
Submitted:
31 January 2026
Posted:
02 February 2026
You are already at the latest version
Abstract
Background: Upadacitinib, a Janus kinase (JAK) inhibitor, is an effective treatment for Ankylosing Spondylitis (AS). Although its efficacy in reducing disease activity is established, real-world data regarding its impact on li-pid profiles and laboratory parameters, particularly in biologic-refractory patients, remain limited. This study aimed to evaluate the short-term effects of Upadacitinib on inflammation, disease activity, and metabolic/lipid parameters in TNF inhibitor-experienced AS patients. Methods: This retrospective cohort study included 61 TNFi-experienced patients (100% TNFi-IR). Demographics, inflammatory markers (CRP, ESR), disease activity (BASDAI), and hematologic, metabolic, and lipid parameters were assessed at baseline, month 1, and month 3. Statistical analyses were performed using repeated measures ANOVA or Wilcoxon signed-rank tests as appro-priate. A p-value < 0.05 was considered statistically significant. Results: The mean age was 42.6 ± 10.8 years, and 55.7% were male. Median disease duration was 8 years [IQR 4–13], and baseline BASDAI was 5.8 ± 1.4. Upadaci-tinib treatment led to significant reductions in CRP (11.4 ± 10.2 → 6.9 ± 5.8 mg/L) and ESR (14.6 ± 11.5 → 10.4 ± 8.7 mm/h) by month 3 (p < 0.01). BASDAI scores improved significantly to 3.6 ± 1.2 (p < 0.001). Regarding labora-tory safety, hemoglobin and albumin levels increased significantly (p < 0.05), whereas other metabolic parameters remained stable. Lipid analysis showed significant increases in total cholesterol, LDL, and HDL by month 3 (p ≤ 0.003); however, the LDL/HDL ratio and triglyceride levels remained unchanged (p > 0.05). Conclusion: In bio-logic-refractory AS patients, Upadacitinib produced rapid and significant reductions in inflammation and dis-ease activity within 3 months. Although quantitative increases in lipid subfractions were observed, the stable LDL/HDL ratio suggests a preserved atherogenic profile, consistent with the “lipid paradox” described in in-flammatory diseases.
Keywords:
Upadacitinib
; ankylosing spondylitis
; JAK inhibitors
; lipid profile
; Spondyloarthritis
1. Introduction
Ankylosing spondylitis (AS) is a chronic, systemic inflammatory rheumatic disease primarily affecting the axial skeleton and sacroiliac joints, characterized by progressive structural damage, chronic pain, and functional impairment [1]. Beyond musculoskeletal involvement, persistent systemic inflammation in AS is intrinsically linked to an increased risk of comorbidities, most notably accelerated atherosclerosis and cardiovascular disease (CVD) [2]. While the introduction of biologic therapies—specifically tumor necrosis factor inhibitors (TNFi) and interleukin-17 inhibitors (IL-17i)—over the past two decades has revolutionized the management of AS, a significant subset of patients fails to achieve sustained remission or experiences intolerance, underscoring a substantial unmet need for alternative therapeutic pathways, particularly for patients with difficult-to-treat, biologic-refractory disease [3].
The Janus kinase (JAK)–signal transducer and activator of transcription (STAT) pathway plays a pivotal role in mediating the signaling of multiple pro-inflammatory cytokines, such as interleukin (IL)-6 and interferon-gamma, which are implicated in the pathogenesis of AS [4]. Upadacitinib, a potent and selective JAK1 inhibitor, has demonstrated significant efficacy in suppressing systemic inflammation and improving clinical outcomes in pivotal Phase 3 trials, including both biologic-naive and TNF-inhibitor refractory populations [5]. Despite its favorable efficacy profile and the convenience of oral administration, JAK inhibitors are known to induce quantitative changes in serum lipid subfractions. Most existing evidence regarding these metabolic shifts originates from highly controlled clinical trial settings. Consequently, there is a distinct need for real-world evidence to evaluate the longitudinal impact of upadacitinib on comprehensive lipid profiles, hematological indices, and metabolic safety in everyday clinical practice, particularly among difficult-to-treat AS patients [6].
Beyond clinical efficacy, the safety profile of JAK inhibitors, particularly their impact on metabolic and lipid homeostasis, has become a focal point of clinical interest [7]. Evidence derived from rheumatoid arthritis (RA) populations has consistently shown quantitative increases in total cholesterol (TC), low-density lipoprotein (LDL-C), and high-density lipoprotein (HDL-C) during JAK inhibitor therapy; however, the long-term cardiovascular implications of these shifts remain a subject of ongoing debate [8]. Data specifically evaluating lipid dynamics in ankylosing spondylitis (AS) remain sparse compared to RA. Furthermore, the short-term interplay between upadacitinib, systemic inflammatory markers, and comprehensive lipid subfractions in a real-world setting has not been adequately characterized. Given that AS patients harbor an inherently elevated risk of cardiovascular comorbidities due to chronic systemic inflammation, elucidating the metabolic signature of upadacitinib is of paramount clinical relevance for evidence-based risk management [9].
Therefore, the aim of this study was to evaluate the short-term effects of upadacitinib on disease activity, inflammatory markers, hematologic parameters, and lipid profiles in biologic-experienced patients with ankylosing spondylitis in a real-world clinical setting.
2. Results
The study included 61 patients with a mean age of 42.6 ± 10.8 years, of whom 55.7% (n = 34) were male and 44.3% (n = 27) were female. The median disease duration was 8 years (IQR 4–13). The majority of patients were diagnosed with ankylosing spondylitis (AS; n = 51, 83.6%), while the remaining patients had psoriatic arthritis (PsA). The entire cohort (100%) consisted of patients with refractory disease who had an inadequate response or intolerance to at least one anti-TNF agent (TNFi-IR). Among the participants, 39.3% (n = 24) had been treated with two or more TNF inhibitors, and 22.9% (n = 14) had previously received an IL-17 inhibitor (Secukinumab). At baseline, patients exhibited high disease activity (mean BASDAI: 5.8 ± 1.4; CRP: 11.4 ± 10.2 mg/L; ESR: 14.6 ± 11.5 mm/h). During upadacitinib treatment, 18% of patients continued concomitant conventional DMARDs, 29.5% continued NSAIDs, and 9.8% received low-dose glucocorticoids. The demographic and baseline clinical characteristics of the participants (n = 61) are presented in Table 1.
Data are presented as mean ± standard deviation or median [interquartile range] for continuous variables and as number (percentage) for categorical variables. BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; TNFi: tumor necrosis factor inhibitor; IL-17i: interleukin-17 inhibitor; DMARD: disease-modifying antirheumatic drug; NSAID: nonsteroidal anti-inflammatory drug.
During the study period, upadacitinib treatment led to a rapid and statistically significant reduction in inflammatory markers and disease activity scores (Table 2). The mean baseline CRP level of 11.4 ± 10.2 mg/L decreased to 7.8 ± 6.5 mg/L at Month 1 and 6.9 ± 5.8 mg/L at Month 3 (p < 0.001). Similarly, ESR decreased from 14.6 ± 11.5 mm/h at baseline to 10.4 ± 8.7 mm/h at Month 3, representing a significant reduction (p = 0.002). BASDAI scores, the primary measure of disease activity, declined from 5.8 ± 1.4 at baseline to 3.6 ± 1.2 at Month 3, indicating clinically meaningful improvement (p < 0.001).
Data are presented as mean ± standard deviation. Changes over time were analyzed using repeated measures ANOVA. p-values < 0.05 were considered statistically significant.
The short-term effects of upadacitinib on disease activity and inflammation are presented in Figure 1.
Evaluation of safety and laboratory parameters (Table 3) revealed significant increases in hemoglobin (Hb) and albumin levels consistent with suppression of systemic inflammation (Hb: p = 0.032; Albumin: p = 0.005), and a significant decrease in platelet counts (p = 0.028). Creatine kinase (CK) levels also showed a statistically significant but clinically modest increase (112.4 ± 54.8 U/L → 144.2 ± 68.5 U/L; p = 0.012). Liver function tests (ALT, AST), glucose, and other hematologic parameters (WBC, lymphocytes) remained stable throughout follow-up, with no safety signals detected (p > 0.05).
Data are presented as mean ± standard deviation. Changes over time were analyzed using repeated measures ANOVA. p-values < 0.05 were considered statistically significant.
During upadacitinib treatment, notable changes were observed in lipid profile parameters (Table 4 and Table 5). Mean total cholesterol increased from 199.4 ± 41.2 mg/dL at baseline to 211.8 ± 38.5 mg/dL at Month 1 and 215.6 ± 35.4 mg/dL at Month 3 (p = 0.001). Similarly, LDL cholesterol showed a significant rise (baseline 118.7 ± 33.6 → Month 1 130.2 ± 31.4 → Month 3 136.5 ± 29.8 mg/dL; p = 0.003). HDL cholesterol levels also increased significantly during treatment (baseline 50.2 ± 12.4 → Month 1 56.4 ± 13.8 → Month 3 58.7 ± 11.5 mg/dL; p = 0.001).
Triglyceride levels showed a modest rise from 145.8 ± 72.1 mg/dL at baseline to 154.2 ± 68.4 mg/dL at Month 1 and 148.6 ± 62.3 mg/dL at Month 3, which was not statistically significant (p = 0.412). Non-HDL cholesterol increased from 149.2 ± 38.5 mg/dL at baseline to 156.9 ± 34.1 mg/dL at Month 3 (p = 0.008), whereas the LDL/HDL ratio remained stable throughout the study (p = 0.845). Figure 2 illustrates the short-term effects of upadacitinib on lipid parameters.
Data are presented as mean ± standard deviation. Changes over time were analyzed using repeated measures ANOVA. p-values < 0.05 were considered statistically significant.
Analysis of Δ values revealed that total cholesterol and LDL cholesterol increased by +16.2 ± 9.1 mg/dL and +17.8 ± 8.4 mg/dL, respectively, from baseline to Month 3 (p < 0.001 and p = 0.001). HDL cholesterol also showed a significant Δ change of +8.5 ± 4.1 mg/dL over the same period (p < 0.001). Changes in triglycerides and LDL/HDL ratio were not significant.
Data are presented as mean ± standard deviation. For triglycerides, the normality assumption was not met; hence, the Wilcoxon signed-rank test was applied. 1 p-value for the difference between baseline (0 Month) and 1 Month, 2 p-value for the difference between baseline (0 Month) and 3 Months, Paired t-test was used for parameters showing normal distribution. p-values < 0.05 were considered statistically
3. Discussion
In this real-world cohort of biologic-experienced patients with ankylosing spondylitis, upadacitinib treatment demonstrated a rapid and robust clinical impact, characterized by a significant reduction in disease activity and systemic inflammatory markers within a three-month period. Consistent with findings from pivotal clinical trials, the significant declines in BASDAI scores, CRP levels, and ESR underscore the effectiveness of upadacitinib even in a refractory population that has failed prior TNF inhibitor therapies [12]. Furthermore, the stability of most hematologic parameters and liver enzymes supports the short-term safety of this JAK1 inhibitor. Notably, while we observed quantitative increases in total cholesterol, LDL-C, and HDL-C levels, the stability of the LDL/HDL ratio and triglyceride levels suggests a preserved atherogenic index [13]. These findings indicate that the lipid shifts observed under upadacitinib therapy likely reflect the metabolic normalization associated with the suppression of high-grade systemic inflammation, rather than a de novo pro-atherogenic state [14].
The rapid and significant reductions in BASDAI scores and inflammatory markers observed in our cohort align with findings from pivotal clinical trials and emerging real-world data on upadacitinib in AS. Specifically, the SELECT-AXIS 1 and 2 trials demonstrated that upadacitinib achieves superior clinical response and improvements in objective inflammatory markers, including ASAS40 and ASDAS/CRP reductions, in both biologic-naïve and TNFi-experienced populations [15,16]. Our real-world findings mirror these results, confirming that the potent anti-inflammatory effects of JAK1 inhibition are reproducible in routine clinical practice, even among difficult-to-treat patients. Regarding metabolic shifts, extensive evidence from meta-analyses of JAK inhibitor therapy—including upadacitinib—shows consistent quantitative increases in total cholesterol, LDL-C, and HDL-C levels while the LDL/HDL ratio remains largely unchanged [17]. This pattern supports the concept of a balanced lipid elevation rather than a de novo pro-atherogenic state, consistent with the described reversal of the lipid paradox with inflammation control in systemic inflammatory diseases [18]. By extending these observations specifically to a biologic-experienced AS cohort, our study provides valuable evidence on the consistency of the upadacitinib safety and metabolic profile across different spondyloarthritis phenotypes.
The observed elevations in lipid subfractions can be interpreted within the framework of the lipid paradox seen in chronic inflammatory states [19]. High-grade systemic inflammation, characterized by elevated IL-6 and TNF levels, typically suppresses cholesterol synthesis and accelerates the catabolism of HDL and LDL, leading to lower circulating lipid levels despite high cardiovascular risk [20]. The initiation of upadacitinib therapy appears to reverse this process by effectively dampening the inflammatory cytokine storm. Our findings showed that total cholesterol, LDL-C, and HDL-C levels increased synchronously; however, the stability of the LDL/HDL ratio—a critical predictor of atherogenic risk—suggests that this is a quantitative rather than a qualitative shift. This metabolic recalibration is consistent with the hypothesis that as the inflammatory burden is lifted, lipid metabolism returns to a premorbid or normalized state [21]. Furthermore, the absence of significant changes in triglyceride levels and the preservation of the non-HDL cholesterol profile support the notion that upadacitinib does not inherently alter the lipid metabolism toward a pro-atherogenic phenotype in the short term [22].
The observed clinical efficacy of upadacitinib likely stems from its selective inhibition of JAK1, which directly modulates the signaling of key pro-inflammatory cytokines such as IL-6, IL-12, and IL-23, all of which are central to the pathogenesis of AS [23]. By effectively disrupting these pathways, upadacitinib achieves a rapid suppression of systemic inflammation, as evidenced by the significant declines in CRP and ESR, alongside marked improvements in patient-reported outcomes like the BASDAI score [24]. The concomitant increases in total cholesterol, LDL-C, and HDL-C observed in our study likely reflect a recalibration of lipid metabolism following the successful dampening of chronic inflammation—a phenomenon well-documented with JAK inhibitors, including upadacitinib, where both LDL-C and HDL-C levels rise while the LDL/HDL ratio remains stable [25]. Crucially, the stability of the LDL/HDL ratio suggests that while absolute lipid values rise, the relative atherogenic risk remains unchanged in the short term. These findings underscore that while proactive metabolic monitoring is warranted, the potent anti-inflammatory benefits of upadacitinib appear to provide a favorable benefit-risk profile during the early treatment phase in biologic-refractory AS patients [26].
The observed elevations in total cholesterol, LDL-C, and HDL-C emphasize the necessity for meticulous cardiovascular (CV) risk assessment in patients treated with upadacitinib, especially considering the inherently heightened CV burden associated with ankylosing spondylitis [27]. Although the stability of the LDL/HDL ratio in our cohort suggests a relatively neutral short-term atherogenic profile, long-term prospective studies are required to ascertain whether sustained lipid elevations translate into a clinically significant increase in major adverse cardiovascular events (MACE) [28]. Current expert consensus and pharmacovigilance guidance recommend baseline lipid screening and periodic monitoring during JAK inhibitor therapy, with lipid-lowering strategies or lifestyle interventions implemented according to individual risk profiles [29]. Our real-world data underscore that metabolic monitoring should be an integral part of routine clinical practice, ensuring that the remarkable anti-inflammatory efficacy of upadacitinib is balanced with proactive cardiovascular risk management.
Several key features strengthen the validity and clinical relevance of our findings. First, this study provides valuable real-world evidence on the use of upadacitinib specifically in biologic-experienced (100% TNFi-IR) patients with AS—a ‘difficult-to-treat’ population that is often underrepresented or strictly selected in pivotal randomized controlled trials. Second, the simultaneous evaluation of multiple clinically meaningful outcomes, ranging from patient-reported indices (BASDAI) to objective inflammatory markers and detailed lipid subfractions, allows for a comprehensive assessment of the interplay between efficacy and metabolic safety. Third, the inclusion of consecutive patients from a single tertiary care center ensured a high degree of data consistency and minimized selection bias, accurately reflecting routine rheumatological practice. Finally, the longitudinal assessment at early time points (Months 1 and 3) captured the rapid kinetics of both clinical response and lipid recalibration, providing essential practical insights for the early monitoring and cardiovascular risk management of AS patients initiating upadacitinib therapy.
Despite its strengths, several limitations of this study warrant consideration. First, the retrospective, single-center design may limit the generalizability of our findings to broader, more diverse populations and precludes the establishment of definitive causal inferences. Second, while our post-hoc power analysis confirmed sufficient power for primary clinical outcomes, the relatively modest sample size may reduce the statistical sensitivity for detecting rare adverse events or subtle metabolic shifts. Third, the short-term follow-up of 3 months restricts our ability to draw conclusions regarding the long-term sustainability of clinical responses or the potential cardiovascular consequences of the observed lipid alterations. Fourth, the absence of a parallel control group means that the observed changes cannot be unequivocally attributed to upadacitinib therapy alone, although the magnitude and temporal consistency of the effects suggest a robust treatment association. Finally, as with any retrospective study, the reliance on electronic medical records may have introduced information bias or resulted in missing data for certain secondary parameters. Notwithstanding these limitations, our study provides valuable ‘real-world’ insights into the early metabolic and clinical profile of upadacitinib in a refractory AS population.
Future research should prioritize long-term, prospective investigations in larger, multicenter cohorts of biologic-experienced AS patients to confirm the durability of upadacitinib’s clinical efficacy in real-world settings. Extended longitudinal follow-up is particularly crucial to evaluate whether the observed lipid shifts translate into long-term cardiovascular outcomes and to establish evidence-based monitoring intervals for metabolic parameters. Furthermore, head-to-head comparative studies with other JAK inhibitors or interleukin-17 inhibitors could refine treatment positioning and sequencing strategies for refractory disease. Finally, mechanistic explorations are needed to further elucidate the complex molecular pathways linking JAK inhibition, the resolution of systemic inflammation, and the subsequent recalibration of lipid metabolism.
4. Materials and Methods
4.1. Study Design and Patient Population
This retrospective cohort study was conducted at the Rheumatology Outpatient Clinic of XX University Faculty of Medicine. Medical records of patients with ankylosing spondylitis (AS) who initiated upadacitinib therapy (15 mg once daily) after an inadequate response or intolerance to at least one tumor necrosis factor inhibitor (TNFi)—including etanercept, adalimumab, infliximab, certolizumab, or golimumab—were retrospectively reviewed.
Eligible patients were required to have a confirmed diagnosis of AS according to either the Modified New York Criteria [10] or the Assessment of SpondyloArthritis international Society (ASAS) classification criteria [11], and to have received upadacitinib for clinical indications determined by the treating rheumatologist.
To ensure the validity of the metabolic and lipid analyses, patients with a history of familial hyperlipidemia, those receiving lipid-lowering therapy (statins or fibrates) at baseline, or those with incomplete clinical or laboratory data at baseline or during follow-up were excluded from the study.
The study protocol was approved by the XX University Faculty of Medicine Ethics Committee for Noninterventional Studies (Approval No: 6; Date: 24/12/2025) and was conducted in accordance with the principles of the Declaration of Helsinki. Owing to the retrospective nature of the study, the requirement for informed consent was waived by the Ethics Committee.
The patient selection process is summarized in Figure 3, which illustrates the inclusion and exclusion criteria applied to the initial cohort of AS patients evaluated for upadacitinib treatment following an inadequate response or intolerance to TNF inhibitors.
4.2. Clinical and Laboratory Assessments
Baseline demographic characteristics, disease duration, and concomitant medications—including non-steroidal anti-inflammatory drugs (NSAIDs), conventional synthetic disease-modifying antirheumatic drugs (csDMARDs; methotrexate, sulfasalazine, leflunomide), and low-dose oral corticosteroids (≤10 mg/day prednisolone equivalent)—were extracted from electronic medical records.
Disease activity was assessed using the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI). BASDAI scores were recorded at baseline and at Months 1 and 3 following the initiation of upadacitinib therapy to evaluate longitudinal changes in clinical response.
Laboratory assessments were performed on fasting venous blood samples obtained after at least 8 hours of fasting at baseline and during follow-up visits (Months 1 and 3). Inflammatory markers included C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). Hematologic parameters comprised white blood cell count, hemoglobin, platelet count, and absolute lymphocyte count. Metabolic and safety assessments included alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum albumin, fasting glucose, and creatine kinase (CK) levels.
A comprehensive lipid profile was evaluated, including total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglycerides (TG). Secondary lipid indices—non-HDL cholesterol (TC minus HDL-C) and the LDL/HDL ratio—were calculated to further characterize the atherogenic lipid profile.
All clinical and laboratory parameters were analyzed longitudinally to assess the short-term effects of upadacitinib on disease activity, systemic inflammation, and metabolic homeostasis in patients with ankylosing spondylitis.
4.3. Statistical Analysis
Statistical analyses were performed using SPSS software, version 27.0 (IBM Corp., Armonk, NY, USA). The normality of continuous variables was assessed using the Kolmogorov–Smirnov test, complemented by visual inspection of Q–Q plots. Continuous variables were expressed as mean ± standard deviation (SD) for normally distributed data and as median with interquartile range (IQR) for non-normally distributed data. Categorical variables were summarized as frequencies and percentages.
Longitudinal changes in clinical and laboratory parameters measured at baseline, Month 1, and Month 3 were analyzed using repeated-measures analysis of variance (ANOVA) for normally distributed variables. For variables that did not satisfy normality assumptions, the Friedman test was applied. When overall comparisons were statistically significant, post hoc pairwise comparisons with Bonferroni correction were performed to identify differences between specific time points.
For direct comparisons between two predefined time points (baseline vs. Month 1 and baseline vs. Month 3), the paired-sample t-test was used for normally distributed variables, whereas the Wilcoxon signed-rank test was applied for non-normally distributed variables.
All statistical tests were two-tailed, and a p-value < 0.05 was considered statistically significant. To evaluate the adequacy of the sample size, a post hoc power analysis was conducted using G*Power software (version 3.1.9.7). Based on the primary clinical outcome—change in BASDAI score from baseline to Month 3—with an assumed effect size of 0.5 and an alpha level of 0.05, the sample size of 61 patients yielded a statistical power exceeding 90%, indicating that the study was sufficiently powered to detect clinically meaningful changes over time.
5. Conclusions
In conclusion, this real-world study demonstrates that upadacitinib provides rapid and significant clinical improvement and potent anti-inflammatory effects in biologic-refractory patients with ankylosing spondylitis. While upadacitinib therapy is associated with quantitative increases in total cholesterol, LDL-C, and HDL-C levels within the first three months, the stability of the LDL/HDL ratio suggests a metabolic normalization—consistent with the reversal of the inflammatory lipid paradox—rather than an immediate pro-atherogenic shift. These findings underscore the favorable short-term safety and efficacy of upadacitinib in a difficult-to-treat AS population. Nevertheless, given the chronic nature of AS and its associated cardiovascular burden, our results highlight the importance of integrating proactive metabolic monitoring into routine clinical practice to ensure a balanced approach between disease control and long-term cardiovascular risk management.
Author Contributions
Conceptualization, Z.A.A. and D.Y.; methodology, Ö.K.; software, Z.A.A.; validation, M.Ç.; formal analysis, Z.A.A.; investigation, D.Y.; resources, Ö.K.; data curation, D.Y.; writing—original draft preparation, Z.A.A.; writing—review and editing, M.Ç.; visualization, Ö.K.; supervision, M.Ç.; project administration, D.Y.; funding acquisition, Z.A.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of Dicle University Faculty of Medicine Ethics Committee for Noninterventional Studies (Approval No: 6; Date: 24/12/2025).
Informed Consent Statement
Patient consent was waived due to retrospective nature of the study.
Data Availability Statement
The data that support the findings of this study are not publicly available due to ethical and privacy restrictions but are available from the corresponding author upon reasonable request.
Acknowledgments
The authors have no acknowledgments to declare.The authors have reviewed and edited the output and take full responsibility for the content of this publication.”.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AS | Ankylosing Spondylitis |
| PsA | Psoriatic Arthritis |
| CVD | Cardiovascular Disease |
| TNFi | Tumor Necrosis Factor Inhibitor |
| IL-17i | Interleukin-17 Inhibitor |
| JAK | Janus Kinase |
| STAT | Signal Transducer and Activator of Transcription |
| CRP | C-Reactive Protein |
| ESR | Erythrocyte Sedimentation Rate |
| BASDAI | Bath Ankylosing Spondylitis Disease Activity Index |
| NSAIDs | Non-Steroidal Anti-Inflammatory Drugs |
| csDMARDs | Conventional Synthetic Disease-Modifying Anti-Rheumatic Drugs |
| ALT | Alanine Aminotransferase |
| AST | Aspartate Aminotransferase |
| CK | Creatine Kinase |
| TC | Total Cholesterol |
| LDL-C | Low-Density Lipoprotein Cholesterol |
| HDL-C | High-Density Lipoprotein Cholesterol |
| TG | Triglycerides |
| MACE | Major Adverse Cardiovascular Events |
References
- Braun, J.; Sieper, J. Ankylosing spondylitis. Lancet 2007, 369, 1379–1390. [Google Scholar] [CrossRef]
- Mathieu, S.; Gossec, L.; Dougados, M.; Soubrier, M. Cardiovascular profile in ankylosing spondylitis: a systematic review and meta-analysis. Arthritis Care Res (Hoboken) 2011, 63, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Deodhar, A.; Strand, V.; Conaghan, P.G.; Sullivan, E.; Blackburn, S.; Tian, H.; Gandhi, K.; Jugl, S.M.; Alten, R. Unmet needs in ankylosing spondylitis patients receiving tumour necrosis factor inhibitor therapy; results from a large multinational real-world study. BMC Rheumatol. 2020, 4, 19. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Biehl, A.; Gadina, M.; Hasni, S.; Schwartz, D.M. JAK-STAT Signaling as a Target for Inflammatory and Autoimmune Diseases: Current and Future Prospects. Drugs. 2017, 77, 521-546. https://doi.org/10.1007/s40265-017-0701-9. Erratum in: Drugs. 2017, 77, 939. https://doi.org/10.1007/s40265-017-0736-y. Erratum in: Drugs. 2017, 7s7, 1261. https://doi.org/10.1007/s40265-017-0772-7.
- Baraliakos, X.; van der Heijde, D.; Sieper, J.; Inman, R.D.; Kameda, H.; Maksymowych, W.P.; Lagunes-Galindo, I.; Bu, X.; Wung, P.; Kato, K.; Shmagel, A.; Deodhar, A. Efficacy and safety of upadacitinib in patients with active ankylosing spondylitis refractory to biologic therapy: 2-year clinical and radiographic results from the open-label extension of the SELECT-AXIS 2 study. Arthritis Res Ther. 2024, 26, 197. [Google Scholar] [CrossRef]
- Garmish, O.; Smiyan, S.; Hladkykh, F.; Koshak, B.; Komorovsky, R. The Effects of Disease-Modifying Antirheumatic Drugs on Cardiovascular Risk in Inflammatory Joint Diseases: Current Evidence and Uncertainties. Vasc Health Risk Manag. 2025, 21, 593–605. [Google Scholar] [CrossRef]
- Schwartz, D.M.; Kanno, Y.; Villarino, A.; Ward, M.; Gadina, M.; O’Shea, J.J. JAK inhibition as a therapeutic strategy for immune and inflammatory diseases. Nat Rev Drug Discov. 2017, 16, 843–862. https://doi.org/10.1038/nrd.2017.201. Epub 2017 Nov 6. Erratum in: Nat Rev Drug Discov. 2017, 17, 78. https://doi.org/10.1038/nrd.2017.267.
- Burmester, G.R.; Cohen, S.B.; Winthrop, K.L.; Nash, P.; Irvine, A.D.; Deodhar, A.; Mysler, E.; Tanaka, Y.; Liu, J.; Lacerda, A.P.; Palac, H.; Shaw, T.; Mease, P.J.; Guttman-Yassky, E. Safety profile of upadacitinib over 15 000 patient-years across rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis and atopic dermatitis. RMD Open. 2023, 9, e002735. [Google Scholar] [CrossRef]
- Papagoras, C.; Markatseli, T.E.; Saougou, I.; Alamanos, Y.; Zikou, A.K.; Voulgari, P.V.; Kiortsis, D.N.; Drosos, A.A. Cardiovascular risk profile in patients with spondyloarthritis. Joint Bone Spine 2014, 81, 57–63. [Google Scholar] [CrossRef]
- van der Linden, S.; Valkenburg, H.A.; Cats, A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 1984, 27, 361–368. [Google Scholar] [CrossRef]
- Rudwaleit, M.; van der Heijde, D.; Landewé, R.; Listing, J.; Akkoc, N.; Brandt, J.; Braun, J.; Chou, C.T.; Collantes-Estevez, E.; Dougados, M.; Huang, F.; Gu, J.; Khan, M.A.; Kirazli, Y.; Maksymowych, W.P.; Mielants, H.; Sørensen, I.J.; Ozgocmen, S.; Roussou, E.; Valle-Oñate, R.; Weber, U.; Wei, J.; Sieper, J. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): validation and final selection. Ann Rheum Dis. 2009, 68, 777–783. [Google Scholar] [CrossRef]
- van der Heijde D, Baraliakos X, Sieper J, Deodhar A, Inman RD, Kameda H, Zeng X, Sui Y, Bu X, Pangan AL, Wung P, Song IH. Efficacy and safety of upadacitinib for active ankylosing spondylitis refractory to biological therapy: a double-blind, randomised, placebo-controlled phase 3 trial. Ann Rheum Dis. 2022, 81, 1515–1523. [CrossRef] [PubMed]
- Popescu, D.; Badescu, M.C.; Rezus, E.; Tanase, D.M.; Ouatu, A.; Dima, N.; Buliga-Finis, O.N.; Gosav, E.M.; Rezus, C. Effects of Janus Kinase Inhibitors on Cardio-Vascular Risk in Rheumatic Diseases: A Prospective Pilot Study. J Clin Med. 2025, 14, 4676. [Google Scholar] [CrossRef]
- Kwan, A.; Ingrid, E.; Jiang, M.; Lim, K.K.T. The cardiovascular risk of JAK inhibitors in treating rheumatic diseases. Int J Rheum Dis. 2024, 27, e15308. [Google Scholar] [CrossRef]
- van der Heijde, D.; Song, I.H.; Pangan, A.L.; Deodhar, A.; van den Bosch, F.; Maksymowych, W.P.; Kim, T.H.; Kishimoto, M.; Everding, A.; Sui, Y.; Wang, X.; Chu, A.D.; Sieper, J. Efficacy and safety of upadacitinib in patients with active ankylosing spondylitis (SELECT-AXIS 1): a multicentre, randomised, double-blind, placebo-controlled, phase 2/3 trial. Lancet 2019, 394, 2108–2117. [Google Scholar] [CrossRef]
- Baraliakos, X.; van der Heijde, D.; Sieper, J.; Inman, R.D.; Kameda, H.; Maksymowych, W.P.; Lagunes-Galindo, I.; Bu, X.; Wung, P.; Kato, K.; Shmagel, A.; Deodhar, A. Efficacy and safety of upadacitinib in patients with active ankylosing spondylitis refractory to biologic therapy: 2-year clinical and radiographic results from the open-label extension of the SELECT-AXIS 2 study. Arthritis Res Ther. 2024, 26, 197. [Google Scholar] [CrossRef]
- Clarke, B.; Yates, M.; Adas, M.; Bechman, K.; Galloway, J. The safety of JAK-1 inhibitors. Rheumatology 2021, 60, ii24–ii30. [Google Scholar] [CrossRef]
- Paolino, G.; Valenti, M.; Carugno, A.; Bianco, M.; Didona, D.; Di Nicola, M.R.; Acutis, P.L.; Cantisani, C.; Bianchi, V.G.; Zerbinati, N.; Narcisi, A.; Costanzo, A.; Mercuri, S.R. Serum Lipids Alterations in Patients Under Systemic JAK Inhibitors Treatments in Dermatology: Clinical Aspects and Management. Medicina (Kaunas) 2025, 61, 54. [Google Scholar] [CrossRef]
- Myasoedova, E.; Crowson, C.S.; Kremers, H.M.; Roger, V.L.; Fitz-Gibbon, P.D.; Therneau, T.M.; Gabriel, S.E. Lipid paradox in rheumatoid arthritis: the impact of serum lipid measures and systemic inflammation on the risk of cardiovascular disease. Ann Rheum Dis. 2011, 70, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Thurmann, K.E.; Mukherjee, T.G.; White, M.D. Inflammation-Driven Lipid Suppression in Hospitalized Patients: Insights Into the Inflammatory Lipid Paradox From a Retrospective Study. Cureus 2025, 17, e89488. [Google Scholar] [CrossRef] [PubMed]
- Makris, A.; Barkas, F.; Sfikakis, P.P.; Liberopoulos, E.; Agouridis, A.P. The Effect of Upadacitinib on Lipid Profile and Cardiovascular Events: A Meta-Analysis of Randomized Controlled Trials. J Clin Med. 2022, 11, 6894. [Google Scholar] [CrossRef]
- Özdoğan, O.; Yaraş, S. Upadacitinib in Biologic-Experienced Inflammatory Bowel Disease: Real-World Efficacy, Safety, and Laboratory Outcomes. Medicina (Kaunas) 2025, 61, 1692. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, M.F.; Bhatnagar, S.; Parmentier, J.M.; Nakasato, P.; Wung, P. Upadacitinib: Mechanism of action, clinical, and translational science. Clin Transl Sci. 2024, 17, e13688. [Google Scholar] [CrossRef]
- Yao, Q.; Zhu, Y.; Ma, Y.; Pu, Y.; Yang, X.; Zhang, Z. Efficacy and safety of upadacitinib, a selective JAK-1 inhibitor in treatment of ankylosing spondylitis: a meta-analysis. BMC Rheumatol. 2025, 9, 19. [Google Scholar] [CrossRef]
- Isufi, D.; Javanmardi, N.; Jensen, M.B.; Loft, N.; Skov, L.; Elberling, J.; Thomsen, S.F.; Alinaghi, F. Risk of Dyslipidemia Associated With Oral Janus Kinase Inhibitors: A Systematic Review and Meta-Analysis of Randomized Placebo-Controlled Trials. Int J Dermatol 2025. [Google Scholar] [CrossRef]
- Charles-Schoeman, C.; Giles, J.T.; Lane, N.E.; Choy, E.; Furst, D.E.; Vencovský, J.; Wilson, A.G.; Burmester, G.R.; Coombs, D.; Penn, S.K.; Khan, N.; Yee, J.B.; Rahawi, K.; McInnes, I.B. Impact of Upadacitinib on Laboratory Parameters and Related Adverse Events in Patients with RA: Integrated Data Up to 6.5 Years. Rheumatol Ther. 2024, 11, 157–175. [Google Scholar] [CrossRef] [PubMed]
- Klisic, A.; Kotur-Stevuljevic, J.; Cure, O.; Kizilkaya, B.; Beyazal Celiker, F.; Er, H.; Mercantepe, F. Cardiovascular Risk in Patients with Ankylosing Spondylitis. J Clin Med. 2024, 13, 6064. [Google Scholar] [CrossRef] [PubMed]
- Issakulova, А.; Yessirkepov, M.; Zimba, O.; Kocyigit, B.F. Cardiovascular risk in axial spondyloarthritis: the interplay of inflammation, traditional risk factors, and management strategies. Rheumatol Int. 2025, 45, 214. [Google Scholar] [CrossRef] [PubMed]
- Yang, V.; Kragstrup, T.W.; McMaster, C.; Reid, P.; Singh, N.; Haysen, S.R.; Robinson, P.C.; Liew, D.F.L. Managing Cardiovascular and Cancer Risk Associated with JAK Inhibitors. Drug Saf. 2023, 46, 1049–1071. [Google Scholar] [CrossRef]
Figure 1.
Short-term effects of upadacitinib on disease activity and inflammation. Line graphs depict the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) scores (left axis) and C-reactive protein (CRP, mg/L; right axis) at baseline, Month 1, and Month 3. Both parameters show a marked decrease, indicating that upadacitinib exerts rapid clinical and anti-inflammatory effects within the first month of treatment.
Figure 1.
Short-term effects of upadacitinib on disease activity and inflammation. Line graphs depict the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) scores (left axis) and C-reactive protein (CRP, mg/L; right axis) at baseline, Month 1, and Month 3. Both parameters show a marked decrease, indicating that upadacitinib exerts rapid clinical and anti-inflammatory effects within the first month of treatment.
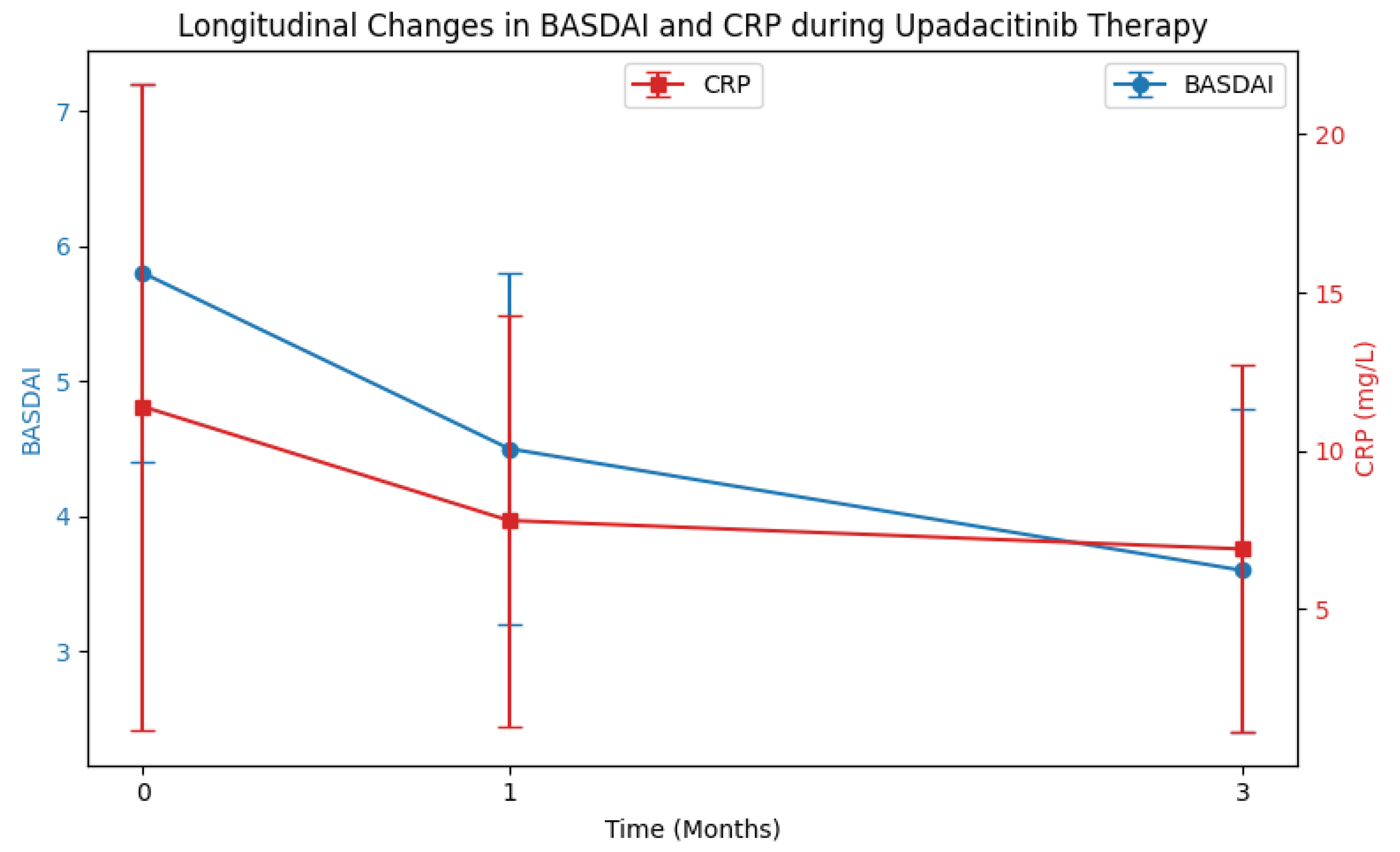
Figure 2.
Short-term effects of upadacitinib on lipid profile. Panel A: Total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C) levels at baseline and Month 3. Asterisks (*) indicate p < 0.05, representing statistically significant increases. Panel B: LDL/HDL ratio at baseline and Month 3. Thin bars with different colors were used (baseline: blue, Month 3: salmon). The ratio remained stable, demonstrating that despite increases in lipid subfractions, the atherogenic profile is preserved.
Figure 2.
Short-term effects of upadacitinib on lipid profile. Panel A: Total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C) levels at baseline and Month 3. Asterisks (*) indicate p < 0.05, representing statistically significant increases. Panel B: LDL/HDL ratio at baseline and Month 3. Thin bars with different colors were used (baseline: blue, Month 3: salmon). The ratio remained stable, demonstrating that despite increases in lipid subfractions, the atherogenic profile is preserved.
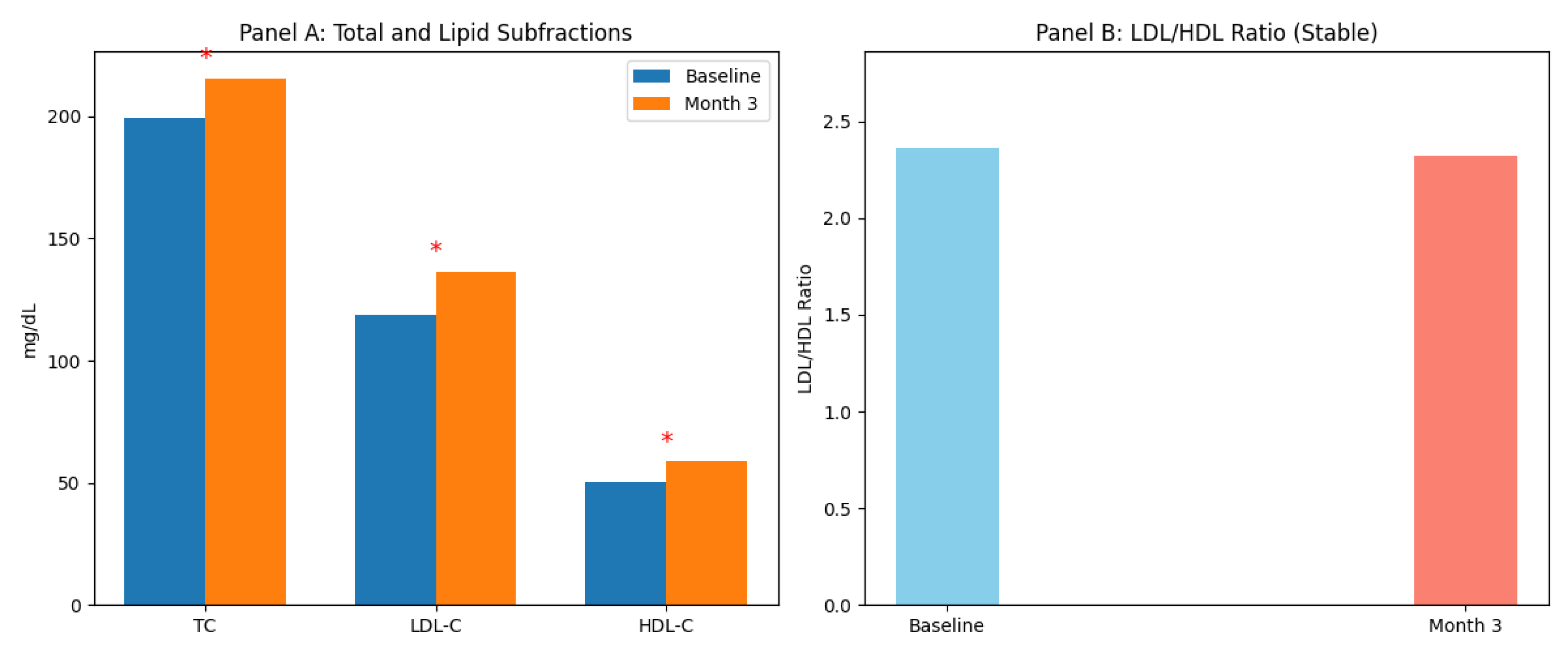
Figure 3.
Patient Selection Flowchart. This flowchart illustrates the inclusion and exclusion process for ankylosing spondylitis (AS) patients who initiated upadacitinib therapy. Inclusion criteria: inadequate response or intolerance to at least one TNF inhibitor, confirmed AS diagnosis according to the Modified New York or ASAS criteria. Exclusion criteria: history of familial hyperlipidemia, use of lipid-lowering therapy at baseline, or incomplete clinical/laboratory data.
Figure 3.
Patient Selection Flowchart. This flowchart illustrates the inclusion and exclusion process for ankylosing spondylitis (AS) patients who initiated upadacitinib therapy. Inclusion criteria: inadequate response or intolerance to at least one TNF inhibitor, confirmed AS diagnosis according to the Modified New York or ASAS criteria. Exclusion criteria: history of familial hyperlipidemia, use of lipid-lowering therapy at baseline, or incomplete clinical/laboratory data.
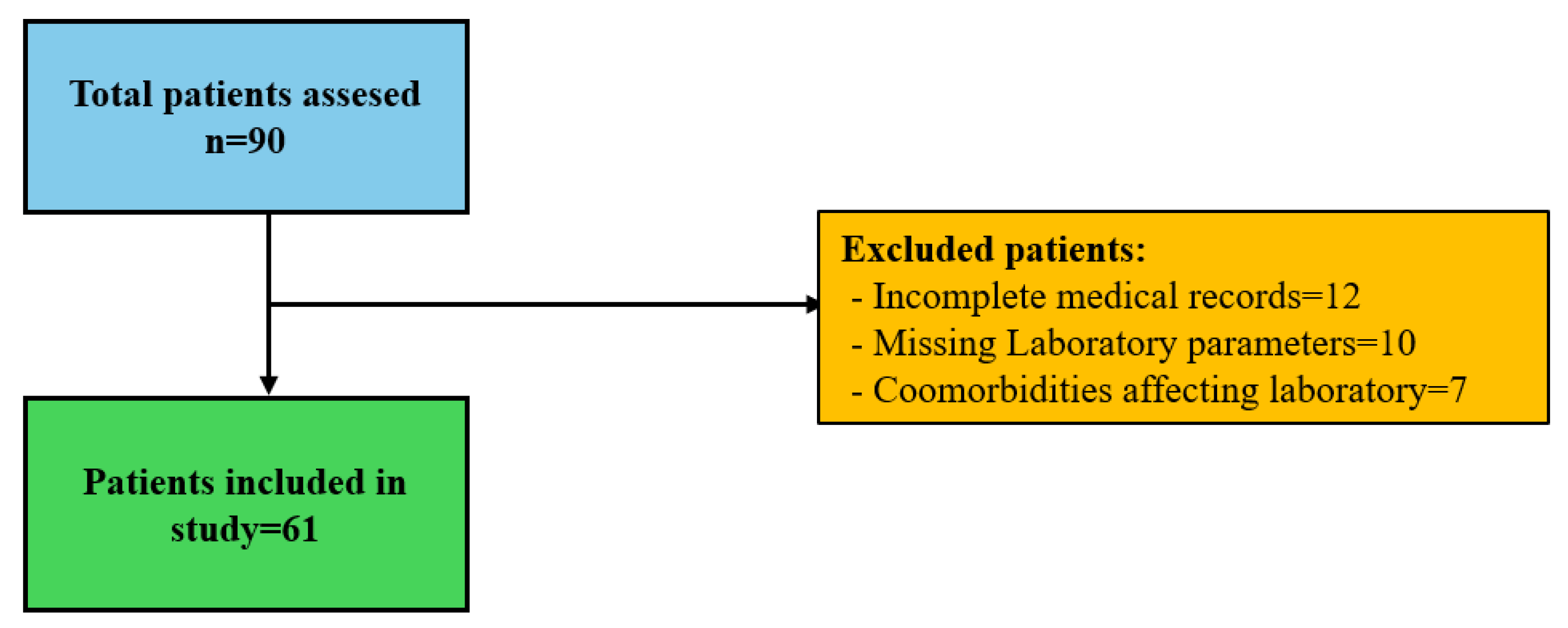

Table 1.
Demographic and Baseline Clinical Characteristics of Participants (n = 61).
| Variable | Value (n = 61) |
|---|---|
| Age (years) | 42.6 ± 10.8 |
| Sex, n (%) | |
| Female | 27 (44.3) |
| Male | 34 (55.7) |
| Disease duration (years) | 8 [4,5,6,7,8,9,10,11,12,13] |
| Diagnosis, n (%) | |
| Ankylosing Spondylitis (AS) | 51 (83.6) |
| Psoriatic Arthritis (PsA) / Other | 10 (16.4) |
| Baseline disease activity, Mean ± SD | |
| BASDAI score | 5.8 ± 1.4 |
| CRP (mg/L) | 11.4 ± 10.2 |
| ESR (mm/h) | 14.6 ± 11.5 |
| History of biologic therapy, n (%) | |
| Biologic-experienced (TNFi-IR) | 61 (100) |
| Used 1 TNF inhibitor | 37 (60.7) |
| Used 2 TNF inhibitors | 18 (29.5) |
| Used ≥3 TNF inhibitors | 6 (9.8) |
| Previous Secukinumab (IL-17i) use | 14 (22.9) |
| Concomitant treatments, n (%) | |
| Conventional DMARDs (MTX, SSZ, LEF) | 11 (18.0) |
| NSAID use | 18 (29.5) |
| Low-dose glucocorticoids | 6 (9.8) |
Table 2.
Inflammatory markers and disease activity during Upadacitinib treatment (n = 61).
| Parameter | Baseline (Month 0) | Month 1 | Month 3 | p-value |
|---|---|---|---|---|
| CRP (mg/L) | 11.4 ± 10.2 | 7.8 ± 6.5 | 6.9 ± 5.8 | <0.001 |
| ESR (mm/h) | 14.6 ± 11.5 | 11.2 ± 9.8 | 10.4 ± 8.7 | 0.002 |
| BASDAI score | 5.8 ± 1.4 | 4.2 ± 1.3 | 3.6 ± 1.2 | <0.001 |
Table 3.
Changes in Hematologic, Metabolic, and Muscle Enzyme Parameters During Upadacitinib Treatment (n = 61).
Table 3.
Changes in Hematologic, Metabolic, and Muscle Enzyme Parameters During Upadacitinib Treatment (n = 61).
| Parameter | Baseline (0 Month) | 1 Month | 3 Months | p-value |
|---|---|---|---|---|
| Hematologic | ||||
| WBC (×103/μL) | 8.85 ± 2.1 | 8.14 ± 1.8 | 8.22 ± 1.9 | 0.064 |
| Hemoglobin (g/dL) | 13.6 ± 1.4 | 13.9 ± 1.2 | 14.1 ± 1.3 | 0.032 |
| Lymphocyte (×103/μL) | 2.65 ± 0.8 | 2.42 ± 0.7 | 2.51 ± 0.8 | 0.115 |
| Platelet (×103/μL) | 315 ± 78 | 288 ± 65 | 294 ± 72 | 0.028 |
| Metabolic & Liver | ||||
| ALT (U/L) | 24.8 ± 12.4 | 26.1 ± 14.2 | 27.5 ± 15.8 | 0.452 |
| AST (U/L) | 21.4 ± 8.6 | 22.8 ± 9.4 | 23.1 ± 10.2 | 0.512 |
| Albumin (g/dL) | 4.1 ± 0.4 | 4.3 ± 0.3 | 4.4 ± 0.3 | 0.005 |
| Glucose (mg/dL) | 94.6 ± 15.2 | 96.2 ± 12.8 | 95.8 ± 14.1 | 0.841 |
| Creatine Kinase (CK) (U/L) | 112.4 ± 54.8 | 138.6 ± 62.1 | 144.2 ± 68.5 | 0.012 |
Table 4.
Changes in Lipid Parameters During Upadacitinib Treatment (n = 61).
| Parameter (mg/dL) | Baseline (0 Month) | 1 Month | 3 Months | p-value* |
|---|---|---|---|---|
| Total Cholesterol | 199.4 ± 41.2 | 211.8 ± 38.5 | 215.6 ± 35.4 | 0.001 |
| LDL-Cholesterol | 118.7 ± 33.6 | 130.2 ± 31.4 | 136.5 ± 29.8 | 0.003 |
| HDL-Cholesterol | 50.2 ± 12.4 | 56.4 ± 13.8 | 58.7 ± 11.5 | 0.001 |
| Triglycerides | 145.8 ± 72.1 | 154.2 ± 68.4 | 148.6 ± 62.3 | 0.412 |
| Non-HDL Cholesterol | 149.2 ± 38.5 | 155.4 ± 36.2 | 156.9 ± 34.1 | 0.008 |
| LDL/HDL Ratio | 2.36 ± 0.8 | 2.31 ± 0.7 | 2.32 ± 0.6 | 0.845 |
Table 5.
Changes in Lipid Parameters from Baseline During Follow-up (n = 61).
| Parameter (mg/dL) | Δ (0–1 Month) (Mean ± SD) | p1 | Δ (0–3 Months) (Mean ± SD) | p2 |
|---|---|---|---|---|
| Total Cholesterol | +12.4 ± 8.6 | 0.004 | +16.2 ± 9.1 | <0.001 |
| LDL-Cholesterol | +11.5 ± 7.2 | 0.008 | +17.8 ± 8.4 | 0.001 |
| HDL-Cholesterol | +6.2 ± 3.5 | 0.002 | +8.5 ± 4.1 | <0.001 |
| Triglycerides* | +8.4 ± 12.5 | 0.158 | +2.8 ± 14.2 | 0.482 |
| LDL/HDL Ratio | −0.05 ± 0.12 | 0.624 | −0.04 ± 0.15 | 0.812 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



