
Submitted:
09 February 2026
Posted:
09 February 2026
You are already at the latest version
Abstract
(1) Background: Malnutrition increases the risk of complications, prolongs the period of hospitalization, worsens the results of treatment and increases the costs of hospital stay. Patient’s lack of knowledge on how to cope with it may increase the occurrence of these unfavorable consequences. The aim of this study was to assess hospitalised patients awareness of foods for special medical purposes (FSMP) and to determine the perception of the dietitian’s role in the hospital treatment process. (2) Methods: The survey was conducted among patients hospitalized in one of the hospital in the Małopolska region. The sample consisted of 100 respondents. Participation in the research was anonymous and voluntary. The author’s survey contained 14 closed- and open-ended questions. The answers were single or multiple choice. A knowledge test was used to determine the level of awareness among respondents. The maximum score was 8. Appropriately selected tests were applied to the collected data, such as Spearman’s correlation, Shaprio-Wilk’s normality test, Leven’s and Mann-Witney’s tests. The level of statistical significance was assumed to be p ≤ 0.05. (3) Results: Respondents were most familiar with the term Nutridrnik (68%). Nestlé was the most popular brand. Only 66% declared they knew what foods for special medical purposes were used for. Most were unfamiliar with the concept of immunomodulatory ingredients. Statistically significant correlation was found between age and knowledge. Older patients achieved lower scores (rho=-0.32, p=0.001). No statistical significance was found between gender or comorbidities and knowledge on the discussed topic. A dietitian was pointed out as the expert in selecting FSMP (78.6%). It is crucial that 87% of respondents believe that FSMP consumption may be beneficial for nutritional status. (4) Conclusion: The results indicate limited hospitalised patients knowledge of foods for special medical purposes. The role of dietitians in the treatment process is highly valued. Educational efforts hospitals are necessary to improve patient awareness. This can also improve the effectiveness of nutritional therapy, as well as preventive measures aimed at improving the patient’s nutritional status.
Keywords:
foods for special medical purposes
; malnutrition
; nutritional treatment
1. Introduction
One of the many problems faced by hospitalized patients, especially the elderly, is malnutrition [1]. Malnutrition, as defined by the WHO, ASPEN, and ESPEN, is an imbalance between the supply and utilization of nutrients. It can involve both deficiency and excess of nutrients, as well as diet-related diseases. Malnutrition is associated with a poorer prognosis, an increased risk of complications, and prolonged hospitalization [2,3,4]. It is a clinical condition resulting from poor nutrition or a disease that causes digestive and malabsorption disorders, or symptoms that negatively affect appetite, resulting in reduced intake of micro and macronutrients [5,6]. It is estimated that up to 50% of hospitalized patients may suffer from disease-related malnutrition, and 30% of patients will develop malnutrition during their hospital stay [7,8]. According to a review by Salari et al. [2025] malnutrition among older adults worldwide is 18.6%. Malnutrition results in numerous adverse changes in the body, such as changes in body composition (loss of muscle mass and fat tissue) and deterioration of muscle function, including cardiac, renal, and respiratory muscle function [9]. Gastrointestinal function regresses through impact on the function of the pancreas, intestinal villus, and colon, which can cause diarrhea and further impairment of digestion and absorption [5]. Malnourished patients have prolonged hospital stays and a higher risk of mortality, poorer response to treatment, impaired wound healing and immune function, and prolonged recovery time after procedures [10,11]. Elderly people and those with underlying health conditions (oncology, neurological, and critically ill patients) are particularly at risk [8,10]. A key approach to preventing malnutrition is proper assessment of nutritional status, which allows for early detection and mitigation of its progression and negative consequences. Effective tools include scales that include questions about weight loss over a selected period, current body weight, existing diseases, and food consumption.
If malnutrition is detected or is at high risk, appropriate intervention should be initiated. It has been estimated that investing $1 in nutritional therapy will yield a $54 return on investment [12]. Depending on the needs and capabilities, dietary fortification with ONS, enteral nutrition, or parenteral nutrition is used, according to the ESPEN protocol [13]. If the patient is unable to consume adequate amounts of food, a dietary consultation is recommended to establish an oral diet, possibly supplemented with oral nutritional supplements (ONS). ONS are food for special medical purposes (FSMP), preparations that allow for easy delivery of energy and protein in a small volume. Depending on the disease state, selected preparations may be enriched or omitted with certain essential ingredients. ONS can be classified in various ways. There are hypocaloric (0.5-0.9 kcal/ml), isocaloric (0.9-1.2 kcal/ml), and hypercaloric (1.3-2.4 kcal/ml). Based on their ingredient content, they are classified as high-energy, high-protein and mixed [14]. Proteins can be in varying degrees of hydrolysis polymeric, oligomeric and monomeric. Many different types allow them to be tailored to specific diseases. Formulations with reduced monosaccharides and saccharose, content, a low glycemic index, and added dietary fiber are intended for diabetics. In liver diseases at risk of encephalopathy, formulas with added branched-chain amino acids (BCAAs), fiber, and medium-chain triglycerides (MCTs) are recommended. For chronic kidney disease, hypercaloric ONS with reduced protein content (approximately 6% of energy) and electrolytes are used [15]. Immunonutrition is the supply of selected ingredients that modulate the immune response and inflammatory processes [16]. These preparations contain omega-3 fatty acids, selected amino acids such as glutamine and arginine, nucleotides, and prebiotic fiber. Formulas recommended for patients with difficult-to-heal wounds, ulcers, burns, and pressure sores contain arginine, collagen, and fatty acids, which stimulate repair processes and modulate the immune response [17,18]. For patients requiring dialysis, high-energy and high-protein ONS are used. For individuals with cow’s milk protein allergies and vegan, a formula based on plant proteins (soy) is recommended. Single-ingredient products such as protein, fiber, and thickeners are also available [15].
A lot of scientific data indicates that nutritional support through the use of ONS, along with oral diet fortification, can be crucial as an intervention against malnutrition and disease-related malnutrition [19,20,21,22,23,24]. It is crucial that both healthcare professionals and patients are aware of the potential benefits of using these supplements. Patients often show reluctance to use these supplements due to their non-conventional nature and difficulty persuading them to supplement their diet despite difficulties with swallowing, chewing, or appetite.
The aim of this study was to assess hospitalised patients awareness of foods for special medical purposes (FSMP) and to determine the perception of the dietitian’s role in the hospital treatment process.
2. Materials and Methods
The survey was conducted among patients hospitalized in one of the hospital in the Małopolska region. The sample consisted of 100 respondents. Participation in the research was anonymous and voluntary. The author’s survey contained 15 closed- and open-ended questions, 14 of which were included in this manuscript; one question was rejected due to insignificant responses. The answers were single or multiple choice. Participant characteristics are presented in Table 1.
Some respondents did not answer the questions regarding age and gender, hence the variable number of respondents (n= 98 or 99).
Respondents were also asked about comorbidities, the answers are presented in Figure 1.
The most common medical conditions reported by respondents included hypertension (27.6%) and multiple morbidities (24.1%). Specific medical conditions included diabetes (13.8%), hypothyroidism (12.1%), and cancer (12.1%).
2.1. Statiscical Analysis
A knowledge test was used to determine the level of awareness among respondents. The maximum score was 8. The results were interpreted as follows: <25% - lack of knowledge, <50% - low level of knowledge, <75% - average level of knowledge, >=75% - high level of knowledge. A statistical analysis was conducted based on the data obtained. The Spearman correlation coefficient was used to determine the direction and strength of the relationship between age and knowledge of special medical purposes. The following procedure was used to verify knowledge between genders and the correlation between comorbidities and knowledge. The Shapiro-Wilk test was used to test for normality of residual distribution, the Levene test to determine the homogeneity of variance between the compared groups, and the Mann-Whitney test to analyze the significance of differences in knowledge levels, taking into account gender or the presence of comorbidities. The assumed level of statistical significance in the analysis was p ≤ 0.05.
3. Results and Discussion
As shown in Figure 2 the term “Nutridrink” was most frequently used by survey participants (68%). It is one of the trade names of a product from the leading brand FSMP on the Polish market. It can demonstrates the effectiveness of marketing campaigns on television and social media. Despite respondents’ limited awareness of the product, the generic name ONS is still associated. Slightly fewer respondents indicated familiarity with “foods for special medical purposes” (37%) and oral nutritional supplements (35%) (the survey was conducted in Polish, therefore the translated term and the English version were provided). Less frequently selected were responses regarding familiarity with all of the terms (14%) and unfamiliarity with any of them (12%). The smallest proportion of respondents selected the ONS answer (the untranslated version) (2%).
The largest group of respondents would emphasize energy, kilocalories, and protein (53%), indicating an understanding of the role of individual macronutrients in the diet (Figure 3). Older adults should consume 1.2–1.5 g of protein/kg of body weight/day in acute or chronic conditions, and this intake should be increased to 2.0 g/kg/day in severe conditions or malnutrition. 30 kcal/kg/day is the recommended energy requirement, but other factors should be considered and recommendations should be individualized [13]. In a review of the ESPEN guidelines, the authors identified varying energy and protein requirements depending on the disease state [25]. For example, in the intensive care unit, it is recommended to implement enteral nutrition for up to 48 hours or parenteral nutrition between 3 and 7 days. If EN is not possible, the recommended energy requirement is 20–25 kcal/kg of body weight/day and 1.3 g protein/kg of body weight/day [26]. For geriatric patients 30 kcal/kg of body weight/day is recommended. Oral nutritional support should provide at least 400 kcal, including at least 30 g of protein and at least 1.0 g/kg of body weight [13]. A significant proportion of respondents indicated protein and saturated fat (25%), as well as saturated fat and carbohydrates (16%). Nine percent of respondents would emphasize energy and simple carbohydrates. Twenty-six percent of respondents declared they did not know the answer to this question.
According to the results in Figure 4 respondents most frequently cited Nestlé (58%), Nutricia (40%), and Activ Lab (27%). Olimp Labs (20%), Fresenius Kabi (6%), and Nutrego (5%) were mentioned less frequently. Thirty percent of respondents declared they were unaware of any company producing foods for special medical purposes. The high brand awareness of Nestlé and Nutricia may be due to their strong market position, broad product offerings, and active promotional and educational activities. The lower recognition of the remaining companies suggests limited availability to patients or lower marketing expenditures. At the same time, the fact that nearly one-third of respondents were unable to identify any manufacturer indicates the need for further education about foods for special medical purposes among patients. If patients do not recognize the brand, they are likely unfamiliar with the product range, which may limit the possibility of using specific products as the best choice for a given patient.
Among all respondents, 66% declared they had knowledge of the purpose of using special medical devices. However, 34% of this study participants provided a negative answer. To verify the correctness of the affirmative answer, the following question (Figure 6) was asked: „You would use FSMP on people ? (only people who answered yes to the previous question answered)”.
Figure 5.
Percentage of respondents who answered the question100% „Do you know what food for special medical purposes are used for?”.
Figure 5.
Percentage of respondents who answered the question100% „Do you know what food for special medical purposes are used for?”.
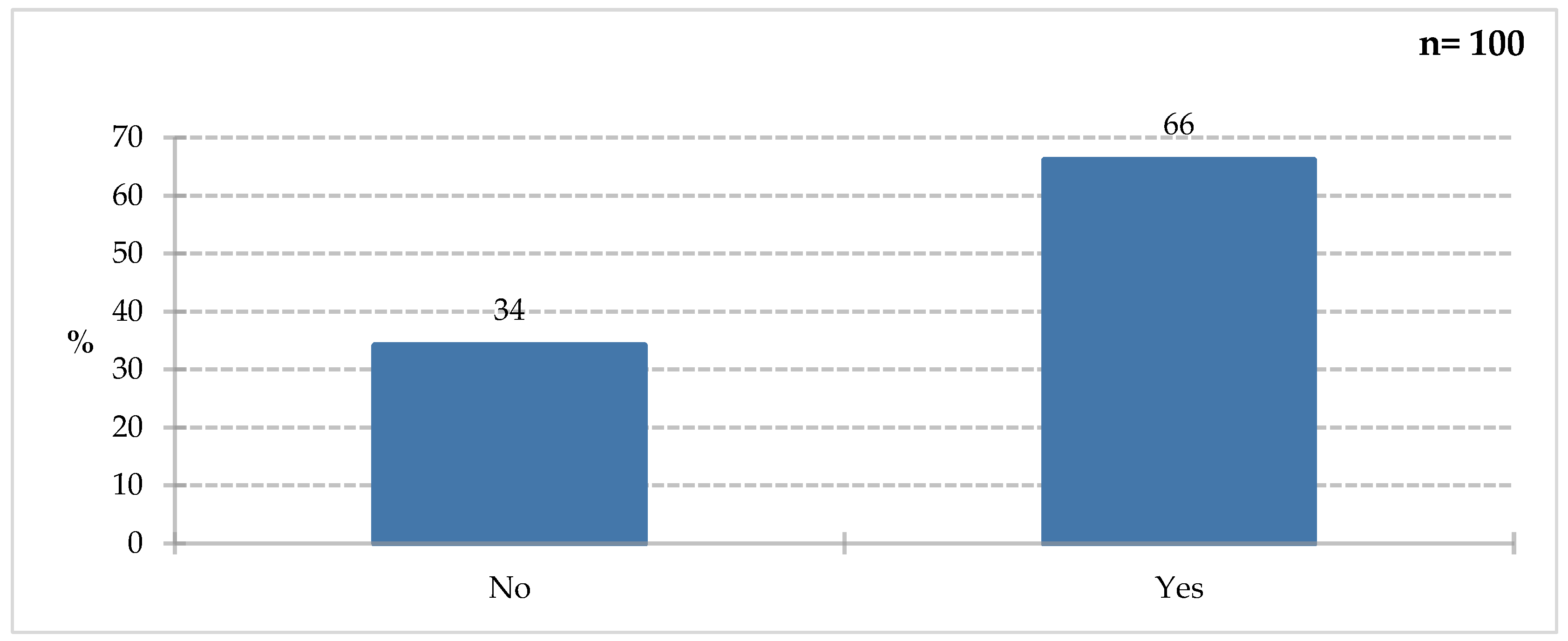
Figure 6.
Percentage of respondents who answered the question 68% „You would use FSMP on people ? (only people who answered yes to the previous question answered)”.
Figure 6.
Percentage of respondents who answered the question 68% „You would use FSMP on people ? (only people who answered yes to the previous question answered)”.
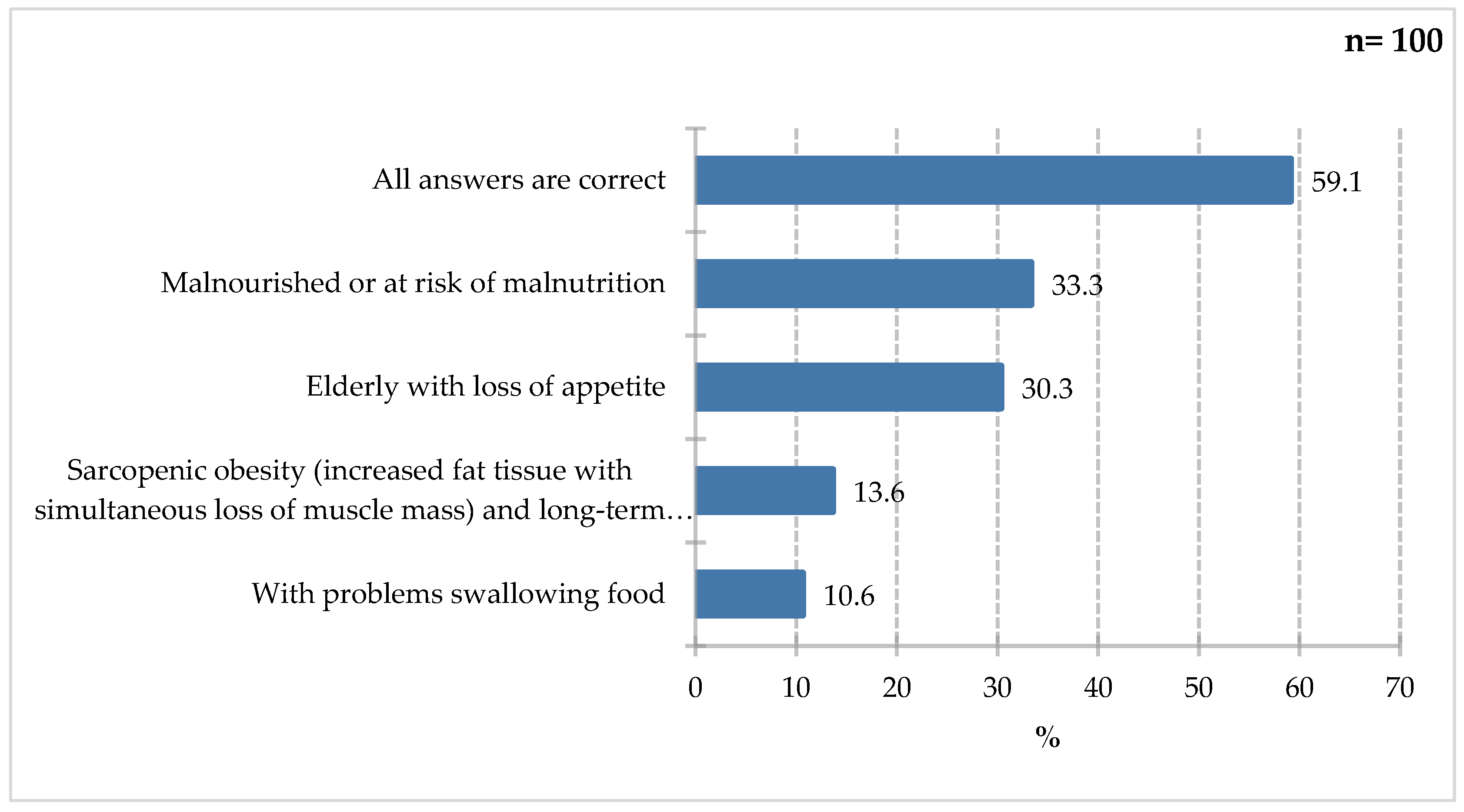
Respondents most frequently indicated the use of special medical purposes in individuals with malnutrition or at risk of malnutrition (33.3%) and in elderly individuals with a lack of appetite (30.3%). Slightly less frequently selected were patients with sarcopenic obesity, characterized by increased body fat combined with loss of muscle mass and long-term hospitalization (13.6%), as well as individuals with swallowing difficulties (10.6%). Furthermore, 59.1% of respondents indicated that all of the above answers were correct, indicating a deeper understanding of the issue of malnutrition in this patient group, as all of the above factors are indications for oral dietary fortification with ONS as the first step towards proper nutritional intervention. Indications for ONS use include:
- perioperative period – patients undergoing major procedures, gastrointestinal surgery, wound healing [27,28];
- oncological diseases – insufficient oral intake, prevention of malnutrition [29];
- elderly patients – Individuals with sarcopenia, frailty syndrome, reduced appetite [13];
- nephrology, pulmonology, neurology, psychiatry – debilitating, chronic diseases causing reduced intake, appetite disorders, and swallowing disorders [28].
The results of the Figure 7 indicate that respondents most frequently selected the glycemic index and fiber response (46%). Fewer participants indicated high simple sugar and fiber content (24%), high simple sugar and protein content (15%), and high saturated fat and fiber content (12%). Thirty-one percent of respondents declared a lack of knowledge in this area. Diabetes is a disease affecting a growing part of society. It often coexists with other conditions and carries complications such as e.g., diabetic foot and prolonged hospital stays. Patients with the disease, as well as others at increased risk, should be aware of the ingredients to look out for, which will also facilitate the decision-making process of selecting ONS for patients with glycemic disorders. According to the Polish recommendations [2025], it is necessary to pay attention to the glycemic load and index of a meal, and to consume adequate macronutrients, including fiber-rich carbohydrates (minimum 25 g/day or 15 g of fiber/1000 kcal of diet) [30]. Limiting the consumption of simple sugars, especially added and free sugars, is crucial, in favor of low-calorie sweeteners. Attention has also been paid to the supply and quality of fats – limiting saturated fats to 10% of the diet’s energy value, in favor of plant-based fats [30].
The majority of respondents (78%) were unfamiliar with immunomodulatory ingredients; only 22% of survey participants declared they were familiar with them (Figure 8). To confirm their knowledge, they were asked to list them in the next question (Figure 9).
A large proportion of the responding group mentioned vitamin C (44.4%) and vitamin D (38.9%), with slightly smaller groups highlighting ingredients such as omega-3 fatty acids, and zinc (22.2%), selenium iron, and vitamin A. Finally, the “other” category, selected by 50% of study participants, included less relevant responses such as elderberry, the aforementioned fruits or vegetables, but also vitamin E, probiotics, and vitamin E, which fall into this category. Vitamin C, as a cofactor of many enzymes and an one of the important antioxidant, can have immunomodulatory effects. Adequate dietary levels of vitamin C reduce C-reactive protein levels. By stimulating neutrophil migration, it improves wound healing. Studies indicate that vitamin C supplementation may shorten the duration of infection [28,31,32,33]. The action of vitamin D is widely described in the literature. It influences the secretion of cytokines (IL− 12, IL− 2, IFN−γ) by macrophages, regulates gene expression and cell differentiation [28,34]. There is a correlation between the activity of B and T lymphocytes and antigen-presenting cells and vitamin D. It inhibits the secretion of c-reactive protein and IL-6 [35].
As shown in the Figure 10 respondents most frequently indicated B-group vitamins and collagen (25%). Less frequently selected were arginine and omega-3 fatty acids (13%), fiber and saturated fatty acids (3%), and saturated fatty acids and arginine (2%). A significant proportion of respondents (65%) declared they did not know the answer to this question. A literature review by Arribas-López et al. [2021] indicated a positive effect of arginine and glutamine supplementation on wound healing or related parameters [36]. In turn, patients supplemented with arginine, vitamin C, and zinc showed a clinically significant improvement in pressure ulcer healing [37]. A study by Cheshmeh et al. [2021] also found a beneficial effect of arginine on pressure ulcer healing. Arginine and its metabolites improve wound healing through metabolism and nitric oxide (NO) synthesis, but attention is also drawn to the addition of other components, such as an adequate supply of calories and protein [38]. Elahi et al. [2012], in a review on the effects of fish oil, including omega-3 fatty acids, described various mechanisms and effects on the healing of stage 1 pressure ulcers. They indicated the formation of blood vessels in the ulcer, shortened hospital stays in surgical patients, and stimulation of cytokine activity [40]. In turn, in patients in the intensive care unit, the use of fish oil locally as dressings has a beneficial effect in preventing pressure ulcer development [41]. According to the review by Dospra et al. [2024] supplementation with eicosapentaenoic acid (EPA) in the postoperative period may contribute to reducing the risk of infection, supporting the wound healing process and shortening the recovery time of patients [42].
Survey participants most often cited a dietitian (78.6%) as the specialist they would seek advice on selecting special medical supplies. Physicians (38.8%) and pharmacists (11.2%) were significantly less likely to choose one. Nurses were cited by 5.1% of respondents (Figure 11). Although, by law, only a physician can prescribe ONS for a hospitalized patient, a dietitian can be an important part of the process. Patient responses also indicate a growing trust in this professional group.
Forty-five percent of respondents confirmed that they had experience with this type of food during their hospital stay (Figure 12).
Figure 12.
Percentage of respondents who answered the question100% „Have you ever use food for special medical purposes during your hospitalization?”.
Figure 12.
Percentage of respondents who answered the question100% „Have you ever use food for special medical purposes during your hospitalization?”.
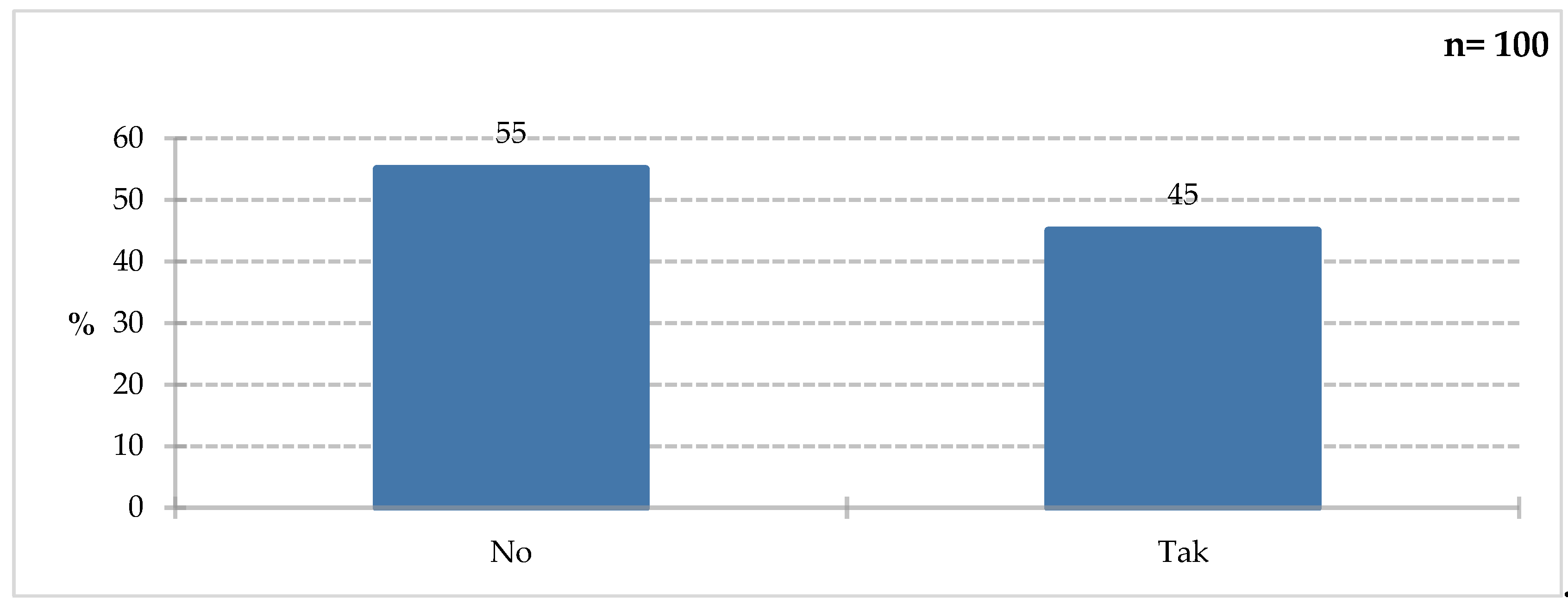
Figure 13.
Percentage of respondents who answered the question 100% „Which of the following symptoms would you notice as risk factors for malnutrition?”.
Figure 13.
Percentage of respondents who answered the question 100% „Which of the following symptoms would you notice as risk factors for malnutrition?”.
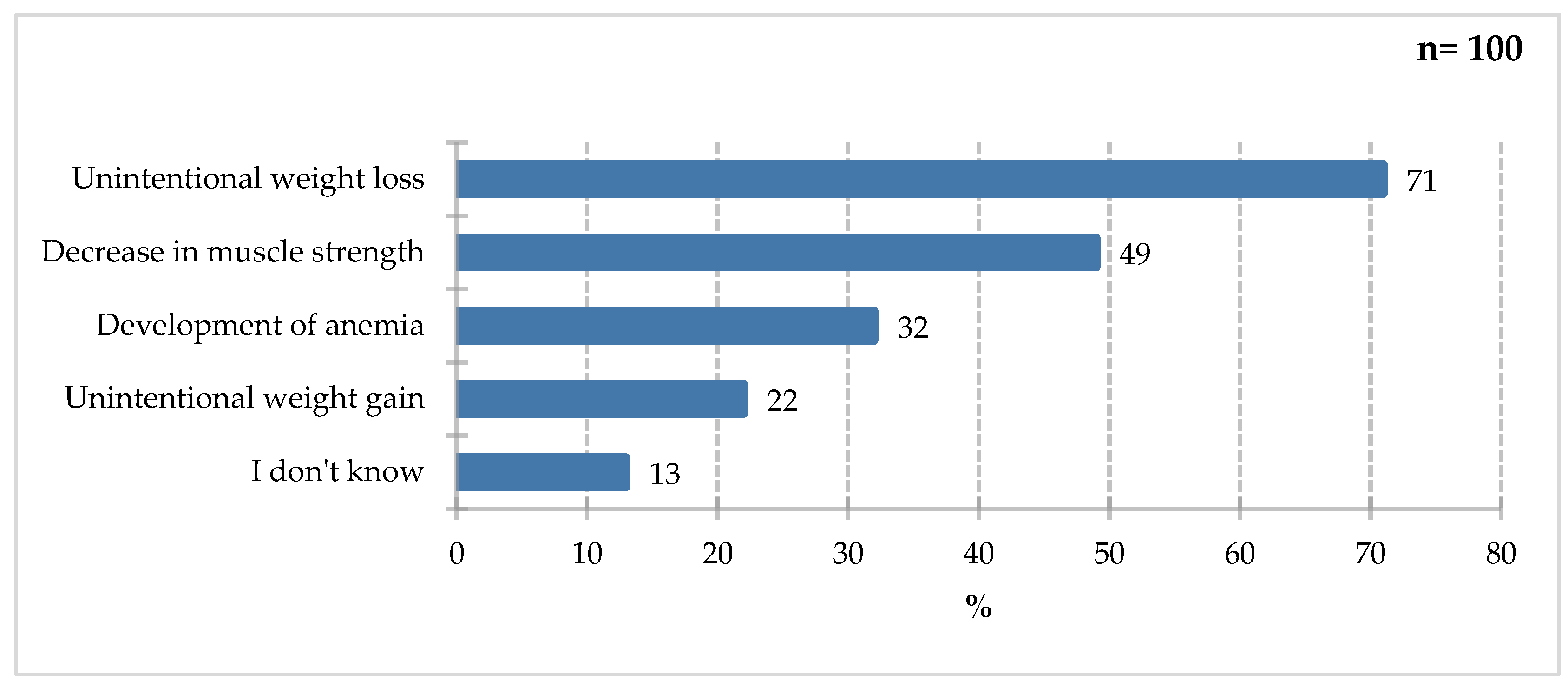
The largest share of study participants would report unintentional weight loss (71%). Decreased muscle strength (49%) and the development of anemia (32%) were also frequently mentioned. Unintentional weight gain (22%) and lack of knowledge on the subject (13%) were less frequently mentioned. Underweight in adults is defined as a BMI below 18.5. Consequences of insufficient dietary intake include impaired function, negative impact on muscle mass and fitness, sarcopenia, and the development of anemia. Unintentional weight gain can lead to overweight and obesity, but it does not correlate with an increased risk of underweight, which does not exclude the occurrence of sarcopenia and qualitative malnutrition in excess body weight [43].
Respondents most often believed that collaboration with a dietitian on hospital wards was necessary (75%). It was recommended, but not essential, according to 18% of respondents; only 4% declared it unnecessary, while 3% had no opinion on the matter (Figure 14). It’s encouraging that patients are beginning to understand the role of nutrition and the need for interdisciplinary collaboration. Dietitians in hospitals play a role as important as other medical professionals, assessing nutritional status, providing nutritional education to patients, fortifying a natural diet, and collaborating with the interdisciplinary team to determine nutritional treatment. According to a 2018 report, the role of dietitians in hospitals is still misunderstood. In the audited facilities, nutritional education was lacking, with each dietitian serving between 76 and 740 patients, and additional duties unrelated to their competencies were assigned, such as warehouseman, kitchen assistant, or archivist [44]. This may be due to the lack of regulations regarding the scope of duties and competences of the dietitian. Bator [2017] assessed the nutritional knowledge of healthcare workers, and the results were clear: the staff’s knowledge was insufficient and the dietitian should be responsible for providing nutritional education to patients [45]. Folwarski and Wernio [2023] clearly described the benefits of employing a dietitian in hospitals, such as improved detection of malnutrition and shorter hospital stays, as well as significant savings due to the accuracy of nutritional intervention tailored to the patient’s condition and needs [12]. Mogiłko and Zarzeczny [2024], in turn, emphasize the dietitian’s important role in the prehabilitation process, as one of the new but crucial tasks in patient care. This includes the selection of individualized nutritional recommendations, assessment of nutritional status, and continuous monitoring of outcomes [46].
Figure 14.
Percentage of respondents who answered the question 100% „How do you assess the need for cooperation with a dietitian in hospital wards?”.
Figure 14.
Percentage of respondents who answered the question 100% „How do you assess the need for cooperation with a dietitian in hospital wards?”.
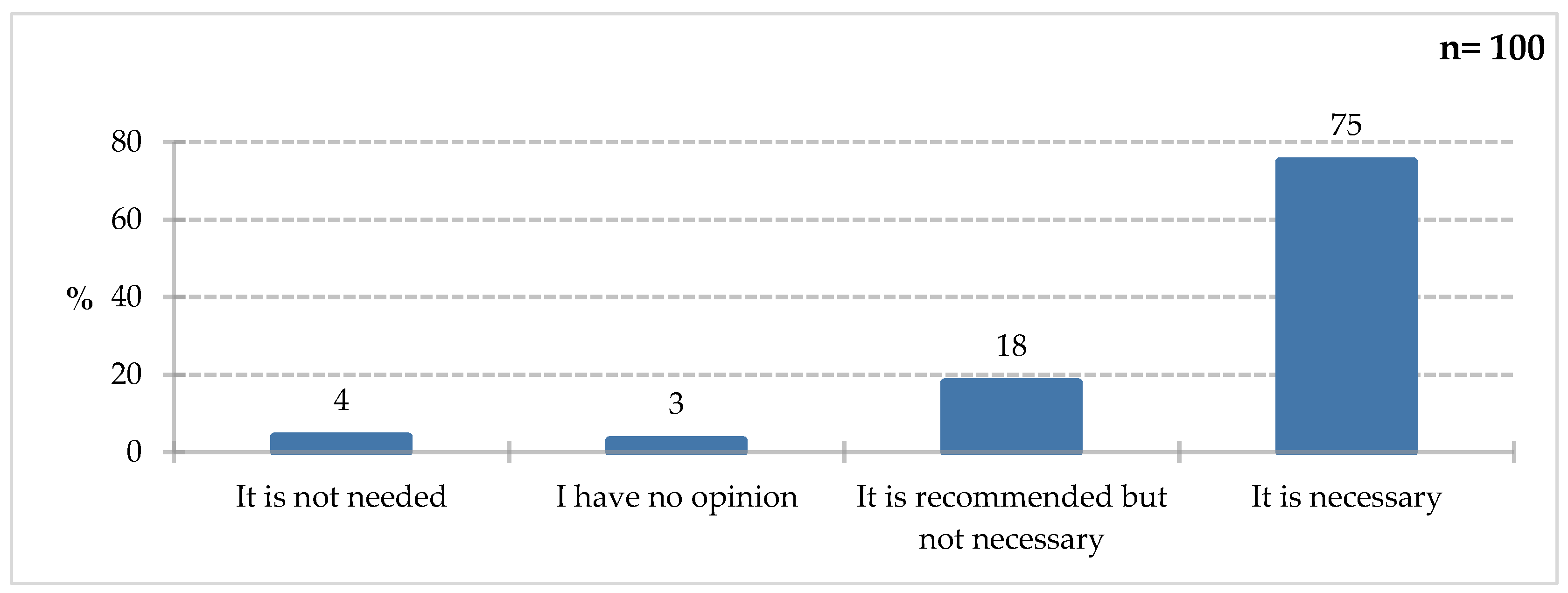
Figure 15.
Percentage of respondents who answered the question 100% „Do you think that the use of FSMP purposes can be an important measure to improve or maintain the nutritional status of hospitalized patients?”.
Figure 15.
Percentage of respondents who answered the question 100% „Do you think that the use of FSMP purposes can be an important measure to improve or maintain the nutritional status of hospitalized patients?”.
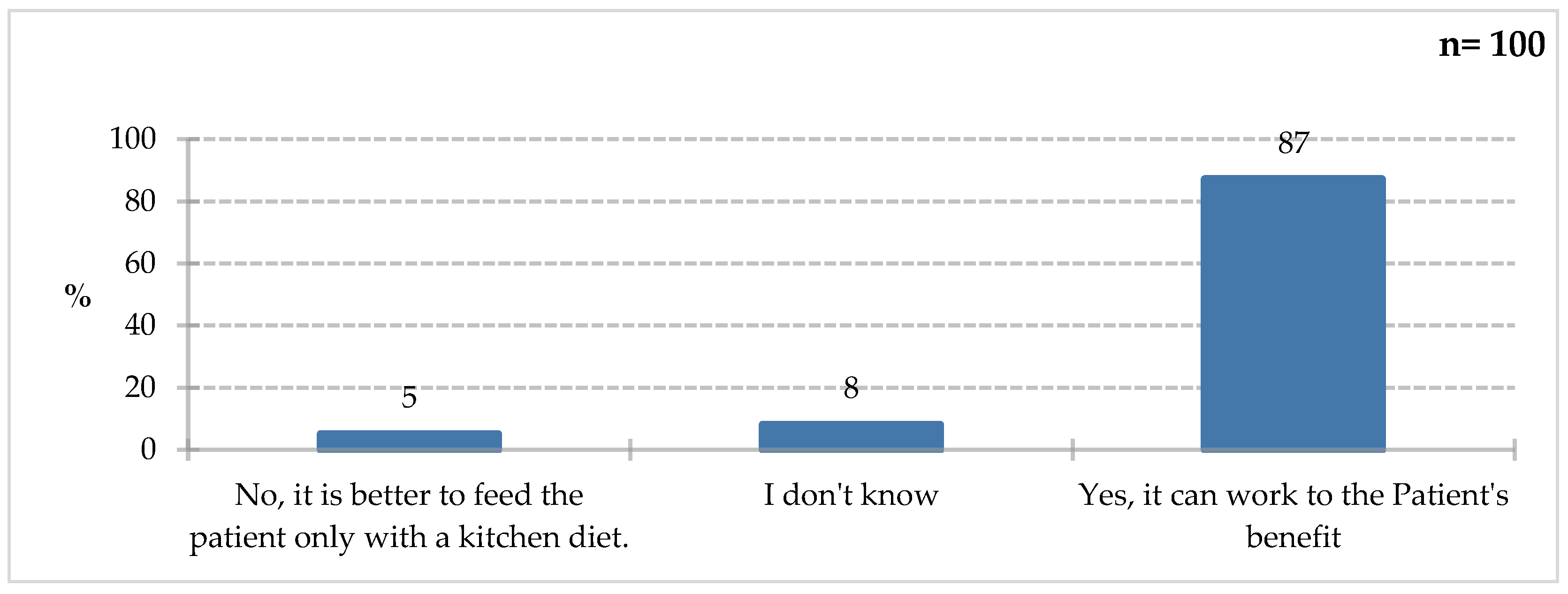
The vast majority of respondents (87%) agreed that the use of foods for special medical purposes can be a significant step towards improving or maintaining the nutritional status of hospitalized patients, pointing to the potential benefits for these patients. As previously indicated, ONS are used in many medical conditions. It is worth noting that 13% of respondents either lack knowledge on this topic or believe that a traditional kitchen diet is sufficient. This indicates the need for educational initiatives.

Table 2.
Knowledge of study participants - basic descriptive statistics.

In the knowledge test regarding foods for special medical purposes, participants scored an average of 3.90 (SD = 1.867) points out of 8 possible points. The mean percentage score was 48.75% (SD = 23.33). The interpretation of participants’ knowledge is presented in the graph (<25% - lack of knowledge, <50% - low level of knowledge, <75% - average level of knowledge, >=75% - high level of knowledge).
Figure 16.
Distribution of knowledge among study participants.
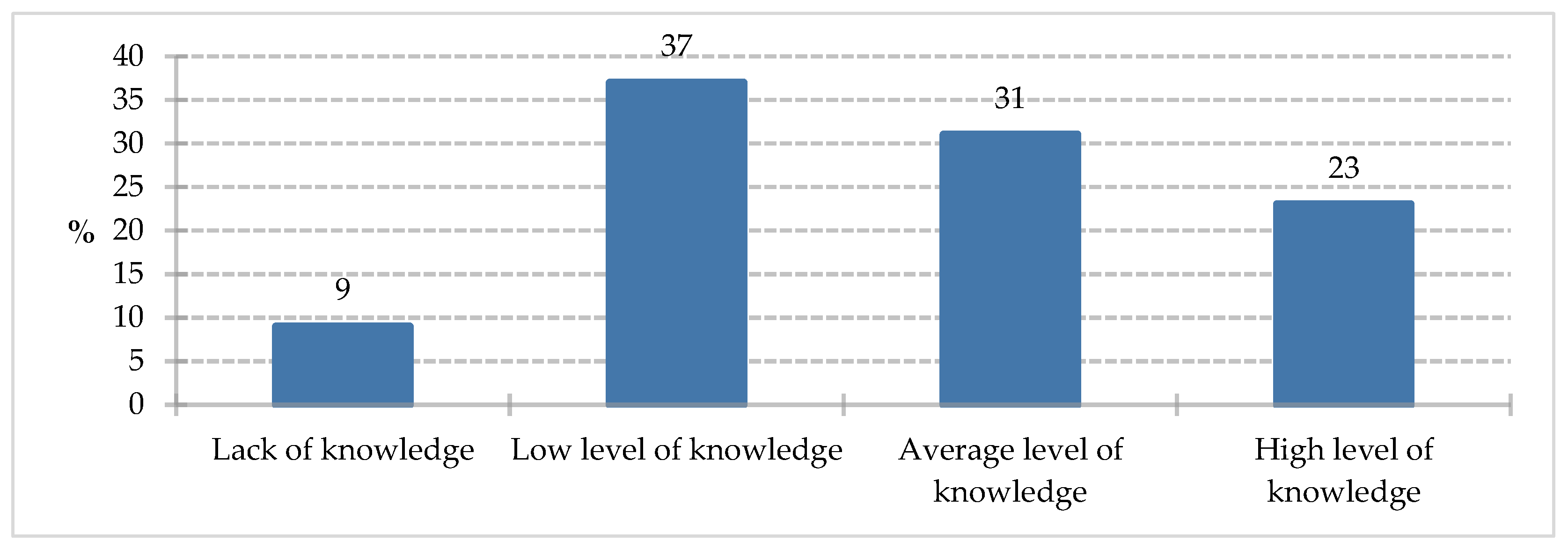
Respondents most often demonstrated a low level of knowledge in the test (37%). An average level of knowledge was recorded for 31% of study participants. A high level of knowledge was achieved by 23% of respondents, and a lack of knowledge in the area under study was noted by 9% of participants.
To determine the direction and strength of the relationship between age and knowledge about specialty foods, Spearman’s monotonic correlation coefficient was used. The results of the analysis are presented in Table 3.
The results of the Spearman’s rho correlation analysis indicate a significant correlation between age and knowledge about special-purpose foods, rho = -0.32, p = 0.001, n = 98 - the strength of the correlation turned out to be moderate, the direction of the correlation turned out to be negative - with increasing age, the level of knowledge about special-purpose foods decreases significantly.
The observed negative association between age and knowledge of foods for special medical purposes is clinically relevant, particularly in the context of geriatric care. Older patients are at the highest risk of disease-related malnutrition, sarcopenia, and functional decline, while simultaneously demonstrating lower awareness of available nutritional interventions. These findings highlight the need for targeted, age-adapted nutritional education strategies in hospital settings, with particular emphasis on geriatric patients, for whom simplified communication, repeated counseling, and close cooperation with dietitians may be crucial elements of effective malnutrition prevention and lifecare. Such an approach aligns with the concept of lifecare, emphasizing not only the provision of nutritional support, but also patient-centered education as an integral component of comprehensive malnutrition management in older adults.
The most important descriptive statistics regarding knowledge, broken down by gender, are presented in the table (Table 4).
The Shapiro-Wilk test was used to test the normality of the residual distribution. The results are presented in Table 5.
The results of the Shapiro-Wilk test indicate a non-normal distribution of residuals for the knowledge level variable.
The table presents the results of the analysis of equality of variance for the ‘Knowledge’ variable, conducted using Leven’s test (Table 6).
The results of the Leven’s test indicate that the variances of the compared groups were unequal for the ‘Knowledge’ variable.
The Mann-Withney test was used to analyze the significance of differences in knowledge levels (dependent variable) while taking into account gender (independent variable). The results are presented in Table 7.
The results of the study, using the Mann-Withney test, suggest that the level of knowledge does not differ statistically significantly between women and men.
Basic descriptive statistics regarding knowledge, broken down by comorbidities, are presented in Table 8.
The Shapiro-Wilk test was used to test the normality of the residual distribution. The results are presented in Table 9.
Data analysis, conducted using the Shapiro-Wilk test, revealed a non-normal distribution of residuals for the knowledge level variable. Levene’s test was used to analyze the equality of variances for the ‘Knowledge’ variable.
Table 10.
‘Knowledge’ - Leven’s test results (equality of variances).
| p | df2 | df1 | F | Variable | |
| 0,047 | 98 | 1 | * | 4,06 | Knowledge |
The results of the study, based on Leven’s test, indicate a lack of equality of variances between the compared groups in terms of knowledge level.
The Mann-Withney test was used to analyze the significance of differences in knowledge level (dependent variable) while taking into account the presence of comorbidities (independent variable). The obtained results are presented in Table 11.
The Mann-Withney test did not reveal any significant differences in the level of knowledge between people with comorbidities and those without them.
Numerous studies confirm the effectiveness of FSMP in various physiological conditions and individual diseases. The use of ONS for at least 7 days in patients in the preoperative period for gastrointestinal procedures reduces the incidence of infections and the length of hospitalization [19]. A literature review by Tangvik et al. [2020] examined the effects of ONS supplementation in patients with dementia on daily dietary intake, nutritional status, and cognitive and functional function, focusing on malnourished patients. ONS consumption had a positive effect on nutritional status, daily protein and energy intake, but no correlation was detected with improved cognitive or functional function. One study included 65-year-olds classified as at moderate to high risk of malnutrition using the Malnutrition Universal Screening Tool (MUST). Participants were divided into two groups: control and treatment for 180 days. The control group received two servings per day of ONS containing beta-hydroxy-beta-methylbutyrate with dietary counseling or the treatment group received two servings per day of a placebo supplement with dietary counseling. The results clearly established that ONS supplemented with HMB and vitamin D, along with dietary counseling, significantly improved nutritional and functional outcomes in older adults at risk of malnutrition compared with placebo supplementation combined with dietary counseling [11]. Liu et al. [2021] analyzed 22 studies of ONS consumption in patients undergoing hemodialysis (HD) or peritoneal dialysis (PD), who are at high risk of malnutrition due to their disease. The ONS group had significantly higher serum albumin levels, body mass index (BMI), and handgrip strength (HGS) from the beginning to the end of the intervention. No significant differences were observed between groups in terms of lean body mass, phase angle, C-reactive protein concentration, and serum phosphorus and potassium levels. The effectiveness of ONS in elderly patients with anorexia has also been assessed. Their use has been shown to improve appetite to some extent and have a beneficial effect on body weight and food intake. Researchers also suggest a reduction in the incidence of pressure sores and diarrhea, as well as lower treatment costs, but these data should be comprehensively studied [22]. Benefits of ONS consumption have also been observed in malnourished children in developing countries, particularly on growth and weight gain. Adequate nutritional status in children characteristically improves motor and cognitive function in adolescents [23]. Baldwin et al. [2021] suggest that the effects of ONS consumption in selected patient groups should be further investigated, given the unclear benefits of their use, based on 22 literature reviews [24]. Therefore, actions aimed at expanding and shaping the knowledge and awareness of hospitalized patients, but also their medical caregivers, are becoming a priority.
The study’s limitations include the small number of respondents. Interpretation problems were initially caused by questions that respondents answered multiple times.
4. Conclusions
The relationship between age and knowledge of special medical purposes was examined – with increasing age, knowledge in this area significantly decreases. There were no significant differences between gender and the level of knowledge of respondents. There were no significant differences between the presence of comorbidities and the level of knowledge of respondents. The results indicate limited patient knowledge of foods for special medical purposes. Educational efforts in hospitals are necessary to improve patient awareness and the effectiveness of nutritional therapy, as well as preventive measures to improve patient nutritional status. Nutritional interventions must be properly implemented in hospitals to continuously strive to improve the nutritional status of patients and, consequently, improve the effects of treatment. A significant factor in patient awareness of selected ONS is their advertising, which demonstrates how to reach specific groups. In particular, the observed decline in nutritional knowledge with increasing age indicates that geriatric patients should be considered a priority group for targeted, age-adapted nutritional education and interdisciplinary lifecare strategies aimed at effective malnutrition prevention.
Author Contributions
Conceptualization, A.R.; T.L, A.K, A. S.; methodology, A.R., T.L, A.K.; resources: P.S.; formal analysis, A.R., T.L., A.K.; investigation, A.R., A.S..; data curation, A.R.; writing—original draft preparation, A.R.; writing—review and editing, A.K.; T.L, visualization, A.R,; supervision, A.K., T.L., P.S.; project administration, A.K., and P.S,; funding acquisition, A.R, A.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by research subsidy 070015-D020 and the activation of the Doctoral School of the University of Agriculture in Kraków AD12. The scientific team was responsible for all stages of this study.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of the Rector’s Committee for the Ethics of Scientific Research Involving Human Subjects (354/2025 26/01/2026).
Informed Consent Statement
Consent was obtained from the patients for publication of this article.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
Not applicable.
References
- Serón-Arbeloa, C.; Labarta-Monzón, L.; Puzo-Foncillas, J.; Mallor-Bonet, T.; Lafita-López, A.; Bueno-Vidales, N.; Montoro-Huguet, M. Malnutrition Screening and Assessment. Nutrients 2022, 14, 2392. [Google Scholar] [CrossRef]
- World Health Organization. Malnutrition. 1 March 2024. Available online: https://www.who.int/news-room/fact-sheets/ (accessed on 28 December 2024).
- Sobotka, L.; Allison, S.P.; Forbes, A.; Meier, R.F.; Schneider, S.M.; Soeters, P.B.; Stanga, Z.; Van Gossum, A. Basics in Clinical Nutrition, 5th ed.; Galen: Prague, Czech Republic, 2019. [Google Scholar]
- White, J.V.; Guenter, P.; Jensen, G.; Malone, A.; Schofield, M. the Academy Malnutrition Work Group; the A.S.P.E.N. Malnutrition Task Force; the A.S.P.E.N. Board of Directors. Consensus Statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: Characteristics Recommended for the Identification and Documentation of Adult Malnutrition (Undernutrition). J. Parenter. Enter. Nutr. 2012, 36, 275–283. [Google Scholar]
- Saunders, J.; Smith, T. Malnutrition: causes and consequences. Clinical Medicine 2010, Vol 10(No 6), 624–7. [Google Scholar] [CrossRef]
- Bellanti, F.; lo Buglio, A.; Quiete, S.; Vendemiale, G. Malnutrition in Hospitalized Old Patients: Screening and Diagnosis, Clinical Outcomes, and Management. Nutrients 2022, 14, 910. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for Europe. Disease-related malnutrition: a time for action. 26 August 2025. Available online: https://www.who.int/europe/publications/i/item/WHO-EURO-2023-8931-48703-72392.
- Doganay, M; Halil, MG; Kaymak, C; Selek, U; Topcuoglu, MA; Yalcin, S. Expert opinion on the current conceptual, clinical and therapeutic aspects of disease related malnutrition and muscle loss: a multidisciplinary perspective. Front. Nutr. 2025, 12, 1509689. [Google Scholar] [CrossRef]
- Salari, N; Darvishi, N; Bartina, Y; Keshavarzi, F; Hosseinian-Far, M; Mohammadi, M. Global prevalence of malnutrition in older adults: A comprehensive systematic review and meta-analysis. Public Health Pract (Oxf) 2025, 9, 100583. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tseng, H.-K.; Cheng, Y.-J.; Yu, H.-K.; Chou, K.-T.; Pang, C.-Y.; Hu, G.-C. Malnutrition andFrailty Are Associated withaHigherRiskof ProlongedHospitalization and Mortality in Hospitalized Older Adults. Nutrients 2025, 17, 221. [Google Scholar] [CrossRef]
- Huang Chew, S. T.; Chuan Tan, N.; Cheong, M.; Baggs, J. O. G.; Choe, Y.; How How, C.; Chow, W. L.; Yan Ling Tan, C.; Kwan, S. C.; Husain, F. S.; Ling Low, Y.; Thi Thu Huynh, D.; Ling Tey, S. Impact of specialized oral nutritional supplement on clinical, nutritional, and functional outcomes: A randomized, placebo controlled trial in community-dwelling older adults at risk of malnutrition. Clinical Nutrition 2021, 40, 1879e1892. [Google Scholar] [CrossRef] [PubMed]
- Folwarski, M.; Wernio, E. Cost-effectiveness of clinical nutrition. Advances in Clinical Nutrition 2023, vol 18, 1–8. [Google Scholar] [CrossRef]
- Volkert, D.; Beck, A. M.; Cederholm, T.; Cruz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C. C.; Sobotka, L.; van Asselt, D.; Wirth, R.; Bischoff, S. C. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clinical Nutrition 2019, 38, 10–47. [Google Scholar] [CrossRef]
- Grajeta, H. Malnutrition—Causes, consequences and treatment. Bromatol. Chem. Toksykol. 2021, 54, 133–147. [Google Scholar]
- Kłęk, S.; Budnik-Szymoniuk, M.; Cebularski, W.; Czuczwar, M.; Grabowska-Wo’zniak, E.; Koczur- Szozda, E.; Folwarski, M.; Gajewska, D.; Górecka, A.; Jankowski, M.; et al. Standardy ˙ Zywienia Dojelitowego i Pozajelitowego; Krakowskie Wydawnictwo Scientifica Sp.z.o.o.: Karków, Poland, 2019. [Google Scholar]
- Cintoni, M.; Mele, M.C. The Role of Immunonutrition in Patients. Nutrients 2023, 15, 780. [Google Scholar] [CrossRef]
- Mrozikiewicz-Rakowska, B.; Jawie’n, A.; Szewczyk, M.; Sopata, M.; Korzon-Burakowska, A.; Dziemidok, P.; Gorczyca-Siudak, D.; Tochman-Gawda, A.; Krasi’nski, Z.; Rowi’nski, O.; et al. Post˛epowanie z chorym z zespołem stopy cukrzycowej. Pol. J. Wound Manag. 2022, 19, 1–30. [Google Scholar]
- Ghaly, P.; Iliopoulos, J.; Ahmad, M. The role of nutrition in wound healing: an overview. British Journal of Nursing 2021, Vol 30 TISSUE VIABILITY SUPPLEMENT, No 5. [Google Scholar] [CrossRef]
- Wobith, M.; Weimann, A. Oral Nutritional Supplements and Enteral Nutrition in Patients with Gastrointestinal Surgery. Nutrients 2021, 13, 2655. [Google Scholar] [CrossRef]
- Tangvik, R. J.; Bruvik, F. K.; Drageset, J.; Kyte, K.; Hunskar, I. Effects of oral nutrition supplements in persons with dementia: Asystematic review. Geriatric Nursing 2020, 42, 117 123. [Google Scholar] [CrossRef]
- Liu, P. J.; Guo, J.; Zhang, Y.; Wang, F.; Yu, K. Effects of oral nutritional supplements on the nutritional status and inflammatory markers in patients on maintenance dialysis: a systematic review and meta-analysis of randomized clinical trials. Clinical Kidney Journal 2023, vol. 16(no. 11), 2271–2288. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhao, S.; Wu, S.; Yang, X.; Feng, H. Effectiveness of Oral Nutritional Supplements on Older People with Anorexia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2021, 13, 835. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Li, F.; Hannon, B.A.; Hustead, D.S.; Aw, M.M.; Liu, Z.; Chuah, K.A.; Low, Y.L.; Huynh, D.T.T. Effect of Oral Nutritional Supplementation on Growth in Children with Undernutrition: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3036. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, Ch.; Smith, R.; Gibbs, M.; Weekes, E.; Emery, P. W. Quality of the Evidence Supporting the Role of Oral Nutritional Supplements in the Management of Malnutrition: An Overview of Systematic Reviews and Meta-Analyses. Advances in Nutrition Volume 2021, Volume 12(Issue 2), 503–522. [Google Scholar] [CrossRef]
- Gostyńska, A.; Stawny, M.; Dettlaff, K.; Jelińska, A. Clinical Nutrition of Critically Ill Patients in the Context of the Latest ESPEN Guidelines. Medicina 2019, 55, 770. [Google Scholar] [CrossRef]
- Singer, P.; Reintam Blaser, A.; Berger, M. M.; Alhazzani, W.; Calder, P. C.; Casaer, M. P.; Hiesmayr, M.; Mayer, K.; Montejo, J. C.; Pichard, C.; Preiser, J-C.; van Zanten, A. R. H.; Oczkowski, S.; Szczeklik, W.; Bischoff, S. C. ESPEN guideline on clinical nutrition in the intensive care unit. Clinical Nutrition 2019, 38, 48–79. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist; Lobo, D. N.; Martindale, R. G.; Waitzberg, D.; Bischoff, S. C.; Singer, P. ESPEN practical guideline: Clinical nutrition in surgery. Clinical Nutrition 2021, 40, 4745–4761. [Google Scholar] [CrossRef]
- Bartoszewska, L.; Majewska, K.; Matras, P.; Adryjanek, R.; Bana’n, E.; Brodkowicz-Król, M.; Burkacka, M.; Chrzanowska, U.; Fołtyn, I.; Goral, K.; et al. Zywienie Dojelitowe i Pozajelitowe; Wydawnictwo Lekarskie PZWL: Warszawa, Poland, 2023. [Google Scholar]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; Krznari, Z.; Laird, B.; Larsson, M.; Laviano, A.; Mühlebach, S.; Muscaritoli, M.; Oldervoll, L.; Ravasco, P.; Solheim, T.; Strasser, F.; de van der Schueren, M.; Preiser, J-Ch. ESPEN guidelines on nutrition in cancer patients. Clinical Nutrition 2017, 36, 11–48. [Google Scholar] [CrossRef]
- Araszkewicz, A.; Cyganek, K.; Cypryk, K.; Broncel, M. Standards of Care in Diabetes. In T he position of Diabetes Poland – 2025; 2025. [Google Scholar] [CrossRef]
- Iddir, M.; Brito, A.; Dingeo, G.; Fernandez Del Campo, S. S.; Samouda, H.; La Frano, M. R.; Bohn, T. Strengthening the Immune System and Reducing Inflammation and Oxidative Stress through Diet and Nutrition: Considerations during the COVID-19 Crisis. Nutrients 2020, 12, 1562. [Google Scholar] [CrossRef]
- Polak, E.; St˛epie’n, A.E.; Gol, O.; Tabarkiewicz, J. Potential Immunomodulatory Effects from Consumption of Nutrients in Whole Foods and Supplements on the Frequency and Course of Infection: Preliminary Results. Nutrients 2021, 13, 1157. [Google Scholar] [CrossRef] [PubMed]
- Zielińska-Pisklak, M.; Szeleszczuk, Ł.; Kuras, M. The role of vitamin C and zinc in supporting the immune system. Drug in Poland 2013, VOL 23 NR 11-12’13, 271/272. [Google Scholar]
- Krzysik, M.; Biernat, J.; Grajeta, H. The influence of Chosen Nutrients on Immune System Functioning Part II. Immunomodulatory Effects of Vitamins and Trace Elements on the Human Body. Advances in Clinical and Experimental Medicine 2007, 16(1), 123–133. [Google Scholar]
- Lewandowska, A. Immunomodulatory properties of vitamin D and its use in the prevention and treatment of diseases resulting from immune system malfunctions. Interdisciplinary Journal 2023, 3((15)/2023). [Google Scholar] [CrossRef]
- Arribas-López, E.; Zand, N.; Ojo, O.; Snowden, M.J.; Kochhar, T. The Effect of Amino Acids on WoundHealing: ASystematic Review and Meta-Analysis on Arginine and Glutamine. Nutrients 2021, 13, 2498. [Google Scholar] [CrossRef]
- Desneves, K. J.; Todorovic, B. E.; Cassar, A.; Crowe, T. C. Treatment with supplementary arginine, vitamin C and zinc in patients with pressure ulcers: A randomised controlled trial. Clinical Nutrition 2005, Volume 24(Issue 6), 979–987. [Google Scholar] [CrossRef] [PubMed]
- Cheshmeh, S.; Hojati, N.; Mohammadi, A.; Rahmani, N.; Moradi, S.; Pasdar, Y.; Elahi, N. The use of oral and enteral tube- fed arginine supplementation in pressure injury care: A systematic review and meta- analysis. Nursing Open. 2021, 9, 2552–2561. [Google Scholar] [CrossRef]
- Chu, A. S.; Delmore, B. Arginine: What You Need to Know for Pressure Injury Healing. ADVANCES IN SKIN & WOUND CARE 2021, 34, 630–6. [Google Scholar]
- Elahi, N.; Mojdeh, S.; Poordad, A. The effect of fish oil on improvement of first stage bed sore. Iranian Journal of Nursing and Midwifery Research | May-June 2012 2012, Vol. 17 |(Issue 4). [Google Scholar]
- Sadeghi, S. S.; Azami, H.; Borzou, S. R.; Bashar, F. R.; Tapak, L.; Haddadi, R. Evaluation of the effect of fish oil in the prevention of pressure ulcers in patients admitted to the intensive care unit. Contemporary Clinical Trials Communications 2023, 32, 101063. [Google Scholar] [CrossRef]
- Dospra, M.; Pavlou, P.; Papageorgiou, S.; Varvaresou, A. Recent Studies on the Healing Properties of Eicosapentaenoic Acid. Appl. Sci. 2024, 14, 5884. [Google Scholar] [CrossRef]
- Uzogara, S. G. Underweight, the Less Discussed Type of Unhealthy Weight and Its Implications: A Review. American Journal of Food Science and Nutrition Research 2016, 3(5), 126–142. [Google Scholar]
- Kotynia, Z.; Szewczyk, P.; Tuzikiewicz-Gnitecka, G. Żywienie pacjentów w szpitalach, kontrola i audyt. 2018, Nr 4. [Google Scholar]
- Bator, K. B. Nutrition knowledge of healthcare staff. Nursing and Public Health 2017, 7(3), 177–187. [Google Scholar] [CrossRef]
- Mogiłko, N.; Zarzeczny, P. The role of a dietitian in prehabilitation. Advances in Clinical Nutrition 2024, Volume 19, 100–106. [Google Scholar]
Figure 1.
Comorbidities of respondents.
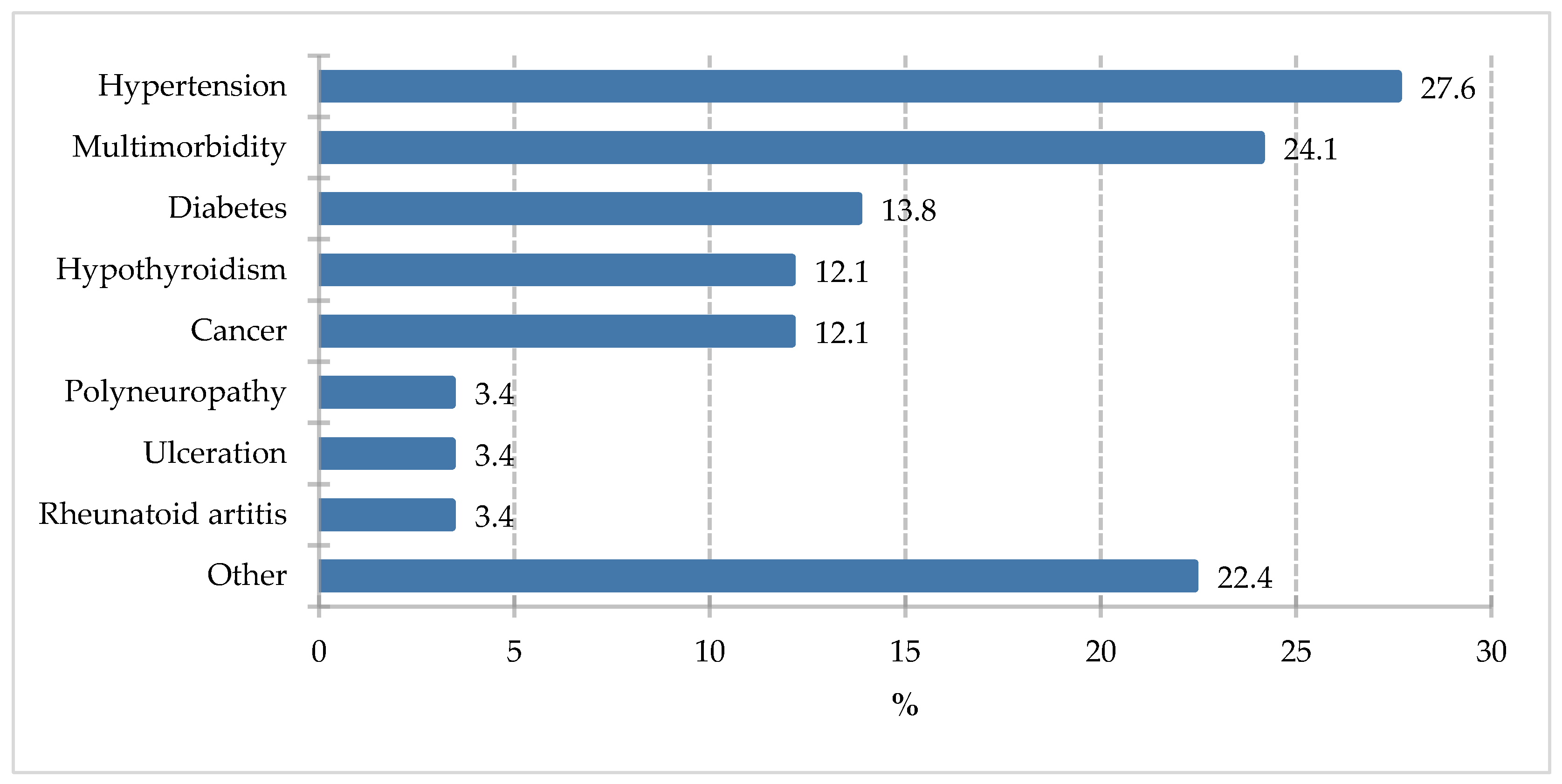
Figure 2.
Percentage of respondents who answered the question 100% „Do you know the following concepts?”.
Figure 2.
Percentage of respondents who answered the question 100% „Do you know the following concepts?”.

Figure 3.
Percentage of respondents who answered the question 100% „Which ingredients would you pay attention to in your diet if you were to unintentionally lose significant weight in a short period of time?”.
Figure 3.
Percentage of respondents who answered the question 100% „Which ingredients would you pay attention to in your diet if you were to unintentionally lose significant weight in a short period of time?”.
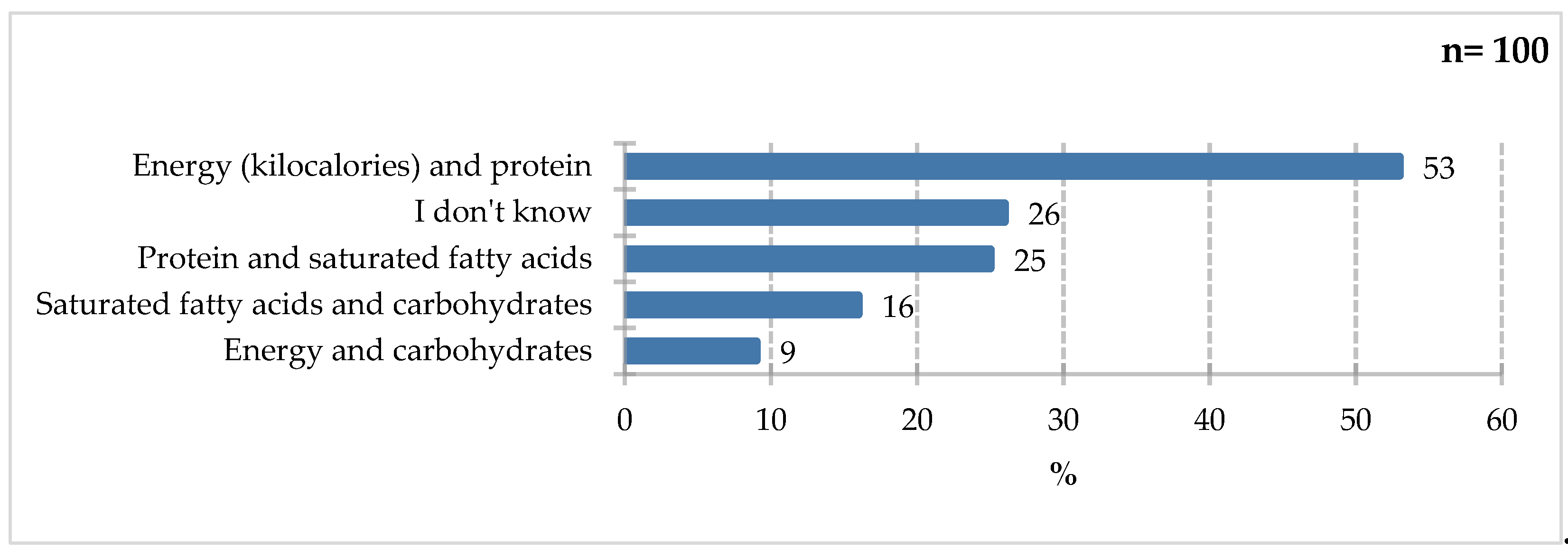
Figure 4.
Percentage of respondents who answered the question 100% „Do you know companies that produce products for special medical purposes?”.
Figure 4.
Percentage of respondents who answered the question 100% „Do you know companies that produce products for special medical purposes?”.
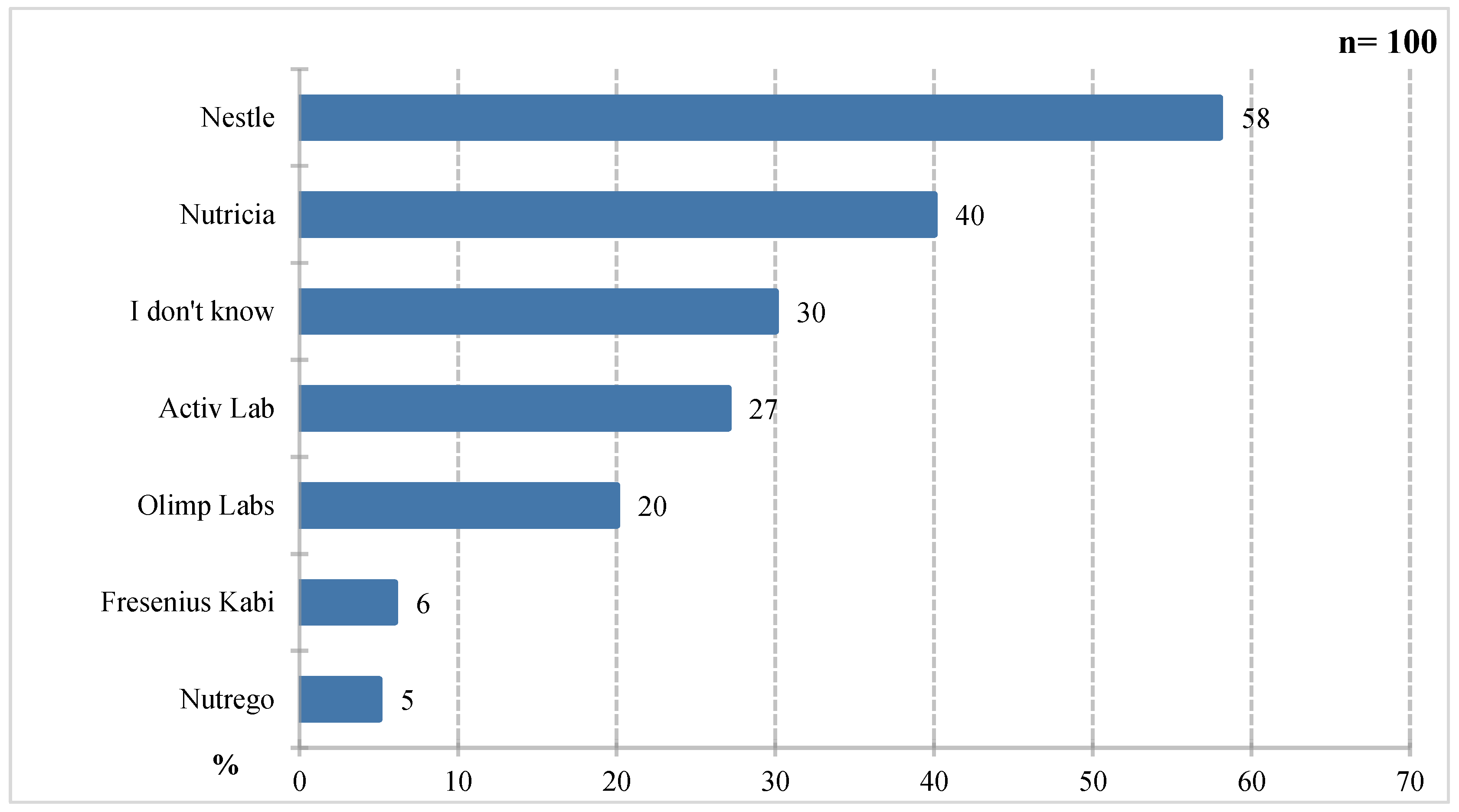
Figure 7.
Percentage of respondents who answered the question100% „Which ingredients would you pay attention to when choosing a product for people with diabetes?”.
Figure 7.
Percentage of respondents who answered the question100% „Which ingredients would you pay attention to when choosing a product for people with diabetes?”.
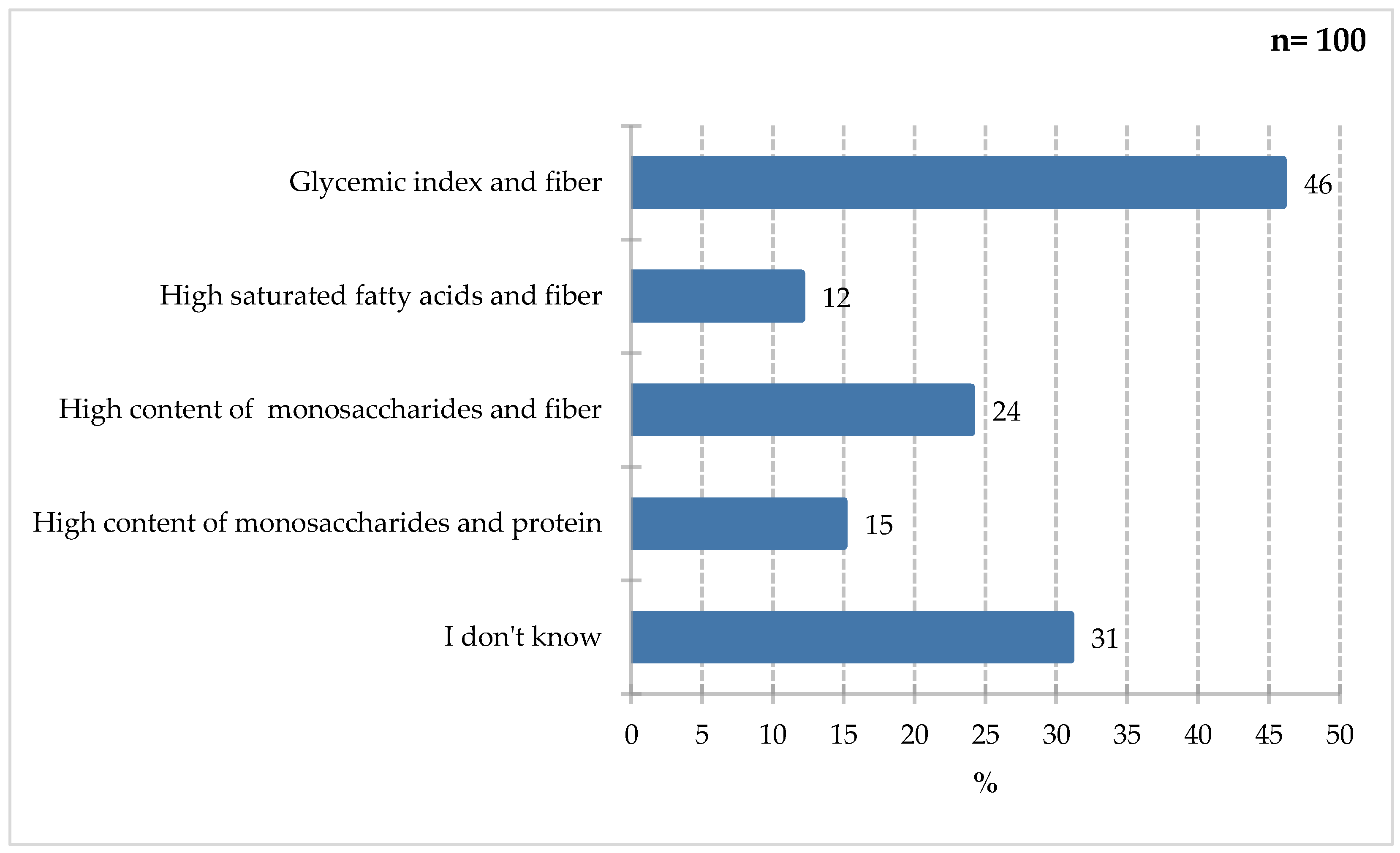
Figure 8.
Percentage of respondents who answered the question 100% „Do you know any immunomodulatory ingredients that can improve the body’s immunity?”.
Figure 8.
Percentage of respondents who answered the question 100% „Do you know any immunomodulatory ingredients that can improve the body’s immunity?”.
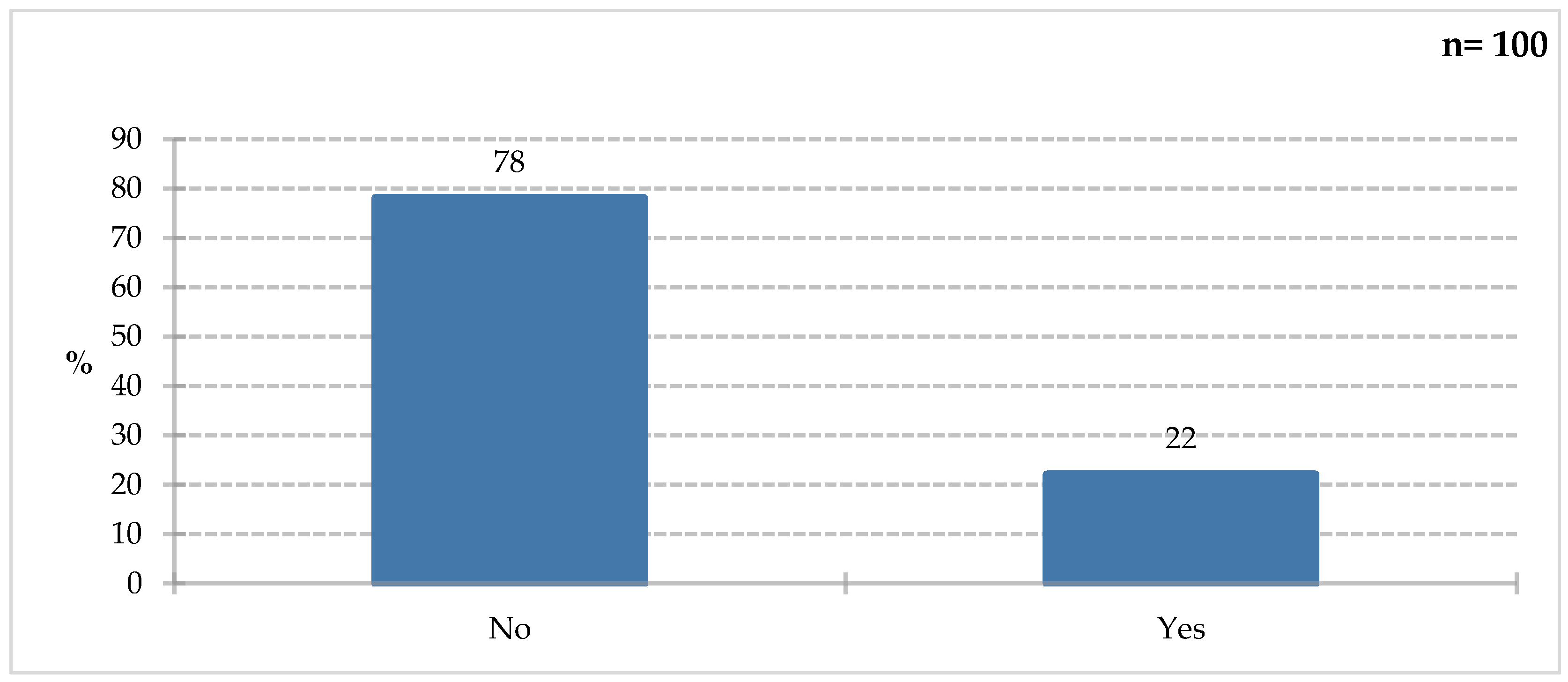
Figure 9.
Percentage of respondents who answered the question 18% „If you answered YES in question 7, please specify which ingredients”.
Figure 9.
Percentage of respondents who answered the question 18% „If you answered YES in question 7, please specify which ingredients”.
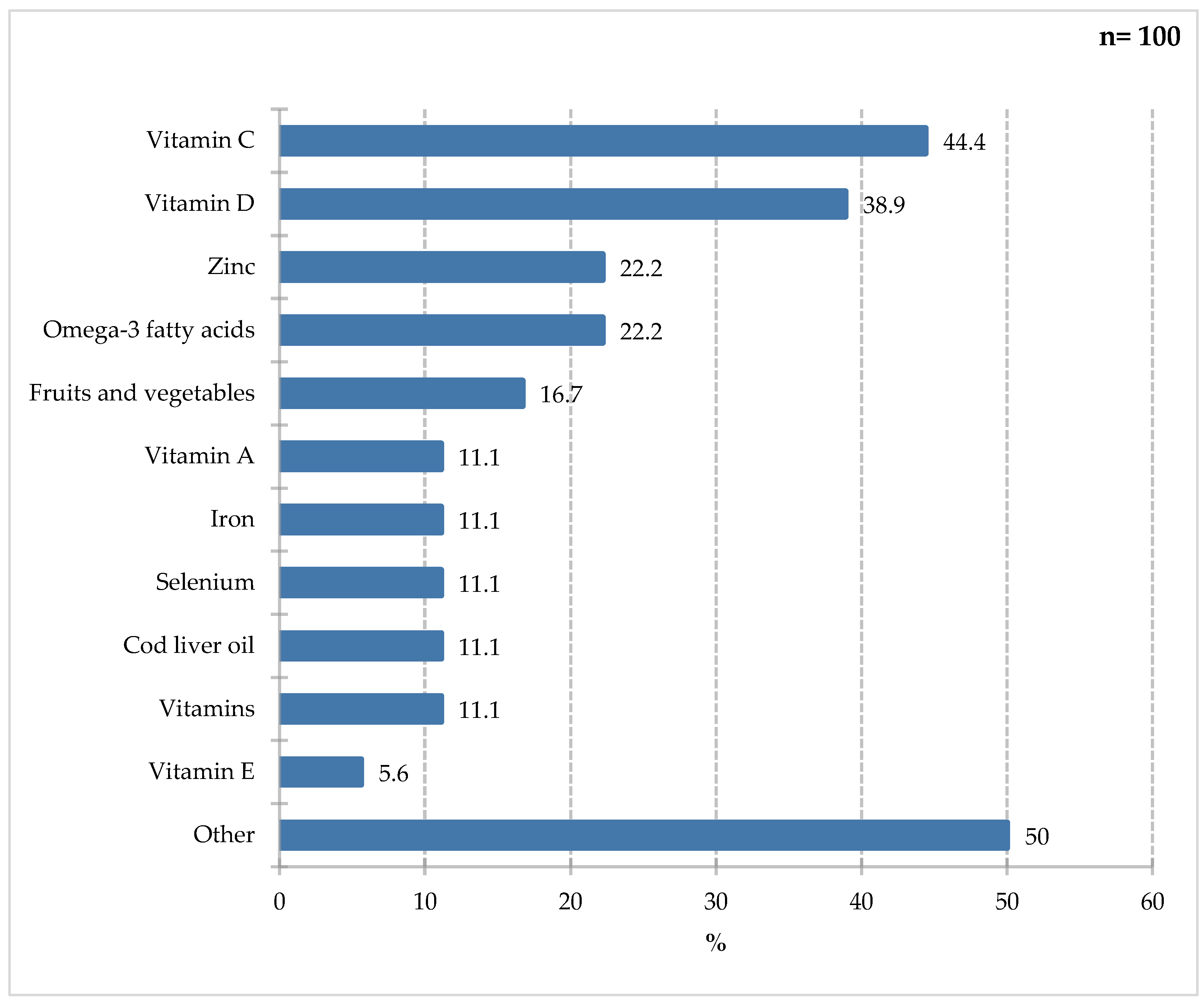
Figure 10.
Percentage of respondents who answered the question 100% „Which ingredients would you recommend to people with difficult-to-heal wounds and pressure sores?”.
Figure 10.
Percentage of respondents who answered the question 100% „Which ingredients would you recommend to people with difficult-to-heal wounds and pressure sores?”.
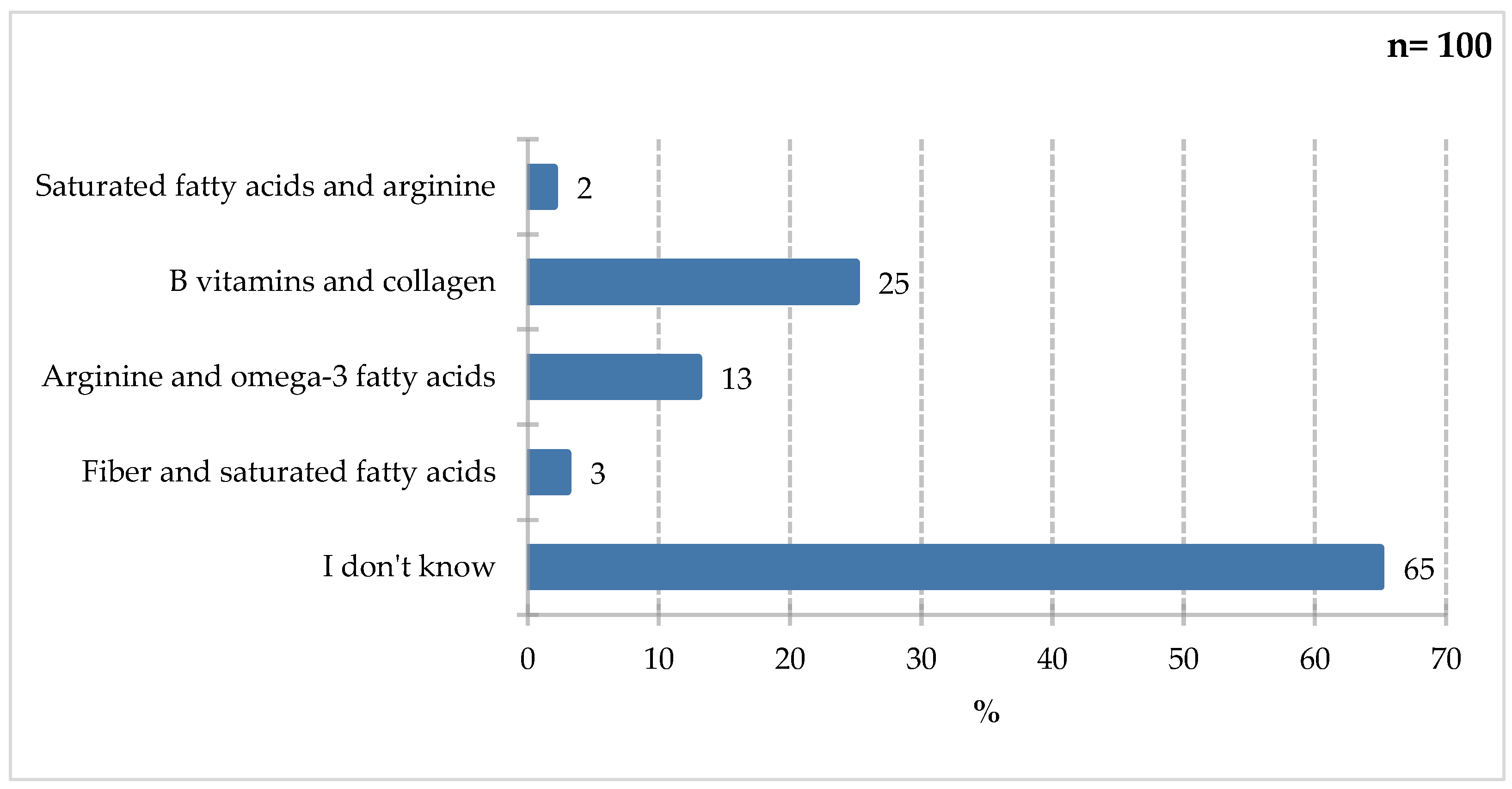
Figure 11.
Percentage of respondents who answered the question 98% „Which specialist would you turn to for advice on the selection of FSMP?”.
Figure 11.
Percentage of respondents who answered the question 98% „Which specialist would you turn to for advice on the selection of FSMP?”.
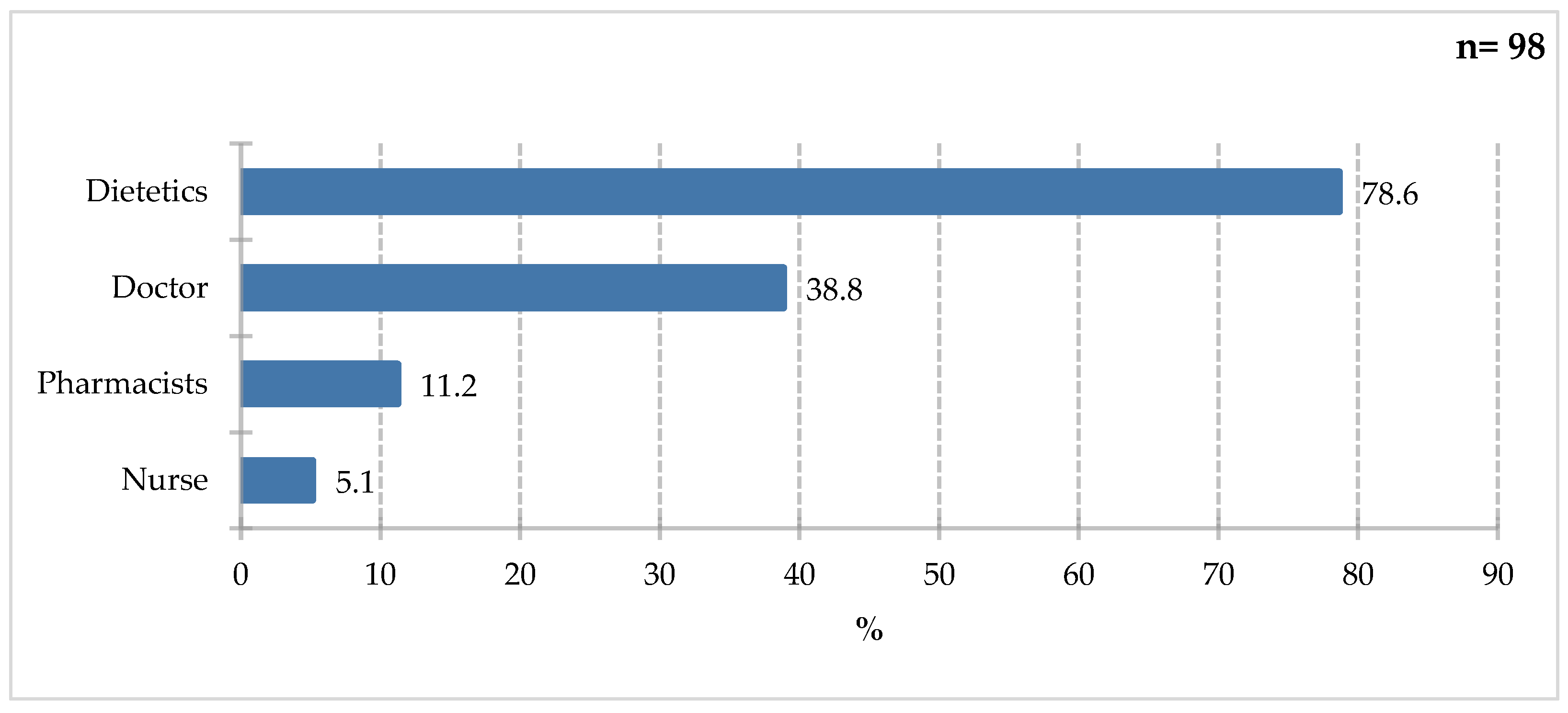
Table 1.
Basic characteristics of the respondents.
| n(%) | n | 99. |
| 99 | Gender | |
| 53 (53,5%) | Female | |
| 46 (46,5%) | Male | |
| 98 | Age | |
| 19 (19,4%) | 18-35 | |
| 38 (38,8%) | 36-55 | |
| 25 (25,5%) | 56-70 | |
| 16 16,3%) | over 70 |
Table 3.
Results of Spearman’s rho correlation analysis.

Table 4.
Results of descriptive statistics with the division into the ‘Gender’ variable.
| IQR | Maks. | Min. | Me | SD | M | N | Gender | |
| 4,00 | 7,00 | 0,00 | 5,00 | 2,06 | 4,23 | 53 | K | Knowledge |
| 2,75 | 7,00 | 1,00 | 3,00 | 1,55 | 3,57 | 46 | M |
Table 5.
‘Knowledge’ - analysis of the normality of the distribution of residuals.

Table 6.
‘Knowledge’ - Results of Leven’s Test of Equality of Variances.

Table 7.
Results of the Mann-Whitney test - significance of differences between two independent groups in terms of the ‘Knowledge’ variable, independent variable: ‘Gender’.
Table 7.
Results of the Mann-Whitney test - significance of differences between two independent groups in terms of the ‘Knowledge’ variable, independent variable: ‘Gender’.
| rrb | p | U | Variable |
| 0,20 | 0,081 | 1,465,00 | Knowledge |
Table 8.
‘Knowledge’ - descriptive statistics, broken down by the grouping variable ‘Comorbidities yes or no’.
Table 8.
‘Knowledge’ - descriptive statistics, broken down by the grouping variable ‘Comorbidities yes or no’.
| IQR | Maks. | Min. | Me | SD | M | N | Comorbidities yes or no | |
| 2,00 | 7,00 | 0,00 | 4,00 | 1,70 | 3,76 | 42 | No | Knowledge |
| 4,00 | 7,00 | 1,00 | 3,50 | 1,98 | 4,00 | 58 | Yes |
Table 9.
‘Knowledge’ - Results of the Shapiro-Wilk test for the normality of the residual distribution.
Table 9.
‘Knowledge’ - Results of the Shapiro-Wilk test for the normality of the residual distribution.
| p | W | Variable | |
| 0,001 | *** | 0,95 | Knowledge |
Table 11.
Mann-Withney Test Results - Significance of Differences Between Two Independent Groups in the ‘Knowledge’ Variable, Independent Variable: ‘Comorbidities Yes or No’.
Table 11.
Mann-Withney Test Results - Significance of Differences Between Two Independent Groups in the ‘Knowledge’ Variable, Independent Variable: ‘Comorbidities Yes or No’.
| rrb | p | U | Variable |
| -0,05 | 0,671 | 1,157,50 | Knowledge |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



