Submitted:
03 February 2026
Posted:
06 February 2026
You are already at the latest version
Abstract
Valve-in-ring (ViR) transcatheter mitral valve replacement (TMVR) is an established therapeutic option for patients with failed surgical mitral valve repair at high surgical risk. Left ventricular outflow tract (LVOT) obstruction and prosthesis-related complications are well described, but other postprocedural findings remain poorly characterized. We report a challenging case of a persistent LVOT mass following ViR TMVR. A 78-year-old man underwent transapical ViR TMVR with a Sapien 3 valve for mitral stenosis. Early post-procedural echocardiography showed normal prosthetic function and no LVOT obstruction. During inpatient cardiac rehabilitation, transthoracic echocardiography revealed a mobile mass into the LVOT. The patient didn’t show any clinical, microbiological, or laboratory evidence of infection. Blood cultures were negative, and the mass showed no changes despite anticoagulation. Two- and three-dimensional transesophageal echocardiography demonstrated a mobile structure attached to the mitral prosthetic ring by a thin peduncle. After comprehensive multimodality assessment, thrombus and infective endocarditis were considered unlikely. The mass was ultimately interpreted as a displaced remnant of the native anterior mitral leaflet. Given the prohibitive surgical risk and absence of complications, conservative management with echocardiographic follow-up was adopted. This case emphasizes the role of advanced echocardiography and multimodality analysis in avoiding misdiagnosis and inappropriate therapeutic interventions.
Keywords:
valve-in-ring
; transcatheter heart valve replacement
; native mitral valve remnant
; 3D transesophageal echocardiography
; structural heart disease
1. Introduction
Valve-in-ring (ViR) transcatheter mitral valve replacement (TMVR) has emerged as a valuable therapeutic option for patients with failed surgical mitral valve repair who are deemed at high or prohibitive surgical risk. Data from prospective trials and large registries have demonstrated acceptable short- and mid-term clinical and hemodynamic outcomes in carefully selected patients [1,2]. Nevertheless, ViR TMVR remains a complex procedure, and both acute and late complications continue to be reported.
Among the most feared complications, left ventricular outflow tract (LVOT) obstruction has been extensively described, particularly in patients with a long or redundant anterior mitral leaflet. The interaction between preserved native leaflet tissue and the implanted transcatheter valve may lead to dynamic LVOT compromise, prompting the development of preventive techniques such as intentional anterior leaflet modification [3,4]. Other reported complications include valve malposition, residual mitral regurgitation, paravalvular leak, and prosthesis dysfunction [5].
However, the presence of a persistent mobile mass within the LVOT after ViR TMVR, mimicking thrombus or infective endocarditis and ultimately suspected to represent a remnant of the native mitral valve, has not been previously described as a distinct mass-like finding. We report a diagnostically challenging case that highlights the importance of multimodality imaging and careful differential diagnosis following ViR TMVR.
2. Case Presentation
A 78-year-old man with a history of surgical mitral valve repair performed in 2001 was referred for worsening exertional dyspnea due to progressive mitral valve stenosis. Given the high operative risk, the Heart Team recommended a transcatheter approach. In May 2025, the patient underwent ViR TMVR via a transapical approach using a balloon-expandable Edwards Sapien 3 bioprosthesis (29 mm). The procedure was uneventful, with optimal valve positioning and no immediate peri-procedural complications.
A few days before TMVR, the patient had undergone percutaneous coronary intervention with drug-eluting stent implantation in the left anterior descending artery and first diagonal branch.
Early postoperative transthoracic echocardiography (TTE) demonstrated normal prosthetic valve function, no residual mitral regurgitation, and no evidence of LVOT obstruction. Severe tricuspid regurgitation was noted but was not associated with hemodynamic instability.
On May 30th, 2025, during admission to an in-hospital cardiac rehabilitation program, a routine TTE revealed an iso-echogenic, mobile, pedunculated mass located near the aortic valve plane and protruding into the LVOT. The precise site of attachment could not be clearly identified. The mass measured approximately 11 x 9 x 17 mm.
Throughout hospitalization, the patient remained asymptomatic. No fever or signs of systemic infection were observed. Laboratory investigations showed normal procalcitonin levels and only mild, non-specific elevation of inflammatory markers. Blood cultures were repeatedly negative, except for a single isolate of Staphylococcus epidermidis, which was considered contamination.
Given the possibility of a thrombotic mass, oral anticoagulation with warfarin was initiated. A follow-up TTE performed after approximately two weeks of anticoagulation (with INR in therapeutic range) showed no change in the size or morphology of the mass.
A transesophageal echocardiogram (TEE, Figure 1 and Figure 2) confirmed the presence of a mildly hyperechogenic mobile mass.
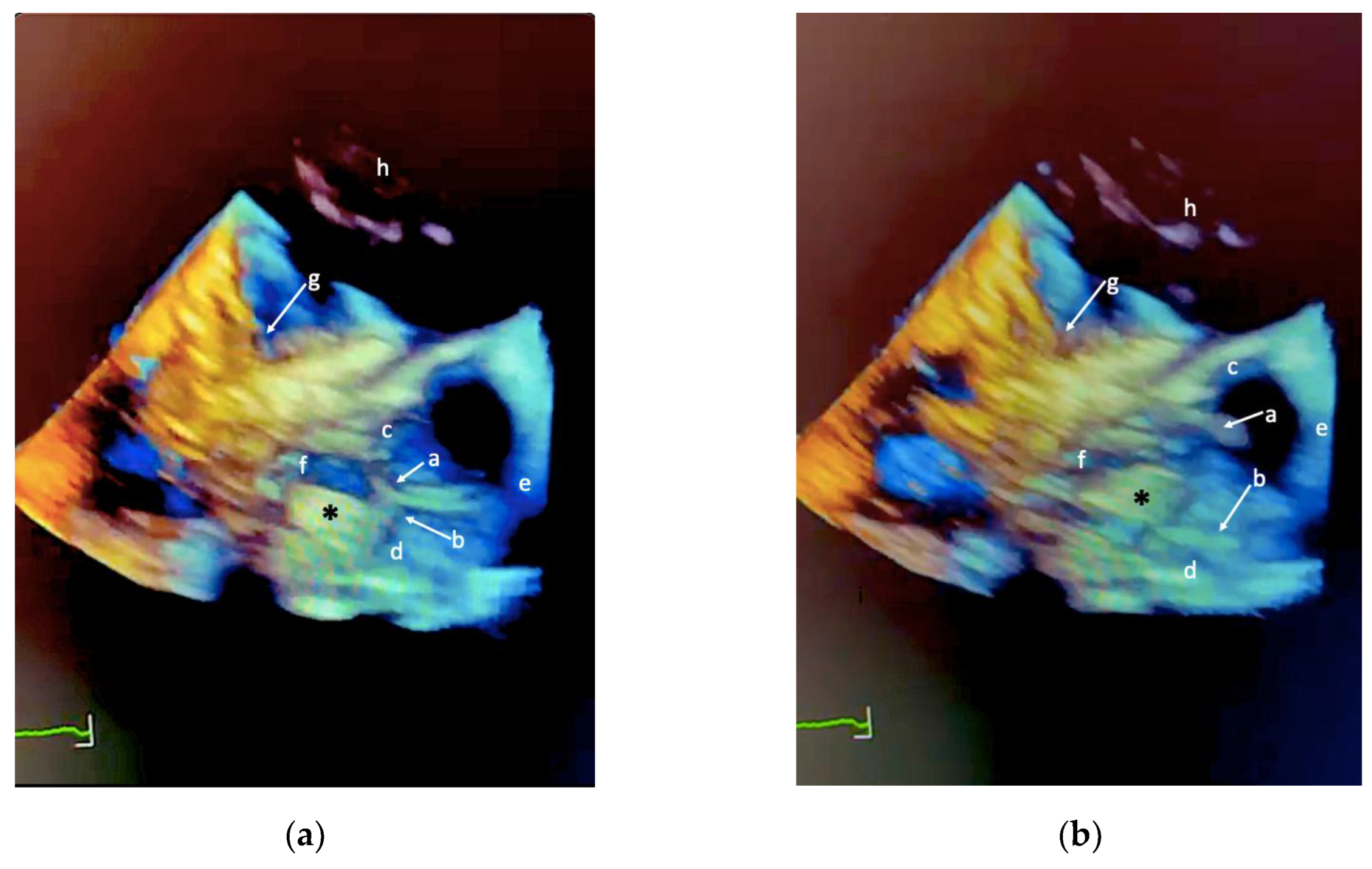
However, acoustic shadowing from the mitral prosthetic ring limited accurate identification of its anchoring site. To improve anatomical characterization, a three-dimensional TEE (Figure 3) was subsequently performed using a different imaging platform. This examination revealed a highly mobile mass attached to the mitral prosthetic ring by a very thin peduncle, extending toward the LVOT. Although the initial appearance raised concern for infective endocarditis, further multiparametric evaluation favored an alternative diagnosis.
A final TTE before discharge confirmed persistence and stability of the mass, with no evidence of embolization or hemodynamic compromise. Given the patient’s prohibitive surgical risk, reintervention was not recommended by the Heart Team.
At follow-up, a telephone contact revealed that the patient died in August 2025 due to pulmonary infection and its related complications, in the context of multiple comorbidities and frailty, and not as a consequence of the underlying cardiac condition.
3. Discussion
This case illustrates a rare and diagnostically challenging finding following ViR TMVR: a persistent mobile mass protruding into the LVOT. The main differential diagnoses included thrombus formation, infective endocarditis, native mitral valve remnant, and, less likely, a primary cardiac tumor.
A thrombotic origin was initially considered because of its potential reversibility. However, several findings argued against this hypothesis. The LVOT is characterized by high-velocity blood flow, making thrombus persistence unlikely. Moreover, the mass remained unchanged after prolonged therapeutic anticoagulation, and its echocardiographic appearance was not typical of thrombotic material.
Infective endocarditis was also considered, particularly given the highly mobile and pedunculated morphology observed on three-dimensional TEE. Nevertheless, the complete absence of clinical signs of infection, persistently negative blood cultures, normal procalcitonin levels, and only mild, non-specific inflammatory marker elevation strongly argued against this diagnosis.
The hypothesis of a remnant of the native mitral valve (most likely a displaced portion of the anterior leaflet) appeared the most plausible explanation. Preservation of native leaflet tissue during TMVR is a well-recognized contributor to LVOT-related complications, and strategies aimed at reducing leaflet interference have been developed [3,4]. While the literature has largely focused on dynamic LVOT obstruction, little attention has been paid to the potential for leaflet remnants to assume abnormal positions after ViR TMVR.
In our case, the echocardiographic texture of the mass, its stability over time, resistance to high-flow conditions, and lack of response to anticoagulation support a fibrous or calcified structure rather than thrombus or vegetation. Late complications related to preserved native mitral tissue have previously been described in surgical series, lending further plausibility to this interpretation [6].
Advanced imaging modalities such as cardiac magnetic resonance or positron emission tomography were considered. However, given the patient’s advanced age, frailty, and the limited impact of additional imaging on management, a conservative strategy based on serial echocardiographic follow-up was adopted. Despite the absence of embolic events, the persistence of a mobile LVOT mass implies a potential embolic risk, warranting close surveillance.
To our knowledge, this represents the first detailed description of a suspected native mitral valve remnant presenting as a mobile LVOT mass after valve-in-ring TMVR, a finding that appears to be rare and poorly characterized.
4. Conclusions
This case underscores the complexity of post-procedural findings after ViR TMVR and the importance of careful differential diagnosis when a mobile intracardiac mass is detected. Multimodality echocardiography, particularly three-dimensional TEE, is crucial for distinguishing among thrombus, vegetation, and native tissue remnants. Awareness of this potential complication may help avoid unnecessary or inappropriate therapeutic interventions.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/doi/s1, Video S1: 3D Transesophageal echocardiography with mobile intracardiac mass.
Funding
This paper received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of ICS Maugeri, IRCCS (protocol code CTSM 197-25, November 6th, 2025).
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to single patient privacy.
Acknowledgments
This work was supported by the Ricerca Corrente funding scheme of the Ministry of Health, Italy.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| 2D | Two-dimensional |
| 3D | Three-dimensional |
| LVOT | left ventricular outflow tract |
| TEE | transesophageal echocardiogram |
| TMVR | transcatheter mitral valve replacement |
| TTE | transthoracic echocardiography |
| ViR | Valve-in-ring |
References
- Guerrero, M.; Wang, D.D.; Eleid, M.F.; et al. One-year outcomes of transcatheter mitral valve replacement in the MITRAL trial: Valve-in-ring arm. JACC Cardiovasc. Interv. 2021, 14, 846–858. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, M.; Vemulapalli, S.; Xiang, Q.; et al. Five-year outcomes of transcatheter mitral valve replacement: Valve-in-valve, valve-in-ring, and valve-in-mitral annular calcification. JACC Cardiovasc. Interv. 2023, 16, 2211–2227. [Google Scholar] [CrossRef] [PubMed]
- Greenbaum, A.B.; Babaliaros, V.C.; Chen, M.Y.; et al. Long or redundant leaflet complicating transcatheter mitral valve replacement. Catheter. Cardiovasc. Interv. 2018, 92, 627–632. [Google Scholar] [PubMed]
- Khan, J.M.; Babaliaros, V.C.; Greenbaum, A.B.; et al. Intentional laceration of the anterior mitral valve leaflet to prevent left ventricular outflow tract obstruction during transcatheter mitral valve replacement. JACC Cardiovasc. Interv. 2016, 9, 1835–1843. [Google Scholar] [PubMed]
- Buzzati, N.; De Bonis, M.; Denti, P.; Alfieri, O. Odd residual regurgitation after mitral valve-in-ring. JACC Cardiovasc. Interv. 2020, 13, 1372–1375. [Google Scholar] [CrossRef] [PubMed]
- Esper, E.; Ferdinand, F.D.; Aronson, S. Prosthetic mitral valve replacement: Late complications after native valve preservation. Ann. Thorac. Surg. 1997, 63, 541–543. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Transesophageal echocardiography of the left ventricular outflow tract (LVOT) acquired during systole, illustrating the anatomical relationships between a mobile intracardiac mass (*) and adjacent cardiac structures. (a) Two-dimensional (2D) B-mode image. (b) 2D color Doppler image. In both panels: a = right coronary aortic cusp; b = non-coronary aortic cusp; c = right sinus of Valsalva; d = non-coronary sinus of Valsalva; e = ascending aorta; f = LVOT; g = mitral leaflet; h = left atrium; i = acoustic shadowing from the prosthetic mitral annulus.
Figure 1.
Transesophageal echocardiography of the left ventricular outflow tract (LVOT) acquired during systole, illustrating the anatomical relationships between a mobile intracardiac mass (*) and adjacent cardiac structures. (a) Two-dimensional (2D) B-mode image. (b) 2D color Doppler image. In both panels: a = right coronary aortic cusp; b = non-coronary aortic cusp; c = right sinus of Valsalva; d = non-coronary sinus of Valsalva; e = ascending aorta; f = LVOT; g = mitral leaflet; h = left atrium; i = acoustic shadowing from the prosthetic mitral annulus.
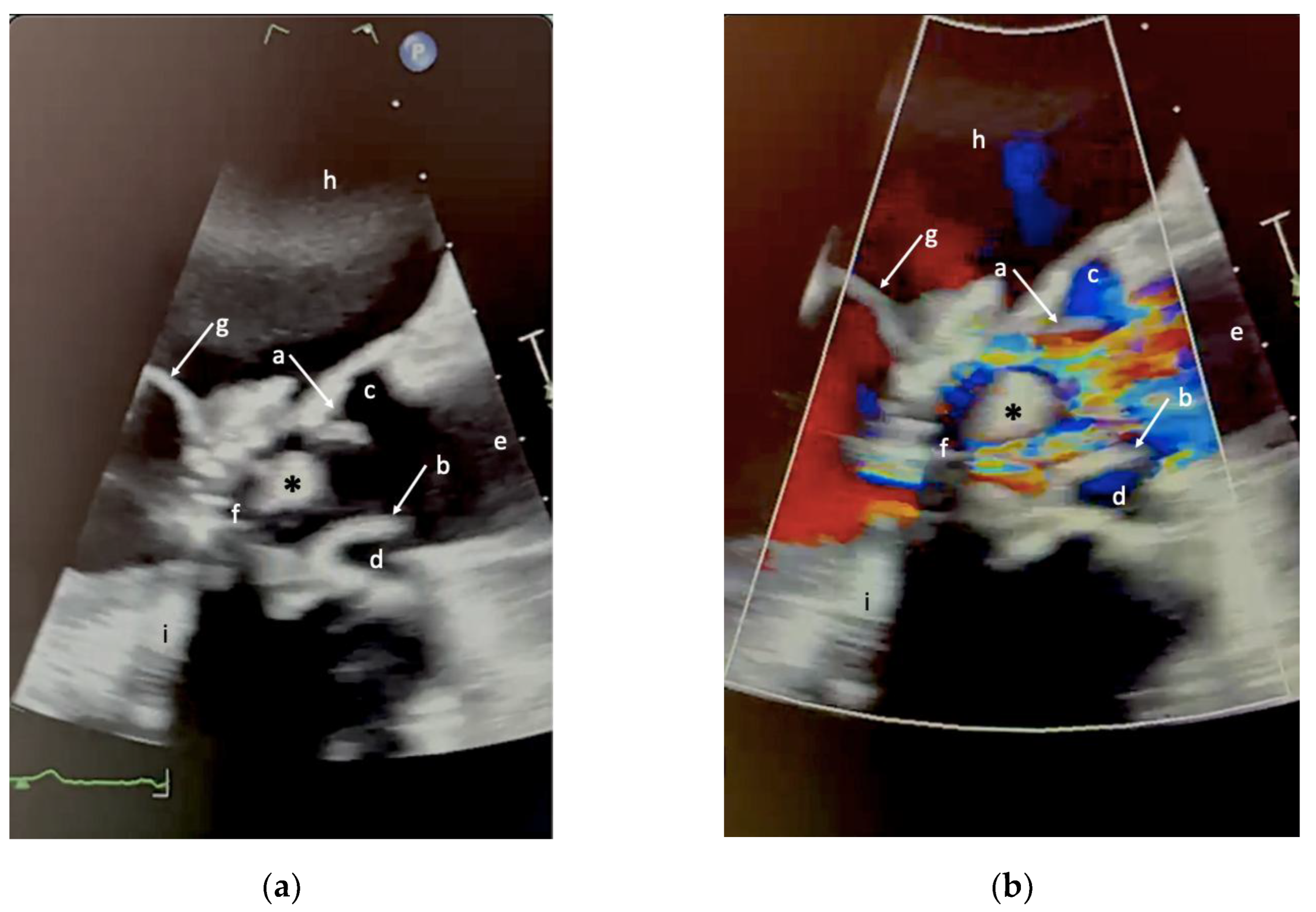
Figure 2.
Transesophageal echocardiography of the left ventricular outflow tract (LVOT) illustrating the anatomical relationships between the mobile intracardiac mass (*) and adjacent cardiac structures during diastole and systole. (a) Two-dimensional (2D) B-mode image in diastole. (b) 2D B-mode image in systole. Anatomical labels (a - i) correspond to those reported in Figure 1.
Figure 2.
Transesophageal echocardiography of the left ventricular outflow tract (LVOT) illustrating the anatomical relationships between the mobile intracardiac mass (*) and adjacent cardiac structures during diastole and systole. (a) Two-dimensional (2D) B-mode image in diastole. (b) 2D B-mode image in systole. Anatomical labels (a - i) correspond to those reported in Figure 1.
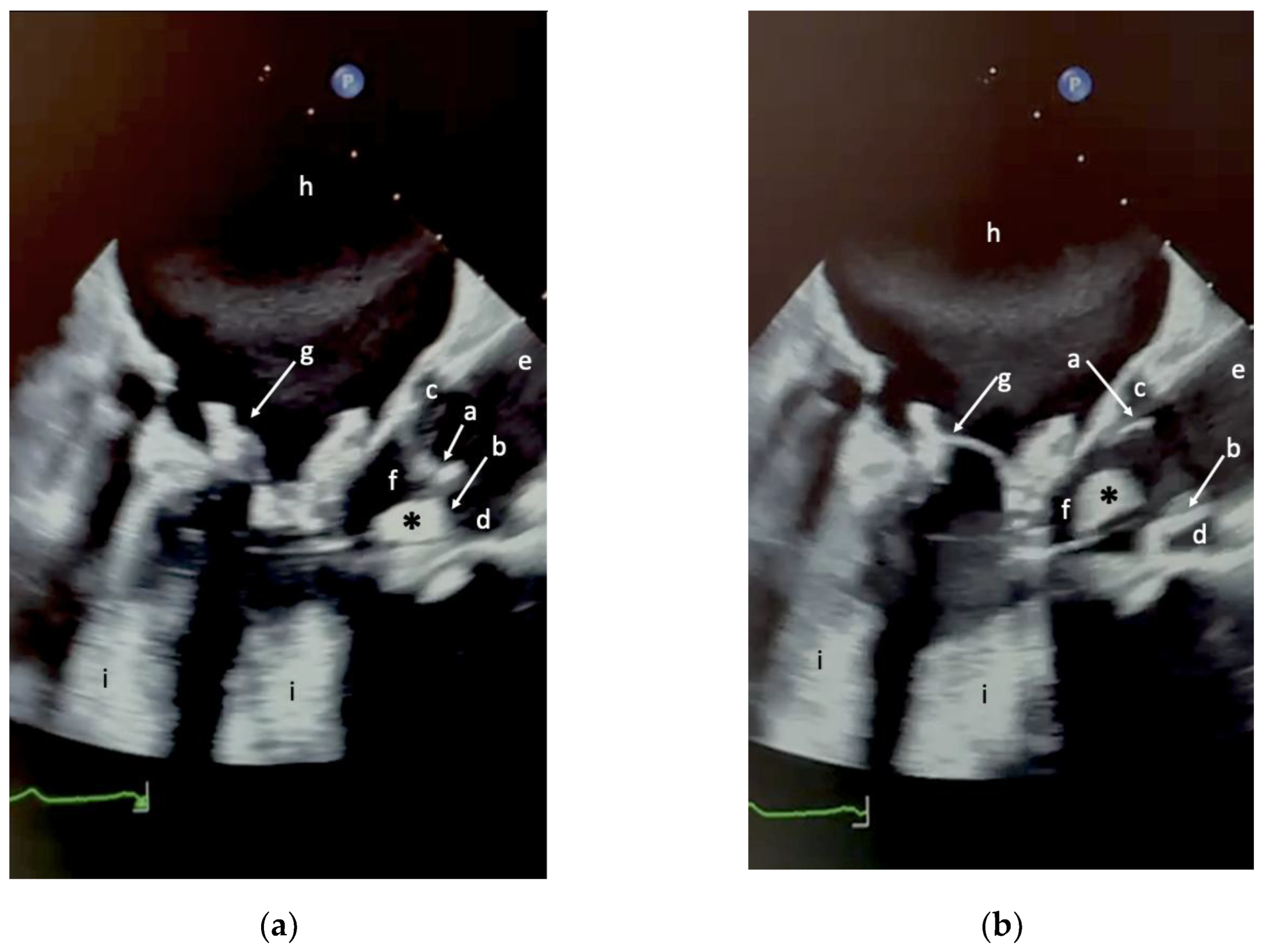
Figure 3.
3D Transesophageal echocardiography of the left ventricular outflow tract (LVOT) illustrating the anatomical relationships between the mobile intracardiac mass (*) and adjacent cardiac structures during diastole and systole. (a) Two-dimensional (2D) B-mode image in diastole. (b) 2D B-mode image in systole. Anatomical labels (a - h) correspond to those reported in Figure 1 and Figure 2.
Figure 3.
3D Transesophageal echocardiography of the left ventricular outflow tract (LVOT) illustrating the anatomical relationships between the mobile intracardiac mass (*) and adjacent cardiac structures during diastole and systole. (a) Two-dimensional (2D) B-mode image in diastole. (b) 2D B-mode image in systole. Anatomical labels (a - h) correspond to those reported in Figure 1 and Figure 2.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



