
Submitted:
06 February 2026
Posted:
09 February 2026
You are already at the latest version
Abstract
Background: Two-stage revision arthroplasty is widely accepted as the reference standard for chronic periprosthetic joint infection (PJI) after total knee arthroplasty (TKA); however, reinfection or persistent infection occurs in a substantial subset of patients. We aimed to identify independent predictors of uncontrolled PJI following two-stage revision using an extended, single-center co-hort. Methods: We retrospectively reviewed 177 knees with PJI after TKA treated with a uniform two-stage revision protocol between September 2011 and February 2022. Patients were classified as controlled (no further infection-related surgery or antimicrobial therapy ≥2 years after reim-plantation) or uncontrolled (persistent infection after the first stage or reinfection after reim-plantation). Demographics, comorbidities, laboratory parameters, perioperative factors, and microbiological characteristics were compared. Multivariate logistic regression was used to identify independent predictors of uncontrolled infection. Results: Among 177 knees, 145 (81.9%) achieved infection control and 32 (18.1%) were classified as uncontrolled. On multivariate analysis, liver cirrhosis (odds ratio [OR] 11.27; 95% confidence interval [CI] 1.004–126.614; p = 0.0496), the presence of a sinus tract at the first infection-control surgery (OR 3.37; 95% CI 1.374–8.254; p = 0.0079), higher erythrocyte sedimentation rate (ESR) prior to reimplantation (OR 1.02 per mm/hr; 95% CI 1.001–1.033; p = 0.0391), and fungal pathogens (OR 9.13; 95% CI 2.073–40.248; p = 0.0035) inde-pendently predicted uncontrolled PJI. Demographic variables and most routine preoperative laboratory markers, including C-reactive protein before the first stage, were not associated with treatment failure. Conclusions: Liver cirrhosis, the presence of a sinus tract, elevated ESR prior to reimplantation, and fungal infection are independent risk factors for uncontrolled PJI after two-stage revision TKA. Preoperative risk stratification incorporating these variables may assist in optimizing reimplantation timing, tailoring antimicrobial strategies, and improving patient counseling.
Keywords:
total knee arthroplasty
; periprosthetic joint infection
; two-stage revision
; risk factors
; liver cirrhosis
; sinus tract
; fungal infection
; erythrocyte sedimentation rate
1. Introduction
Periprosthetic joint infection (PJI) remains one of the most serious complications following total knee arthroplasty (TKA), leading to substantial morbidity, increased healthcare costs, and a high risk of implant failure [1,2]. The incidence of PJI after primary TKA ranges from 0.5% to 2%, with even higher rates reported following revision procedures [3,4]. As the global volume of primary and revision TKA continues to increase, the absolute burden of PJI is expected to rise accordingly [5,6].
For chronic infections, two-stage revision arthroplasty is widely accepted as the reference standard, with reported infection eradication rates ranging from 70% to 90% [7,8,9]. This approach typically involves complete removal of all prosthetic components and cement, thorough debridement of infected and necrotic tissue, placement of an antibiotic-loaded cement spacer, pathogen-directed intravenous antimicrobial therapy, and subsequent reimplantation after an antibiotic-free interval [10,11]. Despite its widespread use and generally favorable outcomes, persistent infection after the first stage or reinfection following reimplantation occurs in a notable proportion of patients [12,13].
Accurately identifying patients at elevated risk of uncontrolled infection may refine clinical decision-making regarding the timing of reimplantation, the aggressiveness of debridement, the choice and duration of antimicrobial therapy, and patient counseling [14,15]. Previous studies have suggested multiple potential risk factors for failure after staged procedures, including host comorbidities, wound complications, serologic and inflammatory markers, and specific pathogens [16,17,18,19]. However, reported findings have been heterogeneous and frequently limited by modest sample sizes, variable definitions of treatment success, and inconsistent surgical protocols [20,21].
Our institution previously reported outcomes from a cohort of 70 knees treated with a uniform two-stage protocol [22]. Building on that work, we analyzed an extended cohort of 177 knees managed over a longer study period using consistent surgical principles and standardized outcome definitions. This study expands upon our previously published cohort (Kim et al., Knee Surgery & Related Research, 2020) by incorporating additional cases and extended follow-up to further validate and refine predictors of uncontrolled infection.
The objective of this study was to identify independent predictors of uncontrolled PJI following two-stage revision TKA in an extended, single-center cohort treated with uniform protocols and prespecified outcome definitions.
2. Materials and Methods
2.1. Study Design and Ethical Approval
This retrospective cohort study was conducted at a tertiary academic center. The present study represents an extended cohort analysis, expanding upon a previously reported institutional series by including additional patients and an extended follow-up period. The study protocol was approved by the Institutional Review Board of Keimyung University Dongsan Medical Center (IRB approval number: 2025-11-025) and was conducted in accordance with the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective design, de-identification of data, and minimal risk to participants.
2.2. Setting and Surgical Protocol
All included cases were managed using a uniform and standardized two-stage revision protocol for chronic knee periprosthetic joint infection (PJI), consistent with established international guidelines [23,24].
Stage one consisted of complete removal of all prosthetic components and cement using hand instruments and high-speed burrs to ensure thorough cement extraction, followed by aggressive synovectomy and debridement of all infected, necrotic, or suspicious tissue. Copious pulsatile lavage was performed, and an antibiotic-loaded polymethylmethacrylate (PMMA) cement spacer was implanted.
Intravenous pathogen-directed antibiotics were administered for approximately 6 weeks after stage one, guided by infectious disease consultation and culture sensitivities. After completion of intravenous antibiotic therapy, patients underwent an antibiotic-free interval of approximately 4 weeks, during which they were monitored clinically for signs of persistent or recurrent infection. Prior to reimplantation, all patients underwent comprehensive clinical evaluation, serologic testing (C-reactive protein [CRP] and erythrocyte sedimentation rate [ESR]), and joint aspiration for cell count, differential, and culture according to surgeon protocol [25].
Stage two involved spacer removal, repeat thorough debridement of all suspicious tissue, copious pulsatile lavage, and reimplantation using revision components. Metal augments and stems were utilized as indicated based on the severity of bone deficiency. When infection control was deemed adequate based on preoperative assessment, first-generation cephalosporins were administered for a short postoperative course (24–48 hours).
A schematic flow diagram summarizing patient selection and the standardized two-stage revision protocol is shown in (Figure 1).
2.3. Participants: Eligibility, Definitions, and Grouping
Inclusion criteria were: knees meeting accepted diagnostic criteria for PJI [26] following primary total knee arthroplasty (TKA); treatment with the standardized two-stage revision protocol between September 2011 and February 2022; and a minimum of 24 months of follow-up after reimplantation for patients who underwent stage two. Exclusion criteria included bilateral simultaneous cases, incomplete medical records, or less than 24 months of follow-up after reimplantation.
Outcome Definitions Were Established a Priori
Controlled infection (Controlled group) was defined as the absence of additional infection-related surgery or antimicrobial therapy for at least 2 years after reimplantation, with resolution of clinical signs and symptoms of infection.
Uncontrolled infection (Uncontrolled group) was defined as persistent infection after stage one precluding safe reimplantation, or any clinically diagnosed reinfection after reimplantation requiring additional surgical intervention and/or prolonged antimicrobial therapy, including same-organism reinfection, different-organism reinfection, and culture-negative clinical infection.
2.4. Variables and Data Collection
Data abstraction was performed using a predefined codebook to standardize variable definitions and minimize misclassification bias. Variables were selected based on clinical relevance and prior literature.
Collected variables included demographics (age, sex, body mass index [BMI], affected side, symptom intervals); comorbidities (tobacco use, cardiovascular disease, diabetes mellitus, cerebrovascular accident, dual antiplatelet therapy, immunocompromised status, liver cirrhosis, and mental health disorders); inflammatory and biochemical laboratory values (hemoglobin, albumin, estimated glomerular filtration rate [eGFR], CRP, and ESR) measured before stage one and before reimplantation; perioperative factors (blood transfusion, inflammatory arthritis, post-traumatic arthritis, presence of a sinus tract, prior joint infection, and bacteremia during the spacer period); and microbiological characteristics (pathogen categories including methicillin-sensitive organisms, methicillin-resistant organisms, Pseudomonas species, fungal infections, and polymicrobial infections).
2.5. Microbiological Methods
At the time of stage one surgery, intraoperative tissue specimens (a minimum of three samples obtained from distinct anatomical sites) were collected using sterile technique. Aerobic and anaerobic cultures were incubated for up to 14 days in accordance with institutional protocols. Fungal cultures were performed when clinically suspected or when bacterial cultures remained negative despite ongoing clinical signs of infection. Antimicrobial selection and treatment duration were determined based on culture results in consultation with infectious disease specialists.
2.6. Statistical Analysis
Continuous variables were assessed for normality and summarized as appropriate. Between-group comparisons were performed using the Mann–Whitney U test or independent t-test for continuous variables and the chi-square or Fisher’s exact test for categorical variables.
All clinically relevant variables were initially evaluated using univariate analyses. Variables demonstrating potential associations (p < 0.10) and those considered clinically important were subsequently entered into multivariate logistic regression models to identify independent predictors of uncontrolled infection. Results are reported as odds ratios (ORs) with 95% confidence intervals (CIs).
All analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA).
3. Results
3.1. Cohort Characteristics
A total of 177 knees in 177 patients were included in the final analysis, comprising 145 knees (81.9%) in the Controlled group and 32 knees (18.1%) in the Uncontrolled group. Baseline demographic and clinical characteristics of the study cohort are summarized in (Table 1).
3.2. Univariate Analyses
All clinically relevant variables were initially assessed using univariate analyses. Comparisons between the Controlled and Uncontrolled groups are summarized in Table 2.
Among comorbidities, liver cirrhosis was significantly more frequent in the Uncontrolled group, while tobacco use showed a trend toward higher prevalence. Laboratory findings measured before stage one surgery did not differ significantly between groups; however, inflammatory markers assessed before reimplantation, particularly the erythrocyte sedimentation rate (ESR), were significantly higher in the Uncontrolled group.
With respect to perioperative and microbiological factors, the presence of a sinus tract at stage one surgery and fungal infection were both significantly more common in the Uncontrolled group. Complete univariate results are presented in (Table 2).
3.3. Multivariate Logistic Regression
After adjustment for potential confounders, four variables remained independently associated with uncontrolled infection. Liver cirrhosis, the presence of a sinus tract at stage one surgery, higher pre-reimplantation ESR, and fungal infection were identified as significant independent predictors of uncontrolled infection. Detailed results of the multivariate logistic regression analysis are shown in Table 2.
3.4. Treatment Outcomes
At a minimum follow-up of 2 years, the overall infection control rate was 81.9%. Among the 32 patients in the Uncontrolled group, 8 patients (25.0%) had persistent infection after stage one that precluded reimplantation, whereas 24 patients (75.0%) experienced reinfection after reimplantation.
4. Discussion
In this extended single-center cohort of 177 knees treated with a standardized two-stage revision protocol for periprosthetic joint infection (PJI), we identified four independent predictors of uncontrolled infection: liver cirrhosis, the presence of a sinus tract at the first infection-control surgery, elevated erythrocyte sedimentation rate (ESR) prior to reimplantation, and fungal pathogens. These factors represent complementary dimensions of infection control failure, integrating host vulnerability, local disease burden, residual systemic inflammation, and pathogen-related characteristics.
Among host-related factors, liver cirrhosis emerged as a particularly strong predictor of uncontrolled infection, with an adjusted odds ratio exceeding 10. Cirrhosis is well known to be associated with immune dysfunction involving impaired neutrophil activity, complement deficiency, and dysregulated cytokine responses, all of which may compromise the host’s ability to eradicate infection. In addition, altered pharmacokinetics and pharmacodynamics of antimicrobial agents in cirrhotic patients may further limit effective treatment. From a clinical perspective, these findings underscore the importance of recognizing liver cirrhosis as a high-risk condition when planning two-stage revision, warranting early multidisciplinary involvement and careful preoperative counseling regarding the likelihood of infection control [27,28,29,30,31].
Local disease burden also played a critical role in treatment failure. The presence of a sinus tract at the time of the first-stage surgery was independently associated with uncontrolled infection, reflecting chronic infection, compromised soft-tissue envelopes, and a direct conduit for microbial persistence. These findings suggest that surgeons should anticipate more extensive debridement in such cases and consider adjunctive strategies, including staged soft-tissue reconstruction, to optimize local conditions prior to reimplantation [32,33,34].
With respect to systemic inflammatory markers, ESR measured immediately prior to reimplantation independently predicted outcome, whereas serologic markers obtained before stage one surgery did not. This distinction suggests that residual inflammatory activity after initial source control may be more relevant than baseline inflammatory burden at presentation. Persistently elevated or non-declining ESR values may therefore serve as a warning signal, prompting caution in reimplantation timing and reinforcing the value of serial serologic monitoring during the interstage period [35,36,37,38,39,40].
Pathogen-related factors further influenced outcomes. Fungal infections were associated with a markedly increased risk of uncontrolled infection. Fungal PJI is inherently challenging due to diagnostic difficulties, low-grade inflammatory responses, biofilm formation, and limited antimicrobial options. Our findings are consistent with prior reports demonstrating poor outcomes following standard two-stage protocols in fungal PJI and support the need for tailored treatment strategies, including prolonged antifungal therapy and, in selected cases, consideration of alternative surgical approaches such as resection arthroplasty [41,42,43,44,45,46,47].
Overall, our results align with and extend existing literature on risk factors for failure after two-stage revision. Previous studies have highlighted the importance of host comorbidities and immunocompromised states as determinants of outcome, and our data further strengthen the evidence for liver cirrhosis as a specific high-risk condition [17,48,49].
The association between sinus tracts and treatment failure has also been reported in prior series [50,51]. In addition, while prior studies have reported inconsistent results regarding serologic markers, our observation that ESR measured immediately prior to reimplantation independently predicts outcome provides additional nuance to existing evidence [37,52]. The overall infection control rate observed in this cohort is comparable to success rates reported in recent systematic reviews, supporting the external validity of our findings [9].
This study has several strengths, including a relatively large single-center cohort managed with a uniform surgical and antimicrobial protocol, extended follow-up, and comprehensive assessment of host, laboratory, perioperative, and microbiological variables. Limitations include the retrospective design with potential residual confounding, single-center data that may limit generalizability, reliance on culture-based pathogen identification, and wide confidence intervals for some predictors reflecting low event rates. Despite these limitations, this study provides robust real-world evidence and offers clinically applicable insights for risk stratification in two-stage revision for PJI.
5. Conclusions
In this extended single-center cohort of patients undergoing two-stage revision for PJI after total knee arthroplasty, liver cirrhosis, the presence of a sinus tract at the first-stage surgery, elevated ESR prior to reimplantation, and fungal pathogens were independently associated with uncontrolled infection. These factors provide a practical framework for preoperative risk stratification and clinical decision-making. Incorporating host, local, serologic, and microbiological risk factors into treatment planning may facilitate more judicious timing of reimplantation, optimization of antimicrobial strategies in high-risk patients, and realistic patient counseling. Prospective multicenter studies are warranted to validate these findings and to develop quantitative risk prediction models.
Author Contributions
Conceptualization, C.-J.Y. and K.-C.B.; methodology, C.-J.Y. and E.-S.S.; formal analysis, E.-S.S. and C.-J.Y.; investigation, E.-S.S. and N.-H.W.; data curation, E.-S.S. and N.-H.W.; writing—original draft preparation, C.-J.Y.; writing—review and editing, K.-C.B.; supervision, K.-C.B.; project administration, K.-C.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Keimyung University Dongsan Medical Center 2025-11-025; date of approval 17, Nov., 2025.
Informed Consent Statement
Patient consent was waived due to the retrospective design and de-identified data analysis.:
Data Availability Statement
The de-identified data presented in this study are available on request from the corresponding author. The data are not publicly available due to institutional review board restrictions and patient privacy considerations.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kurtz, S.M.; Lau, E.; Watson, H.; Schmier, J.K.; Parvizi, J. Economic burden of periprosthetic joint infection in the United States. J Arthroplasty 2012, 27, 61–65.e61. [Google Scholar] [CrossRef]
- Beam, E.; Osmon, D. Prosthetic Joint Infection Update. Infect Dis Clin North Am 2018, 32, 843–859. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Lau, E.; Schmier, J.; Ong, K.L.; Zhao, K.; Parvizi, J. Infection burden for hip and knee arthroplasty in the United States. J Arthroplasty 2008, 23, 984–991. [Google Scholar] [CrossRef]
- Alrayes, M.M.; Sukeik, M. Two-stage revision in periprosthetic knee joint infections. World J Orthop 2023, 14, 113–122. [Google Scholar] [CrossRef]
- Singh, J.A.; Yu, S.; Chen, L.; Cleveland, J.D. Rates of Total Joint Replacement in the United States: Future Projections to 2020-2040 Using the National Inpatient Sample. J Rheumatol 2019, 46, 1134–1140. [Google Scholar] [CrossRef]
- Kamath, A.F.; Ong, K.L.; Lau, E.; Chan, V.; Vail, T.P.; Rubash, H.E.; Berry, D.J.; Bozic, K.J. Quantifying the Burden of Revision Total Joint Arthroplasty for Periprosthetic Infection. J Arthroplasty 2015, 30, 1492–1497. [Google Scholar] [CrossRef]
- Mortazavi, S.M.; Vegari, D.; Ho, A.; Zmistowski, B.; Parvizi, J. Two-stage exchange arthroplasty for infected total knee arthroplasty: predictors of failure. Clin Orthop Relat Res 2011, 469, 3049–3054. [Google Scholar] [CrossRef] [PubMed]
- Ekhtiari, S.; Gazendam, A.; Saidahmed, A.; Petruccelli, D.; Winemaker, M.J.; de Beer, J.D.; Shah, V.; Wood, T.J. Risk factors for recurrence of periprosthetic joint infection following operative management: a cohort study with average 5-year follow-up. Ann Jt 2023, 8, 2. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.Y.; Lu, Y.D.; Bell, K.L.; Wang, J.W.; Ko, J.Y.; Wang, C.J.; Kuo, F.C. Predictors of Treatment Failure After 2-Stage Reimplantation for Infected Total Knee Arthroplasty: A 2- to 10-Year Follow-Up. J Arthroplasty 2018, 33, 2234–2239. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Bae, K.C.; Kim, D.W.; Choi, B.C. Risk factors of uncontrolled periprosthetic knee joint infection after two-stage reimplantation. Knee Surg Relat Res 2020, 32, 22. [Google Scholar] [CrossRef]
- Argenta, L.C.; Morykwas, M.J.; Marks, M.W.; DeFranzo, A.J.; Molnar, J.A.; David, L.R. Vacuum-assisted closure: state of clinic art. Plast Reconstr Surg 2006, 117, 127s–142s. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Whitehouse, M.R.; Lenguerrand, E.; Blom, A.W.; Beswick, A.D. Re-Infection Outcomes Following One- And Two-Stage Surgical Revision of Infected Knee Prosthesis: A Systematic Review and Meta-Analysis. PLoS One 2016, 11, e0151537. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Whitehouse, M.R.; Blom, A.W.; Beswick, A.D. Re-Infection Outcomes following One- and Two-Stage Surgical Revision of Infected Hip Prosthesis: A Systematic Review and Meta-Analysis. PLoS One 2015, 10, e0139166. [Google Scholar] [CrossRef]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis 2013, 56, e1–e25. [Google Scholar] [CrossRef] [PubMed]
- Tande, A.J.; Patel, R. Prosthetic joint infection. Clin Microbiol Rev 2014, 27, 302–345. [Google Scholar] [CrossRef] [PubMed]
- Kubista, B.; Hartzler, R.U.; Wood, C.M.; Osmon, D.R.; Hanssen, A.D.; Lewallen, D.G. Reinfection after two-stage revision for periprosthetic infection of total knee arthroplasty. Int Orthop 2012, 36, 65–71. [Google Scholar] [CrossRef]
- Klemt, C.; Tirumala, V.; Smith, E.J.; Padmanabha, A.; Kwon, Y.M. Development of a Preoperative Risk Calculator for Reinfection Following Revision Surgery for Periprosthetic Joint Infection. J Arthroplasty 2021, 36, 693–699. [Google Scholar] [CrossRef]
- Kuiper, J.W.; Willink, R.T.; Moojen, D.J.; van den Bekerom, M.P.; Colen, S. Treatment of acute periprosthetic infections with prosthesis retention: Review of current concepts. World J Orthop 2014, 5, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kang, C.I.; Lee, J.H.; Joung, M.; Moon, S.; Wi, Y.M.; Chung, D.R.; Ha, C.W.; Song, J.H.; Peck, K.R. Risk factors for treatment failure in patients with prosthetic joint infections. J Hosp Infect 2010, 75, 273–276. [Google Scholar] [CrossRef]
- Senneville, E.; Joulie, D.; Legout, L.; Valette, M.; Dezèque, H.; Beltrand, E.; Roselé, B.; d’Escrivan, T.; Loïez, C.; Caillaux, M.; et al. Outcome and predictors of treatment failure in total hip/knee prosthetic joint infections due to Staphylococcus aureus. Clin Infect Dis 2011, 53, 334–340. [Google Scholar] [CrossRef]
- Bejon, P.; Berendt, A.; Atkins, B.L.; Green, N.; Parry, H.; Masters, S.; McLardy-Smith, P.; Gundle, R.; Byren, I. Two-stage revision for prosthetic joint infection: predictors of outcome and the role of reimplantation microbiology. J Antimicrob Chemother 2010, 65, 569–575. [Google Scholar] [CrossRef]
- Cancienne, J.M.; Werner, B.C.; Bolarinwa, S.A.; Browne, J.A. Removal of an Infected Total Hip Arthroplasty: Risk Factors for Repeat Debridement, Long-term Spacer Retention, and Mortality. J Arthroplasty 2017, 32, 2519–2522. [Google Scholar] [CrossRef]
- Sakellariou, V.I.; Poultsides, L.A.; Vasilakakos, T.; Sculco, P.; Ma, Y.; Sculco, T.P. Risk Factors for Recurrence of Periprosthetic Knee Infection. J Arthroplasty 2015, 30, 1618–1622. [Google Scholar] [CrossRef]
- Lenguerrand, E.; Whitehouse, M.R.; Beswick, A.D.; Kunutsor, S.K.; Foguet, P.; Porter, M.; Blom, A.W. Risk factors associated with revision for prosthetic joint infection following knee replacement: an observational cohort study from England and Wales. Lancet Infect Dis 2019, 19, 589–600. [Google Scholar] [CrossRef]
- McNally, M.; Sousa, R.; Wouthuyzen-Bakker, M.; Chen, A.F.; Soriano, A.; Vogely, H.C.; Clauss, M.; Higuera, C.A.; Trebše, R. Infographic: The EBJIS definition of periprosthetic joint infection. Bone Joint J 2021, 103-b, 16–17. [Google Scholar] [CrossRef]
- Parvizi, J.; Gehrke, T.; Chen, A.F. Proceedings of the International Consensus on Periprosthetic Joint Infection. Bone Joint J 2013, 95-b, 1450–1452. [Google Scholar] [CrossRef]
- Shahi, A.; Parvizi, J.; Kazarian, G.S.; Higuera, C.; Frangiamore, S.; Bingham, J.; Beauchamp, C.; Valle, C.D.; Deirmengian, C. The Alpha-defensin Test for Periprosthetic Joint Infections Is Not Affected by Prior Antibiotic Administration. Clin Orthop Relat Res 2016, 474, 1610–1615. [Google Scholar] [CrossRef]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J Arthroplasty 2018, 33, 1309–1314.e1302. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; Lario, M.; Álvarez-Mon, M. Cirrhosis-associated immune dysfunction: distinctive features and clinical relevance. J Hepatol 2014, 61, 1385–1396. [Google Scholar] [CrossRef] [PubMed]
- Bonnel, A.R.; Bunchorntavakul, C.; Reddy, K.R. Immune dysfunction and infections in patients with cirrhosis. Clin Gastroenterol Hepatol 2011, 9, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Arvaniti, V.; D’Amico, G.; Fede, G.; Manousou, P.; Tsochatzis, E.; Pleguezuelo, M.; Burroughs, A.K. Infections in patients with cirrhosis increase mortality four-fold and should be used in determining prognosis. Gastroenterology 2010, 139, 1246–1256, 1256.e1241–1245. [Google Scholar] [CrossRef] [PubMed]
- Verbeeck, R.K. Pharmacokinetics and dosage adjustment in patients with hepatic dysfunction. Eur J Clin Pharmacol 2008, 64, 1147–1161. [Google Scholar] [CrossRef]
- Tetreault, M.W.; Wetters, N.G.; Moric, M.; Gross, C.E.; Della Valle, C.J. Is synovial C-reactive protein a useful marker for periprosthetic joint infection? Clin Orthop Relat Res 2014, 472, 3997–4003. [Google Scholar] [CrossRef] [PubMed]
- Shimbo, K.; Kawamoto, H.; Koshima, I. Muscle/musculocutaneous versus fasciocutaneous free flap reconstruction in the lower extremity: A systematic review and meta-analysis. Microsurgery 2022, 42, 835–847. [Google Scholar] [CrossRef]
- Li, C.; Renz, N.; Trampuz, A.; Ojeda-Thies, C. Twenty common errors in the diagnosis and treatment of periprosthetic joint infection. Int Orthop 2020, 44, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Ghanem, E.; Parvizi, J.; Burnett, R.S.; Sharkey, P.F.; Keshavarzi, N.; Aggarwal, A.; Barrack, R.L. Cell count and differential of aspirated fluid in the diagnosis of infection at the site of total knee arthroplasty. J Bone Joint Surg Am 2008, 90, 1637–1643. [Google Scholar] [CrossRef]
- Hoell, S.; Moeller, A.; Gosheger, G.; Hardes, J.; Dieckmann, R.; Schulz, D. Two-stage revision arthroplasty for periprosthetic joint infections: What is the value of cultures and white cell count in synovial fluid and CRP in serum before second stage reimplantation? Arch Orthop Trauma Surg 2016, 136, 447–452. [Google Scholar] [CrossRef]
- Kusuma, S.K.; Ward, J.; Jacofsky, M.; Sporer, S.M.; Della Valle, C.J. What is the role of serological testing between stages of two-stage reconstruction of the infected prosthetic knee? Clin Orthop Relat Res 2011, 469, 1002–1008. [Google Scholar] [CrossRef]
- George, J.; Kwiecien, G.; Klika, A.K.; Ramanathan, D.; Bauer, T.W.; Barsoum, W.K.; Higuera, C.A. Are Frozen Sections and MSIS Criteria Reliable at the Time of Reimplantation of Two-stage Revision Arthroplasty? Clin Orthop Relat Res 2016, 474, 1619–1626. [Google Scholar] [CrossRef]
- Shahi, A.; Tan, T.L.; Chen, A.F.; Maltenfort, M.G.; Parvizi, J. In-Hospital Mortality in Patients With Periprosthetic Joint Infection. J Arthroplasty 2017, 32, 948–952.e941. [Google Scholar] [CrossRef]
- Cobo, J.; Miguel, L.G.; Euba, G.; Rodríguez, D.; García-Lechuz, J.M.; Riera, M.; Falgueras, L.; Palomino, J.; Benito, N.; del Toro, M.D.; et al. Early prosthetic joint infection: outcomes with debridement and implant retention followed by antibiotic therapy. Clin Microbiol Infect 2011, 17, 1632–1637. [Google Scholar] [CrossRef]
- Azzam, K.; McHale, K.; Austin, M.; Purtill, J.J.; Parvizi, J. Outcome of a second two-stage reimplantation for periprosthetic knee infection. Clin Orthop Relat Res 2009, 467, 1706–1714. [Google Scholar] [CrossRef]
- Kuiper, J.W.; van den Bekerom, M.P.; van der Stappen, J.; Nolte, P.A.; Colen, S. 2-stage revision recommended for treatment of fungal hip and knee prosthetic joint infections. Acta Orthop 2013, 84, 517–523. [Google Scholar] [CrossRef]
- Phelan, D.M.; Osmon, D.R.; Keating, M.R.; Hanssen, A.D. Delayed reimplantation arthroplasty for candidal prosthetic joint infection: a report of 4 cases and review of the literature. Clin Infect Dis 2002, 34, 930–938. [Google Scholar] [CrossRef]
- Cobo, F.; Rodríguez-Granger, J.; López, E.M.; Jiménez, G.; Sampedro, A.; Aliaga-Martínez, L.; Navarro-Marí, J.M. Candida-induced prosthetic joint infection. A literature review including 72 cases and a case report. Infect Dis (Lond) 2017, 49, 81–94. [Google Scholar] [CrossRef]
- Ueng, S.W.; Lee, C.Y.; Hu, C.C.; Hsieh, P.H.; Chang, Y. What is the success of treatment of hip and knee candidal periprosthetic joint infection? Clin Orthop Relat Res 2013, 471, 3002–3009. [Google Scholar] [CrossRef]
- Anagnostakos, K.; Kelm, J.; Schmitt, E.; Jung, J. Fungal periprosthetic hip and knee joint infections clinical experience with a 2-stage treatment protocol. J Arthroplasty 2012, 27, 293–298. [Google Scholar] [CrossRef]
- Green, C.C.; Valenzuela, M.M.; Odum, S.M.; Rowe, T.M.; Springer, B.D.; Fehring, T.K.; Otero, J.E. Hypoalbuminemia Predicts Failure of Two-Stage Exchange for Chronic Periprosthetic Joint Infection of the Hip and Knee. J Arthroplasty 2023, 38, 1363–1368. [Google Scholar] [CrossRef] [PubMed]
- Logroscino, G.; Campana, V.; Pagano, S.; Taccari, F.; Fantoni, M.; Saracco, M. Risk factors for failure of two-stage revision arthroplasty for infected hip prosthesis: review of the literature and single centre cohort analysis. Eur Rev Med Pharmacol Sci 2019, 23, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Jhan, S.W.; Lu, Y.D.; Lee, M.S.; Lee, C.H.; Wang, J.W.; Kuo, F.C. The risk factors of failed reimplantation arthroplasty for periprosthetic hip infection. BMC Musculoskelet Disord 2017, 18, 255. [Google Scholar] [CrossRef] [PubMed]
- Krizsan, G.; Sallai, I.; Veres, D.S.; Prinz, G.; Szeker, D.; Skaliczki, G. Rifampicin resistance and risk factors associated with significantly lower recovery rates after two-stage revision in patients with prosthetic joint infection. J Glob Antimicrob Resist 2022, 30, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Ghanem, E.; Azzam, K.; Seeley, M.; Joshi, A.; Parvizi, J. Staged revision for knee arthroplasty infection: what is the role of serologic tests before reimplantation? Clin Orthop Relat Res 2009, 467, 1699–1705. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram of patient selection and standardized two-stage revision protocol. Patients treated with two-stage revision for periprosthetic joint infection were included. Uncontrolled PJI was defined as persistent or recurrent infection after reimplantation.
Figure 1.
Flow diagram of patient selection and standardized two-stage revision protocol. Patients treated with two-stage revision for periprosthetic joint infection were included. Uncontrolled PJI was defined as persistent or recurrent infection after reimplantation.
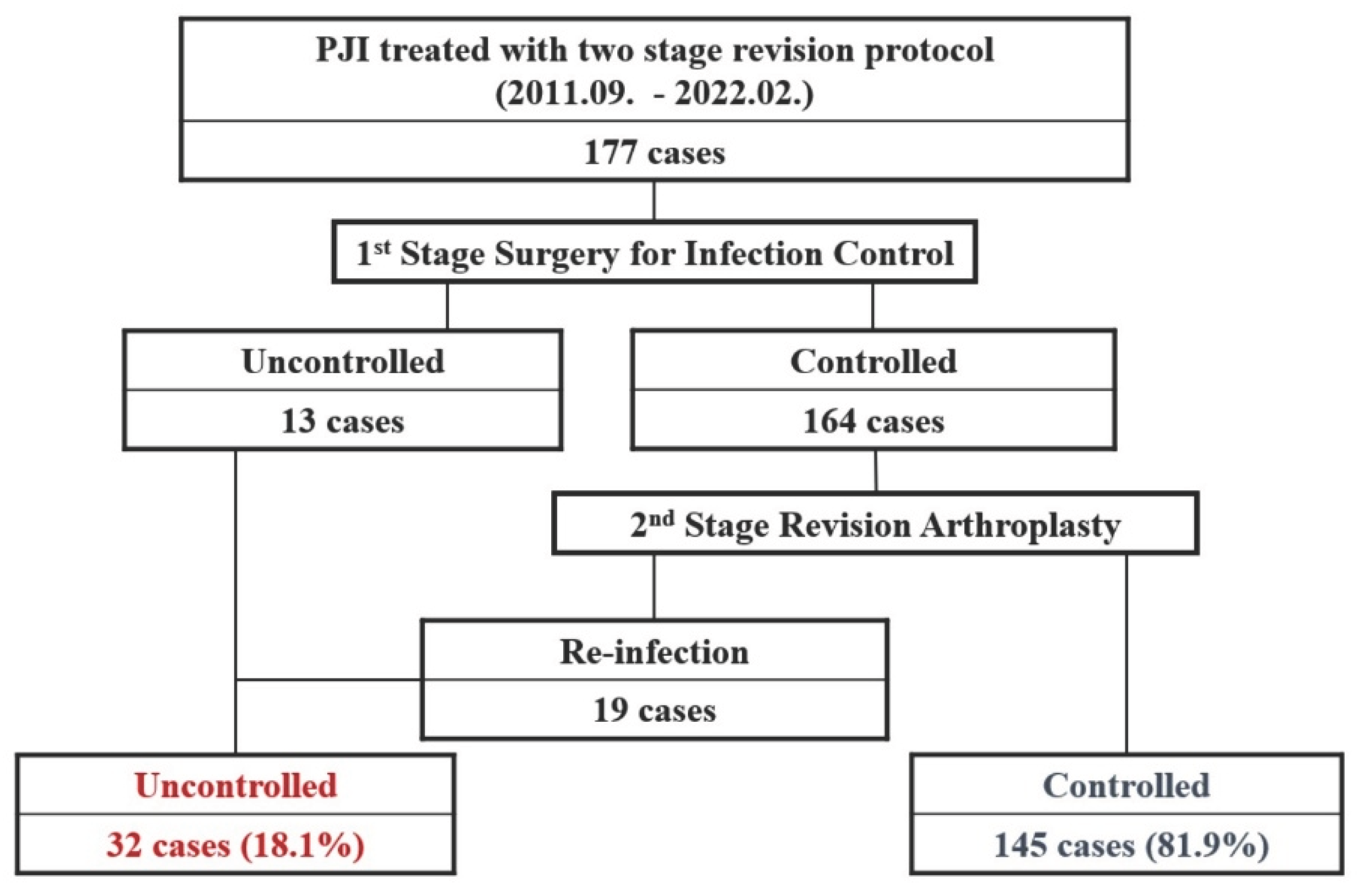

Table 1.
Baseline demographic and clinical characteristics of the study cohort.
| Controlled group N=145 |
Uncontrolled group N = 32 |
p Value | |
|---|---|---|---|
| n(%) or Median (Q1, Q3) | n(%) or Median (Q1, Q3) | ||
| Gender | 0.7197b | ||
| Male | 32(22.07) | 8(25) | |
| Female | 113(77.93) | 24(75) | |
| Age (years) | 69 (63, 72) | 65 (60,72) | 0.2816a |
| Affected Side (Rt. : Lt.) | 0.4142b | ||
| Rt | 75(51.72) | 14(43.75) | |
| Lt | 70(48.28) | 18(56.25) | |
| Height (cm), Mean ± SD | 156.3 ± 8.2 | 155.3 ± 7.5 | 0.5320c |
| Weight (kg), Mean ± SD | 62.7 ± 9.6 | 64.5 ± 12.0 | 0.3581c |
| BMI | 25 (23.2, 27.9) | 26.8 (24.1, 29.1) | 0.0881a |
| Interval between Symptom Onset and 1st infection control surgery for PJI (days) |
74 (27, 182) | 100 (19, 196) | 0.8503a |
(a) Mann-Whitney U test; (b) Chi-square test; (c) Independent Two-sample t-test.
Table 2.
Univariate comparisons and multivariate logistic regression analysis of factors associated with uncontrolled periprosthetic joint infection.
Table 2.
Univariate comparisons and multivariate logistic regression analysis of factors associated with uncontrolled periprosthetic joint infection.
| Controlled Group |
Uncontrolled group | Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n(%) | n(%) | Odds Ratio | Wald CI(95%) | p Value | Odds Ratio | Wald CI(95%) | p Value | ||
| Past Medical History | |||||||||
| Tobacco use | No | 141(97.24) | 29(90.63) | Reference | |||||
| Yes | 4(2.76) | 3(9.38) | 3.64 | 0.77, 17.16 | 0.1019 | ||||
| Cardiovascular disease | No | 121(83.45) | 28(87.5) | Reference | |||||
| Yes | 24(16.55) | 4(12.5) | 0.72 | 0.23, 2.24 | 0.5713 | ||||
| Diabetes mellitus (DM) | No | 88(60.69) | 20(62.5) | Reference | |||||
| Yes | 57(39.31) | 12(37.5) | 0.93 | 0.42, 2.04 | 0.8493 | ||||
| Stroke Hx. (History of cerebral infarction) |
No | 135(93.1) | 31(96.88) | Reference | |||||
| Yes | 10(6.9) | 1(3.13) | 0.44 | 0.05, 3.53 | 0.4362 | ||||
| Dual Anti-platelet use | No | 142(97.93) | 31(96.88) | Reference | |||||
| Yes | 3(2.07) | 1(3.13) | 1.53 | 0.15, 15.18 | 0.7174 | ||||
| Immunocompromised status | No | 130(89.66) | 29(90.63) | Reference | |||||
| Yes | 15(10.34) | 3(9.38) | 0.90 | 0.24, 0.3 | 0.8696 | ||||
| Liver cirrhosis (LC) | No | 144(99.31) | 29(90.63) | Reference | |||||
| Yes | 1(0.69) | 3(9.38) | 14.90 | 1.50, 148.29 | 0.0212 | 11.27 | 1.004, 126.614 | 0.0496 | |
| Mental health disorder (MDD, alcoholics, etc.) |
No | 140(96.55) | 30(93.75) | Reference | |||||
| Yes | 5(3.45) | 2(6.25) | 1.87 | 0.34, 10.08 | 0.4682 | ||||
| Pre-operative Laboratory Findings before 1st infection control surgery for PJI | |||||||||
| Hemoglobin (Hb, g/dL) | 11.16 ± 1.56 | 11.22 ± 1.34 | 1.03 | 0.80, 1.32 | 0.8373 | ||||
| Albumin (Alb, g/dL) | 3.81 ± 0.42 | 3.85 ± 0.39 | 1.27 | 0.49, 3.26 | 0.6241 | ||||
| Estimated glomerular filtration rate (eGFR, mL/min/1.73m2) | 86.81 ± 30.43 | 88.61 ± 25.95 | 1.00 | 0.90, 1.02 | 0.756 | ||||
| C-reactive protein (CRP, mg/dL) |
7.70 ± 8.96 | 4.91 ± 5.39 | 0.95 | 0.89, 1.01 | 0.1029 | ||||
| Erythrocyte sedimentation rate (ESR, mm/hr) | 86.99 ± 29.92 | 81.13 ± 29.28 | 0.99 | 0.98, 1.01 | 0.322 | ||||
| Pre-operative Laboratory Findings before Revision TKA | |||||||||
| Hemoglobin (Hb, g/dL) | 11.61 ± 1.35 | 11.65 ± 1.35 | 1.02 | 0.76, 1.37 | 0.8795 | ||||
| Albumin (Alb, g/dL) | 4.67 ± 7.57 | 3.99 ± 0.32 | 0.68 | 0.24, 1.90 | 0.46 | ||||
| Estimated glomerular filtration rate (eGFR, mL/min/1.73m2) | 85.53 ± 26.53 | 86.91 ± 25.25 | 1.00 | 0.99, 1.02 | 0.7929 | ||||
| C-reactive protein (CRP, mg/dL) | 0.51 ± 0.8 | 0.85 ± 0.99 | 1.46 | 0.99, 2.16 | 0.0565 | ||||
| Erythrocyte sedimentation rate (ESR, mm/hr) | 39.04 ± 25.18 | 52.23 ± 26.11 | 1.02 | 1.00, 1.03 | 0.0127 | 1.02 | 1.001, 1.033 | 0.0391 | |
| Peri-operative Risk Factors | |||||||||
| Peri-operative Transfusion | No | 40(27.59) | 5(15.63) | Reference | |||||
| Yes | 105(72.41) | 27(84.38) | 2.06 | 0.74, 5.71 | 0.1663 | ||||
| Presence of Sinus tract at the time of 1st infection control surgery | No | 124(85.52) | 18(56.25) | Reference | |||||
| Yes | 21(14.48) | 14(43.75) | 4.54 | 1.99, 10.61 | 0.0004 | 3.37 | 1.374, 8.254 | 0.0079 | |
| Inflammatory arthritis (e.g., RA) |
No | 143(98.62) | 32(100) | Reference | |||||
| Yes | 2(1.38) | 0(0) | 0.88 | 0.2, 26.24 | 0.9477a | ||||
| Post-traumatic arthritis | No | 143(98.62) | 31(96.88) | Reference | |||||
| Yes | 2(1.38) | 1(3.13) | 2.73 | 0.02, 37.12 | 0.4057 | ||||
| History of Joint Infection before Primary TKA | No | 139(95.86) | 30(93.75) | Reference | |||||
| Yes | 6(4.14 | 2(6.25) | 1.76 | 0.3, 8.03 | 0.6046 | ||||
| Bacteremia at PROSTALAC | No | 128(88.28) | 32(100) | Reference | |||||
| Yes | 17(11.72) | 0(0) | 0.11 | 0.01, 2.09 | 0.143a | ||||
| Type of Pathogens | |||||||||
| Methicillin Sensitive Organisms [MS gram(+) + MS gram (-) ] |
No | 118(81.38) | 29(90.63) | Reference | |||||
| Yes | 27(18.62) | 3(9.38) | 0.45 | 0.12, 1.59 | 0.2169 | ||||
| Methicillin Resistant Organisms [MR gram(+) + MR gram (-) ] |
No | 86(59.31) | 24(75) | Reference | |||||
| Yes | 59(40.69) | 8(25) | 0.49 | 0.20, 1.16 | 0.1024 | ||||
| Pseudomonas species | No | 142(97.93) | 30(93.75) | Reference | |||||
| Yes | 3(2.07) | 2(6.25) | 3.16 | 0.51, 19.71 | 0.2189 | ||||
| Fungus | No | 142(97.93) | 24(75) | Reference | |||||
| Yes | 3(2.07) | 8(25) | 15.78 | 3.91, 63.70 | 0.0001 | 9.13 | 2.073, 40.248 | 0.0035 | |
| Multiple pathogens | No | 141(97.24) | 29(90.63) | Reference | |||||
| Yes | 4(2.76) | 3(9.38) | 3.64 | 0.77,17.16 | 0.1019 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



