Submitted:
04 February 2026
Posted:
05 February 2026
You are already at the latest version
Abstract
Current immunization metrics primarily focus on population-level coverage and disease prevention but lack standardized tools to assess vaccine exposure patterns at the individual level during early infancy for comparing national immunization schedules. Background/Objectives: This study develops a necessary, age-adjusted metric to quantify early-life vaccine exposure in infants under one year, specifically designed for post-implementation vaccination policy evaluation to support the optimization of national immunization schedules directed to enhance safety and maintain high vaccine coverage. Methods: We introduce the Vaccine Exposure Index (VEI), an age-adjusted measure that quantifies cumulative vaccine exposure in infants under 12 months. The VEI accounts for the number, intensity, and timing of vaccine doses, providing a standardized approach to evaluate how schedules distribute exposure in infants across countries. A lower VEI reflects reduced intensity of neonatal exposure to vaccines, while a higher VEI indicates more concentrated early-life exposure. The VEI serves as a novel surveillance tool to guide and improve immunization schedules. Results: To demonstrate its applicability and utility as a comparative tool, we calculated the VEI using national immunization schedules from a sample of fourteen advanced countries and two highly populated nations with varying vaccination practices. We also used available data on neurodevelopmental outcomes (specifically autism spectrum disorder rates, while acknowledging the hot and contradictory debate) to empirically test the VEI's potential as an indicator of scheduling intensity. Results suggest that countries with a higher intensity of early-life exposure (higher VEI) tend to have vaccination schedules associated with a higher average number of vaccines and doses, often including vaccination at birth and concentrated administration at 6 and 12 months. Conclusions: The VEI serves as a vital comparative tool for identifying immunization schedules with concentrated early-life exposure and evaluating their alignment with nations having balanced and less concentrated vaccination schedules by 12 months in infants. The proposed VEI index does not question the necessity of vaccines or advocate for reduced coverage; rather, it provides a structured framework for optimizing the timing and dose distribution to minimize potential risks while simultaneously maintaining high vaccine coverage and community protection. By enabling cross-country comparisons and highlighting successful models (e.g., those achieving high coverage with lower VEI scores), this index offers a path for health policy optimization, promoting developmentally sensitive scheduling, and guiding future research on long-term outcomes to build greater public trust and security in immunization programs. Hence, the study presents as an exploratory framework and hypothesisgenerating findings that could inform future research on optimizing vaccine timing while maintaining high coverage and safety.
Keywords:
childhood immunization
; immunization schedule
; vaccine exposure
; vaccine risk
; autism
; Europe
; China
1. Introduction
Vaccination is one of the most effective public health interventions, based on radical innovation of vaccines, credited with the eradication and control of numerous infectious diseases in human society (Nath, 2023; Coccia, 2016). However, vaccine schedules and national immunization programs have become increasingly complex and concentrated—especially in the first year of life—with differences in vaccines and doses between countries (CDC, 2025; Coccia, 2021; Coccia and Bellitto, 2018; Institute of Medicine. 2013; National Academies of Sciences, 2024). Nath (2023, p. 621) acknowledges that: “vaccines have evolved over the years from crude extracts to more refined messenger RNA or protein based vaccines . . . the safety profile has also improved. Despite such measures, vaccines are not without side effects, including those that affect the nervous system.” Doja and Roberts (2006) emphasize that rigorous epidemiological methods are essential to guide evidence-based health policies. Mawson and Jacob (2025, p. 1) suggest that “data for 47,155 nine-year-old children revealed . . . that the current vaccination schedule may be contributing to multiple forms of neurodevelopmental disorders”; cf., (Institute of Medicine, 2012). However, in literature lacks a standardized metric to analyze and assess vaccine exposure during early infancy for comparing national immunization schedules (cf., National Academies of Sciences, Engineering, 2025). Surveillance systems and WHO’s global pharmacovigilance programs are essential for monitoring vaccine safety, but they should be complemented by proactive research aimed at optimizing vaccine scheduling. The objective here is not to reduce protection for infants, who must remain fully safeguarded against preventable diseases as early as possible, but rather compare vaccination schedules to detect immunization programs that distribute vaccine doses more effectively across the first years of life in order to minimize potential risks associated with concentrated early exposure. A compelling example is Denmark’s immunization schedule, which spaces core vaccines—such as diphtheria, tetanus, pertussis, polio, Hib, and PCV—at 3, 5, and 12 months . This approach achieves excellent protection while avoiding excessive clustering of doses in the first months of life. Importantly, Denmark maintains very high national immunization coverage, with vaccination rates of approximately 97% for diphtheria, tetanus, pertussis, and polio, ensuring that virtually all infants are protected against these serious diseases (Denmark, 2025). Adopting similar evidence-based scheduling strategies globally could help maintain strong protection for infants while reducing potential risks, thereby improving public health outcomes without compromising safety (Institute of Medicine, 2004; Magazzino et al., 2022; Coccia, 2022; 2022a, 2022b, 2023). The motivation of this study is due to children that in modern society receive more vaccines at earlier ages than ever before (National Academies of Sciences, Engineering, 2024). In many countries, including the United States and Japan, infants are administered up to 20 doses of vaccines covering 13 or more diseases before their first birthday (CDC, 2025; Japanese Pediatric Society, 2025). Although vaccination is an effective public health intervention, these intensive immunization schedules (having a concentrated administration from 0 to 12 months of different vaccines in childhood) can interact with the rapidly changing physiology of infants under 12 months, increasing the likelihood of unexpected reactions or side effects during this sensitive developmental period (Institute of Medicine, 2024, 2012; Mawson & Jacob, 2025; National Academies of Sciences, 2024). A main gap in literature is the lack of a standardized metric to assess vaccine exposure intensity in infants, in particular an index that can assess the concentration and cumulative vaccine exposure in early infancy by integrating three key dimensions: the number of vaccines, the intensity of doses, and the age at administration. Without such a tool, it is difficult to compare vaccine schedules in infants between countries to evaluate the potential impact on organs, metabolism, and nervous system that are still developing, and possible side effects. In this context, the main research question guiding this study is:
Can an age-adjusted vaccine exposure index serve as a valid and reliable tool for improving infant immunization schedules across countries, supporting healthier outcomes in population?
Answering this question has significant implications for both scholars and health policymakers. For researchers, this index provides a new methodological approach to study vaccination schedules, neurodevelopment, and public health outcomes. For policymakers, it offers a data-driven foundation method for improving immunization schedules to align them with epidemiological evidence. This study addresses that question and gap in literature by proposing the Age-adjusted Vaccine Exposure Index (VEI) —a composite measure that captures the number of vaccines and timing of administration in infants ≤1 year, offering a measure of early-life vaccine concentration. The proposed age-adjusted vaccine exposure index (VEI) is designed in a way that is comparable across countries. In particular, VEI mainly incorporates, total number of vaccines administered before 12 months and the age (months in infants) at administration of these vaccines. By aggregating these variables, the proposed VEI provides a simple an interpretable score that reflects the intensity and timing of vaccine exposure in infancy. This index can be used to compare countries, assess trends in vaccination over time, and evaluate associations with neurodevelopmental outcomes and other side effects. The goal of this research is fundamentally to inform safer vaccination policies that unequivocally maintain or enhance comprehensive immunization coverage while diligently minimizing potential adverse effects, particularly neurological ones, through optimized scheduling. Hence, the core scientific contribution of this study is the introduction of the Vaccine Exposure Index (VEI)—a novel, standardized metric designed to precisely quantify the intensity of cumulative vaccine exposure in infants less than one year old. This metric fills a significant and crucial methodological gap in the current scientific literature, which predominantly focuses only on national coverage rates and lacks specific tools to assess the vaccine concentration of varying immunization schedules. The VEI is not a tool for questioning vaccine coverage, but a simple mechanism for optimization. By allowing for cross-country benchmarking and identification of "best practices" (where high coverage is achieved with lower early-life exposure intensity), this study directly aligns with recent calls from public health authorities for enhanced vaccine safety surveillance and evidence-based health policy reform, ultimately aiming to bolster public trust and ensure the long-term sustainability of comprehensive, early-life immunization programs in society. In this context, Nath (2023) argues that there is an urgent need for coordinated global action involving manufacturers, healthcare agencies, scientists, and legislators to investigate vaccine-related neurological adverse events and develop strategies to prevent them, improving national immunization program schedules in countries (Ramachandran and Grose, 2024). The VEI can serve as a valuable tool for these aspects, comparing national immunization schedules, monitoring trends, and designing interventions that balance disease prevention with safety in infants having a rapidly changing physiology. Especially, the introduction of the VEI aims to optimize vaccine scheduling, not to question safety or advocate reduction in vaccine use. The Vaccine Exposure Index (VEI) is also an essential tool that enables robust international comparisons (global benchmarking) and the identification of best practices—those successful models that achieve and sustain high vaccination coverage and public safety while minimizing early-life vaccine intensity (GBD, 2023; Haeuser et al., 2025). By providing a standardized framework for evidence-based cross-national analysis, the VEI directly contributes to health policy optimization grounded in the foundational necessity of high vaccination coverage. It links this coverage with enhanced vaccine safety, offering a mechanism to minimize disorders by adjusting administration timing and scheduling. Overall, while vaccines are unequivocally essential for public health, optimizing their administration—especially in the timing and concentration in the first year of life—is a necessary step that may help reduce potential side effects. Hence, the VEI offers a scientifically rigorous path forward for researchers, clinicians, and policymakers seeking to achieve a superior balance between maximum immunization efficacy and enhanced safety in society, ultimately reinforcing the long-term public acceptance and success of comprehensive immunization programs.
Next section describes the conceptual framework with proposed age-adjusted vaccine exposure index (VEI) in immunization schedule for infants to 12 months and an empirical evidence of this index considering the autism spectrum disorder (ASD) between countries, a neurodevelopmental condition characterized by impairments in social interaction, communication, and behavior, which has seen a marked rise in prevalence globally (Talantseva et al., 2023; Grosvenor et al., 2024). These topics are controversial in science and object of on-going studies (Eicher et al., 2026). Research supports that autism is primarily a genetic condition, with minimal influence from environmental factors (National Academies of Sciences, 2025). For example, Bailey et al. (1995) demonstrated that monozygotic twins show a significantly higher concordance rate for autism compared to dizygotic twins, indicating a strong genetic basis. These findings suggest that genetic predisposition may play a role in autism development, while environmental contributions can be limited or non-causal. Some scholars also argue that assortative mating—the tendency for individuals to select partners with similar traits—may contribute to autism prevalence. When two individuals with autistic spectrum disorder (ASD) traits marry, the genetic load in their offspring may increase beyond the diagnostic threshold (Baron-Cohen & Hammer, 1997; Baron-Cohen, 2006). This hypothesis could partly explain why countries such as India, where arranged marriages remain more common than marriages based on personal choice and shared traits, report lower ASD prevalence (Nair et al., 2025). However, this explanation is far from conclusive. The study by Nair (2025) only shows lower autism incidence, which may be more strongly linked to socioeconomic and cultural factors, such as poverty, limited healthcare infrastructure, and reduced diagnostic capacity, rather than assortative mating alone. In fact, autism rates in other countries where assortative mating also occurs—such as Mozambique and Niger—are still lower than in the United States (911 and 798 per 100k in 2023, respectively, compared to 969 in the USA). Yet these countries have also low vaccination coverage for diphtheria, tetanus, pertussis, and polio (around 70% in Mozambique and 85% in Niger), compared to 94% in the USA, alongside other contextual factors. These observations underscore the complexity of autism epidemiology: differences in prevalence likely reflect a combination of genetic, cultural, socioeconomic, healthcare, and vaccination policy factors, rather than a single cause. This reinforces the need for multi-dimensional research to disentangle these influences and relations.
Despite many studies suggest no causal link between vaccines and autism (Gulati et al., 2025; National Academies of Sciences, 2025), the global prevalence of autism spectrum disorder in children is increasing (Issac et al., 2025) and environmental and healthcare-related exposures—including manifold vaccines in nation childhood immunization schedules—have been proposed as possible contributing factors. Some scientific investigations have identified statistical associations between vaccine dose intensity and ASD incidence, particularly in high-income countries (Mawson and Jacob, 2025; Nath, 2023; Ramachandran and Grose, 2024). Although it is a contested topic, this study here uses ASD as a case study to verify the goodness of proposed VEI directed to assess vaccination policies and some effects of intensive immunization schedules in countries, supporting hypothesis-generating findings. Therefore, discussions about vaccine timing and exposure should not be interpreted as implying causation between immunization and autism, as current scientific consensus attributes autism to genetic determinants.
2. Materials
- ▪
- Indicators of vaccinometrics and mathematical formulation of proposed age-adjusted vaccine exposure index (VEI)
The components of age-adjusted vaccine exposure index (VEI) in immunization schedule for infants to 6 and 12 months in country are defined mathematically as follows.
- ○
- Monthly vaccine exposure in infants (MVE)
These indicators indicate monthly vaccine exposure of infants in the proposed index VEI, as a consequence MVE6 months and MVE12 months are the numerator in the equations (eqs. 9-10 of VEI).
- ○
- Average Age of infants during vaccination (AA)
These indicators are used to normalize vaccinations in infants in the proposed index VEI, as a consequence AA6 months and AA12 months are the denominator in the next equations (eqs. 9-10 of VEI).
Other useful indicators of vaccinometrics are:
- ○
- Average number of vaccines (AV)
- ○
- Average number of vaccine doses (AD)
The proposed age-adjusted vaccine exposure index (VEI) measures vaccine exposure in infants by combining two key indicators just defined: the monthly vaccine exposure serves as the numerator (eqs 1-2), while the average age of infants during immunization (eqs. 3-4) acts as the denominator, normalizing exposure across age groups. Mathematically,
Hence, this analytical approach provides a standardized metric for evaluating vaccine exposure in early infancy and enables the design of VEI for assessing childhood immunization schedules at 6 and 12 months between countries, referred to as VEI6 and VEI12 and given by:
Where:
= Total monthly vaccine exposure administered from birth to 6 months.
= Total monthly vaccine exposure administered from birth to 12 months.
and = Average age of infants during vaccination in respective periods.
The VEI index has the following property:
- ○
- Lower VEI indicates a lower concentration of vaccines in childhood immunization schedule of country
- ○
- Higher VEI indicates a higher concentration of vaccines in childhood immunization schedule of country
The age-adjusted vaccine exposure index (VEI) is an increasing function from the value 0 (no vaccination and vaccine exposure in infants) to higher values, indicating a high vaccine exposure (vaccines × doses) in infants to 6 and 12 months. Moreover, VEI is not intended to model immunological mechanisms such as immune memory, cross-reactivity, or trained immunity. Rather, it serves as a comparative metric for evaluating vaccine scheduling intensity across countries during the first year of life. The index accounts for the number, timing, and concentration of vaccine doses, providing a standardized measure of early-life vaccine exposure. This quantitative approach robustly supports essential cross-country analysis and crucial health policy evaluation without, in any way, questioning the commitment to comprehensive vaccine coverage. Consequently, the VEI provides a unique, evidence-based tool for enhanced surveillance, offering a structured framework for monitoring and strategically mitigating potential risks associated with intense early-life scheduling. The central and novel perspective of this study is to strongly encourage immunization strategies that seek to expertly balance the paramount goal of disease prevention (maintaining or improving high vaccine coverage) with the commitment to long-term neurological health. In doing so, the VEI lays vital groundwork for future studies directed at rigorously optimizing the health policies governing national immunization program schedules across all countries, ensuring both maximum public health protection and enhanced vaccine safety.
- ▪
- Data and empirical evidence to validate age-adjusted vaccine exposure index (VEI)
This study applies the age-adjusted vaccine exposure index (VEI) to real-world immunization schedules from a sample of 12 countries to evaluate its effectiveness and validate its utility as a surveillance tool directed to optimize vaccine scheduling. While most vaccination metrics focus on population-level coverage, VEI introduces an individual-scale measure of early-life vaccine exposure, considering the number, intensity, and timing of doses during the first year of life. By calculating VEI scores for national immunization schedules, the study identifies patterns in vaccine concentration and age distribution, enabling cross-country comparisons. VEI suggests that countries with higher scores often administer more vaccines at younger ages, including birth doses. The Vaccine Exposure Index (VEI), of course, absolutely does not question or advocate for a reduction in vaccine coverage. Instead, it provides a structured, quantitative framework for optimizing the timing of vaccination doses with the explicit dual goal of minimizing potential risks while rigorously maintaining maximum disease prevention. By applying the VEI to diverse, real-world immunization schedules globally, this study demonstrates its practical potential for guiding evidence-based, scientifically informed policy adjustments. Hence, this study lays the essential groundwork for monitoring immunization schedules and national programs in order to achieve superior safety and efficacy, thereby sustaining high public confidence and comprehensive coverage.
- −
- Sample of countries for empirical evidence
The validation of the proposed age-adjusted vaccine exposure index (VEI) in infant immunization schedules (0–12 months) is done measuring concentration of vaccines in infants and using Autism Spectrum Disorder (ASD) as a reference condition of possible disorders, though is a controversial topic. Extensive research shows no causal link between vaccines and ASD (Gulati et al., 2025), but some studies also report statistical associations between vaccine dose intensity and ASD prevalence, especially in high-income countries (Mawson and Jacob, 2025; Nath, 2023). Given the global rise in ASD (Talantseva et al., 2023; Grosvenor et al., 2024), this study evaluates VEI’s effectiveness across countries to assess whether intensive childhood immunization schedules, having a concentration of vaccines to 12 months, correlates with differential levels of ASD in countries for hypothesis-generating findings. This study is based on real data from national immunization schedules in a homogenous sample of advanced countries—Singapore, South Korea, Japan, Australia, Canada, the United States, Sweden, Denmark, Norway, Finland, Italy, and the United Kingdom (see Supplemental Information). These countries were selected because they share similar immunization schedules and vaccines as well as diagnostic standards for autism, maintain a low threshold for diagnosis, and offer high-quality healthcare systems. Their immunization programs are broadly comparable, making them suitable for a consistent cross-country analysis of vaccine scheduling patterns and early-life exposure and autism diagnosis. Two other countries are also analyzed, China and India: they were not included in the main sample to avoid statistical distortions that could arise from their very large populations and markedly different socioeconomic and healthcare contexts. In fact, including these countries in the core analysis could introduce bias and reduce the comparability of results across nations with similar public health systems. Instead, India and China were analyzed as specific case studies to test the robustness for hypothesis-generating findings. in diverse settings. This approach strengthens the study by ensuring that the main statistical analysis remains internally consistent, while still exploring how the findings performs in countries with different demographic and policy environments.
- −
- Data and Sources for Statistical Analysis
The data and sources are indicated in Table 1 with description of specific variables.
- −
- Statistical analysis procedure to validate proposed age-adjusted vaccine exposure index (VEI)
The statistical analysis is based on the mentioned sample of countries, analyzing all information in Table 1 from national immunization schedules in countries (Table S1) and World Population Review (2025). The study design focuses on logical groupings for measuring the proposed vaccinometrics (measures of vaccine exposure) and the index VEI in infants, and whether statistical evidence supports the hypothesis that the autism incidence between countries can be explained by the level of vaccine exposure index in infants (concentration of manifold vaccines). The first categorization under study to assess the proposed age-adjusted vaccine exposure index (VEI) in infant immunization schedules (0–12 months) is between:
- ○
- Higher Autism rate countries: Singapore, South Korea, Japan, Australia, Canada, USA (according to data in World Population Review, 2025).
- ○
- Lower Autism rate countries: Sweden, Denmark, Norway, Finland, Italy, UK (according to data in World Population Review, 2025).
The study design also focuses on other logical groupings to analyze the VEI index, considering:
- ○
- countries that administer vaccines at birth versus other that start later
- ○
- countries that administer vaccines for varicella, hepatitis B and Japanese encephalitis versus other countries that do not consider these vaccines in the childhood vaccination schedule.
- ○
- Firstly, the variables in Table 1 are analyzed with descriptive statistics given by arithmetic mean, standard deviation, skewness and kurtosis to assess the distributions and their normality. Variables with non-normal distribution are transformed into log-scale, to have a normal distribution for appropriate and robust parametric analyses.
Secondly, proposed metrics for infants ≤1 year and less than 6 months, were also analyzed using the Independent Samples t-Test to determine whether there was statistical evidence that the associated means over time are significantly different between the two main reference groups (countries with higher vs. lower average values of autism rate per 100k people). The hypotheses used for the Independent Samples t-Test are:
H’0: µ1 = µ2, the two-population means of groups are equal between
H’1: µ1 ≠ µ2, the two-population means of groups are not equal
Thirly, partial correlation between autism rate per 100k people and proposed metrics (controlling % vaccination rate for diphtheria, tetanus, and pertussis, measles and polio disease), with test of significance having one-tailed, is applied.
Fourthly, an analysis of dependence was performed using linear regression models for the overall sample. The linear model of simple regression considers the autism rate per 100k as a function both of monthly vaccine exposure to 12 months in infants or age-adjusted vaccine exposure index (VEI). The basic linear model is:
y = dependent variable (log Autism rate 2021 per 100k)
log yi = α + β log xi + ui
x= explanatory variable: log monthly vaccine exposure to 12 months in infants or log age-adjusted vaccine exposure index (VEI)
α = constant; β = regression coefficient; u = error term; i= countries
The model is extended with a multivariate regression considering the Autism rate per 100k people on explanatory variables given simultaneously by both age-adjusted vaccine exposure index (VEI) and % vaccination rate for diphtheria, tetanus, and pertussis, measles and polio disease. The specification of this log-log model is:
where:
y = dependent variable (log Autism rate 2021 per 100k)
x1 = age-adjusted vaccine exposure index (VEI) to 12 months
x2 = Vaccination rate for Diphtheria, Tetanus, and Pertussis, Measles and Polio diseases
Other terms are defined as in the equation (11).
Graphical representation of the regression line (11) is basic to locate countries in the space, also considering vertical and horizontal lines indicating average values of variables. These lines create four quadrants in the space. Each quadrant is labeled with a policy implications. Statistical analyses are done with SPSS software 29.00.
3. Results
First of all, these findings are strictly associative and exploratory directed to hypothesis-generating findings; they do not establish causality. This analysis aims to examine patterns within immunization schedules without questioning the efficacy of vaccines, which remain one of public health’s greatest achievements. Instead, we focus on the structural 'clustering' of vaccines—specifically the practice of adding new immunizations to the infant schedule under 12 months of age. Our goal is to generate hypotheses regarding how these concentrated exposures might interact during critical developmental windows. This study should be viewed as an exploratory framework intended to inform future research on optimizing vaccine timing while maintaining high safety and coverage standards, rather than an assertion of harm.
Descriptive statistics in Table 2 shows arithmetic mean and standard deviation of basic variables and indicators under study here in countries categorized per main groups and if some types of vaccines are or not administered. First of all, group of countries having a higher average of autism rate of 1273.33 per 100,000 people, called higher autism rate countries, vs. the second group that has a lower average rate of autism (834.44 per 100k people), shows a marginal higher percent vaccination rate for diseases (diphtheria, tetanus, and pertussis, measles and polio) of 95% vs. 94.5%; moreover average age of infants during the vaccination by 12 months, according to national immunization program schedules in these countries, is lower (4.9 months) in the group with higher average rate of autism (results also show that average age of infants during the vaccination by 6 months is lower −3.09 months− always in countries having higher average rate of autism). As far as total average number of vaccines and doses to 12 months, in countries having a higher autism rate is higher with about 15 vaccines and 20 doses vs. 8 vaccines and 9 doses in countries with a lower autism rate; whereas average number of vaccines and doses to 6 months has a similar situation: in higher autism rate countries is higher (about 10 vaccines and 15 doses vs. 9 vaccines and 6.5 doses in countries with a lower autism rate). Moreover, countries having a higher autism rate administer about 1.2 vaccines and 1.64 doses per month by 1 year in infants vs. 0.7 vaccines and 0.8 doses per month in infants of countries with lower autism rate; in the period of 6 months, similar situation. This result generates an average monthly vaccine exposure to 12 months (vaccines × doses / 12 months) in infants of countries having a higher autism rate of about 24.3 vs. about 7 in infants of countries with lower autism rate, whereas average monthly vaccine exposure to 6 months (vaccines × doses / 6 months) in infants of countries having a higher autism rate is about 24.2 vs. about 8.4 in infants of countries with lower autism rate. The combined vaccine exposure index to 12 months in infants (VEI12), which is a main synthesis of these metrics based on both vaccine exposure and average age in infants according to the immunization program schedule, shows in countries with higher autism rate an average value of 5, whereas VEI12 is 1.25 in lower autism rate countries. VEI at 6 months in countries with higher autism rate is 8 vs. 3 in lower autism rate countries. The comparative analysis, considering other logical categorization, shows the following results. We report only the index VEI at 12 months for the sake of briefness. For details see Table 2. Countries that do not vaccine at the birth have a VEI12=1 vs. VEI12=5 in countries that vaccine at birth; moreover, countries that do not administer varicella vaccine have a VEI12=1 vs. VEI12=4.6 (higher vaccine exposure) in countries that administer this vaccine; countries that do not administer hepatitis B vaccine have a VEI12=1.2 vs. VEI12=4.01 (higher vaccine exposure) in countries that administer it. Finally two countries (South Korea and Japan) administer also Japanese encephalitis vaccine, results show a very high average VEI12=5.8 (high vaccine exposure) associated with one of the highest incidence of autism rate worldwide (1450 per 100k people in the year 2021; see, World Population Review, 2025). In short, countries with a higher rate of autism tend to have a lower average age of infants during vaccine administration according to their national immunization schedules and a higher average number of vaccines and doses (high concentration), including vaccination at birth, varicella and hepatitis B vaccines, which generate a higher early-life vaccine exposure both a 6 and 12 months. As a consequence VEI provide a main proxy of possible risks of adverse effects in infants having less than or equal to 1 year, when undergoing to a high concentration of vaccines.
Although this proposed index VEI is a descriptive, non-biological metric, it can assess different national immunization schedules between countries. Empirical results of VEI show that earlier vaccine administration in infants can generate, in some cases, disorders. According to some studies, infants in their first year undergo rapid maturation of both innate and adaptive immunity. Initially, they rely on maternal antibodies passed via the placenta and breast milk, while their own immune systems—particularly underdeveloped antigen-presenting cells, T cells, B cells, and Ig-mediated responses—are still evolving. Research highlights that their vaccine-induced immune responses differ significantly from those of older children or adults. A systems-level study (using a routine two-month vaccine panel) revealed unique patterns in monocyte, B-cell, and T-cell activation, indicating that an infant’s immune system is essentially at its “immunity boot camp” phase (Tregoning, 2022; Nouri et al., 2023). Adaptive immunity in neonates is inherently dampened: key components necessary for robust, long-lasting immunity—such as stable T and B cell maturation and memory—develop slowly. These immunological limitations must be carefully considered when devising vaccine schedules. Moreover, maternal antibodies can interfere with vaccine antigens, potentially reducing vaccine efficacy when administered too early (Semmes et al., 2021). Emerging evidence suggests that perturbations in early immune development—for instance, through premature or frequent antigen exposure via early vaccination—could carry risks. Early-life administration of vaccines may interact with the maturing immune network in ways that are not fully understood and could theoretically contribute to immune dysregulation or priming toward allergies or autoimmune tendencies. A recent review underscores the importance of precise timing, adjuvant choice, and integrating maternal immunization to optimize infant vaccine responsiveness while minimizing immune-system stress (Tregoning, 2022; Semmes et al., 2021). Additionally, studies highlight that disruptions to the infant microbiome—such as through antibiotics—can blunt vaccine responses significantly by altering immune maturation and antibody production pathways (O'Leary, 2025). In short, during the first year of life, infants' immune systems are in a delicate balancing act—still immature yet evolving to mount effective responses. Administering vaccines too early or without strategic scheduling and support may not only reduce efficacy but could also interact unpredictably with the developing immune network, with potential long-term implications.
In Table 3, with the exception of the total vaccination rate and the average age of infants vaccinated up to 6 months, the Independent Samples Test shows statistically significant differences for the variables analyzed, with p-values < .001, < .01, or < .05. Therefore, we can reject the null hypothesis and conclude that the mean values of the proposed metrics for countries with higher autism rates are significantly different (as described in Table 2) than those for the second group, which includes countries with lower autism rates per 100,000 people.
Partial correlation in Table 4 shows that Autism rate per 100k people (controlling vaccination rate % rate for diphtheria, tetanus, and pertussis, measles and polio diseases in population) has a negative significant coefficient with average age in infants vaccinated to 12 months (r=−0.71, p-value< 0.01): i.e., vaccinations in younger infants are associated with a high ASD risk1; whereas it has a positive significant coefficient with total vaccines done to 12 months (r=0.87, p-value< 0.001), with total vaccines done to 6 months (r=0.77, p-value< 0.01), with total doses done to 12 months (r=0.79, p-value< 0.01), with total doses done to 6 months (r=0.80, p-value< 0.001), with total vaccine exposure to 12 months (r=0.85, p-value< 0.001), with total vaccine exposure to 6 months (r=0.83, p-value< 0.001), and especially with vaccine exposure index (VEI) to 12 months (r=0.85, p-value< 0.001) and with vaccine exposure index (VEI) to 6 months (r=0.80, p-value< 0.001): i.e., concentration of vaccines in infants having less than 12 months seems to be associated with a higher autism risk. In short, Table 4 about the relationship between variables and test of association suggests that rates of autism tend to have a negative correlation with average age in infants during vaccinations at 12 months and a positive association with average number of vaccines and doses at 6 and 12 months, and proposed vaccine exposure index (VEI) at 6 and 12 months: therefore this analyses present hypothesis-generating findings that concentration of vaccines at younger infants seems to be associated with a higher autism risk.
Parametric estimates in Table 5 of the linear model based on autism rate as function of monthly vaccine exposure in infants to 1 year (log-log model) show that a 1% increase in the monthly vaccine exposure to infants ≤ 1 year, it increases the level of autism rate by 0.16% (p-value 0.05). Estimated relation based on autism rate as function of vaccine exposure index (VEI) in infants to 1 year also shows that a 1% increase in this VEI index (that combines monthly vaccine exposure index and average age of infants ≤ 1 year), it increases the level of autism rate by 0.14% (p-value 0.05). Multivariate regression also in Table 5 shows stronger results. Partial coefficient of vaccine exposure index in infants ≤ 1 year (controlling vaccination rate for diphtheria, tetanus, and pertussis, measles and polio diseases) suggests that a 1% growth, it increases the autism rate per 100k people by 0.16 (p-value 0.001). The coefficient of determination R2 explains about 78% of the variance in the data. The F ratio of the variance explained by the model to the unexplained variance is significant (p-value<0.001), then predictors reliably predict response variable (i.e., autism rate). These results seem to show a main relation that autism rates increases are driven by a high concentration of vaccines and related doses to infants ≤ 1 year. Figure 1 shows the graphical representation of the relation of autism rate on vaccine exposure index in infants ≤ 1 year with the location of countries under study. Figure 1 also has vertical and horizontal lines indicating average values of variables that create 4 quadrants. Countries are concentrated in three main quadrants.
Sensitivity Analysis and Robustness
In regression models, robustness and reproducibility are critical for validating findings, especially with our sample size of 12 advanced countries. In our study, as described above, we examined the relationship between autism rates per 100,000 children (log-transformed) and the proposed Vaccine Exposure Index (VEI). The regression model yielded an R = 0.674, explaining approximately 45.5% of variance (R² = 0.455), with a statistically significant association (F = 8.341, p = 0.016). The estimated coefficient for VEI was B = 0.143 (p = 0.016), indicating that higher VEI values are positively associated with autism rates (Table 5). To test robustness, we implemented a bootstrap procedure with 1,000 resamples, using a bias-corrected and accelerated (BCa) 95% confidence interval. Sensitivity analysis using bootstrapping provides a powerful non-parametric approach to assess the stability of estimated coefficients and confidence intervals. Bootstrapping repeatedly resamples the original dataset with replacement to generate empirical distributions of the parameters, enabling more reliable inference without relying solely on asymptotic assumptions. Results confirmed stability: the VEI coefficient remained positive across resamples, with a BCa interval of 0.058 to 0.469 and a bootstrap-adjusted significance of p = 0.048. The small bias (0.021) and consistent standard error (0.075) further support reproducibility. The intercept also demonstrated negligible bias and tight confidence bounds, reinforcing model reliability (Table 6). This sensitivity analysis demonstrates that the observed association is not an artifact of sampling variability. Bootstrapping strengthens confidence in the regression findings by providing empirical evidence that the VEI-autism relationship persists under repeated resampling, thereby enhancing the credibility of conclusions drawn from the proposed index. Hence, the small bias (0.021) and the fact that the bootstrap significance level remains below 0.05 provide strong evidence of reproducibility. Even when the data is shuffled and resampled 1,000 times, the positive relationship between the VEI index and autism rates persists, confirming the model's reliability for hypothesis-generating findings and further scientific inquiry in this direction.
Figure 1 presents a compelling visual analysis of the relationship between the Age-adjusted Vaccine exposure Index (VEI) and autism rates in infants ≤1 year across a sample of countries. The scatterplot is divided into four quadrants by vertical and horizontal lines representing the average values of VEI and autism incidence. This quadrant-based categorization reveals distinct patterns in national immunization strategies and their potential associations with neurodevelopmental outcomes.
- Bottom-Left Quadrant (Low VEI, Low Autism Rate) includes countries such as Norway, Denmark, Finland, and Sweden. These nations administer fewer vaccine doses in the first year of life and exhibit lower autism rates. These Scandinavian countries with lower VEI scores demonstrate that high immunization coverage can be achieved without early and intensive vaccine schedules. These nations delay non-critical vaccines, avoid vaccination at birth, and exclude certain vaccines like varicella and hepatitis B from the first months of life. In short, these countries demonstrate that it is possible to maintain high vaccination coverage while minimizing early-life vaccine exposure. Their policies reflect a cautious approach that prioritizes long-term neurological health alongside disease prevention. Their schedules could inform revisions in countries with higher VEI scores.
- Top-Right Quadrant (High VEI, High Autism Rate). Countries including Australia, Canada, the United States, Singapore, Japan, and South Korea are positioned here. These nations administer a higher number of vaccine doses to infants under one year, often starting at birth, and show above-average autism rates. Their schedules tend to be more intensive, with early and frequent vaccinations (Frenkel, 2021). These countries with high VEI scores often administer multiple vaccines to 0-6 months and maintain dense schedules through the first year. While these programs aim to maximize protection, they may inadvertently generate adverse effects, particularly in vulnerable populations. In the U.S., autism prevalence rose from 1 in 150 children in 2000 to 1 in 31 by 2022 (CDC, 2025a). During this period, the infant immunization schedule expanded from approximately 11 vaccines to 15 before age one (CDC, 2025b). This intensification of early-life vaccine exposure may contribute to neurodevelopmental stress. International trends mirror this trajectory. Australia’s infant schedule in national immunization program increased from about 9 vaccines in 1994 to 14 in 2025, especially for Aboriginal and Torres Strait Islander children (Australian Government, 2025). Japan’s 2025 schedule includes early administration of BCG, DPT-IPV-Hib, and pneumococcal vaccines, with multiple doses before 6 months (Japan Pediatric Society, 2025; Japan, 2025). While these programs aim to maximize protection against infectious diseases, the elevated VEI scores suggest a greater early-life vaccine exposure, which may warrant further investigation into potential risks, especially in infants. Health policy reassessment in these nations should consider delaying non-essential vaccines, reducing dose intensity, and tailoring schedules for at-risk infants, such as those born preterm or with a family history of neurodevelopmental disorders (cf., (Mawson and Jacob, 2025). The VEI enables cross-country comparisons for optimizing vaccine schedules to balance efficacy and safety. Hence, by integrating VEI into national health planning, policymakers can identify high-vaccine exposure schedules, monitor trends, and design interventions that reduce early-life vaccine exposure. As Doja and Roberts (2006) argue, evidence-based policy must be grounded in rigorous epidemiological analysis—precisely what the VEI enables. Ultimately, the VEI supports a shift from one-size-fits-all immunization toward personalized, developmentally informed vaccination strategies, improving both safety and public trust (Coccia, 2023, 2022, 2022a).
- Bottom-Right Quadrant (High VEI, Low Autism Rate). Italy and the United Kingdom occupy this quadrant. Although their autism rates are below the average, their VEI scores are relatively high. In particular, Italy’s 2025 schedule shows early and intensive vaccine administration, including hexavalent vaccines and MenB within the first months. Vaccines in national immunization program schedules of these countries have considerably increased compared to 1980s-2000s period (Italy, 2025). This positioning may indicate a transitional phase in vaccine policy, with tendencies toward more intensive schedules and critical zone in space of figure 1. These countries could benefit from re-evaluating their immunization strategies, potentially aligning more closely with the Nordic model to reduce early-life exposure without compromising coverage. A Surveillance enhancement health policy can be integrating VEI into existing pharmacovigilance systems to improve early detection of adverse trends and support evidence-based policy reform.
- Top-Left Quadrant (Low VEI, High Autism Rate). Notably, no countries in the study fall into this quadrant. This absence reinforces the hypothesis-generating findings that higher vaccine exposure may be associated with higher autism rates, although causality cannot be inferred.
In brief, the VEI provides a powerful tool for evaluating and comparing between countries infant immunization schedules. This study suggests that vaccine efficacy and safety can be balanced through thoughtful scheduling. VEI application can optimize vaccine scheduling, minimize potential side effects, and guide global health policy toward more balanced and individualized vaccination strategies for a vast and safe coverage in human society. As Doja and Roberts (2006) emphasize, rigorous epidemiological methods are essential to disentangle associations and inform evidence-based policy.
4. Discussion
This study introduces the age-adjusted Vaccine Exposure Index (VEI) as a crucial, novel metric specifically engineered to compare and optimize national immunization schedules by possible adjusting the timing and intensity of doses without, under any circumstances, compromising the essential goals of vaccine safety or comprehensive vaccine coverage to face diseases. The empirical evidence analyzes national immunization schedules from a group of 12 advanced countries having homogeneous socioeconomic contexts and effective health systems: Singapore, South Korea, Japan, Australia, Canada, the United States, Sweden, Denmark, Norway, Finland, Italy, and the United Kingdom. In particular, these countries were selected because they share similar national childhood immunization schedules and vaccines, diagnostic standards and criteria for autism, maintain a low threshold for diagnosis and high-quality healthcare systems. The immunization programs of these advanced countries are broadly comparable, making them suitable for cross-country evaluation of early-life vaccine exposure and meaningful comparisons of scheduling intensity and timing using the proposed index VEI without confounding factors such as limited healthcare access or inconsistent reporting. Highly populated countries such as India and China, are also interesting cases study, but they were excluded from the main analysis of just mentioned countries to avoid distortions in statistical analysis. However, a preliminary comparison of these two countries having the majority of the global population reveals notable differences. According to World Population Review (2025), autism rate per 100,000 population is estimated at 484 in China and 509 in India. Vaccination coverage in 2023 for DTP3 (diphtheria, tetanus, pertussis), Polio (POL3) and MCV1 (measles) was 97% in China and slightly lower in India (91% for DTP3 and Polio, 93% for MCV1). Immunization schedules indicate that by 12 months, infants in China typically receive about 10 vaccines and 12 doses (Chinese CDC, 2021), whereas in India, the vaccination schedule includes approximately 14 vaccines and 19 doses (Ministry of Health & Family Welfare, 2018). These basic information show that India has a higher autism prevalence, although causality is not implied, reflecting greater cumulative exposure in vaccines compared to China (Table 7). These findings, associated to previous statistical analysis, can further support hypothesis-generating relation to be in-depth investigated.
These preliminary results underscore the potential of a comparative tool for evaluating vaccine scheduling intensity and guiding immunization strategies across diverse health systems. The findings suggest that countries with higher autism prevalence tend to exhibit elevated VEI values, reflecting a concentrated vaccine administration at younger ages in infants and higher dose intensity (Casey et al., 2020). To reiterate, while these results do not establish causality, they highlight the importance of comparative analyses when designing vaccination schedules. The findings based on statistical evidence here suggest that early and intensive vaccine exposure may be associated with increased autism prevalence, although causality is not claimed. This aspect needs to be investigated to reduce misconceptions and propose path forward, also based on comparative analyses between countries with appropriate metrics (e.g., VEI) as suggested here. In fact, regression models provide additional insight. Multivariate regression, controlling for core vaccination rates, shows a 0.16% increase in autism rate per 1% rise in VEI. Although this is a contested topic, these findings here align with existing literature that has explored the potential neurodevelopmental effects of vaccine exposure. Tomljenovic and Shaw (2011) raised concerns about aluminum adjuvants in vaccines and their role in neuroimmune disorders. The association between aluminum adjuvants in the vaccines and autism spectrum disorder is suggested by multiple lines of evidence (cf., Boretti, 2021; Strunecka et al., 2018). Ramachandran and Grose (2024) documented rare but serious neurological events following varicella vaccination, while Mawson and Jacob (2025, p.1) suggested that: “current vaccination schedule may be contributing to multiple forms of neurodevelopmental disorders (NDDs); that vaccination coupled with preterm birth was strongly associated with increased odds of NDDs compared to preterm birth in the absence of vaccination; and increasing numbers of visits that included vaccinations were associated with increased risks of autism spectrum disorder (ASD)”. Geiger et al. (2017) has analyzed diagnoses of autism spectrum disorder, tic disorder, attention deficit disorder/attention deficit hyperactivity disorder, compared to controls, following exposure to Hg from thimerosal-containing Haemophilus influenzae type b vaccines administrated within the first 15 months of life, showing a significant association. In general, the infant immune system is still developing during the first year of life, and exposure to multiple immunological stimuli in a short timeframe could potentially influence neurodevelopment in vulnerable populations (Shapiro et al., 2021; Tomljenovic & Shaw, 2011). Strunecka et al. (2018) argue that children are exposed to such sequential immune stimulation via a growing number of environmental excitotoxins, vaccines, and persistent viral infections, and show that fluoride and aluminum (Al3+) can exacerbate the pathological problems by worsening excitotoxicity. The concept of proposed age-adjusted vaccine exposure (VEI) aligns with emerging insights into immune ontogeny. Brophy-Williams et al. (2021) emphasize that the neonatal immune system undergoes rapid maturation, and early antigen exposure can shape lifelong immune trajectories. This underscores the need for balanced vaccination scheduling, as timing influences both protective efficacy and immune programming. Similarly, Pasetti et al. (2020) demonstrate that maternal immunity and early-life exposures interact to determine infant immune responses, reinforcing the rationale for balancing vaccine timing with physiological readiness. Garcia-Fogeda et al. (2023) review within-host antibody dynamics, showing that immune responses vary significantly with age and prior exposures. High-intensity vaccination in the first months may alter antibody kinetics, potentially affecting long-term immunity. Instead, Pollard and Bijker (2021) further argue that vaccination policies must integrate principles of immunological development in infants to optimize outcomes, a goal consistent with the VEI framework. Recent work on immune response variability across the life course (Metcalf et al., 2025) suggests that early immune experiences can lead to convergence or divergence in later responses, influencing susceptibility to disease and possibly neurodevelopmental trajectories. While the debate on vaccines and autism remains contentious between scholars, policymakers, journalists, people, etc., these hypothesis-generating findings here support continued investigation into how exposure patterns and concentration of vaccines in childhood immunization program schedules—not vaccine presence per se—might interact with neurodevelopmental processes in children. Technological advances offer opportunities to refine such analyses. Anderson et al. (2025) and Elfatimi et al. (2025) highlight the role of computational tools and AI in modeling vaccine effects and predicting outcomes, which could enhance the predictive power of indices like VEI. Moreover, predictive markers of immunogenicity (Van Tilbeurgh et al., 2021) and exposome-based immunity training (Adams et al., 2020) suggest that exposure order and intensity matter for immune system calibration, lending theoretical support to the idea of adjusting schedules to reduce clustering of doses in early infancy.
The study here highlights the importance of considering vaccine timing and intensity of doses in infants for immunization policy (Hughes et al., 2016). By integrating vaccine concentration and age, it offers a practical tool for surveillance and evidence-based scheduling adjustments. This proposed approach here, with a comparative analysis, seeks to harmonize immunization schedules in similar countries to optimize effects on disease prevention with developmental health, advancing a paradigm of precision vaccinology. Hence, these insights are valuable for researchers, clinicians, and policymakers seeking to balance the benefits of immunization with the neurological safety. It is important to emphasize that these results are exploratory and do not imply a causal link. Our research focuses on immunization schedules, not the safety of vaccines themselves—which are among the most successful public health interventions in human society. We are particularly interested in the trend of clustering multiple immunizations within the first year of life. This study presents hypothesis-generating findings leading to the main scientific question: does this concentrated early exposure require more detailed investigation? Of course, this work here is a call for further research into optimizing schedules to ensure the best possible outcomes for timing, safety, and community protection
5. Conclusions
The introduction of the age-adjusted vaccine exposure index (VEI) provides a novel framework for complementing global efforts to compare vaccination schedules between countries and optimize immunization strategies. The larger significance of this vaccine exposure index (VEI) as a novel and standardized metric is to fill a critical gap in the literature, where most studies have focused on vaccine efficacy and population-level coverage, but few have addressed the individual-level intensity and timing of vaccine administration in infants. By integrating the number of vaccines, doses, and age of administration, the VEI provides a comprehensive measure of early-life vaccine exposure, enabling researchers and policymakers to compare over space and time immunization schedules between and within countries and assess the appropriateness. This approach responds to growing concerns in the scientific community about the potential impact of early and intensive vaccine exposure, especially in vulnerable populations like preterm infants (Davis et al., 1999; Fortmann et al., 2022; Mawson and Jacob,2025; Schmitt et al., 2025). In fact, immunization programs, such as those in the United States, Japan, etc. have historically prioritized high coverage and disease prevention (Roper et al., 2021), proposed VEI index here shows comparative analyses to improve schedules. This aligns with Sustainable Development Goals, where immunization is recognized as a cornerstone of child health and equity (Decouttere et al., 2021). Modeling studies underscore the complexity of immune system development and vaccine response. Morrocchi et al. (2024) highlight in vitro models that simulate neonatal immune responses, revealing that timing and antigen load significantly influence immunogenicity. These findings support the rationale behind VEI, which integrates age and vaccine intensity to monitor exposure patterns. Similarly, Pickering et al. (2020) stress that vaccine licensure and recommendations must consider evolving evidence on safety and efficacy, reinforcing the need for adaptive scheduling frameworks. Safety remains a critical dimension of immunization policy. Conklin et al. (2021) review historical vaccine safety concerns, noting that transparent surveillance tools are essential for maintaining public trust. VEI serves this role by enabling cross-country comparisons and identifying schedules with concentrated early exposure, which may warrant further evaluation. Moreover, maternal immunization strategies—advocated by Quincer et al. (2024) and Santilli et al. (2025)—illustrate how timing adjustments can enhance infant protection without reducing coverage, a principle consistent with VEI’s objectives. Global health frameworks emphasize leveraging vaccines to reduce antimicrobial resistance (Vekemans et al., 2021), underscoring the importance of maintaining robust immunization while refining schedules in infants. The VEI reframes the research problem by shifting the focus from binary debates about vaccine safety to a quantitative, comparative, and developmental perspective. This reframing opens new perspectives for research, including personalized immunization strategies, and cross-national benchmarking of best practices in public health (Kargı and Coccia, 2024; Coccia, 2023; Rodewald et al., 2023; Shattock et al. 2024). In particular, the age-adjusted vaccine exposure index (VEI) goes beyond traditional linear parameters such as the number of vaccines or antigen quantity administered in infancy. While these metrics provide a basic measure of immunization intensity, they fail to capture the comparison of immunological processes between countries that shape early-life immune development. VEI is a descriptive, non-biological metric, and introduces a multidimensional perspective by integrating timing, dose concentration, and age-adjusted exposure, offering insights into how clustered vaccinations may interact with critical developmental stages. By quantifying exposure, VEI provides a proxy for evaluating these complex interactions indirectly. High VEI values indicate schedules with concentrated early dosing. This does not imply risk or causality but supports, with a comparison with other countries, analyses of the effects in society about coverage, emergence diseases, etc. during infancy. VEI offers a data-driven approach to harmonize disease prevention and long-term health, paving the way for precision vaccinology and informed policy reforms. Thus, VEI complements existing vaccinology principles by bridging quantitative measures with qualitative aspects of immune system maturation, supporting a more holistic approach to immunization policy. For policymakers globally, the VEI offers a highly practical and powerful tool for evidence-based analyses. Its specific aim is to compare immunization scheduling between countries and optimize the timing and administration of vaccine by strategically maintaining high and comprehensive coverage while simultaneously reducing the intensity of early-life vaccine exposure. This dual-focus approach has the potential to minimize adverse effects, crucially leading to significantly improved public trust in national immunization programs. In doing so, this research contributes fundamentally to a more robust and balanced approach to global vaccination policy, ensuring that essential disease protection is achieved with the highest possible standards of safety and public confidence (Buttery and Clothier, 2022; Benati and Coccia, 2022; Kargı et a., 2023; Vajdy et al., 2023).
- ▪
- Health policy implications of this study
The age-adjusted vaccine exposure index (VEI) is not merely an analytical metric; it is a practical tool intended to compare schedules and inform immunization policy for improving immunization strategies. By quantifying cumulative vaccine exposure in infants under one year, VEI enables policymakers to evaluate the intensity of national schedules and identify opportunities for optimization. This approach moves beyond coverage rates to address how vaccine clustering and early administration may interact with infant immune development. The health policy implications of this study are substantial, offering a new framework for evaluating and improving national immunization schedules through the proposed age-adjusted vaccine exposure index (VEI). Figure 1 illustrates how countries cluster into distinct quadrants based on their VEI scores and autism rates. Countries such as Norway, Denmark, Finland, and Sweden, located in the bottom-left quadrant, exemplify best practices. These nations maintain high vaccination coverage while minimizing early-life vaccine exposure through delayed administration of non-critical vaccines and lower dose intensity. Their schedules suggest that it is possible to balance disease prevention with long-term neurological health. In contrast, countries in the top-right quadrant—including Australia, Canada, the United States, Singapore, Japan, and South Korea—administer a higher number of vaccines and doses at earlier ages, often starting at birth. These intensive schedules are associated with higher VEI scores and elevated autism rates, raising concerns, especially in vulnerable populations. While these programs aim to maximize protection, they may benefit from reassessing the timing and intensity of vaccine delivery. Italy and the United Kingdom, positioned in the bottom-right quadrant, show relatively high VEI scores but lower autism rates. This aspect may reflect a transitional phase in policy, suggesting an opportunity to align more closely with Nordic models to reduce early-life exposure without compromising coverage in order to optimize vaccine scheduling.
Generally speaking, VEI supports several health policy applications. The Vaccine Exposure Index (VEI) provides a quantitative, not biological, measure of early-life vaccine intensity by considering the number and timing of doses administered during the first year of life. This approach can guide health policy for countries having a high intensive immunization schedule, unlike of other nations, such as Denmark that infant immunization schedule omits certain early vaccines, such as hepatitis B at birth, and delays others beyond the neonatal period. Despite this reduced early exposure, Denmark maintains high coverage rates and reports a comparatively lower incidence of Autism Spectrum Disorder (ASD) in children. Large-scale Danish cohort studies involving over one million children confirm no causal link between vaccines and autism, reinforcing that optimizing timing does not compromise safety (Andersson et al., 2025; Scott, 2025). Denmark, in particular, exemplifies a “leaner” infant immunization schedule. While vaccines are essential for preventing infectious diseases, evidence suggests that strategic scheduling—guided by VEI—can minimize early immune stress without reducing coverage or efficacy. In addition, first, VEI can guide adjustments in vaccine spacing, reducing concentrated dosing during critical developmental windows without compromising protection. Second, it helps prioritize at-risk infant groups, such as those with prematurity or underlying conditions, by tailoring schedules to minimize early-life exposure intensity. Third, VEI allows policymakers to compare immunizations schedules between countries and evaluate cumulative exposure thresholds. This aspect of VEI facilitates comparative analysis of national schedules, enabling countries to benchmark their practices against models with lower VEI scores—such as Scandinavian nations that achieve high coverage while delaying non-essential vaccines and avoiding birth doses. Integrating VEI into WHO and national guidelines would advance precision vaccinology, harmonizing disease prevention with long-term health. Currently, global recommendations prioritize coverage and disease prevention, but they rarely account for cumulative exposure intensity in infants, especially when new vaccines have the approval by federal agencies that protect public health and added in immunization schedules, which should also consider the number sand doses of other vaccines administered by 12 months to avoid interactions, such as new RSV vaccine (Blauvelt et al., 2025; Shaaban et al., 2025). Hence, VEI could serve as an analytical tool within existing frameworks, complementing WHO’s principles of safety, efficacy, and equity. For example, national immunization technical advisory groups (NITAGs) could use VEI to evaluate proposed schedules, identifying periods of concentrated dosing and assessing whether adjustments—such as delaying non-essential vaccines beyond the neonatal phase—might reduce theoretical risks without compromising protection. This proposed approach aligns with WHO’s emphasis on adaptive strategies for diverse populations and supports harmonization across countries by enabling cross-schedule comparisons. Furthermore, VEI could be integrated into digital health platforms and surveillance systems, providing policymakers with real-time insights into comparative analyses, exposure patterns and facilitating predictive modeling for long-term outcomes. In short, the Vaccine Exposure Index (VEI) provides the necessary quantitative evidence to fundamentally shift immunization policy away from a rigid, one-size-fits-all approach and firmly toward personalized, evidence-based vaccination policies. To reiterate, policy-related implications of proposed index does not assess vaccine safety or risk. These strategies are meticulously designed to rigorously maintain the highest possible immunization coverage for the population while simultaneously optimizing timing with a “leaner” infant immunization schedule that does not compromise safety (Andersson et al., 2025; Scott, 2025). In short, while vaccines are essential for preventing infectious diseases, evidence suggests that strategic scheduling—guided by VEI—can minimize early immune stress without reducing coverage or efficacy, thereby ensuring both comprehensive disease prevention and enhanced safety for every child.
These implementations in best practices of public health and practical policy implications are also supported by the fact that VEI fully respects ethical principles by relying exclusively on publicly available data from national immunization schedules. No individual-level or sensitive health information is used, ensuring compliance with privacy and confidentiality standards. This proposed approach guarantees transparency and reproducibility, as all calculations are based on standardized, open-access sources. Furthermore, the fundamental purpose of the Vaccine Exposure Index (VEI) is unequivocally not to question or undermine comprehensive coverage, but rather to furnish policymakers with a robust, evidence-based tool for comparing and optimizing immunization strategies about infants with safety-conscious manner. The ethical integrity of this metric also extends to fostering essential stakeholder engagement. By presenting results in a transparent, clear, and comparative format, the VEI facilitates constructive dialogue among health authorities, pediatric experts, public health organizations, and the public. Its potential integration into key decision-making frameworks—such as WHO guidelines or national technical advisory groups—would directly support inclusive, data-driven policy development. This ensures that any recommendations derived from the VEI are strongly grounded in rigorous scientific evidence and are perfectly aligned with global health priorities, including equity and the paramount goal of universal disease prevention. To put it differently, the VEI promotes responsible innovation in vaccinology by enabling crucial cross-country benchmarking and identifying validated best practices that achieve safety and high coverage, all without imposing reductionist or prescriptive changes to essential immunization programs. The goal of VEI is to compare immunization schedules and improve public health outcomes while maintaining trust in immunization programs. Overall, then, policymakers can use the Vaccine Exposure Index (VEI) to benchmark immunization schedules, identify practices with high cumulative vaccine exposure, and design interventions that minimize early-life exposure in infants under 12 months. This approach also encourages reconsidering the routine addition of every newly approved vaccine to schedules within the first year of life, helping to avoid excessive concentration and potential related risks. In this policy perspective, countries with lower VEI scores, such as those in Scandinavia, demonstrate that high coverage can be achieved with less intensive schedules, offering virtuous models of immunization programs. As a consequence, the VEI thus supports a shift toward personalized, developmentally informed immunization strategies, enhancing both safety and public trust in vaccination programs.
Importantly, the purpose of this study is not to question vaccines, which are among the most significant achievements in public health. Rather, the focus is on the structure of immunization schedules. In some countries, each new vaccine approval leads to its inclusion in the infant schedule, often under 12 months of age. This clustering may create potential interactions among multiple vaccines during a critical developmental phase. Our analysis is therefore hypothesis-generating, exploring whether concentrated early exposure warrants further investigation—not asserting harm. Hence, conclusion of this study presents hypothesis-generating findings with an approach that is entirely focused on comparing and optimizing vaccine scheduling, not reducing doses or coverage. Current safety information from the U.S. Centers for Disease Control and Prevention (CDC) shows that vaccines approved by the FDA are authorized for administration starting from a specific age range—defined by a start point and an endpoint. However, many national programs tend to administer these vaccines as soon as the start point is reached, creating a concentration of doses in the earliest months of life. Our approach suggests distributing these vaccines more evenly over time, including administration beyond 12 months and up to 24 months, whenever possible, and before children enter kindergarten. This strategy aims to maintain full protection while reducing the clustering of multiple vaccines in the first year of life. For example, Denmark’s immunization program spaces core vaccines, achieving excellent protection while avoiding excessive early clustering. Importantly, Denmark maintains very high coverage rates (around 97%), ensuring virtually all infants are protected. In short, the goal is to strengthen global vaccination policies by diluting vaccine administration beyond the first year, rather than concentrating them under 12 months, while continuing to safeguard infant health and maintain high immunization coverage.
- ▪
- Limitations and future prospects
This study introduces the age-adjusted Vaccine Exposure Index (VEI) as an innovative metric for quantifying early-life vaccine exposure in infants under 12 months, providing a standardized framework to compare national immunization schedules. The empirical findings indicate that early and intensive vaccination schedules may be associated with increased neurodevelopmental risks that reflect strictly associative findings; of course, no causal relationship is claimed. The study is presented as an exploratory framework that could inform future research on comparing immunization schedules and optimizing vaccine timing while maintaining high coverage and safety. In fact, proposed index is verified in a homogeneous sample of advanced countries with comparable socioeconomic conditions, similar health infrastructures, and broadly aligned immunization strategies. These nations predominantly follow WHO recommendations and utilize vaccines produced by a limited set of global manufacturers, ensuring consistency in antigen composition and safety standards across schedules. While minor variations exist in timing and sequence, the core vaccines—such as DTP, MMR, polio, and Hib—are universally administered within the first year, making cross-country comparisons meaningful. Previous comparative analyses confirm that these countries share similar disease burdens and vaccination coverage targets, reducing confounding factors related to epidemiology or resource disparities. Hence, the proposed Vaccine Exposure Index (VEI) does not aim to oversimplify public health decisions but rather provides a standardized metric for assessing early-life vaccine intensity within comparable contexts. This facilitates evidence-based evaluation of immunization strategies among advanced nations, where policy adjustments can be considered without undermining disease control objectives. The VEI offers a potential tool for policymakers to compare, evaluate and optimize vaccination strategies globally, aiming to balance disease prevention with adverse effects. By enabling cross-country comparisons, this metric could inform evidence-based adjustments to immunization practices, particularly for vulnerable populations. While catch-up schedules, optional versus mandatory vaccines, and differences in reporting and implementation exist, their impact within this sample is minimal because the analysis concentrates on core vaccines universally administered in infancy where implementation is highly uniform across these countries. We acknowledge that contextual limitations remain but proposed conclusions apply specifically to advanced nations with similar epidemiological profiles and vaccine availability. The proposed Vaccine Exposure Index (VEI) is intended as a universal metric but as a comparative tool for countries with broadly aligned immunization strategies. This targeted scope ensures that policy insights derived from VEI remain valid within the defined context while avoiding overgeneralization. Nevertheless, several constraints should be acknowledged, such as: the analysis relies on cross-sectional data from a limited sample of countries and two large nations, which restricts generalizability; although the selected countries exhibit relatively standardized practices, residual variability cannot be fully eliminated and may influence observed associations; autism prevalence data may differ in accuracy and diagnostic criteria across and within countries, affecting comparability; the VEI currently excludes individual-level factors—such as genetic predisposition or preterm birth—that may influence neurodevelopmental outcomes (Pichichero, 2014; Sadeck & Kfouri, 2023). The study relies on cross-sectional data, which captures associations at a single point in time. This design precludes assessment of temporal relationships and long-term effects. The current index also treats all vaccines as equal units of exposure, which is an intentional simplification for the sake of creating a standardized tool, but it may overlook the specific synergistic effects of certain vaccine combinations. Consequently, the findings should be interpreted as exploratory and hypothesis-generating rather than definitive evidence of any causal relationship.
To conclude, the study does not question vaccine safety or efficacy, which are firmly supported by scientific consensus. Vaccines remain essential for preventing infectious diseases and safeguarding public health. The objective here is to compare and examine immunization schedule design between countries—not vaccine content or effectiveness—and to explore whether concentrated early exposure warrants further investigation. All conclusions are framed as hypothesis-generating. Our results warrant further investigation through also individual-level data to validate the patterns observed with cross-national analysis. Further studies should also conduct longitudinal analyses to assess the impact of vaccine timing and intensity across diverse populations and geographic regions. Moreover, next research should integrate, as just mentioned, individual-level health data with national immunization schedules to refine the VEI and support personalized vaccination strategies. Advancing these research avenues would strengthen the evidence base and enhance the VEI’s utility as a policy instrument for comparing immunization program schedules, ultimately contributing to safer and more effective global vaccination practices while safeguarding infant health.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Mario Coccia Conceptualization; methodology; software; validation; formal analysis; investigation; data curation; writing—original draft preparation; writing—review and editing; visualization; supervision.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available on request to the authors.
Acknowledgments
The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| VEI | Age-adjusted Vaccine exposure Index |
| 1 | The term risk here is intended as statistical measure of frequency also considering that in the fields of pharmacovigilance and epidemiology, risk is defined as the probability or likelihood that a specific disease, adverse reaction, or untoward medical event will occur in an individual within a defined timeframe following the administration of a drug. |
References
- Adams, K.; Weber, K. S.; Johnson, S. M. Exposome and immunity training: how pathogen exposure order influences innate immune cell lineage commitment and function. International Journal of Molecular Sciences 2020, 21(22), 8462. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5-TR (5th edition, text revision); Washington, DC; American Psychiatric Association Publishing, 2022. [Google Scholar]
- Anderson, L. N.; Hoyt, C. T.; Zucker, J. D.; McNaughton, A. D.; Teuton, J. R.; Karis, K.; Kumar, N. Computational tools and data integration to accelerate vaccine development: challenges, opportunities, and future directions. Frontiers in Immunology 2025, 16, 1502484. [Google Scholar] [CrossRef]
- Andersson, NW; Bech Svalgaard, I; Hoffmann, SS; et al. Aluminum-adsorbed vaccines and chronic diseases in childhood. A nationwide cohort study. Ann Intern Med 2025. Epub ahead of print. [Google Scholar] [CrossRef]
- Australia (2025) Australian Government, Department of Health, Disability and Ageing, National Immunization Program for children. https://www.health.gov.au/topics/immunisation/when-to-get-vaccinated/national-immunisation-program-schedule, https://www.health.gov.au/sites/default/files/2025-09/national-immunisation-program-schedule_0.pdf.
- Australian Government (1999) Department of Health and Aged Care, Communicable Diseases Intelligence;n. 6 - 10 June 1999, Immunisation coverage in Australian children: a systematic review 1990-1998 – Appendix. Volume 23. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/cda-pubs-cdi-1999-cdi2306-cdi2306a7.htm (accessed on October 2025).
- Bailey, A; Le Couteur, A; Gottesman, I; Bolton, P; Simonoff, E; Yuzda, E; Rutter, M. Autism as a strongly genetic disorder: evidence from a British twin study. Psychol Med. 1995, 25(1), 63–77. [Google Scholar] [CrossRef]
- Baron-Cohen, S; Hammer, J. Parents of Children with Asperger Syndrome: What is the Cognitive Phenotype? J Cogn Neurosci. 1997, 9(4), 548–54. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S. The hyper-systemizing, assortative mating theory of autism. Prog Neuropsychopharmacol Biol Psychiatry 2006, 30(5), 865–72. [Google Scholar] [CrossRef] [PubMed]
- Benati, I.; Coccia, M. Global analysis of timely COVID-19 vaccinations: improving governance to reinforce response policies for pandemic crises; International Journal of Health Governance, 2022; vol. 27, No. 3, pp. 240–253. [Google Scholar] [CrossRef]
- Blauvelt, C. A.; Zeme, M.; Natarajan, A.; Epstein, A.; Roh, M. E.; Morales, A.; Gaw, S. L. Respiratory syncytial virus vaccine and nirsevimab uptake among pregnant people and their neonates. JAMA network open 2025, 8(2), e2460735–e2460735. [Google Scholar] [CrossRef]
- Boretti, A. Reviewing the association between aluminum adjuvants in the vaccines and autism spectrum disorder. Journal of trace elements in medicine and biology: organ of the Society for Minerals and Trace Elements (GMS) 2021, 66, 126764. [Google Scholar] [CrossRef]
- Brophy-Williams, S.; Fidanza, M.; Marchant, A.; Way, S.; Kollmann, T. R. One vaccine for life: Lessons from immune ontogeny. Journal of paediatrics and child health 2021, 57(6), 782–785. [Google Scholar] [CrossRef]
- Buttery, J. P.; Clothier, H. Information systems for vaccine safety surveillance. Human Vaccines & Immunotherapeutics 2022, 18(6), 2100173. [Google Scholar] [CrossRef]
- Canada. Government of Canada, Recommended immunization schedules: Canadian Immunization Guide. 2025. Available online: https://www.canada.ca/en/public-health/services/publications/healthy-living/canadian-immunization-guide-part-1-key-immunization-information/page-13-recommended-immunization-schedules.html#p1c12a2.
- Benzaken, Casey L.; Miller, Joshua D.; Onono, Maricianah; Young, Sera L. Development of a cumulative metric of vaccination adherence behavior and its application among a cohort of 12-month-olds in western Kenya. Vaccine, Volume 2020, 38(Issue 18), 3429–3435. [Google Scholar] [CrossRef]
- Çatlı, Nermin Eylül; Özyurt, Gonca. The relationship between autism and autism spectrum disorders and vaccination: review of the current literature. Trends in Pediatrics. Review. Open Access 2025. [Google Scholar] [CrossRef]
- CDC. Data and Statistics on Autism Spectrum Disorder. 27 May 2025. Available online: https://www.cdc.gov/autism/data-research/index.html#cdc_data_surveillance_section_3-cdcs-addm-network.
- CDC. Autism Spectrum Disorder (ASD). 2025a. Available online: https://www.cdc.gov/autism/data-research/index.html#cdc_data_surveillance_section_3-cdcs-addm-network (accessed on October 2025).
- CDC. Recommended Childhood Immunization Schedule -- United States, 2000. 2025b. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm4902a4.htm (accessed on October 2025).
- Chinese center for disease control and prevention (2021). Available online: https://en.chinacdc.cn/health_topics/immunization/202203/t20220302_257317.html.
- Coccia, M. Problem-driven innovations in drug discovery: co-evolution of the patterns of radical innovation with the evolution of problems; Health Policy and Technology, 2016; vol. 5, n. 2, pp. 143–155. [Google Scholar] [CrossRef]
- Coccia, M. Effects of human progress driven by technological change on physical and mental health; STUDI DI SOCIOLOGIA, 2021; N. 2; pp. 113–132. [Google Scholar] [CrossRef]
- Coccia, M. COVID-19 in society between 2020 (without vaccinations) and 2021 (with vaccinations): A case study; Journal of Social and Administrative Sciences - J. Adm. Soc. Sci. - JSAS, 2022; Vol. 9, n. 2, pp. 113–130. [Google Scholar] [CrossRef]
- Coccia, M. Improving preparedness for next pandemics: Max level of COVID-19 vaccinations without social impositions to design effective health policy and avoid flawed democracies; Environmental Research, 2022; Volume 213, p. 113566. [Google Scholar] [CrossRef]
- Coccia, M. COVID-19 pandemic over 2020 (with lockdowns) and 2021 (with vaccinations): similar effects for seasonality and environmental factors. Environmental Research 2022a, Volume 208, n. 112711. [Google Scholar] [CrossRef]
- Coccia, M. Optimal levels of vaccination to reduce COVID-19 infected individuals and deaths: A global analysis; Environmental Research, 2022a; vol. 204, Part C, p. 112314. [Google Scholar] [CrossRef]
- Coccia, M. Relation between COVID-19 vaccination and economic development of countries; Turkish Economic Review, 2022b; vol. 9, n. 2, pp. 121–139. [Google Scholar] [CrossRef]
- Coccia, M. COVID-19 Pandemic Crisis: Analysis of origins, diffusive factors and problems of lockdowns and vaccinations to design best policy responses Vol.2; KSP Books; Kadikoy, Istanbul, Turkey, 2023; ISBN 978-625-7813-54-9. (e-Book). [Google Scholar]
- Coccia, M. COVID-19 Vaccination is not a Sufficient Public Policy to face Crisis Management of next Pandemic Threats. Public Organiz Rev 2023, 23, 1353–1367. [Google Scholar] [CrossRef]
- Coccia, M.; Bellitto, M. Human progress and its socioeconomic effects in society; Journal of Economic and Social Thought, 2018; vol. 5, n. 2, pp. 160–178. [Google Scholar] [CrossRef]
- Conklin, L.; Hviid, A.; Orenstein, W. A.; Pollard, A. J.; Wharton, M.; Zuber, P. Vaccine safety issues at the turn of the 21st century. BMJ Global Health 2021, 6 (Suppl 2), e004898. [Google Scholar] [CrossRef]
- Davis, RL; Rubanowice, D; Shinefield, HR; et al. Immunization Levels Among Premature and Low-Birth-Weight Infants and Risk Factors for Delayed Up-to-Date Immunization Status. JAMA 1999, 282(6), 547–553. [Google Scholar] [CrossRef]
- Decouttere, C.; De Boeck, K.; Vandaele, N. Advancing sustainable development goals through immunization: a literature review. Globalization and Health 2021, 17(1), 95. [Google Scholar] [CrossRef]
- Denmark. Statens Serum Institut. Childhood vaccination programme. 2025. Available online: https://en.ssi.dk/vaccination/the-danish-childhood-vaccination-programme.
- Doja, A; Roberts, W. Immunizations and autism: a review of the literature. Can J Neurol Sci 2006, 33(4), 341–6. [Google Scholar] [CrossRef] [PubMed]
- Eicher, T.; Quackenbush, J.; Ne'eman, A. Challenging Claims of an Autism Epidemic - Misconceptions and a Path Forward. The New England journal of medicine 2026, 394(4), 313–315. [Google Scholar] [CrossRef]
- Elfatimi, E.; Lekbach, Y.; Prakash, S.; BenMohamed, L. Artificial intelligence and machine learning in the development of vaccines and immunotherapeutics—yesterday, today, and tomorrow. Frontiers in Artificial Intelligence 2025, 8, 1620572. [Google Scholar] [CrossRef]
- Estes, A; Munson, J; Rogers, SJ; Greenson, J; Winter, J; Dawson, G. Long-term outcomes of early intervention in 6-year-old children with autism spectrum disorder. J Am Acad Child Adolescent Psych 2015, 54, 580–87. [Google Scholar] [CrossRef]
- Finland. Finnish Institute for Health and Welfare. Vaccination programme for children and adults. 2025. Available online: https://thl.fi/en/topics/infectious-diseases-and-vaccinations/information-about-vaccinations/vaccination-programme-for-children-and-adults.
- Fortmann, MI; Dirks, J; Goedicke-Fritz, S; Liese, J; Zemlin, M; Morbach, H; Härtel, C. Immunization of preterm infants: current evidence and future strategies to individualized approaches. Semin Immunopathol 2022, 44(6), 767–784. [Google Scholar] [CrossRef]
- Frenkel, LD. The global burden of vaccine-preventable infectious diseases in children less than 5 years of age: Implications for COVID-19 vaccination. How can we do better? Allergy Asthma Proc. 2021, 42(5), 378–385. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Fogeda, I.; Besbassi, H.; Lariviere, Y.; Ogunjimi, B.; Abrams, S.; Hens, N. Within-host modeling to measure dynamics of antibody responses after natural infection or vaccination: A systematic review. Vaccine 2023, 41(25), 3701–3709. [Google Scholar] [CrossRef]
- GBD 2023 Vaccine Coverage Collaborators. Global, regional, and national trends in routine childhood vaccination coverage from 1980 to 2023 with forecasts to 2030: a systematic analysis for the Global Burden of Disease Study 2023. Lancet 2025, 406(10500), 235–260. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Geier, D. A.; Kern, J. K.; Homme, K. G.; Geier, M. R. Abnormal Brain Connectivity Spectrum Disorders Following Thimerosal Administration: A Prospective Longitudinal Case-Control Assessment of Medical Records in the Vaccine Safety Datalink. Dose-response: a publication of International Hormesis Society 2017, 15(1), 1559325817690849. [Google Scholar] [CrossRef]
- Global Burden of Disease Study 2021 Autism Spectrum Collaborators. The global epidemiology and health burden of the autism spectrum: findings from the Global Burden of Disease Study 2021. Lancet Psychiatry 2025, 12(2), 111–121. [CrossRef]
- Grosvenor, LP; Croen, LA; Lynch, FL; Marafino, BJ; Maye, M; Penfold, RB; Simon, GE; Ames, JL. Autism Diagnosis Among US Children and Adults, 2011-2022. JAMA Netw Open 2024, 7(10), e2442218. [Google Scholar] [CrossRef] [PubMed]
- Gulati, S; Sharawat, IK; Panda, PK; Kothare, SV. The vaccine-autism connection: No link, still debate, and we are failing to learn the lessons. Autism 2025, 29(7), 1639–1645. [Google Scholar] [CrossRef]
- Haeuser, Emily; et al. Global, regional, and national trends in routine childhood vaccination coverage from 1980 to 2023 with forecasts to 2030: a systematic analysis for the Global Burden of Disease Study 2023. The Lancet 2025, 406(Issue 10500), 235–260. [Google Scholar] [CrossRef] [PubMed]
- Howlin, P; Magiati, I. Autism spectrum disorder: outcomes in adulthood. Curr Opin Psychiatry 2017, 30, 69–76. [Google Scholar] [CrossRef]
- Hughes, MM; Katz, J; Englund, JA; Khatry, SK; Shrestha, L; LeClerq, SC; Steinhoff, M; Tielsch, JM. Infant vaccination timing: Beyond traditional coverage metrics for maximizing impact of vaccine programs, an example from southern Nepal. Vaccine 2016, 34(7), 933–41. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Immunization Safety Review: Vaccines and Autism; Washington, DC; The National Academies Press, 2004. [Google Scholar] [CrossRef]
- Institute of Medicine. Adverse Effects of Vaccines: Evidence and Causality; Washington, DC; The National Academies Press, 2012. [Google Scholar] [CrossRef]
- Institute of Medicine. The Childhood Immunization Schedule and Safety: Stakeholder Concerns, Scientific Evidence, and Future Studies; Washington, DC; The National Academies Press, 2013. [Google Scholar] [CrossRef]
- Issac, A; Halemani, K; Shetty, A; Thimmappa, L; Vijay, VR; Koni, K; Mishra, P; Kapoor, V. The global prevalence of autism spectrum disorder in children: a systematic review and meta-analysis. Osong Public Health Res Perspect 2025, 16(1), 3–27. [Google Scholar] [CrossRef]
- Italy (2025), Regione Lombardia, Calendario Vaccinale. Available online: https://www.wikivaccini.regione.lombardia.it/wps/portal/site/wikivaccini/DettaglioRedazionale/vaccinazioni-disponibili/calendario-vaccinale.
- Japan. Changes in the Immunization Schedule Recommended by the Japan Pediatric Society, May 19, 2025. 2025. Available online: https://www.jpeds.or.jp/uploads/files/20250205_Immunization_Schedule_english.pdf.
- Japanese Pediatric Society. Changes in the Immunization Schedule Recommended. 2025. Available online: https://www.jpeds.or.jp/uploads/files/20250205_Immunization_Schedule_english.pdf (accessed on 22 October 2025).
- Kargı, B.; Coccia, M.; Uçkaç, B. C. How does the wealth level of nations affect their COVID19 vaccination plans? Economics, Management and Sustainability 2023, 8(2), 6–19. [Google Scholar] [CrossRef]
- Kargı, B.; Coccia, M. Rethinking the Role of Vaccinations in Mitigating COVID-19 Mortality: A Cross-National Analysis. KMÜ Sosyal ve Ekonomik Araştırmalar Dergisi, KMU Journal of Social and Economic Research 2024, 26(47), 1173–1192. [Google Scholar] [CrossRef]
- Lai, JKY; Weiss, JA. Priority service needs and receipt across the lifespan for individuals with autism spectrum disorder. Autism Res 2017, 10, 1436–47. [Google Scholar] [CrossRef]
- Lord, C; Charman, T; Havdahl, A; et al. The Lancet Commission on the future of care and clinical research in autism. Lancet 2022, 399, 271–334. [Google Scholar] [CrossRef]
- Magazzino, C.; Mele, M.; Coccia, M. A machine learning algorithm to analyze the effects of vaccination on COVID-19 mortality; Epidemiology and infection, 2022; pp. 1–24. [Google Scholar] [CrossRef]
- Mawson, AR; Jacob, B. Vaccination and Neurodevelopmental Disorders: A Study of Nine-Year-Old Children Enrolled in Medicaid. Science, Public Health Policy and the Law 2025, 6, 55–61. Available online: https://publichealthpolicyjournal.com/vaccination-and-neurodevelopmental-disorders-a-study-of-nine-year-old-children-enrolled-in-medicaid/ (accessed on December 7, 2025).
- Metcalf, C. J. E.; Graham, A. L.; Yates, A. J.; Cummings, D. A. Convergence and divergence of individual immune responses over the life course. Science 2025, 389(6760), 604–609. [Google Scholar] [CrossRef]
- Ministry of health; family welfare. Government of India, National Health Mission, National Immunization Schedule. 2018. Available online: https://nhm.gov.in/New_Updates_2018/NHM_Components/Immunization/report/National_%20Immunization_Schedule.pdf.
- Miravalle, AA; Schreiner, T. Neurologic complications of vaccinations. Handb Clin Neurol 2014, 121, 1549–57. [Google Scholar] [CrossRef] [PubMed]
- Morrocchi, E.; van Haren, S.; Palma, P.; Levy, O. Modeling human immune responses to vaccination in vitro. Trends in immunology 2024, 45(1), 32–47. [Google Scholar] [CrossRef]
- Nair, KS; George, RL; Remya, VR; A R, P; Saji, CV; Mullasseril, RR; Shenoi, RA; Nair, J; Krishna, R; N K, K; Thomas, A; Varughese, D; Chandra, G; Mohanakumar, KP; Rajamma, U. Prevalence Estimates of Neurodevelopmental Disorders (NDD) in a South Indian Population. Ann Neurosci 2025, 09727531251348188. [Google Scholar] [CrossRef] [PubMed]
- Nath, A. Neurologic Complications With Vaccines: What We Know, What We Don't, and What We Should Do. Neurology 2023, 101(14), 621–626. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine 2025. Statement on CDC’s Changes to Guidance on Vaccines and Autism. 2025. Available online: https://www.nationalacademies.org/news/statement-on-cdc-s-changes-to-guidance-on-vaccines-and-autism?utm_source=NASEM+News+and+Publications&utm_campaign=b32b20d912-NAP+Mail+New+2025.11.24&utm_medium=email&utm_term=0_-1c0f2fa5e6-112916397&mc_cid=b32b20d912&mc_eid=ddceeca657 (accessed on December 2025).
- National Academies of Sciences; Engineering; and Medicine. Guidance on Routine Childhood Immunizations; Washington, DC; The National Academies Press, 2024. [Google Scholar] [CrossRef]
- National Academies of Sciences; Engineering; and Medicine. The Comprehensive Autism Care Demonstration: Solutions for Military Families; Washington, DC; The National Academies Press, 2025. [Google Scholar] [CrossRef]
- National Academies of Sciences; Engineering; and Medicine. Vaccine Risk Monitoring and Evaluation at the Centers for Disease Control and Prevention; Washington, DC; The National Academies Press, 2025. [Google Scholar] [CrossRef]
- Norway (2025). Norwegian Institute of Public Health. Vaccination of children in Norway. [Internet]. Oslo: The Norwegian Directorate of Health; updated Thursday, April 4, 2024 [retrieved Friday, October 3, 2025]. Available from: https://www.helsenorge.no/en/information-in-english/vaccination-of-children/ and https://www.fhi.no/en/va/childhood-immunisation-programme/when-will-your-child-be-offered-vaccines/.
- Nouri, N.; Cao, R.G.; Bunsow, E.; et al. Young infants display heterogeneous serological responses and extensive but reversible transcriptional changes following initial immunizations. Nat Commun 2023, 14, 7976. [Google Scholar] [CrossRef]
- O'Leary, K. Antibiotics reduce vaccine responses in infants; Nat Med, 30 Apr 2025. [Google Scholar] [CrossRef]
- Pasetti, M. F.; Ackerman, M. E.; Hoen, A. G.; Alter, G.; Tsang, J. S.; Marchant, A. Maternal determinants of infant immunity: Implications for effective immunization and maternal-child health. Vaccine 2020, 38(28), 4491. [Google Scholar] [CrossRef] [PubMed]
- Pichichero, ME. Challenges in vaccination of neonates, infants and young children. Vaccine 2014, 32(31), 3886–94, Epub. [Google Scholar] [CrossRef]
- Pickering, L. K.; Meissner, H. C.; Orenstein, W. A.; Cohn, A. C. Principles of vaccine licensure, approval, and recommendations for use. In Mayo Clinic Proceedings; Elsevier, March 2020; Vol. 95, No. 3, pp. 600–608. [Google Scholar]
- Pollard, A. J.; Bijker, E. M. A guide to vaccinology: from basic principles to new developments. Nature Reviews Immunology 2021, 21(2), 83–100. [Google Scholar] [CrossRef]
- Principi, N; Esposito, S. Aluminum in vaccines: Does it create a safety problem? Vaccine 2018, 36(39), 5825–5831. [Google Scholar] [CrossRef] [PubMed]
- Quincer, E. M.; Cranmer, L. M.; Kamidani, S. Prenatal maternal immunization for infant protection: a review of the vaccines recommended, infant immunity and future research directions. Pathogens 2024, 13(3), 200. [Google Scholar] [CrossRef]
- Ramachandran, P; Grose, C. Serious neurological adverse events in immunocompetent children and adolescents caused by viral reactivation in the years following varicella vaccination. Rev Med Virol 2024, 34(3), e2538. [Google Scholar] [CrossRef]
- Reuters. Autism rates: Why are they on the rise. By Nancy Lapid, April 17. 2025; Available online: https://www.reuters.com/business/healthcare-pharmaceuticals/why-are-autism-rates-rising-2025-01-14/.
- Rodewald, L; Maes, E; Stevenson, J; Lyons, B; Stokley, S; Szilagyi, P. Immunization performance measurement in a changing immunization environment. Pediatrics 2023, 103 4 Pt 2, 889–97. [Google Scholar] [CrossRef]
- Roper, L.; Hall, M. A. K.; Cohn, A. Overview of the United States’ immunization program. The Journal of infectious diseases 2021, 224 (Supplement_4), S443–S451. [Google Scholar] [CrossRef]
- Sadarangani, M.; Kollmann, T.; Bjornson, G.; Heath, P.; Clarke, E.; Marchant, A.; Munoz, F. M. The Fifth International Neonatal and Maternal Immunization Symposium (INMIS 2019): securing protection for the next generation. Msphere 2021, 6(1), 10–1128. [Google Scholar] [CrossRef]
- Sadeck, LDSR; Kfouri, RÁ. An update on vaccination in preterm infants. J Pediatr (Rio J) 2023, 99 Suppl 1(Suppl 1), S81–S86. [Google Scholar] [CrossRef]
- Sandbank, M; Bottema-Beutel, K; Crowley LaPoint, S; et al. Autism intervention meta-analysis of early childhood studies (Project AIM): updated systematic review and secondary analysis. BMJ 2023, 383, e076733. [Google Scholar] [CrossRef]
- Santilli, V.; Sgrulletti, M.; Costagliola, G.; Beni, A.; Mastrototaro, M. F.; Montin, D.; Moschese, V. Maternal Immunization: Current Evidence, Progress, and Challenges. Vaccines 2025, 13(5), 450. [Google Scholar] [CrossRef]
- Schmitt, C.; Goedicke-Fritz, Sybelle; Fortmann, Ingmar; Zemlin, Michael. Vaccinations in preterm infants: Which and when? Seminars in Fetal and Neonatal Medicine 2025, 101670. [Google Scholar] [CrossRef]
- Scientific American. The Real Reasons Autism Rates Are Up in the U.S. By Jessica Wright & Spectrum. 3 March 2017. Available online: https://www.scientificamerican.com/article/the-real-reasons-autism-rates-are-up-in-the-u-s/#.
- Scott, J. Why Denmark’s vaccine schedule works for Denmark — but not for the United States. The two countries have fundamentally different health care systems and disease burdens. STAT10. 2025. Available online: https://www.statnews.com/2025/12/19/denmark-vaccine-schedule-vs-us/.
- Semmes, EC; Chen, JL; Goswami, R; Burt, TD; Permar, SR; Fouda, GG. Understanding Early-Life Adaptive Immunity to Guide Interventions for Pediatric Health. Front Immunol 2021, 11, 595297. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shaaban, F. L.; Groenendijk, R. W.; Baral, R.; Caballero, M. T.; Crowe, J. E.; Englund, J. A.; Bont, L. J. The path to equitable respiratory syncytial virus prevention for infants: challenges and opportunities for global implementation; The Lancet Global Health, 2025. [Google Scholar]
- Shapiro, G. K.; Kaufman, J.; Brewer, N. T.; Wiley, K.; Menning, L.; Leask, J.; BeSD Working Group. A critical review of measures of childhood vaccine confidence. Current opinion in immunology 2021, 71, 34–45. [Google Scholar] [CrossRef] [PubMed]
- Shattock, Andrew J; et al. Contribution of vaccination to improved survival and health: modelling 50 years of the Expanded Programme on Immunization. The Lancet 2024, 403(Issue 10441), 2307–2316. [Google Scholar] [CrossRef] [PubMed]
- Shaw, KA; Williams, S; Patrick, ME; Valencia-Prado, M; Durkin, MS; Howerton, EM; Ladd-Acosta, CM; Pas, ET; Bakian, AV; Bartholomew, P; Nieves-Muñoz, N; Sidwell, K; Alford, A; Bilder, DA; DiRienzo, M; Fitzgerald, RT; Furnier, SM; Hudson, AE; Pokoski, OM; Shea, L; Tinker, SC; Warren, Z; Zahorodny, W; Agosto-Rosa, H; Anbar, J; Chavez, KY; Esler, A; Forkner, A; Grzybowski, A; Agib, AH; Hallas, L; Lopez, M; Magaña, S; Nguyen, RHN; Parker, J; Pierce, K; Protho, T; Torres, H; Vanegas, SB; Vehorn, A; Zhang, M; Andrews, J; Greer, F; Hall-Lande, J; McArthur, D; Mitamura, M; Montes, AJ; Pettygrove, S; Shenouda, J; Skowyra, C; Washington, A; Maenner, MJ. Prevalence and Early Identification of Autism Spectrum Disorder Among Children Aged 4 and 8 Years - Autism and Developmental Disabilities Monitoring Network, 16 Sites, United States, 2022. MMWR Surveill Summ 2025, 74(2), 1–22. [Google Scholar] [CrossRef] [PubMed]
- Singapour (2025) Government of Singapore, Communicable Diseases Agency, Vaccinations, Table 1: National Childhood Immunisation Schedule. https://www.cda.gov.sg/public/vaccinations and https://isomer-user-content.by.gov.sg/18/00b7fdea-24a1-4c26-b67e-d6618f31d6cb/NCIS_Sept%202025.pdf.
- South Korea (2025). Vaccination for infants, Yangcheon-Gu Office, Seul. https://www.yangcheon.go.kr/english/english/04/10402030000002016110903.jsp and https://www.gunsan.go.kr/_cms/board/eFileDownload/434/1449916/12b2c60c49317fc21ea41eb435a79159.
- Strunecka, A.; Blaylock, R. L.; Patocka, J.; Strunecky, O. Immunoexcitotoxicity as the central mechanism of etiopathology and treatment of autism spectrum disorders: A possible role of fluoride and aluminum. Surgical neurology international 2018, 9, 74. [Google Scholar] [CrossRef]
- Sweden. Vaccination programmes. The Public Health Agency of Sweden. 2025. Available online: https://www.folkhalsomyndigheten.se/the-public-health-agency-of-sweden/communicable-disease-control/vaccinations/vaccination-programmes/ (accessed on October, 2025).
- Swedish Council on Health Technology Assessment. Vaccines to Children: Protective Effect and Adverse Events: A Systematic Review [Internet]. SBU Yellow Report No. 191; Stockholm; Swedish Council on Health Technology Assessment (SBU), Feb 2009. [PubMed]
- Talantseva, OI; Romanova, RS; Shurdova, EM; Dolgorukova, TA; Sologub, PS; Titova, OS; Kleeva, DF; Grigorenko, EL. The global prevalence of autism spectrum disorder: A three-level meta-analysis. Front. Psychiatry 2023, 14, 1071181. [Google Scholar] [CrossRef]
- Tomljenovic, L; Shaw, CA. Do aluminum vaccine adjuvants contribute to the rising prevalence of autism? J Inorg Biochem. 2011, 105(11), 1489–99. [Google Scholar] [CrossRef] [PubMed]
- Tregoning G. 2022. Neonatal Immunology, Category: Immune Development, British Society for immunology. https://www.immunology.org/public-information/bitesized-immunology/immune-development/neonatal-immunology; https://www.immunology.org/sites/default/files/2022-08/Neonatal%20Immunology.pdf (accessed 12 January 2026).
- UK. NHS vaccinations and when to have them. 2025. Available online: https://www.nhs.uk/vaccinations/nhs-vaccinations-and-when-to-have-them/ (accessed on October, 2025).
- USA (2025). CDC, Vaccines & Immunizations , Child and Adolescent Immunization Schedule by Age (Addendum updated August 7, 2025). https://www.cdc.gov/vaccines/hcp/imz-schedules/child-adolescent-catch-up.html; https://www.cdc.gov/vaccines/hcp/imz-schedules/downloads/child/0-18yrs-child-combined-schedule.pdf (Accessed October, 2025).
- Vajdy, M.; Rath, B. A.; Talaat, K. R. Immunological aspects of vaccine safety. Frontiers in immunology 2023, 14, 1212148. [Google Scholar] [CrossRef]
- Van Tilbeurgh, M.; Lemdani, K.; Beignon, A. S.; Chapon, C.; Tchitchek, N.; Cheraitia, L.; Manet, C. Predictive markers of immunogenicity and efficacy for human vaccines. Vaccines 2021, 9(6), 579. [Google Scholar] [CrossRef] [PubMed]
- Vazquez, JA; Rao, ASRS. 2025 Immunizations, Autism, and Statistical Analysis. Am J Med 2025, 138(9), 1175–1176. [Google Scholar] [CrossRef] [PubMed]
- Vekemans, J.; Hasso-Agopsowicz, M.; Kang, G.; Hausdorff, W. P.; Fiore, A.; Tayler, E.; Lipsitch, M. Leveraging vaccines to reduce antibiotic use and prevent antimicrobial resistance: a World Health Organization action framework. Clinical Infectious Diseases 2021, 73(4), e1011–e1017. [Google Scholar] [CrossRef] [PubMed]
- World Population Review (2025), Autism Rates by Country 2025. Available online: https://worldpopulationreview.com/country-rankings/autism-rates-by-country.
- World Population Review (2025a), Vaccination Rates by Country 2025. Available online: https://worldpopulationreview.com/country-rankings/vaccination-rates-by-country.
Figure 1.
Regression line of the autism rate on vaccine exposure index (VEI) in infants ≤ 1 year with the location of countries under study. Note: Each quadrant is labeled with policy implications: critical zone – high vaccine exposure and high autism rates; protective policy zone – low vaccine exposure and low autism rates; transitional zone – high vaccine exposure but currently low autism rates; emerging risk zone –not populated in current data.
Figure 1.
Regression line of the autism rate on vaccine exposure index (VEI) in infants ≤ 1 year with the location of countries under study. Note: Each quadrant is labeled with policy implications: critical zone – high vaccine exposure and high autism rates; protective policy zone – low vaccine exposure and low autism rates; transitional zone – high vaccine exposure but currently low autism rates; emerging risk zone –not populated in current data.
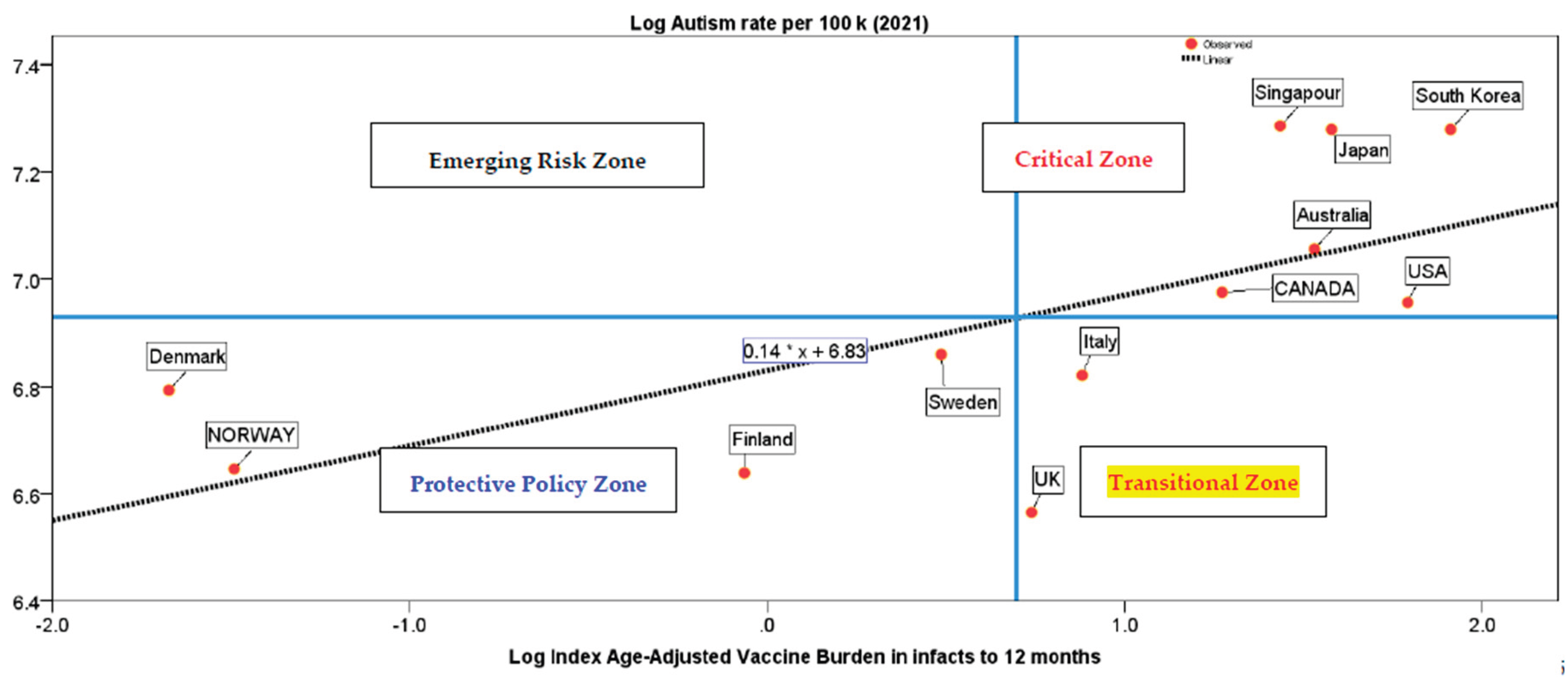

Table 1.
Data, sources and variables.
| Variables and sources | Description |
| Period under study | Year 2020, 2021 (last year available) in dataset |
| Countries. Source: World Population Review (2025), https://worldpopulationreview.com/country-rankings/autism-rates-by-country | Countries and related autism rate in World Population Review (2025): Singapore, South Korea, Japan, Australia, Canada, USA, Sweden, Denmark, Norway, Finland, Italy, and the UK |
| Autism rate 2021 per 100k people in countries under study, Source: World Population Review (2025), https://worldpopulationreview.com/country-rankings/autism-rates-by-country | Normalized rates indicate the number of children out of 100,000 who have been diagnosed at any age with autism, year 2021. |
| Months of infants (having ≤ 1 year) in immunization dates | Month of infants (having ≤ 1 year) to which vaccines are administered, set according to the country's recommended childhood vaccination schedule and designed by public health bodies. |
| Total number of vaccines to infants from birth to 6 months and from birth to 12 months | Total number of vaccines administered to infants having less than 1 year (recommended or compulsory) from national childhood immunization schedule in sample of countries under study. Sources of data in Table S1. |
| Number of doses of vaccines to infants ≤ 1 year from birth to 6 months and from birth to 12 months | Total number of doses of vaccines administered to infants having less than 1 year (recommended or compulsory) from national childhood immunization schedule in sample of countries under study. Sources of data in Table S1. |
| Vaccination Rates (%), Source: World Population Review (2025a), Vaccination Rates by Country 2020, https://worldpopulationreview.com/country-rankings/vaccination-rates-by-country | Average Percentage of Vaccination Rates 2020, Vaccinations address the following diseases: DTP3 - Diphtheria, Tetanus, and Pertussis; MCV1 - Measles and POL3 – Polio; Data estimates from WHO/UNICEF Estimates of National Immunization Coverage |
| Details for National Immunization Program Schedules for children | See Table S1 in Supplemental Information |
Table 2.
Descriptive statistics (M=arithmetic mean; SD=Standard Deviation).
| Groups of countries | Vacc Rate % | Autism Rate |
Average Age infants 12 months |
Average Age infants 6 months | Total Vacc. to 12 months | Total Vacc. to 6 months | Total Doses. to 12 months | Total Doses. to 6 months | Vaccine exposure to 12 months | |
| LOWER Autism rate | M | 94.56 | 834.33 | 5.90 | 3.42 | 8.00 | 7.17 | 9.33 | 6.50 | 83.50 |
| SD | 2.40 | 98.78 | 0.63 | 0.70 | 2.83 | 1.72 | 5.32 | 3.73 | 62.22 | |
| HIGHER Autism rate | M | 95.00 | 1273.33 | 4.90 | 3.09 | 14.83 | 9.83 | 19.67 | 14.83 | 291.50 |
| SD | 2.89 | 200.67 | 0.45 | 0.39 | 0.98 | 1.60 | 3.67 | 3.06 | 56.94 | |
| NO Varicella vaccine | M | 94.80 | 817.80 | 5.91 | 3.63 | 7.20 | 6.60 | 8.40 | 6.00 | 66.60 |
| SD | 2.60 | 100.73 | 0.70 | 0.50 | 2.28 | 1.14 | 5.37 | 3.94 | 51.94 | |
| Varicella Vaccine | M | 94.76 | 1222.43 | 5.03 | 2.98 | 14.43 | 9.86 | 18.86 | 14.00 | 273.86 |
| SD | 2.71 | 227.37 | 0.54 | 0.45 | 1.40 | 1.46 | 3.98 | 3.56 | 69.86 | |
| NO Hep. B Vaccine | M | 94.25 | 829.75 | 5.73 | 3.54 | 7.50 | 6.75 | 9.75 | 7.00 | 78.75 |
| SD | 2.64 | 112.14 | 0.65 | 0.53 | 2.52 | 1.26 | 5.12 | 3.74 | 51.11 | |
| Hepatitis B Vaccine | M | 95.04 | 1165.88 | 5.24 | 3.11 | 13.38 | 9.38 | 16.88 | 12.50 | 241.88 |
| SD | 2.63 | 264.38 | 0.76 | 0.55 | 3.25 | 1.92 | 6.71 | 5.37 | 111.20 | |
| NO Birth Vaccines | M | 94.80 | 817.80 | 5.91 | 3.63 | 7.20 | 6.60 | 8.40 | 6.00 | 66.60 |
| SD | 2.60 | 100.73 | 0.70 | 0.50 | 2.28 | 1.14 | 5.37 | 3.94 | 51.94 | |
| Birth Vaccine | M | 94.67 | 1238.00 | 4.75 | 2.96 | 14.80 | 9.60 | 19.20 | 14.60 | 283.80 |
| SD | 3.10 | 202.41 | 0.28 | 0.24 | 1.10 | 1.67 | 3.90 | 3.36 | 60.06 | |
| Unclear | M | 95.00 | 1183.50 | 5.74 | 3.04 | 13.50 | 10.50 | 18.00 | 12.50 | 249.00 |
| SD | 2.36 | 376.89 | 0.09 | 1.00 | 2.12 | 0.71 | 5.66 | 4.95 | 114.55 | |
| Groups of countries | Vaccine exposure to 6 months | Average vaccines by 12 months | Average vaccines by 6 months | Average Doses by 12 months |
Average Doses by 6 months |
Monthly vaccine exposure to 12 months | Monthly vaccine exposure to 6 months | Vaccine exposure Index to 12 months | Vaccine exposure Index to 6 months | |
| LOWER Autism rate | M | 50.33 | 0.67 | 1.19 | 0.78 | 1.08 | 6.96 | 8.39 | 1.25 | 2.83 |
| SD | 33.38 | 0.24 | 0.29 | 0.44 | 0.62 | 5.19 | 5.56 | 0.95 | 2.32 | |
| HIGHER Autism rate | M | 145.00 | 1.24 | 1.64 | 1.64 | 2.47 | 24.29 | 24.17 | 5.00 | 7.91 |
| SD | 34.77 | 0.08 | 0.27 | 0.31 | 0.51 | 4.74 | 5.80 | 1.18 | 2.18 | |
| NO Varicella vaccine | M | 42.40 | 0.60 | 1.10 | 0.70 | 1.00 | 5.55 | 7.07 | 1.01 | 2.11 |
| SD | 30.34 | 0.19 | 0.19 | 0.45 | 0.66 | 4.33 | 5.06 | 0.84 | 1.68 | |
| Varicella Vaccine | M | 137.14 | 1.20 | 1.64 | 1.57 | 2.33 | 22.82 | 22.86 | 4.63 | 7.70 |
| SD | 37.95 | 0.12 | 0.24 | 0.33 | 0.59 | 5.82 | 6.32 | 1.46 | 2.07 | |
| NO Hep. B Vaccine | M | 50.00 | 0.63 | 1.13 | 0.81 | 1.17 | 6.56 | 8.33 | 1.21 | 2.52 |
| SD | 29.02 | 0.21 | 0.21 | 0.43 | 0.62 | 4.26 | 4.84 | 0.83 | 1.64 | |
| Hepatitis B Vaccine | M | 121.50 | 1.11 | 1.56 | 1.41 | 2.08 | 20.16 | 20.25 | 4.08 | 6.80 |
| SD | 56.50 | 0.27 | 0.32 | 0.56 | 0.90 | 9.27 | 9.42 | 2.06 | 3.18 | |
| NO Birth Vaccines | M | 42.40 | 0.60 | 1.10 | 0.70 | 1.00 | 5.55 | 7.07 | 1.01 | 2.11 |
| SD | 30.34 | 0.19 | 0.19 | 0.45 | 0.66 | 4.33 | 5.06 | 0.84 | 1.68 | |
| Birth Vaccine | M | 138.80 | 1.23 | 1.60 | 1.60 | 2.43 | 23.65 | 23.13 | 5.03 | 7.93 |
| SD | 34.97 | 0.09 | 0.28 | 0.32 | 0.56 | 5.01 | 5.83 | 1.32 | 2.44 | |
| Unclear | M | 133.00 | 1.13 | 1.75 | 1.50 | 2.08 | 20.75 | 22.17 | 3.63 | 7.13 |
| SD | 60.81 | 0.18 | 0.12 | 0.47 | 0.82 | 9.55 | 10.14 | 1.72 | 0.98 |
Table 3.
Independent Samples Test based on average mean of variables under study in higher and lower autism rate groups of countries, log scale in variables.
Table 3.
Independent Samples Test based on average mean of variables under study in higher and lower autism rate groups of countries, log scale in variables.
| Levene’s Test for Equality of Variances | t-test for Equality of Means | |||||
| Variables | Equal Variances | F | Sig. | t-test | Degrees of Freedom | Sig. (2-tailed) |
| Vaccination Rate Total |
assumed | 0.394 | 0.544 | -0.282 | 10 | 0.784 |
| not assumed | -0.282 | 9.679 | 0.784 | |||
| Autism rate 100k | assumed | 3.81 | 0.079 | -5.133 | 10 | 0.001 |
| not assumed | -5.133 | 9.246 | 0.001 | |||
| Average Age Infants vaccinated to 12 months | assumed | 0.871 | 0.373 | 3.224 | 10 | 0.009 |
| not assumed | 3.224 | 9.822 | 0.009 | |||
| Average Age Infants vaccinated to 6 months | assumed | 2.962 | 0.116 | 0.854 | 10 | 0.413 |
| not assumed | 0.854 | 7.807 | 0.418 | |||
| Total Vaccines done to 12 months (V12) | assumed | 10.742 | 0.008 | -4.654 | 10 | 0.001 |
| not assumed | -4.654 | 5.4 | 0.005 | |||
| Total Vaccines done to 6 months (V6) | assumed | 0.214 | 0.654 | -2.78 | 10 | 0.019 |
| not assumed | -2.78 | 8.933 | 0.022 | |||
| Total Doses done to 12 months (D12) | assumed | 13.241 | 0.005 | -2.927 | 10 | 0.015 |
| not assumed | -2.927 | 5.704 | 0.028 | |||
| Total Doses done to 6 months (D6) | assumed | 13.914 | 0.004 | -3.09 | 10 | 0.011 |
| not assumed | -3.09 | 5.817 | 0.022 | |||
| Vaccine exposure done to 12 months (V12×D12) | assumed | 12.262 | 0.006 | -3.691 | 10 | 0.004 |
| not assumed | -3.691 | 5.391 | 0.012 | |||
| Vaccine exposure done to 6 months (V6×D6) | assumed | 14.469 | 0.003 | -3.282 | 10 | 0.008 |
| not assumed | -3.282 | 5.641 | 0.018 | |||
| Average Vaccines done by 12 months | assumed | 10.742 | 0.008 | -4.654 | 10 | 0.001 |
| not assumed | -4.654 | 5.4 | 0.005 | |||
| Average Vaccines done by 6 months | assumed | 0.214 | 0.654 | -2.78 | 10 | 0.019 |
| not assumed | -2.78 | 8.933 | 0.022 | |||
| Average Doses done by 12 months | assumed | 13.241 | 0.005 | -2.927 | 10 | 0.015 |
| not assumed | -2.927 | 5.704 | 0.028 | |||
| Average Doses done by 6 months | assumed | 13.914 | 0.004 | -3.09 | 10 | 0.011 |
| not assumed | -3.09 | 5.817 | 0.022 | |||
| Monthly vaccine exposure to 12 months | assumed | 12.262 | 0.006 | -3.691 | 10 | 0.004 |
| not assumed | -3.691 | 5.391 | 0.012 | |||
| Monthly vaccine exposure to 6 months | assumed | 14.469 | 0.003 | -3.282 | 10 | 0.008 |
| not assumed | -3.282 | 5.641 | 0.018 | |||
| Age-Adjusted Vaccine exposure Index to 12 months | assumed | 13.406 | 0.004 | -3.767 | 10 | 0.004 |
| not assumed | -3.767 | 5.426 | 0.011 | |||
| Age-Adjusted Vaccine exposure Index to 6 months | assumed | 11.263 | 0.007 | -2.975 | 10 | 0.014 |
| not assumed | -2.975 | 5.541 | 0.027 | |||
Note: T-test groups are based on higher vs. lower autism rate countries.
Table 4.
Partial Correlation, (1-tailed), controlling Vaccination Rates (%) in population.
|
Control Variables: General vaccination rate in population |
A | B | C | D | E | F | G | H | I | L | M | ||
| Autism Rate | A | r | 1 | -0.71 | -0.39 | 0.87 | 0.77 | 0.79 | 0.80 | 0.85 | 0.83 | 0.85 | 0.80 |
| sig. | . | 0.007 | 0.117 | 0 | 0.003 | 0.002 | 0.001 | 0 | 0.001 | 0.001 | 0.001 | ||
| Average Age infants by 12 months | B | r | 1 | 0.60 | -0.78 | -0.57 | -0.84 | -0.84 | -0.85 | -0.81 | -0.88 | -0.82 | |
| sig. | 0.025 | 0.002 | 0.033 | 0.001 | 0.001 | 0.001 | 0.001 | 0 | 0.001 | ||||
| Average Age infants by 6 months | C | r | 1 | -0.62 | -0.52 | -0.64 | -0.60 | -0.65 | -0.60 | -0.66 | -0.70 | ||
| sig. | 0.022 | 0.052 | 0.017 | 0.026 | 0.015 | 0.025 | 0.014 | 0.008 | |||||
| Average Vaccines infants by 12 months | D | r | 1 | 0.91 | 0.86 | 0.85 | 0.94 | 0.90 | 0.94 | 0.90 | |||
| sig. | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||||||
| Average Vaccines infants by 6 months | E | r | 1 | 0.81 | 0.80 | 0.88 | 0.88 | 0.85 | 0.87 | ||||
| sig. | 0.001 | 0.002 | 0.00 | 0.00 | 0.00 | 0.00 | |||||||
| Average Doses infants by 12 months | F | r | 1 | 1.00 | 0.98 | 0.99 | 0.98 | 0.99 | |||||
| sig. | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||||||||
| Average Doses infants by 6 months | G | r | 1 | 0.97 | 0.99 | 0.97 | 0.98 | ||||||
| sig. | 0.00 | 0.00 | 0.00 | 0.00 | |||||||||
| Vaccine exposure to 12 months | H | r | 1 | 0.99 | 1.00 | 0.99 | |||||||
| sig. | 0.00 | 0.00 | 0.00 | ||||||||||
| Vaccine exposure to 6 months | I | r | 1 | 0.98 | 0.99 | ||||||||
| sig. | 0.00 | 0.00 | |||||||||||
| Age-Adjusted Vaccine exposure Index to 12 months | L | r | 1 | 0.99 | |||||||||
| sig. | 0.00 | ||||||||||||
| Age-Adjusted Vaccine exposure Index to 6 months | M | r | 1 | ||||||||||
| sig. | . |
Table 5.
Parametric estimates of the linear model considering as response variables Autism rate 2021 per 100k people (log-log linear model with simple and multivariate regression).
Table 5.
Parametric estimates of the linear model considering as response variables Autism rate 2021 per 100k people (log-log linear model with simple and multivariate regression).
| Simple regression | Explanatory variable: Monthly vaccine exposure in infants to 1 year | ||||
| Dependent variable | Constant, α | Coefficient, β1 | Stand. Coeff. Beta | R2 | F |
| Autism rate 2021 per 100k | 6.16*** | 0.16* | 0.68 | 0.46 | 8.38* |
| Explanatory variable: Index vaccine exposure (VEI12) in infants to 1 year | |||||
| Constant, α | Coefficient, β1 | Stand. Coeff. Beta | R2 | F | |
| Autism rate 2021 per 100k | 6.83*** | 0.14* | 0.67 | 0.46 | 8.34* |
| Multivariate regression | Response variable: Autism rate 2021 per 100k | ||||
| Predictors | |||||
| Constant | −18.24* | ||||
| Vaccine exposure index in infants to 1 year (VEI12) | 0.16*** | ||||
| Vaccination rate for Diphtheria, Tetanus, and Pertussis, Measles and Polio diseases | 5.51** | ||||
| R2 | 0.78 | ||||
| F | 16.31*** | ||||
Note: ***=p-value<0.001, **=p-value<0.01,*=p-value<0.05.
Table 6.
Bootstrap on regression analysis.
| Bootstrap for Coefficients | Bootstrap a) | BCa 95% Confidence Interval | |||||
| B | Bias | Std. Error | Sig. (2-tailed) |
Lower | Upper | ||
| (Constant) | 6.83 | -0.032 | 0.101 | <.001 | 6.631 | 6.902 | |
| Index vaccine exposure (VEI12) in infants to 1 year | 0.143 | 0.021 | 0.075 | 0.048 | 0.058 | 0.469 | |
Note: Bootstrap specifications: number of samples 1000, confidence interval 95%, Confidence Interval Type is Bias-corrected and accelerated (BCa); a) Unless otherwise noted, bootstrap results are based on 1000 bootstrap samples.
Table 7.
Vaccines, doses and autism rate in China and India.
| China | India | |
| Total Vaccines | 10 | 14 |
| Total Doses | 12 | 19 |
| Vaccination Coverage DTP3, POL3 | 97% | 91% |
| Vaccination Coverage MCV1 | 97% | 93% |
| Autism rate 2023 per 100k | 484 | 509 |
Note: DTP3 (diphtheria, tetanus, pertussis), POL3 (Polio), MCV1 (Measles).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



