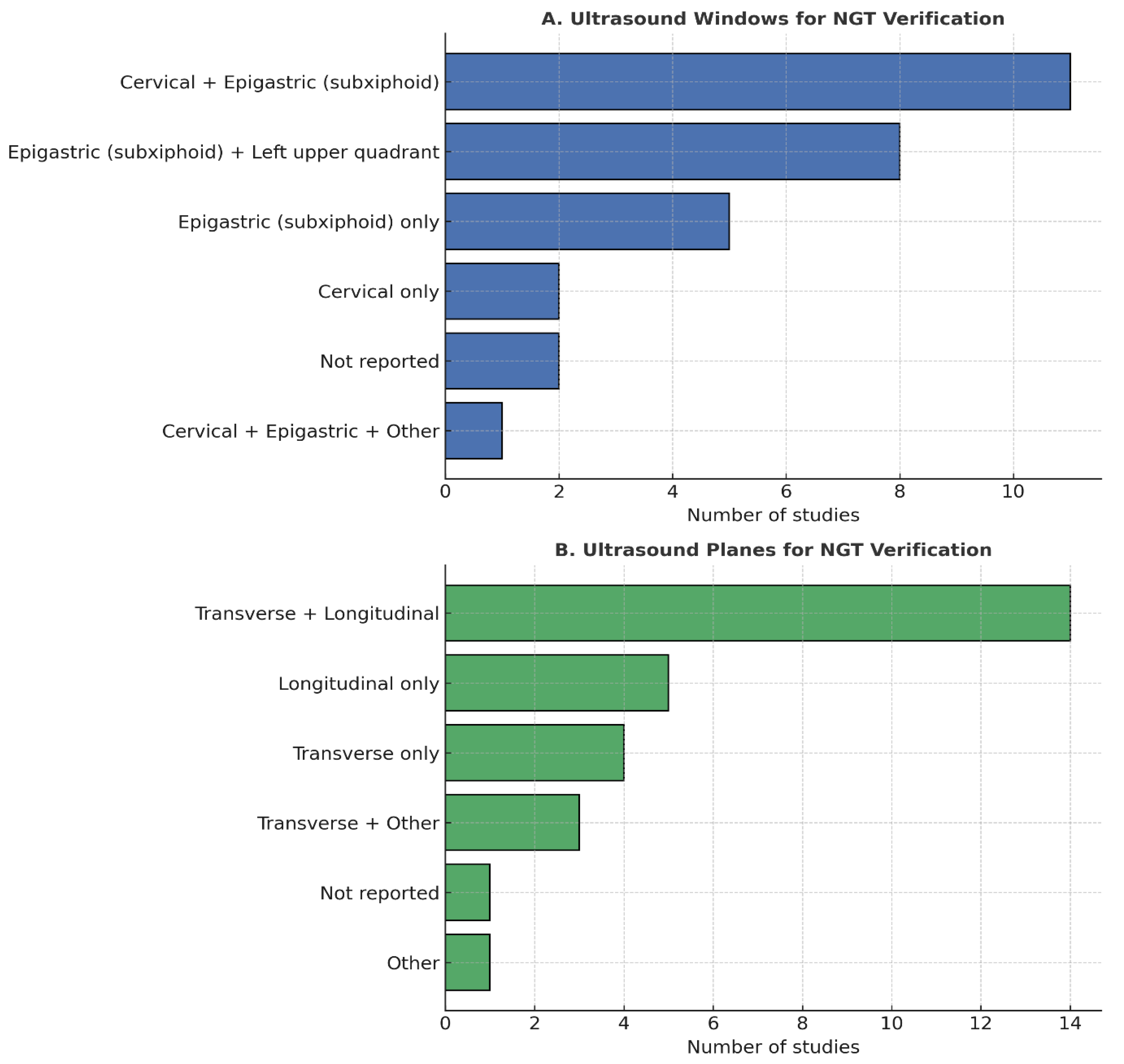
Figure 5.
Key recommendations from the literature on ultrasound-guided NGT verification.

Table 1.
Main characteristics of the studies included in the narrative review.
| Refs. | Study Aim | Design | Setting | Sample |
| [4] | To prospectively evaluate the effectiveness of ultrasound-guided nasogastric tube placement and procedure-related parameters in ICU patients | Observacional study | ICU | 56 patients |
| [12] | To evaluate the diagnostic accuracy and direct costs of three bedside methods—ultrasound, epigastric auscultation, and pH measurement—for confirming nasoenteral tube placement compared with radiography | Observacional study | Clinical wards | 76 patients, 87 tube insertions |
| [22] | To investigate the effectiveness of point-of-care ultrasonography for verifying NGT placement in community-dwelling adults, and to evaluate its feasibility as a first-line reference in comparison with the gastric aspirate pH test | Observacional study | Other | 68 patients |
| [23] | To evaluate the diagnostic accuracy of nurse-performed ultrasonography in confirming the position of nasogastric tubes in the emergency department, compared with conventional methods and radiography | Observacional study | Emergency | 72 patients |
| [24] | To describe the feasibility and effectiveness of bedside ultrasonography to guide nasogastric tube placement in COVID-19 patients in isolation wards | Case report | Other | 2 elderly patients |
| [25] | To describe the use of bedside ultrasound for confirming nasogastric tube placement in a patient with severe COVID-19, when conventional methods were inconclusive or infeasible | Case report | Other | 1 elderly patient |
| [26] | To evaluate the agreement between the BUS and the plain radiography to confirm the positioning of the EC in critically ill patients, as well as to analyze the potential impact of this exam on the time to start the enteral nutrition | Observacional study | ICU | 83 patients |
| [27] | To evaluate the concordance between nurse and physician in determining the location of the nasoenteral tube using bedside ultrasonography, and to describe the main difficulties encountered by the nurse when performing the technique | Observacional study | ICU | 30 patients |
| [28] | To estimate the diagnostic accuracy of 2-point ultrasonography (esophagus + stomach) for confirming gastric tube placement in the prehospital setting | Observacional study | Emergency | 32 patients |
| [29] | To estimate the diagnostic accuracy of ultrasound in confirming gastric tube placement in the prehospital setting | Observacional study | Other | 130 patients |
| [30] | To describe and illustrate the use of abdominal ultrasonography for confirming the correct position of a nasogastric tube in the stomach, using a new dynamic turbulence test | Case report | ICU | 1 patient |
| [31] | To evaluate the accuracy and feasibility of bedside sonography performed by ICU physicians to confirm the position of weighted-tip nasogastric feeding tubes, compared with radiography | Observacional study | ICU | 33 patients; 35 procedures |
| [32] | To assess the diagnostic accuracy of bedside abdominal ultrasound (BAU) in confirming correct nasogastric tube placement compared with chest radiography | Observacional study | Other | 526 inpatients |
| [33] | To provide precise estimates and assess the accuracy of dynamic fogging detection by abdominal US in patient with a positive US (visible NGT) in oesophageal position to confirm correct tube placement | Observacional study | ICU | 182 patients |
| [34] | To investigated the accuracy of collor doppler ultrasonography for NGT placement confirmation in the ED setting | Observacional study | Emergency | 144 patients |
| [35] | To evaluate the risk of gastric insufflation with gastric ultrasound during increasing peak airway pressures in two different second-generation LMAs with and without an inserted gastric tube | Randomized controlled trial | ICU | 152 patients |
| [36] | To evaluate the diagnostic accuracy of point-of-care ultrasonography in confirming feeding tube placement in mechanically ventilated ICU patients compared to chest radiography. | Observacional study | ICU | 80 patients |
| [37] | To evaluate the ability of emergency nurses, after structured training, to confirm correct nasogastric tube placement using ultrasound compared with chest radiography. | Observacional study | ICU | 84 patients |
| [38] | To evaluate the diagnostic accuracy of ultrasound performed by nonradiologists for verifying nasogastric tube placement in mechanically ventilated ICU patients, compared with chest radiography | Observacional study | ICU | 25 patients |
| [39] | To evaluate the feasibility and diagnostic accuracy of ultrasonography for confirming NGT placement in COVID-19 patients, especially after frequent posture changes between prone and supine | Observacional study | ICU | 276 patients |
| [40] | To compare the accuracy and safety of real-time point-of-care ultrasonography-guided nasogastric tube insertion with the conventional blind insertion technique in the emergency department | Randomized controlled trial | Emergency | 118 patients |
| [41] | To validate a new ultrasound method of assessing gastric residual volume and nasogastric tube positioning performed by trained ICU nurses, compared with the standard protocol | Observacional study | ICU | 90 patients; 360 assessments |
| [42] | Not applicable | Not applicable | Emergency | Not applicable |
| [43] | To compare the accuracy of neck and subxiphoid ultrasound with chest radiography for verifying nasogastric tube placement in emergency department patients | Observacional study | Emergency | 49 patients |
| [44] | To prospectively evaluate the effectiveness of ultrasound in confirming correct enteral feeding tube placement in mechanically ventilated ICU patients and compare time to diagnosis with abdominal X-ray | Observacional study | ICU | 41 patients; 41 tube insertions |
| [45] | To evaluate the diagnostic accuracy of color flow Doppler ultrasonography in verifying nasogastric tube position compared to conventional two-dimensional ultrasound and chest radiography | Observacional study | Emergency | 100 patients |
| [46] | To estimate the diagnostic accuracy of a novel 4-point ultrasonography protocol to confirm nasogastric tube placement in critically ill ICU patients | Observacional study | ICU | 114 patients |
| [47] | To compare the effectiveness of auscultation, pH measurement, and ultrasonography in verifying nasogastric tube placement among patients with low consciousness in the emergency center | Observacional study | Emergency | 47 patients |
| [48] | To describe a novel approach using bedside two-dimensional ultrasound to confirm nasogastric tube placement in the emergency department | Case report | Emergency | 1 male patient |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



