Submitted:
04 February 2026
Posted:
05 February 2026
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The clinical features and risk factors of post‑acute sequelae of SARS‑CoV‑2 infection (PASC) in children remain incomplete. This study aims to clarify the manifestations and identify predictors of PASC in pediatric patients previously hospitalized for COVID‑19. Methods: We conducted this retrospective cohort study at the China Medical University Children’s Hospital in Taiwan, including 143 children aged 3-18 hospitalized for the acute COVID-19 during the Omicron pandemic from April 2022 to July 2023. PASC was assessed through phone calls, online survey, and in-person follow-ups. Data encompassing demographics, clinical presentations, laboratory results, and acute-phase treatment were collected and compared between children with and without PASC. Each child was assigned total clinical scores based on the acute-phase symptoms and treatment. We evaluated the association of the total clinical scores with PASC among study children. The receiver operating characteristic (ROC) analysis was used to determine the optimal cutoff for total clinical scores, which best differentiated occurrence of PASC. Results: Among the 143 discharged children, 35.7% (n = 51) developed PASC. Children with PASC tended to be older (mean age: 7.6 vs. 6.3 years, p = 0.05) and greater body weight (29.1 vs. 23.7 kg, p = 0.05). PASC children exhibited higher reverse transcriptase-polymerase chain reaction (RT-PCR) cycle threshold (Ct) values (17.1 vs. 14.2, p = 0.04) during the acute phase than those without PASC. There were no significant disparities in other laboratory results, length of intensive care unit (ICU) stays, bacterial coinfections, oxygen supplementation, and medication usage between two groups. Notably, compared to the control group, the total clinical scores were significantly higher in the PASC group (37.9 vs. 31.5, p = 0.02), with an optimal cutoff value of 37.7 yielding an area under the curve (AUC) of 0.70. Conclusions: This study identified a significant proportion of children developing PASC following hospitalization for acute COVID-19. Older age, greater body weight, and larger RT-PCR Ct values during the acute phase emerged as potential risk factors for developing PASC. Moreover, the clinical scoring system constructed in this study may help to predict the risk of developing PASC after discharge.
Keywords:
clinical features
; children
; COVID-19
; hospitalization
; post-acute sequelae of SARS-CoV-2 infection
; risk factors
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, which emerged in late 2019, has rapidly become a global pandemic affecting individuals of all age groups [1]. Initially, pediatric patients appeared to experience milder forms of coronavirus disease 2019 (COVID-19). However, increasing evidence demonstrates that pediatric patients with persistent symptoms after recovering from the acute infection phase, known as post-acute sequelae of SARS-CoV-2 infection (PASC) or long COVID [2,3]. PASC refers to patients with persist clinical symptoms occurring beyond four weeks following initial acute infection which affects multiple organ systems and significantly impair quality of life [4,5,6].
A meta-analysis of adult studies has demonstrated that the risk of developing PASC is closely related to the severity of the initial COVID-19 infection. The study has identified that age, hospitalization due to initial COVID-19 infection, and various comorbidities, such as diabetes, obesity, and cardiovascular disease, may serve as potential predictors [7]. While extensively documented in adults, limited studies have assessed the incidence, risk factors, and clinical manifestations of PASC in pediatric populations, and heterogeneous in methodology and ethnicities, making conclusive evidence challenging [8,9]. Several studies have identified potential risk factors, including age, obesity, and pre-existing comorbid conditions, affect the development of PASC among children [5,10]. Furthermore, hospitalization during the acute phase has been recognized as a pivotal risk factor, suggesting a link between the severity of initial COVID-19 and PASC in children [11,12]. Nonetheless, data addressing post-acute sequelae among hospitalized pediatric populations remain sparse [11,12].
Although age, underlying chronic conditions, and the overall severity of the initial illness have been proposed as potential predictors, these associations with PASC remain inconclusive [10,13]. As such, establishing clear risk profiles and understanding the spectrum of symptomatology among pediatric patients with PASC is crucial for enabling clinicians to identify vulnerable children and implement targeted post-discharge monitoring.
This study aims to evaluate clinical manifestations and identify risk factors associated with PASC in a pediatric cohort previously hospitalized due to acute COVID-19; and develop a composite clinical scoring system via integrating acute-phase clinical features to better predict subsequent risk of PASC among children with severe initial illness in acute COVID-19.
Methods
Data Sources and Study Cohort
This retrospective cohort study was conducted at the China Medical University Children's Hospital (CMUCH), a tertiary medical center located in central Taiwan. In this study, we enrolled children aged 3 to 18 years who were hospitalized with acute COVID-19 from April 2022 to July 2023 during the Omicron wave. Diagnosis of acute COVID-19 was confirmed by reverse transcriptase-polymerase chain reaction (RT-PCR) or rapid antigen testing (ART). RT-PCR and ART were performed at the time of acute illness onset, when patients first presented with COVID-19–related symptoms. No serial PCR tests were performed after symptom resolution or discharge, as repeated sampling was not part of the institutional protocol for pediatric patients. The ART used in our hospital was the Abbott Panbio™ COVID-19 Antigen Rapid Test (Abbott Diagnostics, USA), which detects SARS-CoV-2 nucleocapsid protein antigen from nasopharyngeal swabs and has been authorized by the Taiwan Food and Drug Administration (TFDA) for clinical use. Hospitalization was indicated for children with acute illness requiring inpatient management, such as dehydration needing intravenous fluids, respiratory distress or hypoxemia, febrile seizures or other neurological symptoms, suspected bacterial co-infection, or significant comorbid or immunocompromised conditions. Following hospital discharge, participants were monitored for PASC through phone calls, online survey, and in-person visits. PASC was defined as the persistence of symptoms beyond four weeks after recovery from acute COVID-19, consistent with major pediatric studies and intended to capture early post-acute manifestations in children [6,12,14,15]. The PASC evaluation protocol was established in December 2022. Patients hospitalized from April to November 2022 were assessed retrospectively via phone calls and online surveys post-discharge, whereas those hospitalized from December 2022 onward were evaluated prospectively during routine follow-up visits or via phone or online if they did not return.
PASC was evaluated using an institutional questionnaire, the “Post-COVID-19 Physical and Psychological Evaluation Questionnaire”, which was administered uniformly via telephone, online, or in-person at least 4 weeks after discharge. The questionnaire was used to record post-COVID-19 symptoms across multiple domains and to compare them with the child’s pre-COVID-19 status, which helped distinguish PASC-related symptoms from long-standing, unchanged conditions. Assessments were conducted by trained research nurses (via phone or online) or attending pediatricians (in person), and the final determination of PASC was confirmed by pediatric infectious disease specialists. Only new or significantly intensified symptoms persisting for more than four weeks were classified as PASC. Children with persistent or evolving symptoms underwent additional evaluations at eight and/or twelve weeks; no routine follow-up was conducted beyond twelve weeks. The flowchart illustrating the enrollment process in this study is provided in Figure E1. The study was approved by the Institutional Review Board of CMUH (CMUH113-REC1-126), and all study procedures adhered to the applicable guidelines and regulations.
Figure E1.
Flow chart of subject identification.
Study Outcome
After being discharged following acute COVID-19 infection, children were stratified into two groups based on the results of the follow-up investigation: those with PASC and those without. Detailed clinical data during hospitalization were collected from electronic medical records (EMR), including basic demographics, COVID-19 vaccination status, underlying comorbidities, symptoms at admission, disease severity, laboratory test results, supportive therapies, administered medications, and any complications. Diagnosis of PASC was based on a comprehensive follow-up process that included telephone interviews, online surveys, and in-person evaluations. Any child reported one or more persistent symptoms more than four weeks beyond the acute COVID period was classified as having PASC.
Clinical Score Assignment
To comprehensively evaluate the diverse clinical manifestations during the acute COVID-19 phase, we constructed a composite clinical scoring system using EMR data extracted from the study children. In this scoring system, all symptoms were categorized into five distinct domains with total score of 100 points, assigning up to 20 points of each domain (Table E1). The five domains are defined as follows: 1.) the respiratory system domain includes symptoms such as cough, rhinorrhea, sore throat, sputum, and dyspnea; 2.) the gastrointestinal system domain incorporates symptoms as vomiting, diarrhea, and abdominal pain; 3.) the neurologic system domain covers a range of neurological symptoms, including seizures, with the presence of any neurological symptom recorded as positive; 4.) the general appearance domain is characterized by features such as anorexia, fatigue, myalgia, and fever; and 5.) the medication use domain specifically addresses the use of antibiotics during the acute phase.
This scoring system allowed for simultaneous consideration of multifaceted clinical conditions during the acute phase and facilitated the analysis of their relationship with the risk of developing PASC.

Table E1.
Scoring assignment of clinical categories during COVID-19 acute phase.
| Clinical category | Score |
| Respiratory system | 20 |
| Cough | 4 |
| Rhinorrhea | 4 |
| Sore throat | 4 |
| Sputum | 4 |
| Dyspnea | 4 |
| Gastrointestinal system | 20 |
| Vomiting | 6.67 |
| Diarrhea | 6.67 |
| Abdominal pain | 6.67 |
| Neurologic system | 20 |
| Neurological symptoms | 20 |
| General appearance | 20 |
| Anorexia | 5 |
| Fatigue | 5 |
| Myalgia | 5 |
| Fever | 5 |
| Medication | 20 |
| Antibiotic use | 20 |
| Total score | 100 |
Statistical Analysis
For baseline demographic and clinical characteristics, continuous variables were reported as means and standard deviations (SD) which were tested by Student’s t test, while discrete variables were reported as counts and percentages which were tested by the chi-squared test.
Student’s t test was used to compare total clinical scores and the scores from each clinical domain between PASC cases and controls. We subsequently conducted logistic regression with adjustment of age and body weight to estimate the association of total clinical scores with PASC among study children. The receiver operating characteristic (ROC) analysis was used to determine the optimal cutoff (the value with optimal sensitivity and specificity) for total clinical scores, representing the best differentiated occurrence of PASC. The discriminatory ability was captured by the area under the curve (AUC). Generally, AUC equal to or greater than 0.7 is considered satisfactory for predictive models [16].
Statistical significance was defined as a p-value less than 0.05 or 95% confidence intervals (CIs) that did not include the null value of one. All analyses were performed using SAS version 9.4 for Windows (SAS Institute, Cary, NC, USA).
Results
A total of 143 hospitalized children with confirmed SARS-CoV-2 infection (mean age, 6.8 ± 3.8 years; 85 boys, 59.4%) were included. COVID-19 infection was confirmed by either real-time RT-PCR (n = 66) or antigen rapid test (ART, n = 77). Among the 66 children with RT-PCR confirmation, all samples were collected at acute presentation (64 in the emergency department, 2 in outpatient clinics prior to admission). Table 1 presents the demographic and clinical characteristics of the study children (51 PASC cases and 92 controls). Fever characteristics during acute illness were similar between PASC cases and controls (peak temperature 39.5 ± 0.8 °C in both, p = 0.96; duration 3.2 ± 1.9 vs. 2.6 ± 1.9 days, p = 0.07; Table 1). Significant differences were observed in age (7.6 ± 4.3 vs. 6.3 ± 3.4 years, p = 0.05), weight (29.1 ± 16.4 vs. 23.7 ± 12.8 kg, p = 0.05) and reverse transcriptase-polymerase chain reaction (RT-PCR) cycle threshold (Ct) value (17.1 ± 6.1 vs. 14.2 ± 3.8, p = 0.04) between PASC cases and controls (Table 1).
The distributions of clinical features during the acute phase between PASC cases and controls were shown in Figure 1 and Table E2. We examined the associations of clinical features and biomedical data during the acute phase, separately, with PASC in the study children. Table 2 and Table E3 summarize the in-hospital management characteristics between children with and without PASC. Most treatment and care-related parameters during hospitalization were comparable between the two groups. Among the study population, 13 children (9.1%) received remdesivir and 3 (2.1%) received paxlovid during hospitalization. Remdesivir and paxlovid were used more often in children with PASC than in controls (15.7% vs. 5.4%, p = 0.08; 3.9% vs. 1.1%, p = 0.60), but these differences did not reach statistical significance. When remdesivir and paxlovid were considered together as any antiviral therapy, use was significantly more frequent in PASC cases than in controls (19.6% vs. 6.5%, p = 0.02). Table 3 shows that total clinical scores from five composite clinical domains during the acute phase were positively associated between PASC cases and controls (adjusted odds ratios (AOR) = 1.03; 95% CI: 1.00-1.05).
Table 2.
Association between clinical features during the acute phase with PASC in 143 children with hospitalized COVID-19 infection.
Table 2.
Association between clinical features during the acute phase with PASC in 143 children with hospitalized COVID-19 infection.
|
Total (N=143) |
Cases (N=51) |
Control (N=92) | P | |
| ICU, n (%), day | 0.52 | |||
| 0 | 128 (89.5) | 44 (86.3) | 84 (91.3) | |
| 1−7 | 12 (8.4) | 5 (9.8) | 7 (7.6) | |
| 8−14 | 1 (0.7) | 1 (2.0) | 0 (0.0) | |
| ≥ 15 | 2 (1.4) | 1 (2.0) | 1 (1.1) | |
| HFNC oxygen, n (%) | 0.10 | |||
| No | 136 (95.1) | 46 (90.2) | 90 (97.8) | |
| Yes | 7 (4.9) | 5 (9.8) | 2 (2.2) | |
| Oxygen use, n (%) | 0.33 | |||
| No | 133 (93.0) | 46 (90.2) | 87 (94.6) | |
| Yes | 10 (7.0) | 5 (9.8) | 5 (5.4) | |
| Antibiotic use, n (%) | 0.15 | |||
| No | 95 (66.4) | 30 (58.8) | 65 (70.7) | |
| Yes | 48 (33.6) | 21 (41.2) | 27 (29.3) | |
| Bacteria co-infection, n (%) | 0.42 | |||
| No | 136 (95.1) | 50 (98.0) | 86 (93.5) | |
| Yes | 7 (4.9) | 1 (2.0) | 6 (6.5) | |
| Dexamethasone, n (%) | 1.00 | |||
| No | 136 (95.1) | 49 (96.1) | 87 (94.6) | |
| Yes | 7 (4.9) | 2 (3.9) | 5 (5.4) | |
| IVIG, n (%) | 0.13 | |||
| No | 139 (97.2) | 48 (94.1) | 91 (98.9) | |
| Yes | 4 (2.8) | 3 (5.9) | 1 (1.1) | |
| Antiviral agents,n (%) | ||||
| Remdesivir | 13 (9.1%) | 8 (15.7%) | 5 (5.4%) | 0.08 |
| Paxlovid | 3 (2.1%) | 2 (3.9%) | 1 (1.1%) | 0.60 |
| Remdesivir or Paxlovid | 16 (11.2%) | 10 (19.6%) | 6 (6.5%) | 0.02 |
Abbreviation: PASC: post-acute sequelae of SARS-CoV-2 infection; ICU: intensive care unit; HFNC: high-flow nasal cannula; IVIG: intravenous immunoglobulin. Bacterial co-infection (n = 7): Campylobacter jejuni enteritis (n = 2) and Salmonella spp. enteritis (n = 2) by gastrointestinal multiplex PCR; Escherichia coli UTI (n = 2) by urine culture; Mycoplasma pneumoniae bronchitis (n = 1) by IgM serology. Blood cultures were performed in all 143 patients; all were negative.”.
Table E2.
Association between clinical symptoms during the acute phase with PASC in 143 children with hospitalized COVID-19 infection.
Table E2.
Association between clinical symptoms during the acute phase with PASC in 143 children with hospitalized COVID-19 infection.
| Symptoms |
Total (N=143) |
Cases (N=51) |
Controls (N=92) |
P |
| Cough, n (%) | 93 (65.0) | 35 (68.6) | 58 (63.0) | 0.50 |
| Rhinorrhea, n (%) | 60 (42.0) | 21 (41.2) | 39 (42.4) | 0.89 |
| Sore throat, n (%) | 39 (27.3) | 15 (29.4) | 24 (26.1) | 0.67 |
| Sputum, n (%) | 39 (27.3) | 16 (31.4) | 23 (25.0) | 0.41 |
| Dyspnea, n (%) | 16 (11.2) | 9 (17.6) | 7 (7.6) | 0.07 |
| Vomiting, n (%) | 45 (31.5) | 17 (33.3) | 28 (30.4) | 0.72 |
| Diarrhea, n (%) | 18 (12.6) | 7 (13.7) | 11 (12.0) | 0.76 |
| Abdominal pain, n (%) | 31 (21.7) | 14 (27.5) | 17 (18.5) | 0.21 |
| Anorexia, n (%) | 74 (51.8) | 27 (52.9) | 47 (51.1) | 0.83 |
| Fatigue, n (%) | 66 (46.2) | 26 (51.0) | 40 (43.5) | 0.39 |
| Neurological symptoms, n (%) | 40 (28.0) | 15 (29.4) | 25 (27.2) | 0.78 |
| Seizure, n (%) | 23 (16.1) | 7 (13.7) | 16 (17.4) | 0.57 |
| Myalgia, n (%) | 27 (18.9) | 10 (19.6) | 17 (18.5) | 0.87 |
Abbreviation: PASC: post-acute sequelae of SARS-CoV-2 infection.
Table E3.
Association between biomedical tests during the acute phase with PASC in 143 children with hospitalized COVID-19 infection.
Table E3.
Association between biomedical tests during the acute phase with PASC in 143 children with hospitalized COVID-19 infection.
|
Total (N=143) |
Cases (N=51) |
Controls (N=92) |
P | |
| Mean ± SD | ||||
| WBC, per μL | 7150.9 ± 4285.7 | 7326.1 ± 3353.7 | 7052.7 ± 4743.4 | 0.69 |
| Neutrophil | 66.3 ± 19.9 | 69.2 ± 18.9 | 64.7 ± 20.4 | 0.21 |
| Lymphocyte | 21.7 ± 18.0 | 19.4 ± 16.5 | 23.0 ± 18.7 | 0.26 |
| Monocyte | 9.9 ± 4.5 | 9.7 ± 4.1 | 10.0 ± 4.7 | 0.69 |
| Eosinophil | 1.1 ± 2.2 | 1.1 ± 2.8 | 1.1 ± 1.9 | 0.94 |
| Basophil | 0.4 ± 0.3 | 0.3 ± 0.2 | 0.4 ± 0.4 | 0.43 |
| Bandneutrophil | 0.5 ± 2.0 | 0.3 ± 1.8 | 0.6 ± 2.2 | 0.45 |
| MDW | 24.8 ± 4.8 | 24.0 ± 5.2 | 25.2 ± 4.6 | 0.20 |
| Platelet, per μL | 211635.9 ± 87300.2 | 224396.1 ± 83649.0 | 204484.6 ± 88931.4 | 0.19 |
| MPV | 7.7 ± 0.9 | 7.6 ± 0.9 | 7.7 ± 0.9 | 0.51 |
| Hb, g/dL | 12.9 ± 1.6 | 12.9 ± 1.2 | 12.9 ± 1.8 | 0.95 |
| RBC, x106 per μL | 4.6 ± 0.5 | 4.6 ± 0.4 | 4.6 ± 0.5 | 0.56 |
| Hct | 37.2 ± 3.6 | 37.5 (3.6) | 37.1 (3.6) | 0.49 |
| hsCRP, mg/dL | 1.8 ± 3.7 | 1.7 ± 3.4 | 1.9 ± 3.9 | 0.76 |
| ALT, U/L | 23.9 ± 61.4 | 19.2 ± 40.0 | 26.6 ± 71.0 | 0.44 |
| Cr, mg/dL | 0.4 ± 0.2 | 0.5 ± 0.2 | 0.4 ± 0.1 | 0.13 |
| GFR, mL/min/1.73m2 | 123.9 ± 22.2 | 121.8 ± 23.1 | 125.1 ± 21.7 | 0.42 |
| Glucose, mg/dL | 103.1 ± 26.5 | 108.1 ± 33.9 | 100.3 ± 20.9 | 0.15 |
| Na, mmol/L | 137.8 ± 2.6 | 138.0 ± 2.7 | 137.8 ± 2.6 | 0.67 |
| K, mmol/L | 3.9 ± 0.3 | 3.9 ± 0.3 | 3.9 ± 0.3 | 0.95 |
Abbreviation: PASC: post-acute sequelae of SARS-CoV-2 infection; WBC: white blood count; MDW: monocyte distribution width; MPV: mean platelet volume; Hb: hemoglobin; RBC: red blood count; Hct: hematocrit; hsCRP: high-sensitivity C-reactive protein; ALT: alanine aminotransferase ; Cr: Creatinine; GFR: glomerular filtration rate; Na: Sodium; K: potassium.
Table 3.
Association between total scores and scores of clinical categories during the acute phase with PASC in 143 children with hospitalized COVID-19 infection.
Table 3.
Association between total scores and scores of clinical categories during the acute phase with PASC in 143 children with hospitalized COVID-19 infection.
| Clinical categories | Cases | Controls | P* |
| mean ± SD | |||
| Respiratory system | 6.85±5.52 | 7.68±5.98 | 0.41 |
| Gastrointestinal system | 4.22±5.49 | 5.07±5.31 | 0.38 |
| Neurologic system | 3.68±7.79 | 5.60±9.07 | 0.19 |
| General appearance | 10.98±5.33 | 11.10±5.92 | 0.90 |
| Medication | 5.75±9.10 | 8.40±9.97 | 0.12 |
| Total score | 31.47±15.34 | 37.85±15.50 | 0.02 |
Abbreviation: PASC: post-acute sequelae of SARS-CoV-2 infection. *P_trend <0.05 is in bold.
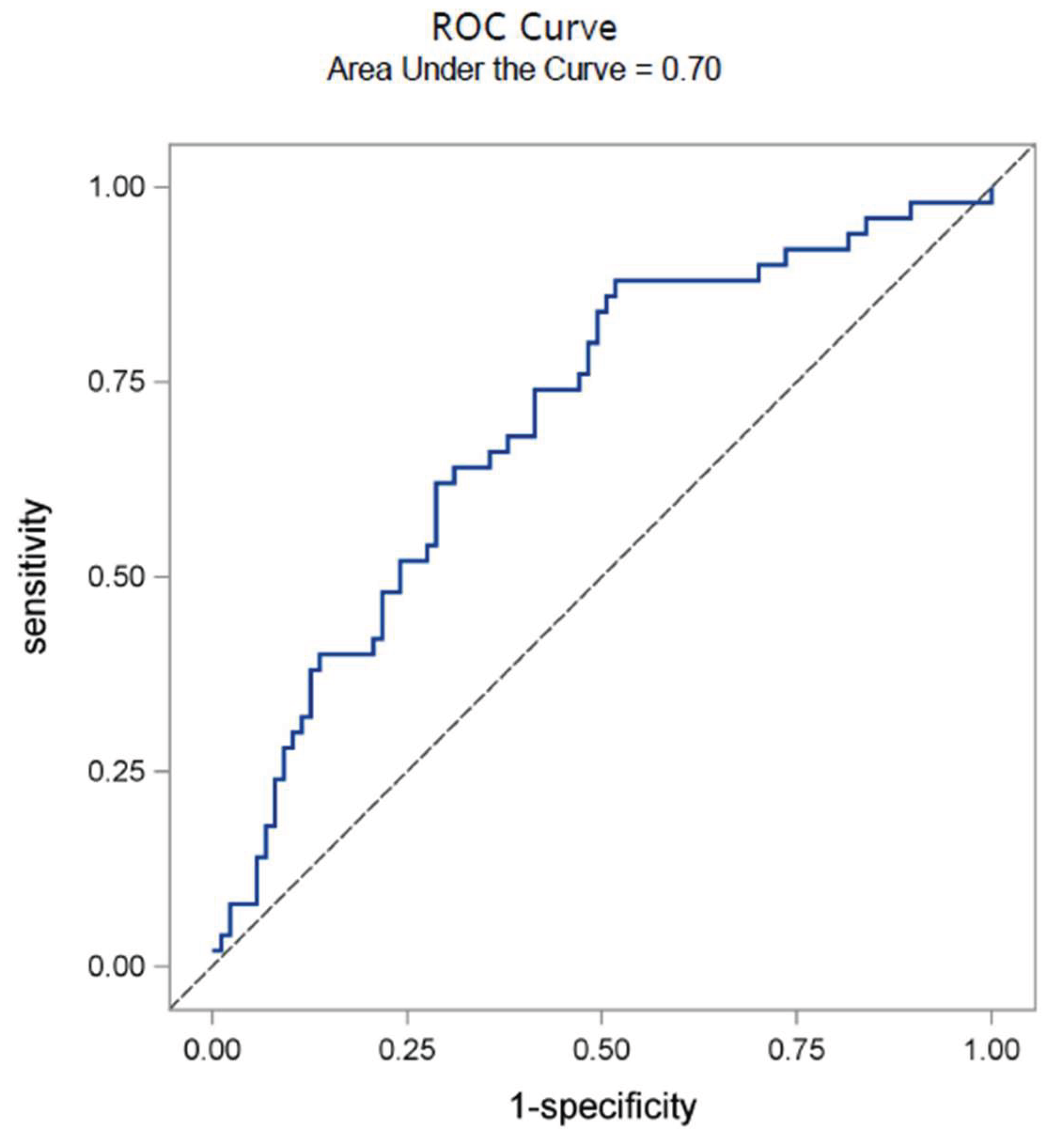
The association between various clinical parameters during the acute phase and the development of PASC is presented in Table E4. A model incorporating total clinical scores, age, body mass index (BMI), and fever duration yielded a c-statistic of 0.70 (95% CI, 0.61–0.79). The discriminative ability of total clinical scores during the acute phase was evaluated using ROC analysis (Figure 2). The analysis identified an optimal cutoff value of 37.7 for the total clinical scores, with a corresponding area under the curve (AUC) of 0.70.
Table E4.
Association between scores of composite clinical conditions during the acute phase with PASC in 143 children with hospitalized COVID-19 infection.
Table E4.
Association between scores of composite clinical conditions during the acute phase with PASC in 143 children with hospitalized COVID-19 infection.
| Effect | Odds ratio (95% CI) | P |
| Total clinical scores | 1.02 (1.00- 1.05) | 0.06 |
| Age | 1.08 (0.96- 1.23) | 0.20 |
| BMI | 1.07 (0.94- 1.22) | 0.30 |
| Fever duration | 1.17 (0.95- 1.43) | 0.14 |
| c-statistic (95% CI) | 0.7 (0.61- 0.79) |
Abbreviation: PASC: post-acute sequelae of SARS-CoV-2 infection.
Figure 2.
Receiver operating characteristic curves for total clinical scores from composite clinical conditions during the acute phase in PASC children by using a cutoff value of 37.7.
Figure 2.
Receiver operating characteristic curves for total clinical scores from composite clinical conditions during the acute phase in PASC children by using a cutoff value of 37.7.
Among the 51 children identified with PASC, the most frequent persistent symptom domains at 4 weeks were respiratory (44.8%), constitutional/psychological (30.2%), neurologic/cognitive (17.7%), and gastrointestinal (10.4%).
Discussion
In this retrospective cohort study of 143 children discharged after the acute COVID-19 hospitalization, we observed a notable prevalence (35.7%) of PASC. Our findings indicate that older age, greater body weight, and larger RT-PCR cycle threshold (Ct) values during the acute phase are associated with an increased risk of developing PASC. Furthermore, we developed a novel composite clinical scoring system which integrates respiratory, gastrointestinal, neurologic, and constitutional symptoms, as well as antibiotic use. This system demonstrated moderate discriminative ability (AUC = 0.70) under the optimal cutoff value 37.7 for total clinical scores during the acute phase for predicting PASC after discharge. This scoring system represents a promising tool for capturing pediatric COVID-19 survivors at risk.
The composite clinical score offers a simple, bedside tool using routinely documented symptoms and treatments to identify children at higher risk of PASC during hospitalization. A total score ≥ 37.7 (AUC = 0.70) flags patients who may benefit from earlier and more structured post-discharge intervention, including earlier follow-up for higher-risk children, multidisciplinary assessment (pediatric infectious disease, pulmonology, neurology, or rehabilitation), targeted symptom management (e.g., fatigue recovery, respiratory therapy, cognitive support), and strengthened caregiver education on red-flag symptoms and expected recovery.
Several adult models have been proposed to predict long COVID using acute-phase data, including: the LC risk score [17], the Gutenberg COVID-19 Study (GCS) Post-COVID Risk and Diagnostic Scores [18], a community-based model from the United States [19], and a hospitalized cohort model from Ukraine [20]. Similar pediatric tools are scarce. Our study represents an early attempt to adapt such acute-phase clinical risk stratification to children, emphasizing its potential utility in early identification and intervention. Unlike adult models heavily weighted by age or obesity, ours prioritizes clinical severity to remain actionable across developmental stages. Future harmonization with adult tools could enable lifespan risk prediction.
The prevalence of PASC symptoms remains uncertain, especially among children hospitalized in the acute phase. Recent studies have reported a wide range in the prevalence of pediatric PASC, with estimates ranging from 10% to 27% in children after hospitalized discharge 2 to 5 months [5,10]. The estimated prevalence of 35.7% derived from our study is higher than that in previous reports, which may be attributable to differences in patient populations, follow-up duration, and PASC definitions across studies.
In adult cohorts, severe initial COVID-19, older age, and multiple comorbidities have been linked to an increased risk of long-term sequelae [7]. Although children typically experience milder acute COVID-19 disease courses, emerging evidence indicates that pediatric PASC is not uncommon, which may be related to various risk factors, such as age, a history of allergic diseases [5], pre-existing comorbidities [21], and obesity [11]. In this study, we also observed that age and body weight were associated with an increased risk of developing PASC. Additionally, we observed that an elevated RT-PCR cycle threshold (Ct) value during the acute phase, which may reflect delayed viral clearance or an altered host immune response, was associated with an increased risk of PASC. Ct values were interpreted with the understanding that lower Ct values correspond to higher viral loads; however, single time-point measurements and the lack of standardized serial testing limit the precision of virologic inferences.
Acute COVID-19 is inherently a multisystem disease; its pathophysiology is complex and multifaceted, involving direct viral injury, immune-mediated damage, cytokine storm, and coagulation dysregulation [7,22,23,24,25]. Proposed mechanisms responsible for the development of PASC include immune dysregulation, disruption of the gut microbiota, autoimmunity, clotting abnormalities, and endothelial dysfunction, as well as dysfunctional neurological signaling [22,26]. Recognizing that acute COVID-19 affects multiple organ systems, we developed a comprehensive clinical scoring system derived from acute-phase conditions to predict the occurrence of PASC. This scoring tool integrates data from the acute phase including respiratory, gastrointestinal, neurologic, and constitutional symptoms, as well as the use of antibiotics. We included antibiotic use as one domain in calculating total clinical scores because antibiotics can have broad effects on the body, including impacts on the gut microbiome, which has been suggested to play a role in the pathophysiology of PACS [27].
Although older age and higher body weight were associated with PASC in univariate analyses, they were not included in the composite scoring system. The tool was designed to quantify acute multisystem clinical involvement using universally documented symptoms and treatments, independent of demographic variables. In an exploratory model that combined the composite score with age, BMI, and fever duration, the c-statistic was 0.70 (95 % CI 0.61–0.79), comparable to the AUC of 0.70 using the score alone, indicating that adding demographic variables provided only limited incremental discrimination. Future iterations may explore hybrid models incorporating age or BMI to improve discriminative performance, particularly in external validation cohorts
Strengths and Limitations
This study has several strengths. First, the study utilized data from a tertiary medical center in central Taiwan during the Omicron wave, providing a contemporary snapshot of clinical features in an Asian pediatric population, a underrepresented group in previous reports predominantly from Western countries [3,12]. Secondly, we comprehensively collected demographic and clinical data as well as laboratory data during both the acute and post-COVID-19 phases. Third, our multimodal follow-up strategy (via phone, electronic communication, or in-person visits) ensured that persistent symptoms were reliably captured, enhancing the quality of outcome ascertainment.
However, several limitations should be noted. First, as a retrospective, single-center cohort study, our findings may be subject to selection bias, and may not be fully generalizable to other pediatric populations. Secondly, although our total clinical scoring system may be a promising tool, it requires external validation in independent cohorts to confirm its predictive utility. More analyses exploring the associations between specific acute symptoms and subsequent PASC will require larger pediatric cohorts with sufficient statistical power and longer follow-up. Third, unmeasured confounding factors, such as genetic, environmental, or behavioral influences, could not be accounted for. Fourth, the study defined PASC as symptoms persisting beyond four weeks, consistent with major pediatric studies. However, duration beyond two months, as specified by the WHO definition (October 2021), was not assessed. This limits duration-based classification but remains informative for pediatric risk stratification and follow-up planning. Fifth, post-COVID-19 assessments relied on a self-developed questionnaire without standardized, validated patient-reported outcome measures. Fatigue, pain, and functional ability were captured qualitatively rather than through validated scoring instruments, limiting reproducibility and cross-cohort comparability. Sixth, the study did not systematically distinguish upper from lower respiratory tract infection or include standardized imaging assessments, thereby limiting evaluation of whether lower respiratory involvement or radiographic abnormalities predict PASC.
Conclusions
Our study demonstrates that PASC is a significant concern among children following COVID-19 hospitalization. Age, body weight, RT-PCR Ct values and during the acute phase are associated with PASC. Our total clinical scoring system may serve as a valuable tool for early identification of children at risk for PASC, enabling timely and targeted interventions. Future prospective, multi-center studies are needed to validate these findings and further elucidate the underlying mechanisms of pediatric PASC.
Ethics approval and consent to participate
The study was approved by the Institutional Review Board of China Medical University Hospital (CMUH113-REC1-126); informed consent was waived due to the retrospective design of the study.
Clinical Trial
Not applicable.
Consent for publication
Not applicable.
Availability of data and material
All data generated or analyzed during this study are included in this published article and its Supplementary Information files. No additional individual level data are available.
Competing interests
The authors declare no conflicts of interest in relation to this work.:
Authors' contributions
H.-C.L. (Huan-Cheng Lai), Y.-L.H., P.-C.C., H.-J.T., and J.-Y.W. in conceptualized and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript. H.-C.L. (Huan-Cheng Lai), Y.-L.H., P.-C.C., Y.-F.T., C.-H.W., and L.S.-H.W. designed the data collection instruments, collected data, performed the initial analyses, and reviewed and revised the manuscript. K.-S.H., C.-H.L., H.-C.L. (Hsiao-Chuan Lin), and K.-P.H. conceptualized and designed the study, designed the data collection instruments, and reviewed the manuscript. H.-J.T. and J.-Y.W. conceptualized and designed the study, coordinated and supervised data collection, and critically reviewed the manuscript for important intellectual content. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by following grants: NSTC 113-2314-B-039-057-; NSTC 114-2314-B-039-012- from the National Science and Technology Council, Taiwan; a research grant (1JA8) from the Center for Allergy, Immunology, and Microbiome (A.I.M.), China Medical University Hospital, Taichung, Taiwan; DMR-112-043, DMR-112-047, DMR-112-052, DMR-113-042, C1110831002-6, DMR-114-024, and DMR-114-109 from the China Medical University Hospital, Taichung, Taiwan.
Acknowledgments
We are grateful to all the medical staff of China Medical University Children’s Hospital (CMUCH) and China Medical University Hospital for providing administrative, technical, and funding support. We thank the staff of the medical research unit of CMUCH.
References
- Hu, B; Guo, H; Zhou, P; Shi, ZL. : Characteristics of SARS-CoV-2 and COVID-19. Nat Rev Microbiol 2021, 19(3), 141–154. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, P; Pittet, LF; Curtis, N. How Common is Long COVID in Children and Adolescents? Pediatr Infect Dis J 2021, 40(12), e482–e487. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S; Wegman-Ostrosky, T; Ayuzo Del Valle, NC; Perelman, C; Sepulveda, R; Rebolledo, PA; Cuapio, A; Villapol, S. Long-COVID in children and adolescents: a systematic review and meta-analyses. Sci Rep 2022, 12(1), 9950. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, T; Allin, B; Nugawela, MD; Rojas, N; Dalrymple, E; Pinto Pereira, S; Soni, M; Knight, M; Cheung, EY; Heyman, I. Long COVID (post-COVID-19 condition) in children: a modified Delphi process. Arch Dis Child 2022, 107(7), 674–680. [Google Scholar] [CrossRef]
- Osmanov, IM; Spiridonova, E; Bobkova, P; Gamirova, A; Shikhaleva, A; Andreeva, M; Blyuss, O; El-Taravi, Y; DunnGalvin, A; Comberiati, P. Risk factors for post-COVID-19 condition in previously hospitalised children using the ISARIC Global follow-up protocol: a prospective cohort study. Eur Respir J 2022, 59(2). [Google Scholar] [CrossRef]
- Chaichana, U; Man, KKC; Chen, A; Wong, ICK; George, J; Wilson, P; Wei, L. Definition of Post-COVID-19 Condition Among Published Research Studies. JAMA Netw Open 2023, 6(4), e235856. [Google Scholar] [CrossRef]
- Tsampasian, V; Elghazaly, H; Chattopadhyay, R; Debski, M; Naing, TKP; Garg, P; Clark, A; Ntatsaki, E; Vassiliou, VS. Risk Factors Associated With Post-COVID-19 Condition: A Systematic Review and Meta-analysis. JAMA Intern Med 2023, 183(6), 566–580. [Google Scholar] [CrossRef]
- Buonsenso, D; Munblit, D; De Rose, C; Sinatti, D; Ricchiuto, A; Carfi, A; Valentini, P. Preliminary evidence on long COVID in children. Acta Paediatr 2021, 110(7), 2208–2211. [Google Scholar] [CrossRef]
- Ludvigsson, JF. Case report and systematic review suggest that children may experience similar long-term effects to adults after clinical COVID-19. Acta Paediatr 2021, 110(3), 914–921. [Google Scholar] [CrossRef]
- Funk, AL; Kuppermann, N; Florin, TA; Tancredi, DJ; Xie, J; Kim, K; Finkelstein, Y; Neuman, MI; Salvadori, MI; Yock-Corrales, A. Post-COVID-19 Conditions Among Children 90 Days After SARS-CoV-2 Infection. JAMA Netw Open 2022, 5(7), e2223253. [Google Scholar] [CrossRef]
- Maddux, AB; Berbert, L; Young, CC; Feldstein, LR; Zambrano, LD; Kucukak, S; Newhams, MM; Miller, K; FitzGerald, MM; He, J. Health Impairments in Children and Adolescents After Hospitalization for Acute COVID-19 or MIS-C. Pediatrics 2022, 150(3). [Google Scholar] [CrossRef] [PubMed]
- Rao, S; Lee, GM; Razzaghi, H; Lorman, V; Mejias, A; Pajor, NM; Thacker, D; Webb, R; Dickinson, K; Bailey, LC. Clinical Features and Burden of Postacute Sequelae of SARS-CoV-2 Infection in Children and Adolescents. JAMA Pediatr 2022, 176(10), 1000–1009. [Google Scholar] [CrossRef] [PubMed]
- Asadi-Pooya, AA; Nemati, H; Shahisavandi, M; Akbari, A; Emami, A; Lotfi, M; Rostamihosseinkhani, M; Barzegar, Z; Kabiri, M; Zeraatpisheh, Z. Long COVID in children and adolescents. World J Pediatr 2021, 17(5), 495–499. [Google Scholar] [CrossRef] [PubMed]
- Molteni, E; Sudre, CH; Canas, LS; Bhopal, SS; Hughes, RC; Antonelli, M; Murray, B; Klaser, K; Kerfoot, E; Chen, L. Illness duration and symptom profile in symptomatic UK school-aged children tested for SARS-CoV-2. Lancet Child Adolesc Health 2021, 5(10), 708–718. [Google Scholar] [CrossRef]
- Toepfner, N; Brinkmann, F; Augustin, S; Stojanov, S; Behrends, U. Long COVID in pediatrics-epidemiology, diagnosis, and management. Eur J Pediatr 2024, 183(4), 1543–1553. [Google Scholar] [CrossRef]
- Akobeng, AK. Understanding diagnostic tests 3: Receiver operating characteristic curves. Acta Paediatr 2007, 96(5), 644–647. [Google Scholar] [CrossRef]
- Babicki, M; Lejawa, M; Osadnik, T; Kapusta, J; Banach, M; Jankowski, P; Mastalerz-Migas, A; Kaluzinska-Kolat, Z; Kolat, D; Chudzik, M. LC risk score - development and evaluation of a scale for assessing the risk of developing long COVID. Arch Med Sci 2024, 21(1), 121–130. [Google Scholar] [CrossRef]
- Baumkotter, R; Yilmaz, S; Chalabi, J; Ten Cate, V; Mamoor Alam, AS; Golriz Khatami, S; Zahn, D; Hettich-Damm, N; Prochaska, JH; Schmidtmann, I. Risk tools for predicting long-term sequelae based on symptom profiles after known and undetected SARS-CoV-2 infections in the population. Eur J Epidemiol 2025, 40(7), 789–801. [Google Scholar] [CrossRef]
- Sun, X; Di Fusco, M; Lupton, LL; Yehoshua, A; Alvarez, MB; Allen, KE; Puzniak, L; Lopez, SMC; Cappelleri, JC. Predictors of Long COVID Among Symptomatic US Adults Testing Positive for SARS-CoV-2 at a National Retail Pharmacy. Healthcare (Basel) 2024, 12(23), 2321. [Google Scholar] [CrossRef]
- Honchar, O; Ashcheulova, T; Chumachenko, T; Chumachenko, D. Early prediction of long COVID-19 syndrome persistence at 12 months after hospitalisation: a prospective observational study from Ukraine. BMJ Open 2025, 15(1), e084311. [Google Scholar] [CrossRef]
- Morello, R; Mariani, F; Mastrantoni, L; De Rose, C; Zampino, G; Munblit, D; Sigfrid, L; Valentini, P; Buonsenso, D. Risk factors for post-COVID-19 condition (Long Covid) in children: a prospective cohort study. EClinicalMedicine 2023, 59, 101961. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A; Sehgal, K; Gupta, A; Madhavan, MV; McGroder, C; Stevens, JS; Cook, JR; Nordvig, AS; Shalev, D; Sehrawat, TS. Post-acute COVID-19 syndrome. Nat Med 2021, 27(4), 601–615. [Google Scholar] [CrossRef] [PubMed]
- Trougakos, IP; Stamatelopoulos, K; Terpos, E; Tsitsilonis, OE; Aivalioti, E; Paraskevis, D; Kastritis, E; Pavlakis, GN; Dimopoulos, MA. Insights to SARS-CoV-2 life cycle, pathophysiology, and rationalized treatments that target COVID-19 clinical complications. J Biomed Sci 2021, 28(1), 9. [Google Scholar] [CrossRef] [PubMed]
- Bohn, MK; Hall, A; Sepiashvili, L; Jung, B; Steele, S; Adeli, K. Pathophysiology of COVID-19: Mechanisms Underlying Disease Severity and Progression. Physiology (Bethesda) 2020, 35(5), 288–301. [Google Scholar] [CrossRef]
- Kumar, S; Veldhuis, A; Malhotra, T. Neuropsychiatric and Cognitive Sequelae of COVID-19. Front Psychol 2021, 12, 577529. [Google Scholar] [CrossRef]
- Davis, HE; McCorkell, L; Vogel, JM. Topol EJ: Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol 2023, 21(3), 133–146. [Google Scholar] [CrossRef]
- Wang, C; Ramasamy, A; Verduzco-Gutierrez, M; Brode, WM; Melamed, E. Acute and post-acute sequelae of SARS-CoV-2 infection: a review of risk factors and social determinants. Virol J 2023, 20(1), 124. [Google Scholar] [CrossRef]
Figure 1.
Distribution of clinical symptoms during the acute phase with regards to the status of PASC in 143 children with hospitalized COVID-19 infection. Note: PASC: post-acute sequelae of SARS-CoV-2 infection.
Figure 1.
Distribution of clinical symptoms during the acute phase with regards to the status of PASC in 143 children with hospitalized COVID-19 infection. Note: PASC: post-acute sequelae of SARS-CoV-2 infection.
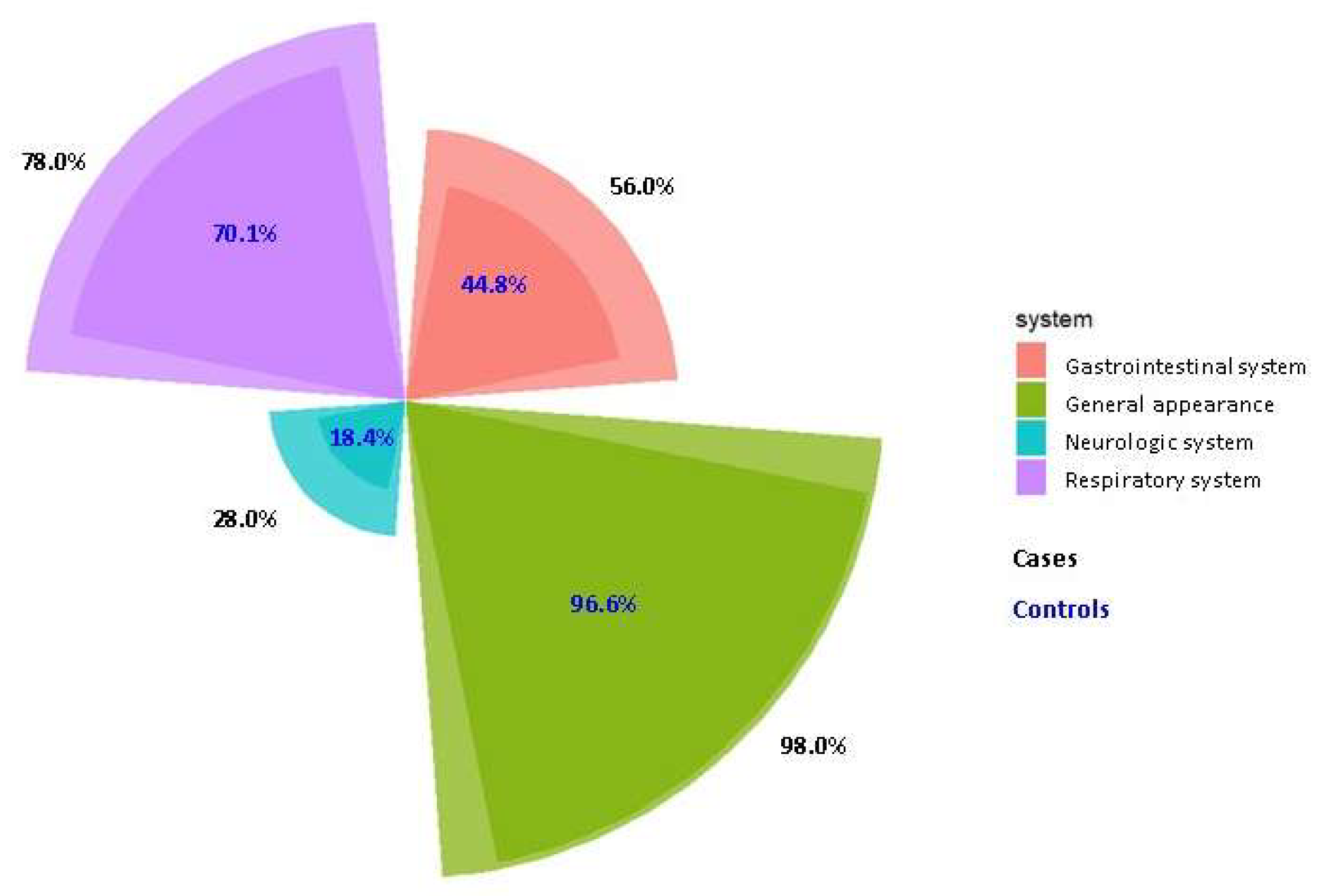
Table 1.
Baseline characteristics among 143 children with PASC in children with hospitalized COVID-19 infection.
Table 1.
Baseline characteristics among 143 children with PASC in children with hospitalized COVID-19 infection.
|
Total (N=143) |
Cases (N=51) |
Controls (N=92) |
P* | |
| Demographic data | ||||
| Age, mean ± SD, year | 6.8 ± 3.8 | 7.6 ± 4.3 | 6.3 ± 3.4 | 0.05 |
| Age, n (%), year | 0.10 | |||
| 3−6 | 87 (60.8) | 27 (52.9) | 60 (65.2) | |
| 7−12 | 41 (28.7) | 15 (29.4) | 26 (28.3) | |
| 13−18 | 15 (10.5) | 9 (17.7) | 6 (6.5) | |
| Sex, n (%) | 0.91 | |||
| Male | 85 (59.4) | 30 (58.8) | 55 (59.8) | |
| Female | 58 (40.6) | 21 (41.2) | 37 (40.2) | |
| Height, mean ± SD, cm | 120.0 ± 20.7 | 124.3 ± 23.0 | 117.6 ± 19.1 | 0.06 |
| Weight, mean ± SD, kg | 25.6 ± 14.4 | 29.1 ± 16.4 | 23.7 ± 12.8 | 0.05 |
| BMI, mean ± SD | 16.5 ± 3.5 | 17.3 ± 3.7 | 16.1 ± 3.4 | 0.06 |
| Clinical data | ||||
| Vaccine, n (%) | 0.24 | |||
| No | 56 (39.7) | 17 (33.3) | 39 (43.3) | |
| Yes | 85 (60.3) | 34 (66.7) | 51 (56.7) | |
| Comorbidity, n (%) | 0.20 | |||
| No | 94 (65.7) | 30 (58.8) | 64 (69.6) | |
| Yes | 49 (34.3) | 21 (41.2) | 28 (30.4) | |
| Duration of hospitalization, mean ± SD, day | 3.5 ± 3.0 | 3.9 ± 3.0 | 3.3 ± 3.1 | 0.34 |
| Duration of hospitalization, n (%), day | 0.25 | |||
| 1−3 | 101 (70.6) | 33 (64.7) | 68 (73.9) | |
| ≥ 4 | 42 (29.4) | 18 (35.3) | 24 (26.1) | |
| Fever temperature, mean ± SD, °C | 39.5 ± 0.8 | 39.5 ± 0.8 | 39.5 ± 0.8 | 0.96 |
| Fever temperature, n (%), °C | 0.86 | |||
| 37.8−38.9 | 29 (24.0) | 12 (26.7) | 17 (22.4) | |
| 39.0−39.9 | 51 (42.1) | 18 (40.0) | 33 (43.4) | |
| ≥ 40.0 | 41 (33.9) | 15 (33.3) | 26 (34.2) | |
| Duration of fever day, mean ± SD | 2.9 ± 1.9 | 3.2 ± 1.9 | 2.6 ± 1.9 | 0.07 |
| Duration of fever day, n (%) | 0.29 | |||
| 0 | 6 (4.4) | 2 (4.0) | 4 (4.6) | |
| 1−3 | 97 (70.8) | 31 (62.0) | 66 (75.9) | |
| 4−6 | 27 (19.7) | 13 (26.0) | 14 (16.1) | |
| ≥ 7 | 7 (5.1) | 4 (8.0) | 3 (3.4) | |
| RT-PCR Ct value, mean ± SD | 15.4 ± 5.1 | 17.1 ± 6.1 | 14.2 ± 3.8 | 0.04 |
| Antigen rapid test (ART) positive, n (%) | 77 (53.8) | 23 (45.1) | 54 (58.7) | 0.12 |
Abbreviation: PASC: post-acute sequelae of SARS-CoV-2 infection; BMI: body mass index; SD: standard deviation; RT-PCR: reverse transcriptase-polymerase chain reaction; Ct: cycle threshold. *P<0.05 is in bold. Vaccine Vaccinated children were defined as those who had received at least one dose of any COVID-19 vaccine (Moderna or Pfizer-BioNTech) before hospitalization, consistent with Taiwan’s national pediatric vaccination policy during the Omicron wave (April 2022 – July 2023). Comorbidities included: Congenital heart diseases (e.g., ASD, PFO, double outlet right ventricle, pulmonary hypertension), neurologic disorders (e.g., epilepsy, cerebral palsy, hypoxic encephalopathy), chromosomal or genetic abnormalities (e.g., 17q12 deletion, SCN1A and NAXE mutations), chronic lung diseases (e.g., bronchopulmonary dysplasia, asthma, ventilator dependence), autoimmune or hematologic disorders (e.g., SLE, autoimmune polymyositis, acute lymphoblastic leukemia, hereditary spherocytosis), endocrine/metabolic disorders (e.g., type I diabetes mellitus, rickets of prematurity), and other chronic conditions (e.g., ileal atresia post-operation, pituitary neoplasm, atopic dermatitis).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



