Submitted:
31 January 2026
Posted:
04 February 2026
You are already at the latest version
Abstract
Background: Vestibular symptoms and objective vestibular dysfunction have been reported in patients with autoimmune, autoinflammatory, and rheumatologic diseases, but available evidence remains fragmented and methodologically heterogeneous. Previous studies have often addressed audiovestibular involvement as a combined entity, limiting disease-specific interpretation of vestibular outcomes. Methods: A PRISMA 2020–based systematic review was conducted using predefined eligibility criteria targeting vestibular outcomes in autoimmune, autoinflammatory, and systemic rheumatologic diseases. Observational studies reporting vestibular symptoms and/or objective vestibular test results were included. Vestibular data were extracted even when studies reported combined audiovestibular outcomes. Certainty of evidence was assessed using the GRADE approach. Results: Twenty-nine studies were included in the qualitative synthesis, comprising 18 primary observational studies and 11 reviews. Vestibular involvement was reported across multiple diseases, including systemic sclerosis, giant cell arteritis, ankylosing spondylitis, psoriatic arthritis, Behçet disease, primary Sjögren syndrome, rheumatoid arthritis, systemic lupus erythematosus, antiphospholipid syndrome, and vasculitic disorders. Objective vestibular abnormalities were most frequently identified using caloric testing, balance integration measures, videonystagmography, and video head impulse testing. Systemic sclerosis and giant cell arteritis showed more consistently reported vestibular findings, although heterogeneity in assessment methods precluded quantitative synthesis. Conclusions: Vestibular involvement occurs across autoimmune and systemic inflammatory diseases, but overall certainty of evidence remains limited. Standardized vestibular assessment and longitudinal studies are needed to better define disease-specific vestibular phenotypes.
Keywords:
vestibular dysfunction
; autoimmune diseases
; rheumatologic diseases
; systemic sclerosis
; giant cell arteritis
; benign paroxysmal positional vertigo
; balance disorders
; vestibular assessment
; systematic review
; GRADE
1. Introduction
Vestibular symptoms and objective vestibular dysfunction have been increasingly reported in patients with systemic autoimmune and rheumatologic diseases. Clinical manifestations such as vertigo, dizziness, imbalance, and benign paroxysmal positional vertigo have been described across a wide range of conditions, suggesting that immune-mediated mechanisms may affect vestibular structures either directly or indirectly. However, the available evidence remains fragmented and methodologically heterogeneous, largely due to differences in study design, patient selection, disease activity, and vestibular assessment strategies [1].
Most previous investigations have addressed audiovestibular involvement as a combined entity, frequently prioritizing hearing-related outcomes and relegating vestibular findings to secondary or descriptive observations. As a result, vestibular outcomes are often underrecognized, inconsistently reported, or assessed using non-standardized methods, limiting disease-specific interpretation and cross-study comparability. This lack of focused vestibular evaluation hampers the ability to define consistent vestibular phenotypes and to accurately assess the strength of evidence supporting vestibular involvement in systemic immune-mediated diseases [1,2].
Autoimmune involvement of the inner ear has long been recognized as a clinical entity, classically described as autoimmune inner ear disease. Early clinical reviews reported that vestibular symptoms—including imbalance, ataxia, and episodic or positional vertigo—may be present in up to half of affected patients and frequently coexist with systemic autoimmune diseases [3]. These observations provided an initial clinical framework supporting immune-mediated mechanisms affecting both cochlear and vestibular structures, although objective vestibular testing was not systematically applied at that time [3].
A further limitation is that most available syntheses have addressed inner ear involvement using a combined audiovestibular approach, analyzing hearing and balance disorders together, often pooling heterogeneous diseases and outcomes. This has been useful to map the overall otologic spectrum but has also diluted vestibular-specific information, particularly when objective vestibular testing was variably applied or inconsistently reported [1,2,5,6]. Consequently, comparisons across diseases remain difficult and are rarely supported by standardized vestibular endpoints.
Within this heterogeneous field, vestibular involvement has been reported in multiple autoimmune and systemic inflammatory conditions, including systemic sclerosis, giant cell arteritis, ankylosing spondylitis, psoriatic arthritis, Behçet disease, primary Sjögren syndrome, rheumatoid arthritis, systemic lupus erythematosus, antiphospholipid syndrome, Anti-Neutrophil Cytoplasmic Antibodies (ANCA)-associated vasculitis, sarcoidosis, and Cogan syndrome [7,8,9,10,11,12,13,14,15,16,17,18,19,22,24,25,26,27,28,29,30]. However, the strength and consistency of available evidence vary widely between diseases, and the majority of primary studies are observational.
Among systemic autoimmune diseases, systemic sclerosis has emerged as the condition with the most consistent evidence of vestibular involvement. Observational studies have demonstrated objective vestibular abnormalities in systemic sclerosis, including altered caloric responses, impaired sensory integration on balance testing, and an increased prevalence of benign paroxysmal positional vertigo [7,8]. A recent systematic review and meta-analysis confirmed that vertigo is significantly more prevalent in patients with systemic sclerosis compared with control populations, although objective vestibular outcomes could not be quantitatively pooled due to methodological heterogeneity [9].
Vestibular involvement has also been reported in other systemic inflammatory and rheumatologic diseases. In giant cell arteritis, independent studies have described a strong association with benign paroxysmal positional vertigo, supporting a vascular or ischemic mechanism affecting vestibular end organs [10,22], with partial symptom improvement after corticosteroid therapy reported in some cases [24]. In ankylosing spondylitis and psoriatic arthritis, case–control studies have demonstrated impaired vestibular sensory integration and an increased prevalence of positional vertigo compared with healthy controls [11,12].
More recently, objective vestibular abnormalities have been identified in diseases traditionally considered less frequently associated with vestibular dysfunction. In Behçet’s disease, video head impulse testing and head-shake maneuvers have revealed horizontal canal dysfunction and increased rates of head-shake–induced nystagmus [13]. In primary Sjögren syndrome, subclinical vestibular involvement has been demonstrated using vestibular evoked myogenic potentials and video head impulse testing [14]. Similarly, in rheumatoid arthritis, large case–control studies using videonystagmography and caloric testing have reported both central-type oculomotor abnormalities and peripheral vestibular hypofunction [15].
Vestibular manifestations have additionally been described in systemic lupus erythematosus, antiphospholipid syndrome, ANCA-associated vasculitis, sarcoidosis, and Cogan syndrome, although the evidence in these conditions remains heterogeneous and largely observational [16,17,18,19]. In thrombotic autoimmune conditions such as antiphospholipid syndrome, recurrent vertigo has been linked to thrombotic and microvascular mechanisms involving the inner ear circulation, a finding supported by recent systematic reviews [17,30]. Finally, autoimmune comorbidity has also been described in Ménière’s disease cohorts, raising questions about immune contributions to recurrent vertigo syndromes in selected patients. An association between Ménière’s disease and systemic autoimmune disorders has been supported by large observational studies. In a multicenter cohort including nearly 700 patients with Ménière’s disease, Gázquez et al. reported a significantly increased prevalence of systemic autoimmune diseases, particularly rheumatoid arthritis, systemic lupus erythematosus, and ankylosing spondylitis, compared with the general population. Importantly, autoimmune diseases were more frequently observed in patients with Ménière’s disease and migraine, suggesting the existence of a distinct immune-mediated clinical phenotype. These findings support an autoimmune background in a subset of patients with Ménière’s disease and provide a broader context for immune-mediated vestibular disorders [23].
The aim of the present systematic review was to synthesize and critically appraise the available evidence on vestibular involvement in the most prominent and highest scientific quality of studies in systemic autoimmune, autoinflammatory, and rheumatologic diseases, focusing specifically on vestibular outcomes rather than combined audiovestibular manifestations. Secondary objectives were to compare vestibular findings across diseases and to assess certainty of evidence using the GRADE framework.
2. Materials and Methods
This systematic review was conducted and reported in accordance with the PRISMA 2020 statement [20].
2.1. Search Strategy
A comprehensive literature search was performed in PubMed/MEDLINE, Embase, Web of Science, and the Cochrane Library from database inception to the final search date (December 2025). The search strategy combined controlled vocabulary and free-text terms related to vestibular involvement and autoimmune diseases, including: vestibular, vertigo, dizziness, balance, autoimmune, rheumatologic, systemic sclerosis, vasculitis, giant cell arteritis, ankylosing spondylitis, psoriatic arthritis, Behçet, Sjögren, rheumatoid arthritis, and systemic lupus erythematosus. Reference lists of relevant reviews and included articles were manually screened to identify additional eligible studies [1,2,6].
2.2. Eligibility Criteria
Studies were included if they met the following criteria:
(1) observational design (cohort, case–control, or cross-sectional);
(2) evaluation of patients with autoimmune, autoinflammatory, or systemic rheumatologic diseases;
(3) reporting vestibular symptoms and/or objective vestibular test results;
(4) availability of extractable vestibular data.
Studies were excluded if they:
(1) focused exclusively on auditory outcomes;
(2) were case reports, conference abstracts, editorials, or animal studies;
(3) lacked sufficient methodological detail;
(4) reported overlapping patient cohorts without novel vestibular data.
2.3. Study Selection
After duplicate removal, titles and abstracts were independently screened for eligibility. Full-text articles were retrieved and assessed when abstracts suggested potential relevance. Discrepancies were resolved by consensus. The study selection process is summarized in the PRISMA flow diagram (Figure 1) [20].
2.4. Data Extraction
For each included primary study, the following data were extracted: first author, year of publication, disease category, study design, sample size, vestibular assessment methods, vestibular outcomes, and main findings. Reviews were analyzed separately to contextualize the primary evidence. Data extraction was performed using a standardized form and cross-checked for accuracy.
2.5. Risk of Bias Assessment
2.6. Certainty of Evidence
The certainty of evidence for vestibular involvement across diseases was evaluated using the GRADE framework [21]. Evidence derived from observational studies was initially rated as low certainty and subsequently downgraded or upgraded based on risk of bias, inconsistency, indirectness, imprecision, and other considerations.
Given the absence of randomized or longitudinal vestibular studies in this field, highest scientific quality was interpreted as well-designed observational studies and systematic reviews.
3. Results
3.1. Study Selection
The systematic literature search identified a total of 29 eligible studies for qualitative synthesis after removal of duplicates and application of predefined inclusion and exclusion criteria (Figure 1). These comprised 18 primary observational studies addressing vestibular involvement in specific diseases and 11 reviews providing clinical, epidemiological, or mechanistic context. No randomized controlled trials were identified. All included studies were published in peer-reviewed journals.
3.2. Characteristics of Included Studies
The characteristics of the 18 primary observational studies are summarized in Table 1. Most studies employed a case–control or cross-sectional design and included adult patients with established diagnoses of systemic autoimmune or rheumatologic diseases. Sample sizes varied widely across studies, ranging from small cohorts to larger disease-specific populations.
The 11 review articles included narrative reviews, systematic reviews, and one systematic review with meta-analysis. These reviews addressed vestibular involvement either directly or as part of broader audiovestibular or immune-mediated inner ear frameworks and are summarized in Table 2.
3.3. Vestibular Involvement Across Autoimmune and Rheumatologic Diseases
Vestibular symptoms and/or objective vestibular abnormalities were reported across a wide spectrum of diseases, including systemic sclerosis, giant cell arteritis, ankylosing spondylitis, psoriatic arthritis, Behçet disease, primary Sjögren syndrome, rheumatoid arthritis, systemic lupus erythematosus, antiphospholipid syndrome, ANCA-associated vasculitis, sarcoidosis, and Cogan syndrome.
Across studies, vestibular involvement was evaluated using a combination of clinical symptom assessment (vertigo, dizziness, imbalance, and benign paroxysmal positional vertigo) and objective vestibular testing, most commonly caloric testing, videonystagmography (VNG), clinical tests of sensory integration and balance, and video head impulse testing (vHIT). The choice of vestibular assessment methods varied substantially between studies, limiting direct comparisons.
In systemic sclerosis, multiple independent studies reported a higher prevalence of vertigo, balance impairment, and benign paroxysmal positional vertigo compared with control populations. Objective abnormalities were frequently identified using caloric testing and balance integration measures. These findings were consistently reported across different cohorts.
In giant cell arteritis, vestibular involvement was predominantly characterized by an increased prevalence of benign paroxysmal positional vertigo confirmed by positional testing. Although objective vestibular testing beyond positional maneuvers was limited, findings were reproducible across independent observational studies.
In ankylosing spondylitis and psoriatic arthritis, vestibular involvement was mainly reflected by impaired balance performance and increased rates of positional vertigo. Studies frequently relied on clinical balance tests and posturography, with fewer studies incorporating semicircular canal–specific vestibular assessments.
In Behçet disease, objective vestibular abnormalities were identified using vHIT and oculomotor or positional maneuvers, suggesting peripheral semicircular canal involvement in selected cohorts. In primary Sjögren syndrome, vestibular abnormalities were often subclinical and detected through physiological vestibular testing rather than overt vestibular symptoms.
In rheumatoid arthritis, vestibular findings were heterogeneous, with studies reporting both peripheral vestibular hypofunction and central-type oculomotor abnormalities. Similar heterogeneity was observed in systemic lupus erythematosus, where vestibular involvement was primarily symptom-based and objective testing was inconsistently applied.
Vestibular involvement in antiphospholipid syndrome, ANCA-associated vasculitis, sarcoidosis, and Cogan syndrome was reported in a limited number of studies, typically small observational cohorts or case series, precluding robust disease-specific comparisons.
3.4. Certainty of Evidence (GRADE Assessment)
Certainty of evidence for vestibular involvement was assessed using the GRADE framework, considering the overall body of evidence available for each disease (Table 3). For systemic sclerosis and giant cell arteritis, certainty of evidence was rated as moderate at best, within the limitations inherent to observational study designs and heterogeneous vestibular assessment methods.
For ankylosing spondylitis, psoriatic arthritis, Behçet disease, primary Sjögren syndrome, rheumatoid arthritis, systemic lupus erythematosus, and antiphospholipid syndrome, certainty of evidence was rated as low, primarily due to small sample sizes, methodological heterogeneity, and limited use of standardized vestibular testing. For ANCA-associated vasculitis, sarcoidosis, and Cogan syndrome, certainty of evidence was rated as very low, reflecting sparse and predominantly descriptive data.
4. Discussion
This systematic review shows that vestibular involvement has been reported across a broad range of systemic autoimmune and rheumatologic diseases, although the evidence remains heterogeneous and largely observational. By focusing on vestibular outcomes, this work addresses an important limitation of prior audiovestibular syntheses, where vestibular findings were frequently embedded within combined outcomes and assessed using non-uniform diagnostic strategies [1,2,5,6].
Across the included conditions, systemic sclerosis (SSc) and giant cell arteritis (GCA) were the diseases in which vestibular findings were most consistently reported across multiple independent primary studies, rather than supported by high-level causal evidence. In SSc, case–control studies reported higher rates of vertigo and balance impairment, as well as an increased prevalence of benign paroxysmal positional vertigo (BPPV), compared with controls [7,8]. A recent systematic review and meta-analysis supports a higher frequency of vertigo in SSc. However, objective vestibular outcomes could not be quantitatively pooled because of heterogeneous testing protocols and outcome definitions [9]. Collectively, these data suggest a reproducible association between SSc and vestibular symptoms, while emphasizing the need for standardized vestibular endpoints to enable robust comparisons and pooling.
In GCA, observational studies reported a higher prevalence of BPPV confirmed by positional testing [10,22]. Although these findings do not establish causality, they align with narrative syntheses of systemic vasculitis proposing that ischemic involvement of labyrinthine circulation may contribute to vestibular syndromes in this setting [24]. Importantly, the certainty of evidence should be interpreted within the limitations of observational designs, and mechanistic explanations should be framed as plausible rather than definitive [24].
Evidence from spondyloarthritis-related diseases suggests a tendency toward vestibular/balance involvement. In ankylosing spondylitis and psoriatic arthritis, studies using sensory integration and balance measures, and in some cases posturography, reported higher rates of balance impairment and positional vertigo compared with controls [11,12,25,26]. While these findings are clinically relevant, differences in vestibular assessment strategies and the frequent reliance on non-specific balance endpoints limit disease-specific phenotyping and cross-study comparability. More recent studies have expanded objective vestibular assessment to additional autoimmune diseases. In Behçet disease, abnormalities detected using video head impulse testing and oculomotor/positional maneuvers suggest peripheral semicircular canal involvement in selected cohorts [13,27]. In primary Sjögren syndrome, vestibular abnormalities were often subclinical and identified through physiological testing [14]. In rheumatoid arthritis, vestibular findings were heterogeneous across studies, with both peripheral hypofunction and central-type oculomotor abnormalities reported, likely reflecting differences in patient selection and testing protocols [15,28]. Vestibular involvement has also been described in systemic lupus erythematosus, antiphospholipid syndrome, ANCA-associated vasculitis, sarcoidosis, and Cogan syndrome, but the evidence base remains sparse and methodologically diverse [16,17,18,19,21,29,30].
Ménière’s disease was not considered a systemic autoimmune disorder in this review. However, it was included as a related clinical model of recurrent vertigo with documented autoimmune comorbidity. Large observational data indicate an increased prevalence of systemic autoimmune diseases among patients with Ménière’s disease, supporting an autoimmune background in a subset and highlighting potential immune contributions to vertigo persistence [23]. These findings provide contextual support for immune-mediated vestibular symptom chronicity, while remaining distinct from disease-specific vestibular testing evidence.
The clinical concept of immune-mediated inner ear involvement predates modern vestibular testing and was historically framed as autoimmune inner ear disease (AIED). Classical reviews described frequent vestibular symptoms and a relevant coexistence with systemic autoimmune disorders [3]. More recently, mechanistic reviews have emphasized the role of resident macrophages and innate immune signaling within the inner ear, providing biological plausibility for immune-mediated effects on vestibular end organs, even though these data are not confirmatory of clinical vestibular dysfunction [31]. In parallel, biomarker-focused scoping work highlights the ongoing lack of sensitive and specific diagnostic immune biomarkers for routine clinical use, which may partly explain the heterogeneity of clinical phenotypes and outcomes reported across studies [32]. Recent narrative syntheses on AIED pathogenesis and treatment similarly underscore that therapeutic responses to corticosteroids or immunosuppressive agents are variable and largely supported by observational evidence, reinforcing the need for standardized vestibular phenotyping and longitudinal designs [33].
Overall, applying the GRADE framework indicates that the certainty of evidence is moderate at best for a limited subset of conditions and low to very low for most diseases, primarily due to observational study designs, limited sample sizes, and inconsistency in vestibular assessment methodologies [20]. Future studies should prioritize standardized vestibular testing protocols (including clearly defined symptom definitions and objective endpoints), longitudinal follow-up, and transparent reporting of disease activity and treatments to clarify disease-specific vestibular phenotypes and their clinical implications.
5. Conclusions
Vestibular involvement has been reported across a wide spectrum of systemic autoimmune and rheumatologic diseases. However, the overall certainty of evidence remains limited and is predominantly based on observational data. Among the conditions reviewed, systemic sclerosis and giant cell arteritis show the most consistently reported vestibular findings across independent studies, although the certainty of evidence should be interpreted as moderate at best and within the limitations inherent to observational designs. For most other diseases, evidence remains low or very low due to heterogeneous methodologies, small sample sizes, and inconsistent vestibular assessment strategies. Future research should prioritize standardized vestibular testing protocols, longitudinal designs, and transparent reporting of disease activity and treatment exposure to better define disease-specific vestibular phenotypes and their clinical implications.
Author Contributions
Amor-Dorado and González-Gay shared senior authorship.
Funding
This research received no external funding.
Acknowledgments
Prof. González-Gay research is supported by the Spanish Ministry of Health, Instituto de Salud Carlos III (ISCIII), PI24/00554, and co-funded by the European Union; and the Spanish Red de Investigación RICORS - RD24/0007/0031 fondos de Next Generation EU, financing acting on "Mecanismo de Recuperación y Resiliencia (MRR)".
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ralli, M.; Greco, A.; Turchetta, R.; Altissimi, G.; de Vincentiis, M. Audiovestibular symptoms in systemic autoimmune diseases. J. Immunol. Res. 2018, 2018, 5798103. [Google Scholar] [CrossRef] [PubMed]
- Girasoli, L.; Cazzador, D.; Padoan, R.; Delogu, M.; Zanoletti, E.; Martini, A. Update on vertigo in autoimmune disorders: From diagnosis to treatment. J. Immunol. Res. 2018, 2018, 5072582. [Google Scholar] [CrossRef]
- Bovo, R.; Aimoni, C.; Martini, A. Immune-mediated inner ear disease. Acta Otolaryngol. 2006, 126, 1012–1021. [Google Scholar] [CrossRef] [PubMed]
- Athanasopoulos, D.; Papathanasiou, M.; Tsivgoulis, G. Inner ear involvement in autoimmune and autoinflammatory diseases. Autoimmun. Rev. 2024, 23, 103368. [Google Scholar] [CrossRef]
- Breslin, N.K.; Varadarajan, V.V.; Suresh, K.; et al. Autoimmune inner ear disease: A systematic review of management. Otolaryngol. Head Neck Surg. 2020, 162, 463–472. [Google Scholar] [CrossRef]
- Amor-Dorado, J.C.; Arias-Núñez, M.C.; Miranda-Filloy, J.A.; González-Juanatey, C.; Llorca, J.; González-Gay, M.A. Audiovestibular manifestations in patients with limited systemic sclerosis and centromere protein-B antibodies. Medicine (Baltimore) 2008, 87, 131–141. [Google Scholar] [CrossRef]
- Amor-Dorado, J.C.; Barreira-Fernández, M.P.; Arias-Núñez, M.C.; Gómez-Acebo, I.; Llorca, J.; González-Gay, M.A. Benign paroxysmal positional vertigo and clinical test of sensory interaction and balance in systemic sclerosis. Otol. Neurotol. 2008, 29, 1155–1161. [Google Scholar] [CrossRef]
- Salvador, C.; Martínez, C.; Riera, A.; et al. Audiovestibular involvement in systemic sclerosis: A systematic review and meta-analysis. In Eur. Arch. Otorhinolaryngol.; 2025. [Google Scholar] [CrossRef]
- Amor-Dorado, J.C.; Llorca, J.; Costa-Ribas, C.; García-Porrúa, C.; González-Gay, M.A. Giant cell arteritis: A new association with benign paroxysmal positional vertigo. Laryngoscope 2004, 114, 1420–1425. [Google Scholar] [CrossRef]
- Amor-Dorado, J.C.; Barreira-Fernández, M.P.; Vázquez-Rodríguez, T.R.; et al. Audiovestibular manifestations in patients with ankylosing spondylitis. Medicine (Baltimore) 2011, 90, 99–109. [Google Scholar] [CrossRef]
- Amor-Dorado, J.C.; Barreira-Fernández, M.P.; Piña, T.; et al. Investigations into audiovestibular manifestations in patients with psoriatic arthritis. J. Rheumatol. 2014, 41, 2018–2026. [Google Scholar] [CrossRef]
- Ertugrul, O.; Mutlu, A.; Zindanci, I.; et al. Audiological and vestibular measurements in Behçet’s disease. Eur. Arch. Otorhinolaryngol. 2019, 276, 1625–1632. [Google Scholar] [CrossRef]
- Ulusoy, B.; Limon, M.; Yılmaz, S.; et al. Effects of primary Sjögren’s syndrome on hearing and vestibular systems. J. Laryngol. Otol. 2022, 136, 923–930. [Google Scholar] [CrossRef]
- Özkırış, M.; Kapusuz, Z.; Günaydın, İ.; et al. Does rheumatoid arthritis have an effect on audiovestibular tests? Eur. Arch. Otorhinolaryngol. 2014, 271, 1383–1387. [Google Scholar] [CrossRef] [PubMed]
- Karataş, M.; Onat, A.M.; Durmuş, O.; et al. Vestibular dysfunction in patients with systemic lupus erythematosus. J. Neurol. Sci. 2007, 254, 6–10. [Google Scholar] [CrossRef]
- Huppert, D.; Strupp, M.; Möller, A.; Brandt, T. Recurrent vertigo in patients with antiphospholipid syndrome. J. Neurol. 2013, 260, 1829–1833. [Google Scholar] [CrossRef]
- Kim, J.; Jung, J.Y.; Park, H.J.; et al. Vestibular dysfunction in patients with ANCA-associated vasculitis. Clin. Exp. Rheumatol. 2012, 30, S41–S45. [Google Scholar]
- Greco, A.; Fusconi, M.; Gallo, A.; et al. Audiovestibular involvement in Cogan’s syndrome. Autoimmun. Rev. 2016, 15, 347–353. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; et al. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Amor-Dorado, J.C.; Llorca, J.; García-Porrúa, C.; et al. Audiovestibular manifestations in giant cell arteritis. Medicine (Baltimore) 2003, 82, 13–26. [Google Scholar] [CrossRef]
- Gázquez, I.; Soto-Varela, A.; Aran, I.; et al. High prevalence of systemic autoimmune diseases in patients with Ménière’s disease. PLoS ONE 2011, 6, e26759. [Google Scholar] [CrossRef]
- Amor-Dorado, J.C.; Barreira-Fernández, M.P.; Regueiro-Villarín, S.; González-Gay, M.A. Audiovestibular manifestations in systemic vasculitis. Acta Otorrinolaringol. Esp. 2009, 60, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Amor-Dorado, J.C.; Barreira-Fernández, M.P.; Vázquez-Rodríguez, T.R.; et al. Benign paroxysmal positional vertigo and clinical test of sensory interaction and balance in ankylosing spondylitis. Otol. Neurotol. 2011, 32, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Amor-Dorado, J.C.; Barreira-Fernández, M.P.; Llorca, J.; González-Gay, M.A. Oculographic and posturographic findings in psoriatic arthritis. Otol. Neurotol. 2017, 38, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Yazici, H.; Tüzün, Y.; Pazarli, H.; et al. Vestibular involvement in Behçet disease. Acta Otolaryngol. 2001, 121, 224–228. [Google Scholar]
- Ziavra, N.; Politi, E.N.; Kastanioudakis, I.; et al. Hearing loss and vestibular dysfunction in rheumatoid arthritis. Clin. Rheumatol. 2010, 29, 279–284. [Google Scholar] [CrossRef]
- Kariya, S.; Cureoglu, S.; Fukushima, H.; et al. Vestibular involvement in sarcoidosis. Acta Otolaryngol. 2014, 134, 296–301. [Google Scholar] [CrossRef]
- Chen, J.J.; Hsu, C.W.; Chen, Y.W.; et al. Audiovestibular dysfunction related to antiphospholipid syndrome. Diagnostics 2024, 14, 2522. [Google Scholar] [CrossRef]
- Li, X.; Zhang, Y.; Wang, Y.; et al. Immune microenvironment and autoimmune inner ear disease. Front. Immunol. 2025, 30. [Google Scholar]
- Miwa, T.; Okano, H. Macrophages in autoimmune inner ear disease. Int. J. Mol. Sci. 2022, 23, 10458. [Google Scholar] [CrossRef]
- Gomaa, N.A.; Jimoh, Z.; Campbell, S.; Zenke, J.K.; Szczepek, A.J. Biomarkers for inner ear disorders: Scoping review on the role of biomarkers in hearing and balance disorders. Diagnostics 2021, 11, 42. [Google Scholar] [CrossRef]
- Wang, M.; Zhang, P.; Li, Q.; Kong, C. Investigating the process of autoimmune inner ear disease: Unveiling the intricacies of pathogenesis and therapeutic strategies. Int. J. Med. Sci. 2025, 22, 179–187. [Google Scholar] [CrossRef]
Figure 1.
PRISMA 2020 flow diagram illustrating study selection for the systematic review of vestibular involvement in autoimmune and systemic rheumatologic diseases.
Figure 1.
PRISMA 2020 flow diagram illustrating study selection for the systematic review of vestibular involvement in autoimmune and systemic rheumatologic diseases.
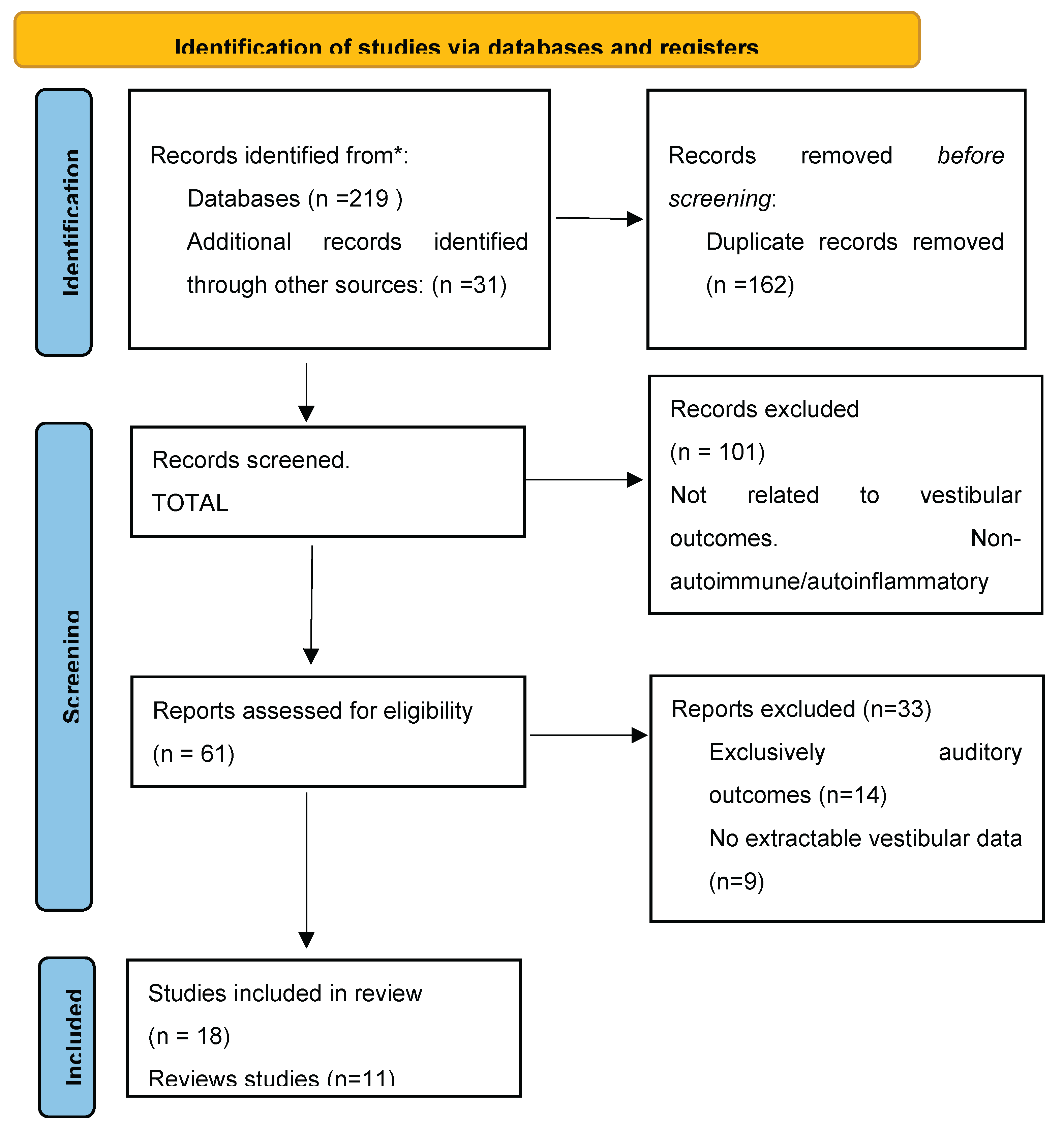

Table 1.
Primary studies reporting vestibular involvement in autoimmune and rheumatologic diseases.
| Author (Year) | Disease | Study Design | Participants (Patients/Controls) | Vestibular Assessment | Vestibular Outcomes | Main Vestibular Findings |
|---|---|---|---|---|---|---|
| Amor-Dorado et al. (2003) | Giant cell arteritis | Prospective cohort | 44 / 44 | Positional tests, caloric test | Vertigo, peripheral vestibulopathy | Vestibular dysfunction significantly more frequent than in controls |
| Amor-Dorado et al. (2004) | Giant cell arteritis | Case–control | 44 / 44 | Dix–Hallpike maneuver | BPPV | Strong association between GCA and BPPV |
| Amor-Dorado et al. (2008a) | Limited systemic sclerosis | Case–control | 35 / 59 | Caloric test, CTSIB, oculography | Chronic imbalance | Objective vestibular abnormalities significantly more frequent |
| Amor-Dorado et al. (2008b) | Systemic sclerosis | Case–control | 42 / 74 | Dix–Hallpike, CTSIB | BPPV, postural instability | Increased prevalence of BPPV and abnormal sensory integration |
| Amor-Dorado et al. (2011a) | Ankylosing spondylitis | Case–control | 59 / 46 | Caloric test, CTSIB | Dizziness, imbalance | Peripheral vestibular hypofunction and impaired balance integration |
| Amor-Dorado et al. (2011b) | Ankylosing spondylitis | Case–control | 59 / 46 | Dix–Hallpike, CTSIB | BPPV | Higher BPPV prevalence than in controls |
| Amor-Dorado et al. (2014) | Psoriatic arthritis | Case–control | 60 / 60 | Caloric test, CTSIB | Dizziness, imbalance | Significant vestibular dysfunction compared with controls |
| Amor-Dorado et al. (2017) | Psoriatic arthritis | Case–control | 60 / 60 | Oculography, CTSIB, CDP | Postural instability | Objective abnormalities in balance control |
| Gázquez et al. (2011) | Ménière’s disease + autoimmune disease | Multicenter cohort | >600 / – | Clinical criteria (AAO–HNS) | Episodic vertigo | Autoimmune comorbidity associated with more persistent vertigo |
| Karataş et al. (2007) | Systemic lupus erythematosus | Observational | 28 / – | Clinical vestibular assessment | Vertigo, dizziness | High frequency of vestibular symptoms |
| Ertugrul et al. (2019) | Behçet disease | Prospective case–control | 31 / 31 | vHIT, head-shake test, DHI | Peripheral vestibular dysfunction | Horizontal canal dysfunction and head-shake–induced nystagmus significantly more frequent |
| Yazici et al. (2001) | Behçet disease | Observational | 29 / – | Clinical assessment | Vertigo | Vestibular symptoms reported as part of systemic involvement |
| Ziavra et al. (2010) | Rheumatoid arthritis | Case–control | 25 / 20 | Caloric test | Dizziness | Peripheral vestibular hypofunction more frequent than in controls |
| Özkırış et al. (2014) | Rheumatoid arthritis | Prospective case–control | 81 / 81 | VNG, caloric test, positional tests | Central and peripheral vestibular dysfunction | VNG abnormalities in 38.3%; canal paresis in 13.6% |
| Ulusoy et al. (2022) | Primary Sjögren syndrome | Case–control | 35 / 35 | vHIT, cVEMP, oVEMP | Subclinical vestibular dysfunction | Reduced vHIT gain and abnormal VEMP latencies |
| Kim et al. (2012) | ANCA-associated vasculitis | Cohort | 32 / – | Caloric test | Imbalance | Vestibular dysfunction associated with disease activity |
| Kariya et al. (2014) | Sarcoidosis | Observational | 18 / – | Clinical ± VNG | Vertigo | Peripheral inflammatory vestibular involvement |
| Greco et al. (2016) | Cogan syndrome | Cohort | 25 / – | VNG | Severe vertigo | Immune-mediated vestibulopathy |
| Huppert et al. (2013) | Antiphospholipid syndrome | Case–control | 22 / 22 | Clinical assessment | Recurrent vertigo | Vestibular symptoms more frequent than in controls |
Risk of bias assessment: Overall, a moderate risk of bias was identified across most primary studies, reflecting their observational design. A high risk of bias was observed in the studies by Karataş et al. [16], Yazici et al. [28], and Kariya et al. [30]. AAO–HNS, American Academy of Otolaryngology–Head and Neck Surgery; BPPV, benign paroxysmal positional vertigo; CDP, computerized dynamic posturography; CTSIB, Clinical Test of Sensory Interaction and Balance; DHI, Dizziness Handicap Inventory; vHIT, video head impulse test; VNG, videonystagmography; VEMP, vestibular evoked myogenic potentials.
Table 2.
Reviews addressing vestibular involvement in autoimmune and systemic rheumatologic diseases.
Table 2.
Reviews addressing vestibular involvement in autoimmune and systemic rheumatologic diseases.
| Author (Year) | Type of Review | Diseases Included | Vestibular Scope | Main Contribution |
|---|---|---|---|---|
| Ralli et al. (2018) | Narrative clinical review | Systemic autoimmune diseases (SLE, RA, Sjögren, Behçet, vasculitis, Cogan syndrome, sarcoidosis) | Clinical vestibular symptoms | Highlights frequency and underrecognition of vestibular symptoms in systemic autoimmune diseases |
| Girasoli et al. (2018) | Narrative clinical review | Autoimmune disorders | Clinical vestibular syndromes | Provides an overview of immune-mediated vertigo and diagnostic considerations |
| Bovo et al. (2006) | Narrative clinical review | Autoimmune inner ear disease (AIED) | Vertigo, imbalance, episodic and positional vertigo | Classical clinical description of AIED, emphasizing frequent vestibular symptoms and coexistence with systemic autoimmune diseases |
| Amor-Dorado et al. (2009) | Narrative clinical review | Systemic vasculitides (GCA, Takayasu arteritis, PAN, ANCA-associated vasculitis, Behçet disease, Cogan syndrome, RA, SSc, SLE, Sjögren syndrome) | Vertigo, nystagmus, BPPV | Early comprehensive synthesis linking vasculitis and vestibular involvement, particularly in giant cell arteritis |
| Breslin et al. (2020) | Systematic review | Autoimmune inner ear disease | Vestibular outcomes (secondary) | Focused mainly on hearing outcomes; vestibular data inconsistently reported |
| Gázquez et al. (2011) | Narrative review / cohort synthesis | Ménière’s disease with autoimmune comorbidity | Recurrent vertigo | Demonstrates increased prevalence of systemic autoimmune diseases in Ménière’s disease |
| Athanasopoulos et al. (2024) | Narrative mechanistic review | Autoimmune and autoinflammatory diseases | Mechanistic (non-clinical) | Discusses immune-inflammatory and vascular mechanisms affecting the inner ear |
| Miwa & Okano (2022) | Narrative mechanistic review | Autoimmune inner ear disease | Experimental / translational (non-clinical) | Demonstrates macrophage-mediated immune mechanisms in the inner ear; supports biological plausibility of vestibular involvement |
| Li et al. (2025) | Narrative mechanistic review | Autoimmune inner ear disorders | Mechanistic (non-clinical) | Reviews immune microenvironment and inflammatory pathways in inner ear disease |
| Salvador et al. (2025) | Systematic review and meta-analysis | Systemic sclerosis | Clinical vestibular outcomes | Reports increased prevalence of vertigo in systemic sclerosis; objective vestibular findings highly heterogeneous |
| Chen et al. (2024) | Systematic review | Antiphospholipid syndrome | Clinical vestibular outcomes | Summarizes evidence linking APS with recurrent vertigo and vestibular dysfunction |
AIED, autoimmune inner ear disease; APS, antiphospholipid syndrome; BPPV, benign paroxysmal positional vertigo; GCA, giant cell arteritis; PAN, polyarteritis nodosa; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; SSc, systemic sclerosis.
Table 3.
Certainty of evidence for vestibular involvement assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. Certainty ratings were assigned by disease, based on the overall body of relevant evidence available for each autoimmune or rheumatologic condition.
Table 3.
Certainty of evidence for vestibular involvement assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. Certainty ratings were assigned by disease, based on the overall body of relevant evidence available for each autoimmune or rheumatologic condition.
| Disease | Vestibular Outcomes | Evidence Base | Main Limitations | Certainty of Evidence (GRADE) |
|---|---|---|---|---|
| Systemic sclerosis | Vertigo, balance impairment, BPPV | Multiple observational case–control studies; systematic review and meta-analysis | Observational designs; heterogeneous vestibular testing; lack of longitudinal data | Moderate at best, within observational limitations |
| Giant cell arteritis | BPPV, vertigo | Observational cohort and case–control studies | Small sample sizes; limited objective vestibular testing | Moderate at best, within observational limitations |
| Ankylosing spondylitis | Balance impairment, BPPV | Observational case–control studies | Non-specific balance endpoints; heterogeneous methods | Low |
| Psoriatic arthritis | Balance impairment | Observational case–control studies | Small cohorts; limited vestibular specificity | Low |
| Behçet disease | Vestibular hypofunction, abnormal vHIT | Observational studies | Limited number of studies; inconsistent outcomes | Low |
| Primary Sjögren syndrome | Subclinical vestibular abnormalities | Single observational study | Small sample size; lack of replication | Low |
| Rheumatoid arthritis | Peripheral and central vestibular abnormalities | Observational studies | Conflicting findings; heterogeneous testing | Low |
| Systemic lupus erythematosus | Vertigo, vestibular dysfunction | Observational studies | Symptom-based outcomes; limited objective data | Low |
| Antiphospholipid syndrome | Recurrent vertigo | Observational studies; systematic review | Sparse primary data; indirect vestibular outcomes | Low |
| ANCA-associated vasculitis | Vestibular dysfunction | Small observational series | Very limited evidence | Very low |
| Sarcoidosis | Vestibular involvement | Case series | Rare condition; non-comparative data | Very low |
| Cogan syndrome | Vestibular dysfunction | Observational studies | Rare disease; mixed audiovestibular outcomes | Very low |
BPPV, benign paroxysmal positional vertigo; GRADE, Grading of Recommendations Assessment, Development and Evaluation; vHIT, video head impulse test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



