Submitted:
03 February 2026
Posted:
05 February 2026
You are already at the latest version
Abstract
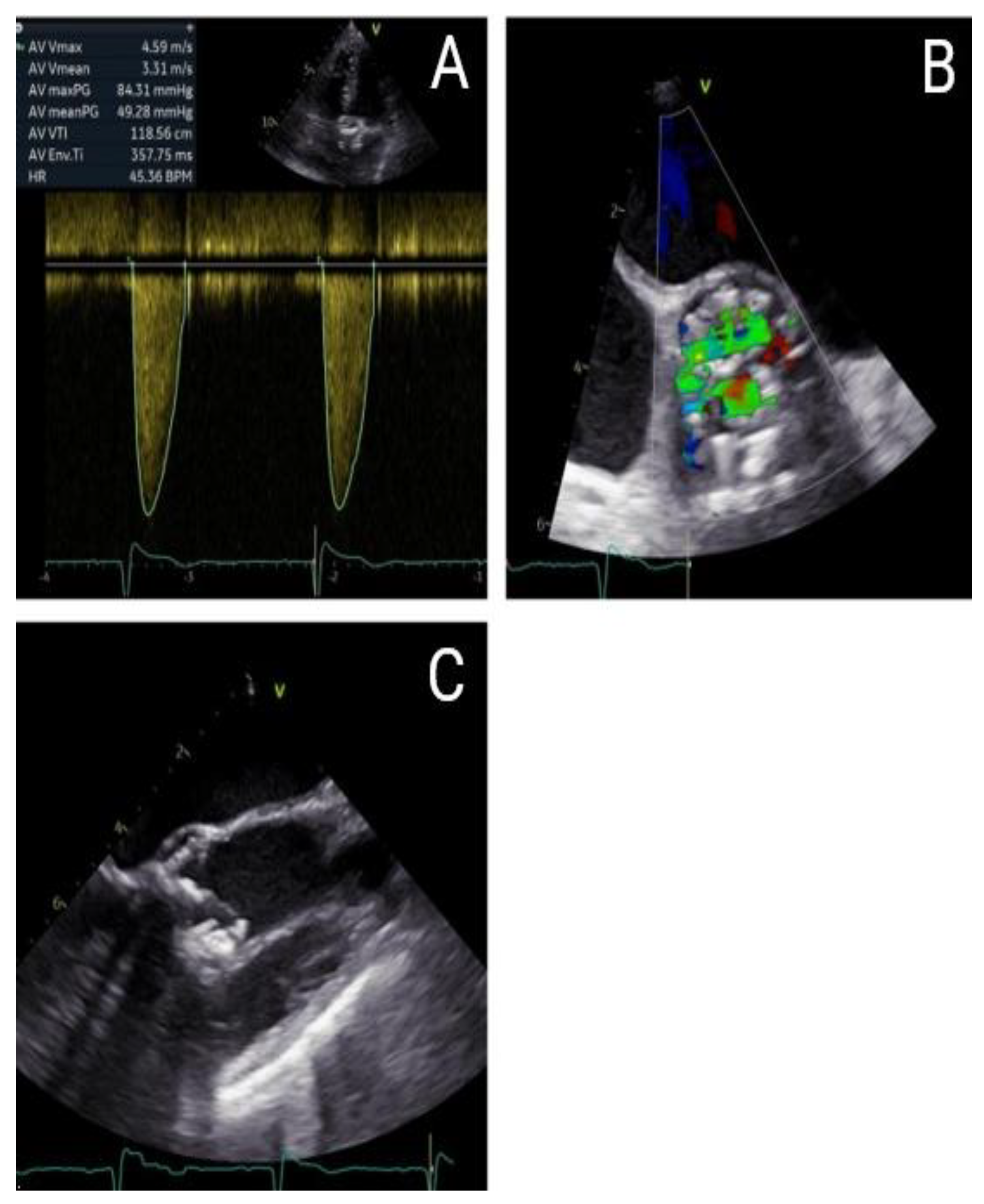
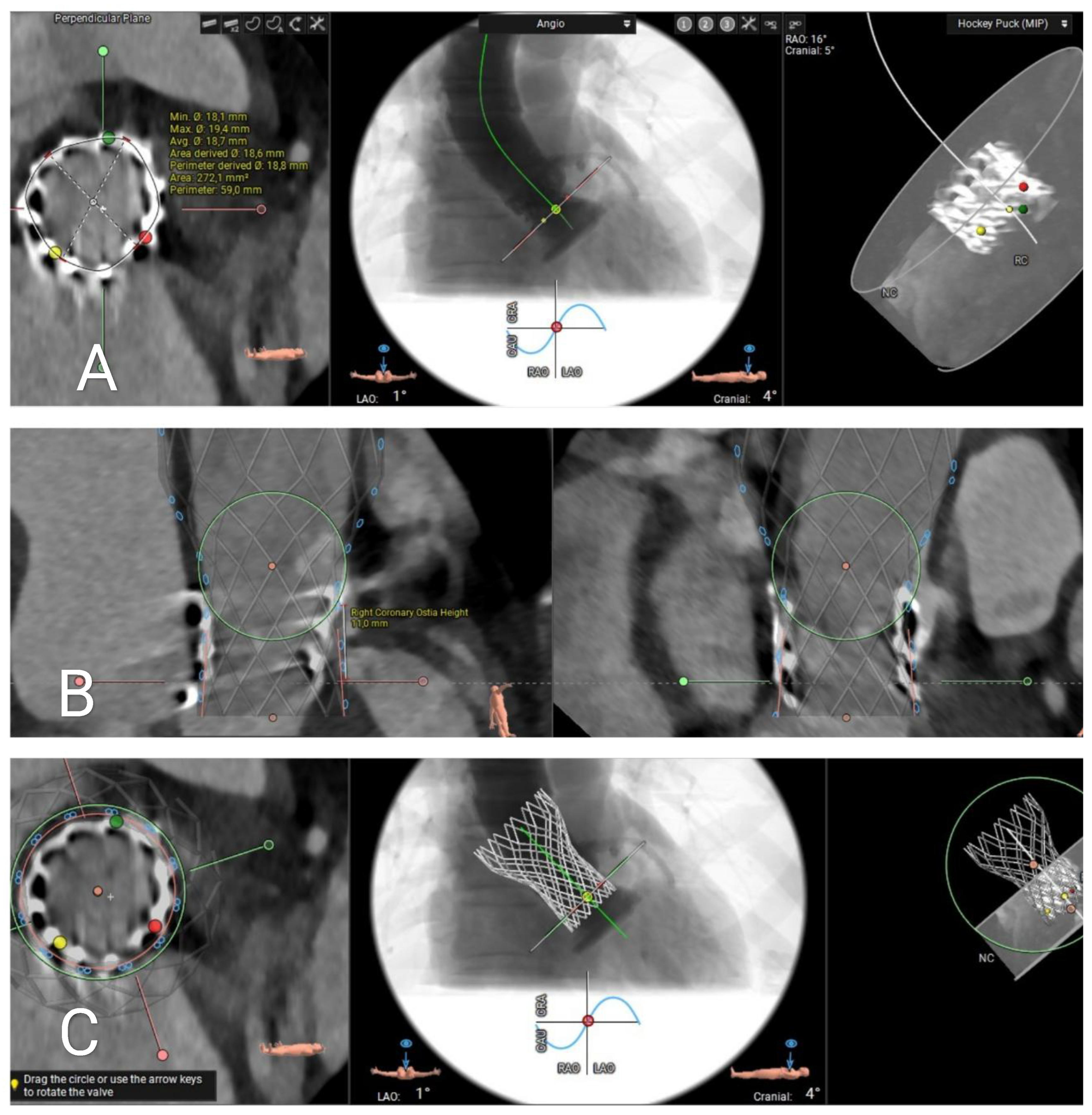
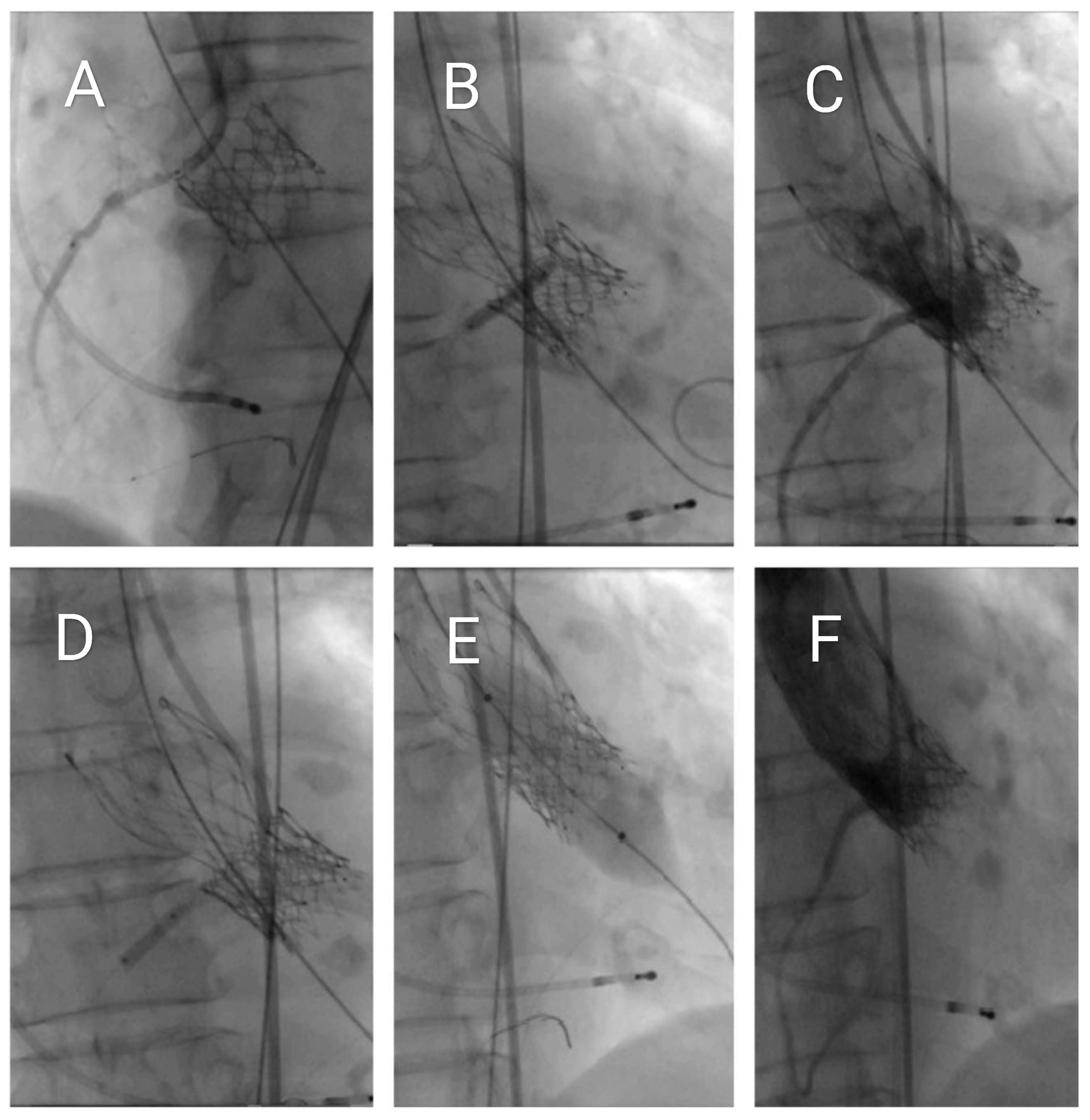
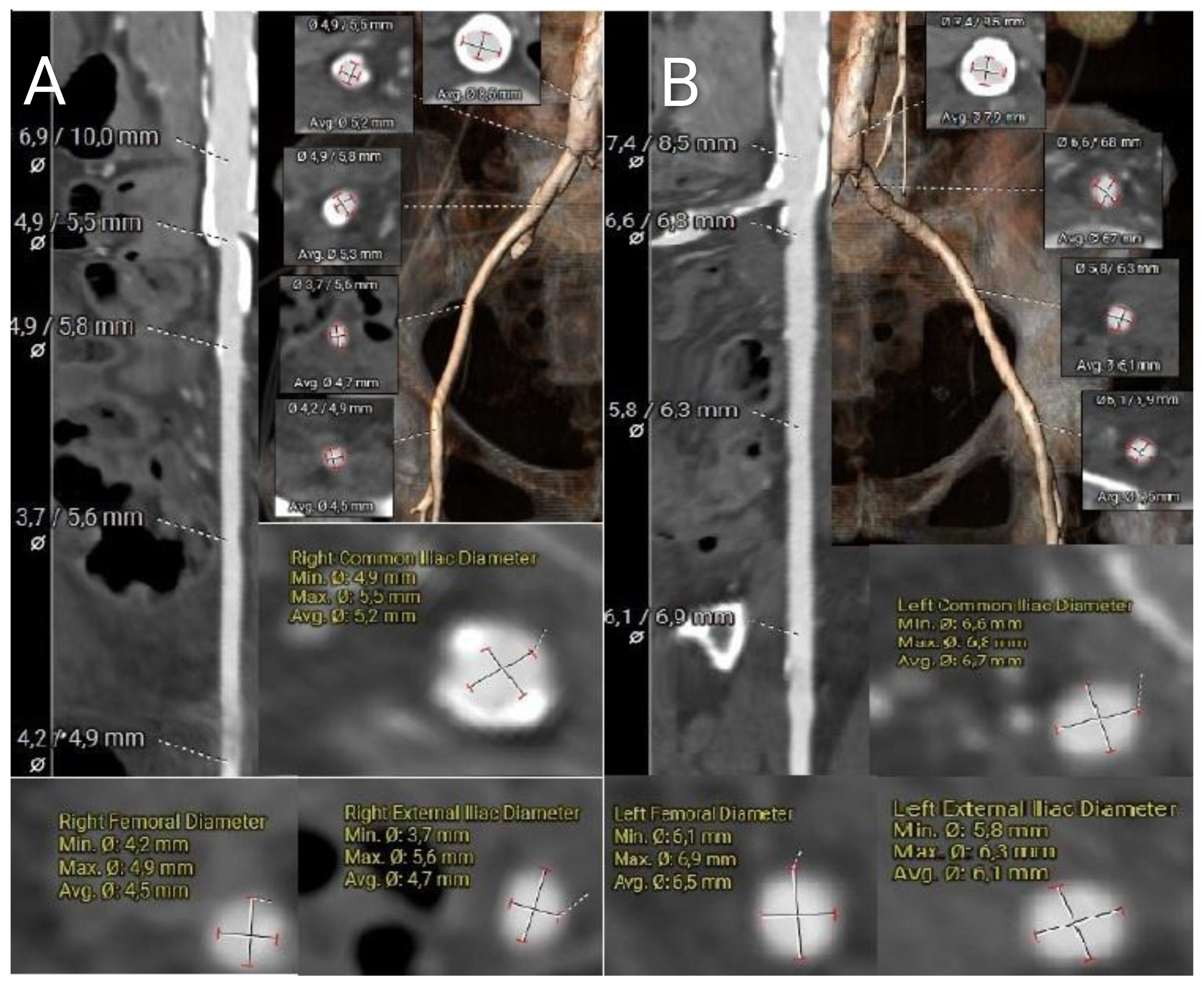
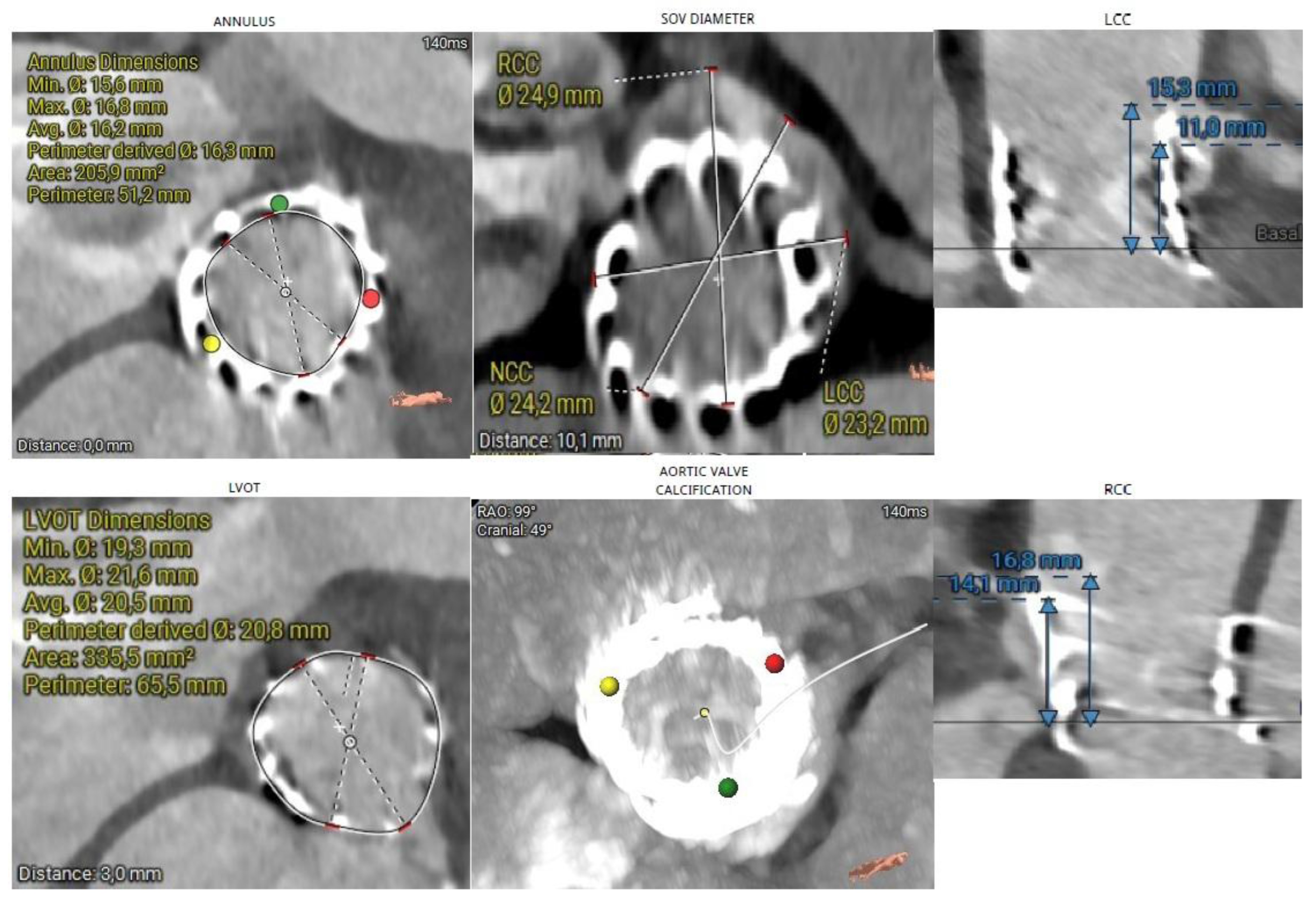
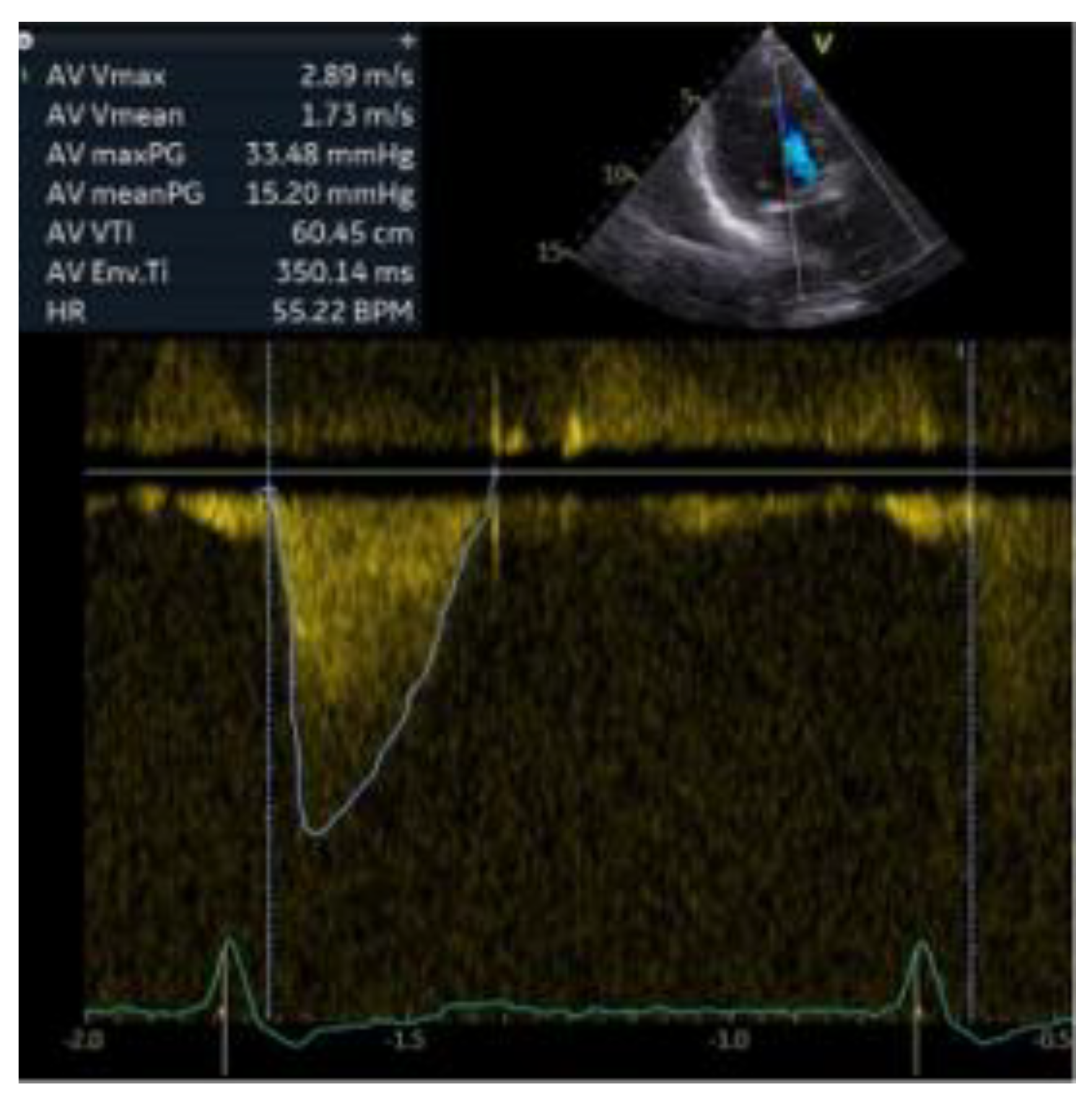
Background: Redo transcatheter aortic valve implantation (TAVI) in patients with prior transapical SAPIEN 3 valves carries a significant risk of coronary obstruction. Chimney stenting is an established strategy to maintain coronary perfusion in high-risk valve-in-valve (ViV) procedures. Case Description: An 87-year-old woman presented with NYHA class IV symptoms due to severe restenosis of a 20-mm SAPIEN 3 valve implanted in 2017. Computed tomography revealed stent extension beyond the sinotubular junction, posing a risk of right coronary artery (RCA) occlusion. A transfemoral redo-TAVI using a 23-mm Medtronic Evolut FX+ valve was performed with pre-positioned chimney stenting. During valve deployment, inferior ST-segment elevation occurred, necessitating immediate RCA stenting. A second distal RCA stent addressed residual stenosis. Final angiography confirmed preserved coronary flow and optimal valve function; Discussion: Careful preprocedural evaluation—including CT-based assessment of coronary height, sinus anatomy, and virtual valve modeling—is essential in high-risk ViV or redo-TAVI cases. The chimney technique provides an effective bailout for acute coronary obstruction, while procedural strategies such as commissural alignment and the cusp-overlap technique can optimize procedural and hemodynamic outcomes.; Conclusions: Planned coronary protection using chimney stenting enables safe and effective redo transfemoral TAVI in patients with complex anatomy and prior transapical valve implantation, ensuring hemodynamic success and minimizing complications.
Keywords:
1. Introduction
2. Case Description
3. Discussion
4. Patient Perspective
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of open access journals |
| TLA | Three letter acronym |
| LD | Linear dichroism |
References
- Ibrahim, H., Chaus, A., Alkhalil, A., Prescher, L., Kleiman, N. (2024). Coronary artery obstruction after transcatheter aortic valve implantation: past, present, and future. Circulation: Cardiovascular Interventions, 17(6), e012827. [CrossRef]
- Praz, F., Borger, M. A., et al. (2025). 2025 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. European Heart Journal, 46(44), 4635–4736. [CrossRef]
- Mercanti, F., Rosseel, L., Neylon, A., Bagur, R., Sinning, J.M., Nickenig, G., et al. (2020). Chimney stenting for coronary occlusion during TAVR: insights from the Chimney Registry. JACC: Cardiovascular Interventions, 13(6), 751–761. [CrossRef]
- Barbanti, M., Tamburino, C., et al. (2023). Feasibility of Redo-Transcatheter Aortic Valve Replacement in Sapien Valves Based on In Vivo Computed Tomography Assessment. Journal of the American College of Cardiology: Cardiovascular Interventions, 16(5), 501–512. https://pubmed.ncbi.nlm.nih.gov/37988440/.
- Beneduce, A., Khokhar, A.A., Curio, J., et al. (2025). Chimney stenting for preventing coronary obstruction in redo-TAVI with BEV within SEV (bench-model). EuroIntervention, 21(12), e692–e703. https://research.regionh.dk/en/publications/chimney-stenting-for-preventing-coronary-obstruction-in-redo-tavi.
- Basman, C., Mustafa, A., Pirelli, L., Thampi, S., Kodra, A., Scheinerman, S.J., Kliger, C. (2023). Kissing balloon inflation for transcatheter aortic valve replacement and abutting ostial coronary artery stent. Journal of Cardiology Cases, 28(4), 141–143. [CrossRef]
- Otto, C.M., Nishimura, R.A., Bonow, R.O., et al. (2021). 2020 ACC/AHA guideline for the management of patients with valvular heart disease. Journal of the American College of Cardiology, 77(4), e25–e197. [CrossRef]
- Bapat, V.N., Fukui, M., Zaid, S., et al. (2024). A guide to transcatheter aortic valve design and systematic planning for a Redo-TAV (TAV-in-TAV) procedure. JACC: Cardiovascular Interventions, 17, 1631–1651. [CrossRef]
- Ratanapo, S. (2024). CT planning with Redo TAV app guiding strategy to prevent coronary obstruction for TAV-in-TAV procedure. Presented at: NY Valves 2024; 6 June 2024; New York, NY. Available from: https://www.tctmd.com/slide/ct-planning-redo-tav-app-guiding-strategy-prevent-coronary-obstruction-tav-tav-procedure.
- Baumgartner, H., Falk, V., Bax, J.J., et al. (2022). 2021 ESC/EACTS guidelines for the management of valvular heart disease. European Heart Journal, 43(7), 561–632. [CrossRef]
- Blanke, P., Weir-McCall, J., Achenbach, S., et al. (2019). Computed tomography imaging in the context of transcatheter aortic valve implantation (TAVI)/transcatheter aortic valve replacement (TAVR): An expert consensus document. JACC: Cardiovascular Imaging, 12(1), 1–24. [CrossRef]
- Di Mario, C., Goodwin, M., Ristalli, F., et al. (2021). A prospective registry of intravascular lithotripsy-enabled vascular access for transfemoral transcatheter aortic valve implantation. EuroIntervention, 16(14), e1125–e1132. [CrossRef]
- Barbash, I.M., Barbanti, M., Webb, J.G., et al. (2019). Transcatheter aortic valve implantation in calcified iliofemoral arteries: feasibility and outcome of endovascular lithotripsy. EuroIntervention, 15(7), e1006–e1011. [CrossRef]
- Medtronic. (2025). Medtronic Evolut TAVR systems receive FDA approval for expanded Redo-TAVR indication [online]. 28 Aug 2025 [cited 15 Oct 2025]. Available from: https://news.medtronic.com/2025-08-28-Medtronic-Evolut-TAVR-systems-receive-FDA-approval-for-expanded-Redo-TAVR-indication.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



