Submitted:
06 February 2026
Posted:
06 February 2026
You are already at the latest version
Abstract
Paramedics and other public safety personnel experience a high prevalence of mental health conditions, yet stigma and access barriers often limit engagement with professional care. As part of a post-pandemic mental health study, we evaluated the feasibility and utility of providing voluntary, personalized mental health feedback reports to paramedics in two Ontario services. During compulsory continuing medical education sessions in the fall of 2024, 995 paramedics (96% of eligible) completed a survey with screening tools for various mental disorders. Participants could choose to receive a confidential report summarizing their screening results. Overall, 58% opted to receive a report, of whom 38% completed a follow-up survey approximately two months later. Participants who screened positive for posttraumatic stress disorder, major depressive disorder, or generalized anxiety disorder were significantly more likely to report contacting a mental health professional than those screening negative (27% vs. 7.8%; Odds Ratio 4.35, p<0.001), corresponding to an estimated pseudo-number needed to treat of five. Qualitative comments indicated that feedback reports increased awareness, validated symptoms, and, in some cases, prompted help-seeking or behavior change. These findings suggest that voluntary, low-burden mental health check-ins are a feasible strategy to identify at-risk paramedics and facilitate connection to care.
Keywords:
public safety personnel
; paramedics
; post-traumatic stress injuries
; mental health
; posttraumatic stress disorder
; occupational health
1. Introduction
The mental health and well-being of Public Safety Personnel (PSP) in Canada has been a national policy priority for the past 10 years [1]. As an umbrella term, PSP broadly refers to front-line workers mandated to ensure the safety and security of Canadians [2], including police officers, firefighters, corrections officers, and paramedics, among others. PSP experience frequent exposure to trauma [3] with a correspondingly high prevalence of mental disorder symptoms [4], including posttraumatic stress disorder (PTSD) and other forms of post-traumatic stress injuries (PTSI).
Paramedics are a distinct branch of the public safety professions in that their mandate and organizational culture straddle both public safety and health care. In Canada, paramedics are increasingly engaged in complex primary health and social care roles through community paramedicine programs that deploy paramedics in roles adjacent to traditional emergency (i.e., 9-1-1) response [5] amid persistent family physician shortages [6]. At the same time, a growing body of research illustrates that paramedics experience substantial work-related mental health sequelae [7,8,9]. Prior to the COVID-19 pandemic, a national survey by Carleton and colleagues estimated the prevalence of PTSD among paramedics at approximately 1 in 4, with 30% screening positive for major depressive disorder and a similar proportion screening positive for one of several anxiety disorders [4]. High rates of suicidal ideation [10], disturbed sleep [11], chronic pain [12] and co-morbid chronic health conditions [13] have also been reported, along with frequent workers compensation claims related to traumatic stress injuries [14]. Given the growing reliance of Canadians on paramedics for increasingly complex healthcare needs [15,16], promoting mental health and well-being within the paramedic workforce represents an important public policy objective.
Routine mental health monitoring and various forms of mental health “check-ins” have been proposed as potential strategies to support workforce well-being in the public safety professions [17]. For example, “safeguard programs” in policing require members to attend regular psychological assessments conducted by mental health professionals [18]. However, PSP have historically faced challenges accessing timely, culturally competent mental health care [19,20]. Stigma, in particular, has been a pressing issue among PSP affecting both the expression of help-seeking behaviors and the willingness to access professional care. Within this construction, seeking out or accessing mental health support creates concerns around the suitability of the member for public safety work, their reliability as a co-worker, and eligibility for promotion [21,22,23] – all of which conspire to make PSP reluctant to disclose distressing symptoms or access care. As a result, PSP, including paramedics, tend to rely on informal sources of mental health support, such as colleagues, family, or friends, rather than professional services [24].
These realities raise important questions about the cultural acceptability and practical utility of routine mental health check-ins as an occupational health strategy. For such approaches to be useful, PSP must be willing to participate, perceive the feedback as credible and useful, and be able to access appropriate professional care when indicated. Despite widespread recognition of the need to support PSP mental health, there is limited empirical evidence on whether voluntary, feedback-based mental health check-ins are capable of facilitating access to care among paramedics.
As part of a broader post-pandemic epidemiological study of paramedic mental health, we examined the feasibility and utility of providing voluntary, personalized mental health feedback reports to consenting participants. Our objectives were to: (1) assess the proportion of participants who opted to receive a feedback report; (2) evaluate recipients’ perceptions of the usefulness of the information provided; and (3) estimate the ability of the feedback process to connect paramedics with elevated mental disorder symptoms to professional mental health care.
2. Materials and Methods
2.1. Overview and Setting
This study was conducted in Ontario, Canada, and recruited participants from two paramedic services in Southern Ontario. Essex-Windsor Emergency Medical Services (EW-EMS), located in Southwestern Ontario, employs 350 Primary and Advanced Care Paramedics (P/ACPs) and serves a mixed suburban and rural geography of 1,600km2 with a population of approximately 468,000 residents. Peel Regional Paramedic Services (PRPS) employs approximately 700 paramedics and serves a predominantly suburban geography of 1,200km2 in the Greater Toronto Area with a population of 1.6 million residents.
In Ontario, land ambulance paramedic services are publicly funded and delivered primarily by lower-tier municipal or regional governments as distinct entities from police and fire. Entry to practice requires the completion of a college diploma to qualify as a Primary Care Paramedic (PCP). PCPs may complete an additional year of training to obtain Advanced Care Paramedic (ACP) certification. ACPs are typically triaged to higher acuity and life-threatening 9-1-1 calls. Paramedics in Ontario are unionized and earn an average annual income of approximately $74,000 CAD.
2.2. Recruitment
We recruited paramedics from both sites during compulsory in-person Continuing Medical Education (CME) sessions in the fall of 2024. Paramedics are required to attend CME sessions twice annually to maintain certification to practice. These sessions are organized by the paramedic service, with all active-duty paramedics (i.e., not on leave) required to attend and compensated at their usual rate of pay.
For the PRPS site, one author (JM) attended each CME session and delivered a 10-minute presentation describing the study and participation procedures, including the option to receive a mental health report and its content. At EW-EMS, this presentation was video recorded and played at the start of each CME day. Both presentations emphasized that participation was voluntary and that their data would not be shared with the paramedic service.
2.2. Data Collection
Consenting paramedics completed an eight-page pen-and-paper survey that included a demographic questionnaire and the following self-report mental disorder screening instruments: the 21-item posttraumatic stress disorder checklist (PCL-5) [25], the 9-item patient health questionnaire (PHQ-9) for major depressive disorder [26], the 7-item generalized anxiety disorder questionnaire (GAD-7) [27], the 7-item insomnia severity index (ISI) [28], and the 10-item alcohol use disorder identification test (AUDIT) [29].
All instruments were scored according to the established thresholds for each instrument. For PTSD, participants answered a binary question regarding lifetime exposure to an index trauma, defined as actual or threatened death, serious injury, or sexual violence that happened to them directly, happened to a close family member or friend, or was encountered as part of their job. Participants endorsing trauma exposure completed the PCL-5 in reference to the index trauma or the event currently causing the most distress. Consistent with prior research among PSP, a positive PTSD screen required endorsement of at least moderate symptoms within each symptom cluster and a summed score greater than 32 [4]. Positive screens for major depressive disorder and generalized anxiety disorder were defined as summed scores greater than 9 on the PHQ-9 and GAD-7, respectively. A summed score of 15 or greater on the ISI indicated clinically significant insomnia. AUDIT scores greater than 8 were interpreted as potentially hazardous alcohol use with scores of 15 or greater indicating possible dependence.
Current suicidal ideation was assessed using item 9 on the PHQ-9, which asked participants how often they had experienced thoughts of being “better off dead or harming (themselves) in some way” over the past 14 days. Response options ranged from “not at all” to “nearly every day”. Any response other than “not at all” was considered indicative of current suicidal ideation.
The PCL-5, PHQ-9, and GAD-7 have robust validity evidence and have been widely used in prior Canadian PSP research [4,17], in addition to being used in population-level mental health surveillance by Statistics Canada during the COVID-19 pandemic [30].
The demographic questionnaire collected information on gender (man, woman, transgender or non-binary), race (using categories derived from the Canadian Institutes of Health Information guidelines), age, relationship status (single, non-cohabitating relationship, married/common-law, divorced/separated), educational attainment (college certificate, college diploma, undergraduate degree, graduate degree), professional role (front-line, supervisory/leadership), certification level (primary or advanced care), years of experience, and 2SLGBTQI+ identity. These variables were captured in an earlier study on paramedic mental health in Peel Region [31] and were constructed in alignment with demographic data collected by Statistics Canada’s survey on COVID-19 and mental health.
Prior to the study launch, we pilot tested the survey among paramedics for clarity, readability, layout and completion time, making minor edits to the wording of instructions and formatting of the survey booklet. Survey packages included the consent form, a list of locally available mental health resources, and a $10 Tim Horton’s gift card. Participants were free to keep the gift card irrespective of their participation in the study.
Consenting paramedics could complete the survey anonymously or elect to provide their name and email address to receive a personalized mental health feedback report (described below). Completed surveys were placed in opaque envelopes, sealed by participants, and deposited into a locked study drop box. Surveys from PRPS were collected daily, while surveys from EW-EMS were collected weekly. Upon collection, surveys from confidential-stream participants were reviewed to identify individuals reporting current suicidal ideation, who were triaged for prompt follow-up according to study safety protocols. Survey data were abstracted into electronic format, reviewed against the paper survey for accuracy, with paper records subsequently destroyed.
2.3. Mental Health Reports
Confidential-stream participants received a 1–2-page mental health feedback report based on their screening scores. The reports were standardized in format and characterized symptom severity and risk level for each screening instrument using the language and scoring thresholds associated with each tool. For example, the PHQ-9 scores are categorized as “minimal” (0-4), “mild” (5-9), “moderate” (10-14), “moderately severe” (15-19), and “severe” (20 or higher).
For scores below the threshold for a positive screen (e.g., <10 on the PHQ-9), reports included the following interpretive text:
“The information you have provided suggests your symptoms are mild and are not of serious mental health concern. These symptoms, even when mild, can be distressing to you. You can benefit from access to mental health services, whether your symptoms are mild or significant”
Likewise, if a participant’s score exceeded the test positivity threshold, we included the following text:
“The information you have provided suggests your symptoms are significant and are of genuine mental health concern”
This language was derived in consultation with members from the Canadian Institute of Public Safety Research and Treatment and mirrors what is available on a public-facing self-screening website intended for PSP.
Because the PCL-5 does not provide gradations of symptom severity beyond a binary screening threshold [32], we defined a “sub-clinical” range of summed scores (13-32) to identify participants reporting potentially distressing symptoms below the positive screening threshold. This range was derived by taking one standard deviation above the mean PCL-5 score observed in a large national sample of Canadian PSP [4]. Participants within this range received the following text:
“The information you have provided suggests your symptoms may be associated with the early stages of PTSD, and you would likely benefit from proactively accessing evidence-based care”
Each report concluded with a brief narrative summary synthesizing the participant’s overall risk profile across measures. Surveys indicating suicidal ideation were reviewed by a psychiatrist (NA) to refine recommendations for follow-up care. Participants with concerning scores were encouraged to access professional mental health care. The feedback reports stressed that the information conveyed was non-diagnostic.
Reports included a list of locally available mental health resources, including first responder-focused peer support services, provincial psychologist directories, and 9-8-8, the national suicide crisis helpline. For PRPS participants, reports also referenced an existing partnership with a local hospital providing expedited mental health assessment, typically within 48 hours on weekdays. Participants from PRPS with concerning scores received an additional two-page brochure outlining referral procedures. A sample report is provided as supplementary material.
2.4. Follow-Up Survey
Approximately 6-8 weeks after receiving their feedback report, we emailed confidential-stream participants and asked them to complete a web-based follow-up survey. The survey assessed participants’ perceptions of the usefulness and accuracy of the report using anchored 7-point Likert scales. The participants were also asked whether they had accessed any recommended resources, contacted a mental health professional, or intended to seek professional care in the future. These questions were developed through the consensus of the research team and in consultation with health and well-being representatives from the paramedic services. The survey included a free-text field for additional unstructured comments.
2.5. Analyses
We analyzed our data four ways. First, we used descriptive statistics to characterize the sample and estimate the prevalence of mental disorder symptoms at each site. Second, we used analysis of variance (ANOVA) and chi-square tests to examine group differences by site, participation stream (anonymous vs. confidential), and demographic characteristics, with particular attention to potential selection effects and follow-up survey response bias.
Third, we estimated a pseudo-number needed (NNT) [33] using a per-protocol framework. The intervention group comprised participants who screened positive for PTSD, major depressive disorder, or generalized anxiety disorder and reported contacting a mental health professional in the follow-up survey. The counterfactual condition consisted of participants who screened negative for these conditions but reported contacting a mental health professional. The NNT was calculated as the inverse of the absolute risk reduction, defined as the difference in event rates between the intervention and counterfactual conditions. Sensitivity analyses were conducted using alternative assumptions about the counterfactual, including treating all follow-up survey non-responders as controls. All quantitative analyses were conducted in SPSS version 31.
2.6. Research Ethics
This study was approved by Research Ethics Boards at the University of Toronto (protocol 46717 and the University of Windsor (same protocol number) All participants provided written informed consent prior to completing the survey. Study protocols permitted breach of confidentiality to facilitate emergency intervention if a participant was deemed to be at imminent risk of serious bodily harm or death, although this was not required.
3. Results
Between September 1 and December 31, 2024, a total 1,031 paramedics across both sites attended CME sessions. We received 1,007 surveys from consenting participants. After excluding 12 surveys due to incomplete questionnaires or large portions of missing data, the final sample comprised 995 participants, yielding an overall response rate of 96%. Most participants were from the Peel Region site (68%; n=675), with 320 participants (32%) from Essex-Windsor.
Overall, 588 participants (58%) opted for the confidential stream, with more enrolment in the confidential stream in Peel Region than Essex-Windsor (62% vs. 51%, p=0.002). Participant flow is shown in Figure 1.
3.1. Participant Demographics
Across both sites, most participants were men (61%), White (72%), in a relationship (73%), and reported a college diploma as their highest level of education (63%). Most participants worked full-time (73%) in a patient-facing role (92%) and practiced as Primary Care Paramedics (74%). Seven percent identified as members of the 2SLGBTQI+ community. Missing demographic data were rare, with age being the most frequently skipped field (n=26; 3.8%). Full demographic characteristics, including site-level comparisons, are presented in Table 1.
3.2. Mental Disorder Symptom Prevalence
Overall, 117 participants (12%) screened positive for PTSD, with an additional 270 (27%) reporting sub-clinical PTSD symptoms. In total, 244 (25%) screened positive for major depressive disorder, 233 (23%) for generalized anxiety disorder, 303 (30%) for insomnia, and 210 (21%) for potentially hazardous alcohol consumption; 49 participants (5%) screened positive for probable alcohol dependence. Across both sites, 339 participants (34%) screened positive for at least one of PTSD, major depressive disorder, or generalized anxiety disorder.
Symptom prevalence was generally similar across sites, although major depressive disorder was more prevalent in Peel Region than in Essex-Windsor (26% vs. 20%, p=0.035). There were no significant site-level differences in the overall prevalence of PTSD, major depressive disorder, or generalized anxiety disorder (36% in Peel Region vs. 30% in Essex-Windsor, p=0.088).
Symptom prevalence also did not differ meaningfully between participants in the confidential and anonymous streams (sub-clinical PTSD: 27.8% vs. 26.1%, p=0.556; clinical PTSD: 11.5% vs. 12.1%, p=0.774; MDD: 24.2% vs. 24.9%, p=0.779; GAD: 24.2% vs. 22.2%, p=0.474; insomnia: 29.8% vs. 30.9%, p=0.711; hazardous alcohol consumption: 20.7% vs. 21.3%, p=0.844). Overall, 33.6% of confidential-stream participants screened positive for PTSD, major depressive disorder, or generalized anxiety disorder, compared with 34.6% of anonymous-stream participants (p=0.756).
3.3. Delivery of Mental Health Reports
We sent personalized mental health feedback reports to 578 confidential stream participants across both sites. In 10 cases, reports could not be delivered due to invalid or missing email addresses. Among Peel Region participants, the reports were delivered an average of 6.0 days (SD 6.4) after CME attendance. Among participants classified as “highly worrisome cases” (n=31), the mean time to report delivery was longer (9.4 vs. 5.7 days, p=0.002).
Due to differences in survey collection procedures, time-to-report delivery could not be reliably estimated for participants at the Essex-Windsor site.
3.4. Follow-Up Survey Responses
Among participants with a verified email address who received a report, 221 (38%) completed the follow-up survey. Response rates were similar across sites (37% in Peel Region vs. 40.2% in Essex-Windsor, p=0.479).
Compared with non-responders, follow-up survey responders were slightly more experienced (12 vs. 11 years, p=0.009), more likely to be in a relationship (80% vs. 72%, p=0.01), more likely to have completed university education (42% vs. 35%, p=0.03), and more likely to screen positive for major depressive disorder (29.8% vs. 20.7%, p=0.01). The overall prevalence of PTSD, major depressive disorder, or generalized anxiety disorder did not differ significantly between responders and non-responders (38% vs. 31%, p=0.08).
Most participants agreed that the report was useful (n=180; 81%) and consistent with how they perceived their mental health (n=204; 92%). Overall, 30 participants (13%) reported that they accessed the mental health resources listed in the report, 33 (15%) reported contacting a mental health professional, and 75 (34%) indicated an intention to do so in the future. Responses did not differ significantly by site (Table 2).
Follow-up respondents who screened positive for PTSD, major depressive disorder, or generalized anxiety disorder were more likely to have contacted a mental health professional compared with responders who screened negative (27% vs. 7.8%, OR 4.35, 95% CI 1.99-9.48, p<0.001). This corresponded to an absolute risk reduction of 19.2% for a pseudo-NNT of approximately five.
3.5. Survey Comments
Ninety participants provided approximately 3,000 words of free-text comments in the follow-up survey. The results of our qualitative content analysis are summarized in Table 3.
The participants were broadly supportive of the research and particularly valued the opportunity to receive personalized feedback: “I appreciate the opportunity to receive this report”. Many stated the report provided insight into their mental health that would otherwise have been difficult to obtain, and in some cases, motivated behavior change.
“This information is valuable in increasing my awareness of my current mental state and the resources available to me, should I require them.”
“The description of alcohol use relating to a high risk of mental health concerns seemed more than expected for (my intake). However, I have begun to make changes in my intake … As well, I have taken into consideration the negative health effects of any intake of alcohol in general.”
Even still, the amount of insight that could be gleaned from the report was limited by its brevity, with several participants wanting more detailed feedback: “I didn’t think the survey was in-depth enough, but then again, we had time constraints”. The feedback we could offer to participants was within the light of the lamppost from the screening measures, which provided an incomplete picture: “I didn’t flag for anything and I found that surprising. A report saying you’re healthy when you don’t feel that way is interesting”.
The goal of the participant feedback was to connect at-risk paramedics to mental health care, leveraging existing programs and resources available within the two sites. However, the access pathways were imperfect, as one participant explained:
“I knew my mental health wasn’t great and this (report) just backed up my thinking and nudged me to get help. I called the number that (my service) provides to all paramedics, which allows us to be seen within 48 hours by a mental health professional. Unfortunately, I was told the initial assessment would be over $600. … That amount of money was way too expensive for me, unfortunately, so it was a discouraging dead end.”
The comment was from an early career paramedic who screened positive for major depressive disorder and lacked employer-funded psychotherapy benefits.
Finally, a notable number of participants reported that they were already engaged in mental health care prior to study participation. Among follow-up respondents who screened positive for PTSD, major depressive disorder, or generalized anxiety disorder (n=85), 42 (49%) either contacted a mental health professional following receipt of the report or indicated that they were already connected to care.
4. Discussion
The goal of this study was to evaluate the utility of voluntary, personalized mental health feedback reports as a companion process within a broader epidemiological study of paramedic mental health in two Ontario services. Among nearly 1,000 participants, approximately 60% opted to receive a feedback report, and 15% of recipients indicated that they accessed mental health services as a result. Participants with at least moderate symptoms of PTSD, major depressive disorder, or generalized anxiety disorder were approximately four times more likely to report contacting a mental health professional. Among this at-risk group, our findings suggest that for every five reports delivered, one participant went on to access professional mental health care. While not a formal interventional trial, this magnitude of association suggests that voluntary feedback reports may represent a low-burden and potentially efficient mechanism for facilitating access to care, with important implications for both research and policy.
From a research perspective, these findings contribute to the growing literature on the mental health impacts of the COVID-19 pandemic on paramedics in Ontario. Earlier studies have documented elevated rates of burnout, PTSD, and other mental health concerns among healthcare workers in Canada [37,38,39] and the United States [40], with emerging evidence of substantial mental health sequelae among emergency medical services personnel in the United States [41,42,43,44]. However, comparable post-pandemic data for Canadian paramedics remain limited; in a pre-pandemic study conducted among paramedics in Peel Region, 11% screened positive for PTSD, 15% for major depressive disorder, and 15% for generalized anxiety disorder [31]. In the present study, the prevalence of PTSD symptoms was similar, while symptoms of depression and anxiety were substantially more prevalent, suggesting a sustained or evolving mental health burden following the pandemic period.
Our findings also underscore the vulnerability of paramedics as an occupational group at elevated risk for mental disorder symptoms. Population-level mental health surveillance conducted by Statistics Canada during the COVID-19 pandemic used repeated, stratified random samples of Canadians and the same screening instruments employed in this study to monitor symptoms of PTSD, major depressive disorder, and generalized anxiety disorder [30]. At its peak prevalence in February-May 2021, approximately 25% of Canadians screened positive for at least one of these conditions [45]. By contrast, more than one year after the World Health Organization declared the public health emergency of global concern over, 36% of participants in our study met the screening criteria for PTSD, major depressive disorder, or generalized anxiety disorder. This disparity highlights the persistent and disproportionate mental health burden experienced by paramedics.
From a policy perspective, our findings offer preliminary evidence that mental health “check-ins” are a feasible occupational health strategy for paramedics. Participants frequently described the feedback reports as offering insight into their mental health status and helping to contextualize their symptoms, even when those symptoms did not meet thresholds for a positive screen. Other research among Canadian public safety personnel has similarly highlighted the value of routine mental health monitoring, including recent work among Royal Canadian Mounted Police members using short daily or monthly mental health surveys to track well-being indicators over time [17,46]. Emerging data from the RCMP study shows promising relationships between more frequent mental health monitoring and reductions in PTSI symptoms [17], suggesting that monitoring itself can be an intervention that improves mental health. Both findings are important, given the high prevalence of mental disorder symptoms among PSP; however, awareness is most useful when at-risk members can meaningfully action the information afforded by monitoring strategies.
Accessing trauma-informed mental health care has historically been challenging for public safety personnel, including paramedics. Organizational cultures within the public safety professions have often emphasized self-reliance and stigmatized help-seeking, with mental health treatment perceived as a threat to career progression or professional credibility [20,22,23]. Likewise, concerns over the confidentiality of employer-provided support services [47] often mean that PSP primarily rely on informal sources of support following potentially psychologically traumatic events, such as colleagues, family, or friends [24,48,49]. Even PSP who receive mental health training remain extremely reluctant to engage with professional services, accessing mental health professionals only as a ‘last resort’ [50]. Paramedics, in particular, have been found to have generally high levels of mental health knowledge, but are paradoxically disinclined to seek out professional care, with lower service use intentions than other PSP [48].These challenges are compounded by concerns about the availability of culturally competent care, with reports from PSP describing encounters with providers who lack familiarity with the realities of public safety work [51]. In this context, fact that nearly all eligible paramedics participated in the survey and that more than half voluntarily provided identifiable information is striking.
One possible explanation for the apparent willingness of the paramedics to share such sensitive information may be that the participants placed greater trust in a research team that was clearly independent from service leadership and included investigators with lived experience as paramedics. If so, this finding suggests that structural safeguards to ensure confidentiality, coupled with social credibility and distance from management, may be critical to the acceptability of mental health monitoring initiatives in this population. Taken together, these findings suggest that voluntary, culturally informed, and routine mental health monitoring - whether delivered through screening-based feedback or other modalities - may represent a scalable approach to supporting mental health and facilitating timely access to care among public safety personnel. We note, however, that manually inputting and transcribing data in our study slowed the process considerably. Provided data security can be maintained, automation and the use of artificial intelligence software have the potential to streamline this workflow and improve efficiency.
4.1. Limitations
Several limitations should be considered when interpreting these findings. First, the screening instruments used in the study are not diagnostic and positive screens should not be interpreted as equivalent to diagnoses derived from structured clinical interviews. Second, the response rate to the follow-up survey was lower than we hoped and responders differed from non-responders on several demographic characteristics, introducing the possibility of response bias. However, the overall prevalence of PTSD, major depressive disorder, and generalized anxiety disorder symptoms was similar between responders and non-responders, suggesting that symptom burden itself was unlikely to have driven any selection effect that may exist.
Third, although the participating sites reflect common models of paramedic service delivery in Ontario, similarities in operational structure do not necessarily suggest similarity in organizational culture, particularly with respect to mental health. Readers should take care in extrapolating our findings to other settings. Finally, the estimation of the pseudo-number needed to treat rests on assumptions about the counterfactual condition. Specifically, we assumed that participants who received a feedback report but screened negative for PTSD, major depressive disorder, or generalized anxiety disorder would behave similarly to participants who opted not to receive a report. This assumption cannot be empirically tested, as anonymous-stream participants could not be followed longitudinally. Arguably this may make our estimate conservative, given the unexpectedly high proportion of participants who reported already being engaged in mental health care.
5. Conclusions
Of the 995 participants surveyed across two paramedic services, more than 1 in 3 screened positive for PTSD, major depressive disorder, or generalized anxiety disorder, suggesting a persistent and significant mental health burden following the COVID-19 pandemic. Nearly 60% of participants opted to receive a feedback report, and most found the information provided in the report to be helpful in making decisions about their mental health. Paramedics who screened positive for PTSD, major depressive disorder, or generalized anxiety disorder were four times more likely to contact a mental health professional compared with paramedics who screened negative. For every five reports we sent to symptomatic paramedics, one contacted a mental health professional. This suggests that voluntary mental health screening is both feasible and capable of connecting at-risk paramedics to mental health care. Facilitating timely connections to care may help mitigate the downstream workforce impacts associated with untreated mental health conditions, including disability, attrition, and reduced operational capacity.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, JM and EAD; methodology, JM, and EAD, NA.; formal analysis, JM.; investigation, JM, EAD, and NA.; resources, AB, MMM, and WT.; data curation, JM, EAD.; writing—original draft preparation, JM.; writing—review and editing, JM, EAD, AB, MMM, WT, and NA.; supervision, NA.; project administration, JM and EAD.; funding acquisition, JM and EAD. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Peel Regional Paramedic Services (no grant number) and Local 277 of the Ontario Public Services Employees Union (OPSEU/SEFPO) (no grant number).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the University of Toronto Research Ethics Board (protocol number 46717).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data may be made available on a case-by-case basis to interested investigators subject to a privacy review and data sharing agreement.
Acknowledgments
We are grateful to the paramedics from both sites that risk their health, safety, and well-being in service of our communities and who took the time to participate in this study. We wish to express our gratitude and appreciation to the following individuals for their assistance with participant recruitment and data collection: From Peel Regional Paramedic Services, Priya Kakar, Sarah Ropp, and Grace Teves; from Essex-Windsor Emergency Medical Services: Larry Trpkovski, Michella Mollicone, and Slawomir Pulcer. We are grateful to the senior leadership teams of both Peel Regional Paramedic Services and Essex-Windsor Emergency Medical Services for their support of this research. We also thank the Local Executive Committee of the Ontario Public Services Employees Union (OPSEU/SEFPO) Local 277 their support of the study. Finally, we thank Dr. Nick Carleton for providing arms-length conceptual and methodological advice.
Conflicts of Interest
JM is employed by Peel Regional Paramedic Services as a clinician-investigator and received employment income to complete this study. JM is also a bargaining unit member of OPSEU/SEFPO 277. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. NA is employed as a physician with Insight Health Solutions Trillium Health Partners. Information about mental health services offered by Insight Health Solutions was provided to participants from Peel Regional Paramedic Services.
Abbreviations
The following abbreviations are used in this manuscript:
| ACP | Advanced Care Paramedic |
| ANOVA | Analysis of Variance |
| AUDIT | Alcohol Use Disorders Identification Test |
| CAD | Canadian Dollars |
| CME | Continuing Medical Education |
| EW-EMS | Essex-Windsor Emergency Medical Services |
| GAD | Generalized Anxiety Disorder |
| GAD-7 | 7-Item Generalized Anxiety Disorder Scale |
| ISI | Insomnia Severity Index |
| MDD | Major Depressive Disorder |
| NNT | Number Needed to Treat |
| OR | Odds Ratio |
| PCP | Primary Care Paramedic |
| PCL-5 | Posttraumatic Stress Disorder Checklist for DSM-5 |
| PHQ-9 | 9-Item Patient Health Questionnaire |
| PRPS | Peel Regional Paramedic Services |
| PSP | Public Safety Personnel |
| PTSD | Posttraumatic Stress Disorder |
| PTSI | Post-Traumatic Stress Injuries |
| RCMP | Royal Canadian Mounted Police |
| SD | Standard Deviation |
| SPSS | Statistical Package for the Social Sciences |
| WHO | World Health Organization |
| 2SLGBTQI | Two Spirit, Lesbian, Gay, Bisexual, Transgender, Queer/Questioning, Intersex, and additional gender identities |
References
- Public Health Agency of Canada. Federal framework on post-traumatic stress disorder (PTSD): Report to Parliament 2025. 2025.
- Public Safety Canada. Evaluation of the initiatives to address post-traumatic stress injuries (PTSI) among public safety officers. 2023. [Google Scholar]
- Carleton, R.N.; Afifi, T.O.; Taillieu, T.; Turner, S.; Krakauer, R.; Anderson, G.S.; MacPhee, R.S.; Ricciardelli, R.; Cramm, H.A.; Groll, D.; et al. Exposures to potentially traumatic events among public safety personnel in Canada. Canadian Journal of Behavioural Science / Revue canadienne des sciences du comportement 2019, 51, 37–52. [Google Scholar] [CrossRef]
- Carleton, R.N.; Afifi, T.O.; Turner, S.; Taillieu, T.; Duranceau, S.; LeBouthillier, D.M.; Sareen, J.; Ricciardelli, R.; MacPhee, R.; Groll, D.; et al. Mental disorder symptoms among public safety personnel in Canada. Can J Psychiatry 2018, 63, 54–64. [Google Scholar] [CrossRef]
- Tavares, W.; Kaas-Mason, S.; Spearen, C.; Kedzierski, N.; Watts, J.; Moran, P.; Leyenaar, M.S. Redesigning paramedicine systems in Canada with “IMPACC”. Paramedicine 2024. [Google Scholar] [CrossRef]
- Li, K.; Frumkin, A.; Bi, W.G.; Magrill, J.; Newton, C. Biopsy of Canada's family physician shortage. Fam Med Community Health 2023, 11. [Google Scholar] [CrossRef]
- Hoell, A.; Kourmpeli, E.; Dressing, H. Work-related posttraumatic stress disorder in paramedics in comparison to data from the general population of working age. A systematic review and meta-analysis. Front Public Health 2023, 11, 1151248. [Google Scholar] [CrossRef]
- Chan, S.C.; Jenkins, J.L.; Zhang, A.; Everly, G.S., Jr.; Roemer, E.C.; Hsu, E.B.; Han, G.; Sharma, R.; Asenso, E., Jr.; Bidmead, D.; et al. Incidence, Prevalence, and Severity of Mental Health Issues Among Emergency Medical Service Clinicians: A Systematic Review and Meta-Analysis. The Journal of emergency medicine 2025, 79, 427–442. [Google Scholar] [CrossRef]
- McGlynn, C.; Choudhury, A. Mental Health Safety Challenges Among Pre-Hospital Emergency Medical Service Providers: A Scoping Review. IISE Trans Occup Ergon Hum Factors 2025, 1–32. [CrossRef]
- Carleton, R.N.; Afifi, T.O.; Turner, S.; Taillieu, T.; LeBouthillier, D.M.; Duranceau, S.; Sareen, J.; Ricciardelli, R.; MacPhee, R.S.; Groll, D.; et al. Suicidal ideation, plans, and attempts among public safety personnel in Canada. Canadian Psychology/Psychologie canadienne 2018, 59, 220–231. [Google Scholar] [CrossRef]
- Angehrn, A.; Teale Sapach, M.J.N.; Ricciardelli, R.; MacPhee, R.S.; Anderson, G.S.; Carleton, R.N. Sleep Quality and Mental Disorder Symptoms among Canadian Public Safety Personnel. Int J Environ Res Public Health 2020, 17. [Google Scholar] [CrossRef] [PubMed]
- Carleton, R.N.; Afifi, T.O.; Turner, S.; Taillieu, T.; El-Gabalawy, R.; Sareen, J.; Asmundson, G.J.G. Chronic pain among public safety personnel in Canada. Canadian Journal of Pain 2017, 1, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Carleton, R.N.; Afifi, T.O.; Taillieu, T.; Turner, S.; El-Gabalawy, R.; Sareen, J.; Asmundson, G.J.G. Anxiety-related psychopathology and chronic pain comorbidity among public safety personnel. J Anxiety Disord 2018, 55, 48–55. [Google Scholar] [CrossRef]
- Edgelow, M.; Brar, S.; Fecica, A. Worker's compensation usage and return to work outcomes for Ontario public safety personnel with mental stress injury claims: 2017–2021. Frontiers in Organizational Psychology 2023, 1. [Google Scholar] [CrossRef]
- Agarwal, G.; Pirrie, M.; Angeles, R.; Marzanek, F.; Paterson, J.M.; Nguyen, F.; Thabane, L. Community Paramedicine Program in Social Housing and Health Service Utilization: A Cluster Randomized Clinical Trial. JAMA Netw Open 2024, 7, e2441288. [Google Scholar] [CrossRef]
- Agarwal, G.; Angeles, R.; Brar, J.; Pirrie, M.; Marzanek, F.; McLeod, B.; Thabane, L. Effectiveness of the community paramedicine at home (CP@home) program for frequent users of emergency medical services in Ontario: a randomized controlled trial. BMC Health Serv Res 2024, 24, 1462. [Google Scholar] [CrossRef] [PubMed]
- Teckchandani, T.A.; Shields, R.E.; Andrews, K.L.; Nisbet, J.; Afifi, T.O.; Asmundson, G.J.G.; Maguire, K.Q.; Jamshidi, L.; Neary, J.P.; Krätzig, G.P.; et al. Monthly Mental Health Self-Monitoring and Positive Changes in Mental Health Disorder Symptoms Scores Among Royal Canadian Mounted Police Cadets. International Journal of Cognitive Behavioral Therapy 2025, 18, 425–454. [Google Scholar] [CrossRef]
- Handley, K.; Carleton, R.N.; Deschênes, A.A.; Devlin, J.; Kamkar, K.; Lee, V.; Mackoff, R.; Martin-Doto, C.A.; Shields, N.; Stockdale, K.; et al. Safeguard programs and mandatory mental health checks in Canadian police agencies: history, trends, and future directions. Journal of Community Safety and Well-Being 2025, 10, 38–42. [Google Scholar] [CrossRef]
- Corthesy-Blondin, L.; Genest, C.; Dargis, L.; Bardon, C.; Mishara, B.L. Reducing the impacts of exposure to potentially traumatic events on the mental health of public safety personnel: A rapid systematic scoping review. Psychol Serv 2022, 19, 80–94. [Google Scholar] [CrossRef] [PubMed]
- Newell, C.J.; Ricciardelli, R.; Czarnuch, S.M.; Martin, K. Police staff and mental health: barriers and recommendations for improving help-seeking. Police Practice and Research 2021, 23, 111–124. [Google Scholar] [CrossRef]
- Howe, E.; Czarnuch, S.; Ricciardelli, R.; Leduc, N. Exploring Canadian Public Safety Communicator Mental Health Help-Seeking Behaviors. New Solut 2025, 10482911251326648. [Google Scholar] [CrossRef]
- Ricciardelli, R.; Carleton, R.N.; Mooney, T.; Cramm, H. “Playing the system”: Structural factors potentiating mental health stigma, challenging awareness, and creating barriers to care for Canadian public safety personnel. Health 2020, 24, 259–278. [Google Scholar] [CrossRef]
- Ricciardelli, R.; Andres, E.; Kaur, N.; Czarnuch, S.; Carleton, R.N. Fit for public safety: Informing attitudes and practices tied to the hiring of public safety personnel. Journal of Workplace Behavioral Health 2019, 35, 14–36. [Google Scholar] [CrossRef]
- Donnelly, E.A.; Bradford, P.; Davis, M.; Hedges, C.; Klingel, M. Predictors of posttraumatic stress and preferred sources of social support among Canadian paramedics. Cjem 2016, 18, 205–212. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.; Witte, T.K.; Domino, J.L. The posttraumatic stress disorder checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. Journal of Traumatic Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J. The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder. Arch Intern Med 2006, 1666, 1092–1097. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Medicine 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Saunders, J.B.; Aasland, O.G.; Fabor, T.F.; De La Fuente, J.R.; Grant, M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Survey on COVID-19 and mental health, February to May 2023. 2023. [Google Scholar]
- Mausz, J.; Donnelly, E.A.; Moll, S.; Harms, S.; McConnell, M. Mental Disorder Symptoms and the Relationship with Resilience among Paramedics in a Single Canadian Site. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef]
- Wortmann, J.H.; Jordan, A.H.; Weathers, F.W.; Resick, P.A.; Dondanville, K.A.; Hall-Clark, B.; Foa, E.B.; Young-McCaughan, S.; Yarvis, J.S.; Hembree, E.A.; et al. Psychometric analysis of the PTSD Checklist-5 (PCL-5) among treatment-seeking military service members. Psychol Assess 2016, 28, 1392–1403. [Google Scholar] [CrossRef] [PubMed]
- McAlister, F.A. The "number needed to treat" turns 20--and continues to be used and misused. CMAJ 2008, 179, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nursing and Health Sciences 2013, 15, 398–405. [Google Scholar] [CrossRef]
- Charmaz, K. The logic of grounded theory coding practices and initial coding. In Constructing Grounded Theory, 2nd ed.; Seaman, J., Ed.; Sage Publications: London, 2014; pp. 109–137. [Google Scholar]
- Charmaz, K. Focused coding and beyond. In Constructing Grounded Theory, 2nd ed.; Seaman, J., Ed.; Sage Publications: London, 2014; pp. 138–161. [Google Scholar]
- Singh, J.; Poon, D.E.; Alvarez, E.; Anderson, L.; Verschoor, C.P.; Sutton, A.; Zendo, Z.; Piggott, T.; Apatu, E.; Churipuy, D.; et al. Burnout among public health workers in Canada: a cross-sectional study. BMC Public Health 2024, 24, 48. [Google Scholar] [CrossRef]
- de Wit, K.; Tran, A.; Clayton, N.; Seeburruth, D.; Lim, R.K.; Archambault, P.M.; Chan, T.M.; Rang, L.C.F.; Gray, S.; Ritchie, K.; et al. A Longitudinal Survey on Canadian Emergency Physician Burnout. Annals of emergency medicine 2024, 83, 576–584. [Google Scholar] [CrossRef]
- Gajjar, J.; Pullen, N.; Li, Y.; Weir, S.; Wright, J.G. Impact of the COVID-19 pandemic upon self-reported physician burnout in Ontario, Canada: evidence from a repeated cross-sectional survey. BMJ Open 2022, 12, e060138. [Google Scholar] [CrossRef]
- Sporer, C. Burnout in emergency medical technicians and paramedics in the USA. International Journal of Emergency Services 2021, 10, 366–389. [Google Scholar] [CrossRef]
- Lebeaut, A.; Zegel, M.; Leonard, S.J.; Healy, N.A.; Anderson-Fletcher, E.A.; Vujanovic, A.A. COVID-19-Related Medical Vulnerability and Mental Health Outcomes Among US First Responders. J Occup Environ Med 2023, 65, e283–e289. [Google Scholar] [CrossRef]
- Ebben, R.H.A.; Woensdregt, T.; Wielenga-Meijer, E.; Pelgrim, T.; de Lange, A.; Berben, S.A.A.; Vloet, L.C.M. The impact of COVID-19 on the mental health and well-being of ambulance care professionals: A rapid review. PLoS One 2023, 18, e0287821. [Google Scholar] [CrossRef] [PubMed]
- Soto-Camara, R.; Garcia-Santa-Basilia, N.; Onrubia-Baticon, H.; Cardaba-Garcia, R.M.; Jimenez-Alegre, J.J.; Reques-Marugan, A.M.; Molina-Oliva, M.; Fernandez-Dominguez, J.J.; Matellan-Hernandez, M.P.; Morales-Sanchez, A.; et al. Psychological Impact of the COVID-19 Pandemic on Out-of-Hospital Health Professionals: A Living Systematic Review. J Clin Med 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Piotrowski, A.; Makarowski, R.; Predoiu, R.; Predoiu, A.; Boe, O. Resilience and Subjectively Experienced Stress Among Paramedics Prior to and During the COVID-19 Pandemic. Front Psychol 2021, 12, 664540. [Google Scholar] [CrossRef]
- Statistics Canada. Survey on COVID-19 and mental health, February to May 2021. 2021. [Google Scholar]
- Shields, R.E.; Teckchandani, T.A.; Asmundson, G.J.G.; Nisbet, J.; Krakauer, R.L.; Andrews, K.L.; Maguire, K.Q.; Jamshidi, L.; Afifi, T.O.; Lix, L.M.; et al. Daily survey participation and positive changes in mental health symptom scores among Royal Canadian Mounted Police Cadets. Front Psychol 2023, 14, 1145194. [Google Scholar] [CrossRef] [PubMed]
- Moghimi, E.; Knyahnytska, Y.; Omrani, M.; Nikjoo, N.; Stephenson, C.; Layzell, G.; Frederic Simpson, A.I.; Alavi, N. Benefits of Digital Mental Health Care Interventions for Correctional Workers and Other Public Safety Personnel: A Narrative Review. Front Psychiatry 2022, 13, 921527. [Google Scholar] [CrossRef] [PubMed]
- Krakauer, R.L.; Stelnicki, A.M.; Carleton, R.N. Examining Mental Health Knowledge, Stigma, and Service Use Intentions Among Public Safety Personnel. Front Psychol 2020, 11, 949. [Google Scholar] [CrossRef]
- Kaur, N.; Ricciardelli, R.; Fletcher, A.; Carleton, R.N. ‘You are safe. You are not alone:’ gender and Social Support Coping (SSC) in public safety personnel. Journal of Gender Studies 2021, 1–16. [Google Scholar] [CrossRef]
- Carleton, R.N.; Afifi, T.O.; Turner, S.; Taillieu, T.; Vaughan, A.D.; Anderson, G.S.; Ricciardelli, R.; MacPhee, R.S.; Cramm, H.A.; Czarnuch, S.; et al. Mental health training, attitudes toward support, and screening positive for mental disorders. Cogn Behav Ther 2019, 49, 1–19. [Google Scholar] [CrossRef]
- Edgelow, M.; Legassick, K.; Novecosky, J.; Fecica, A. Return to Work Experiences of Ontario Public Safety Personnel with Work-Related Psychological Injuries. J Occup Rehabil 2023, 33, 796–807. [Google Scholar] [CrossRef]
Figure 1.
Participant flow from both sites during the study.
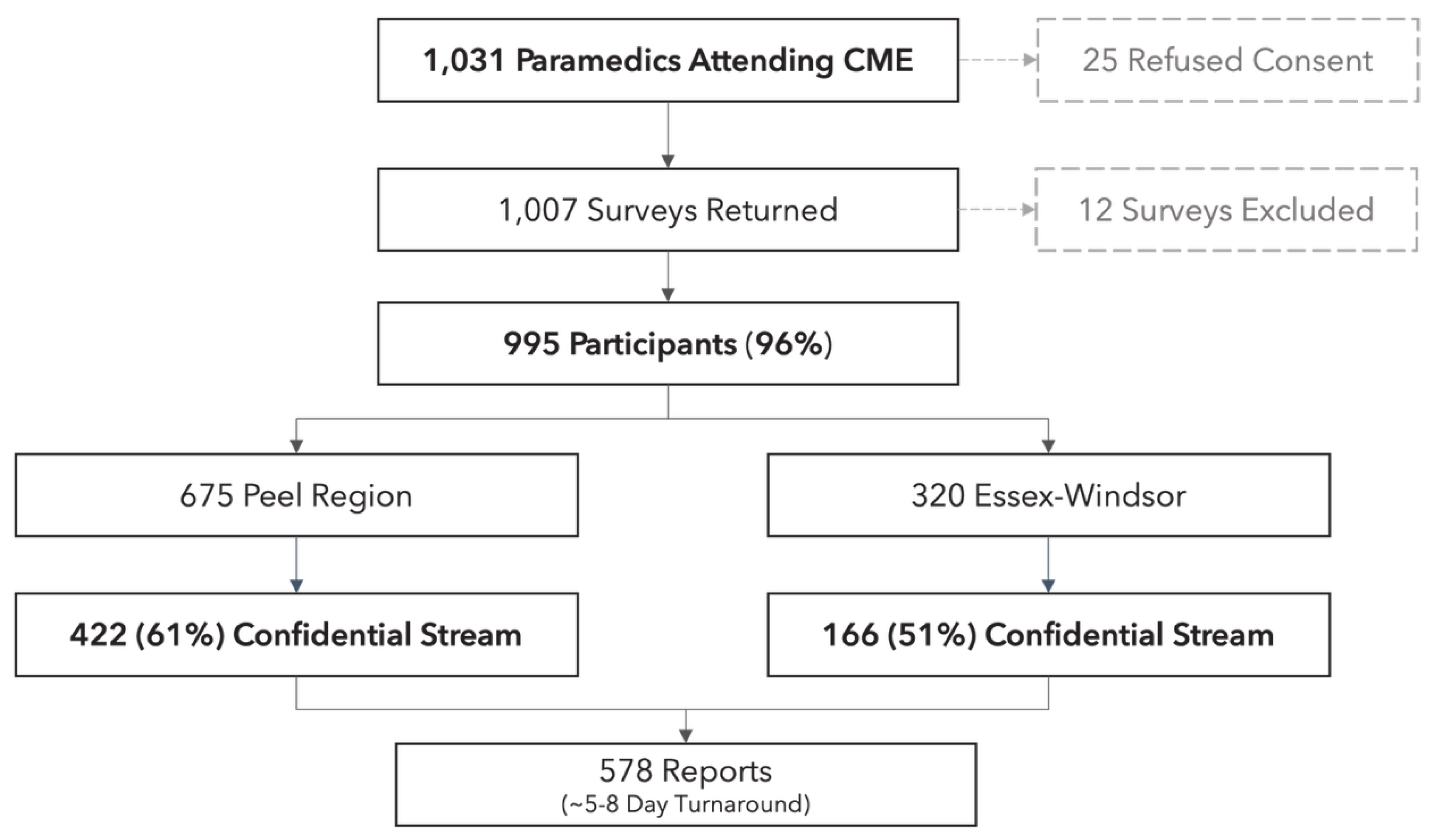

Table 1.
Detailed participant demographic details, reported as n(%), unless otherwise indicated. CP = Community Paramedicine; PCP = Primary Care Paramedic; ACP = Advanced Care Paramedic. †Differs between sites at p<0.05; *Differs between men and women (within site) at p<0.05; **Differs between men and women (within site) at p<0.001.
Table 1.
Detailed participant demographic details, reported as n(%), unless otherwise indicated. CP = Community Paramedicine; PCP = Primary Care Paramedic; ACP = Advanced Care Paramedic. †Differs between sites at p<0.05; *Differs between men and women (within site) at p<0.05; **Differs between men and women (within site) at p<0.001.
| Parameter | All Sites | Peel Region | Essex-Windsor | ||||
| Overall | Men | Women | Overall | Men | Women | ||
| Age (Mean [SD]) | 36.1 (9.1) | 35.9 (8.7) | 36.4 (8.7) | 35.0 (8.6)* | 36.4 (9.8) | 37.6 (10.1) | 34.7 (9.0) |
| Confidential Stream | 588 (59.0) | 422 (62.5) | 246 (36.4) | 172 (25.4) | 166 (51.8) † | 107 (56.0) | 57 (44.5)* |
| Race (White) | 719 (72.9) | 437 (65.4) | 254 (61.8) | 182 (71.3)* | 282 (88.6) † | 162 (85.2) | 120 (93.7)* |
| In a Relationship | 732 (73.5) | 491 (72.8) | 316 (76.3) | 174 (67.4)* | 241 (75.7) | 152 (80.4) | 89 (68.9)* |
| 2SLGBTQI+ | 71 (7.1%) | 48 (7.1) | 19 (4.5) | 27 (10.4)** | 23 (7.2) | 8 (4.2) | 15 (11.6)* |
| Education Certificate Diploma Undergraduate Graduate |
46 (4.6) 583 (58.5) 331 (33.2) 26 (2.6) |
23 (3.4) 340 (50.5) 282 (41.9) 24 (3.5) |
19 (4.6) 218 (52.7) 157 (38.0) 15 (3.6) |
4 (1.5) 121 (46.8) 124 (48) 9 (3.4) |
23 (7.2) 242 (76.3) 49 (15.4) † 2 (0.6) |
14 (7.4) 145 (76.7) 28 (14.8) 1 (0.5) |
9 (7.0) 97 (75.7) 21 (16.4) 1 (0.7) |
| Full-Time Employment | 729 (73.2) | 505 (74.9) | 306 (73.9) | 197 (76.3) | 224 (70.) | 139 (72.7) | 85 (65.8) |
| Current Role Front-Line Leadership CP |
920 (92.4) 56 (5.6) 63 (6.3) |
633 (94) 32 (4.7) 27 (4.0) |
382 (92.4) 26 (6.2) 10 (2.4) |
249 (96.5) 6 (2.3)* 17 (6.5)* |
286 (90.5) 24 (7.6) 36 (113) † |
166 (88.2) 18 (10.7) 18 (9.4) |
120 (93.7) 6 (4.6) 18 (14.2) |
| Clinical Certification PCP ACP |
733 (73.6) 256 (25.7) |
462 (68.6) 211 (31.3) |
264 (63.6) 151 (36.3) |
198 (76.4)** 60 (23.2) |
275 (85.9) 45 (14.0) † |
154 (80.6) 37 (19.3) |
121 (93.7)** 8 (6.2) |
| Experience (Mean [SD]) Recruit Early Career Mid-Career Senior Career |
11 (8.7) 154 (15.5) 167 (16.8) 540 (54.2) 128 (12.9) |
10.4 (8.1) 104 (15.6) 119 (17.8) 372 (55.8) 71 (10.6) |
10.8 (8.2) 57 (13.9) 76 (18.5) 237 (57.8) 40 (9.7) |
9.9 (7.9) 47 (18.3) 43 (16.7) 135 (52.7) 31 (12.1) |
12.1 (9.7) † 50 (15.6) 48 (15.0) 165 (51.6) 57 (17.8) † |
13.0 (10.1) 22 (11.5) 27 (14.1) 102 (53.4) 40 (20.9) |
10.7 (8.9) 28 (21.7) 21 (16.2)* 63 (48.4)* 17 (13.1) |
Table 2.
Follow-up survey questions and responses stratified by site. Questions 1 and 2 used an anchored Likert scale (1 = Do Not Agree at all; 7 = Agree Entirely). Response options for Questions 2, 3, and 4 were yes/no.
Table 2.
Follow-up survey questions and responses stratified by site. Questions 1 and 2 used an anchored Likert scale (1 = Do Not Agree at all; 7 = Agree Entirely). Response options for Questions 2, 3, and 4 were yes/no.
| Question | All Sites | Peel Region | Essex-Windsor |
| The report was useful in helping you make decisions about your mental health (mean [SD]) | 5.6 (1.1) | 5.5 (1.1) | 5.7 (1.0) |
| The information in the report was consistent with how you felt about your mental health (mean [SD]) | 5.8 (0.9) | 5.9 (0.9) | 5.7 (0.9) |
| Did you access any of the resources provided with your report? (n [%]) | Yes = 30 (13.5%) | Yes = 23 (14.8%) | Yes = 7 (10.6%) |
| Did you contact a mental health professional because of your report? (n [%]) | Yes = 33 (14.9%) | Yes = 24 (15.4%) | Yes = 9 (13.6%) |
| Do you intend to contact a mental health professional in the future because of your report? (n [%]) | Yes = 75 (33.9%) | Yes = 57 (36.7%) | Yes = 18 (27.2%) |
Table 3.
Qualitative content analysis of free-text comments collected from follow-up survey participants.
Table 3.
Qualitative content analysis of free-text comments collected from follow-up survey participants.
| Theme | N | Description | Sample Quotes |
| Already Receiving Care | 30 | Participant descriptions of existing relationships with practitioners from whom they are accessing mental health care | “(The report) was essentially a confirmation of what I already knew. Fortunately, I have a good therapist I am seeing already” “I shared the report with my current (mental healthcare provider). We discussed it. They agreed with (the content) and how it was representative of where I am with my mental health” “I have been receiving mental health support since our benefits increased. This survey was great. … Thank you for taking care of us.” “I suspected I could benefit from therapy. I have a provider but have not had a session in a while. I have since gone back for regular visits.” |
| Gaining Insight | 16 | Comments from the participants about how the mental health reports provided them actionable insights into their mental health and well-being | “This was very informative and a good self-reflection. Thank you” “Interesting to see what you learn about yourself when you are forced to do some introspection. Maybe some habits aren’t healthy” “As a new paramedic who is just starting her career, I wanted to understand my risk factors and be proactive about my mental health.” “I have been thinking about seeing a professional for some time and this will be one of the things that eventually leads me to it.” “My results informed me that I was at severe risk for insomnia … I (saw) my family doctor. I’m now medicated to help me sleep and I’m feeling clearer every day” “The report was eye opening for me. Despite feeling well mentally, I’ve since been in contact with a psychologist. I’ve also encouraged others to do the same. Thank you for doing this.” |
| Expressing Support for the Research | 29 | Expressions of gratitude and support for the research. Some participants also commented that the survey should be more in-depth or offered regularly as a form of “mental health check-in” |
“Great idea to conduct (this) survey and share its findings with the participants” “Please continue doing this important work” “Thanks so much for looking into our minds, hearts, and souls” “Thank you for improving mental health support in (our service)” “It was a great experience to finally sit down and reflect on my own mental health with some sort of screening tool/assessment and not just wonder what my mental health status might be.” “Thank you for the report. Taken well to heart” “I wish studies like this were regularly conducted in our line of work as the benefits are immeasurable” “I think this would be a good screening tool for all employees to take and have follow-up if needed” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



