Submitted:
06 February 2026
Posted:
09 February 2026
You are already at the latest version
Abstract
Meridian theory is central to Traditional Chinese Medicine (TCM), yet contemporary explanations often oscillate between anatomical reductionism and non-operational metaphor, limiting hypothesis generation and study design. This Perspective proposes an “extended meridian waveguide” framework that treats meridians as distributed, lossy, coupled multiphysics pathways rather than a single discrete anatomical conduit. The model operationalizes meridian condition using a compact state vector spanning measurable proxy classes (mechanical, electrical/impedance, temperature, biochemical/metabolic proxies, interstitial milieu, fascial glide, neural excitability, pressure, perfusion/flow, and context-dependent coupling), and represents pathway organization as a weighted graph whose edges encode state-dependent propagation and attenuation. Interventions are formalized as defined inputs that perturb local state and reweight adjacent couplings, yielding predictions expressed as propagation signatures (anisotropy along vs across a corridor), phase/lag structure, junction-dependent routing switches, and mode-specific proxy patterns across modalities. The paper outlines staged, minimal validation workflows emphasizing differential signatures and explicit disconfirmation criteria rather than binary “effect/no effect” comparisons. Optional modality axes are modular and removable without altering the core model’s testable claims.
Keywords:
meridian theory
; acupuncture theory
; mechanism research
; systems modeling
; measurement proxies
1. Introduction
Meridian theory is central to Traditional Chinese Medicine (TCM), yet contemporary explanations often oscillate between (i) anatomical reductionism that cannot accommodate system-level patterning and (ii) non-falsifiable metaphors that are difficult to operationalize in research and education. This gap is particularly visible when attempting to relate meridian phenomena to measurable physiology without forcing a one-to-one mapping onto discrete structures.
This Perspective article proposes a systems-oriented model—an “extended meridian waveguide”—that treats meridians as distributed, multi-parameter conduction pathways. The aim is not to replace classical theory, but to provide a compact, testable language that can bridge meridian concepts to modern biophysics and systems science, enabling clearer hypotheses, experimental designs, and potentially clinically relevant, testable predictions.
2. Scope and Non-Goals
This paper defines an operational state vector for meridian condition, models meridians as coupled multiphysics pathways represented by a weighted graph, and provides testable, measurement-linked predictions together with a staged validation roadmap. It does not claim to have proven meridians as a single discrete anatomical structure, does not make treatment-efficacy claims, does not introduce exotic or nonstandard physics, and does not report any personal data or personal protocols. The evidence and claim posture is tiered: grounded biophysical facts are cited (Tier A), model definitions are stated as explicit modeling choices (Tier B), mechanistic couplings are framed as hypotheses (Tier C), and predictions are expressed as measurable signatures that could support or falsify specific components (Tier D).
3. Prior Hypotheses and Partial Models
Several lines of work motivate treating meridians as distributed pathways rather than single conduits. Connective-tissue / fascia-based accounts link acupoints and meridian trajectories to connective tissue planes and their mechanical signaling capacity1-4.
Separately, anatomical work describing a widespread interstitial fluid-filled network (the “interstitium”) has prompted commentary on whether interstitial pathways could contribute to at least some meridian-related phenomena, without requiring a one-to-one structural mapping5,6.
In parallel, modern bioelectricity research shows that tissues support endogenous voltage/ionic networks capable of long-range coordination and state-dependent responses, providing a conservative rationale for including an electrochemical/impedance axis (E) as a candidate state variable7.
These threads do not, by themselves, resolve the meridian question; instead, they justify an integrative modeling approach in which multiple coupled variables can propagate and interact along preferential tissue pathways.
Additional hypotheses in the meridian literature have proposed candidate anatomical or physical substrates, including the primo vascular system (Bonghan ducts/vessels) as a potential infrastructural correlate of meridian pathways10. Review-level syntheses continue to emphasize heterogeneity across reported correlates (e.g., thermal and impedance patterns) and the lack of a single definitive conduit, supporting the view that meridian phenomena may be multifactorial11,12. Definitional work has framed meridians as distal tissue tracts whose properties change with organ state, providing a modern tissue-based starting point that an integrative state-vector approach can extend13.
Importantly, the present framework takes a conservative stance relative to coherence- or quantum-field formalisms. While some models attempt to formalize long-range coordination using field/coherence or quantum-inspired constructs14, the waveguide model here is intentionally classical and lossy, using measurable tissue-state proxies (mechanics, impedance, temperature, perfusion, timing) and making no claim of nondissipative transmission or nonstandard physics.
Classical-doctrine correspondence (brief): In classical TCM, pathway concepts such as the sinew channels (jingjin), network vessels (luo), and the “interior-exterior” coupling of zang-fu function with channel behavior describe a layered, distributed system rather than a single conduit. The waveguide model is offered as a translation layer: it does not redefine Qi, but provides testable proxy variables that can be used to relate classical descriptions of propagation, constraint, and phase to measurable tissue-state changes, including the need to consider cultural/chronological dimensions when translating classical constructs15.
4. Core Proposal
In this paper, we operationalize the term “meridian” as a distributed pathway that can support propagation, filtering, and coupling of multiple physical variables (“state variables”) across tissue domains.
Operational note: this does not assert a single discrete conduit. Rather, we treat meridian behavior as an emergent, lossy “waveguide” formed by overlapping tissue layers (e.g., fascia, interstitium, neurovascular bundles, connective tissue planes, and fluid/ionic microenvironments) that can transmit and transform perturbations.
The model uses a state vector to represent the local meridian condition at a point (or segment) and allows interventions (needling, manual therapy, heat, pressure, movement, electrical stimulation, light, and environmental inputs) to be expressed as perturbations of that state vector. In this framework, the clinically observed “meridian response” is modeled as propagation/coupling of perturbations across the network.
5. Model Formalism
5.1. State Vector and Coupling Terms
We define a state vector S(x,t) along a 1-D curvilinear coordinate x that follows a meridian-aligned pathway segment:
S(x,t) = [M, E, Θ, Φ, I, F, N, P, V, C]
where: M = effective mechanical compliance/strain state; E = effective electrical/impedance state (including ionic conductance proxies); Θ = temperature; Φ = biochemical/metabolic state proxy; I = interstitial/ionic milieu (e.g., extracellular fluid composition and hydration-related proxies); F = fascial glide/viscoelastic friction proxy; N = neural excitability proxy; P = interstitial/compartment pressure proxy (including lymphatic congestion proxies); V = perfusion/flow proxy (microcirculation/vascular flow); C = coupling strength between layers (mechanical–electrical–fluid–neural), treated as a context-dependent parameter rather than an independent “energy” variable.
Optional axes (A/O/B) are presented only as non-required extensions for groups that already collect those modalities. The core framework stands on M/E/Θ/Φ/I/F/N/P/V with coupling C and does not require optical, magnetic, or other additional modality claims. If reviewers or readers reject A/O/B, they can be removed without altering the core definitions, predictions, or test workflow.

Table 1.
State-vector components and example measurable proxies (illustrative, non-exhaustive).
| Component | Meaning (model) | Example measurable proxies (illustrative) |
|---|---|---|
| M | Mechanical compliance/strain state | Elastography/strain; stiffness; ROM-linked stiffness |
| E | Electrical/impedance state (ionic conductance proxies) | Skin impedance/admittance; galvanic response; bioimpedance |
| Θ | Temperature | Thermometry; thermography; local skin temperature gradients |
| Φ | Biochemical/metabolic state proxy | Metabolic surrogates (context-dependent); oxygenation/lactate proxies (if available) |
| I | Interstitial/ionic milieu (ECF composition/hydration-related proxies) | Hydration proxies; edema tendency; interstitial surrogates |
| F | Fascial glide/viscoelastic friction proxy | Ultrasound fascial sliding; shear-wave measures; glide tests |
| N | Neural excitability proxy | Pressure sensitivity thresholds; reflex/excitability surrogates; EMG tone (if available) |
| P | Interstitial/compartment pressure proxy (incl. lymphatic congestion proxies) | Circumference/edema; tissue turgor; lymph-related surrogates |
| V | Perfusion/flow proxy | Capillary refill; Doppler microflow; near-infrared perfusion surrogates |
| C | Context-dependent coupling strength across layers (not an energy variable) | Cross-modal lag/phase relations; coupling indices from multi-proxy time series |
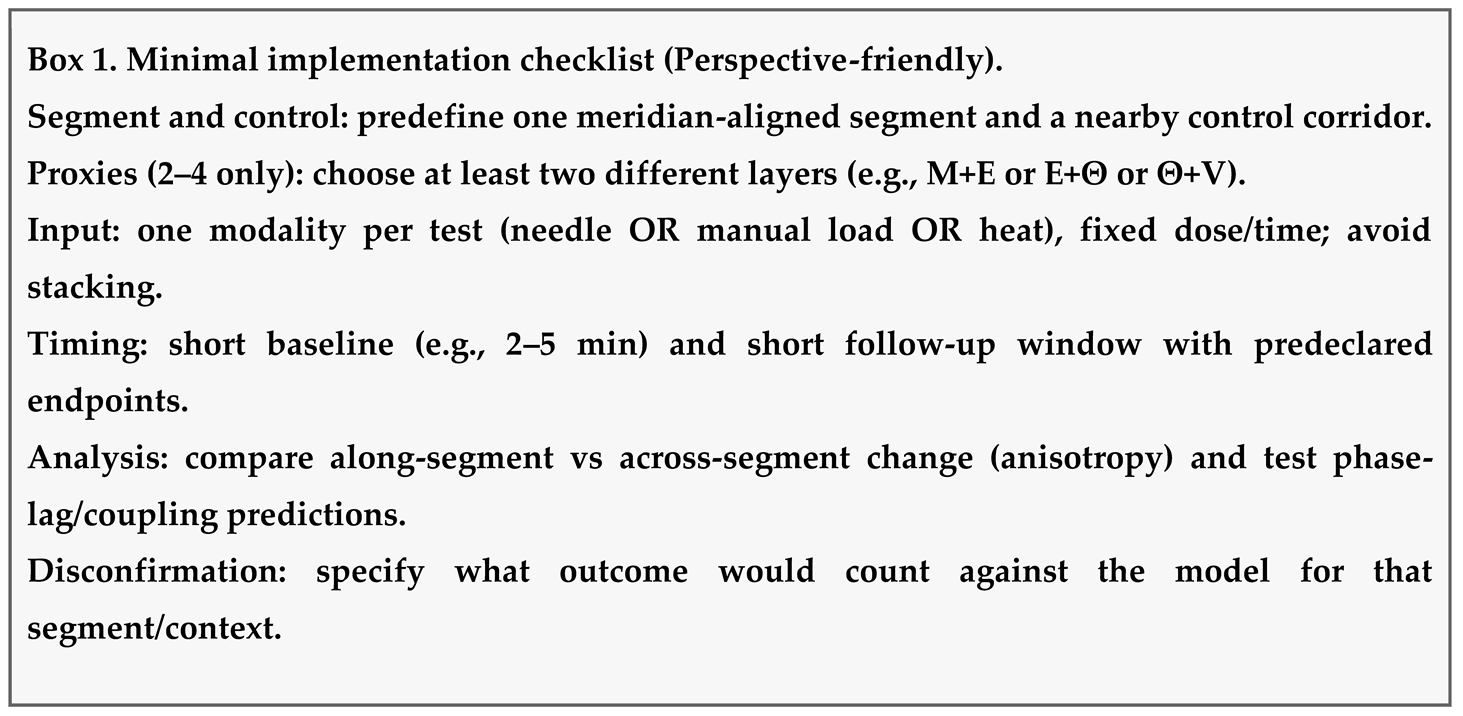
5.1.1. Operationalization: Minimal Workflow for Testing Predictions
Figure 2. Minimal operationalization workflow for testing predictions.
(1) Segment selection: choose one pathway segment x ∈ [x0,x1] and a nearby non-meridian control corridor.
(2) Baseline window: record a short baseline for 2–4 proxies spanning different layers (e.g., M+V or E+Θ).
(3) Defined input u(t): apply a single, well-specified perturbation (manual load, needle, heat) with fixed dose/time.
(4) Readout: test whether predicted directionality + coupling holds (e.g., expected phase lag between M→E→V, or differential propagation/attenuation along vs across the segment). Primary outcome is pattern structure (propagation/attenuation/coupling), not a binary “works/doesn’t work.”
Coupling is expected: changes in one component can drive changes in others. For example, mechanotransduction links mechanical deformation to ionic and signaling changes through mechanosensitive channels (e.g., Piezo-family channels), providing a plausible bridge between manual/needling stimuli and electrochemical responses8.
5.2. Minimal Segment Formalism (Optional)
For a single meridian segment, define a 1-D coordinate x along the dominant pathway direction (‖). A minimal continuous-state representation can use four core fields: u(x,t) mechanical displacement/strain proxy, V(x,t) effective ionic/electrical potential state, T(x,t) temperature, and P(x,t) fluid-pressure proxy (interstitial/blood/lymph).
A conservative physical feature is anisotropy: transmission differs along the line versus across it. This can be expressed as direction-dependent parameters (e.g., mechanical impedance Z_mech(‖) vs Z_mech(⟂), and electrical conductivity σ‖ vs σ⟂).
Dynamics can be written generically as coupled, damped wave-and-diffusion behavior with state-dependent coefficients, for example: ∂tX = A(x,X)X + D(x,X)∂xxX + B(x)·u_in(t), where X=[u,V,T,P]ᵀ and u_in(t) is a localized intervention input. The manuscript’s state-vector/graph view is the network (discretized) counterpart of this segment picture.
If vibration/sonic inputs are considered (optional axis A), the same segment can be characterized by a frequency response (transfer function) H_mech(f) describing which bands transmit with low attenuation versus reflect at impedance mismatches (nodes).
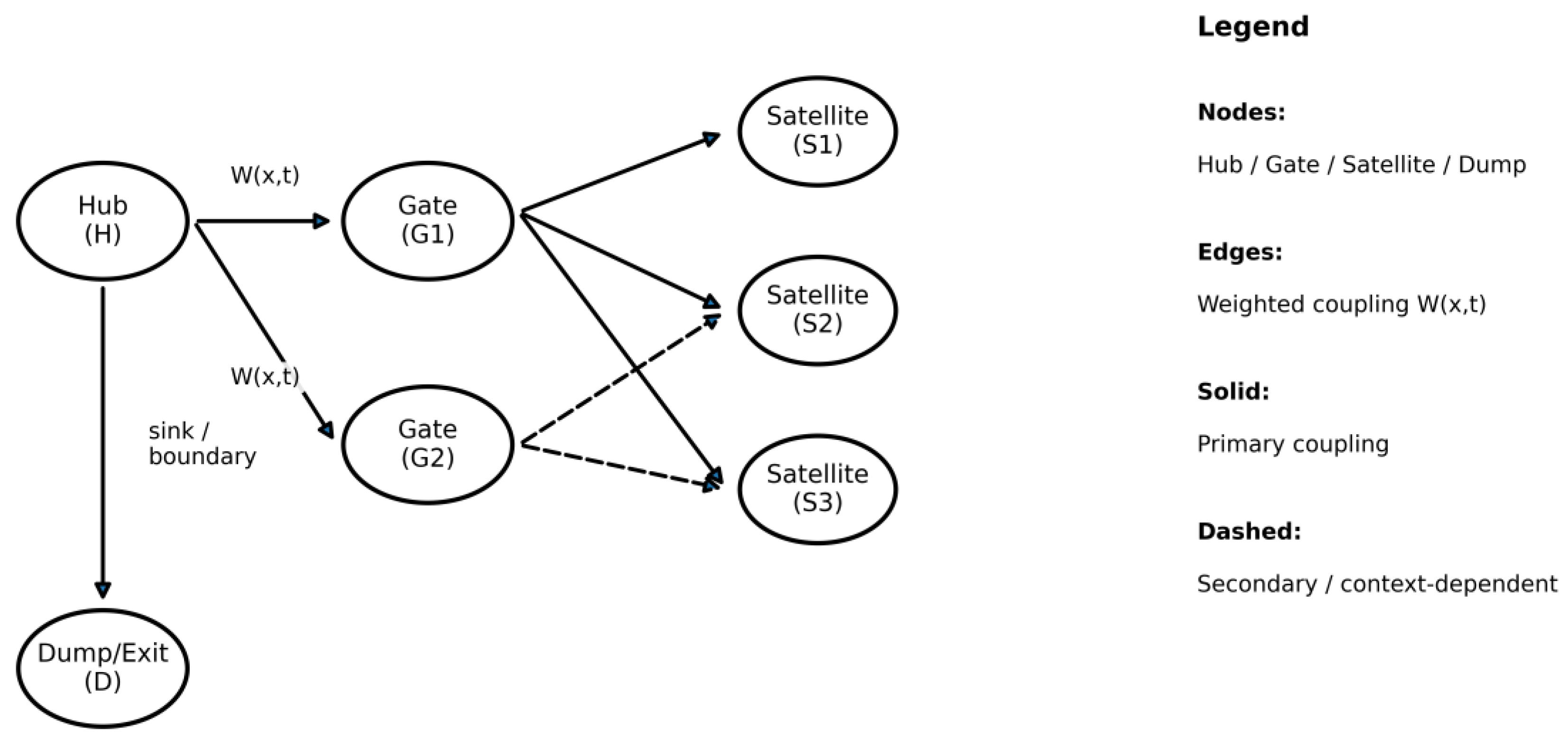
5.3. Network Representation: Meridians as Graph Waveguides
The model treats the meridian system as a weighted graph G(V,E), where vertices represent key anatomical/functional nodes (acupoints, junctions, segmental gates, myofascial intersections) and edges represent waveguide segments. Edge weights encode local state-vector-dependent conductance/attenuation for each variable, allowing the same pathway to carry multiple coupled “signals.”
Figure 1. Meridian network as a functional weighted graph (schematic).
5.3.1. Practical Estimation of Edge Weights (Data-Driven, Non-Circular)
To avoid circular inference, edge weights should be estimated from independent proxy measurements rather than from treatment outcomes. A practical approach is: (i) choose one variable family (e.g., E via skin impedance) and one stimulus (fixed input), (ii) measure baseline and input-evoked changes at a small set of nodes along the segment, (iii) fit a simple attenuation/transfer model along the path (e.g., exponential decay or discrete transfer between adjacent nodes), and (iv) repeat under a second operating point (e.g., after controlled heat or movement) to test state dependence. Weights can then be generalized to multi-variable edges by repeating this process for different proxies (M, Θ, V) and treating cross-modal coupling as an additional fitted term.
This graph formalism is intended to be consistent with commonly reported practice phenomena: (i) distal effects via long-range propagation, (ii) switching between pathways via gating at junctions, (iii) resonance-like amplification when periodic inputs match local tissue dynamics, and (iv) “pattern” shifts when a small number of high-centrality nodes are perturbed.
5.4. Why a “Waveguide” Analogy Is Useful
In wave physics, a waveguide supports propagation of signals and information while shaping them through impedance, dispersion, reflection, and coupling between modes. Translating this concept to meridians provides a disciplined vocabulary for describing how interventions can produce both local and distal responses without requiring a single anatomical conduit.
Connective tissue planes and fascia form continuous body-wide networks; contemporary fascia reviews emphasize both continuity and functional diversity across layers 2,3. Acupuncture research has also proposed relationships between acupoints/meridians and connective tissue planes, consistent with a distributed pathway concept 4. The waveguide analogy does not claim that meridians are literally electromagnetic waveguides; rather, it states that meridian function can be modeled as guided propagation in a coupled multiphysics medium.
5.5. Interventions as State Perturbations
An intervention can be formalized as a time-varying input u(t) that perturbs the meridian state vector S(x,t) at a node (acupoint/junction) or along an edge (segment). “Why it works” is the consequence of shifting variables that set local conductance/attenuation (effective impedance), coupling between variables (mode coupling), and routing preference through the network (which edges become high-gain vs low-gain at that moment).
State variables are proxy classes rather than single structures: mechanical stiffness/strain (M), fascial glide/shear compliance (F), ionic/electrical impedance (E), temperature gradients (Θ), perfusion/flow proxies (V), and regulatory phase (Φ; timing, autonomic bias, and memory). Optional axes capture additional modalities when relevant: acoustic/sonic or vibration coupling/entrainment (A), optical dose/exposure (O), and magnetic/EM coupling (B). The operating point is the current configuration of these variables along the path connecting the stimulated site to the observed distal effect. For reviewers preferring a strictly conservative stance, A/O/B can be omitted without altering the falsifiable routing and state-dependence claims of the core vector.
The model predicts two familiar observations: state-dependent response (the same point can behave differently across contexts because edge weights change), and threshold/hysteresis effects (small inputs can trigger large distal shifts when a segment crosses a coupling threshold, while repetition can show diminishing returns if the system adapts by restoring impedance or re-routing).
Interventions “give a result” when they reduce attenuation and/or increase coupling so the perturbation can propagate beyond the local tissue domain. Examples: ΔM↓ and ΔF↑ can redistribute strain/fluid shifts across tissue planes; ΔΘ↑ can shift ΔV and thereby influence ΔE; and ΔP (posture/movement) can alter boundary conditions, changing which pathway becomes the dominant route for propagation.
u(t) has a dose geometry: amplitude, duration, waveform (continuous vs pulsed), and spatial support (point-local vs segmental). Illustrative target sets: needling/rotation/electrostimulation → ΔM/ΔF with secondary ΔE/ΔΦ; heat/moxibustion → ΔΘ with downstream ΔV; manual therapy/tuina/cupping → ΔM/ΔF/ΔV; movement/posture → ΔP with broad M/F changes; topical/chemical inputs → boundary ΔE/ΔΦ; vibration/sonic stimulation → ΔA with entrainment-linked ΔΦ and mechanical coupling (ΔM/ΔF); photobiomodulation/light → ΔO with downstream ΔV/ΔE/ΔΦ; and magnetic/PEMF inputs → ΔB with downstream ΔE/ΔV/ΔΦ. These imply distinct measurable signatures.
This view explains non-response (wrong variable targeted, insufficient dose, resistive operating point), delayed response (Φ-dominated timing/threshold crossing), and distal specificity (propagation follows the temporarily highest-gain route). It turns the model into a reasoning scaffold: explicitly choose variable targets and network location, then evaluate by measuring proxy changes locally and distally and comparing the propagation pattern to the predicted routing.
6. Testable Predictions and Minimal Validation Roadmap
The model is intentionally structured to enable falsifiable predictions. Examples include:
Illustrative worked example (one segment, one input, two proxies)
Select a forearm segment aligned with a chosen meridian trajectory and a matched nearby control corridor. Record baseline skin impedance (E proxy) and superficial temperature (Θ proxy) for 3 minutes at three points along the segment and three matched control points. Apply a single standardized thermal input at the proximal node (heat pad with fixed temperature and duration). Prediction: Θ will change locally in both corridors, but E will show a stronger along-segment propagated signature (greater distal change and/or a consistent lag pattern) in the meridian-aligned corridor if the segment’s coupling C and glide F are in a permissive operating state. Disconfirmation for this context: no repeatable along-segment advantage over control across sessions and operating states.
(1) State-dependent conduction: Distal effects should depend on local operating point (“impedance”) states. For a given acupoint, distal outcomes will be stronger when the intervening segment shows higher fascial glide (F) and lower mechanical stiffness (M).
(2) Mode-coupling signatures: Interventions that primarily modulate Θ (heat), O (light), A (vibration/sonic), or B (magnetic/EM) should show distinguishable distal signatures from those primarily modulating M/E (manual/needling), measurable via different proxy combinations (e.g., thermography vs impedance vs optical-dose logs vs vibration/field parameters).
(3) High-centrality nodes and junction gating: A small subset of nodes with high graph centrality should disproportionately influence global patterns; perturbing these nodes should shift multiple downstream proxies and can reveal “routing switches” at junctions.
(4) Phase/timing dependence: Outcomes should vary with N and Φ (autonomic and timing state). The same perturbation applied under different phase conditions (e.g., different baseline tone or after movement/heat) should change propagation distance and distal proxy timing.
(5) Cross-modality convergence: Two different interventions that produce similar ΔS (similar changes in the state vector) should yield similar distal proxy patterns, even if the physical modality differs (e.g., manual vs thermal vs vibration), supporting the state-vector abstraction.
(6) Falsification anchor: If distal proxy changes do not show state dependence, mode-specific signatures, or junction-dependent routing in repeated controlled tests, the waveguide-graph model (or the chosen S components) must be revised or rejected for that context.
A minimal validation approach could begin with a single meridian segment, collecting multimodal proxies (e.g., elastography/strain for M, skin impedance for E, thermography for Θ, perfusion imaging for V) before/after a standardized perturbation, then testing whether propagation aligns with predicted graph routing and state dependence.
As one example of an empirically anchored proxy pair for the E-axis, in vivo impedance measurements have been linked to collagenous bands / echogenic connective-tissue features in some meridian segments 9.
7. Practice-Oriented Translation for Acupuncture Practice
This framework is intended to help practitioners translate meridian concepts into a practical, non-prescriptive way of thinking about where an intervention is applied, what it is intended to influence, and how to describe change over time. It does not replace classical diagnosis or point selection.
7.1. What an Acupuncturist Can Use Immediately
A common language to explain treatment targets to recipients (pathway segment, not a single point).
A structured way to document change using a small set of observable proxies (movement, warmth, pressure/edema, sensitivity, autonomic tone).
A hypothesis-guided way to consider whether to start locally, distally, or at a putative “gate” region when symptoms appear remote from the likely driver.
A conservative way to integrate adjuncts (manual therapy, heat, movement) as defined inputs u(t) with expected state shifts, rather than ad-hoc stacking.
7.2. A Minimal Mapping and Reassessment Loop
Choose one primary corridor (a meridian-aligned segment) and collect 3-5 baseline proxies before treatment. Apply one main input u(t). Re-check the same proxies immediately after, and again at a short follow-up window (e.g., later the same day). The goal is to detect directional change and coupling (which variables move together), not to prove a mechanism in one session.
Suggested low-burden proxy set (pick 3-5):
M/F: joint range of motion (ROM) measurements or functional movement that the person can repeat reliably; perceived stiffness/glide.
Theta: local warmth/coolness by touch or simple thermometry (if available).
P/V: swelling/pressure sensation, heaviness, capillary refill or simple perfusion proxy (if available).
N: pressure sensitivity / trigger response / pain threshold proxy (repeatable location).
Context: sleep quality, breathing ease, or a brief autonomic proxy (e.g., resting pulse) as a secondary marker.
7.3. How This Model Informs Point Strategy Without Prescribing Points
Segment-first thinking: select a pathway segment that plausibly links the complaint to a driver region. In this model, distal effects may be more likely when the model’s coupling proxy along that segment is high.
Gate regions: if symptoms rebound quickly or shift locations, consider whether a “gate” (high coupling junction) is dominating propagation. Gate-oriented interventions aim to change coupling rather than chase satellites.
Dose and sequencing: when coupling is unstable, prefer single-input sessions and avoid stacking multiple strong modalities in the same window. Use the proxy set to decide whether to repeat, reduce, or change the input next session.
7.4. Lay Explanation (Optional)
A simple explanation consistent with this paper is: “We are treating a pathway, not only a point. The point is an access site that, in this framework, may influence how signals and fluids move along the pathway. We will track a few repeatable signs (movement, warmth, pressure, sensitivity) to see how your body responds.”
7.5. Example Practice Use Cases (Schematic, Non-Prescriptive)
These examples illustrate how a practitioner might use the state-vector/proxy idea to plan and document, without prescribing points or replacing diagnosis:
Musculoskeletal pain with stiffness: prioritize M/F proxies (joint range of motion (ROM) measurements, stiffness/glide). If local needling changes ROM locally but not distally, treat a higher-coupling gate region and reassess whether distal propagation increases.
Head/neck symptoms with frequent rebound: treat as a junction-gating problem. Use a gate-oriented input (single modality) and document whether multiple downstream proxies shift together (coupling), rather than chasing migrating satellites.
Heaviness/pressure-dominant complaints: prioritize P/V proxies (edema/pressure sensation, perfusion markers if available) and track whether thermal or movement inputs shift P/V before pain metrics, indicating a fluidic operating point.
8. Scope Boundaries and Limitations
This paper does not claim that meridians correspond to a single anatomical structure; the model is explicitly multi-substrate and proxy-based (Tier B/C). It also avoids “exotic physics”: the framework is classical, lossy, and test-driven, and the optional A/O/B axes are deliberately removable without collapsing the core claims. The paper makes no treatment-efficacy claims; its predictions focus on measurable propagation and coupling signatures rather than treatment outcomes. Falsifiability is treated explicitly: Section 6 defines disconfirmation criteria such that failure to observe the predicted signatures requires revision or rejection within that stated scope. Overall, the article presents a conceptual framework rather than a complete mechanistic explanation for all meridian phenomena. The state vector is a modeling choice and its components can be revised as evidence accumulates; likewise, if any optional axis is disputed, the core M/E/Θ/Φ/I/F/N/P/V/C formulation and the graph-routing claims remain independently testable. The model also does not assert that any single measurement “is” a meridian; instead, it proposes that multi-parameter patterns and propagation behavior are the appropriate targets of study.
A further guardrail concerns interpretation of broad-spectrum versus specific effects and the meaning of “sham” controls. Commentaries note that acupuncture can show both generalized and symptom-specific effects. Within this framework, broad-spectrum effects can arise when many interventions converge on shared high-centrality nodes or global state variables (e.g., Φ/N/V), whereas specificity can arise when routing and local operating points constrain propagation to a subset of edges. Because most sham procedures still introduce nonzero perturbations (for example, mechanical deformation, cutaneous afference, or temperature change), partial responses are plausible; therefore, falsification should rely on differential signatures—such as routing, phase dependence, and mode-specific proxy patterns—rather than binary “effect/no effect” comparisons alone. Finally, the waveguide analogy should be used carefully: it is a structural metaphor for guided propagation and coupling, not a claim that meridians are equivalent to any single physical waveguide category.
9. Conclusions
The extended meridian waveguide model reframes meridians as distributed, coupled multiphysics pathways representable by a state vector and a weighted graph. This provides an operational bridge between classical meridian theory and measurable biophysics, offering a common language for hypothesis generation, teaching, and study design. The near-term value is pragmatic: clearer intervention targeting, clearer predictions, and clearer methods for minimal, staged validation.
Author Contributions
Conceptualization, model development, writing (original draft), and writing (review & editing): Author. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable (conceptual framework; no human/animal participants or identifiable data).
Informed Consent Statement
Not applicable (conceptual framework; no human/animal participants or identifiable data).
Data Availability Statement
Not applicable. No datasets were generated or analyzed.
Declaration of generative AI: During the preparation of this work the author used ChatGPT (OpenAI) in order to support language editing and formatting. After using, the author reviewed and edited the content as needed and takes full responsibility for the content of the published article.
Conflicts of Interest
The author(s) declare no competing interests.
References
- Schleip, R.; Jäger, H.; Klingler, W. What is ‘fascia’? A review of different nomenclatures. J. Bodyw. Mov. Ther. 2012, 16, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Kumka, M.; Bonar, J. Fascia: a morphological description and classification system based on a literature review. J Can Chiropr Assoc. 2012, 56, 179–191. [Google Scholar] [PubMed]
- Langevin, H.M.; Yandow, J.A. Relationship of acupuncture points and meridians to connective tissue planes. Anat. Rec. 2002, 269, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Langevin, H.M.; Churchill, D.L.; Wu, J.; Badger, G.J.; Yandow, J.A.; Fox, J.R.; Krag, M.H. Evidence of Connective Tissue Involvement in Acupuncture. FASEB J. 2002, 15, 2275–2282. [Google Scholar] [CrossRef] [PubMed]
- Benias, P.C.; Wells, R.G.; Sackey-Aboagye, B.; Klavan, H.; Reidy, J.; Buonocore, D.; Miranda, M.; Kornacki, S.; Wayne, M.; Carr-Locke, D.L.; et al. Structure and Distribution of an Unrecognized Interstitium in Human Tissues. Sci. Rep. 2018, 8, 4947. [Google Scholar] [CrossRef] [PubMed]
- Tomov, N.; Atanasova, D.; Dimitrov, N. Is the Newly Described Interstitial Network the Anatomical Basis of Acupuncture Meridians? A Commentary. Anat. Rec. 2019, 303, 2169–2170. [Google Scholar] [CrossRef] [PubMed]
- Levin, M. Bioelectric signaling: Reprogrammable circuits underlying embryogenesis, regeneration, and cancer. Cell 2021, 184, 1971–1989. [Google Scholar] [CrossRef] [PubMed]
- Young, M.; Lewis, A.H.; Grandl, J. Physics of mechanotransduction by Piezo ion channels. J. Gen. Physiol. 2022, 154, e202113044. [Google Scholar] [CrossRef] [PubMed]
- Ahn, A.C.; Park, M.; Shaw, J.R.; McManus, C.A.; Kaptchuk, T.J.; Langevin, H.M. Electrical Impedance of Acupuncture Meridians: The Relevance of Subcutaneous Collagenous Bands. PLOS ONE 2010, 5, e11907. [Google Scholar] [CrossRef]
- Soh, K.-S. Bonghan Circulatory System as an Extension of Acupuncture Meridians. J. Acupunct. Meridian Stud. 2009, 2, 93–106. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.; Rong, P.J.; Ben, H.; et al. Meridian studies in China: a systematic review. J Acupunct Meridian Stud. 2010, 3, 1–9. [Google Scholar]
- Elahee, S.F.; Pardhan, S.; Behara, D.; et al. Meridian system and mechanism of acupuncture action: A scientific evaluation. World J Acupunct Moxibustion. 2020, 30, 233–238. [Google Scholar] [CrossRef]
- Kovich, A. A new definition of an acupuncture meridian. J Acupunct Meridian Stud. 2019, 12, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Brizhik, L.; Eremko, A.; Pietak, A.; et al. Modeling meridians within the quantum field theory. J Acupunct Meridian Stud. 2019, 12, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Ren, Y.-L.; Chen, Y.-H.; Chen, J.; Tang, X.-J.; Zhang, Z.-M. A “4D” systemic view on meridian essence: Substantial, functional, chronological and cultural attributes. J. Integr. Med. 2022, 20, 96–103. [Google Scholar] [CrossRef] [PubMed]
- LIANG, Y.; ZHOU, J.; DU, J.-Y.; SHAO, X.-M.; FANG, J.-Q. Prospects for the development of acupuncture analgesia from an international perspective. World J. Acupunct. - Moxibustion 2023, 33, 6–8. [Google Scholar] [CrossRef]
- Liu, W.H. Brief discussion on the broad-spectrum effect and specific effect of acupuncture-moxibustion. World J Acupunct Moxibustion. 2023, 33, 294–295. [Google Scholar] [CrossRef]
- Xie, Y.-X.; Xiong, Z.-Y.; Liu, C.-Z.; Yan, S.-Y. Placebo effect of acupuncture in clinical study. World J. Acupunct. - Moxibustion 2023, 33, 309–313. [Google Scholar] [CrossRef]
Figure 2.
Minimal operationalization workflow for testing predictions. Select a meridian-aligned segment and nearby control corridor, choose 2–4 measurable proxies across layers, apply one defined input u(t), and evaluate propagation/attenuation/phase-lag patterns along vs across the segment to support or falsify specific coupling assumptions.
Figure 2.
Minimal operationalization workflow for testing predictions. Select a meridian-aligned segment and nearby control corridor, choose 2–4 measurable proxies across layers, apply one defined input u(t), and evaluate propagation/attenuation/phase-lag patterns along vs across the segment to support or falsify specific coupling assumptions.
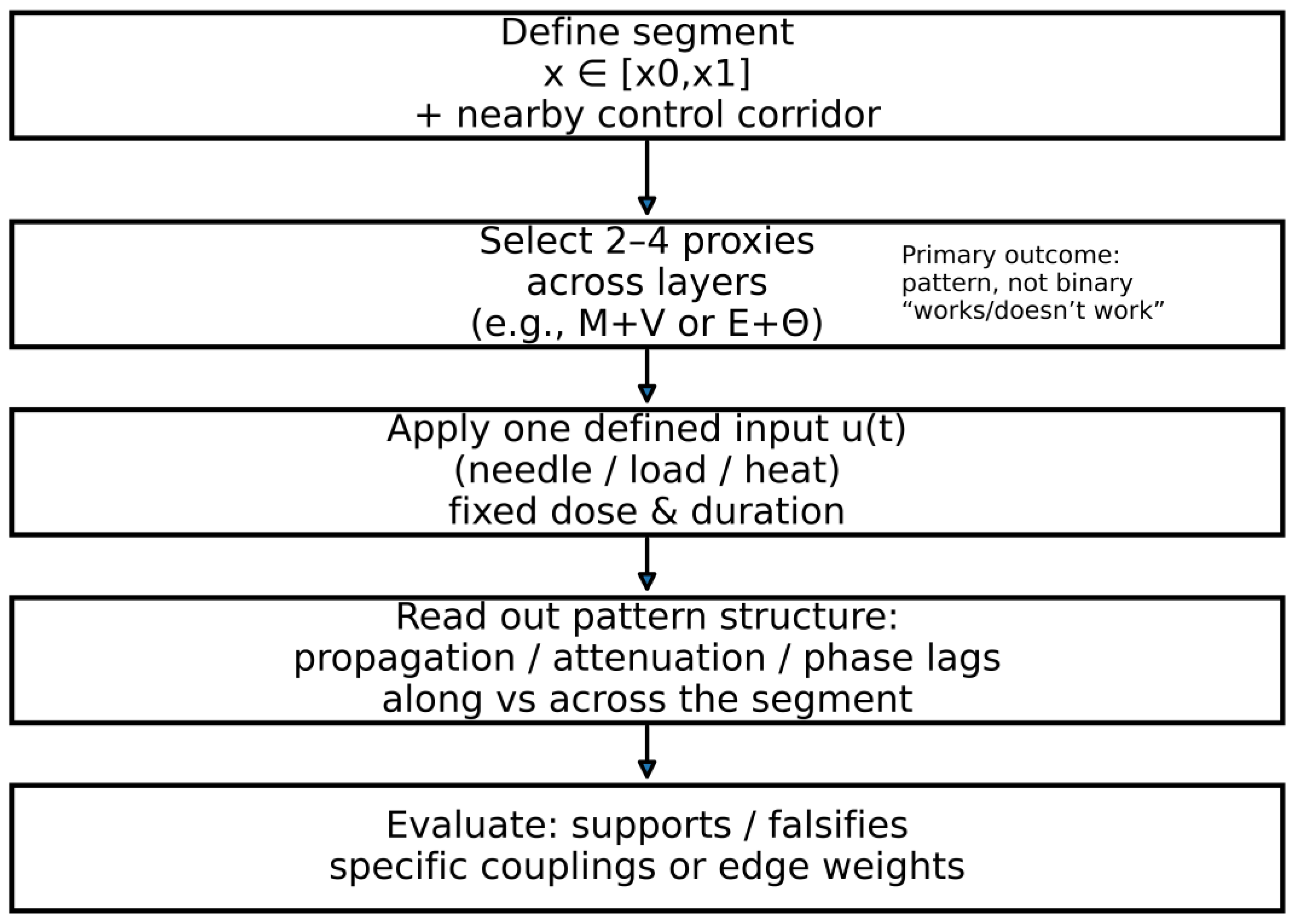
Figure 1.
Meridian network as a functional weighted graph (schematic). Nodes are typed by network role (Hub, Gate, Satellite, Dump/Exit, Proxy). Edge thickness denotes coupling strength; interventions u(t) can perturb local node state and/or reweight adjacent couplings, producing downstream changes in measured proxies.
Figure 1.
Meridian network as a functional weighted graph (schematic). Nodes are typed by network role (Hub, Gate, Satellite, Dump/Exit, Proxy). Edge thickness denotes coupling strength; interventions u(t) can perturb local node state and/or reweight adjacent couplings, producing downstream changes in measured proxies.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



