
Submitted:
09 February 2026
Posted:
09 February 2026
You are already at the latest version
Abstract
Background: Dying in the preferred place is considered an indicator of quality of end-of-life care. Advance care planning and home palliative care may increase the likelihood of dying at home. This study aimed to assess whether recording patients’ preferred place of care or death is associated with the actual place of death among patients followed by home palliative care teams. Methods: We conducted a retrospective observational study including adult patients who died in 2022 and were followed by a home palliative care team in Madrid, Spain. Sociodemographic and clinical variables, recorded preferred place of care or death, and actual place of death were extracted from electronic health records. Associations were analysed using bivariate tests and multivariable logistic regression. Results: A total of 464 patients were included (53% women; mean age 80.8 years). Overall, 82.5% died at home. A preferred place of care or death was recorded for 64% of patients; among them, 97.6% expressed a preference for home, and 89% of these patients died at home. In the multivariable analysis, older age and female sex were independently associated with death at home. Recording a preferred place of care or death was not independently associated with the place of death. Conclusions: Most patients followed by home palliative care teams died at home. Older age and female sex were associated with a higher probability of home death. Although most patients with a recorded preference for home died at home, recording preferences alone was not independently associated with the place of death. Systematic documentation of preferences may support advance care planning and patient-centred decision-making.
Keywords:
end-of-life care
; terminal care
; death
; home patient-centered care
; hospice
; hospital
; palliative care
; place of death
; preferences
; advanced care planning
1. Background
Most people express a preference to die at home when facing advanced or life-limiting illness [1,2,3]. However, in Spain and in other countries with similar socioeconomic characteristics, most deaths still occur in hospitals or institutional settings, while only about one third take place at home [4,5,6,7,8]. Dying in the preferred place is considered an indicator of quality of end-of-life care and a key component of a “good death” [2,3,9,10].
Previous studies have shown that the probability of dying at home is influenced by multiple clinical and social factors, including older age [5,7,8,14], the presence of a primary caregiver [11,13,15], functional decline [10,11,14], socioeconomic status [16,17], rural residence [7,15], marital status [5,7] and sex, although findings regarding sex remain inconsistent [6,7,14,18].
Home palliative care (HPC) services play a central role in enabling patients to remain at home at the end of life. Their involvement has been associated with fewer emergency department visits and a lower probability of hospital death [4,11,17,19,20]. Similarly, primary care follow-up and the availability of social and healthcare resources increase the likelihood of dying at home [14,15,21,22].
In this context, advance care planning (ACP) is particularly relevant. ACP is defined as a process that supports patients in understanding and sharing their values, goals and preferences regarding future medical care [25]. ACP has been associated with reduced hospital deaths and increased home deaths [20,26]. One of its most accessible components in routine practice is the documentation of the patient’s preferred place of death.
Although several studies have examined factors associated with place of death, few have specifically evaluated whether recording the preferred place of death in the clinical record is associated with the actual place of death among patients receiving home palliative care [27]. This represents an important gap, as documenting preferences may reflect the existence of ACP discussions and may facilitate shared decision-making and coordinated care [28].
The primary objective of this study was to analyse whether the explicit recording of the preferred place of care or death in patients followed by a home palliative care team was associated with a greater probability of dying in the preferred place. Secondary objectives were to explore other sociodemographic and clinical factors associated with the place of death.
2. Methods
2.1. Study Design and Setting
We conducted a retrospective observational cohort study including patients followed by a home palliative care (HPC) team in Madrid, Spain. The HPC team ESAPD Centro provides home-based palliative care to an urban population of approximately 671,000 inhabitants with diverse socioeconomic characteristics [29].
Home palliative care in Madrid is delivered by multidisciplinary teams integrated into the public primary care system, which provides universal coverage and free access at the point of care. These teams work in coordination with primary care services and specialised palliative care units.
2.2. Study Population
The study population comprised all adult patients (≥18 years) who were followed by the HPC team and died in 2022. Inclusion criteria were active follow-up by the team and at least one face-to-face home visit.
Patients were excluded if the place of death was not recorded, if death occurred under special circumstances (e.g. euthanasia), or if discrepancies in death-related data could not be resolved.
2.3. Sample Size and Sampling
No sample size calculation was performed because all patients who met the selection criteria (n = 464) were included. The flowchart of participant eligibility is shown in Figure 1.
2.4. Data Source and Variables
Data were extracted from the electronic medical record system (“AP Madrid”), which includes a specific palliative care protocol completed by healthcare professionals during patient assessment and follow-up. Sociodemographic variables (sex, age, presence of a primary caregiver), clinical variables (type of advanced disease: oncological or non-oncological), and information related to death (patients’ and their families’ preferred place of death and care (home/health centre), changes in these preferences, and actual place of death (home/health centre)) were extracted.
The main exposure variable was the recorded preferred place of care or death. The primary outcome was the actual place of death. Although preferred place of care and preferred place of death are conceptually distinct, they were analysed together due to the structure of routine clinical records, which frequently combine both concepts.lik
2.5. Statistical Analysis
Continuous variables are expressed as medians and interquartile ranges (IQRs, 25–75%) or means and standard deviations SDs. Categorical data are expressed as absolute and relative frequencies. A descriptive analysis of the sociodemographic and clinical characteristics and place of death of the study population was performed, with relative and absolute frequencies and measures of central tendency and dispersion reported according to the characteristics of the variables. Bivariate analyses were performed to assess associations between the place of death and sociodemographic, clinical and preference-related variables, using the chi-square test for categorical variables and Student’s t test for continuous variables.
Variables that showed a statistically significant association in bivariate analyses or were considered clinically relevant were entered into a multivariable logistic regression model to identify factors independently associated with death at home. Results are reported as odds ratios (ORs) with 95% confidence intervals (95% CI).
Statistical significance was defined as p < 0.05. All analyses were performed using IBM SPSS Statistics version 26.0.
3. Results
3.1. Patient Characteristics
A total of 464 people were included; 53% were women, the mean age was 80.8 years (SD ± 13.0 The median duration of follow-up by the HPC team was 20 days (IQR 7–57), and 24.1% of patients had a recorded primary caregiver.
Regarding diagnosis, 61% of patients had oncological disease, most frequently digestive system cancers. Among non-oncological conditions, heart failure was the most common diagnosis (Appendix A).
Overall, 82.5% of patients died at home, 14.1% in hospital and 3.4% in a mid-stay palliative care unit.
A preferred place of death was recorded for 24.6% of patients, whereas a preferred place of care or death was recorded for 64.0%. Among patients with a recorded preference, 97.6% expressed a preference for home and 2.4% for a non-home setting. Of those who preferred home, 89,0% died at home.
Baseline characteristics and preferred and actual places of death are shown in Table 1.
3.2. Factors Associated with the Place of Death
Patients who died at home were older than those who died in institutional settings (mean difference: 3,8 years; p < 0,05). Women died at home more frequently than men (86,2% vs 78,4%, p < 0,05) (Table 2.)
Home death occurred in 87,2% of non-oncological patients and in 79,6% of oncological patients (p < 0,05). No significant differences were observed according to the presence of a primary caregiver.
The association between having a recorded preference for home and the actual place of death was not statistically significant (p = 0.87).
3.3. Factors Associated with Recording Preferences
Women were more likely than men to have a recorded preferred place of death (26.4% vs 22.5%). Additionally, a greater percentage of women (58.72%) who desired to die at home did so, but the difference with the corresponding percentage of men was not statistically significant (p = 0.087). Among patients who expressed a preference for home, women achieved this preference more frequently than men (53.1% vs 46.9%, p = 0.042).
A higher proportion of oncological patients had a recorded preference compared with non-oncological patients (58.8% vs 41.2%). There were no relevant differences in the preferred place of death according to the specific type of pathology.
3.4. Multivaribale Analysis
In the multivariable logistic regression model, older age (OR 1,02; 95% CI 1,00–1,04; p = 0,026) and female sex (OR 0,60; 95% CI 0,37–0,98; p = 0,042) were independently associated with death at home (Table 3).
Recording a preferred place of care or death was not independently associated with the place of death after adjustment.
4. Discussion
This study examined factors associated with place of death among patients followed by a HPC team in an urban area of Madrid. Most patients died at home, and older age and female sex were independently associated with home death. Although most patients with a recorded preference for home ultimately died at home, recording preferences was not independently associated with the place of death after adjustment.
The high proportion of home deaths observed in our study exceeds that reported in most population-based studies [4,5,6,7,8]. This likely reflects the characteristics of patients referred to HPC teams, for whom a decision regarding end-of-life care location has often already been made prior to referral. In addition, access to specialised HPC and coordinated primary care may facilitate symptom control and prevent unnecessary hospital admissions.
Older age was associated with a greater probability of dying at home, consistent with previous studies [5,7,8,14]. This may be explained by greater acceptance by patients, families and healthcare providers of the appropriateness of focusing on comfort-oriented care rather than hospital transfer. Disease trajectories may also be more predictable in older patients, facilitating earlier palliative care involvement. Previous studies have shown that elderly patients with advanced illnesses prefer to die at home since they are closer to their loved ones, which alleviates the burden of symptomatology without increasing the burden on the caregiver, particularly when they are accompanied by services such as those provided by HPC teams and primary care doctors [30].
In our cohort, women were more likely to die at home than men. Findings regarding sex differences in place of death are inconsistent in the literature [6,7,14,18], although some studies have shown that, similar to our findings, more women die at home than men do [20]. Possible explanations include greater involvement of women in ACP discussions and avoiding hospitalization. Moreover, notably, women generally die at an older age, which may influence care decisions [8,20]. However, for a patient to die at home, the presence of an effective caregiver is necessary; owing to cultural influences, it is more likely that this role is played by a woman (wife, daughter, or sister), and thus men are more likely to have caregivers. However, information on caregiver characteristics was not available in our study and should be addressed in future research, since the sex of the caregiver could play an important role in the place of death [31]. To this end, we also note that our study was conducted primarily in an urban environment in one of the largest cities in Europe, and it could be interesting to conduct further studies addressing this variable [32].
We did not observe a significant association between the presence of a recorded caregiver and the place of death, contrary to previous studies [11,13,15]. This may be due to under-recording or misclassification of this variable in routine clinical practice. However, this result may reflect a recording bias for this variable; in previously mentioned studies [31,32], having a primary caregiver positively influenced dying in the patient’s desired location.
Although ACP has been associated with increased home death [20,26], our results suggest that recording preferences alone is insufficient to determine the place of death. Documentation may be a marker of ongoing discussions rather than a causal factor. Achieving the preferred place of death likely requires adequate resources, caregiver support and coordinated care. Likewise, it is important to expand the knowledge on how cultural differences can influence both the place of death and the preferences of each person, as well as the predisposition to start ACP [3].
This study has several limitations. First, this study is limited by its retrospective design and the use of routinely collected data, which may lead to information bias and under-recording. Consequently, depending on the professional, certain information may be underreported. On the other hand, patients who prefer to die at home may state as such more clearly; therefore, there is an increased probability that it will be included in the clinical history, thus allowing their desires to be fulfilled more easily. Thus, variability in the quality of the records—in terms of whether the patient has expressed his or her preference to the team or to his or her family or whether there has been a change in that preference and the professional has not recorded it—can be expected. In summary, the quality of the information available to us may be limited, resulting in information bias.
Second, caregiver-related variables and socioeconomic factors were not included, which may have influenced the place of death. Also, the study was conducted in a single urban area, which may limit generalisability. Although our study focused on a highly urbanized area and was not multicentric, it presents a wide range of deprivation indices as measured through the MEDEA index [29], as it included areas with very different levels of education, country of origin or socioeconomic level, providing greater strength to the data collected [5,7,15]. These unmeasured variables may partly explain the high rate of home deaths observed, independently of preference recording.
A major strength of this study is the use of real-world data from a large and heterogeneous population, enhancing external validity for similar urban settings. Similarly, the study has a large and heterogeneous sample size that, by exhibiting a relatively balanced distribution between the groups, supports its external validity and favours its translation to other care contexts.
In clinical practice, systematically exploring and documenting patients’ preferences regarding place of care and death may support patient-centred decision-making and help align care with patients’ values. However, achieving the preferred place of death likely requires not only documentation but also adequate resources, caregiver support and coordinated care.
5. Conclusion
This study evaluated the factors that were associated with fulfilling the preferences for place of death. Older age and female sex were independently associated with a higher probability of home death. Although most patients who expressed a preference for home achieved this outcome, recording the preferred place of care or death was not independently associated with the place of death.
Systematically exploring and documenting patients’ preferences regarding place of care and death remains an important component of ACP and patient-centred care, but must be accompanied by sufficient resources and coordinates support to ensure that preferences can be fulfilled. Taking into account the preferences of patients allows the people directly involved in their care to establish appropriate therapeutic objectives and avoid aggressive measures or treatments and unnecessary expenses; thus, the patient is able to participate in decision-making about their own health.
List of Abbreviations
| AECC | Asociación Española Contra el Cáncer (Spanish Association Against Cancer) |
| PC | Palliative care |
| HPC | Home palliative care |
| AD | Alzheimer's disease |
| ALS | Amyotrophic lateral sclerosis |
| MS | Multiple sclerosis |
| COPD | Chronic obstructive pulmonary disease |
| ACP | Advance care planning |
| SERMAS | Servicio Madrileño de Salud (Madrid Health Service) |
| MSPCU | Mid-stay palliative care units |
| APCU | Acute palliative care hospitalization unit |
Appendix A. Clinical Characteristics of the Participants
| Group | Subgroup | % in subgroup | Pathology | N | % |
| Nononcological | Neurodegenerative diseases | 20.7 | Alzheimer's disease (AD) | 8 | 1.72 |
| Parkinson's disease | 3 | 0.65 | |||
| Dementia with Lewy bodies | 1 | 0.22 | |||
| Prion disease | 1 | 0.22 | |||
| Amyotrophic lateral sclerosis (ALS) | 5 | 1.08 | |||
| Multiple sclerosis (MS) | 2 | 0.43 | |||
| Other dementias/neurodegenerative diseases | 17 | 3.66 | |||
| Respiratory diseases | 17.8 | Chronic obstructive pulmonary disease (COPD) | 15 | 3.23 | |
| Interstitial lung diseases | 6 | 1.29 | |||
| Other chronic respiratory diseases | 11 | 2.37 | |||
| Organ deficiencies | 28.5 | Heart failure | 34 | 7.33 | |
| Chronic kidney disease | 13 | 2.8 | |||
| Hepatic insufficiency | 4 | 0.86 | |||
| Vascular diseases | 5.6 | Stroke | 7 | 1.51 | |
| Other | 3 | 0.65 | |||
| Other nononcological diseases | 27.4 | Advanced geriatric disease | 31 | 6.68 | |
| Other | 18 | 3.88 | |||
| Oncological | Digestive | 36.9 | Colon cancer | 37 | 7.97 |
| Rectal cancer | 13 | 2.8 | |||
| Pancreatic cancer | 20 | 4.31 | |||
| Cholangiocarcinoma | 5 | 1.08 | |||
| Hepatocellular carcinoma | 8 | 1.72 | |||
| Oesophageal cancer | 2 | 0.43 | |||
| Gastric cancer | 1 | 0.22 | |||
| Other digestive cancers | 19 | 4.09 | |||
| Respiratory | 17.9 | Bronchus and lung cancer | 51 | 10.99 | |
| Gynaecological | 15.8 | Breast cancer | 24 | 5.17 | |
| Ovarian cancer | 12 | 2.59 | |||
| Endometrial, cervical, uterine body cancers | 8 | 1.72 | |||
| Vulvar cancer | 1 | 0.22 | |||
| Genitourinary | 12.9 | Bladder cancer | 14 | 3.02 | |
| Prostate cancer | 13 | 2.8 | |||
| Renal cancer | 9 | 1.94 | |||
| Other genitourinary cancers | 1 | 0.22 | |||
| Haematological | 3.2 | Multiple myeloma | 4 | 0.86 | |
| Lymphomas | 3 | 0.65 | |||
| Acute myeloid leukaemia | 2 | 0.43 | |||
| Skin and appendages | 2.8 | Melanoma | 7 | 1.51 | |
| Basal cell carcinoma | 1 | 0.22 | |||
| Head and neck | 2.5 | Face, head and neck cancers | 7 | 1.51 | |
| Central nervous system | 1.4 | Glioblastoma multiforme | 4 | 0.86 | |
| Bone and soft tissue | 0.7 | Liposarcoma | 2 | 0.43 | |
| Other oncological diseases | 5.9 | Other cancers | 17 | 3.66 | |
| Total | 464 | 100 |
Author Contributions
ACR: conceptualization, design, data interpretation, writing of the work. RSR: substantial revision of the text. JBC: substantial revision of the text. EPC: methodology, data analysis, substantial revision of the text. ESAPD Espronceda Collaborative Group: data collection and article review. All the authors read and approved the final manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The present study was approved by the Drug Research Ethics Committee of the University Hospital of La Princesa on 6 October 2023 (CEIm act 18/23, approval code: 5357) and by the Local Research Commission Center of Primary Care Management of SERMAS on 11 January 2024 (act 1/2024, committee code: 20230002). The data analysed in this investigation were collected by the professionals who had treated these patients and were anonymized to ensure patient confidentiality.
Informed Consent Statement
Not applicable. This study used secondary data extracted from the AP Madrid electronic medical record system, which includes anonymized clinical and sociodemographic information of patients who received home palliative care. As the data was collected as part of routine clinical care and not through direct participant engagement in this study, no informed consent was required. The data were anonymized to ensure confidentiality and privacy, and all analyses were conducted in accordance with ethical standards.
Data Availability Statement
The datasets generated and analysed during the current study are not publicly available due to privacy restrictions, but can be obtained upon reasonable request.
Acknowledgments
The authors would like to thank Rodrigo Medina García for his valuable advice, as well as the professors of the Master’s Degree in Palliative Care at the Universidad Autónoma de Madrid, especially Ana de Santiago Ruiz, Álvaro Gándara del Castillo, María Varela Cerdeira, Yolanda Vilches Aguirre, and Alberto Alonso Babarro. ESAPD Espronceda Collaborative Group: 1. Gianella-Blanco, Cristina. Specialist in Geriatrics. Palliative Care Unit. Pere Virgili Social and Health Center (Barcelona). 2. Muñoz-Tornero, Ana. Specialist in Family and Community Medicine. Hospital Support Unit, Villaba General Hospital (Madrid). 3. Zavala-Barrientos, Mayra. Specialist in Geriatrics. Laguna Care Center Hospital (Madrid). 4. Morán-Tiesta, Cristina. Specialist in Family and Community Medicine. Master of Palliative Care. ESAPD Espronceda (Madrid). 5. Navarro-Ortega, Cristina. Nurse. Master in Palliative Care from the University of Navarra. ESPAD Espronceda (Madrid). 6. Sanz-Ventureira, Lara. Nurse. Master of Palliative Care from San Jorge University. ESAPD Espronceda (Madrid). During the preparation of this manuscript, the authors used ChatGPT (version 5.2) for grammar correction and translation. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflict of interest.
List of Abbreviations
References
- Gomes, B.; Higginson, I.J.; Calanzani, N.; Cohen, J.; Deliens, L.; Daveson, B.A.; Bechinger-English, D.; Bausewein, C.; Ferreira, P.L.; Toscani, F.; et al. Preferences for place of death if faced with advanced cancer: a population survey in England, Flanders, Germany, Italy, the Netherlands, Portugal and Spain. Ann. Oncol. 2012, 23, 2006–2015. [Google Scholar] [CrossRef]
- Gomes, B.; Calanzani, N.; Gysels, M.; Hall, S.; Higginson, I.J. Heterogeneity and changes in preferences for dying at home: a systematic review. BMC Palliat. Care 2013, 12, 7–7. [Google Scholar] [CrossRef]
- Groenewoud, AS; Sasaki, N; Westert, GP; Imanaka, Y. Preferences in end of life care substantially differ between the Netherlands and Japan: Results from a cross-sectional survey study. Medicine [Internet] 2020, 99(44), e22743. Available online: https://pubmed.ncbi.nlm.nih.gov/33126312/. [CrossRef] [PubMed]
- Alonso-Babarro, A.; Astray-Mochales, J.; Domínguez-Berjón, F.; Gènova-Maleras, R.; Bruera, E.; Díaz-Mayordomo, A.; Cortes, C.C. The association between in-patient death, utilization of hospital resources and availability of palliative home care for cancer patients. Palliat. Med. 2012, 27, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.; Pivodic, L.; Miccinesi, G.; Onwuteaka-Philipsen, B.D.; A Naylor, W.; Wilson, D.M.; Loucka, M.; Csikos, A.; Pardon, K.; Block, L.V.D.; et al. International study of the place of death of people with cancer: a population-level comparison of 14 countries across 4 continents using death certificate data. Br. J. Cancer 2015, 113, 1397–1404. [Google Scholar] [CrossRef] [PubMed]
- Black, H.; Waugh, C.; Munoz-Arroyo, R.; Carnon, A.; Allan, A.; Clark, D.; Graham, F.; Isles, C. Predictors of place of death in South West Scotland 2000–2010: Retrospective cohort study. Palliat. Med. 2016, 30, 764–771. [Google Scholar] [CrossRef]
- Cabañero-Martínez, M.J.; Nolasco, A.; Melchor, I.; Fernández-Alcántara, M.; Cabrero-García, J. Place of death and associated factors: a population-based study using death certificate data. Eur. J. Public Heal. 2019, 29, 608–615. [Google Scholar] [CrossRef]
- Lopes, S.; de Sousa, A.B.; Delalibera, M.; Namukwaya, E.; Cohen, J.; Gomes, B. The rise of home death in the COVID-19 pandemic: a population-based study of death certificate data for adults from 32 countries, 2012–2021. eClinicalMedicine 2024, 68, 102399. [Google Scholar] [CrossRef]
- Patrick, D.L.; A Engelberg, R.; Curtis, J. Evaluating the Quality of Dying and Death. J. Pain Symptom Manag. 2001, 22, 717–726. [Google Scholar] [CrossRef]
- Gomes, B.; Higginson, I.J. Factors influencing death at home in terminally ill patients with cancer: systematic review. BMJ 2006, 332, 515–521. [Google Scholar] [CrossRef]
- Costa, V.; Earle, C.C.; Esplen, M.J.; Fowler, R.; Goldman, R.; Grossman, D.; Levin, L.; Manuel, D.G.; Sharkey, S.; Tanuseputro, P.; et al. The determinants of home and nursing home death: a systematic review and meta-analysis. BMC Palliat. Care 2016, 15, 8–8. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Capel, M.; Jones, G.; Gazi, T. The importance of identifying preferred place of death. BMJ Support. Palliat. Care 2015, 9, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Babarro, A.; Bruera, E.; Varela-Cerdeira, M.; Boya-Cristia, M.J.; Madero, R.; Torres-Vigil, I.; De Castro, J.; González-Barón, M. Can This Patient Be Discharged Home? Factors Associated With At-Home Death Among Patients With Cancer. J. Clin. Oncol. 2011, 29, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Busquet-Duran, X.; Manresa-Domínguez, J.M.; Llobera-Estrany, J.; López-García, A.I.; Moreno-Gabriel, E.; Torán-Monserrat, P. Complejidad asistencial y lugar de muerte en atención domiciliaria paliativa. Gac. Sanit. 2022, 37, 102266. [Google Scholar] [CrossRef]
- Aguilar Huerta, O; Bayón Cubero, IC; Fernández Gutiérrez, AL; Regadera González, M. Does primary care intervention have an impact in the place of death for patients in a palliative care program? Aten Primaria 2021, 53(8). [Google Scholar]
- Nolasco, A.; Fernández-Alcántara, M.; Pereyra-Zamora, P.; Cabañero-Martínez, M.J.; Copete, J.M.; Oliva-Arocas, A.; Cabrero-García, J. Socioeconomic inequalities in the place of death in urban small areas of three Mediterranean cities. Int. J. Equity Heal. 2020, 19, 1–11. [Google Scholar] [CrossRef]
- Chen, H.; Nicolson, D.J.; Macleod, U.; Allgar, V.; Dalgliesh, C.; Johnson, M. Does the use of specialist palliative care services modify the effect of socioeconomic status on place of death? A systematic review. Palliat. Med. 2015, 30, 434–445. [Google Scholar] [CrossRef]
- Cabañero-Martínez, MJ; Nolasco, A; Melchor, I; Fernández-Alcántara, M; Cabrero-García, J. Lugar de fallecimiento de las personas con enfermedades susceptibles de cuidados paliativos en las diferentes comunidades autónomas de España. An Sist Sanit Navar 2020, 43(1), 69–80. [Google Scholar]
- Gomes, B.; Higginson, I.J.; McCrone.
- Tan, W.S.; Bajpai, R.; Low, C.K.; Ho, A.H.Y.; Wu, H.Y.; Car, J. Individual, clinical and system factors associated with the place of death: A linked national database study. PLOS ONE 2019, 14, e0215566. [Google Scholar] [CrossRef]
- Abe, K.; Miyawaki, A.; Kobayashi, Y.; Watanabe, T.; Tamiya, N. Place of death associated with types of long-term care services near the end-of-life for home-dwelling older people in Japan: a pooled cross-sectional study. BMC Palliat. Care 2020, 19, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Abe, K.; Kawachi, I.; Watanabe, T.; Tamiya, N. Association of the Frequency of In-Home Care Services Utilization and the Probability of In-Home Death. JAMA Netw. Open 2021, 4, e2132787–e2132787. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.S.; Chae, Y.M.; Lee, C.G.; Kim, S.-Y.; Lee, S.-W.; Heo, D.S.; Kim, J.S.; Lee, K.S.; Hong, Y.S.; Yun, Y.H. Factors influencing preferences for place of terminal care and of death among cancer patients and their families in Korea. Support. Care Cancer 2005, 13, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.K.; Dodek, P.; Rocker, G.; Groll, D.; Gafni, A.; Pichora, D.; Shortt, S.; Tranmer, J.; Lazar, N.; Kutsogiannis, J.; et al. What matters most in end-of-life care: perceptions of seriously ill patients and their family members. Can. Med Assoc. J. 2006, 174, 627–633. [Google Scholar] [CrossRef]
- Sudore, RL; Lum, HD; You, JJ; Hanson, LC; Meier, DE; Pantilat, SZ; et al. Defining Advance Care Planning for Adults: A Consensus Definition From a Multidisciplinary Delphi Panel. J Pain Symptom Manage 2017, 53(5), 821–832.e1. [Google Scholar] [CrossRef]
- Skorstengaard, M.H.; Jensen, A.B.; Andreassen, P.; Brogaard, T.; Brendstrup, E.; Løkke, A.; Aagaard, S.; Wiggers, H.; Neergaard, M.A. Advance care planning and place of death, hospitalisation and actual place of death in lung, heart and cancer disease: a randomised controlled trial. BMJ Support. Palliat. Care 2019, 10, e37–e37. [Google Scholar] [CrossRef]
- Dixon, J.; King, D.; Knapp, M. Advance care planning in England: Is there an association with place of death? Secondary analysis of data from the National Survey of Bereaved People. BMJ Support. Palliat. Care 2016, 9, 316–325. [Google Scholar] [CrossRef]
- Abel, J.; Pring, A.; Rich, A.; Malik, T.; Verne, J. The impact of advance care planning of place of death, a hospice retrospective cohort study. BMJ Support. Palliat. Care 2013, 3, 168–173. [Google Scholar] [CrossRef]
- Felícitas Domínguez-Berjón, M; Carme Borrell /; Cano-Serral, G; Esnaola, S; Nolasco, A; Isabel, Pasarín / M; et al. Constructing a deprivation index based on census data in large Spanish cities [the MEDEA project]; Gac Sanit, 2008; Vol. 22. [Google Scholar]
- Barata, AN; Salvetti, A; Bussotti, Alessandro; Demurtas, Jacopo. Dying at Home. In Practical issues in geriatrics; 30 Dec 2021; pp. 357–66. [Google Scholar]
- Gott, M.; Morgan, T.; Williams, L. Gender and palliative care: a call to arms. Palliat. Care Soc. Pr. 2020, 14. [Google Scholar] [CrossRef]
- Brundisini, F.; Giacomini, M.; DeJean, D.; Vanstone, M.; Winsor, S.; Smith, A. Chronic disease patients' experiences with accessing health care in rural and remote areas: a systematic review and qualitative meta-synthesis. 2013, 13, 1–33. [Google Scholar]
Figure 1.
Flowchart of eligible participants.
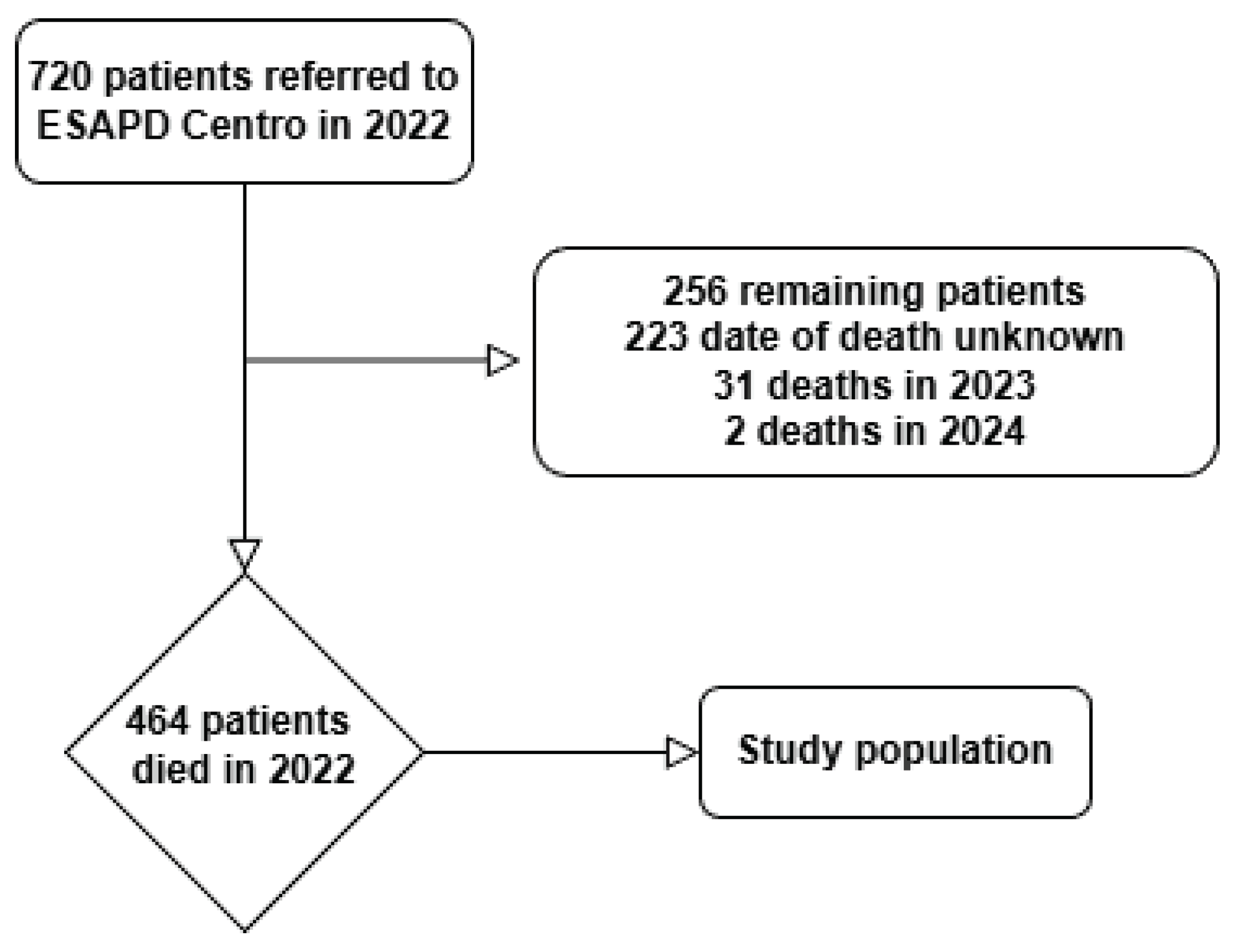

Table 1.
Baseline characteristics of the study population (n = 464). Abbreviations: SD, standard deviation; IQR, interquartile range.
Table 1.
Baseline characteristics of the study population (n = 464). Abbreviations: SD, standard deviation; IQR, interquartile range.
| n = 464 | % | ||
|---|---|---|---|
| Sex (Female) | 246 | 53 | |
| Had a caregiver (Yes) | 112 | 24.1 | |
| Age (years, SD) | 80.8±13.0 | ||
| HPC follow-up duration (days, IQR) | 20 (7-57) | ||
| Place of death | Home | 383 | 82.5 |
| Hospital | 65 | 14.1 | |
| Mid-stay Palliative Care Unit | 16 | 3.4 | |
| Preferred place of death | Not recorded | 350 | 75.4 |
| Home | 109 | 23.5 | |
| Hospital | 5 | 1.1 | |
| Preferred place of care or death | Not recorded | 167 | 36 |
| Home | 290 | 62.5 | |
| Hospital | 5 | 1.1 | |
| Mid-stay Palliative Care Unit | 2 | 0.4 | |
Table 2.
Factors associated with death at home (bivariate analysis). p-values from chi-square test or Student’s t-test as appropriate.
Table 2.
Factors associated with death at home (bivariate analysis). p-values from chi-square test or Student’s t-test as appropriate.
| Variable | Home death n (%) | Non-home death n (%) | p-value |
|---|---|---|---|
| Female sex | 212 (86.2%) | 34 (13.8%) | <0.05 |
| Male sex | 171 (78.4%) | 47 (21.6%) | <0.05 |
| Age (mean, years) | 82.1 | 78.3 | <0.05 |
| Non-oncological disease | 156 (87.2%) | 23 (12.8%) | <0.05 |
| Oncological disease | 227 (79.6%) | 58 (20.4%) | <0.05 |
| Primary caregiver | Not significant | Not significant | >0.05 |
| Preference for home recorded | Not significant | Not significant | 0.87 |
Table 3.
Multivariable logistic regression for death at home. Abbreviations: OR, odds ratio; CI, confidence interval.
Table 3.
Multivariable logistic regression for death at home. Abbreviations: OR, odds ratio; CI, confidence interval.
| Variable | OR | 95% CI | p-value |
|---|---|---|---|
| Age (per year) | 1.02 | 1.00–1.04 | 0.026 |
| Female sex | 0.60 | 0.37–0.98 | 0.042 |
| Oncological disease | Not significant | — | >0.05 |
| Preference recorded | Not significant | — | >0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



